 Li-Chin Liao
Li-Chin Liao Yun-Yu Chen
Yun-Yu Chen Yun-Ching Fu
Yun-Ching Fu Hui-Chih Hung2,5,12*
Hui-Chih Hung2,5,12*

95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Cardiovasc. Med. , 14 March 2025
Sec. Pediatric Cardiology
Volume 12 - 2025 | https://doi.org/10.3389/fcvm.2025.1522603
Introduction: Atrial septal defect (ASD) increases pulmonary to systemic flow ratio (Qp/Qs) which is an important determinant factor for treatment. N-terminal pro-B-type natriuretic peptide (NT-proBNP) levels are correlated with volume overloading of the heart. This study aims to explore the relationship between Qp/Qs and NT-proBNP levels in children with ASD.
Materials and methods: Between January 2010 and December 2023, 464 patients under 20 years old with ASD who underwent cardiac catheterization and received NT-proBNP test were enrolled retrospectively. Baseline characteristics such as sex, body weight, and age were recorded. Qp/Qs was measured during standardized right heart catheterization according to Fick principle.
Results: A significant positive correlation existed between NT-proBNP and Qp/Qs (R = 0.507, P < 0.001), with an R2 of 0.258. The linear regression model indicates that a one-unit (pg/ml) increase in NT-proBNP corresponded to a 0.003-unit increase in Qp/Qs (P < 0.001). Patients with a Qp/Qs ratio ≥ 2 had significantly higher NT-proBNP levels than those with a ratio <2 (P < 0.001).
Conclustion: This study, the largest cohort to date, reveals the correlation between non-invasive NT-proBNP level and invasive Qp/Qs measurement in children with ASD.
Atrial septal defects (ASDs) represent around 10–15 percent of all congenital heart diseases. The estimated occurrence at birth is approximately 1–2 per 1,000 live births (1–4). The left-to-right shunt in ASD increases pulmonary to systemic flow ratio (Qp/Qs) ratio, leading to hemodynamic changes by increasing the volume load on the right heart and affecting the left heart (5–7). The indication for surgical repair is a Qp/Qs greater than 2.0, as this imposes a significant burden on the heart (8, 9). N-terminal pro-B-type natriuretic peptide (NT-proBNP) is a hormone secreted by the heart in response to elevated pressure, volume overload, or cardiac stress. Previous studies have shown a correlation between NT-proBNP levels and volume overloading of the heart. However, there were limited studies with small sample sizes that explore the relationship between Qp/Qs ratio and NT-proBNP levels in patients with ASD (10–12). Early intervention has the potential to reduce morbidity and mortality in children (7, 13, 14). However, Accurate measurement of Qp/Qs typically requires cardiac catheterization, which is an invasive procedure. In contrast, NT-proBNP levels can be determined quickly and non-invasively through a simple blood test. Our aim is to explore the correlation between Qp/Qs and NT-proBNP levels. If such a correlation exists, NT-proBNP could potentially serve as a non-invasive predictor of the hemodynamic burden in patients with ASD.
Between January 2010 and December 2023, 464 patients under 20 years old with ASD who underwent cardiac catheterization and received NT-proBNP test were enrolled retrospectively. The exclusion criteria were those who had congenital heart disease other than ASD, and patients who were not suitable for cardiac catheterization. This study was approved by the Committee on Human Studies (Institutional Review Board) at Taichung Veterans General Hospital (TCVGH-IRB no. CG16272B).
Baseline characteristics were collected including sex, body weight, age, and body surface area. All patients had no other congenital heart or systemic disease. All patients underwent right cardiac catheterization under conscious sedation. Hemodynamic parameters, such as pulmonary blood flow (Qp) and systemic blood flow (Qs), were calculated using the Fick formula. A normal Qp/Qs ratio is 1, with a ratio exceeding 2 typically indicating a significant left-to-right shunt and volume overload. Pulmonary hypertension (PH) is diagnosed when the mean pulmonary artery pressure exceeds 20 mmHg, as measured directly in the cardiac catheterization lab. Venous blood was collected without fasting beforehand and 5–10 ml blood was stored in a tube without anticoagulant after admission and was transferred immediately to the hospital's Department of Laboratory Medicine. The normal reference range of NTproBNP was 0–125 pg/ml in our laboratory. The defect size was measured using standard echocardiographic techniques, including subcostal, precordial, or apical imaging over at least two cardiac cycles, with the results averaged.
Continuous variables were presented as mean ± standard deviation (SD), and categorical variables were summarized as absolute numbers and percentages. Group comparisons for continuous variables were conducted using Student's t-test for two groups, while categorical variables were analyzed using the Chi-square test. Linear regression was employed to assess the relationship between NT-proBNP (independent variable) and Qp/Qs (dependent variable), with the strength of the association quantified by the correlation coefficient (R) and the coefficient of determination (R2). To further evaluate the effect of Qp/Qs groups on NT-proBNP levels after multivariable adjustment, a generalized estimating equations (GEE) model with a linear link function was utilized. The multivariable model was adjusted for age, sex, body surface area, mean right atrium pressure (RAm), mean pulmonary artery pressure (PAm), fluoroscopy time, and procedure time. The results from the GEE analysis were reported as beta coefficients with 95% confidence intervals (CIs). Data were analyzed using SPSS Statistics (Version 23.0, Chicago, IL, USA). A p-value <0.05 was considered significant.
The baseline characteristics of the 464 patients with ASD enrolled in this study are presented in Table 1. The cohort consisted of 200 males (43.1%) and 264 females (56.9%) with a mean age of 7.8 ± 4.7 years. The mean body weight was 27.4 ± 16.6 kg. Hemodynamic assessment via right heart catheterization revealed a RAm of 5.3 ± 3.3 mmHg and a PAm of 17.3 ± 4.9 mmHg. The mean Qp/Qs ratio was 1.89 ± 0.67, with 130 patients (28.0%) presenting a Qp/Qs ratio ≥ 2. The mean NT-proBNP level was 84.4 ± 97.6 pg/ml. Notably, patients with a Qp/Qs ratio ≥ 2 had significantly higher NT-proBNP levels (P < 0.001), higher PAm (P < 0.001), longer fluoroscopy time (P = 0.003), and longer procedure time (P < 0.001) compared to those with a Qp/Qs ratio < 2.
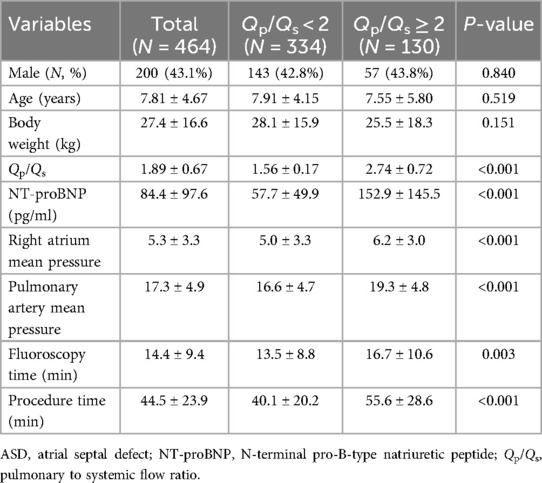
Table 1. Baseline characteristics of children with ASD.
Figure 1 illustrates the scatter plot of the association between NT-proBNP and Qp/Qs, demonstrating a significant positive correlation (R = 0.507, P < 0.001) with an R2 of 0.258. The linear regression model estimated that for each unit increase in NT-proBNP, there was a corresponding increase in Qp/Qs by 0.003 units (P < 0.001). This indicates a moderate association between higher NT-proBNP levels and increased Qp/Qs ratios. Figure 2 depicts the NT-proBNP levels stratified by Qp/Qs group (<2 vs. ≥2). Patients with a Qp/Qs ratio ≥ 2 exhibited significantly higher NT-proBNP levels compared to those with a Qp/Qs ratio < 2 (P < 0.001). The box plot shows the distribution of NT-proBNP levels within each group, highlighting the greater dispersion and higher median levels in the Qp/Qs ≥ 2 group.
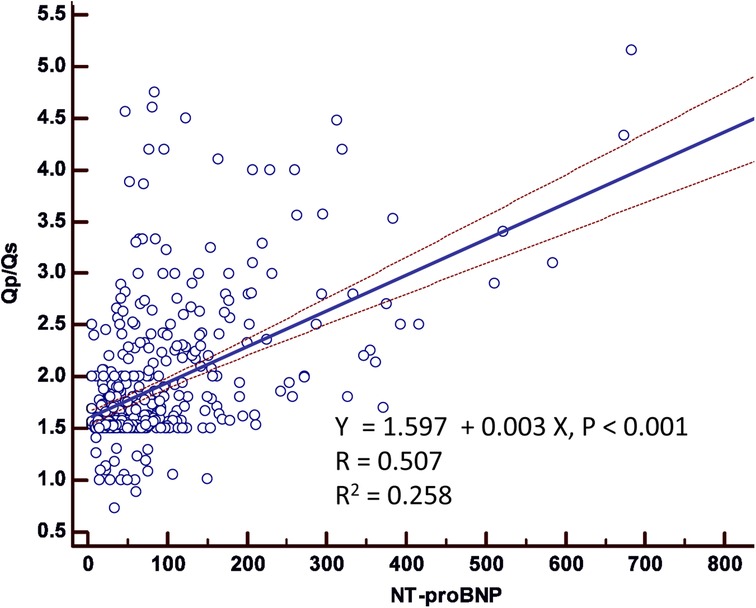
Figure 1. Scatter plot of association between NT-proBNP and Qp/Qs.
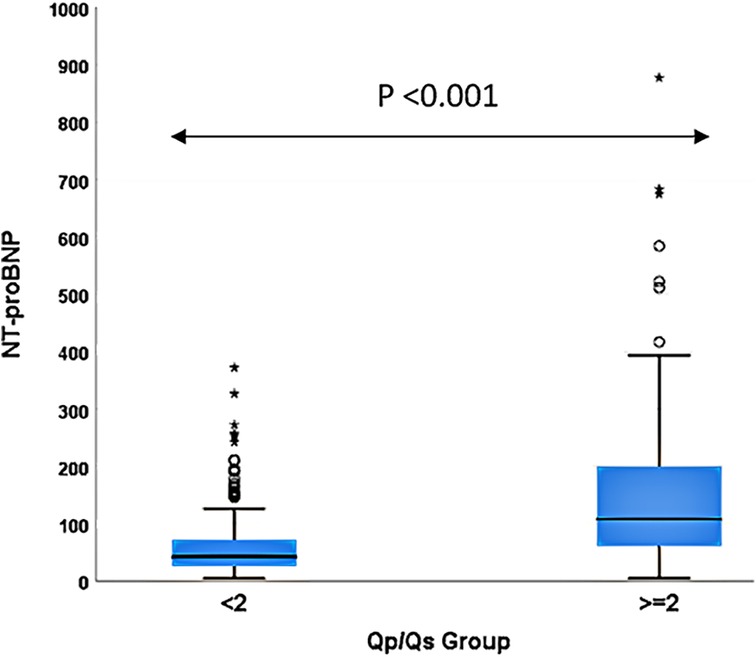
Figure 2. NT-proBNP levels according to Qp/Qs groups.
Univariable analysis (Table 2) revealed a significant association between the Qp/Qs ratio and NT-proBNP levels. For continuous Qp/Qs, the analysis showed that for each unit increase in Qp/Qs, NT-proBNP levels increased by 74.4 pg/ml (95% CI: 62.8–86.0, P < 0.001). Those with a Qp/Qs ratio ≥ 2 showed a significant increase in NT-proBNP levels (Beta: 95.3, 95% CI: 69.8–120.7, P < 0.001). Multivariable analysis, adjusted for age, sex, body surface area, RAm, PAm, fluoroscopy time, and procedure time, confirmed that a higher Qp/Qs ratio remained independently associated with elevated NT-proBNP levels. Specifically, the multivariable model indicated that for each unit increase in Qp/Qs, NT-proBNP levels increased by 68.3 pg/ml (95% CI: 47.0–89.6, P < 0.001). Furthermore, in the multivariable model, patients with a Qp/Qs ratio ≥ 2 continued to show significantly higher NT-proBNP levels compared to those with Qp/Qs < 2 (Beta: 72.7, 95% CI: 50.8–94.5, P < 0.001).
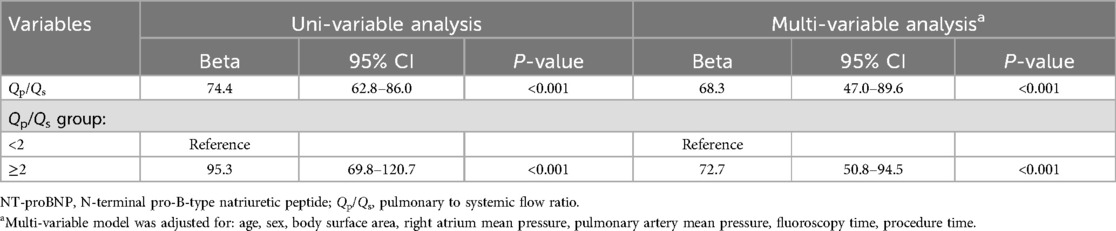
Table 2. Effect of Qp/Qs groups on NT-proBNP levels after multivariable adjustment.
Further analysis presented in Table 3 examined the effect of NT-proBNP levels on Qp/Qs ratios. Univariable analysis indicated that continuous NT-proBNP levels were significantly associated with Qp/Qs, with a Beta of 0.003 (95% CI: 0.002–0.004, P < 0.001). Stratifying NT-proBNP into groups using <125 pg/ml as the reference, patients with NT-proBNP levels ≥125 pg/ml exhibited significantly higher Qp/Qs ratios (Beta: 0.755, 95% CI: 0.567–0.943, P < 0.001). The multivariable analysis, adjusted for the same covariates, corroborated these findings, showing that NT-proBNP levels ≥125 pg/ml remained significantly associated with higher Qp/Qs ratios (Beta: 0.664, 95% CI: 0.470–0.858, P < 0.001). Our study revealed significant differences in NT-ProBNP level between the Qp/Qs < 2 and Qp/Qs ≥ 2 groups (57.7 ± 49.9 vs. 152.9 ± 145.5 pg/ml; P < 0.001). The scatter plot of the association between NT-proBNP and Qp/Qs showed a significant correlation (P = 0.001).
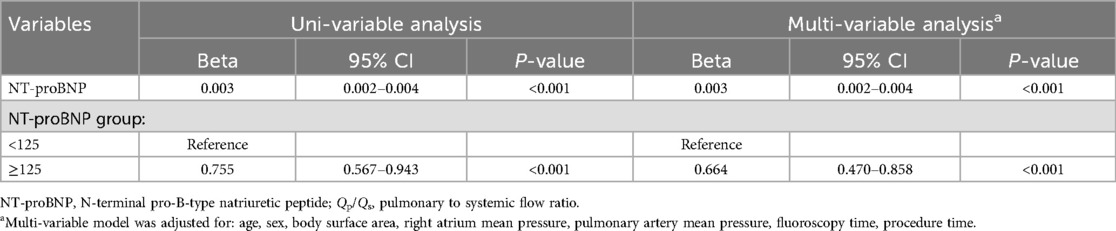
Table 3. Effect of NT-proBNP groups on Qp/Qs levels after multivariable adjustment.
This study represents the largest cohort to date examining the strong relationship between non-invasive NT-proBNP levels and invasive Qp/Qs measurements in children with ASD. Smaller-scale studies with limited sample sizes have reported that NT-proBNP levels were higher in their ASD group (79 pg/ml) than in the control cohort (57 pg/ml), with statistical significance (P < 0.05). This finding highlights the potential of NT-proBNP level to serve as a diagnostic indicator for ASD size, aligning with echocardiographic assessments (15). Additionally, a prior study found elevated serum NT-proBNP levels in individuals with larger defects. These studies indicate that employing NT-proBNP level as a diagnostic marker can effectively anticipate the size of these cardiac defects (16).
The persistent left-to-right shunt in heart defects continuously influences the pulmonary artery, inducing vascular remodeling. This process leads to a progressive increase in arterial pressure and resistance, ultimately resulting in pulmonary hypertension. Numerous humoral regulators actively participate in the intricate regulation of the cardiovascular system during the progression of this condition. The levels of circulating NTproBNP have been shown to be correlated with pulmonary hypertension. NTproBNP levels have also been correlated with mean pulmonary pressure, pulmonary vascular resistance, right atrial pressure, and cardiac index (17, 18). Elevated NTproBNP levels might indicate remodeling of the right ventricle, resulting in compromised systolic function of the right ventricle (19). We observed a positive correlation between NTproBNP increase and shunt volume, as measured by cardiac catheterization, in patients with ASD. NTproBNP demonstrated acceptable accuracy in predicting intracardiac shunt magnitude in ASD cases. A previous study with a smaller sample size demonstrated an association between B-type natriuretic peptide (BNP) levels and shunt severity in septal defect patients, indicating a significant positive correlation between plasma BNP levels and the magnitude of the shunts (20). Combining NTproBNP with Doppler echocardiography enhances prognostic accuracy, sensitivity, specificity, and predictive values for pulmonary hypertension in CHD patients. These outcomes align with the findings of Yin et al. that showed a combined assessment of NTproBNP/BNP and doppler echocardiography enhances diagnostic value and aids in clinical decision-making (21, 22). The combination of Doppler echocardiography with NTproBNP provides enhanced diagnostic efficacy for pulmonary artery hypertension associated with CHD. This is particularly notable when Doppler echocardiography yields negative results in screening for pulmonary arterial hypertension in patients (23–26). Holmstrom et al. and Choi et al. have suggested that consecutive BNP measurements can offer clinically relevant insights, and may be useful in the assessment of shunt severity as well as approach to managing preterm infants diagnosed with a patent ductus arteriosus (27, 28). BNP determinations could aid in the identification of children with septal defects complicated by pulmonary hypertension (29).
However, there are some limitations in this study. First, neither Qp/Qs nor NT-proBNP could accurately predict the size of the ASD. This may be due to measurement errors as well as the association between larger ASD size and increased pulmonary pressure. Second, for clinical convenience, we did not adjust NT-proBNP levels based on age, which could introduce bias. Lastly, this study is a retrospective cohort study that have several limitations, including reliance on potentially incomplete or inaccurate data, difficulty in controlling for confounding factors, selection bias due to the non-random selection of participants, and challenges in establishing clear causality due to time errors. These limitations necessitate careful interpretation of the study's findings to ensure reliability and validity. Large multi-institutional studies will need to be conducted to conclusively determine the clinical value of NT-proBNP as a biomarker for shunt severity in pediatric patients with ASD. In conclusion, our study demonstrates a correlation between non-invasive NT-proBNP levels and invasive Qp/Qs measurements in children with ASD.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving humans were approved by the Committee on Human Studies (Institutional Review Board) at Taichung Veterans General Hospital (TCVGH-IRB no. CG16272B). The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participants' legal guardians/next of kin in accordance with the national legislation and institutional requirements.
LL: Conceptualization, Data curation, Formal Analysis, Writing – original draft, Writing – review & editing. YC: Data curation, Formal Analysis, Writing – original draft, Writing – review & editing. YF: Supervision, Writing – original draft, Writing – review & editing. HH: Methodology, Supervision, Writing – original draft, Writing – review & editing.
The author(s) declare that no financial support was received for the research and/or publication of this article.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declare that no Generative AI was used in the creation of this manuscript.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Wu MH, Chen HC, Lu CW, Wang JK, Huang SC, Huang SK. Prevalence of congenital heart disease at live birth in Taiwan. J Pediatr. (2010) 156:782–5. doi: 10.1016/j.jpeds.2009.11.062
2. van der Linde D, Konings EE, Slager MA, Witsenburg M, Helbing WA, Takkenberg JJ, et al. Birth prevalence of congenital heart disease worldwide: a systematic review and meta-analysis. J Am Coll Cardiol. (2011) 58:2241–7. doi: 10.1016/j.jacc.2011.08.025
3. Schwedler G, Lindinger A, Lange PE, Sax U, Olchvary J, Peters B, et al. Frequency and spectrum of congenital heart defects among live births in Germany: a study of the competence network for congenital heart defects. Clin Res Cardiol. (2011) 100:1111–7. doi: 10.1007/s00392-011-0355-7
4. Reller MD, Strickland MJ, Riehle-Colarusso T, Mahle WT, Correa A. Prevalence of congenital heart defects in metropolitan Atlanta, 1998–2005. J Pediatr. (2008) 153:807–13. doi: 10.1016/j.jpeds.2008.05.059
5. Alexander EA, Levinsky NG. An extrarenal mechanism of potassium adaptation. J Clin Invest. (1968) 47:740–8. doi: 10.1172/JCI105769
6. Guo G, Booms P, Halushka M, Dietz HC, Ney A, Stricker S, et al. Induction of macrophage chemotaxis by aortic extracts of the mgR Marfan mouse model and a GxxPG-containing fibrillin-1 fragment. Circulation. (2006) 114:1855–62. doi: 10.1161/CIRCULATIONAHA.105.601674
7. Eichhorn P, Ritter M, Suetsch G, von Segesser LK, Turina M, Jenni R. Congenital cleft of the anterior tricuspid leaflet with severe tricuspid regurgitation in adults. J Am Coll Cardiol. (1992) 20:1175–9. doi: 10.1016/0735-1097(92)90375-W
8. Saito T, Ohta K, Nakayama Y, Hashida Y, Maeda A, Maruhashi K, et al. Natural history of medium-sized atrial septal defect in pediatric cases. J Cardiol. (2012) 60:248–51. doi: 10.1016/j.jjcc.2012.05.005
9. Murphy JG, Gersh BJ, McGoon MD, Mair DD, Porter CB, Ilstrup DM, et al. Long-term outcome after surgical repair of isolated atrial septal defect. Follow-up at 27 to 32 years. N Engl J Med. (1990) 323:1645–50. doi: 10.1056/NEJM199012133232401
10. Wang TJ, Larson MG, Levy D, Benjamin EJ, Leip EP, Omland T, et al. Plasma natriuretic peptide levels and the risk of cardiovascular events and death. N Engl J Med. (2004) 350:655–63. doi: 10.1056/NEJMoa031994
11. Spinar J, Spinarova L, Malek F, Ludka O, Krejci J, Ostadal P, et al. Prognostic value of NT-proBNP added to clinical parameters to predict two-year prognosis of chronic heart failure patients with mid-range and reduced ejection fraction—a report from FAR NHL prospective registry. PLoS One. (2019) 14:e0214363. doi: 10.1371/journal.pone.0214363
12. Saunders JT, Nambi V, de Lemos JA, Chambless LE, Virani SS, Boerwinkle E, et al. Cardiac troponin T measured by a highly sensitive assay predicts coronary heart disease, heart failure, and mortality in the Atherosclerosis Risk in Communities Study. Circulation. (2011) 123:1367–76. doi: 10.1161/CIRCULATIONAHA.110.005264
13. de Lemos JA, McGuire DK, Drazner MH. B-type natriuretic peptide in cardiovascular disease. Lancet. (2003) 362:316–22. doi: 10.1016/S0140-6736(03)13976-1
14. Kitamura T, Ogorochi T, Miyajima A. Multimeric cytokine receptors. Trends Endocrinol Metab. (1994) 5:8–14. doi: 10.1016/1043-2760(94)90115-5
15. Jan SL, Fu YC, Hwang B, Lin SJ. B-type natriuretic peptide in children with atrial or ventricular septal defect: a cardiac catheterization study. Biomarkers. (2012) 17:166–71. doi: 10.3109/1354750X.2011.649494
16. Radman M, Mack R, Barnoya J, Castañeda A, Rosales M, Azakie A, et al. The effect of preoperative nutritional status on postoperative outcomes in children undergoing surgery for congenital heart defects in San Francisco (UCSF) and Guatemala City (UNICAR). J Thorac Cardiovasc Surg. (2014) 147:442–50. doi: 10.1016/j.jtcvs.2013.03.023
17. Lewis RA, Durrington C, Condliffe R, Kiely DG. BNP/NT-proBNP in pulmonary arterial hypertension: time for point-of-care testing? Eur Respir Rev. (2020) 29:200009. doi: 10.1183/16000617.0009-2020
18. Nagaya N, Nishikimi T, Uematsu M, Satoh T, Kyotani S, Sakamaki F, et al. Plasma brain natriuretic peptide as a prognostic indicator in patients with primary pulmonary hypertension. Circulation. (2000) 102:865–70. doi: 10.1161/01.CIR.102.8.865
19. Testani JM, St John Sutton MG, Wiegers SE, Khera AV, Shannon RP, Kirkpatrick JN. Accuracy of noninvasively determined pulmonary artery systolic pressure. Am J Cardiol. (2010) 105:1192–7. doi: 10.1016/j.amjcard.2009.11.048
20. Ozhan H, Albayrak S, Uzun H, Ordu S, Kaya A, Yazici M. Correlation of plasma B-type natriuretic peptide with shunt severity in patients with atrial or ventricular septal defect. Pediatr Cardiol. (2007) 28:272–5. doi: 10.1007/s00246-006-0014-3
21. Zhang X, Zhai Z, Geng X, Zhu Y, Yang S, Chen T, et al. Doppler echocardiography combined with NTproBNP/BNP in the diagnosis of pulmonary artery hypertension associated with congenital heart disease. Comput Math Methods Med. (2023) 2023:1896026. doi: 10.1155/2023/1896026
22. Yin D, Wang Y, Zheng M, Wei H, Li M, Lv T, et al. Comparison of pulmonary artery pressure measurement with Doppler echocardiography or with right heart catheterization in patients with congenital heart disease. Front Pediatr. (2019) 7:421. doi: 10.3389/fped.2019.00421
23. Mizuno Y, Yoshimura M, Harada E, Nakayama M, Sakamoto T, Shimasaki Y, et al. Plasma levels of A- and B-type natriuretic peptides in patients with hypertrophic cardiomyopathy or idiopathic dilated cardiomyopathy. Am J Cardiol. (2000) 86:1036–40; A11. doi: 10.1016/S0002-9149(00)01147-4
24. Cheng V, Kazanagra R, Garcia A, Lenert L, Krishnaswamy P, Gardetto N, et al. A rapid bedside test for B-type peptide predicts treatment outcomes in patients admitted for decompensated heart failure: a pilot study. J Am Coll Cardiol. (2001) 37:386–91. doi: 10.1016/S0735-1097(00)01157-8
25. Bolger AP, Sharma R, Li W, Leenarts M, Kalra PR, Kemp M, et al. Neurohormonal activation and the chronic heart failure syndrome in adults with congenital heart disease. Circulation. (2002) 106:92–9. doi: 10.1161/01.CIR.0000020009.30736.3F
26. Grabowski M, Filipiak KJ, Karpinski G, Wretowski D, Rdzanek A, Rudzki D, et al. Prognostic value of B-type natriuretic peptide levels on admission in patients with acute ST elevation myocardial infarction. Acta Cardiol. (2005) 60:537–42. doi: 10.2143/AC.60.5.2004976
27. Holmstrom H, Hall C, Thaulow E. Plasma levels of natriuretic peptides and hemodynamic assessment of patent ductus arteriosus in preterm infants. Acta Paediatr. (2001) 90:184–91. doi: 10.1111/j.1651-2227.2001.tb00282.x
28. Choi BM, Lee KH, Eun BL, Yoo KH, Hong YS, Son CS, et al. Utility of rapid B-type natriuretic peptide assay for diagnosis of symptomatic patent ductus arteriosus in preterm infants. Pediatrics. (2005) 115:e255–61. doi: 10.1542/peds.2004-1837
Keywords: atrial septal defect, N-terminal pro-B-type natriuretic peptide, pulmonary to systemic flow ratio, children, intervention
Citation: Liao L-C, Chen Y-Y, Fu Y-C and Hung H-C (2025) Correlation between pulmonary to systemic flow ratio and N-terminal Pro-B-type natriuretic peptide level in children with atrial septal defect. Front. Cardiovasc. Med. 12:1522603. doi: 10.3389/fcvm.2025.1522603
Received: 4 November 2024; Accepted: 27 February 2025;
Published: 14 March 2025.
Edited by:
Jaspal Dua, Liverpool Heart and Chest Hospital NHS Trust, United KingdomReviewed by:
Siddharth Dubey, Kings County Hospital Center, United StatesCopyright: © 2025 Liao, Chen, Fu and Hung. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yun-Ching Fu, eXVuY2hpbmdmdUBnbWFpbC5jb20=; Hui-Chih Hung, aGNodW5nQGRyYWdvbi5uY2h1LmVkdS50dw==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.