 Roberto Baltodano-Arellano1,2Eduardo Alvarez-Tiburcio3Lucia Barriales-Revilla4
Roberto Baltodano-Arellano1,2Eduardo Alvarez-Tiburcio3Lucia Barriales-Revilla4 David Bellido-Yarlequé3Angela Cachicatari1Kelly Cupe-Chacalcaje1Alan La Torre-Zuñiga5
David Bellido-Yarlequé3Angela Cachicatari1Kelly Cupe-Chacalcaje1Alan La Torre-Zuñiga5 Kevin Velarde-Acosta4*
Kevin Velarde-Acosta4*
- 1Cardiac Imaging Area of Cardiology Service, Hospital Guillermo Almenara Irigoyen – EsSalud, Lima, Peru
- 2School of Medicine, Universidad Nacional Mayor de San Marcos, Lima, Peru
- 3Cardiac Surgery Unit, Hospital Guillermo Almenara Irigoyen - EsSalud, Lima, Peru
- 4Clinical Cardiology Service, Hospital Guillermo Almenara Irigoyen - EsSalud, Lima, Peru
- 5Pathological Anatomy Service, Hospital Edgardo Rebagliati Martins - EsSalud, Lima, Peru
A 49-year-old female patient, asymptomatic, presented to the cardiology office for a right atrial mass, identified incidentally in a non-electrocardiogram (ECG)-gated contrast-enhanced computed tomography, performed for follow-up of pulmonary tuberculosis. Echocardiography, surprisingly, showed an anechogenic ovoid mass in the right atrium measuring 40 × 40 mm2, implanted in the interatrial septum without affecting the tricuspid valve. ECG-gated computed tomography angiography (CTA), confirmed the dimensions of the mass, which presented homogeneous content, calcified areas, and a 12-mm pedicle implanted near the ostium of the coronary sinus. Additionally, contrast uptake and infiltration of adjacent structures were ruled out. In the surgical field, an encapsulated mass with blood content was found, which pathology reported as a hematic endocardial cyst (HEC). These are rare cardiac masses, constituting 1.5% of all primary cardiac tumors. It is usually an incidental finding, and its clinical presentation will depend on its dimensions and the intracardiac hemodynamic impact. A highlighting feature is its anechogenic content on ultrasound, however, multimodality imaging allows for making diagnostic assumptions, discerning between primary cardiac tumors, and provides morphological and hemodynamic information useful for therapeutic decision making. The age of the patient, the large size of the HEC, and its location in the interatrial septum make up a completely atypical presentation of this rare disease, which motivated this report.
Case report
Clinical presentation
A 49-year-old woman from the Peruvian Andes presented to the cardiology office due to an incidental tomographic finding of a mass in the right atrium. In the anamnesis, the patient reported being asymptomatic, while the cardiorespiratory physical examination did not show relevant findings. Her medical history was notable for a tuberculous pulmonary nodule removed 2 years previously, for which she received complete treatment for 6 months and required subsequent computed tomography (CT) controls. She had no cardiovascular risk factors or relevant family or socioeconomic history. Laboratory tests were within normal ranges, while the electrocardiogram showed no pathological alterations.
Differential diagnosis
In the presence of a right atrial mass implanted in the interatrial septum, a myxoma should be considered due to its frequency (1–3). Echocardiography and magnetic resonance imaging (MRI) determine structural and tissue characteristics that bring the diagnosis closer. On some occasions, the finding of a thrombus trapped in the foramen ovale has been described in transesophageal echocardiography (TEE) (4, 5). This mass's cystic appearance guides the diagnosis of rarer pathologies such as cardiac hydatid, bronchogenic or endocardial hematic cyst, which are usually diagnosed in pathological anatomy (6–8).
Diagnostic workup
A cardiologic study plan was initiated with transthoracic echocardiography (TTE), which confirmed the presence of an anechogenic ovoid mass in the right atrium measuring 40 mm × 40 mm2, implanted in the interatrial septum without affecting the tricuspid valve (Figure 1A; Supplementary Video S1). In the study with agitated saline solution, echogenicity of the blood-like mass was evident (Figures 1B,D, Supplementary Video S2). No additional relevant findings were found.
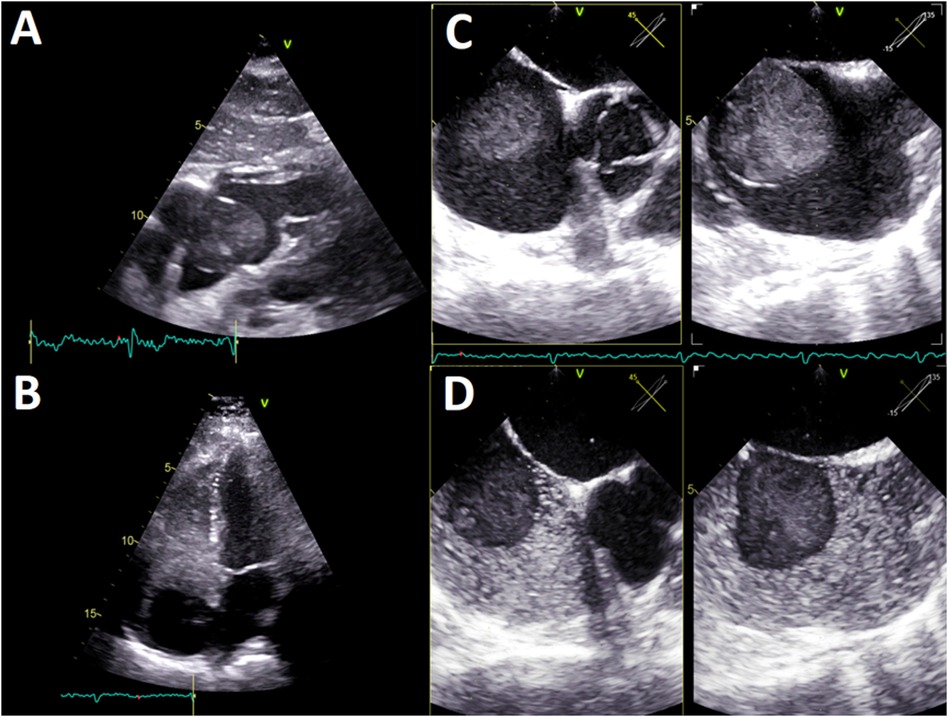
Figure 1 (A) TTE, four-chamber subcostal view. Ovoid mass in the right atrium, with echogenicity almost blood-like and calcification areas. (B) TTE, four-chamber apical view. The agitated saline test shows an anechogenic, 40 × 40 mm2, mass in the right atrium implanted in the interatrial septum. No tricuspid valve compromise was observed. (C) TEE, multiplanar image of the interatrial septum (45°; 135°). A homogeneous pedunculated mass with a thin covering was implanted in the middle-low interatrial septum with pendulum movement. (D) TEE, multiplanar image of the interatrial septum (45°; 135°). The agitated saline test depicts anechogenicity of the hematic mass. TTE, transthoracic echocardiography; TEE, transesophageal echocardiography.
The TEE showed a homogeneous mass covered by a thin layer, implanted in the mid-low septum, and exhibited pendulum movement (Figure 1C, Supplementary Video S3). Furthermore, the previous dimensions were confirmed and no signs suggestive of vascularization were found. Given these findings, the diagnosis work-up was complemented with an ECG-gated CTA, displaying an ovoid, mobile mass of 35 mm in diameter with homogeneous content and calcified areas with a 12-mm pedicle adhered to the lower atrial septum near the coronary sinus ostium (Figure 2).

Figure 2 (A,B) ECG-gated CTA, four-chamber view. A mobile, round, homogenous mass is seen adhered to the right lower interatrial septum. (C,D) ECG-gated CTA, sagittal views of the right atrium. A homogeneous, non-contrast-enhancing mass with calcified areas and defined edges is seen in the right atrium. Note the 12 mm pedicle (red arrow) that attaches it to the interatrial septum, near the fossa ovalis. Likewise, the right coronary artery (orange arrow) is seen, which does not provide collateral to the mass. ECG, electrocardiogram; CTA, computed tomography angiography.
Treatment
With these findings, the patient underwent an open surgical resection of the mass. After the right atriotomy, a violaceous, smooth, tense, and shiny mass was found, suggesting a cyst with bloody content (Figure 3A). The pathological study described a fibrous (collagenous) wall devoid of epithelium and with few inflammatory cells. Furthermore, fibrin content with areas of calcification was reported (Figures 3B,C), confirming the diagnosis of HEC (8–10).
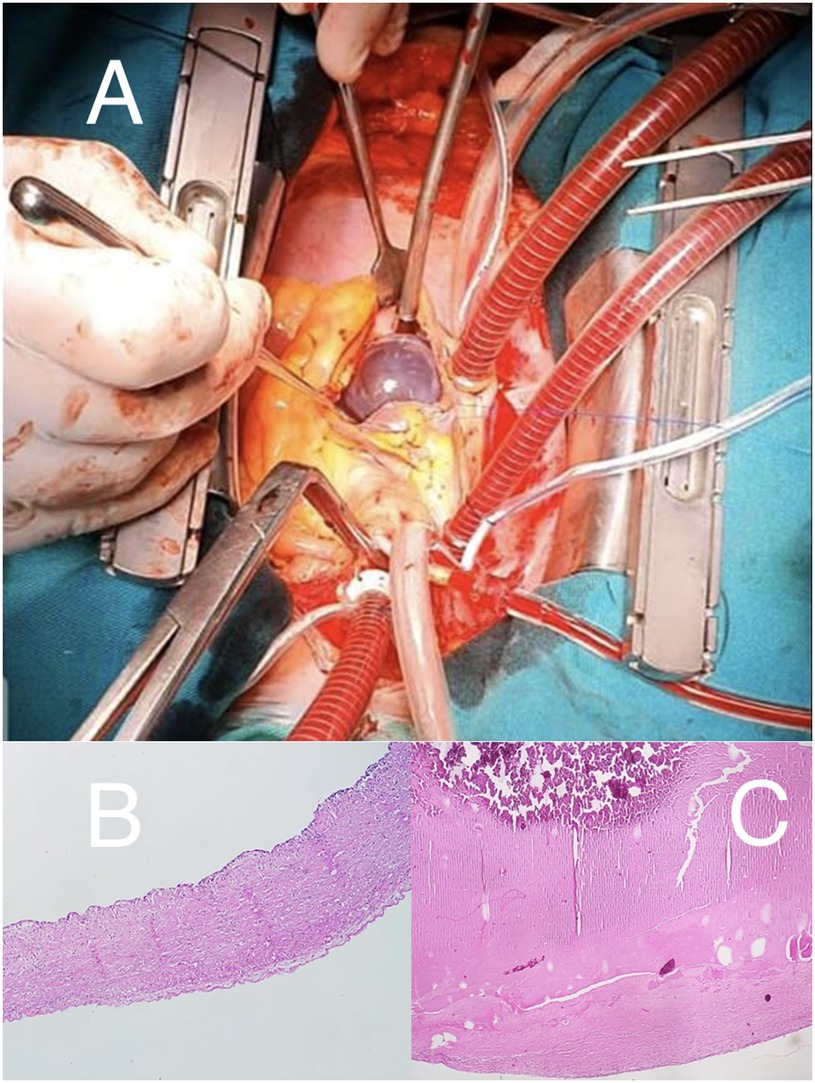
Figure 3 (A) Surgical field. Right atriotomy, with exposure of violaceous, smooth, and shiny mass. (B) Microscopy: fibrous (composed of collagenous layers) cyst wall without epithelial cells. Presence of some lymphocytes. (C) Microscopy: uniform fibrin content with calcification areas (upper region with more intense staining).
Follow-up
At one year of follow-up, the patient did not present relevant symptoms, except for a nonspecific chest pain in the healed surgical wound. Due to a suboptimal acoustic window, TEE was performed, which excluded mass recurrence.
Discussion
HEC constitutes 1.5% of all cardiac tumors (8). It occurs mainly in infants and its preferential location is the heart valves (8, 9, 11). Its origin is still unknown, but two hypotheses are suggested: the first describes ectatic vessels evolving into a hematic cyst, and the second describes local inflammation that develops into a hematoma and transforms into a hematic cyst (8, 9).
To learn about clinical and therapeutic features in adults affected by this rare entity, we did an extensive search of the medical literature in Medline for articles published up to January 2022 (Table 1). Our search revealed that this disease occurs indistinctly in both sexes and the main location of this mass is the mitral valve, as it occurs in infants. Likewise, it allowed us to know that, in our case, the magnitude of the mass, located in an uncommon site, is the largest published in the literature.
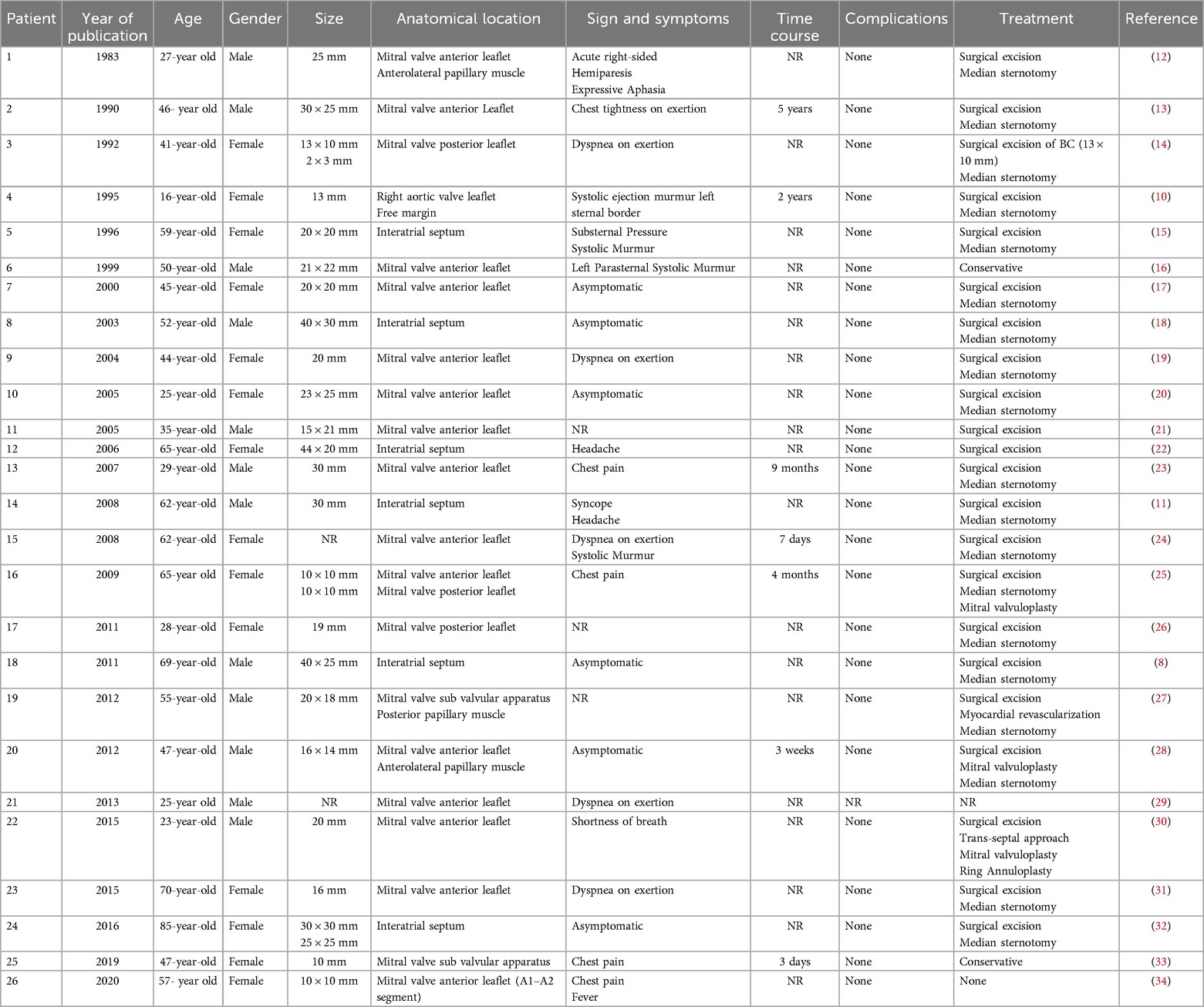
Table 1 Reported cases of hematic cyst in adult patients.
The set of symptoms depends on the mass dimensions and its impact on intracardiac hemodynamics. As cysts may involve the free edges of the valves, patients can present with dyspnea or heart murmurs due to valve regurgitation. Other clinical manifestations described are systemic embolism, syncope, or even sudden death (8, 9). Despite the multiple possibilities of clinical manifestations, the vast majority of findings of this tumor are incidental, as seen in our patient in whom the tumor was discovered in a tomographic control for pulmonary tuberculosis.
Within cardiac imaging studies, echocardiography is essential for the initial examination of intracardiac masses (1–3, 35, 36). It provides morphological information, data on the anatomical relationship, and determines the hemodynamic impact of the HEC. The cysts have particular ultrasound characteristics such as a thin reflective layer and an echolucent content, which could go unnoticed by novice explorers (9, 11). A meticulous analysis of our patient images confirmed these findings. The agitated saline solution study was useful because it highlighted the magnitude and dynamics of the mass, in addition to ruling out interatrial shunts. TEE describes with high precision anatomical aspects of atrial masses and defines carefully the components of a cyst, including the absence of vascularization, as seen in the images of this case (8, 9).
ECG-gated CTA reported a homogeneous mass with calcified areas and defined edges, mobile, without contrast-enhancing or infiltration. Also, it excluded the presence of additional intra-cardiac masses, contributing to better surgical planning (37). Cardiac MRI is an important technique to define contrast uptake in masses. In particular, hematic cysts do not capture medium contrast, because they are not vascularized, unlike a malignant neoplasm (9). Due to the cystic structure, hydatid disease must be ruled out through specific MRI sequences that differentiate it from the hematic cyst. In the former the T1 signal is hypointense and T2 signal hyperintense, while in the latter the T1 and T2 signals are isointense (11). Despite the usefulness of cardiac MRI for the differential diagnosis of cardiac masses, it was not performed in our patient because the magnetic resonator was inoperative during that period; likewise, surgical resection of the cyst had already been decided by the Heart Team based on ultrasound and tomographic features.
The decision to surgically remove an asymptomatic cardiac mass is based on avoiding embolic phenomena and ruling out malignancy. If the nature of this tumor is specified with imaging tests, the surgical time will depend on the speed of growth, hemodynamic impact, and the risks of rupture and embolization (8, 9, 38, 39). Although our patient did not present cardiac symptoms, the intervention was based on age, the low risk of malignancy, the dimensions of the mass and the prevention of embolisms, as occurred in the vast majority of cases reported in the literature.
Conclusions
The HEC is an extremely rare mass that usually affects the heart valves of infants. The characteristics of this report, such as the adult age of the patient, the anatomical location in the interatrial septum, and the gigantic dimensions of the mass, are unprecedented in the medical literature.
Multimodality imaging allows differential diagnosis between primary cardiac tumors and provides useful morphological and hemodynamic information for therapeutic decision making. Surgical removal avoids embolic phenomena and hemodynamic disturbances. Finally, the purplish, smooth, shiny, blood-bag-like surgical piece is a distinguishable feature of this cardiac mass.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
Ethics statement
Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author contributions
RB-A: Conceptualization, Data curation, Formal Analysis, Software, Supervision, Visualization, Writing – original draft, Writing – review & editing. EA-T: Writing – original draft. LB-R: Conceptualization, Data curation, Software, Validation, Visualization, Writing – original draft, Writing – review & editing. DB-Y: Writing – original draft. AC: Software, Writing – review & editing. KC-C: Software, Writing – original draft, Writing – review & editing. AL: Writing – original draft. KV-A: Conceptualization, Formal Analysis, Supervision, Visualization, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fcvm.2024.1417074/full#supplementary-material
Supplementary Video S1
TTE, subcostal view. Evidence of ovoid mass in the right atrium with mainly hypoechoic contents.
Supplementary Video S2
TTE, apical view 4 chambers. Agitated saline demonstrates a mass in the right atrium with echogenicity similar to blood.
Supplementary Video S3
TEE, X-plane. Saline solution test highlights pear morphology of mass implanted in the interatrial septum.
Supplementary Data Sheet 1
Timeline of patient evolution.
References
1. Tyebally S, Chen D, Bhattacharyya S, Mughrabi A, Hussain Z, Manisty C, et al. Cardiac tumors: JACC CardioOncology state-of-the-art review. JACC CardioOncol. (2020) 2(2):293–311. doi: 10.1016/j.jaccao.2020.05.009
2. Basso C, Rizzo S, Valente M, Thiene G. Cardiac masses and tumours. Heart. (2016) 102(15):1230–45. doi: 10.1136/heartjnl-2014-306364
3. Bussani R, Castrichini M, Restivo L, Fabris E, Porcari A, Ferro F, et al. Cardiac tumors: diagnosis, prognosis, and treatment. Curr Cardiol Rep. (2020) 22(12):169. doi: 10.1007/s11886-020-01420-z
4. Seo WW, Kim SE, Park MS, Lee JH, Park DG, Han KR, et al. Systematic review of treatment for trapped thrombus in patent foramen Ovale. Korean Circ J. (2017) 47(5):776–85. doi: 10.4070/kcj.2016.0295
5. Zoltowska DM, Agrawal Y, Kalavakunta JK. Serpentine thrombus in the heart: a rare case of trapped thrombus in patent foramen ovale. BMJ Case Rep. (2018) 2018:bcr2017223469. doi: 10.1136/bcr-2017-223469
6. Oraha AY, Faqe DA, Kadoura M, Kakamad FH, Yaldo FF, Aziz SQ. Cardiac hydatid cysts; presentation and management. A case series. Ann Med Surg (Lond). (2018) 30:18–21. doi: 10.1016/j.amsu.2018.04.001
7. Fukudome Y, Hieda M, Masui S, Yokoyama T, Futami S, Moriyama S, et al. Case report: bronchogenic cyst in the right atrium of a young woman. Front Cardiovasc Med. (2022) 9:915876. doi: 10.3389/fcvm.2022.915876
8. Mori F, Oddo A, Fabbri V, Perini AP, Stefano PL, Taddei GL. Endocardial blood cyst: a rare site and age of presentation. Echocardiography. (2011) 28(3):E50–2. doi: 10.1111/j.1540-8175.2010.01306.x
9. Bortolotti U, Vendramin I, Lechiancole A, Sponga S, Pucci A, Milano AD, et al. Blood cysts of the cardiac valves in adults: review and analysis of published cases. J Card Surg. (2021) 36(12):4690–98. doi: 10.1111/jocs.15992
10. DeGroff C, Silberbach M, Sahn DJ, Droukas P. Giant blood cyst of the aortic valve. J Am Soc Echocardiogr. (1995) 8(4):543–5. doi: 10.1016/s0894-7317(05)80343-8
11. Centella T, Moya JL, Muñoz M, Reguero EM. Images in cardiovascular medicine. Giant endocardial blood cyst in the right atrium: echocardiographic and magnetic resonance imaging features. Circulation. (2008) 117(25):3250–1. doi: 10.1161/CIRCULATIONAHA.107.734814
12. Hauser AM, Rathod K, McGill J, Rosenberg BF, Gordon S, Timmis GC. Blood cyst of the papillary muscle. Clinical, echocardiographic and anatomic observations. Am J Cardiol. (1983) 51(3):612–3. doi: 10.1016/s0002-9149(83)80109-x
13. Arnold IR, Hubner PJ, Firmin RK. Blood filled cyst of the papillary muscle of the mitral valve producing severe left ventricular outflow tract obstruction. Br Heart J. (1990) 63(2):132–3. doi: 10.1136/hrt.63.2.132
14. Xie SW, Lu OL, Picard MH. Blood cyst of the mitral valve: detection by transthoracic and transesophageal echocardiography. J Am Soc Echocardiogr. (1992) 5(5):547–50. doi: 10.1016/s0894-7317(14)80047-3
15. Niinami H, Ishihara S, Hara S, Tanaka S, Yamaguti E, Takase S. Blood cyst with a calcium stone originating from the right atrial septum. Cardiovasc Surg. (1996) 4(2):260–2. doi: 10.1016/0967-2109(96)82329-5
16. Pelikan HM, Tsang TS, Seward JB. Giant blood cyst of the mitral valve. J Am Soc Echocardiogr. (1999) 12(11):1005–7. doi: 10.1016/s0894-7317(99)70157-4
17. Kuvin J, Saha P, Rastegar H, Salomon RN, Pandian N, Denofrio D. Blood cyst of the mitral valve apparatus in a woman with a history of orthotopic liver transplantation. J Am Soc Echocardiogr. (2004) 17(5):480–2. doi: 10.1016/j.echo.2004.01.013
18. Tanaka H, Ebato M, Narisawa T, Mori T, Masuda M, Suzuki T, et al. Atrial blood cyst with ischemic heart disease. Circ J. (2003) 67(1):91–2. doi: 10.1253/circj.67.91
19. Minneci C, Casolo G, Popoff G, Sulla A, Comin CE, Pedemonti E. A rare case of left ventricular outflow obstruction. Eur J Echocardiogr. (2004) 5(1):72–5. doi: 10.1016/s1525-2167(03)00041-6
20. Yamamoto H, Nakatani S, Niwaya K, Ohnishi T, Uematsu M, Kitakaze M. Images in cardiovascular medicine. Giant blood cyst of the mitral valve: echocardiographic and intraoperative images. Circulation. (2005) 112(22):e341. doi: 10.1161/CIRCULATIONAHA.105.546390
21. Kurtoğlu N, Yildirim T, Uzunlar B, Cevik C, Incedere O, Dindar I. A rare case: blood cyst of the mitral valve. Anadolu Kardiyol Derg. (2005) 5(4):34616330417.
22. Seebacher G, Binder T, Frank H, Wolner E, Mohl W. Cystic formation of the foramen ovale mimicking a right atrial myxoma. Ann Thorac Surg. (2006) 82(6):2296–8. doi: 10.1016/j.athoracsur.2006.04.051
23. Zhang C, Hu J, Ni YM, Jiang ZN, Xu HY. Giant blood cyst tumor in the left ventricular outflow tract. Chin Med J (Engl). (2007) 120(12):1109–10. doi: 10.1097/00029330-200706020-00015
24. Mandegar MH, Roshanali F, Rayatzadeh H. Cyst-like lesion on mitral valve. J Card Surg. (2008) 23(1):97. doi: 10.1111/j.1540-8191.2007.00554.x
25. Dencker M, Jexmark T, Hansen F, Tydén P, Roijer A, Lührs C. Bileaflet blood cysts on the mitral valve in an adult. J Am Soc Echocardiogr. (2009) 22(9):1085.e5–8. doi: 10.1016/j.echo.2009.04.002
26. Kühn A, Schreiber C, Weirich G, Vogt M. Intracardiac blood cyst: rare finding in a complex congenital heart lesion. Eur Heart J. (2012) 33(2):229. doi: 10.1093/eurheartj/ehr222
27. Donndorf P, Bermaoui B, Westphal B, Steinhoff G. Asymptomatic blood cyst of the papillary muscle in an adult undergoing coronary bypass surgery. Interact Cardiovasc Thorac Surg. (2013) 16(3):402–4. doi: 10.1093/icvts/ivs495
28. Park MH, Jung SY, Youn HJ, Jin JY, Lee JH, Jung HO. Blood cyst of subvalvular apparatus of the mitral valve in an adult. J Cardiovasc Ultrasound. (2012) 20(3):146–9. doi: 10.4250/jcu.2012.20.3.146
29. Sun F, Ren W, Bi W, Zhang Y, Guo B. A “balloon” on the mitral valve. J Am Coll Cardiol. (2013) 62(1):81. doi: 10.1016/j.jacc.2012.12.062
30. Halim J, van Schaagen FR, Riezebos RK, Lalezari S. Giant intracardiac blood cyst: assessing the relationship between its formation and previous cardiac surgery. Neth Heart J. (2015) 23(7-8):392–4. doi: 10.1007/s12471-015-0707-4
31. Madhavan S, Jayaprakash K, Jayaprasad N, Sathish G, George R. Blood cyst of the anterior mitral leaflet causing severe mitral regurgitation. Proc (Bayl Univ Med Cent). (2015) 28(3):363–4. doi: 10.1080/08998280.2015.11929275
32. Otsuka H, Arinaga K, Fukuda T, Takaseya T, Shojima T, Takagi K, et al. Double right atrial blood cysts. Ann Thorac Surg. (2016) 101(5):e147–9. doi: 10.1016/j.athoracsur.2015.10.021
33. Ludhwani D, Sheikh B, Sheikh Y. Evaluation of mitral apparatus blood cyst: a case report and review of literature. Cureus. (2019) 11(10):e5812. doi: 10.7759/cureus.5812
34. Ramírez-Mesías DC, Contreras-Valero JF, Pinilla-Monsalve GD, Vesga-Reyes CE. Blood cyst of the mitral valve diagnosed in an adult after systemic thrombolysis. Case Rep Cardiol. (2020) 2020:4320269. doi: 10.1155/2020/4320269
35. Mitchell C, Rahko PS, Blauwet LA, Canaday B, Finstuen JA, Foster MC, et al. Guidelines for performing a comprehensive transthoracic echocardiographic examination in adults: recommendations from the American society of echocardiography. J Am Soc Echocardiogr. (2019) 32(1):1–64. doi: 10.1016/j.echo.2018.06.004
36. Baltodano-Arellano R, Falcón-Quispe L, Cupe-Chacalcaje K, Meléndez-Ramírez G, Cachicatari-Beltran A, Patrón-Chi S, et al. Collection of cardiac masses. Up-to-date echocardiography and cardiac MRI tools. Echocardiography. (2024) 41(2):e15757. doi: 10.1111/echo.15757
37. Sheng C, Yang C, Cheng Y, Li YM. Current status of diagnosis and treatment of primary benign cardiac tumors in children. Front Cardiovasc Med. (2022) 9:947716. doi: 10.3389/fcvm.2022.947716
38. Imai A, Enomoto Y, Shigeta O, Suzuki Y. Right atrial blood cyst in elderly patient: the timing of surgery. Asian Cardiovasc Thorac Ann. (2020) 28(8):500–03. doi: 10.1177/0218492320949406
Keywords: right atrium, cardiac hematic cyst, echocardiography, computed tomography angiography, multimodality imaging
Citation: Baltodano-Arellano R, Alvarez-Tiburcio E, Barriales-Revilla L, Bellido-Yarlequé D, Cachicatari A, Cupe-Chacalcaje K, La Torre-Zuñiga A and Velarde-Acosta K (2024) Case report and literature review: cardiac hematic cyst. Front. Cardiovasc. Med. 11: 1417074. doi: 10.3389/fcvm.2024.1417074
Received: 14 April 2024; Accepted: 18 July 2024;
Published: 30 July 2024.
Edited by:
Matthias Renker, Kerckhoff Clinic, GermanyReviewed by:
Ionut Donoiu, University of Medicine and Pharmacy of Craiova, RomaniaMarcello Chiocchi, University of Rome Tor Vergata, Italy
© 2024 Baltodano-Arellano, Alvarez-Tiburcio, Barriales-Revilla, Bellido-Yarlequé, Cachicatari, Cupe-Chacalcaje, La Torre-Zuñiga and Velarde-Acosta. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Kevin Velarde-Acosta, a2V2aW5fdmVsYXJkZS45M0Bob3RtYWlsLmNvbQ==