
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Cardiovasc. Med. , 17 February 2025
Sec. Clinical and Translational Cardiovascular Medicine
Volume 12 - 2025 | https://doi.org/10.3389/fcvm.2025.1545142
 Paula Andrea Cárdenas-Marín1,2,3Brayan Daniel Cordoba-Melo1,2,3Diana Cristina Carrillo-Gómez2
Paula Andrea Cárdenas-Marín1,2,3Brayan Daniel Cordoba-Melo1,2,3Diana Cristina Carrillo-Gómez2 Hoover León-Giraldo1,3
Hoover León-Giraldo1,3 Iván Mendoza4Noel Flórez2Ricardo Enrique Larrea Gómez5Jessica Mirella Mercedes6
Iván Mendoza4Noel Flórez2Ricardo Enrique Larrea Gómez5Jessica Mirella Mercedes6 Cesar J. Herrera7Julián Lugo-Peña8
Cesar J. Herrera7Julián Lugo-Peña8 Liliana Patricia Cárdenas-Aldaz9
Liliana Patricia Cárdenas-Aldaz9 Victor Rossel10Ricardo Ramírez Ramírez11Hugo Fernando Fernández12Andrés Ulate Retana13J. Daniel Sierra-Lara Martinez14
Victor Rossel10Ricardo Ramírez Ramírez11Hugo Fernando Fernández12Andrés Ulate Retana13J. Daniel Sierra-Lara Martinez14 Estevão Lanna Figueiredo15Wilbert German Yabar Galindo16
Estevão Lanna Figueiredo15Wilbert German Yabar Galindo16 Miguel Angel Quintana Da Silva17Alexander Romero18Paula Silva19Armando Alvarado20Andrea Valencia1
Miguel Angel Quintana Da Silva17Alexander Romero18Paula Silva19Armando Alvarado20Andrea Valencia1 Juan Esteban Gomez-Mesa1,2,3* on behalf of CARDIO COVID 19-20 Research Group
Juan Esteban Gomez-Mesa1,2,3* on behalf of CARDIO COVID 19-20 Research Group
Introduction: Viral infection by SARS-CoV2 is a pandemic affecting over 600 million people worldwide. One of five hospitalized patients may present myocardial injury, strongly associated with disease severity and mortality.
Methodology: Retrospective cross-sectional study of hospitalized COVID-19 patients diagnosed between May 01, 2020, and June 30, 2021, from the database of the Registro Latinoamericano de Enfermedad Cardiovascular y COVID-19 (CARDIO COVID 19–20) with a troponin value recorded during hospitalization. A descriptive analysis of sociodemographic and clinical characteristics was performed. Bivariate analysis was conducted according to the presence or absence of myocardial injury. Survival analysis was made using Kaplan–Meier curves, by the presence of myocardial injury. A multivariate Poisson regression model was performed to determine factors associated with mortality. Statistical analyses were performed using the RStudio V.1.4.1717 package.
Results: A total of 2,134 patients were included, 64.2% were male, and 911 patients had myocardial injury. The median age of the total population was 61 years. Individuals with myocardial injury had a higher prevalence of hypertension, diabetes, and dyslipidemia. Survival probability was lower in this subgroup. Patients with myocardial injury had a 1.95 times higher risk of death. Age, male sex, chronic kidney disease, arrhythmias, decompensated heart failure, requirement of inotropic/vasopressor, and invasive mechanical ventilation were related to higher mortality risk in patients with myocardial injury.
Conclusion: Patients with COVID-19 and myocardial injury exhibit a broad spectrum of cardiac abnormalities. Myocardial injury is associated with a higher disease severity and risk of in-hospital mortality. This multicenter study uniquely represents data from 13 Latin American countries, offering regional insights into the impact of myocardial injury during the COVID-19 pandemic.
Viral infection by SARS-CoV2 emerged as a pandemic, with the first case reported on December 1, 2019, in Hubei, China. COVID-19 has affected over 600 million people globally and resulted in more than 7 million deaths, particularly among older adults with comorbidities such as hypertension, diabetes, and cardiovascular disease, causing a significant social and economic impact (1–4).
The primary system compromised by this disease is respiratory, ranging from mild respiratory symptoms to adult respiratory distress syndrome with potentially fatal outcomes. From a cardiovascular perspective, it can present with de novo cardiac complications, such as myocardial injury (MI) in approximately 8–12% of patients, myocarditis, and arrhythmias in 16.7%, among others (4–6). Additionally, patients with preexisting cardiovascular disease are associated with worse outcomes.
Hospitalized COVID-19 patients may experience elevated troponin levels, which are indicative of MI and are strongly associated with increased morbidity and mortality. The pathophysiology of MI in these patients remains unclear. Proposed mechanisms include direct viral invasion, imbalance between oxygen supply and demand, ischemic injury due to microvascular thrombus formation, and cytokine-mediated damage. Furthermore, an increased risk of thrombotic events due to atherosclerotic plaque rupture during viral infections has been documented (7–22).
There are some systematic reviews, such as the one published in 2021 by Alaa Hasan Alali et al., which included 42 studies evaluating a total of 4,326 hospitalized COVID-19 patients with evidence of MI. This analysis found that MI was associated with higher in-hospital mortality and worse outcomes in patients with severe COVID-19 (23). However, of the 42 studies included, only one was from Latin America: a Mexican cohort of 254 hospitalized COVID-19 patients published in 2020 by Heberto et al. This study reported that 28.7% of patients presented with MI, which was associated with a higher risk of severe complications and significantly increased mortality (63.0% vs. 23.7%) (24). Despite these findings, there is still limited information on the impact of MI on cardiovascular complications and mortality in the Latin American (LA) population. To address this gap, data from the Registro Latinoamericano de Enfermedad Cardiovascular y COVID-19 (CARDIO COVID 19–20 Registry) were analyzed to assess the prevalence and effect of MI on cardiovascular complications, hospital stay, and mortality in a LA population.
The CARDIO COVID 19–20 registry was designed, developed, and executed by Interamerican Council of Heart Failure and Pulmonary Hypertension (CIFACAH) of Inter-American Society of Cardiology (SIAC). Coordination was provided by the Clinical Research Center (CRC) of the Fundación Valle del Lili (FVL) in Cali, Colombia. The protocol received approval from both the CRC and the Human Ethics Committee of FVL (1,835), as well as the Executive Committee of CIFACAH/SIAC. Informed consent was not required for this study. This registry recruited patients between May 01, 2020, and June 30, 2021, and included a total of 3,260 patients from 44 institutions in 14 LA countries (22). Patients from 13 of the 14 countries were included because patients in El Salvador did not have troponin levels during hospitalization.
The present study was an analytical cross-sectional design, prospective in nature, including patients over 18 years old hospitalized for COVID-19, diagnosed via polymerase chain reaction, that were included in the CARDIO COVID 19–20 registry and that had a troponin value recorded during hospitalization. For this analysis, MI was defined as an elevation of troponin levels above normal values for each participating center. To maximize the sample size, only patients with available troponin measurements were included in the analysis. Patients without recorded troponin values were excluded, eliminating the need for imputation or handling of missing data for this variable.
Regarding key variables, such as echocardiographic data, as this was a retrospective study, the number of available echocardiograms was limited to what was documented in the medical records, and no imputation of missing data was performed. Although there were significant differences, these variables were not included in the multivariate models to avoid reducing the sample size and to ensure a more robust analysis.
Variables included in the multivariate Poisson regression models were selected based on a combination of clinical significance, findings from univariate analysis, and evidence from prior literature. This approach ensured that the models accounted for the most relevant predictors while maintaining robustness and interpretability.
For univariate analysis, quantitative variables were expressed as mean and standard deviation (SD) or median and interquartile range (IQR) based on the normality of distribution using the Shapiro–Wilk or Kolmogorov–Smirnov test. In contrast, qualitative variables were expressed as absolute values and percentages. Bivariate analysis considered the presence or absence of MI. A comparison between groups was made using Student's t-test or Mann–Whitney test for quantitative variables and the Chi-square test or Fisher's exact test for categorical variables. Bivariate and multivariate logistic regression models were conducted to estimate the association between different complications and outcomes with the presence of MI.
The survival probability in COVID-19 patients with presence of MI was calculated using the Kaplan–Meier method in order to generate the survival curves for Colombia. Poisson regression models with robust standard errors were utilized to calculate adjusted rate ratios (aRR) and unadjusted rate ratios (RR) and 95% confidence intervals (CI). Model goodness-of-fit was assessed using the Akaike information criterion (AIC). P values <0.05 were considered statistically significant. Statistical analyses were conducted using the RStudio V.1.4.1717 package.
Of the 3,260 patients recruited in the CARDIO COVID 19–20 Registry, 2,134 patients from 13 countries had a recorded troponin value during hospitalization, and 911 of them (42.7%) had an abnormal value or MI. Most of the recruited patients were from Colombia (42.3%), Chile (24.4%), and Costa Rica (6.7%). Among the included patients, those from Venezuela, Guatemala, Brazil, and Argentina had a higher proportion of patients with MI (Figures 1, 2).
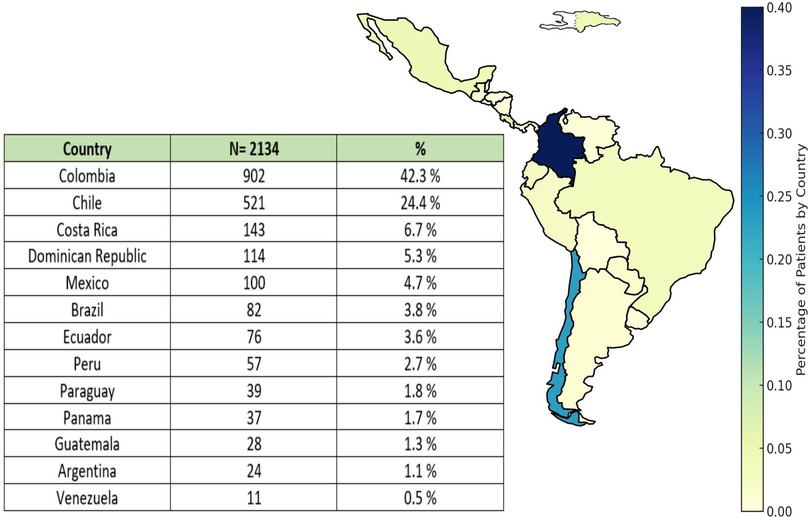
Figure 1. Geographic distribution of hospitalized patients with COVID-19 infection.
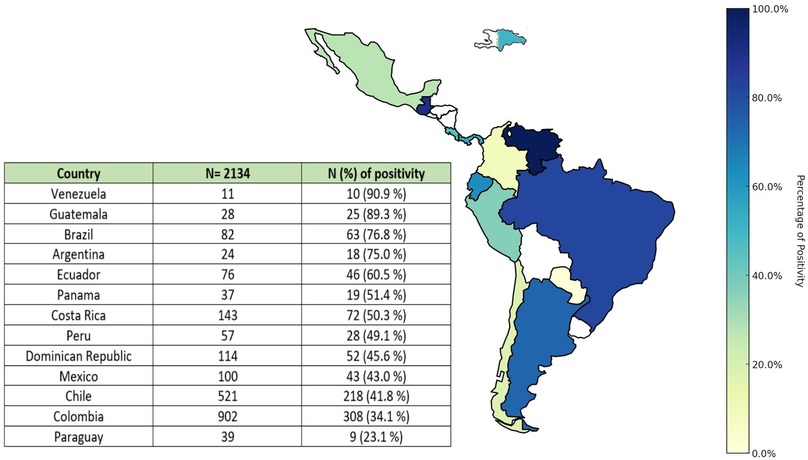
Figure 2. Geographic distribution of patients according to the presence of MI.
Of the total population included in this analysis (2,134), 64.2% were male, with a median age of 61 years. The most frequent comorbidities were overweight/obesity (52.4%), hypertension (49%), diabetes (27.8%), dyslipidemia (14.8%), and smoking (14.2%). Compared to the group without MI, the group with MI was predominantly male (66.7% vs. 60.9%; p = 0.007) and older (median: 66 years vs. 56 years, respectively). Moreover, patients with MI had a higher prevalence of hypertension, diabetes, and dyslipidemia (Table 1).
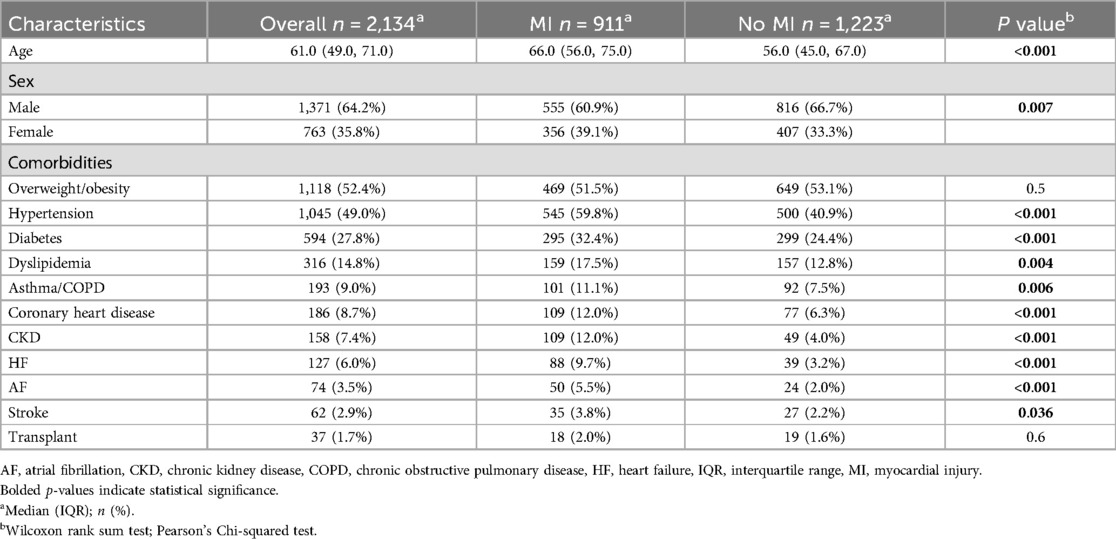
Table 1. Sociodemographic characteristics.
At admission, most common symptoms were dyspnea, fatigue, cough, fever, and myalgias; when comparing both groups, it was observed that except for dyspnea, the others were more frequent in patients without MI, and these differences were statistically significant. Significant differences were also observed in respiratory rate and oxygen saturation (p < 0.001). Regarding laboratory tests, it was observed that patients with MI had higher values of creatinine, hemoglobin, leukocytes, lymphocytes, both sensitive and ultrasensitive C-reactive protein (CRP), lactate dehydrogenase, ferritin, NT-proBNP, and D-dimer, with these differences being statistically significant compared to patients without MI (Table 2).
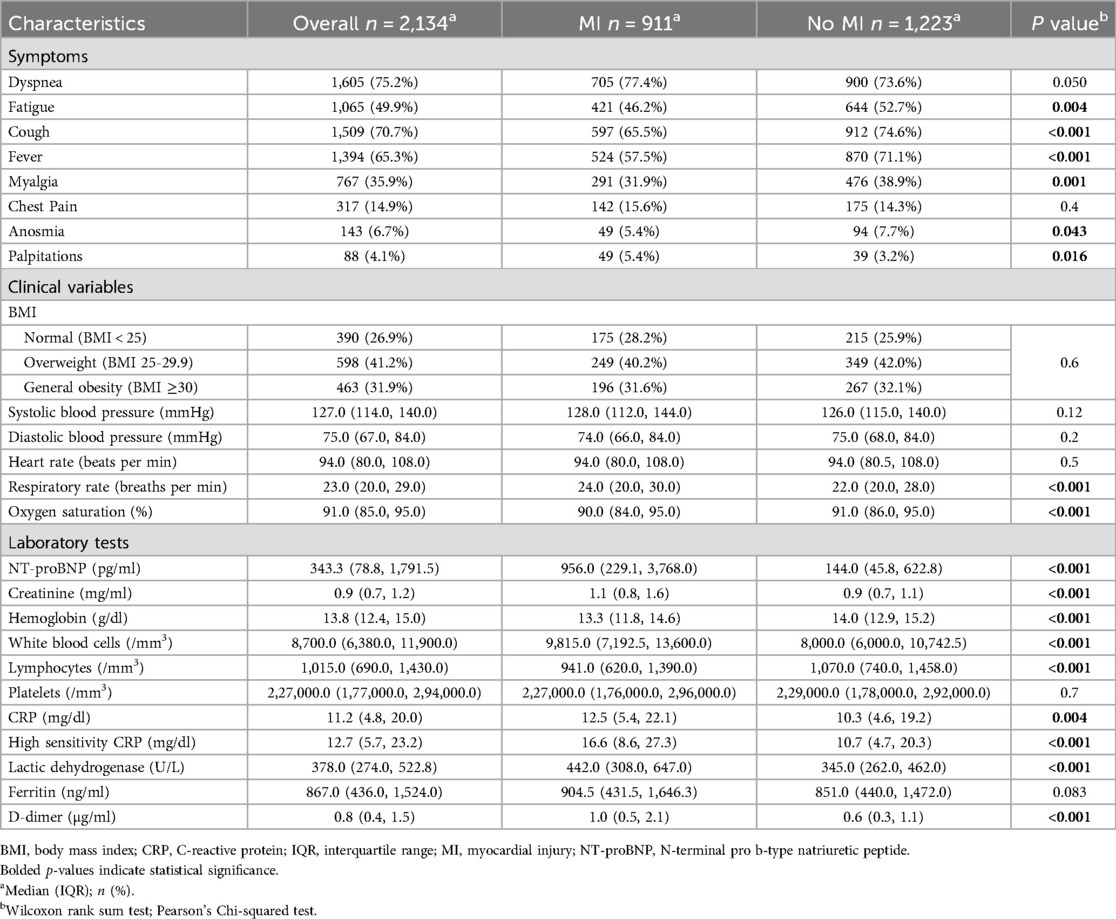
Table 2. Characteristics at admission.
In patients with MI with chest x-ray, a lower proportion of pulmonary infiltrates was found; conversely, a higher proportion of these patients had cardiomegaly (23.8%), pulmonary congestion (25.4%), and pleural effusion (14.2%) with strong statistical significance (p < 0.001) (Table 3).
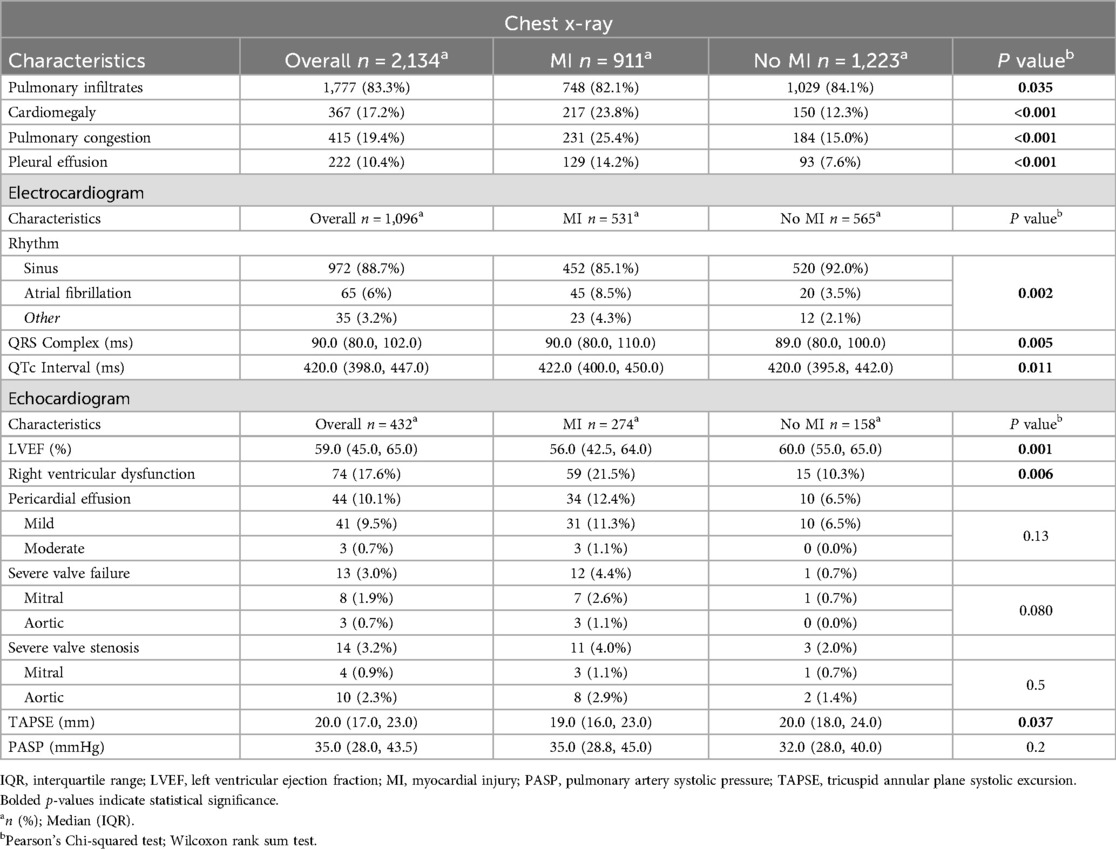
Table 3. Chest x-ray, electrocardiographic and echocardiographic findings.
A total of 1,096 electrocardiograms were performed in hospitalized patients with SARS-COV2 viral infection, of which 88.6% were in sinus rhythm. Patients with MI more frequently presented atrial fibrillation (8.5% vs. 3.5%) (Table 3).
Transthoracic echocardiography (TTE) was performed on 432 patients. The median LVEF was 59%, lower in patients with MI than those without MI (56% vs. 60%). Seventeen per cent of patients had right ventricular dysfunction, more significant in patients with MI (21.5% and 10.3 p = 0.006). 10% of patients with COVID-19 had mild pericardial effusion, with no differences by MI (p = 0.13). Also, there were no differences in prevalence of severe valvopathies (p = 0.5) (Table 3).
Regarding cardiovascular procedures performed, we found that 26 patients (1.2%) required thrombolysis and 50 patients (2.3%) underwent coronary angiography with a higher prevalence in the MI group (4.9% vs. 0.4%, p < 0.001). Of the patients undergoing angiography, 60% (30 patients) required coronary angioplasty and 2 patients required intra-aortic balloon pump implantation (Table 4).
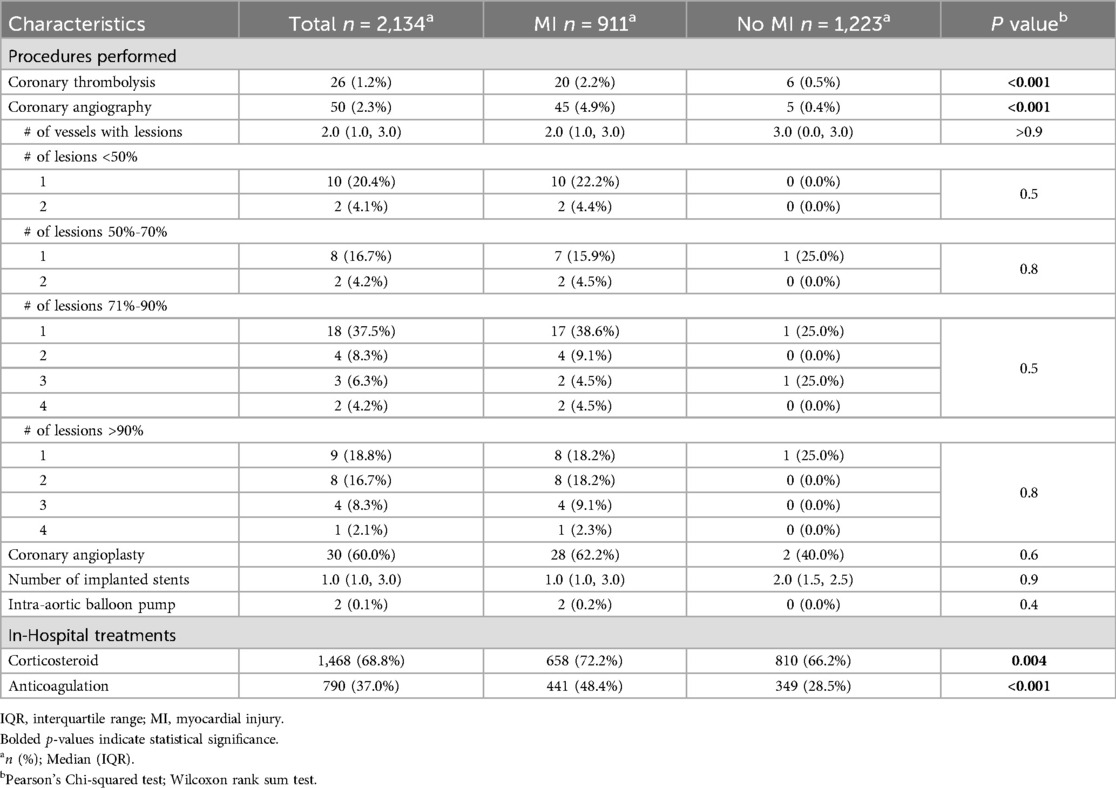
Table 4. In-Hospital treatments and procedures.
In the analysis of in-hospital treatments, patients with MI received anticoagulation more frequently than those without MI (48.4% vs. 28.5%; p < 0.001). Similarly, the use of corticosteroids was significantly higher in the MI group (72.2% vs. 66.2%; p = 0.004) (Table 4). Additional in-hospital treatments are detailed in Supplementary Table S2.
About in-hospital management for COVID-19, 68.8% of patients received corticosteroid therapy, with a higher proportion of patients with MI (72.2% vs. 66.2%, respectively; p = 0.004). Similarly, a higher proportion of patients with MI received anticoagulation (48.4% vs. 28.5%, respectively; p < 0.001). Conversely, thromboprophylaxis was more common in those without MI (71.5% vs. 60.2%, respectively) (p < 0.001).
Among the studied population, 60.8% required intensive care unit (ICU) admission, and 39.6% required invasive mechanical ventilation (IMV) (Supplementary Table S1). Hospital mortality occurred in 25.6% of cases. When evaluating factors associated with MI, patients with cardiac arrhythmia, pulmonary embolism, decompensated heart failure (DHF), inotropic support, as well as IMV had a higher risk of MI (Table 5).

Table 5. Cardiovascular complications and clinical outcomes.
A 90-day survival analysis was conducted for Colombia because we did not have the date of death for the entire population, for which we included 902 patients, among whom 308 patients had MI. A significant difference in survival was observed between the groups according to the presence of MI (184/308 with MI and 547/594 without it). When analyzing survival by sex, was not statistically significant (p = 0.054) (Figure 3).
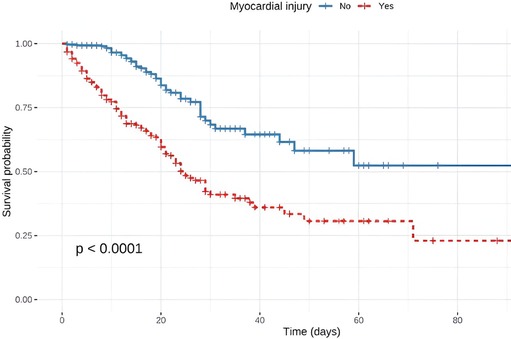
Figure 3. In-hospital survival analysis.
Patients with MI had a 95% higher risk of mortality after adjusting for other variables [aRR: 1.95, 95% confidence interval (CI): 1.66–2.28]. Additionally, it was evident that age, categorized, is significantly associated with mortality risk as age advanced. Male had a 23% higher risk of mortality compared to female.
Other variables such as chronic kidney disease [aRR: 1.31, 95% CI (1.1–1.56)] cardiac arrhythmias [aRR: 1.21, 95% CI (1.05–1.4)], DHF [aRR: 1.23, 95% CI (1.06–1.43)], inotropic support [aRR: 1.34, 95% CI (1.17–1.53)], vasopressor support [aRR: 1.83, 95% CI (1.44–2.33)], and IMV [aRR: 2.43, 95% CI (1.88–3.15)] were also risk factors for mortality (Figure 4).
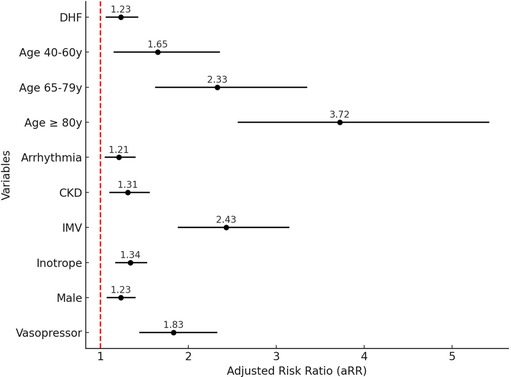
Figure 4. Factors associated with in-hospital mortality. CKD, chronic kidney disease; DHF, decompensated heart failure; IMV, invasive mechanical ventilation.
COVID-19, caused by the SARS-CoV-2 virus, was declared a worldwide pandemic by the World Health Organization (WHO) from January 30, 2020, to May 5, 2023 (25). While primarily a respiratory disease ranging from mild symptoms to acute respiratory distress syndrome, it is also associated with an increased risk of cardiovascular complications, particularly MI. MI, defined as an elevation of cardiac enzymes, is one of the most frequently reported cardiovascular complications in patients with COVID-19, occurring in up to 28% of cases and being strongly associated with worse outcomes and increased mortality (4, 26–28).
This multicenter observational study included 2,134 patients from 44 institutions across 13 LA countries. Among these patients, 911 (42.7%) had MI, as determined by elevated troponin levels during hospitalization. Patients with MI were older (median age 66 vs. 56 years) and had a higher prevalence of comorbidities such as hypertension (59.8%), overweight/obesity (51.5%), diabetes (32.4%), coronary artery disease (12%), and chronic kidney disease (12%). These patients also experienced more severe clinical courses, with higher rates of ICU admission (69.7% vs. 54.1%) and invasive mechanical ventilation (39.6% vs. 32.7%). Overall, in-hospital mortality was significantly higher in patients with MI (43.1% vs. 12.6%; p < 0.0001), compared to an overall mortality rate of 25.6%.
The association between MI and mortality has been described in the literature as multifactorial, correlating with the severity of COVID-19 manifestations and highlighting the importance of identifying high-risk patients (10, 15, 20). Similarly, our study identified MI as an independent marker of in-hospital mortality after adjusting for other major complications. These findings underscore the critical role of MI in determining outcomes for hospitalized COVID-19 patients and emphasize the need for early identification and targeted management of high-risk individuals.
When comparing with international cohorts, the Wuhan cohort reported similar findings, with patients with MI being older (74 vs. 60 years) and having higher prevalence of comorbidities such as hypertension (59.8%) and coronary heart disease (29.3%). In this cohort, the mortality risk for patients with MI was higher (Hazard Ratio: 4.26, 95% CI: 1.92–9.49) compared to our study's observed risk (RR: 1.95) (10). Additionally, patients with MI in Wuhan required more IMV (22% vs. 4.2%) and more frequently received treatments such as corticosteroids, immunoglobulin, and antibiotics (9, 10).
In the cohort of 305 patients published in JAMA, a 18.7% higher mortality rate was found in patients with MI (26.8% vs. 5.2%) compared to those without MI. This cohort also reported higher admission rates to intensive care units (52.1% vs. 30.4%) and a greater requirement for IMV (43.4% vs. 20%) (20).
In terms of diagnostic procedures, 1,096 electrocardiograms and 432 transthoracic echocardiograms (TTE) were performed in our study population. Among these, 26 patients underwent thrombolysis, and 50 underwent coronary angiography. In other studies, such as the JACC cohort of 305 patients, MI was present in 62.6% of cases and was associated with more severe cardiovascular abnormalities, including left ventricular dysfunction (26.3%), alterations in contractility (23.7%), and right ventricular dysfunction (18.4%) (20).
In terms of in-hospital pharmacological treatment, anticoagulant use was reported in 44% of patients overall in the HOPE-COVID19 multicenter study (29). The Spanish study by Arévalos et al. found a higher rate of 86.4%, with lower usage among patients with MI compared to those without (79.2% vs. 88.4%) (30). A Vietnamese cohort reported an even greater overall use of anticoagulants (94.3%), with no significant differences between patients with and without MI (93.0% vs. 96.0%, p = 0.121) (31). In contrast, anticoagulant use in our cohort was lower overall (37%) but significantly higher in patients with MI compared to those without (48.4% vs. 28.5%; p < 0.001). These findings emphasize regional differences in therapeutic strategies and the need to assess how anticoagulant practices influence patient outcomes across diverse settings.
Building on these findings, a comparison of our results in Latin America with other key studies from regions such as the United States, Europe, and Asia reveals notable similarities and differences. In the LA population, MI was associated with a 95% higher risk of mortality (aRR: 1.95, 95% CI: 1.66–2.28). Patients with MI in the LA population were older, with a median age of 66.0 years compared to those without MI, 61.0 years, and younger than those reported in the U.S. meta-analysis, where the mean age of patients with MI was 73 years (32). Similar trends were observed in a systematic review from China, where MI was associated with a threefold increase in mortality risk (RR: 3.85, 95% CI: 2.13–6.96) (16). Additionally, a 2021 systematic review by Alaa Hasan Alali et al. analyzed 4,326 hospitalized COVID-19 patients across 42 studies from multiple countries, including China, Spain, and the USA, and found that elevated troponin levels were strongly associated with poor outcomes, with an odds ratio (OR) of 7.92 (95% CI: 3.70–16.97, p < 0.00001) (23).
A survival analysis was performed on patients from Colombia (902 patients), of which 308 patients had MI and 594 did not. The number of deceased patients was 124 and 47, respectively. A significant difference in mortality was observed between groups based on the presence of MI, with a 75% decrease in survival for patients with MI from day 10 (p < 0.0001). Given the high mortality, a global analysis was performed to identify whether it was secondary to a selection bias due to the inclusion of patients with reported troponin levels, where it was found that of the 1,125 patients who did not undergo the troponin test, 285 patients died (25.5%), while among those who did undergo the test (2,134 patients), there were 546 deaths (25.3%) with no statistically significant difference (p > 0.9). Regarding the specific analysis of Colombia, among the 284 patients who did not undergo the troponin test, 46 (16.2%) died, while among the 902 patients who underwent the test, there were 171 deaths (19.0%) without statistically significant difference (p < 0.3). This interpretation suggests that, in this population, the decision to perform troponin testing does not appear to be associated with a change in the observed mortality rate.
The present multicenter observational study represents a significant effort to include data from multiple institutions across 13 LA countries, reflecting the diverse realities of developing nations during the COVID-19 pandemic. This collaboration highlights the regional challenges and strengths in managing COVID-19, providing a comprehensive perspective on the impact of MI on cardiovascular outcomes in hospitalized patients.
Data collection in this study was retrospective, relying on manual extraction of electronic medical records from multiple institutions, which introduces the risk of information bias due to inconsistencies in record quality and lack of standardization. Additionally, the manual process may have introduced human errors or subjective interpretations. Future studies should consider more robust data collection techniques, such as prospective data collection or automated systems, to minimize human intervention.
Not all patients underwent TTE, and it is likely that only those considered at higher clinical risk were selected for this procedure. This selection bias may have led to an overrepresentation of patients with more severe or clinically significant cardiovascular issues, potentially skewing the results. Furthermore, as all echocardiograms were interpreted locally at each participating institution rather than centrally, variations in interpretation and the lack of standardized protocols for echocardiogram analysis could have introduced additional inconsistencies in the data. A centralized echocardiography reading system, along with the implementation of standardized imaging protocols, would be beneficial in future research to ensure more uniform and reliable interpretation of results.
The survival analysis was performed only for Colombia, as the date of death was not available for the other participating countries. Therefore, a review of the mortality registry for Colombia was necessary to conduct this analysis.
Finally, this study is limited to hospital outcomes, and long-term follow-up data was not available for all patients. Long-term cardiovascular sequelae in troponin-positive COVID-19 patients remain largely unexplored, and future studies should include long-term follow-up to assess the lasting impact on cardiovascular health.
Patients with COVID-19 and MI exhibit a wide spectrum of cardiac abnormalities. MI is associated with a higher risk of complications such as ICU admission, use of inotropic and vasopressor support, and increased hospital mortality. This multicenter observational study uniquely represents data from 2,134 patients across 13 LA countries, highlighting the regional burden and clinical outcomes of MI during the COVID-19 pandemic. Troponin evaluation should be considered in patients with COVID-19 to characterize the underlying cardiac substrate, for risk stratification, and potentially to guide management strategies. The findings underscore the importance of addressing healthcare disparities in Latin America to improve outcomes for high-risk patients.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
The studies involving humans were approved by Comité de Ética en Investigación Biomédica IRB de la Fundación Valle del Lili. The studies were conducted in accordance with the local legislation and institutional requirements. The ethics committee/institutional review board waived the requirement of written informed consent for participation from the participants or the participants' legal guardians/next of kin because Written informed consent was waived because the study involved retrospective analysis of de-identified data collected from electronic medical records, posing minimal risk to participants and ensuring their confidentiality.
PC: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Supervision, Writing – original draft, Writing – review & editing. BC: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Supervision, Writing – original draft, Writing – review & editing. DC: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Supervision, Writing – original draft, Writing – review & editing. HL: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Supervision, Writing – original draft, Writing – review & editing. IM: Investigation, Writing – original draft, Writing – review & editing. NF: Investigation, Writing – original draft, Writing – review & editing. RL: Investigation, Writing – original draft, Writing – review & editing. JM: Investigation, Writing – original draft, Writing – review & editing. CH: Investigation, Writing – original draft, Writing – review & editing. JL: Investigation, Writing – original draft, Writing – review & editing. LC: Investigation, Writing – original draft, Writing – review & editing. VR: Investigation, Writing – original draft, Writing – review & editing. RR: Investigation, Writing – original draft, Writing – review & editing. HF: Investigation, Writing – original draft, Writing – review & editing. AU: Investigation, Writing – original draft, Writing – review & editing. JS: Investigation, Writing – original draft, Writing – review & editing. EL: Investigation, Writing – original draft, Writing – review & editing. WY: Investigation, Writing – original draft, Writing – review & editing. MQ: Investigation, Writing – original draft, Writing – review & editing. AR: Investigation, Writing – original draft, Writing – review & editing. PS: Investigation, Writing – original draft, Writing – review & editing. AA: Investigation, Writing – original draft, Writing – review & editing. AV: Data curation, Formal Analysis, Software, Visualization, Writing – original draft, Writing – review & editing. JG: Conceptualization, Formal Analysis, Investigation, Supervision, Writing – original draft, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. The study was funded by the Centro de Investigaciones Clínicas of Fundación Valle del Lili, Cali, Colombia.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declare that no Generative AI was used in the creation of this manuscript.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fcvm.2025.1545142/full#supplementary-material
1. Wu Z, McGoogan JM. Characteristics of and important lessons from the Coronavirus disease 2019 (COVID-19) outbreak in China: summary of a report of 72314 cases from the Chinese center for disease control and prevention. JAMA. (2020) 323(13):1239. doi: 10.1001/jama.2020.2648
2. Johns Hopkins Coronavirus Resource Center. COVID-19 map. Available online at: https://coronavirus.jhu.edu/map.html (cited September 13, 2023).
3. Mehra MR, Ruschitzka F. COVID-19 illness and heart failure. JACC Heart Fail. (2020) 8(6):512–4. doi: 10.1016/j.jchf.2020.03.004.32360242
4. Wang D, Hu B, Hu C, Zhu F, Liu X, Zhang J, et al. Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus–infected pneumonia in Wuhan, China. JAMA. (2020) 323(11):1061. doi: 10.1001/jama.2020.1585
5. Bansal M. Cardiovascular disease and COVID-19. Diabetes Metab Syndr. (2020) 14(3):247–50. doi: 10.1016/j.dsx.2020.03.013
6. López-Ponce de León JD, Cárdenas-Marín PA, Giraldo-González GC, Herrera-Escandón Á. Coronavirus—COVID 19: más allá de la enfermedad pulmonar, qué es y qué sabemos del vínculo con el sistema cardiovascular. Rev Colomb Cardiol. (2020) 27(3):142–52. doi: 10.1016/j.rccar.2020.04.006
7. Metkus TS, Sokoll LJ, Barth AS, Czarny MJ, Hays AG, Lowenstein CJ, et al. Myocardial injury in severe COVID-19 compared with non–COVID-19 acute respiratory distress syndrome. Circulation. (2021) 143(6):553–65. doi: 10.1161/circulationaha.120.050543
8. Fauci AS, Lane HC, Redfield RR. COVID-19—navigating the uncharted. N Engl J Med. (2020) 382(13):1268–9. doi: 10.1056/nejme2002387
9. Guo T, Fan Y, Chen M, Wu X, Zhang L, He T, et al. Cardiovascular implications of fatal outcomes of patients with coronavirus disease 2019 (COVID-19). JAMA Cardiol. (2020) 5(7):811. doi: 10.1001/jamacardio.2020.1017
10. Shi S, Qin M, Shen B, Cai Y, Liu T, Yang F, et al. Association of cardiac injury with mortality in hospitalized patients with COVID-19 in Wuhan, China. JAMA Cardiol. (2020) 5(7):802. doi: 10.1001/jamacardio.2020.0950
11. Zhou F, Yu T, Du R, Fan G, Liu Y, Liu Z, et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study. Lancet. (2020) 395(10229):1054–62. doi: 10.1016/s0140-6736(20)30566-3
12. Chen T, Wu D, Chen H, Yan W, Yang D, Chen G, et al. Clinical characteristics of 113 deceased patients with coronavirus disease 2019: retrospective study. Br Med J. (2020) 368:m1091. doi: 10.1136/bmj.m1091
13. Huang C, Wang Y, Li X, Ren L, Zhao J, Hu Y, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet. (2020) 395(10223):497–506. doi: 10.1016/s0140-6736(20)30183-5
14. Smeeth L, Thomas SL, Hall AJ, Hubbard R, Farrington P, Vallance P. Risk of myocardial infarction and stroke after acute infection or vaccination. N Engl J Med. (2004) 351(25):2611–8. doi: 10.1056/nejmoa041747
15. Bavishi C, Bonow RO, Trivedi V, Abbott JD, Messerli FH, Bhatt DL. Special article—acute myocardial injury in patients hospitalized with COVID-19 infection: a review. Prog Cardiovasc Dis. (2020) 63(5):682–9. doi: 10.1016/j.pcad.2020.05.013
16. Li J-W, Han T-W, Woodward M, Anderson CS, Zhou H, Chen Y-D, et al. The impact of 2019 novel coronavirus on heart injury: a systematic review and meta-analysis. Prog Cardiovasc Dis. (2020) 63(4):518–24. doi: 10.1016/j.pcad.2020.04.008
17. Lippi G, Lavie CJ, Sanchis-Gomar F. Cardiac troponin I in patients with coronavirus disease 2019 (COVID-19): evidence from a meta-analysis. Prog Cardiovasc Dis. (2020) 63(3):390–1. doi: 10.1016/j.pcad.2020.03.001
18. Kwong JC, Schwartz KL, Campitelli MA, Chung H, Crowcroft NS, Karnauchow T, et al. Acute myocardial infarction after laboratory-confirmed influenza infection. N Engl J Med. (2018) 378(26):2538–41. doi: 10.1056/nejmc1805679
19. Stefanini GG, Montorfano M, Trabattoni D, Andreini D, Ferrante G, Ancona M, et al. ST-elevation myocardial infarction in patients with COVID-19: clinical and angiographic outcomes. Circulation. (2020) 141(25):2113–6. doi: 10.1161/circulationaha.120.047525
20. Giustino G, Croft LB, Stefanini GG, Bragato R, Silbiger JJ, Vicenzi M, et al. Characterization of myocardial injury in patients with COVID-19. J Am Coll Cardiol. (2020) 76(18):2043–55. doi: 10.1016/j.jacc.2020.08.069
21. Yang X, Yu Y, Xu J, Shu H, Xia J, Liu H, et al. Clinical course and outcomes of critically ill patients with SARS-CoV-2 pneumonia in Wuhan, China: a single-centered, retrospective, observational study. Lancet Respir Med. (2020) 8(5):475–81. doi: 10.1016/S2213-2600(20)30079-5
22. Gómez-Mesa JE, Galindo-Coral S, Montes MC, Alarco W, Barisani JL, Magaña A, et al. Latin-American Registry of cardiovascular disease and COVID-19: rationale and design of the CARDIO COVID 19–20 registry. Glob Heart. (2021) 16(1):14. doi: 10.5334/gh.925
23. Alali AH, Smaisem MS, Alsheikh AM, Alshareef AA, Smaisem FS, Alnahar BW, et al. Myocardial injuries among patients with COVID-19: a systematic review. Infez Med. (2021) 29(3):345–54. doi: 10.53854/liim-2903-5
24. Heberto AB, Carlos PCJ, Antonio CRJ, Patricia PP, Enrique TR, Danira MPJ, et al. Implications of myocardial injury in Mexican hospitalized patients with coronavirus disease 2019 (COVID-19). IJC Heart Vasc. (2020) 30:100638. doi: 10.1016/j.ijcha.2020.100638
25. Cucinotta D, Vanelli M. WHO Declares COVID-19 a pandemic. Acta Biomed. (2020) 91(1):157–60. doi: 10.23750/abm.v91i1.9397
26. Topol EJ. COVID-19 can affect the heart. Science. (2020) 370(6515):408–9. doi: 10.1126/science.abe2813
27. Zheng Y-Y, Ma Y-T, Zhang J-Y, Xie X. COVID-19 and the cardiovascular system. Nat Rev Cardiol. (2020) 17(5):259–60. doi: 10.1038/s41569-020-0360-5
28. Calvillo-Argüelles O, Ross HJ. Cardiac considerations in patients with COVID-19. CMAJ. (2020) 192(23):E630. doi: 10.1503/cmaj.200562
29. Santoro F, Núñez-Gil IJ, Viana-Llamas MC, Maroun Eid C, Romero R, Fernández Rozas I, et al. Anticoagulation therapy in patients with coronavirus disease 2019: results from a multicenter international prospective registry (health outcome predictive evaluation for Corona virus disease 2019 [HOPE-COVID19]). Crit Care Med. (2021) 49(6):e624. doi: 10.1097/CCM.0000000000005010
30. Arévalos V, Ortega-Paz L, Rodríguez-Arias JJ, Calvo M, Castrillo L, Salazar A, et al. Myocardial injury in COVID-19 patients: association with inflammation, coagulopathy and in-hospital prognosis. J Clin Med. (2021) 10(10):2096. doi: 10.3390/jcm10102096
31. Vu VH, Nguyen TC, Pham QDD, Pham DN, Le LB, Le KM. Prevalence and impact of myocardial injury among patients hospitalized with COVID-19. Front Cardiovasc Med. (2023) 10:1202332. doi: 10.3389/fcvm.2023.1202332/full
Keywords: myocardial injury, covid-19, cardiovascular complications, hospital mortality, troponin levels
Citation: Cárdenas-Marín PA, Cordoba-Melo BD, Carrillo-Gómez DC, León-Giraldo H, Mendoza I, Flórez N, Larrea Gómez RE, Mercedes JM, Herrera CJ, Lugo-Peña J, Cárdenas-Aldaz LP, Rossel V, Ramírez Ramírez R, Fernández HF, Retana AU, Sierra-Lara Martinez JD, Figueiredo EL, Yabar Galindo WG, Quintana Da Silva MA, Romero A, Silva P, Alvarado A, Valencia A and Gomez-Mesa JE (2025) Impact of myocardial injury on cardiovascular complications in hospitalized patients with COVID-19: insights from Latin America. Front. Cardiovasc. Med. 12:1545142. doi: 10.3389/fcvm.2025.1545142
Received: 14 December 2024; Accepted: 26 January 2025;
Published: 17 February 2025.
Edited by:
DeLisa Fairweather, Mayo Clinic Florida, United StatesReviewed by:
Zhengwu Sun, Dalian Municipal Central Hospital, ChinaCopyright: © 2025 Cárdenas-Marín, Cordoba-Melo, Carrillo-Gómez, León-Giraldo, Mendoza, Flórez, Larrea Gómez, Mercedes, Herrera, Lugo-Peña, Cárdenas-Aldaz, Rossel, Ramírez Ramírez, Fernández, Retana, Sierra-Lara Martinez, Figueiredo, Yabar Galindo, Quintana Da Silva, Romero, Silva, Alvarado, Valencia, Gomez-Mesa. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Juan Esteban Gomez-Mesa, anVhbi5nb21lei5tZUBmdmwub3JnLmNv
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.