
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Cardiovasc. Med. , 14 March 2025
Sec. Hypertension
Volume 12 - 2025 | https://doi.org/10.3389/fcvm.2025.1477729
 Viktoria Gastens1
Viktoria Gastens1 Stefano Tancredi1
Stefano Tancredi1 Blanche Kiszio2Cinzia Del Giovane3Ross T. Tsuyuki4Gilles Paradis5
Blanche Kiszio2Cinzia Del Giovane3Ross T. Tsuyuki4Gilles Paradis5 Arnaud Chiolero1,4
Arnaud Chiolero1,4 Valérie Santschi2*
Valérie Santschi2*
Background: Community-based models of care with the involvement of pharmacists and other nonphysician healthcare professionals can help improve blood pressure (BP) control. We aimed to synthesize the evidence of effectiveness of pharmacist interventions on BP among patients with hypertension.
Methods: We performed systematic searches to identify randomized controlled trials (RCTs) assessing the effect of pharmacist interventions on BP among outpatients (latest search, March 2024). The effect on systolic and diastolic BP change or BP control were pooled using random effects model. Subgroup analysis for the types of pharmacist interventions and healthcare settings were performed. The risk of bias was assessed using the Cochrane Risk of Bias Tool 2. The protocol was registered in PROSPERO (CRD42021279751) and published in an open-access peer-reviewed journal.
Results: Out of 2,330 study records identified in 7 electronic databases, a total of 95 RCTs, with 31,168 participants (control 16,157, intervention 15,011), were included. The intervention was led by the pharmacist in 75% of the studies and in collaboration with other healthcare providers in 25%. Pharmacist interventions included patient education in 88%, feedback to healthcare providers in 49%, and patient reminders in 24% of the studies. Systolic and diastolic BP were reduced after pharmacist intervention by −5.3 mmHg (95% CI: −6.3 to −4.4; I2 = 86%) and −2.3 mmHg (95% CI: −2.9 to −1.8; I2 = 75%), respectively. The reduction of systolic BP tended to be larger if the intervention was collaborative, conducted in outpatient clinics, based on healthcare provider education, or through healthcare provider feedback. Analyses restricted to relatively large or high-quality studies yielded similar estimates, with lower between-studies heterogeneity.
Conclusion: Pharmacist care for patients with hypertension consistently improves BP across various settings and interventions. Pharmacist care is one key element of the solution to the global burden of hypertension and cardiovascular diseases.
PROSPERO registration number: CRD42021279751.
High blood pressure (BP) is the leading contributor to global mortality due to its impact on cardiovascular diseases (CVD), particularly coronary heart disease and stroke (1). A reduction of 5 mmHg in systolic BP can decrease the relative risk of major cardiovascular events by approximately 10% (2) and lowering BP levels is therefore crucial in preventing CVD and reducing their burden. However, many patients are not diagnosed and, if diagnosed, are poorly controlled and do not reach target BP levels; this might be due to limited access to healthcare or lifestyle counseling, clinical inertia, or non-adherence to medication (3).
To improve BP control, one strategy is to involve non-physician healthcare professionals such as pharmacists, nurses, or community health workers in the management of hypertension. The US Community Preventive Services Task Force, and more recently the American College of Cardiology, the American Heart Association, and the European Societies of Cardiology and Hypertension all recommend team-based care in hypertension management, with the involvement of pharmacists (4–7). Indeed, pharmacists have a pivotal role as highly accessible healthcare providers and experts in medication management. For instance, they can provide patient education, e.g., to improve health behaviours, and help patients adhere to medications. Community pharmacists are therefore a logical choice and a valuable asset to contribute to BP management.
Several meta-analyses of randomized trials have shown that pharmacist interventions, either pharmacist directed or in collaboration with other healthcare professionals, can help decrease BP (8, 9). However, the effects of the interventions on BP vary widely, from very large to modest or no effect, and the reasons for this heterogeneity are not entirely clear (8). Even when an effect is observed, the heterogeneity of the interventions can limit the implementation of guidelines and recommendations. Indeed, team-based care interventions are typically multi-component, and it can be challenging to assess the effect of each component. Additionally, the interventions can differ in terms of intensity, target population, settings or the number and type of professionals involved. It is therefore key to try to identify what works best, including duration or the intensity of intervention, patient characteristics or different patient care settings.
We therefore aimed to systematically review, synthesize, and update the evidence of the effect of pharmacist in delivering hypertension care services through directed care or in collaboration with other healthcare professionals on BP level among hypertensive patients. We also evaluated the heterogeneity in the effect of these interventions, specifically to determine which interventions are most effective in different healthcare contexts.
We followed the Cochrane Collaboration and Center for Reviews and Dissemination guidance methods for conducting and reporting systematic reviews and meta-analyses (10, 11) and report the results of this review according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses statement (PRISMA) (12). The protocol for this systematic review was registered on the International Prospective Register of Systematic Reviews (PROSPERO) database (CRD42021279751) and published in an open-access peer-reviewed journal (13).
Inclusion and exclusion study criteria were based on specific (1) study designs, (2) settings, (3) participants, (4) interventions, (5) comparators, and (6) outcomes. Randomized controlled trials (RCTs), cluster RCTs, and cross-over RCTs were eligible. Case reports, case series, non-randomized evaluations, reviews, meta-analyses, conference proceedings, policy papers, study protocols, and expert opinions were excluded. Studies based in a community/ambulatory care setting were included. Studies were considered if they included adult outpatients (18 years or over) with a diagnosis of hypertension, treated or not treated, and if they evaluated the effect of pharmacist interventions—directed or in collaborative care—in outpatients with hypertension compared to usual care. We distinguished between outpatient clinics (hospital or medical facility without overnight stay) and community care (e.g., at a community pharmacy or general practitioner). We included interventions that were delivered by a pharmacist directed or in collaborative care. Outcomes of interest were the mean difference in BP change, or BP control (BP below a predefined target level) at follow-up. We considered all publications in English, French, and German and searched all databases from inception to the date of search.
We searched the following electronic databases: MEDLINE (Ovid) (from 1946 on), Excerpta Medica database (Embase) (from 1947 on), Cochrane Central Register of Controlled Trials (CENTRAL) (from 1947 on), Cochrane Database of Systematic Reviews (CDSR) (from 1995 on), CINAHL (EBSCO) (from 1937 on), Web of Science (from 1900 on), JBI EBP Database (Ovid) (from 1998 on), and Tripdatabase (from 1997 on). The search for unpublished studies included the Grey Literature Report (New York Academy of Medicine, http://www.greylit.org). The search was conducted on 26.03.2024.
The specific search strategies (Supplementary Table S1) were developed by an experienced medical librarian in systematic review searching (BK) in consultation with the project team. They were constructed to include the two main concepts of this systematic review: “hypertension” and “pharmacist intervention”. A three-step search strategy was used in this review. First, an initial limited search of MEDLINE (Ovid) was undertaken using the search terms “Pharmacist intervention”, “Pharmacists”, “Pharmaceutical Services”, “Pharmacy Service, Hospital”, “Pharmacies”, “Pharmacy”, “Hypertension”, “Blood pressure”. Second, an analysis of the text words contained in each article's title, abstract, and index terms was undertaken to expand the list of search terms. Based on the results of this analysis, a more thorough search was conducted in the chosen databases. The search strategy for MEDLINE was created first and was then adapted for each database, including all identified keywords and index terms. Third, the reference lists of all included studies selected for critical appraisal were searched by hand and cited reference searches for all included studies were conducted in Web of Science to find any additional studies not identified during the initial search processes. The methodology search filter to limit retrieval to appropriate study designs, a modified version of the Cochrane Highly Sensitive Search Strategy, was used to identify randomized trials (10).
Study records retrieved by electronic searching were uploaded to the systematic review management software Covidence (14). After the removal of duplicates, titles, and abstracts were independently screened by two reviewers (VG and ST) for inclusion. The reviewers indicated whether a citation is potentially relevant (met inclusion criteria), is clearly not relevant (met exclusion criteria), or if the information is insufficient to make a judgment. We obtained full-text publications for all titles/abstracts that appear to meet inclusion criteria or where there is any uncertainty. Full-text publications were independently examined by two reviewers (VG and ST) to select studies for inclusion. Reasons for exclusion of ineligible studies were recorded. Any disagreement was resolved through discussion and, if required, by consulting a third review author (AC or VS). The selection process was recorded in detail in a Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram (12).
Data extraction was conducted using a prespecified data extraction template in the systematic review management software Covidence (14). Data was independently extracted by two reviewers (VG and ST) from each eligible study. Using a structured data collection form, these two reviewers independently extracted the data listed in Supplementary Table S2.
Primary outcome data to extract was the mean difference between intervention and control group in systolic and diastolic BP change from baseline to follow-up and the corresponding standard error (continuous outcome). If not reported in studies, the mean difference in BP change and standard error was calculated from reported information (BP change per study group, BP at baseline, BP at follow-up, and standard deviation, corresponding confidence intervals or p values of subgroup analyses). If no BP change or BP baseline information was available, the mean difference between intervention and control group at follow-up was used (15). For BP control (dichotomous, secondary outcome), we extracted the proportion of participants reaching a pre-defined BP target level. The target BP could differ from one study to the other.
We classified pharmacist interventions using the following pre-defined categories: (1) pharmacist-directed care (pharmacist initiating and managing care) and (2) pharmacist collaborative care (pharmacist collaborating in interventions conducted by a multidisciplinary healthcare team) (16). Based on the Cochrane Effective Practice and Organization of Care (EPOC) taxonomy interventions, we categorized pharmacist interventions by different target levels (patient, healthcare provider) and types (educational approach, e.g., targeted toward patients to improve their lifestyle; feedback, e.g., to healthcare providers to adapt medication; use of reminder tools, e.g., drug adherence aids) (17).
Two reviewers (VG and ST) independently assessed the risk of bias for each study using the “Cochrane Risk of Bias Tool” for randomized trials (RoB 2) (18). This tool assesses the risk of bias according to the following domains: 1. Randomization process; 2. Effect of assignment to intervention; 3. Missing outcome data; 4. Measurement of the outcome; 5. Selection of the reported result. The risk of bias assessment for cluster-randomized trials and randomized crossover trials was performed with the specific RoB 2 tools for these study designs (18).
We classified the risk of bias for each domain as either “Low risk”, “Some concerns” or “High risk” and provided information from each study together with the reasons for our evaluation (10, 18). Given the type of RCTs included in our review, blinding the participants and the research teams was usually not feasible; only the outcome assessment could be blinded. The quality of BP measurement was also systematically assessed along three criteria: (1) use of clinically validated BP measurement devices; (2) training of outcome assessor; (3) measurement of BP out of the office. In accordance with the revised Cochrane risk of bias tool for randomized trials, RoB2, we derived an overall study risk of bias as follows: “Low risk” with all domains at low risk of bias, “Some concerns” with at least one domain of some concern, “High risk” with high risk of bias in at least one domain or with some concerns for two or more domains (18). We resolved any disagreement in quality assessment through discussions and involvement of an arbitrator (AC or VS) where necessary.
For the continuous outcome, we used the mean difference in BP change between groups whenever available. When this measure was not reported, we used the mean difference in BP between groups at the end of follow-up (15). Calculations for the between-group standard error were based on calculations provided in the Cochrane Handbook (10). The pooled effect was calculated as weighted mean differences in BP between intervention and usual care groups, with 95% confidence intervals (CI). For the dichotomous outcome of BP control, we estimated the pooled relative risk (RR) comparing intervention vs. usual care groups, with 95% CI.
All analyses were conducted with R 4.2.2 (The R Foundation) using the meta software package (19). For the secondary outcome BP control, we calculated the relative risk as the ratio in the proportion of BP control (%) at follow-up in pharmacist intervention group vs. usual care group. A random effects model was used to estimate the pooled effects and results displayed in forest plots. Between-studies heterogeneity was quantified using the I2 statistic. To explore the possible sources of heterogeneity, we conducted subgroup analyses by categories of selected study characteristics: region, setting, type of pharmacist care, healthcare team composition, intervention characteristics. To assess the robustness of our results, we performed sensitivity analyses: among studies at high quality and with larger study size. Publication bias was assessed by visual inspection of funnel plots, and funnel plot asymmetry was examined using the Egger test (10, 20). The Grading of Recommendations Assessment, Development and Evaluation (GRADE) framework was applied to assess the strength of the body of evidence for this systematic review (21). Domains used to assess the certainty of the evidence included risk of bias, inconsistency, indirectness, imprecision, and publication bias. The certainty of evidence was assessed for systolic BP both by including all studies and by excluding studies with a high risk of bias.
A total of 2,330 study records were identified by electronic database searching (Supplementary Table S1) and loaded to the systematic review management software Covidence (14). After removal of duplicates, 2,218 studies were independently screened based on title and abstract by two authors, and 274 full texts were evaluated for eligibility (Figure 1). A total of 95 studies, all published in the English language, were included in our review (23–114), including 31,168 participants (control 16,157, intervention 15,011). The characteristics of each study are presented in Supplementary Table S3. Reasons for exclusion of studies (n = 179) were most commonly not appropriate study design (n = 67), not appropriate patient population (n = 62) and not appropriate intervention (n = 29) (115–117).
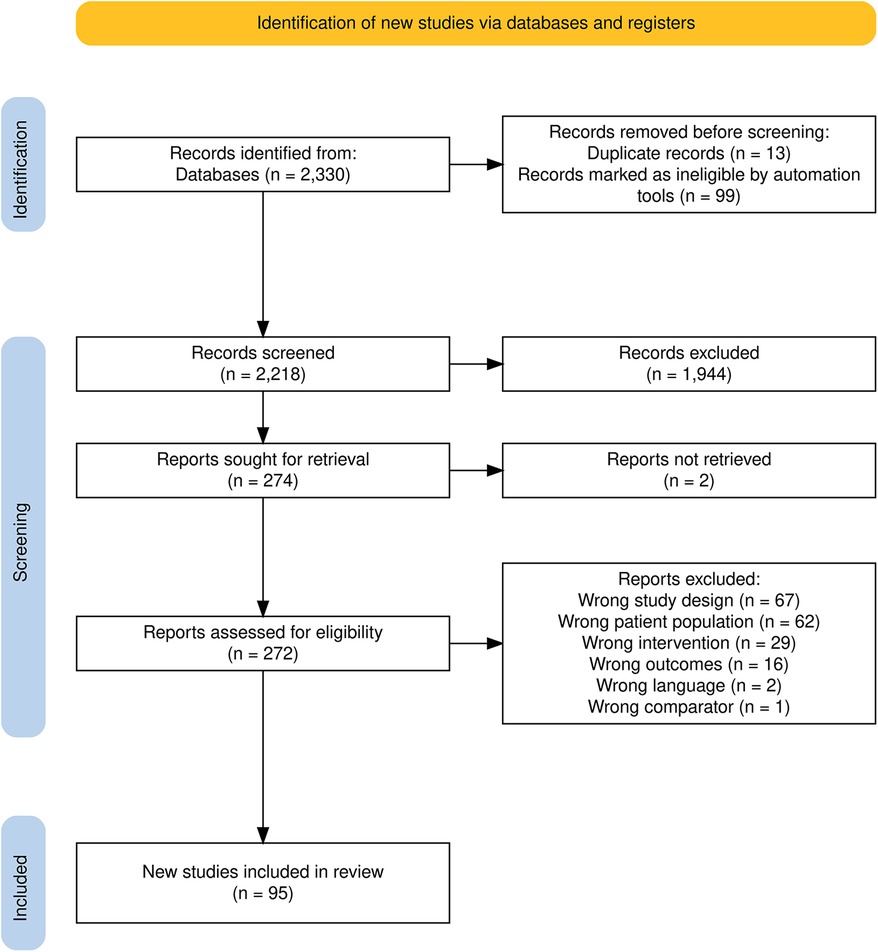
Figure 1. PRISMA 2020 flow diagram of studies identified, included, and excluded in the systematic review (22).
A summary of studies and patient characteristics is shown in Table 1. Included studies were published between 1973 and 2023 and conducted in different regions (North America: n = 47, Europe: n = 17, other: n = 31). The characteristics of the pharmacist interventions are summarized in Table 2. In 75% of the studies, the intervention was led by the pharmacist and in 25% in collaboration with other healthcare providers. In the 24 pharmacist collaborative care studies, the team composition was pharmacist/physician (N = 12); pharmacist/nurse/physician (N = 4); pharmacist/nurse/physician/diabetes educator (N = 2), or pharmacist/nurse (N = 6). Interventions targeted patients in 93% and healthcare providers in 61% of the studies. The types of intervention comprised patient education in 88%, healthcare provider education in 14%, feedback to healthcare providers (e.g., medication change) in 49%, and patient reminders (e.g., drug adherence aids) in 24% of the studies, respectively. Feedback to healthcare providers included medication change, either after independent pharmacist prescribing or recommendations to physicians. Further details of study and pharmacist intervention characteristics for each included study are displayed in Supplementary Table S3.
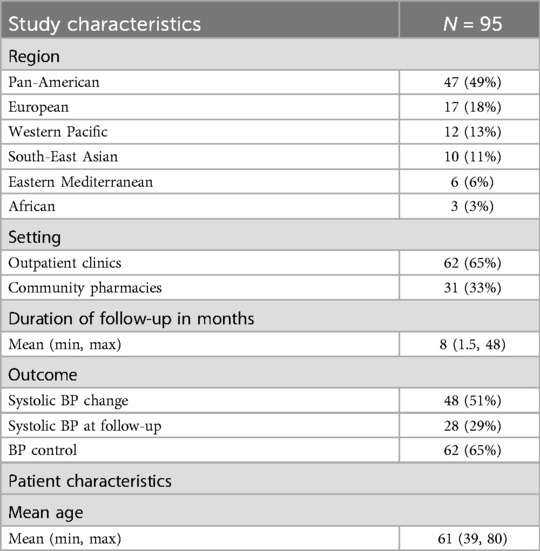
Table 1. Summary of study and patient characteristics of the included studies.
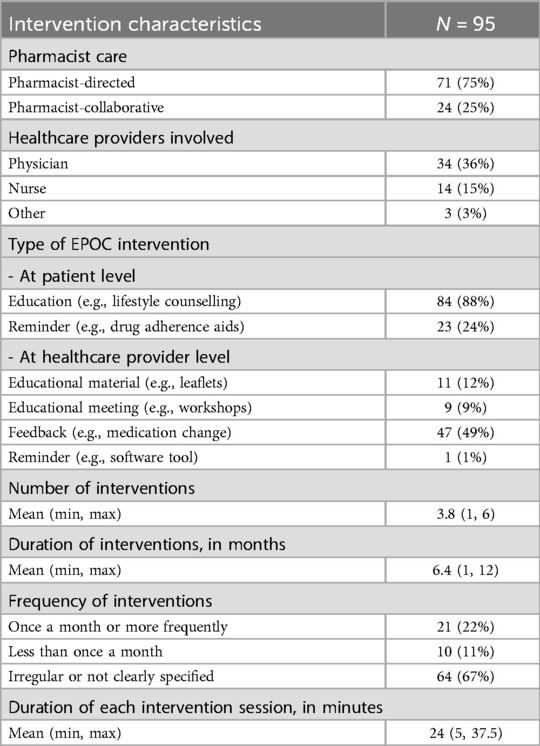
Table 2. Summary of pharmacist intervention characteristics of the included studies.
Results of the risk of bias assessment for each included study and the five domains (randomization process; deviations from intended interventions; missing outcome data; measurement of the outcome; selection of the reported result) are shown in Supplementary Figure S1. Overall, the quality of the studies was relatively low. Some 54 studies (57%) were at high risk of bias, 41 studies (43%) raised some concerns, and no study was assessed at low risk. The method of blood pressure measurement was assessed as appropriate or probably appropriate in 66 studies (69%), inappropriate or probably inappropriate in 5 studies (5%), and missing information in 24 studies (25%).
The forest plots of the mean change in systolic and diastolic BP change are displayed in Figure 2 (76 studies, N = 27,057) and Figure 3 (71 studies, N = 22,652). The pooled results showed that pharmacist care services alone or in collaboration with other healthcare professionals reduced systolic/diastolic BP by −5.3 (95% CI: −6.3 to 4.4)/−2.3 (95% CI: −2.9 to −1.8) mmHg. There was a large between-study heterogeneity, with an I2 of 86% for systolic BP and of 75% for diastolic BP.

Figure 2. Forest plot of the mean difference in systolic blood pressure change between pharmacist and usual care group sorted by year of publication.
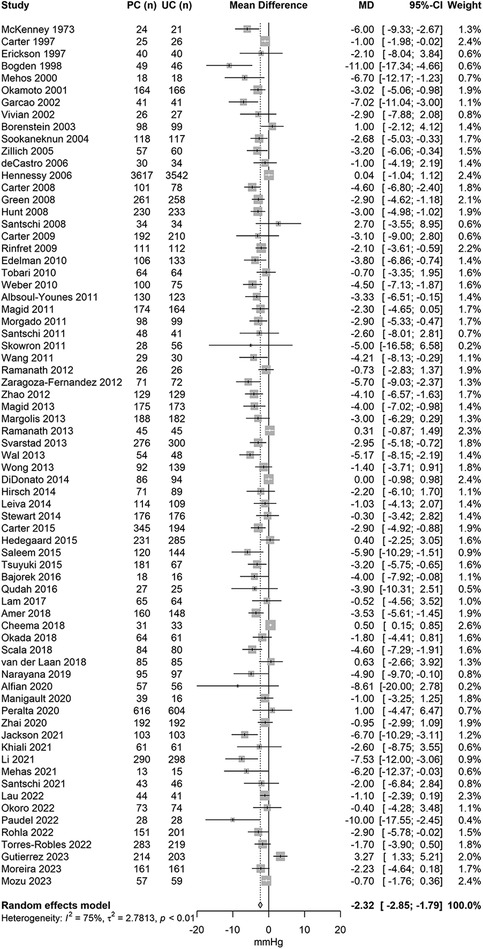
Figure 3. Forest plot of the mean difference in diastolic blood pressure change between pharmacist and usual care by year of publication.
Results of subgroup analyses are displayed in Table 3. Overall, there were no major differences in the effect on BP according to study characteristics or types of intervention. No difference in BP reduction was observed by region of study and pharmacist directed/collaborative care. The effects on systolic BP tended to be slightly larger if the intervention was in an outpatient clinic [−6.0 mmHg (95% CI: −7.2 to −4.8)], collaborative [−6.2 mmHg (95% CI: −7.6 to −4.9)], based on healthcare provider education [−6.1 mmHg (95% CI: −9.2 to −3.0)], or through healthcare provider feedback [−6.1 mmHg (95% CI: −7.2 to −4.9)].
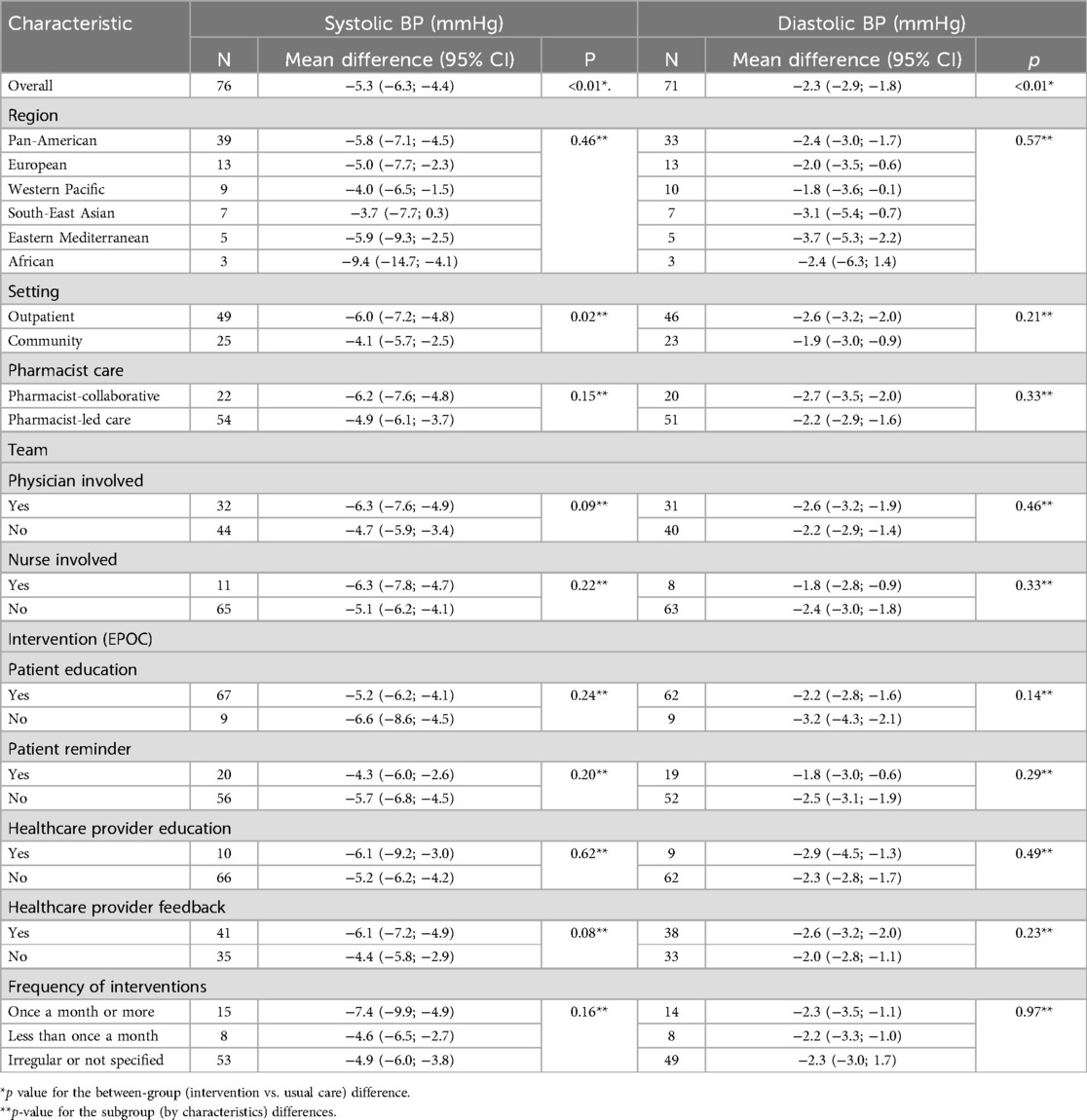
Table 3. Subgroup analyses for the difference in systolic and diastolic blood pressure (BP) with pharmacist care compared with usual care group according to study characteristics.
Sensitivity analysis restricted to studies at relatively low risk of bias yielded similar results (mean difference of −4.8 mmHg (95% CI: −5.9 to −3.7 mmHg; I2 = 87%) for systolic BP (N = 39, including 21,339 participants) and −2.3 mmHg (95% CI: −3.0 to −1.6 mmHg; I2 = 63%) for diastolic BP (N = 35, including 16,780 participants), respectively), but the between-study heterogeneity was much smaller. The forest plots of the mean change in systolic and diastolic BP restricted to studies with a relatively low risk of bias are displayed in Supplementary Figures S2, S3. Sensitivity analysis excluding studies of small size (less than 50 total participants) resulted in a mean difference between pharmacist intervention and usual care of −5.1 mmHg (95% CI: −6.1 to −4.2 mmHg; I2 = 87%) for systolic BP (N = 70, 26,837 participants) and −2.2 mmHg (95% CI: −2.7 to −1.7 mmHg; I2 = 74%) for diastolic BP (N = 65, 21,766 participants). These differences were of the same magnitude compared with the differences observed when all studies were included.
The secondary outcome BP control at follow-up was reported in 62 studies (N = 22,657). At baseline, the median proportion of participants with controlled BP was 0% (25th to 75th percentile: 0.0%–37.4%) in the usual care group and 0% (25th to 75th percentile: 0.0%–35.4%) in the pharmacist care group. At follow-up, the median proportion of participants with controlled BP was 40.8% (25th to 75th percentile: 29.9%–57.0%) in the usual care group and 61.2% (25th to 75th percentile: 46.1%–69.6%) in the pharmacist care group. The mean difference in the change from baseline to follow-up in the proportion of participants with controlled BP was +17.3% (95% CI: + 13.3% to +21.2%) between pharmacist care and usual care group. The pooled results showed a relative risk for BP control after pharmacist intervention of 1.37 (95% CI: 1.27 to 1.47; I2 = 80%; Supplementary Figure S4).
Potential publication bias was observed for both systolic and diastolic BP as suggested by the asymmetry of the funnel plots (Supplementary Figure S5), with Egger test p-value of 0.03 for systolic BP and <0.01 for diastolic BP. When limited to relatively high-quality studies, the funnel plot asymmetry disappeared (Supplementary Figure S6), with Egger test p-values of 0.65 for systolic BP and 0.07 for diastolic BP. The GRADE framework was applied to assess the strength of the body of evidence for this systematic review (Supplementary Table S4) (21). The certainty of evidence for systolic BP was assessed as low when including all studies (the certainty was downgraded due to study limitations and publication bias) and moderate when excluding studies with a high risk of bias (downgrading for study limitation). This means that the true effect is likely to be close to effect estimate, but the possibility that it is substantially different exists.
Our systematic review and meta-analysis of almost 100 studies confirmed a clinically and statistically significant reduction in BP with pharmacist care services. The BP difference as a result of pharmacists' interventions, was a 5.3 mmHg (95% CI: −6.3 to −4.4; I2 = 86%) reduction in systolic BP and a 2.3 mmHg (95% CI: −2.9 to −1.8; I2 = 75%) reduction in diastolic BP. There was also a large effect on BP control. Similar estimates were found when excluding studies at high risk of bias. Our results showed that different types of pharmacists' interventions reduce BP, improve BP control, and support the involvement of pharmacists in BP management. We found that the effects on systolic BP tended to be larger if the intervention was collaborative, based on healthcare provider education, or through healthcare provider feedback. Moreover, we observed a greater improvement in systolic BP in outpatient clinics compared to community pharmacies.
The BP reduction estimates found in this systematic review are comparable to estimates found in previous systematic reviews (8, 118). In a systematic review conducted in 2014 by our team, including 39 RCTs for systolic BP and 36 for diastolic BP, we found a BP reduction of −7.6 mm Hg (95% CI: −9.0 to −6.3 mm Hg) and −3.9 mm Hg (95% CI: −5.1 to −2.8 mm Hg) for SBP and DBP respectively (8). Similar estimates were reported in other studies; Chisholm-Burns et al. found a mean difference between the pharmacist group and the comparison group of −7.8 mm Hg (95% CI: −9.7 to −5.8) in systolic BP, and −2.9 mm Hg (95% CI: −3.8 to −2.0) in diastolic BP (118). Other systematic reviews only assessed specific setting or interventions. For instance, Baral et al. found that the addition of pharmacist-led home BP telemonitoring to usual care leads to a significant decrease in systolic BP (−8.1 mm Hg; 95% CI: −11.2 to −5.0 mm Hg) and diastolic BP (−4.2 mm Hg; 95% CI: −5.6 to −2.8 mm Hg) compared to usual care (119). Our systematic review provides the highest level of evidence to develop public policies to implement pharmacist care in hypertension. This transition from evidence to real-life policies should be supported by implementation studies (120).
The most common interventions, whether directed by the pharmacist or in collaboration with other healthcare professionals, included educating patients (about medications, lifestyle, or compliance), providing feedback to physicians (identifying medication-related problems and suggesting adjustments), and using reminders for medication management. Physician and nurse collaboration were the most common choice for healthcare teams in collaborative interventions. However, analyses aimed at comparing the effectiveness of specific intervention or type of care did not yield significant differences across intervention types. This might be attributed to the fact that multiple types of interventions effectively contribute to reduce BP, or to the challenge of disentangling the multifaceted and heterogeneous nature of these interventions, usually consisting of several components. One possible approach to gain a deeper understanding of the role of each specific intervention type could be to assess the comparative effectiveness of interventions using network meta-analysis (121). As for the effectiveness of pharmacist interventions in different settings, we observed a slightly greater reduction in BP for interventions conducted in outpatient clinics compared to those in community pharmacies. This could be due to several factors. One hypothesis is that patients in outpatient clinics may be more committed to improving their health status, or the consistent contact with healthcare professionals in outpatient clinics could lead to better adherence to recommendations, including medication and lifestyle changes. Furthermore, patients in outpatient clinics could benefit from more extended and focused consultations with pharmacists and other healthcare providers. This additional time allows for more in-depth education and counselling (122). Outpatient clinics are usually connected to larger facilities such as teaching hospitals or university hospitals with more resources than community pharmacies and usually have fixed patient appointments instead of walk-in services.
When interpreting the results of this study, several limitations should be considered. Firstly, trials for pharmacists' intervention face practical challenges in blinding both participants and researchers, increasing risk of bias. Hence, we found no study at low risk of bias, and many included studies were considered at high risk. This limitation also affected the GRADE assessment of the certainty of the evidence, resulting in a low-certainty rating. However, a recent review concluded that it is rare to fulfil the criteria for high-quality evidence with GRADE (123). Low-quality trials are unfortunately a major and pervasive issue in biomedical and clinical research (124). Furthermore, our analyses indicated potential publication bias, i.e., a preference for publishing studies with favourable results of pharmacist interventions over those reporting negative outcomes. This bias disappeared when assessing studies at moderate risk of bias only, or when evaluating diastolic BP. Moreover, we observed high heterogeneity in the included studies. This high heterogeneity may be explained by the large variation in interventions and settings. Due to this complexity and multiple elements of both interventions and usual care, a sharp contrast between the different types of interventions was difficult to show. Despite the very large number of studies, identifying which elements of pharmacists' interventions were the most effective remained difficult and disputable. The assessment of complex healthcare interventions (125, 126), is a standard problem which can limit the ability to make strong statements on what works best. Additional limitations include the absence of specific information regarding usual care in numerous studies and the relatively low number of studies with a long follow up, which makes it difficult to understand the long-term impact of pharmacists' interventions on blood pressure management. We also lack studies evaluating the effect of pharmacist interventions on the occurrence of blood pressure related cardiovascular diseases or mortality. Lastly, there is a need for a cost-effectiveness analysis of these interventions, which would assist in identifying the most preferable intervention for implementation (127). This study's strengths lie in its comprehensive and systematic approach and the substantial number of studies included, conducted across several world regions. Moreover, it adheres to established guidelines, such as the Cochrane guidelines for Systematic Reviews and the PRISMA statement (10, 12).
In conclusion, our systematic review of almost 100 RCTs provides the highest level of evidence for the impact of pharmacist care in hypertension. This evidence should inform changes to the delivery of care in hypertension and would help to address the approximately 50% of patients with uncontrolled hypertension. New policies and research should focus on the implementation of these interventions in real-life settings with rigorously conducted evaluation and monitoring studies including e.g., patient-reported outcomes and cost-effectiveness analyses (128).
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
Ethical review and approval was not required for this study in accordance with the local legislation and institutional requirements. Written informed consent to participate in this study was not required from the participants or the participants' legal guardians/next of kin in accordance with the national legislation and the institutional requirements.
VG: Data curation, Formal Analysis, Investigation, Software, Writing – original draft, Writing – review & editing. ST: Data curation, Formal Analysis, Writing – original draft, Writing – review & editing. BK: Data curation, Writing – original draft, Writing – review & editing. CD: Methodology, Writing – original draft, Writing – review & editing. RT: Writing – original draft, Writing – review & editing. GP: Writing – original draft, Writing – review & editing. AC: Methodology, Supervision, Writing – original draft, Writing – review & editing. VS: Conceptualization, Supervision, Writing – original draft, Writing – review & editing.
The author(s) declare that no financial support was received for the research and/or publication of this article.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fcvm.2025.1477729/full#supplementary-material
1. Poulter NR, Prabhakaran D, Caulfield M. Hypertension. Lancet. (2015) 386:801–12. doi: 10.1016/S0140-6736(14)61468-9
2. Rahimi K, Bidel Z, Nazarzadeh M, Copland E, Canoy D, Ramakrishnan R, et al. Pharmacological blood pressure lowering for primary and secondary prevention of cardiovascular disease across different levels of blood pressure: an individual participant-level data meta-analysis. Lancet. (2021) 397:1625–36. doi: 10.1016/S0140-6736(21)00590-0
3. Olsen MH, Angell SY, Asma S, Boutouyrie P, Burger D, Chirinos JA, et al. A call to action and a lifecourse strategy to address the global burden of raised blood pressure on current and future generations: the lancet commission on hypertension. Lancet. (2016) 388:2665–712. doi: 10.1016/S0140-6736(16)31134-5
4. CPSTF. “Guide to Community Preventive Services. Cardiovascular Disease: Team-Based Care to Improve Blood Pressure Control.,” (2020).
5. Anker D, Tsuyuki RT, Paradis G, Chiolero A, Santschi V. Pharmacists to improve hypertension management: guideline concordance from North America to Europe. Can Pharm J. (2019) 152:180–5. doi: 10.1177/1715163519839675
6. Whelton PK, Carey RM, Aronow WS, Casey DE, Collins KJ, Himmelfarb CD, et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA guideline for the prevention, detection, evaluation, and management of high blood pressure in adults: executive summary: a report of the American College of Cardiology/American Heart Association task force on clinical practice guidelines,” Circulation. (2018) 138:e426–83. doi: 10.1161/CIR.0000000000000597
7. Williams B, Mancia G, Spiering W, Agabiti Rosei E, Azizi M, Burnier M, et al. 2018 ESC/ESH guidelines for the management of arterial hypertension the task force for the management of arterial hypertension of the European society of cardiology and the European society of hypertension. J Hypertens. (2018) 36:1953–2041. doi: 10.1097/HJH.0000000000001940
8. Santschi V, Chiolero A, Colosimo AL, Platt RW, Taffé P, Burnier M, et al. Improving blood pressure control through pharmacist interventions: a meta-analysis of randomized controlled trials. J Am Heart Assoc. (2014) 3:e000718. doi: 10.1161/JAHA.113.000718
9. Santschi V, Chiolero A, Burnand B, Colosimo AL, Paradis G. Impact of pharmacist care in the management of cardiovascular disease risk factors: a systematic review and meta-analysis of randomized trials. Arch Intern Med. (2011) 171:1441–53. doi: 10.1001/archinternmed.2011.399
10. Higgins JPT, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, editors. Cochrane Handbook for Systematic Reviews of Interventions version 6.5 (Updated August 2024). Cochrane (2024). Available online at: www.training.cochrane.org/handbook (Accessed March 05, 2025).
12. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Br Med J. (2021) 372:n71. doi: 10.1136/bmj.n71
13. Gastens V, Kiszio B, Del Giovane C, Tsuyuki R, Paradis G, Chiolero A, et al. Pharmacist interventions to improve hypertension management: protocol for a systematic review of randomised controlled trials. BMJ Open. (2022) 12:e059399. doi: 10.1136/bmjopen-2021-059399
14. Veritas Health Innovation. Covidence systematic review software. Melbourne: Veritas Health Innovation. Available online at: www.covidence.org (Accessed March 05, 2025).
15. da Costa BR, Nüesch E, Rutjes AW, Johnston BC, Reichenbach S, Trelle S, et al. Combining follow-up and change data is valid in meta-analyses of continuous outcomes: a meta-epidemiological study. J Clin Epidemiol. (2013) 66:847–55. doi: 10.1016/j.jclinepi.2013.03.009
16. Koshman SL, Charrois TL, Simpson SH, McAlister FA, Tsuyuki RT. Pharmacist care of patients with heart failure: a systematic review of randomized trials. Arch Intern Med. (2008) 168:687–94. doi: 10.1001/archinte.168.7.687
17. EPOC, Cochrane Effective Practice and Organisation of Care Review Group. Data Collection Checklist, Cochrane Effective Practice and Organisation of Care. Ottawa, ON: Cochrane Effective Practice and Organisation of Care Group (EPOC), Institute of Population Health, University of Ottawa (2002).
18. Sterne JAC, Savović J, Page MJ, Elbers RG, Blencowe NS, Boutron I, et al. Rob 2: a revised tool for assessing risk of bias in randomised trials. Br Med J. (2019) 366:l4898. doi: 10.1136/bmj.l4898
19. Balduzzi S, Rücker G, Schwarzer G. How to perform a meta-analysis with R: a practical tutorial. Evid Based Ment Health. (2019) 22:153–60. doi: 10.1136/ebmental-2019-300117
20. Egger M, Smith GD, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. Br Med J. (1997) 315:629–34. doi: 10.1136/bmj.315.7109.629
21. Holger Schünemann H, Brożek J, Guyatt G, Oxman A. Handbook for grading the quality of evidence and the strength of recommendations using the GRADE approach. (2013). Available online at: https://gdt.gradepro.org/app/handbook/handbook.html (Accessed March 05, 2025).
22. Haddaway NR, Page MJ, Pritchard CC, McGuinness LA. PRISMA2020: an R package and shiny app for producing PRISMA 2020-compliant flow diagrams, with interactivity for optimised digital transparency and open synthesis. Campbell Syst Rev. (2022) 18:e1230. doi: 10.1002/cl2.1230
23. Albsoul-Younes AM, Hammad EA, Yasein NA, Tahaineh LM. Pharmacist-physician collaboration improves blood pressure control. Saudi Med J. (2011) 32:288–92.21384066
24. Alfian SD, van Boven JFM, Abdulah R, Sukandar H, Denig P, Hak E. Effectiveness of a targeted and tailored pharmacist-led intervention to improve adherence to antihypertensive drugs among patients with type 2 diabetes in Indonesia: a cluster randomised controlled trial. Br J Clin Pharmacol. (2021) 87:2032–42. doi: 10.1111/bcp.14610
25. Amer M, Rahman NU, Nazir R, Ur S, Raza A, Riaz H, et al. Impact of pharmacist’s intervention on disease related knowledge, medication adherence, HRQoL and control of blood pressure among hypertensive patients. Pak J Pharm Sci. (2018) 31(6):2607–16.30587468
26. Ashok KM, Elayaraja J, Shailaja K, Ramasamy C. Improving medication adherence and clinical outcomes of hypertensive patients through patient counseling. Res J Pharm Biol Chem Sci. (2011) 2:231–41.
27. Bajorek B, Lemay KS, Magin P, Roberts C, Krass I, Armour CL. Implementation and evaluation of a pharmacist-led hypertension management service in primary care: outcomes and methodological challenges. Pharm Pract. (2016) 14:723. doi: 10.18549/PharmPract.2016.02.723
28. Blenkinsopp A, Phelan M, Bourne J, Dakhil N. Extended adherence support by community pharmacists for patients with hypertension: a randomised controlled trial. Int J Pharm Pract. (2000) 8:165–75. doi: 10.1111/j.2042-7174.2000.tb01002.x
29. Bogden PE, Abbott RD, Williamson P, Onopa JK, Koontz LM. Comparing standard care with a physician and pharmacist team approach for uncontrolled hypertension. J Gen Intern Med. (1998) 13:740–5. doi: 10.1046/j.1525-1497.1998.00225.x
30. Borenstein JE, Graber G, Saltiel E, Wallace J, Ryu S, Jackson A, et al. Physician-pharmacist comanagement of hypertension: a randomized, comparative trial. Pharmacotherapy. (2003) 23:209–16. doi: 10.1592/phco.23.2.209.32096
31. Carter BL, Barnette DJ, Chrischilles E, Mazzotti GJ, Asali ZJ. Evaluation of hypertensive patients after care provided by community pharmacists in a rural setting. Pharmacotherapy. (1997) 17:1274–85. doi: 10.1002/j.1875-9114.1997.tb03092.x
32. Carter BL, Bergus GR, Dawson JD, Farris KB, Doucette WR, Chrischilles EA, et al. A cluster randomized trial to evaluate physician/pharmacist collaboration to improve blood pressure control. J Clin Hypertens. (2008) 10:260–71. doi: 10.1111/j.1751-7176.2008.07434.x
33. Carter BL, Ardery G, Dawson JD, James PA, Bergus GR, Doucette WR, et al. Physician and pharmacist collaboration to improve blood pressure control. Arch Intern Med. (2009) 169:1996–2002. doi: 10.1001/archinternmed.2009.358
34. Carter BL, Coffey CS, Ardery G, Uribe L, Ecklund D, James P, et al. Cluster-randomized trial of a physician/pharmacist collaborative model to improve blood pressure control. Circulation. (2015) 8:235–43. doi: 10.1161/CIRCOUTCOMES.114.001283
35. Cheema E, Sutcliffe P, Weickert MO, Singer DRJ. A randomised controlled trial of the impact of structured written and verbal advice by community pharmacists on improving hypertension education and control in patients with high blood pressure. Eur J Clin Pharmacol. (2018) 74:1391–5. doi: 10.1007/s00228-018-2519-0
36. Contreras-Vergara A, Sifuentes-Franco S, Haack S, Graciano-Machuca O, Rodriguez-Carrizalez AD, López-Contreras AK, et al. Impact of pharmaceutical education on medication adherence and its clinical efficacy in patients with type 2 diabetes and systemic arterial hypertension. Patient Prefer Adherence. (2022) 16:1999–2007. doi: 10.2147/PPA.S370323
37. De Castro MS, Fuchs FD, Costa Santos M, Maximiliano P, Gus M, Beltrami Moreira L, et al. Pharmaceutical care program for patients with uncontrolled hypertension: report of a double-blind clinical trial with ambulatory blood pressure monitoring. Am J Hypertens. (2006) 19:528–33. doi: 10.1016/j.amjhyper.2005.11.009
38. DiDonato KL, Vetter KR, Liu Y, May JR, Hartwig DM. Examining the effect of a medication synchronization or an education program on health outcomes of hypertensive patients in a community pharmacy setting. Innov Pharm. (2014) 5(175):1–9. doi: 10.24926/iip.v5i3.357
39. Earp JA, Ory MG, Strogatz DS. The effects of family involvement and practitioner home visits on the control of hypertension. Am J Public Health. (1982) 72:1146–54. doi: 10.2105/AJPH.72.10.1146
40. Edelman D, Fredrickson SK, Melnyk SD, Coffman CJ, Jeffreys AS, Datta S, et al. Medical clinics versus usual care for patients with both diabetes and hypertension: a randomized trial. Ann Intern Med. (2010) 152:689–96. doi: 10.7326/0003-4819-152-11-201006010-00001
41. Erickson SR, Slaughter R, Halapy H. Pharmacists’ ability to influence outcomes of hypertension therapy. Pharmacotherapy. (1997) 17:140–7. doi: 10.1002/j.1875-9114.1997.tb03687.x
42. Firmino PYM, Vasconcelos TO, Ferreira CC, Moreira LM, Romero NR, Dias LA, et al. Cardiovascular risk rate in hypertensive patients attended in primary health care units: the influence of pharmaceutical care. Braz J Pharm Sci. (2015) 51:617–27. doi: 10.1590/S1984-82502015000300013
43. Garçao J. A. and Cabrita J., “Evaluation of a pharmaceutical care program for hypertensive patients in rural Portugal,” J Am Pharm Assoc, vol. 42, p. 858–64, 2002. doi: 10.1331/108658002762063691
44. Green BB, Cook AJ, Ralston JD, Fishman PA, Catz SL, Carlson J, et al. Effectiveness of home blood pressure monitoring, web communication, and pharmacist care on hypertension control: a randomized controlled trial. Jama. (2008) 299:2857–67. doi: 10.1001/jama.299.24.2857
45. Gupta A, Ellis SD, Burkhardt C, Young K, Mazzotti DR, Mahnken J, et al. Implementing a home-based virtual hypertension programme—a pilot feasibility study. Fam Pract. (2023) 40:414–22. doi: 10.1093/fampra/cmac084
46. Hedegaard U, Kjeldsen LJ, Pottegård A, Henriksen JE, Lambrechtsen J, Hangaard J, et al. Improving medication adherence in patients with hypertension: a randomized trial. Am J Med. (2015) 128:1351–61. doi: 10.1016/j.amjmed.2015.08.011
47. Heisler M, Hofer TP, Schmittdiel JA, Selby JV, Klamerus ML, Bosworth HB, et al. Improving blood pressure control through a clinical pharmacist outreach program in patients with diabetes mellitus in 2 high-performing health systems: the adherence and intensification of medications cluster randomized, controlled pragmatic trial. Circulation. (2012) 125:2863–72. doi: 10.1161/CIRCULATIONAHA.111.089169
48. Hennessy S, Leonard CE, Yang W, Kimmel SE, Townsend RR, Wasserstein AG, et al. Effectiveness of a two-part educational intervention to improve hypertension control: a cluster-randomized trial. Pharmacotherapy. (2006) 26:1342–7. doi: 10.1592/phco.26.9.1342
49. Hirsch JD, Steers N, Adler DS, Kuo GM, Morello CM, Lang M, et al. Primary care–based, pharmacist–physician collaborative medication-therapy management of hypertension: a randomized, pragmatic trial. Clin Ther. (2014) 36:1244–54. doi: 10.1016/j.clinthera.2014.06.030
50. Hunt JS, Siemienczuk J, Pape G, Rozenfeld Y, MacKay J, LeBlanc BH, et al. A randomized controlled trial of team-based care: impact of physician-pharmacist collaboration on uncontrolled hypertension. J Gen Intern Med. (2008) 23:1966–72. doi: 10.1007/s11606-008-0791-x
51. Jackson IL, Ukwe CV. Clinical outcomes of pharmaceutical care intervention in HIV positive patients with hypertension: a randomized controlled study. J Clin Pharm Ther. (2021) 46:1083–94. doi: 10.1111/jcpt.13400
52. Jamieson LH, Scally A, Chrystyn H. A randomised comparison of practice pharmacist-managed hypertension providing level 3 medication review versus usual care in general practice. J Appl Ther Res. (2010) 7:77–86.
53. Kandasamy KR, Natarajan AG, Sebastian JO, Konakalla MA, Sam RO, Rajagopal SS, et al. Impact of pharmacist intervention in screening and education on blood pressure in a rural area in southern India. Asian J Pharm Clin Res. (2016) 9:339–43. doi: 10.22159/ajpcr.2016.v9s3.14782
54. Khiali S, Khezerlo-Aghdam N, Namdar H, Entezari-Maleki T. Pharmacist-directed self-management of blood pressure versus conventional management in patients with hypertension: a randomized control trial. High Blood Press Cardiovasc Prev. (2021) 28:283–90. doi: 10.1007/s40292-021-00445-x
55. Lam AY, Nguyen JK, Parks JJ, Morisky DE, Berry DL, Wolpin SE. Addressing low health literacy with “talking pill bottles”: a pilot study in a community pharmacy setting. J Am Pharm Assoc (2003). (2017) 57:20–9. doi: 10.1016/j.japh.2016.07.003
56. Lau D, Ringrose J, McAlister FA, Fradette M, Wood PW, Boulanger P, et al. Telemonitoring and protocolized case management for hypertensive community dwelling older adults (TECHNOMED): a randomized controlled trial. J Hypertens. (2022) 40:1702–12. doi: 10.1097/HJH.0000000000003202
57. Leiva A, Aguilo A, Fajo-Pascual M, Moreno L, Martı´n MC, Garcia EM, et al. Efficacy of a brief multifactorial adherence-based intervention in reducing blood pressure: a randomized clinical trial. Patient Prefer Adherence. (2014) 8:1683–90. doi: 10.2147/PPA.S66927
58. Li Y, Liu G, Liu C, Wang X, Chu Y, Li X, et al. Effects of pharmacist intervention on community control of hypertension: a randomized controlled trial in zunyi, China. Glob Health Sci Pract. (2021) 9:890–904. doi: 10.9745/GHSP-D-20-00505
59. Liu Q, Zhu X, Shen M, Wu J, Chen S, Wang Z, et al. Community pharmacist services for hypertensive patients: a novel practice in Shanghai, China. INQUIRY. (2021) 58:00469580211020874. doi: 10.1177/00469580211020874
60. Magid DJ, Ho PM, Olson KL, Brand DW, Welch LK, Snow KE, et al. A multimodal blood pressure control intervention in 3 healthcare systems. Am J Manag Care. (2011) 17:e96–103.21774100
61. Magid DJ, Olson KL, Billups SJ, Wagner NM, Lyons EE, Kroner BA. A pharmacist-led, American heart association Heart360 web-enabled home blood pressure monitoring program. Circulation. (2013) 6:157–63. doi: 10.1161/CIRCOUTCOMES.112.968172
62. Malik M, Hussain A, Aslam U, Hashmi A, Vaismoradi M, Hayat K, et al. Effectiveness of community pharmacy diabetes and hypertension care program: an unexplored opportunity for community pharmacists in Pakistan. Front Pharmacol. (2022) 13:710617. doi: 10.3389/fphar.2022.710617
63. Manigault KR, McKinley D, Patel S, Truong C, Nguyen S, Akil A, et al. The impact of a pharmacist-designed mobile application on blood pressure control and medication adherence in patients with hypertension. J Am Coll Clin Pharm. (2020) 3:1286–95. doi: 10.1002/jac5.1296
64. Margolis KL, Asche SE, Bergdall AR, Dehmer SP, Groen SE, Kadrmas HM, et al. Effect of home blood pressure telemonitoring and pharmacist management on blood pressure control: a cluster randomized clinical trial. Jama. (2013) 310:46–56. doi: 10.1001/jama.2013.6549
65. McKenney JM, Brown ED, Necsary R, Reavis HL. Effect of pharmacist drug monitoring and patient education on hypertensive patients. Contemp Pharm Pract. (1978) 1:50–6.
66. McKenney JM, Slining JM, Henderson HR, Devins D, Barr M. The effect of clinical pharmacy services on patients with essential hypertension. Circulation. (1973) 48:1104–11. doi: 10.1161/01.CIR.48.5.1104
67. McLean DL, McAlister FA, Johnson JA, King KM, Makowsky MJ, Jones CA, et al. A randomized trial of the effect of community pharmacist and nurse care on improving blood pressure management in patients with diabetes mellitus: study of cardiovascular risk intervention by pharmacists–hypertension (SCRIP-HTN). Arch Intern Med. (2008) 168:2355–61. doi: 10.1001/archinte.168.21.2355
68. Mehas N, Hudmon KS, Jaynes H, Klink S, Downey L, Zillich AJ. Impact of electronic medication reminder caps on patient adherence and blood pressure. J Pharm Technol. (2021) 37:234–43. doi: 10.1177/87551225211018708
69. Mehos BM, Saseen JJ, MacLaughlin EJ. Effect of pharmacist intervention and initiation of home blood pressure monitoring in patients with uncontrolled hypertension. Pharmacotherapy. (2000) 20:1384–9. doi: 10.1592/phco.20.17.1384.34891
70. Morgado M, Rolo S, Castelo-Branco M. Pharmacist intervention program to enhance hypertension control: a randomised controlled trial. Int J Clin Pharm. (2011) 33:132–40. doi: 10.1007/s11096-010-9474-x
71. Murray MD, Harris LE, Overhage JM, Zhou X-H, Eckert GJ, Smith FE, et al. Failure of computerized treatment suggestions to improve health outcomes of outpatients with uncomplicated hypertension: results of a randomized controlled trial. Pharmacotherapy. (2004) 24:324–37. doi: 10.1592/phco.24.4.324.33173
72. Naqvi IA, Strobino K, Kuen Cheung Y, Li H, Schmitt K, Ferrara S, et al. Telehealth after stroke care pilot randomized trial of home blood pressure telemonitoring in an underserved setting. Stroke. (2022) 53:3538–47. doi: 10.1161/STROKEAHA.122.041020
73. Nguyen-Huynh MN, Young JD, Ovbiagele B, Alexander JG, Alexeeff S, Lee C, et al. Effect of lifestyle coaching or enhanced pharmacotherapy on blood pressure control among Black adults with persistent uncontrolled hypertension: a cluster randomized clinical trial. JAMA Network Open. (2022) 5:e2212397. doi: 10.1001/jamanetworkopen.2022.12397
74. Okada H, Onda M, Shoji M, Sakane N, Nakagawa Y, Sozu T, et al. Effects of lifestyle advice provided by pharmacists on blood pressure: the community pharmacists assist for blood pressure (COMPASS-BP) randomized trial. Biosci Trends. (2017) 11:632–9. doi: 10.5582/bst.2017.01256
75. Okamoto MP, Nakahiro RK. Pharmacoeconomic evaluation of a pharmacist-managed hypertension clinic. Pharmacotherapy. (2001) 21:1337–44. doi: 10.1592/phco.21.17.1337.34424
76. Okoro RN, Umate I, Ohieku JD, Yakubu SI, Adibe MO. The impact of pharmacist-led interventions on blood pressure control among patients with chronic kidney disease: a randomized controlled trial. J Am Coll Clin Pharm. (2022) 5:1062–74. doi: 10.1002/jac5.1677
77. Park JJ, Kelly P, Carter BL, Burgess PP. Comprehensive pharmaceutical care in the chain setting: drug therapy monitoring and counseling by pharmacists contributed to improved blood pressure control in study patients. J Am Pharm Assoc. (1996) 36:443–51. doi: 10.1016/S1086-5802(16)30099-7
78. Paudel N, Shrestha S, Marasine NR, Khanal P, Aryal S, Erku D, et al. Impact of hospital pharmacist-delivered individualised pharmaceutical service intervention on clinical and patient-reported outcomes in patients with hypertension: a randomised controlled trial. Eur J Hosp Pharm. (2023) 30:316–21. doi: 10.1136/ejhpharm-2020-002512
79. Peralta CA, Frigaard M, Rolon L, Seal K, Tuot D, Senyak J, et al. Screening for CKD to improve processes of care among nondiabetic veterans with hypertension: a pragmatic cluster-randomized trial. Clin J Am Soc Nephrol. (2020) 15:174. doi: 10.2215/CJN.05050419
80. Planas LG, Crosby KM, Mitchell KD, Farmer KC. Evaluation of a hypertension medication therapy management program in patients with diabetes. J Am Pharm Assoc. (2009) 49:164–70. doi: 10.1331/JAPhA.2009.08164
81. Qudah B, Albsoul-Younes A, Alawa E, Mehyar N. Role of clinical pharmacist in the management of blood pressure in dialysis patients. Int J Clin Pharm. (2016) 38:931–40. doi: 10.1007/s11096-016-0317-2
82. Ramanath KV, Balaji DBSS, Nagakishore CH, Kumar SM, Bhanuprakash M. A study on impact of clinical pharmacist interventions on medication adherence and quality of life in rural hypertensive patients. J Young Pharm. (2012) 4:95–100. doi: 10.4103/0975-1483.96623
83. Ramanath KV, Venkappa KR. Study the impact of clinical pharmacist provided patient counseling on hypertension management in rural Indian population. Arch Pharm Pract. (2013) 4:28. doi: 10.4103/2045-080X.111579
84. Reid F, Murray P, Storrie M. Implementation of a pharmacist-led clinic for hypertensive patients in primary care–a pilot study. Pharm World Sci. (2005) 27:202–7. doi: 10.1007/s11096-004-2563-y
85. Rinfret S, Lussier M-T, Peirce A, Duhamel F, Cossette S, Lalonde L, et al. The impact of a multidisciplinary information technology–supported program on blood pressure control in primary care. Circulation: Cardiovascular Quality and Outcomes. (2009) 2:170–7. doi: 10.1161/CIRCOUTCOMES.108.823765
86. Rohla M, Haberfeld H, Tscharre M, Huber K, Weiss TW. Pharmacist interventions to improve blood pressure control in primary care: a cluster randomised trial. Int J Clin Pharm. (2023) 45:126–36. doi: 10.1007/s11096-022-01452-1
87. Saleem F, Hassali MA, Shafie AA, Ul Haq N, Farooqui M, Aljadhay H, et al. Pharmacist intervention in improving hypertension-related knowledge, treatment medication adherence and health-related quality of life: a non-clinical randomized controlled trial. Health Expect. (2015) 18:1270–81. doi: 10.1111/hex.12101
88. Santschi V, Rodondi N, Bugnon O, Burnier M. Impact of electronic monitoring of drug adherence on blood pressure control in primary care: a cluster 12-month randomised controlled study. Eur J Intern Med. (2008) 19:427–34. doi: 10.1016/j.ejim.2007.12.007
89. Santschi V, Lord A, Berbiche D, Lamarre D, Corneille L, Prud'homme L, et al. Impact of collaborative and multidisciplinary care on management of hypertension in chronic kidney disease outpatients. J Pharm Health Serv Res. (2011) 2:79–87. doi: 10.1111/j.1759-8893.2011.00038.x
90. Santschi V, Wuerzner G, Pais B, Chiolero A, Schaller P, Cloutier L, et al. Team-Based care for improving hypertension management: a pragmatic randomized controlled trial. Front Cardiovasc Med. (2021) 8:760662. doi: 10.3389/fcvm.2021.760662
91. Scala D, Menditto E, Caruso G, Monetti VM, Orlando V, Guerriero F, et al. Are you more concerned about or relieved by medicines? An explorative randomized study of the impact of telephone counseling by pharmacists on patients’ beliefs regarding medicines and blood pressure control. Patient Educ Couns. (2018) 101:679–86. doi: 10.1016/j.pec.2017.12.006
92. Skowron A, Polak S, Brandys J. The impact of pharmaceutical care on patients with hypertension and their pharmacists. Pharm Pract. (2011) 9:110. doi: 10.4321/S1886-36552011000200009
93. Solomon DK, Portner TS, Bass GE, Gourley DR, Gourley GA, Holt JM, et al. Part 2. Clinical and economic outcomes in the hypertension and COPD arms of a multicenter outcomes study. J Am Pharm Assoc. (1998) 38:574–85. doi: 10.1016/S1086-5802(16)30371-0
94. Sookaneknun P, Richards RME, Sanguansermsri J, Teerasut C. Pharmacist involvement in primary care improves hypertensive patient clinical outcomes. Ann Pharm. (2004) 38:2023–8. doi: 10.1345/aph.1D605
95. Stewart K, George J, Mc Namara KP, Jackson SL, Peterson GM, Bereznicki LR, et al. A multifaceted pharmacist intervention to improve antihypertensive adherence: a cluster-randomized, controlled trial (HAPPy trial). J Clin Pharm Ther. (2014) 39:527–34. doi: 10.1111/jcpt.12185
96. Svarstad BL, Kotchen JM, Shireman TI, Brown RL, Crawford SY, Mount JK, et al. Improving refill adherence and hypertension control in black patients: wisconsin TEAM trial. J Am Pharm Assoc. (2013) 53:520–9. doi: 10.1331/JAPhA.2013.12246
97. Tobari H, Arimoto T, Shimojo N, Yuhara K, Noda H, Yamagishi K, et al. Physician–pharmacist cooperation program for blood pressure control in patients with hypertension: a randomized-controlled trial. Am J Hypertens. (2010) 23:1144–52. doi: 10.1038/ajh.2010.127
98. Torres-Robles A, Benrimoj SI, Gastelurrutia MA, Martinez-Martinez F, Peiro T, Perez-Escamilla B, et al. Effectiveness of a medication adherence management intervention in a community pharmacy setting: a cluster randomised controlled trial. BMJ Qual Saf. (2022) 31:105–15. doi: 10.1136/bmjqs-2020-011671
99. Tsuyuki RT, Houle SKD, Charrois TL, Kolber MR, Rosenthal MM, Lewanczuk R, et al. Randomized trial of the effect of pharmacist prescribing on improving blood pressure in the community: the Alberta clinical trial in optimizing hypertension (RxACTION). Circulation. (2015) 132:93–100. doi: 10.1161/CIRCULATIONAHA.115.015464
100. Van der Laan DM, Elders PJM, Boons CCLM, Nijpels G, Van Dijk L, Hugtenburg JG. Effectiveness of a patient-tailored, pharmacist-led intervention program to enhance adherence to antihypertensive medication: the CATI study. Front Pharmacol. (2018) 9:1057. doi: 10.3389/fphar.2018.01057
101. Vivian EM. Improving blood pressure control in a pharmacist-managed hypertension clinic. Pharmacotherapy. (2002) 22:1533–40. doi: 10.1592/phco.22.17.1533.34127
102. Wal P, Wal A, Bhandari A, Pandey U, Rai AK. Pharmacist involvement in the patient care improves outcome in hypertension patients. J Res Pharm Pract. (2013) 2:123. doi: 10.4103/2279-042X.122386
103. Wang J, Wu J, Yang J, Zhuang Y, Chen J, Qian W, et al. Effects of pharmaceutical care interventions on blood pressure and medication adherence of patients with primary hypertension in China. Clin Res Regul Aff. (2011) 28:1–6. doi: 10.3109/10601333.2010.539230
104. Wang W, Geng L, Sun C, Li H, Wang J. Efficacy of pharmaceutical care in patients with type 2 diabetes mellitus and hypertension: a randomized controlled trial. Int J Clin Pract. (2022) 2022:7681404. doi: 10.1155/2022/7681404
105. Weber CA, Ernst ME, Sezate GS, Zheng S, Carter BL. Pharmacist-physician comanagement of hypertension and reduction in 24-hour ambulatory blood pressures. Arch Intern Med. (2010) 170:1634–9. doi: 10.1001/archinternmed.2010.349
106. Wong MCS, Liu KQL, Wang HHX, Lee CLS, Kwan MWM, Lee KWS, et al. Effectiveness of a pharmacist-led drug counseling on enhancing antihypertensive adherence and blood pressure control: a randomized controlled trial. J Clin Pharm. (2013) 53:753–61. doi: 10.1002/jcph.101
107. Zaragoza-Fernandez MP, Gastelurrutia MA, Cardero M, Martinez-Martinez F. Intensive two-month intervention on diet and lifestyle in uncontrolled hypertensive patients in a community pharmacy. Latin Am J Pharm. (2012) 31:727–33.
108. Zhai P, Hayat K, Ji W, Li Q, Shi L, Atif N, et al. Efficacy of text messaging and personal consultation by pharmacy students among adults with hypertension: randomized controlled trial. J Med Internet Res. (2020) 22:e16019. doi: 10.2196/16019
109. Zhao P-X, Wang C, Qin L, Yuan M, Xiao Q, Guo Y-H, et al. Effect of clinical pharmacist’s pharmaceutical care intervention to control hypertensive outpatients in China. Afr J Pharm Pharmacol. (2012) 6:48–56. doi: 10.5897/AJPP11.633
110. Zillich AJ, Sutherland JM, Kumbera PA, Carter BL. Hypertension outcomes through blood pressure monitoring and evaluation by pharmacists (HOME study). J Gen Intern Med. (2005) 20:1091–6. doi: 10.1111/j.1525-1497.2005.0226.x
111. Gutierrez MM, Sakulbumrungsil R. Effectiveness of a pharmacist-led expert system intervention for medication adherence and blood pressure control of adults with hypertension: a randomized controlled trial. Res Soc Admin Pharm. (2023) 19:931–43. doi: 10.1016/j.sapharm.2023.03.004
112. Luque del Moral R, Gastelurrutia MA, Martinez-Martinez F, Jacomé JA, Dago A, Suarez B, et al. Effect of pharmaceutical intervention in pharmacologically treated hypertensive patients—a cluster-randomized clinical trial: aFPRES-CLM study. J Pers Med. (2023) 13:1484. doi: 10.3390/jpm13101484
113. Moreira PM, Aguiar EC, Castro PR, Almeida KC, Dourado JA, Paula SM, et al. Optimizing hypertension treatment in older patients through home blood pressure monitoring by pharmacists in primary care: the MINOR clinical trial. Clin Ther. (2023) 45:941–6. doi: 10.1016/j.clinthera.2023.06.007
114. Mozu IE, Marfo AFA, Marfo JS, Adomako NO, Ayisi-Boateng NK, Boachie-Ansah P, et al. Utilization of telepharmacy in the management of hypertension. Explor Res Clin Soc Pharm. (2023) 12:100381. doi: 10.1016/j.rcsop.2023.100381
115. Kaczorowski J, Chambers LW, Karwalajtys T, Dolovich L, Farrell B, McDonough B, et al. Cardiovascular health awareness program (CHAP): a community cluster-randomised trial among elderly Canadians. Prev Med. (2008) 46:537–44. doi: 10.1016/j.ypmed.2008.02.005
116. Östbring MJ, Eriksson T, Petersson G, Hellström L. Effects of a pharmaceutical care intervention on clinical outcomes and patient adherence in coronary heart disease: the MIMeRiC randomized controlled trial. BMC Cardiovasc Disord. (2021) 21:1–16. doi: 10.1186/s12872-021-02178-0
117. Scherpbier-de Haan ND, Vervoort GMM, van Weel C, Braspenning JCC, Mulder J, Wetzels JFM, et al. Effect of shared care on blood pressure in patients with chronic kidney disease: a cluster randomised controlled trial. Br J General Pract. (2013) 63:e798–806. doi: 10.3399/bjgp13X675386
118. Chisholm-Burns MA, Lee JK, Spivey CA, Slack M, Herrier RN, Hall-Lipsy E, et al. US Pharmacists’ effect as team members on patient care: systematic review and meta-analyses. Med Care. (2010) 48:923–33. doi: 10.1097/MLR.0b013e3181e57962
119. Baral N, Volgman AS, Seri A, Chelikani V, Isa S, Javvadi SLP, et al. Adding pharmacist-led home blood pressure telemonitoring to usual care for blood pressure control: a systematic review and meta-analysis. Am J Cardiol. (2023) 203:161–8. doi: 10.1016/j.amjcard.2023.06.109
120. Garcia-Cardenas V, Rossing CV, Fernandez-Llimos F, Schulz M, Tsuyuki R, Bugnon O, et al. Pharmacy practice research–a call to action. Res Soc Admin Pharm. (2020) 16:1602–8. doi: 10.1016/j.sapharm.2020.07.031
121. Van Spall HGC, Rahman T, Mytton O, Ramasundarahettige C, Ibrahim Q, Kabali C, et al. Comparative effectiveness of transitional care services in patients discharged from the hospital with heart failure: a systematic review and network meta-analysis. Eur J Heart Fail. (2017) 19(11):1427–43. doi: 10.1002/ejhf.765
122. Nkansah N, Mostovetsky O, Yu C, Chheng T, Beney J, Bond CM, et al. Effect of outpatient pharmacists’ non-dispensing roles on patient outcomes and prescribing patterns. Cochrane Database Syst Rev. (2010) 2010(7):CD000336. doi: 10.1002/14651858.CD000336.pub2
123. Howick J, Koletsi D, Ioannidis JPA, Madigan C, Pandis N, Loef M, et al. Most healthcare interventions tested in cochrane reviews are not effective according to high quality evidence: a systematic review and meta-analysis. J Clin Epidemiol. (2022) 148:160–9. doi: 10.1016/j.jclinepi.2022.04.017
124. Ioannidis JPA, Greenland S, Hlatky MA, Khoury MJ, Macleod MR, Moher D, et al. Increasing value and reducing waste in research design, conduct, and analysis. Lancet. (2014) 383:166–75. doi: 10.1016/S0140-6736(13)62227-8
125. Skivington K, Matthews L, Simpson SA, Craig P, Baird J, Blazeby JM, et al. A new framework for developing and evaluating complex interventions: update of medical research council guidance. Br Med J. (2021) 374:n2061. doi: 10.1136/bmj.n2061
126. Alicia O, Croot L, Duncan E, Rousseau N, Sworn K, Turner KM, et al. Guidance on how to develop complex interventions to improve health and healthcare. BMJ Open. (2019) 9:e029954. doi: 10.1136/bmjopen-2019-029954
127. Marra C, Johnston K, Santschi V, Tsuyuki RT. Cost-effectiveness of pharmacist care for managing hypertension in Canada. Can Pharm J. (2017) 150:184–97. doi: 10.1177/1715163517701109
Keywords: hypertension, blood pressure, pharmacists, pharmaceutical care, systematic review, meta-analysis
Citation: Gastens V, Tancredi S, Kiszio B, Del Giovane C, Tsuyuki RT, Paradis G, Chiolero A and Santschi V (2025) Pharmacists delivering hypertension care services: a systematic review and meta-analysis of randomized controlled trials. Front. Cardiovasc. Med. 12:1477729. doi: 10.3389/fcvm.2025.1477729
Received: 11 September 2024; Accepted: 12 February 2025;
Published: 14 March 2025.
Edited by:
Guido Iaccarino, Federico II University Hospital, ItalyReviewed by:
Giuliano Tocci, Sapienza University of Rome, ItalyCopyright: © 2025 Gastens, Tancredi, Kiszio, Del Giovane, Tsuyuki, Paradis, Chiolero and Santschi. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Valérie Santschi, di5zYW50c2NoaUBlY29sZWxhc291cmNlLmNo
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.