 Flavien Quijoux1,2*
Flavien Quijoux1,2* François Bertin-Hugault2Philippe Zawieja2Marie Lefèvre2
François Bertin-Hugault2Philippe Zawieja2Marie Lefèvre2 Pierre-Paul Vidal1,3Damien Ricard1,4,5
Pierre-Paul Vidal1,3Damien Ricard1,4,5- 1Centre Borelli UMR 9010/Université Paris-Saclay, ENS Paris-Saclay, CNRS, SSA, Université de Paris, Inserm, Paris, France
- 2ORPEA Group, Puteaux, France
- 3Institute of Information and Control, Hangzhou Dianzi University, Hangzhou, China
- 4Service de Neurologie de l'Hôpital d'Instruction des Armées de Percy, Service de Santé des Armées, Clamart, France
- 5Ecole du Val-de-Grâce, Ecole de Santé des Armées, Paris, France
Introduction: While falls among the elderly is a public health issue, because of the social, medical, and economic burden they represent, the tools to predict falls are limited. Posturography has been developed to distinguish fallers from non-fallers, however, there is too little data to show how predictions change as older adults' physical abilities improve. The Postadychute-AG clinical trial aims to evaluate the evolution of posturographic parameters in relation to the improvement of balance through adapted physical activity (APA) programs.
Methods: In this prospective, multicentre clinical trial, institutionalized seniors over 65 years of age will be followed for a period of 6 months through computer-assisted posturography and automatic gait analysis. During the entire duration of the follow-up, they will benefit from a monthly measurement of their postural and locomotion capacities through a recording of their static balance and gait thanks to a software developed for this purpose. The data gathered will be correlated with the daily record of falls in the institution. Static and dynamic balance measurements aim to extract biomechanical markers and compare them with functional assessments of motor skills (Berg Balance Scale and Mini Motor Test), expecting their superiority in predicting the number of falls. Participants will be followed for 3 months without APA and 3 months with APA in homogeneous group exercises. An analysis of variance will evaluate the variability of monthly measures of balance in order to record the minimum clinically detectable change (MDC) as participants improve their physical condition through APA.
Discussion: Previous studies have stated the MDC through repeated measurements of balance but, to our knowledge, none appear to have implemented monthly measurements of balance and gait. Combined with a reliable measure of the number of falls per person, motor capacities and other precipitating factors, this study aims to provide biomechanical markers predictive of fall risk with their sensitivity to improvement in clinical status over the medium term. This trial could provide the basis for posturographic and gait variable values for these elderly people and provide a solution to distinguish those most at risk to be implemented in current practice in nursing homes.
Trial Registration: ID-RCB 2017-A02545-48.
Protocol Version: Version 4.2 dated January 8, 2020.
1. Introduction
Elderly falls are defined by the World Health Organization as “an event in which a person [over the age of 65] inadvertently falls to a lower level on the ground or any other surface than where he or she was previously” (1). But behind this simple definition, the falls of frail people bring together many economic and social issues. The incidence of falls among people over 65 years old is estimated at 30% (2). With the risk of falling increasing with age, 24% of people over 80 years old fall recurrently (i.e., at least twice a year) (3). It was estimated in 2004 in France that 450,000 accidents requiring a visit to hospital emergency departments were linked to falls, making it the most common accident in everyday life. Among these accidents, there were nearly 9,000 fatal falls of elderly people (4). Although the percentage of fatal falls remains low, the consequences are both frequent and disabling. The main factors identified by the French Health Authority (5) are (1) the age of the person, (2) the institutionalization (39% of the residents of retirement homes had at least two falls in 1 year), and (3) the polymorbidity, although this factor is not specific, is an important risk factor. Institutionalized people over 75 years of age have the highest fall rates with 0.6 to 3.6 falls per person per year (6, 7). Frailty, defined as a precarious state where physiological and social factors may increase an existing functional loss (8), must be taken into account to prevent falls. The frailty of elderly people should be measured through the following indicators: weight loss, self-reported exhaustion, physical weakness, slow walking speed, and low physical activity. Although screening for these risk factors is common in geriatric care, the analysis of these factors alone does not provide sufficient sensitivity and specificity to identify individuals at high risk of falling (9). Given these limitations, exhaustive analysis of the fall risk factors has only a limited value, and in practice, a questionnaire on the history of falls and the expertise of the professional are more often preferred to identify people who will eventually fall in the coming months (10).
To quantify the risk of falling in older population, static posturography can then be used (11–14). It examines the orientation and body movements during a quiet stance task through a force platform and the computation of the center of pressure (COP) trajectory. Still, this recording remains an examination reserved to specialists of human biomechanics (15, 16). Indeed, this method could not be applied in current practice mainly because of its ergonomics, cost, and the difficulty of interpreting the results. On the other hand, the development of portable force platforms, such as the Wii Balance Board (WBB) [Nintendo, Tokyo, Japan], has democratized the use of static posturography. The reliability of the measurements made with the WBB has been studied extensively (17–23). With the WBB, it is possible to measure the total sway path length, the mean velocity of the COP, the sway area enclosing the COP displacement, and other parameters classically used for postural control analysis (14, 24–26). However, their statistical interpretation is usually time consuming and incompatible with clinical practice. In addition, the number of parameters derived from the COP trajectory can quickly exceed several dozen and the experimental recording conditions vary greatly between studies (27). Determining which parameters in which experimental conditions are optimal to discriminate future fallers from elderly non-faller remains a difficult task (28–30).
Similarly, it can be interesting to look for predictive markers in the gait analysis, since falling is also correlated with gait disorders (31–33). Thus, by adding inertial measurement units (IMU) on different segments of the body, it is possible to study the spatiotemporal alteration of the gait due to aging or pathologies through inertialocography (ILG) (34, 35) Biomechanics parameters in gait analysis (such as gait speed, number of steps for a U turn, average duration of a step, and so on) allow an early identification of future fallers (36, 37). However, while these two methods of analysis of static and dynamic balance, posturography and ILG, respectively, provide clues for the early detection of elderly people at risk of falling, few studies combine both (38–41). Once identified, people at high risk of falling could then benefit from an optimized and individualized follow-up. Yet, few studies have quantified the variability of biomechanical parameters during longitudinal monitoring, although these data are essential to demonstrate a deviation from the normal evolution of these parameters. This study aims at determining the evolution of the computed predictive markers to physical capacities improvement in elderly people living in nursing home.
Concerning the risk of falling, adapted physical activity (APA) has shown its benefits (42, 43). In addition to reducing the number of falls in the elderly (44–47), APA has shown an improvement in clinical and functional tests (48, 49) as well as in biomechanical markers related to falls in static (50) and dynamic balance (51). Although there is no consensus on the definition of APA, particularly with regard to sports practices or functional tasks included in daily life activities (52), adapted exercises include physical activities of various intensities and generally multi-component. According to the 2008 Physical Activity Guidelines for Americans (53), “exercise is a form of physical activity that is planned, structured, repetitive, and performed with the goal of improving health or fitness.” Physical exercises can be proposed in order to improve predictive markers, gait quality, and finally functional test scores. Therefore, it would be appropriate to provide older persons with the right rehabilitation program to improve their balancing abilities. Non-medication and exercise-based interventions have indeed shown significant effects on the number of falls and associated trauma (54), quantified by a median absolute reduction of 3 falls per participant and a lower rate of traumatic falls by a median reduction of 0.35 traumatic falls per person-year (55). The American Geriatrics Society (46) reported a positive impact of APA, in general, on the physical capacities of the elderly without noting any correlation between the duration or intensity of the efforts and the expected benefits. This difficulty in determining the best program for each individual is also retained by the Cochrane Collaboration, which indicates in its meta-analysis a mitigated effect of interventions to reduce the risk of falls for nursing home residents (44). Hence, despite the recommendations regarding APA for elderly people (56), no optimal APA program seems to be clearly described, especially for nursing home residents (44). In addition, the impact of APA on motor capacities of people with mild-to-severe cognitive impairments remains a matter of debate (57). This highlights the challenge of optimizing the follow-up of elderly people following physical exercise programs.
2. Method and Design
2.1. Aim and Objectives
As part of a wider project aiming to develop a numeric tool for individual longitudinal monitoring using quantitative approaches (58), the objective of the Postadychute-AG clinical trial is to validate the reliability of predictive models previously published (59–63) on prospective follow-up of institutionalized older adults and to quantify their sensitivity to physical rehabilitation. In order to achieve this objective, the risk of falls predicted each month by means of instrumental assessment of balance and gait, respectively, via posturography and ILG, will be compared with the number of falls actually recorded during that month by the nursing home's medical staff. Falls will be recorded daily using a standardized form.
We hypothesize that a score based on both evaluations of static and dynamic balance allows a reliable and unequaled estimation of the risk of falling, after selection of the best biomechanics parameters. This selection is based on systematic reviews (30, 35, 64), machine learning algorithms from previous recordings (11, 12), and on an analysis of locomotion made in consultation for patients with or without neurological disorders (65).
A previous prospective study has shown the value of combining static and dynamic balance analysis to predict the risk of falling in the elderly (66). However, limited data are available for institutionalized people. On the other hand, an improvement in the quality of static balance and gait can be expected after 3 months of physical training (67, 68). The sensitivity of predictive models to the improvement of physical abilities (or their deterioration) remains unknown. Hence, this represents a major challenge to guide rehabilitation and optimize care in order to reduce the number of falls and their consequences (69).
The secondary objective of the Postadychute-AG clinical trial is to evaluate the acceptability of the measurement method by the healthcare personals of the selected nursing homes. If the results of the study prove to be relevant and the instrumental assessment method is well-received by carers, the ultimate goal is to eventually recommend the use of these balance and gait measurements to assist professionals in the diagnosis and management of balance disorders.
2.2. Trial Design
This study is a low-risk and low-constraint multicenter clinical trial following prospectively a cohort of older people (≥ 65 years old) in 16 institutions. Each nursing home will enroll 5–15 participants for 6 months, then renew the list of participants at the end of the 6-month follow-up. All the selected residents from the 16 nursing homes will be included in an APA program after 3 months of follow-up. Hence, they will be monitored during 3 months without APA and then 3 more months with APA. Four different APA programs are planned. One or two APA programs, among the four possible, are then chosen by the healthcare team and can be changed after the 6-month follow-up. The comparisons will be intra-individuals in the different programs, i.e., between pre-APA and post-APA evaluations in a pairwise manner.
To the extent that APA reduces the risk of falling in institutionalized elderly patients (70), we want to test the robustness of the developed predictive models on the evolution of the risk of falling. The objective is to evaluate the sensitivity of models using static and dynamic balance predictive markers. The first 3 months of follow-up without APA will thus serve as a baseline to quantify the evolution of the participants' balance. The 3 months with APA will allow to quantify the improvement in balance abilities. In both phases of the trial (without and with APA), the predictive falls risk score will be correlated with the daily recording of falls.
In order to propose physical activity that is most adapted to the abilities of the people included in the study, 4 groups will be defined as follows:
• (1) The first physical activity group will be designed for older people with a low risk of falling;
• (2) Older people at high risk of falling;
• (3) Those with a high risk of falling but also with cardiovascular problems that necessarily require a adjustment of the physical exercises program;
• (4) The fourth group will consist of people with cognitive impairment that is incompatible with similar care to the other groups, given the deficiencies and attention disorders associated with their mild-to-severe cognitive impairments.
In each institution, one or two physical activity groups will be constituted until the renewing of the list of participants (every 6 months). The total duration of the study is 24 months.
2.2.1. Measurements and Outcomes
The instrumented measurement of balance and gait will need to be related to clinical measurements of motor skills such as the Berg Balance Scale (BBS) (71) or Mini Motor test (MMT) (72) in order to provide relevant information on the motor strategies of older people who fall (73).
In the normal course of resident care, the motor function assessment is already done clinically using functional scales such as the BBS. For more fragile residents, the MMT can be preferred. Both provide a numerical score of the balance capacities. The BBS, or the MMT when more appropriate, will be performed at the inclusion of the resident in the trial. In addition to these two scales, the assessment of the cognitive state of the residents is carried out with the Mini Mental State Examination (MMSE). A pain assessment will also be performed through Algoplus (74), Doloplus (75), or at least quoted from 0 to 10 with the localization indicated. The three scales provide a score to quantify the pain. In case of variability in the use of the different scales, their transformation into a normalized effect size will be calculated. The Autonomy, Gerontology Group Iso Resources (AGGIR) grid (76) is a categorical score to determine the level of dependency of the participants. The AGGIR grid evaluates the dependency of the elderly people by scoring from GIR 1 (presence of continuous human assistance required) to GIR 6 (fully autonomous) the aids needed to perform daily tasks. This grid, as well as the BBS, the MMT, the MMSE, and the pain scales are used clinically on a very frequent basis by the care providers in nursing home. The correlation of biomechanical markers with the clinical evaluations could provide a better understanding of the markers evolution to the healthcare professionals.
In addition to these measures, a systematic search for the main risk factors for falls and cardiovascular disease will be carried out using an assessment form developed for this clinical trials (ORPEA Risk Assessment Sheet [ORAS]). The ORAS form is an assessment of the elderly person's fall and cardiovascular risks for inclusion in the four APA programs planned in Postadychute-AG. It is filled in by healthcare professionals (coordinating physician of the nursing home and physiotherapists). It consists mainly of check boxes. The ORAS form gathers factors predisposing to falls, a neuropsychiatric evaluation, an evaluation of cardiovascular and pulmonary disorders, a stress test adapted to institutionalized elderly people, a frailty questionnaire, a functional measurement of sitting, standing balance and mobility, as well as an evaluation of cognitive abilities. Additional comments and information may be added by the healthcare professional, specifying possible contraindications to the APA that have not been mentioned in the form, if any (see Additional File 3 for more information). The ORAS assessment contains an endurance exercise that aims to assess the feasibility of the participant to sustain continuous physical activity for several minutes. During this stress test, the person is monitored with an electronic tensiometer and a saturometer to check the evolution of blood pressure, heart rate, and oxygen saturation. The same cardiovascular assessment is carried out in the first APA sessions to check the adequacy of the intensity of the exercises with the physical capacities of the participants.
Both recordings (static and dynamics balance measures) will therefore be made monthly for 6 months (Figure 1). The first one is a recording of their static balance standing on a WBB, 25-s eyes open and then 25-s eyes closed, arms along the body. The position of the feet will be wide enough to be comfortable, not exceeding the width of the shoulders. The posturographic data are transmitted to a tablet and presented to the healthcare professional, thanks to a software specially developed for this purpose, with multiple visualizations and a summary of the main COP parameters. The other recording is a 10-m gait exercise both ways with IMU on the feet, lumbar region, and head following this sequence: (1) standing still for 6 s, (2) walking 10 m at the speed chosen to be comfortable, (3) U-turn, (4) walking 10 m at the same speed, and (5) stopping and standing still for 3 s. In both cases, the data are transmitted via Bluetooth to the tablet held by the healthcare professional. Within seconds, the signals are pre-processed (77, 78) and shown to the healthcare professional for interpretation.
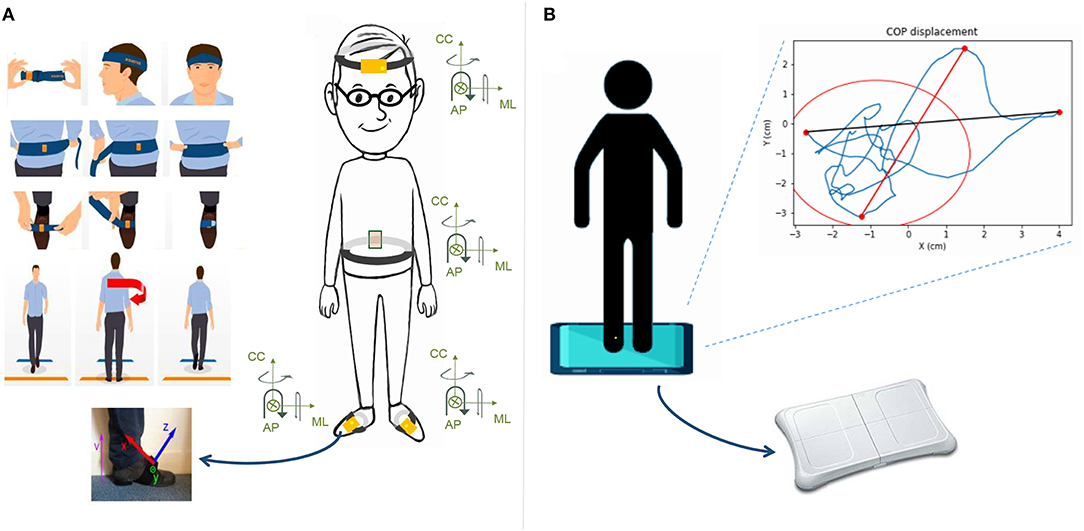
Figure 1. Measurement process for balance analysis. (A) For gait analysis: Four sensors are placed on the top of each foot, on the low back, and on the front of the resident.They are asked to walk 10 m, make a U-turn and come back to the start line. The orientation of each IMU is indicated. (B) For quiet stance analysis: The force platform is a Wii Balance Board on which the participant stands and remains as still as possible for two periods of 25 s (eyes open and eyes closed). The signal of the COP trajectory is then recorded and automatically analyzed.
The recording of these large amounts of data, and their correlation, should make it possible to analyze the various factors that can lead to a fall in the elderly person (79).
2.3. Study Settings and Participants
2.3.1. Regulatory Submission Procedures
This protocol is in conformity with the internationally recognized ethical principles of the Declaration of (80) and its amendments. The protocol, its summary, the information note and the consent form for the study, accompanied by other administrative papers, have been submitted for authorization to the Protection of Persons Committee (CPP) chosen randomly in accordance with the laws in force (authorization dated June 14, 2019). The CPP Nord Ouest IV has validated the safety and methodology of this protocol (National number: 2017 A02545 48, dated June 14, 2019). The protocol is also registered with ANSM under the number 2017-A02545-48. Amendments to the protocol leading to significant changes or modifying the constraints or risks incurred by the participants will first be submitted to the CPP for validation. The data collection and the protection measures have been validated by the National Commission for Information Technology and Civil Liberties (CNIL) (authorization dated December 6, 2019). The results of the study will be exploited after pseudonymization and in an aggregated manner.
2.3.2. Eligibility Criteria
For this study, the participants will have to meet the following inclusion criteria:
• Adults of both sexes, aged 65 years and over, social insurance recipients;
• Living in one of the selected nursing home of the ORPEA private group;
• Not presenting any neurological, vestibular, or visual disorder incompatible with stepping on the WBB platform or walking 10 m without human assistance;
• Being able to safely stepping on the WBB platform (as estimated by the investigating practitioner) and able to maintain a quiet stance for more than 1 min, with eyes open or closed;
• Have obtained an MMSE score higher than 18 on the date of entry into the nursing home or within the last 6 months;
• Having an assumed life expectancy of more than 6 months, as estimated by the coordinating physician of the establishment;
• Having signed the informed consent.
The criteria that do not allow to be included in the study gather (1) non-mobile residents (any person with a musculoskeletal or neurosensory disorder that does not allow him/her to maintain a standing position for more than 1 min on the WBB force platform), (2) history of limb amputation, (3) blindness (assessed using an Amsler grid), or (4) the resident refusal.
The resident can be discharged from the trial by choice or due to an inability to continue static and dynamic assessments (e.g., related to a serious adverse event due to a fall for example). An intention-to-treat analysis will be applied and data from participants who do not complete the protocol will be used until the date of their exclusion from the trial or their death.
2.3.3. Recruitment
Individuals will be recruited from their nursing home in Paris and the Île-de-France region in France. This community will therefore remain relatively homogeneous despite possible differences, particularly with regard to cognitive disorders that may require residence in a protected unit. The cognitive deficits, fall risks, and cardiovascular risks presented by the participants lead to the following allocation in the four APA programs:
• Group 1 “Maintaining Autonomy”: Participants of group 1 have no cardiovascular anomaly detected during the stress test, but possibly some limited cognitive deficits (MMSE > 24 and cognitive abilities considered as sufficient through the ORAS form; Additional File 3). They do not live in a protected unit. They represent a group of robust residents, with limited risk of falling, living autonomously in their rooms and inside the nursing home with or without walking aids. The goal of this first group is to prevent additional risk factors and reduce the consequences of falls.
• Group 2 “Prevention of the risk of falling”: Participants of group 2 have no cardiovascular anomaly detected during the stress test, but possibly some limited cognitive deficits. They possibly can walk alone in the nursing home but still present a significant risk of falling (with a history of recurrent falls in the last 6 months). Patients in wheelchairs can be included in this group if they are able to do stand up on demand. The goal of this second APA program is to improve motor abilities and balance.
• Group 3 “Prevention of the risk of falling and monitoring of cardiovascular disorders in the absence of cognitive impairment”: Group 3 participants have had a recent but stabilized cardiovascular disorder or an abnormality detected during the stress test. These disorders require specific management. Participants in wheelchairs can be included in the group 3. The objective of group 3 is to manage to reduce the risk of falling by adapting the exercises to the cardiovascular capacities, thus improving endurance for better autonomy.
• Group 4 “Prevention of the risk of falls in a context of cognitive deficit”: Participants in group 4 present moderate to severe cognitive deficits. Cognitive impairment will be considered with a MMSE ≤ 24, and/or suffering from dementia, Alzheimer's disease, or a related mild-to-severe cognitive impairment, and/or a unability to follow simple indications through the ORAS form. The participant may live in a protected unit of the nursing home. Participant with a wheelchair, as long as a physical recovery can be expected, can be included in group 4. The objective of group 4 is to prevent disorientation and risk factors for falls by improving general motor capacities.
To summarize the allocation of participants in each group, from the list proposed by the coordinating physician of the nursing home, people are informed about the implementation of the clinical trial in their residence. They obtain the information note and are informed about the study by the clinical trial investigator. They are then assessed using the ORAS form to look for cognitive deficits that will lead to their inclusion in group 4. If the cognitive deficits are limited, the screening for cardiovascular anomalies allows them to be referred to group 3 if necessary. If there are no cardiovascular anomalies during the stress test, and depending on their risk of falling as determined via the ORAS form, participants are allocated to either group 2 or group 1, if their risk of falling is considered high or moderate, respectively (Figure 2).
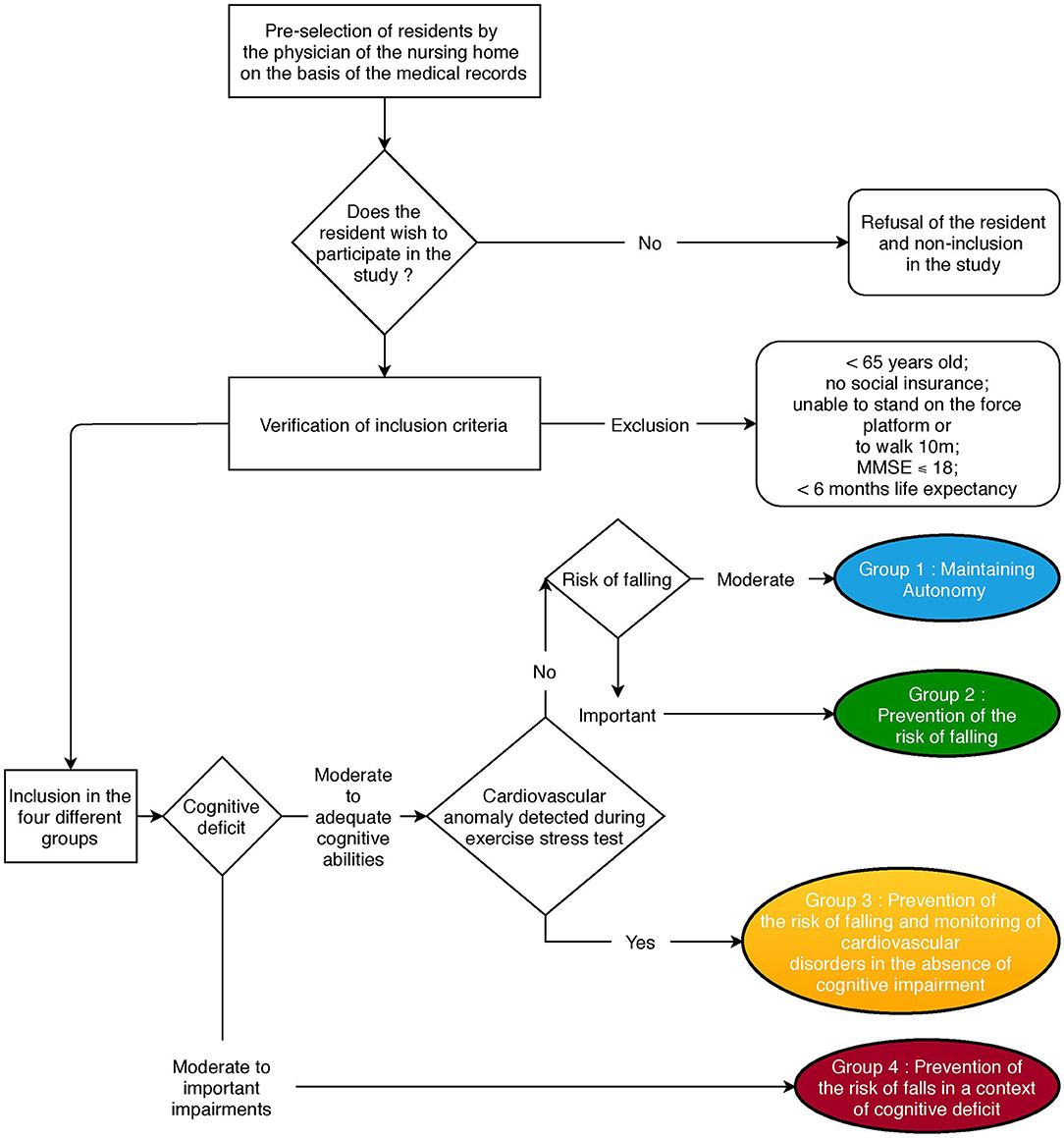
Figure 2. Flowchart of the distribution of residents in the different groups of APA after checking the adequacy of the selection criteria.
2.3.4. Participant Timeline
Following the opening visit of the residences and their inclusion in the clinical trial, the residents likely to be included in the study are listed by the coordinating physician of the center. The investigator then meets with the listed residents to ensure that the inclusion criteria are respected. After information is provided and written informed consent is obtained, the investigator also collects the baseline data necessary to follow the resident for the next 6 months (Table 1). For the 6 months, the static and dynamic balance of the residents will be recorded monthly, while a daily measurement of falls and their circumstances is provided by the health care team. This procedure should reduce the risk of recall bias that is often present with self-reporting of the number of falls by participants. After these 3-month follow-up without APA, the setting up of APA sessions allows to propose a program adapted to the capacities of the selected residents. The choice of an APA program is based upon the most representative participants, i.e., those who are more likely to form a homogeneous group. Over the next 3 months, 24 exercise sessions will be followed by the selected participants, twice a week for 1 h.
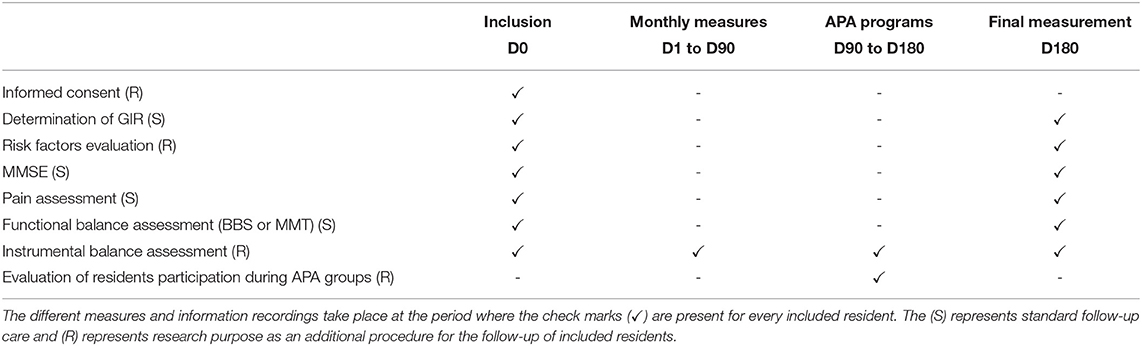
Table 1. Measurements time lines.
The observation period without APA will allow to define a baseline for all participants while the APA programs will be used to test the sensitivity of our predictive models in the improvement of the risk of falling. After these 6 months of follow-up (3 months without APA and 3 months with APA), the residents return to their daily activities and a new cohort is selected within the residence for the next 6-month period.
If participants are already benefiting from physiotherapy or other therapies to reduce the risk of falling, we do not intend to stop other treatments. This choice is explained by the objective of the study, which is not to compare the effects of physical activity between groups but to validate the relevance of predictive markers in relation to the evolution of the risk of falling assessed by clinical evaluation and the number of falls incurred.
2.3.5. Physical Activity Programs
Sessions are organized in groups of 5–10 participants. Each session supervisor (physiotherapist or APA teacher) is in charge of organizing two sessions per week and per group. The sessions last from 45 min to 1 h with at least 20–25 min of effective exercise, the rest of the time being devoted to the installation of the participants and rest periods (Additional File 3). Outside the sessions, some exercises can be carried out in the resident's room, if they have been precisely explained and if the resident do them safely during the group sessions. Compression stockings or walking aids must be kept during the session and verification by a physiotherapist is encouraged.
These four multidimensional programs are composed of exercises that follow the ProFaNe classification, i.e., physical exercises for balance, coordination, endurance, muscular strengthening, three-dimensional exploration, overall physical activity, and flexibility (81). These programs are based on specific training identified as effective in reducing the risk of falling (51, 82). They gather static balance exercises, such as modification of the base of support, and dynamic balance exercises with upper limb–lower limb coordination, exercises focused on trunk motion, functional tasks with the displacement of objects in the three dimensional space, lower limb muscle strengthening, and gait exercises with obstacles (such as mats or foam for example). The training of new motor synergies will allow the restoration of compensation mechanisms, which help to stabilize in case of internal or external disturbance. The training will also encompass sit–stand–walk transfers and optimization of attentional resources (such as multitask activities). Examples of group sessions are presented in the Supplementary Material (Additional File 3).
Once all participants have settled in and the objectives have been explained, the session begins with warm-up exercises of low difficulty on a chair. The session continues with exercises sitting or standing in front of a chair. Then, a rest period is established to restore the cardiovascular and respiratory capacities of the participants. This is also the opportunity to make the participants aware of their physiological capacities through their breathing or heart rate. After a short rest period, the session continues with ball exercises, target games, or any other exercise to be done in a group to federate the participants and energize the session. The exercises are chosen from the catalog provided to practitioners, according to the theme of the session and the position required (Additional File 3) in order to limit the number of transfers. Indeed, changing positions too often could be particularly tiring for the participants and be detrimental to a targeted work. Physical exercises, especially those that require balance, must always be done safely. Warning notes and possible modification of the exercise are provided in the exercises sheets.
It will sometimes be necessary to adapt the exercise, its duration, or the number of repetitions in relation to the capacities of the participants on an individual basis. The progression of the exercises is done by increasing the number of series (from 1 × 10 repetitions to 2 × 10 repetitions for example), the weight of the resistances, the duration in challenging positions, by reducing the support surface, by working in the 3 dimensions of space or by increasing the height of the obstacles or the distance from the targets. Every 10 sessions, the difficulty should be revised.
3. Data Management and Statistical Analysis
Data will be collected by the study investigator and by the coordinating physicians of the institutions. For details concerning falls, the coordinating investigator will collect the standardized forms. For static balance analysis, a pre-processing algorithm is used to filter and resample the signal (83). An algorithm is used to verify the quality of the data from gait recording and automatically detect the steps from the IMU signals (60, 77, 78, 84). The computed parameters used to predict the risk of falling are presented in previous publications for both static (11, 12, 62) and dynamic balance assessment (35, 61, 85). In these studies, non-linear models (Ranking Forest and Gaussian Mixture Model) are used for classification. The validation of these descriptors obtained a good classification in retrospective fall recordings, which suggests that they will also be useful for the prospective classification of the risk of falling. The results will be considered significant at the 5% threshold.
In case of a flagrant behavioral abnormality (e.g., obsessive-compulsive disorder, psychiatric disorder, and so on), the participant's data will be excluded from the study. Missing, unused, or invalid data will not be included in the results or published. All data are stored on protected servers with regular backups. Internal audits are planned to verify the reliability of the data. Given the nature of the study, the expected adverse events gather traumatic problems related to fall from the WBB, during gait or physical activity.
3.1. Sample Size Computation
In order to develop a predictive tool that quantify balance with sufficient sensitivity to the evolution of the risk of falling during a 6-month longitudinal follow-up, it is necessary to quantify the expected improvement of posturographic markers. Previous results have shown the feasibility to estimate the risk of falling with force plates (13, 86) or IMU during walking (31) but, to date, we have not been able to find a study that evaluates monthly and longitudinally the balance via these sensors for institutionalized elderly people. Hence, we used previously published data (87) to estimate the necessary sample size because of the similarity with this study. They attested of an evolution of the COP sway area after 3 months of physical activity. We use the following formula to calculate the number of subjects required (88):
where
• N is the number of participants per group;
• σ2 is the variance of COP surface area from (87);
• Zβ is the normal standard variable for a 90% statistical power (Zβ = 1.28);
• is the normal standard variable for a significant threshold stated at 95%, ();
• d, the difference between two means [d = 0.11cm2 from (87)].
Hence, 72 participants per group are required. We estimate a 20% risk of loss of follow-up for this type of prospective study with the elderly people (89, 90), mainly due to the mortality (3). It seems necessary to include a minimum of 348 participants in total.
3.2. Statistics
The main evaluation criterion is the predictive value of the indicators measured monthly, correlated with the daily recorded number of falls. The predictive value will be quantified by assessing the threshold of the predictive score out of 100 based on a sensitivity of at least 80% and maximum specificity (Youden's index). It will be computed from the receiver operating characteristic (ROC) curve and its area under the curve (AUC), measuring the classification between “high risk of falling” and “low risk of falling” (binary criterion) (91–94). This classification is subsequently checked using the fall record sheets fulfilled by the medical staff. This standardized fall recording should reduce the number of “silent events,” such as forgotten fall as it may appears with fall history questionnaires, and provide more qualitative data around the falls (79).
The predictive value will also be evaluated by measuring the positive predictive value and negative predictive value from the binary classification. We will also look for a correlation between biomechanical markers and the other recorded variables [clinical tests (BBS or MMT), pain, and independence (AGGIR)] as well as the severity of falls according to an adaptation of the Hopkins Falls Grading Scale: “Grade 1: Fall with no immediate physical consequences; Grade 2: Fall with minimal consequences that did not require medical assistance; Grade 3: Fall that required medical assistance but did not lead to hospitalization; Grade 4: Fall that led to hospitalization or death” (95).
The detection of a clinical change through an analysis of variance (ANOVA) will be calculated via the within-subject standard deviation, also called standard error of measurement (SEM). The SEM can be calculated from the square root of the mean square error term in an ANOVA and will be computed throughout the follow-up of the first 3 months, and then will allow to determine the minimal detectable change (MDC) (96, 97). The MDC is the minimum value to attest to a clinical evolution of the subject that cannot be explained by an error in the measurement. This should be more than 2.77 times the SEM of the fall risk score, if the variables are normally distributed. We will use an anchor approach to measure MDC, if it is not possible to measure the within-subject standard deviation (when participants move from one category to another—“low risk of falling” to “high risk of falling”—without being able to make repeated measurements due to hospitalization, for example). These methods correlate the change from a score (here the fall risk score) to an objective external evaluation (the number of falls) (98).
The acceptability of using the predictive score will be measured using the questionnaire (Additional File 3) based on the Technology Acceptance Model and the 7-point Likert scale (99).
4. Discussion
Physical activity, whether associated with other interventions or not, shows a significant decrease in the rate of falls resulting in injury (56). While the beneficial effect of physical exercise on the physiological capacities, even in highly dependent elderly people, has been highlighted in many studies (10, 44, 45, 100–102), the impact of APA programs on posturographic parameters seems to be a matter of debate (103). Nonetheless, it has previously been shown to improve postural stability with a reduction in mediolateral sway (104), total sway length, and mean sway velocity (37, 51). Improvements in the static balance can therefore be expected (105).
On the other hand, the way in which exercise programs are implemented can vary the expected benefits and too little publication presents in details the programs provided. Given this lack of information, the choice of the best methods of implementation, particularly in nursing homes, remains an open question (45). In the Postadychute-AG clinical trial, the choice was made to propose four physical activity programs according to the cognitive deficits, cardiovascular, and fall risks. Repeated measurements of static and dynamic balance, as well as the evaluation of risk factors at the beginning and end of inclusion, will serve to attest to the evolution of the individuals' capacities.
Johansson et al. showed that the WBB could be used to assess the risk of falling in elderly subjects (13). Indeed, beyond a certain threshold value of the COP displacement, the risk of falling is increased by 75% in community dwelling elderly people. Although this study gathered 1,877 participants, the authors were not able to implement regular measurements (only punctual measurements at 6 and 12 months). They highlight the lack of follow-up as a limit to extending their results to the clinical setting. These results are joined by those of other authors using WBB (86) or ILG during walking (31). In a follow-up of 130 participants, (106) observed significant differences in posturographic parameters between fallers and non-fallers based on retrospective data. A conclusion can therefore be drawn on the feasibility of a one-time measurement for assessing the risk of falling at 3, 6, and 12 months. However, the feasibility of periodic monitoring as a method of longitudinal fall risk assessment, combining COP characteristics and gait parameters, remains to be proven (107). In terms of expected outcomes, no studies appear to have studied MDC over several months of follow-up, especially in institutionalized seniors. However, in a previous study (108), the intra-session MDC was estimated to be ±1.2 and ±0.6 mm/s for the AP mean velocity and ML mean velocity variables, respectively. Both variables have very good between-day reliability (0.92 [0.87–0.97] and 0.91 [0.85–0.97], respectively, for the AP and ML directions) (109), which explain the discrimination capacities of these COP variables (108). Even though the variability in COP characteristics is likely to be higher between sessions, rather than within sessions, similar results can be expected.
Gait impairments can have a significant impact on quality of life and independence. In neurological disorders, gait analysis by IMU has shown interest in quantifying and monitoring gait degradation (63). A review of the literature has already highlighted the interest of several markers for distinguishing older fallers (110), such as step length, gait speed, stride length, and contact time variability. From this list, and other variables especially in the U-turn (111), the developed algorithms will be able to provide a risk score combining static and dynamic measures. On the basis of previous results (112), it is likely that the analysis of temporo-spatial variables of gait can effectively distinguish fallers from non-fallers in elderly institutionalized population. The SEM and the MDC of gait velocity were measured at 6.5 and 18.1% at their maximum, respectively, while the variability of the other gait parameters could be higher (113). Hence, markers derived from gait velocity could be sensitive enough to change over repeated measurement in medium-term.
The goal of using a standardized assessment of falls and cardiovascular risks and cognitive deficits, through the ORAS form, is to evaluate risk factors, on the one hand, and to propose a physical activity programme that can be performed by a homogeneous group, on the other hand. All the four programs focus on mobility and physical improvement. However, in order to set up a series of exercises adapted to the deficits, it is necessary to take into account the potential pitfalls inherent to the difficulty of the physical activity as well as the participants capacity of understanding the supervisor's recommendations. It is indeed necessary to take into account the undesirable effects due to physical activity to attest its effectiveness. A recent meta-analysis was unable to find any adverse effects significantly associated with APA, not even muscle soreness (56). There is a lack of reporting adverse effects in prevention programs for older adults (114) and, at the same time, individual clinical trials do not collect sufficient data to study the adverse effects of these programs, which have a low rate of occurrence. In another meta-analysis, no adverse effects were found in any of the 30 included studies (115). Nevertheless, it is important to be vigilant about the prescribed exercise dose or the instructions provided to ensure rest periods and avoid overtraining.
Considering the difficulty of identifying a single cause of falling (116), rather than proposing exercises focused on an identified cause of falls, the creation of the groups should be guided by the possibility of following the supervisor's instructions from the participants, so that people in the same group are able to perform the exercises. The benefits of physical activity in the elderly are global, i.e., improving many functions from balance to gait quality, including cardiovascular, respiratory, and possibly cognitive functions (117–121). Previous results have shown benefits in favor of programs that add in-depth geriatric risk analysis and subgrouping according to individual abilities, especially concerning participants' cognitive impairment (MMSE ≤ 19) (57). The results of trials on the prevention of falls in cognitively intact elderly people are nevertheless difficult to generalize to people with dementia given the difficulty of following the session supervisor's instructions (122). It is then appropriate to propose a group with important cognitive impairments and separate them from persons with preserved functions. For cardiovascular disorders, physical exercise could constitute a risk of adverse event, a factor limiting the benefits of APA and ultimately lead to a disengagement of the participants. Moreover, the correlation between the proposed exercises and the benefits on the different functions remains tenuous in the absence of more data among people living in nursing homes (45), which makes it necessary to tailor the programs according to criteria that seek to homogenize the groups.
5. Conclusion
To counter the limitations of clinical assessments, postural parameters and automated gait analysis could be effective in providing a quantification of balancing capabilities. They would provide a better understanding of the physiological mechanisms impacted by aging (123). In addition, distinguishing elderly people at risk of falling, or predicting future falls during longitudinal follow-up, has been shown to be effective with classic stabilometric parameters (11, 14, 124). At the same time, automated gait analysis allows the extraction of biomechanical parameters to facilitate early diagnosis of future fallers (125, 126). However, too few studies follow elderly people longitudinally with repeated measurements to observe posture degradation. The lack of data is even more striking among institutionalized individuals who, however, would benefit most from being monitored over several months. This lack of information on the usefulness of posturography to follow these people and allow a fine and sensitive evaluation of the risk of falling is the problem that this clinical trial aims to solve. In addition to providing information during a follow-up of institutionalized persons twice 3 months concerning their balance capacities, the implementation of 4 programs of APA could make it possible to evaluate the benefit of such programs on the number of falls as well as on the static and dynamic balance parameters.
Author Contributions
All author have made substantial contributions to the conception and design of the work. The acquisition, analysis, and interpretation of data will be made by FQ. FQ, P-PV, DR, FB-H, and PZ have drafted the work and revised it. All authors have approved the submitted version. P-PV, DR, FB-H, PZ, and ML carried out management and financing activities for the research project.
Funding
This study was approved by the ANRT as part of a public–private industrial partnership between the ORPEA group and the Centre Borelli Laboratory. The number of this grant is CIFRE no. 437/2016. ORPEA group is the promoter of the Postadychute-AG clinical trial.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
We would like to thank ANRT for validating the CIFRE contract for the thesis, reflecting the cooperation between the ORPEA group and the Centre Borelli laboratory. We would like to thank Dr. Dan Kogel, Dr. Jean-Louis Bussière, Dr. Lucie Gagneur, Dr. Patrick Hugeux, Mr. Jean-Claude Gayet, and Mr. Patrick Pecoraro for their participation in the development of the ORAS form and their expertise in selecting exercises for APA programs.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fdgth.2020.604552/full#supplementary-material
Additional File 1. Oras form, for cognitive, cardiac, and fall risks assessment. The evaluation form is in .docx format to be easily read and printed by health care teams. The different elements of the form are to be filled in by the doctor and a rehabilitation worker at least. It is estimated that it will take 30 min to complete, but it is advisable to fill it in several times and with a multidisciplinary approach.
Additional File 2. Exercise sheet. Presents the exercise and associated comments. The title and descriptions provide information on the action to be performed, while contextual information (such as position or difficulty) allows the facilitator to organize the exercise.
Additional File 3. Group session description. Presents the order of exercises during a typical session. The number of repetitions is for information only, so that the speaker can adapt the session according to the theme he or she wishes to work on.
Additional File 4. Fall score usefulness evaluation form. Evaluation of the Cognac-G measurement method by the nursing staff. “Perceived usefulness” and “Perceived ease of use” are assessed with 10 items each. “Intent to use” is assessed with 4 items.
Abbreviations
AGGIR, Autonomy, Gerontology Group Iso Resources; ANOVA, analysis of variance; ANSM, Agence nationale de sécurité du médicament; ANRT, Association Nationale de la Recherche et de la Technologie (National Association for Research and Technology); APA, adapted physical activity; BBS, Berg Balance Scale; CNIL, Commission nationale de l'informatique et des libertés (National Commission for Informatics and Liberties); COP, center of pressure; CPP, Comité de Protection des Personnes (Protection of Persons Committee); IMU, inertial measurement unit; MMSE, Mini Mental State Examination; MMT, Mini Motor Test; MDC, minimum clinically detectable change; ORAS, ORPEA Risk Assessment Sheet; ProFaNE, Prevention of falls network Europe; SEM, standard error of measurement; WBB, Wii Balance Board.
References
2. Tinetti ME, Baker DI, McAvay G, Claus EB, Garrett P, Gottschalk M, et al. A multifactorial intervention to reduce the risk of falling among elderly people living in the community. N Engl J Med. (1994) 331:821–7. doi: 10.1056/NEJM199409293311301
3. Becker C, Kron M, Lindemann U, Sturm E, Eichner B, Walter-Jung B, et al. Effectiveness of a multifaceted intervention on falls in nursing home residents. J Am Geriatr Soc. (2003) 51:306–13. doi: 10.1046/j.1532-5415.2003.51103.x
4. Bourdessol H, and Pin S. Réseau francophone de prévention des traumatismes et de promotion de la sécurité. Institut national de prévention et d'éducation pour la santé. In: Prévention des chutes chez les personnes âgées à domicile: référentiel de bonnes pratiques. Saint Denis: Editions Inpes (2005). p. 30–3.
5. HAS. Analyse de la Posture Statique et/ou Dynamique sur Plate-Forme de Force (Posturographie). Service Evaluation des Actes Professionnels (2007).
6. Rubenstein LZ, Josephson KR, and Robbins AS. Falls in the nursing home. Ann Internal Med. (1994) 121:442–51. doi: 10.7326/0003-4819-121-6-199409150-00009
7. Rubenstein LZ. Falls in older people: epidemiology, risk factors and strategies for prevention. Age Ageing. (2006) 35:ii37–41. doi: 10.1093/ageing/afl084
8. Fried LP, Tangen C, Walston JD, Newman AB, Hirsch C, and Gottdiener J. Frailty in older adults: evidence for a phenotype. J Gerontol. (2001) 56A, 146–56. doi: 10.1093/gerona/56.3.M146
9. Tromp AM, Pluijm SMF, Smit JH, Deeg DJH, Bouter LM, and Lips P. Fall-risk screening test: a prospective study on predictors for falls in community-dwelling elderly. J Clin Epidemiol. (2001) 54:837–44. doi: 10.1016/S0895-4356(01)00349-3
10. Gates S, Smith LA, Fisher JD, and Lamb SE. Systematic review of accuracy of screening instruments for predicting fall risk among independently living older adults. J Rehabil Res Dev. (2008) 45:1105–16. doi: 10.1682/JRRD.2008.04.0057
11. Audiffren J, Bargiotas I, Vayatis N, Vidal PP, and Ricard D. A non linear scoring approach for evaluating balance: classification of elderly as fallers and non-fallers. PLoS ONE. (2016) 11:e0167456. doi: 10.1371/journal.pone.0167456
12. Bargiotas I, Audiffren J, Vayatis N, Vidal PP, Buffat S, Yelnik AP, et al. On the importance of local dynamics in statokinesigram: a multivariate approach for postural control evaluation in elderly. PLoS ONE. (2018) 13:e0192868. doi: 10.1371/journal.pone.0192868
13. Johansson J, Nordstrom A, Gustafson Y, Westling G, and Nordstrom P. Increased postural sway during quiet stance as a risk factor for prospective falls in community-dwelling elderly individuals. Age Ageing. (2017) 46:964–70. doi: 10.1093/ageing/afx083
14. Piirtola M, and Era P. Force platform measurements as predictors of falls among older people—A review. Gerontology. (2006) 52:1–16. doi: 10.1159/000089820
15. Chaudhry H, Bukiet B, Ji Z, and Findley T. Measurement of balance in computer posturography: comparison of methods–A brief review. J Bodywork Movement Therap. (2011) 15:82–91. doi: 10.1016/j.jbmt.2008.03.003
16. Howcroft J, Lemaire ED, Kofman J, and McIlroy WE. Elderly fall risk prediction using static posturography. PLoS ONE. (2017) 12:e0172398. doi: 10.1371/journal.pone.0172398
17. Abujaber S, Gillispie G, Marmon A, and Zeni J. Validity of the Nintendo Wii Balance Board to assess weight bearing asymmetry during sit-to-stand and return-to-sit task. Gait Post. (2015) 41:676–82. doi: 10.1016/j.gaitpost.2015.01.023
18. Bartlett HL, Ting LH, and Bingham JT. Accuracy of force and center of pressure measures of the Wii Balance Board. Gait Post. (2014) 39:224–8. doi: 10.1016/j.gaitpost.2013.07.010
19. Clark RA, Bryant AL, Pua Y, McCrory P, Bennell K, and Hunt M. Validity and reliability of the Nintendo Wii Balance Board for assessment of standing balance. Gait Post. (2010) 31:307–10. doi: 10.1016/j.gaitpost.2009.11.012
20. Huurnink A, Fransz DP, Kingma I, and van Dieen JP. Comparison of a laboratory grade force platform with a Nintendo Wii Balance Board on measurement of postural control in single-leg stance balance tasks. J Biomech. (2013) 46:1392–5. doi: 10.1016/j.jbiomech.2013.02.018
21. Leach J, Mancini M, Peterka R, Hayes T, and Horak F. Validating and calibrating the Nintendo Wii balance board to derive reliable center of pressure measures. Sensors. (2014) 14:18244–67. doi: 10.3390/s141018244
22. Sgro F, Monteleone G, Pavone M, and Lipoma M. Validity analysis of Wii balance board versus baropodometer platform using an open custom integrated application. AASRI Proc. (2014) 8:22–9. doi: 10.1016/j.aasri.2014.08.005
23. Jorgensen MG, Paramanathan S, Ryg J, Masud T, and Andersen S. Novel use of the Nintendo Wii board as a measure of reaction time: a study of reproducibility in older and younger adults. BMC Geriatr. (2015) 15:80. doi: 10.1186/s12877-015-0080-6
24. Carette P, Kemoun G, Watelain E, and Dugue B. Concomitant changes in clinical and posturographic data in elderly fallers during the course of an in-home anti-falling multimodal program—A preliminary investigation. Neurophysiol Clin. (2013) 43:229–36. doi: 10.1016/j.neucli.2013.06.003
25. Maranesi E, Merlo A, Fioretti S, Zemp DD, Campanini I, and Quadri P. A statistical approach to discriminate between non-fallers, rare fallers and frequent fallers in older adults based on posturographic data. Clin Biomech. (2016) 32:8–13. doi: 10.1016/j.clinbiomech.2015.12.009
26. Pizzigalli L, Micheletti M, Mulasso A, and Rainoldi A. The contribution of postural balance analysis in older adult fallers: a narrative review. J Bodyw Mov Ther. (2016) 20:409–17. doi: 10.1016/j.jbmt.2015.12.008
27. Comber L, Sosnoff JJ, Galvin R, and Coote S. Postural control deficits in people with Multiple Sclerosis: a systematic review and meta-analysis. Gait Post. (2018) 61:445–52. doi: 10.1016/j.gaitpost.2018.02.018
28. Palmieri RM, Ingersoll C, Stone MB, and Krause BA. Center-of-pressure parameters used in the assessment of postural control. J Sport Rehabil. (2002) 11:51–66. doi: 10.1123/jsr.11.1.51
29. Visser JE, Carpenter MG, van der Kooij H, and Bloem BR. The clinical utility of posturography. Clin Neurophysiol. (2008) 119:2424–36. doi: 10.1016/j.clinph.2008.07.220
30. Quijoux F, Vienne-Jumeau A, Bertin-Hugault F, Zawieja P, Lefevre M, Vidal PP, et al. Center of pressure displacement characteristics differentiate fall risk in older people: a systematic review with meta-analysis. Ageing Res Rev. (2020) 62:101117. doi: 10.1016/j.arr.2020.101117
31. Mignardot JB, Deschamps T, Barrey E, Auvinet B, Berrut G, Cornu C, et al. Gait disturbances as specific predictive markers of the first fall onset in elderly people: a two-year prospective observational study. Front Aging Neurosci. (2014) 6:22. doi: 10.3389/fnagi.2014.00022
32. Moreira BS, Sampaio RF, and Kirkwood RN. Spatiotemporal gait parameters and recurrent falls in community-dwelling elderly women: a prospective study. Braz J Phys Ther. (2015) 19:61–9. doi: 10.1590/bjpt-rbf.2014.0067
33. Toebes MJP, Hoozemans MJM, Furrer R, Dekker J, and van Dieen JH. Local dynamic stability and variability of gait are associated with fall history in elderly subjects. Gait Post. (2012) 36:527–31. doi: 10.1016/j.gaitpost.2012.05.016
34. Monda M, Goldberg A, Smitham P, Thornton M, and McCarthy I. Use of inertial measurement units to assess age-related changes in gait kinematics in an active population. J Aging Phys Act. (2015) 23:18–23. doi: 10.1123/japa.23.1.18
35. Vienne A, Barrois RP, Buffat S, Ricard D, and Vidal PP. Inertial sensors to assess gait quality in patients with neurological disorders: a systematic review of technical and analytical challenges. Front Psychol. (2017) 8:817. doi: 10.3389/fpsyg.2017.00817
36. Hortobagyi T, Lesinski M, Gabler M, VanSwearingen JM, Malatesta D, and Granacher U. Effects of three types of exercise interventions on healthy old adults' gait speed: a systematic review and meta-analysis. Sports Med. (2015) 45:1627–43. doi: 10.1007/s40279-015-0371-2
37. Low DC, Walsh GS, and Arkesteijn M. Effectiveness of exercise interventions to improve postural control in older adults: a systematic review and meta-analyses of centre of pressure measurements. Sports Med. (2017) 47:101–12. doi: 10.1007/s40279-016-0559-0
38. Bertolotti MG, Cristiani AM, Colagiorgio P, Romano F, Bassani E, Caramia N, et al. A wearable and modular inertial unit for measuring limb movements and balance control abilities. IEEE Sens J. (2016) 16:790–7. doi: 10.1109/JSEN.2015.2489381
39. Chung CC, Soangra R, and Lockhart TE. Recurrence quantitative analysis of postural sway using force plate and smartphone. Proc Hum Factors Ergon Soc Annu Meet. (2014) 58, 1271–5. doi: 10.1177/1541931214581265
40. Li X, Xu H, and Cheung JT. Gait-force model and inertial measurement unit-based measurements: a new approach for gait analysis and balance monitoring. J Exerc Sci Fit. (2016) 14:60–6. doi: 10.1016/j.jesf.2016.07.002
41. Lindemann U, Moe-Nilssen R, Nicolai SE, Becker C, and Chiari L. Assessment of balance in unsupported standing with elderly inpatients by force plate and accelerometers. Aging Clin Exp Res. (2012) 24:37–41. doi: 10.1007/BF03325352
42. Damush TM, Stewart AL, Mills KM, King AC, and Ritter PL. Prevalence and correlates of physician recommendations to exercise among older adults. J Gerontol Ser A Biomed Sci Med Sci. (1999) 54:M423–7. doi: 10.1093/gerona/54.8.M423
43. Elsawy B, and Higgins KE. Physical activity guidelines for older adults. Am Family Phys. (2010) 81:55–9.
44. Cameron ID, Murray GR, Gillespie LD, Robertson MC, Hill KD, Cumming RG, et al. Interventions for preventing falls in older people in nursing care facilities and hospitals. Cochrane Datab Syst Rev. (2010). doi: 10.1002/14651858.CD005465.pub2
45. Gillespie LD, Robertson MC, Gillespie WJ, Sherrington C, Gates S, Clemson L, et al. Interventions for preventing falls in older people living in the community. Cochrane Datab Syst Rev. (2012). doi: 10.1002/14651858.CD007146.pub3
46. Chale-Rush A, Guralnik JM, Walkup MP, Miller ME, Rejeski WJ, Katula JA, et al. Relationship between physical functioning and physical activity in the lifestyle interventions and independence for elders pilot. J Am Geriatr Soc. (2010) 58:1918–24. doi: 10.1111/j.1532-5415.2010.03008.x
47. Chang JT. Interventions for the prevention of falls in older adults: systematic review and meta-analysis of randomised clinical trials. BMJ. (2004) 328:680. doi: 10.1136/bmj.328.7441.680
48. Gine-Garriga M, Roque-Figuls M, Coll-Planas L, Sitja-Rabert M, and Salva A. Physical exercise interventions for improving performance-based measures of physical function in community-dwelling, frail older adults: a systematic review and meta-analysis. Arch Phys Med Rehabil. (2014) 95:753–69.e3. doi: 10.1016/j.apmr.2013.11.007
49. Sauvage LRJ, Myklebust BM, Crow-Pan J, Novak S, Millington P, Hoffman MD, et al. A clinical trial of strengthening and aerobic exercise to improve gait and balance in elderly male nursing home residents. Am J Phys Med Rehabil. (1992) 71:333–42. doi: 10.1097/00002060-199212000-00005
50. Wolf SL, Barnhart HX, Ellison GL, Coogler CE, and FICSIT GA. The effect of Tai Chi Quan and computerized balance training on postural stability in older subjects. Phys Therapy. (1997) 77:371–81. doi: 10.1093/ptj/77.4.371
51. Howe TE, Rochester L, Jackson A, Banks PMH, and Blair VA. Exercise for improving balance in older people. Cochrane Library. (2007). doi: 10.1002/14651858.CD004963.pub2
52. DiPietro L, Al-Ansari SS, Biddle SJ, Borodulin K, Bull FC, Buman MP, et al. Advancing the global physical activity agenda: recommendations for future research by the 2020. WHO physical activity and sedentary behavior guidelines development group. Int J Behav Nutr Phys Act. (2020) 17:1–11. doi: 10.1186/s12966-020-01042-2
53. Leavitt M. Physical Activity Guidelines for Americans. Washington, DC: US Department of Health and Human Services (2008).
54. El-Khoury F, Cassou B, Charles MA, and Dargent-Molina P. The effect of fall prevention exercise programmes on fall induced injuries in community dwelling older adults: systematic review and meta-analysis of randomised controlled trials. BMJ. (2013) 347:f6234. doi: 10.1136/bmj.f6234
55. Guirguis-Blake JM, Michael YL, Perdue LA, Coppola EL, and Beil TL. Interventions to prevent falls in older adults: updated evidence report and systematic review for the US Preventive Services Task Force. JAMA. (2018) 319:1705–16. doi: 10.1001/jama.2017.21962
56. Tricco AC, Thomas SM, Veroniki AA, Hamid JS, Cogo E, Strifler L, et al. Comparisons of interventions for preventing falls in older adults: a systematic review and meta-analysis. JAMA. (2017) 318:1687. doi: 10.1001/jama.2017.15006
57. Jensen J, Nyberg L, Gustafson Y, and Lundin-Olsson L. Fall and injury prevention in residential care-effects in residents with higher and lower levels of cognition. J Am Geriatr Soc. (2003) 51:627–35. doi: 10.1034/j.1600-0579.2003.00206.x
58. Vidal PP, Vienne-Jumeau A, Moreau A, Vidal C, Wang D, Audiffren J, et al. An opinion paper on the maintenance of robustness: towards a multimodal and intergenerational approach using digital twins. Aging Med. (2020) 3:188–194. doi: 10.1002/agm2.12115
59. Audiffren J, Barrois-Muller R, Provost C, Chiarovano E, Oudre L, Moreau T, et al. Évaluation de l' équilibre et prédiction des risques de chutes en utilisant une Wii board balance. Neurophysiol Clin. (2015) 45:403. doi: 10.1016/j.neucli.2015.10.038
60. Oudre L, Barrois-Muller R, Moreau T, Truong C, Dadashi R, Gregory T, et al. Detection automatique des pas a partir de capteurs inertiels pour la quantification de la marche en consultation. Neurophysiol Clin. (2015) 45:394. doi: 10.1016/j.neucli.2015.10.015
61. Barrois R, Gregory T, Oudre LTM, Truong C, Pulini AA, Vienne A, et al. An automated recording method in clinical consultation to rate the limp in lower limb osteoarthritis. PLoS ONE. (2016) 11:e0164975. doi: 10.1371/journal.pone.0164975
62. Bargiotas I, Moreau A, Vienne A, Bompaire F, Baruteau M, de Laage M, et al. Balance impairment in radiation induced leukoencephalopathy patients is coupled with altered visual attention in natural tasks. Front Neurol. (2019) 9:1185. doi: 10.3389/fneur.2018.01185
63. Vienne-Jumeau A, Quijoux F, Vidal PP, and Ricard D. Value of gait analysis for measuring disease severity using inertial sensors in patients with multiple sclerosis: protocol for a systematic review and meta-analysis. Syst Rev. (2019) 8:15. doi: 10.1186/s13643-018-0918-z
64. Vienne-Jumeau A, Quijoux F, Vidal PP, and Ricard D. Wearable inertial sensors provide reliable biomarkers of disease severity in multiple sclerosis: a systematic review and meta-analysis. Ann Phys Rehabil Med. (2020) 63:138–47. doi: 10.1016/j.rehab.2019.07.004
65. Truong C, Barrois-Muller R, Moreau T, Provost C, Vienne-Jumeau A, Moreau A, et al. A data set for the study of human locomotion with inertial measurements units. Image Process On Line. (2019) 9:381–90. doi: 10.5201/ipol.2019.265
66. Bauer CM, Groger I, Rupprecht R, Marcar VL, and Gaßmann KG. Prediction of future falls in a community dwelling older adult population using instrumented balance and gait analysis. Z Gerontol Geriatr. (2016) 49:232–6. doi: 10.1007/s00391-015-0885-0
67. Garcia-Flores FI, Rivera-Cisneros AE, Sanchez-Gonzalez JM, Guardado-Mendoza R, and Torres-Gutierrez JL. Correlation between gait speed and muscular strength with balance for reducing falls among elderly. Cir Cir. (2016) 84:392–7. doi: 10.1016/j.circen.2016.08.012
68. Kang HG, Quach L, Li W, and Lipsitz LA. Stiffness control of balance during dual task and prospective falls in older adults: the ‘MOBILIZE’ Boston Study. Gait Post. (2013) 38:757–63. doi: 10.1016/j.gaitpost.2013.03.022
69. Khanuja K, Joki J, Bachmann G, and Cuccurullo S. Gait and balance in the aging population: fall prevention using innovation and technology. Maturitas. (2018) 110:51–6. doi: 10.1016/j.maturitas.2018.01.021
70. Jensen J, Nyberg L, Rosendahl E, Gustafson Y, and Lundin-Olsson L. Effects of a fall prevention program including exercise on mobility and falls in frail older people living in residential care facilities. Aging Clin Exp Res. (2004) 16:283–92. doi: 10.1007/BF03324553
71. Berg KO, Wood-Dauphinee SL, Williams JI, and Maki B. Measuring balance in the elderly: validation of an instrument. Can J Public Health. (1992) 83:S7–11.
72. Camus A, Mourey F, d'Athis P, Blanchon A, Martin-Hunyadi C, Rekeneire ND, et al. Test moteur minimum. La Revue De Geriatrie. (2002) 27:645–58. doi: 10.1016/j.archger.2004.08.004
73. Patel M, Pavic A, and Goodwin VA. Wearable inertial sensors to measure gait and posture characteristic differences in older adult fallers and non-fallers: a scoping review. Gait Post. (2020) 76:110–21. doi: 10.1016/j.gaitpost.2019.10.039
74. Rat P, Jouve E, Pickering G, Donnarel L, Nguyen L, Michel M, et al. Validation of an acute pain-behavior scale for older persons with inability to communicate verbally: Algoplus. Eur J Pain. (2011) 15:198.e1. doi: 10.1016/j.ejpain.2010.06.012
75. Lefebvre-Chapiro S, and the Doloplus-2 group. The Doloplus-2 scale: evaluating pain in the elderly. Eur J Palliat Care. (2001). 8:191–4. doi: 10.1186/1471-2318-10-9
76. Coutton V. Évaluer la dépendance à l'aide de groupes iso-ressources (GIR):une tentative en France avec la grille aggir. Gerontol Soc. (2001). 24/99:111. doi: 10.3917/gs.099.0111
77. Oudre L, Barrois-Muller R, Moreau T, Truong C, Vienne-Jumeau A, Ricard D, et al. Template-based step detection with inertial measurement units. Sensors. (2018) 18:4033. doi: 10.3390/s18114033
78. Vienne-Jumeau A, Oudre L, Moreau A, Quijoux F, Vidal PP, and Ricard D. Comparing gait trials with greedy template matching. Sensors. (2019) 19:3089. doi: 10.3390/s19143089
79. Mazuz K, Biswas S, and Lindner U. Developing self-management application of fall prevention among older adults: a content and usability evaluation. Front Digit Health. (2020) 2:11. doi: 10.3389/fdgth.2020.00011
80. World Medical Association. World Medical Association declaration of Helsinki: ethical principles for medical research involving human subjects. JAMA. (2013) 310:2191–4. doi: 10.1001/jama.2013.281053
81. Moreland J, Richardson J, Chan D, O'Neill J, Bellissimo A, Grum RM, et al. Evidence-based guidelines for the secondary prevention of falls in older adults. Gerontology. (2003) 49:93–116. doi: 10.1159/000067948
82. Marquer A, and Pérennou D. Quels niveaux de preuve pour la rééducation des troubles de l' équilibre? La Lettre de médecine physique et de réadaptation. (2012) 28:164–9. doi: 10.1007/s11659-012-0314-3
83. Audiffren J, and Contal E. Preprocessing the Nintendo Wii board signal to derive more accurate descriptors of statokinesigrams. Sensors. (2016) 16:1208. doi: 10.3390/s16081208
84. Dot T, Quijoux F, Oudre L, Vienne-Jumeau A, Moreau A, Vidal PP, et al. Non-linear template-based approach for the study of locomotion. Sensors. (2020) 20:1939. doi: 10.3390/s20071939
85. Barrois R. Gait quantitative phenotyping of brain-injured subjects/ (Ph.D. thesis). Paris: Université Paris Descartes (2018).
86. Kwok BC, Clark RA, and Pua YH. Novel use of the Wii Balance Board to prospectively predict falls in community-dwelling older adults. Clin Biomech. (2015) 30:481–4. doi: 10.1016/j.clinbiomech.2015.03.006
87. Ni M, Mooney K, Richards L, Balachandran A, Sun M, Harriell K, et al. Comparative impacts of Tai Chi, balance training, and a specially-designed yoga program on balance in older fallers. Arch Phys Med Rehabil. (2014) 95:1620–8.e30. doi: 10.1016/j.apmr.2014.04.022
88. Charan J, and Biswas T. How to calculate sample size for different study designs in medical research? Indian J Psychol Med. (2013) 35:121. doi: 10.4103/0253-7176.116232
89. Bergland A, Jarnlo GB, and Laake K. Predictors of falls in the elderly by location. Aging Clin Exp Res. (2003) 15:43–50. doi: 10.1007/BF03324479
90. Ramdani S, Tallon G, Bernard PL, and Blain H. Recurrence quantification analysis of human postural fluctuations in older fallers and non-fallers. Ann Biomed Eng. (2013) 41:1713–25. doi: 10.1007/s10439-013-0790-x
91. Clemencon S. AUC optimization and the two-sample problem. In: Advances in Neural Information Processing Systems 22: 23rd Annual Conference on Neural Information Processing Systems 2009. Vancouver, BC (2009).
92. Santos GM, Souza ACS, Virtuoso JF, Tavares GMS, and Mazo GZ. Predictive values at risk of falling in physically active and no active elderly with Berg Balance Scale. Rev Bras Fisioter. (2011) 15:95–101. doi: 10.1590/S1413-35552011000200003
93. Schwesig R, Fischer D, Lauenroth A, Becker S, and Leuchte S. Can falls be predicted with gait analytical and posturographic measurement systems? A prospective follow-up study in a nursing home population. Clin Rehabil. (2013) 27:183–90. doi: 10.1177/0269215512452880
94. Sharifi F, Fakhrzadeh H, Memari A, Najafi B, Nazari N, Khoee MA, et al. Predicting risk of the fall among aged adult residents of a nursing home. Arch Gerontol Geriatr. (2015) 61:124–30. doi: 10.1016/j.archger.2015.06.014
95. Davalos-Bichara M, Lin FR, Carey JP, Walston JD, Fairman JE, Schubert MC, et al. Development and validation of a falls-grading scale. J Geriatr Phys Therapy. (2013) 36:63–7. doi: 10.1519/JPT.0b013e31825f6777
96. Conradsson M, Lundin-Olsson L, Lindelof N, Littbrand H, Malmqvist L, Gustafson Y, et al. Berg balance scale: intrarater test-retest reliability among older people dependent in activities of daily living and living in residential care facilities. Phys Therapy. (2007) 87:1155–63. doi: 10.2522/ptj.20060343
97. Hebert R, Spiegelhalter DJ, and Brayne C. Setting the minimal metrically detectable change on disability rating scales. Arch Phys Med Rehabil. (1997) 78:1305–8. doi: 10.1016/S0003-9993(97)90301-4
98. Copay AG, Subach BR, Glassman SD, Polly DW, and Schuler TC. Understanding the minimum clinically important difference: a review of concepts and methods. Spine J. (2007) 7:541–6. doi: 10.1016/j.spinee.2007.01.008
99. Davis FD, Bagozzi RP, and Warshaw PR. User acceptance of computer technology: a comparison of two theoretical models. Manage Sci. (1989) 35:982–1003. doi: 10.1287/mnsc.35.8.982
100. Pereira CLN, Vogelaere P, and Baptista F. Role of physical activity in the prevention of falls and their consequences in the elderly. Eur Rev Aging Phys Act. (2008) 5:51–8. doi: 10.1007/s11556-008-0031-8
101. Sherrington C, Michaleff ZA, Fairhall N, Paul SS, Tiedemann A, Whitney J, et al. Exercise to prevent falls in older adults: an updated systematic review and meta-analysis. Brit J Sports Med. (2017) 51:1750–8. doi: 10.1136/bjsports-2016-096547
102. Thomas S, Mackintosh S, and Halbert J. Does the ‘Otago exercise programme’ reduce mortality and falls in older adults?: a systematic review and meta-analysis. Age Ageing. (2010) 39:681–7. doi: 10.1093/ageing/afq102
103. Crilly RG, Willems DA, Trenholm KJ, Hayes KC, and Delaquerriere-Richardson LF. Effect of exercise on postural sway in the elderly. Gerontology. (1989) 35:137–43. doi: 10.1159/000213012
104. Suomi R, and Koceja DM. Postural sway characteristics in women with lower extremity arthritis before and after an aquatic exercise intervention. Arch Phys Med Rehabil. (2000) 81:780–5. doi: 10.1053/apmr.2000.4433
105. Lesinski M, Hortobagyi T, Muehlbauer T, Gollhofer A, and Granacher U. Effects of balance training on balance performance in healthy older adults: a systematic review and meta-analysis. Sports Med. (2015) 45:1721–38. doi: 10.1007/s40279-015-0375-y
106. Merlo A, Zemp D, Zanda E, Rocchi S, Meroni F, Tettamanti M, et al. Postural stability and history of falls in cognitively able older adults: the Canton Ticino study. Gait Post. (2012) 36:662–6. doi: 10.1016/j.gaitpost.2012.06.016
107. Svoboda Z, Bizovska L, Janura M, Kubonova E, Janurova K, and Vuillerme N. Variability of spatial temporal gait parameters and center of pressure displacements during gait in elderly fallers and nonfallers: a 6-month prospective study. PLoS ONE. (2017) 12:e0171997. doi: 10.1371/journal.pone.0171997
108. Lafond D, Corriveau H, Hebert R, and Prince F. Intrasession reliability of center of pressure measures of postural steadiness in healthy elderly people. Arch Phys Med Rehabil. (2004) 85:896–901. doi: 10.1016/j.apmr.2003.08.089
109. Lin D, Seol H, Nussbaum MA, and Madigan ML. Reliability of COP-based postural sway measures and age-related differences. Gait Post. (2008) 28:337–42. doi: 10.1016/j.gaitpost.2008.01.005
110. Mortaza N, Osman ANA, and Mehdikhani N. Are the spatio-temporal parameters of gait capable of distinguishing a faller from a non-faller elderly? Eur J Phys Rehabil Med. (2014) 50:15.
111. Gulley E, Ayers E, and Verghese J. A comparison of turn and straight walking phases as predictors of incident falls. Gait Post. (2020) 79:239–43. doi: 10.1016/j.gaitpost.2020.05.002
112. Kwon MS, Kwon YR, Park YS, and Kim JW. Comparison of gait patterns in elderly fallers and non-fallers. Technol Health Care. (2018) 26:427–36. doi: 10.3233/THC-174736
113. Hars M, Herrmann FR, and Trombetti A. Reliability and minimal detectable change of gait variables in community-dwelling and hospitalized older fallers. Gait Post. (2013) 38:1010–4. doi: 10.1016/j.gaitpost.2013.05.015
114. Lin JS, Whitlock EP, Eckstrom E, Fu R, Perdue LA, Beil TL, et al. Challenges in synthesizing and interpreting the evidence from a systematic review of multifactorial interventions to prevent functional decline in older adults. J Am Geriatr Soc. (2012) 60:2157–66. doi: 10.1111/j.1532-5415.2012.04214.x
115. Wang X, Pi Y, Chen P, Liu Y, Wang R, and Chan C. Cognitive motor interference for preventing falls in older adults: a systematic review and meta-analysis of randomised controlled trials. Age Ageing. (2015) 44:205–12. doi: 10.1093/ageing/afu175
116. Soriano TA, DeCherrie LV, and Thomas DC. Falls in the community-dwelling older adult: a review for primary-care providers. Clin Intervent Aging. (2007) 2:545. doi: 10.2147/CIA.S1080
117. Dedeyne L, Deschodt M, Verschueren S, Tournoy J, and Gielen E. Effects of multi-domain interventions in (pre) frail elderly on frailty, functional, and cognitive status: a systematic review. Clin Intervent Aging. (2017) 12:873. doi: 10.2147/CIA.S130794
118. Marmeleira J, Ferreira S, and Raimundo A. Physical activity and physical fitness of nursing home residents with cognitive impairment: a pilot study. Exp Gerontol. (2017) 100:63–9. doi: 10.1016/j.exger.2017.10.025
119. Duck AA, Stewart MW, and Robinson JC. Physical activity and postural balance in rural community dwelling older adults. Appl Nurs Res. (2019) 48:1–7. doi: 10.1016/j.apnr.2019.05.012
120. Bouaziz W, Lang PO, Schmitt E, Kaltenbach G, Geny B, and Vogel T. Health benefits of multicomponent training programmes in seniors: a systematic review. Int J Clin Pract. (2016) 70:520–36. doi: 10.1111/ijcp.12822
121. Elsawy B, and Higgins KE. Physical activity guidelines for older adults. Am Family Phys. (2010) 81:55–9.
122. Vieira ER, Palmer RC, and Chaves PH. Prevention of falls in older people living in the community. BMJ. (2016) 353:i1419. doi: 10.1136/bmj.i1419
123. Nardone A, and Schieppati M. The role of instrumental assessment of balance in clinical decision making. Eur J Phys Rehabil Med. (2010) 46:221–37.
124. Pajala S, Era P, Koskenvuo M, Kaprio J, Tormakangas T, and Rantanen T. Force platform balance measures as predictors of indoor and outdoor falls in community-dwelling women aged 63–76 years. J Gerontol Ser A. (2008) 63:171–8. doi: 10.1093/gerona/63.2.171
125. Panzer VP, Wakefield DB, Hall CB, and Wolfson LI. Mobility assessment: sensitivity and specificity of measurement sets in older adults. Arch Phys Med Rehabil. (2011) 92:905–12. doi: 10.1016/j.apmr.2011.01.004
Keywords: prediction, fall, elderly people, physical activity, balance quantification
Citation: Quijoux F, Bertin-Hugault F, Zawieja P, Lefèvre M, Vidal P-P and Ricard D (2021) Postadychute-AG, Detection, and Prevention of the Risk of Falling Among Elderly People in Nursing Homes: Protocol of a Multicentre and Prospective Intervention Study. Front. Digit. Health 2:604552. doi: 10.3389/fdgth.2020.604552
Received: 09 September 2020; Accepted: 15 December 2020;
Published: 27 January 2021.
Edited by:
Richard Keith Jones, University of Salford, United KingdomReviewed by:
Hao Wang, Shenzhen University General Hospital, ChinaLaura Roche, The University of Newcastle, Australia
Copyright © 2021 Quijoux, Bertin-Hugault, Zawieja, Lefèvre, Vidal and Ricard. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Flavien Quijoux, Zi5xdWlqb3V4QG9ycGVhLm5ldA==