 Borut Jug
Borut Jug Natasa Sedlar Kobe
Natasa Sedlar Kobe Dejana Stojinic1
Dejana Stojinic1 Mitja Lainscak
Mitja Lainscak Jerneja Farkas
Jerneja Farkas
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Cardiovasc. Med. , 30 July 2024
Sec. Cardiovascular Epidemiology and Prevention
Volume 11 - 2024 | https://doi.org/10.3389/fcvm.2024.1373684
Background: This study aimed to quantitatively assess stress, anxiety and obsessive thinking related to coronavirus disease-19 (COVID-19) and qualitatively appraise perceptions in patients after acute myocardial infarction (AMI) undergoing cardiac rehabilitation (CR) during the COVID-19 pandemic.
Methods: We used mixed-methods design in patients referred for CR in 2 centres which delivered uninterrupted service during COVID-19 pandemic. Coronavirus Anxiety Scale (CAS), Obsession with COVID-19 Scale (OCS), COVID-19 Stress Scale (CSS), Hospital Anxiety and Depression Scale (HADS), and in-person interviews (combination of a priori questions and probing) were used to evaluate patient experience and perceptions with COVID-19 and the healthcare services during pandemic.
Results: In total, 109 patients (mean age 59 ± 10, 20% women) were included in quantitative part and in 30 of them we conducted the in-person interviews. About a quarter of patients met HADS threshold for anxiety and depression while CAS and OCS results demonstrated extremely low possibility of coronavirus related dysfunctional thinking (3%) and anxiety (2%). The CSS indicated the most prevalent concerns were related to COVID-19 vaccines safety (60%) and fear of getting infected (60%). During interviews, patients perceived the CR as well as health care providers as safe, trustworthy and with enough support to avoid or manage COVID-19 related health risks.
Conclusions: Overall, patients reported AMI affected their lives more than the COVID-19 pandemic. The COVID-19 related stress and anxiety were relatively low and mostly related to general views of infectious disease. CR was perceived safe and trustworthy in terms of primary disease and COVID-19.
Lay summary: This mixed-method study included 109 patients with acute myocardial infarction who underwent cardiac rehabilitation during the COVID-19 and focused on their experience and perceptions with COVID-19 and the healthcare services during pandemic.
- Patients reported acute myocardial infarction affected their lives more than the COVID-19 pandemic.
- The COVID-19 related concerns were mostly related to general views of infectious disease (vaccine safety, fear of getting infected) whilst cardiac rehabilitation was perceived safe and trustworthy environment during COVID-19.
Cardiac rehabilitation is a complex multifaceted intervention providing exercise training, cardiovascular risk factor control, secondary prevention and psychosocial support (1–3). The majority of cardiac rehabilitation programs provide centre-based services with patients attending at least 36 group sessions over 12 weeks (4, 5); such organisational framework can accommodate enough interventions to improve cardiovascular outcomes, but also provides patients with intensive follow-up and psychosocial support in the immediate post-diagnosis period (3, 6). In Slovenia, a network of cardiac rehabilitation centres (affiliated with eight regional hospitals) has been established in 2017 and provides unifying content and structure of cardiac rehabilitation programs through a uniform national clinical pathway (7, 8).
The coronavirus disease-19 (COVID-19) pandemic, however, severely disrupted the provision of healthcare, including cardiac rehabilitation. Access to cardiac rehabilitation was hindered by diversion of resources, public health guidance and governmental restrictions (9). Responses of cardiac rehabilitation centres in Slovenia varied from complete shut-downs to carefully adapting programs to the challenges of the COVID-19 pandemic, as reported for other countries (10, 11). While promising alternatives, such as home-based and telerehabilitation, are viable options for cardiac rehabilitation (11, 12), their immediate implementation during the pandemic proved challenging (13); most programs, therefore, continued to provide centre-based rehabilitation on-site, with additional provisions for disease control, including ventilation, face coverings, regular testing, and provision of timely COVID-19 related information (4, 5, 14).
The impact of COVID-19 on cardiovascular healthcare was immediately tangible, while its long-term ramifications have yet to emerge in full (15). In the general population, increased sedentary behaviours, unhealthy eating patterns, along with stress and anxiety during the pandemic have been extensively reported (16–18). In patients undergoing outpatient cardiac rehabilitation, the closure of centres resulted in lost opportunities for functional improvements, motivation, supervision and group-based social support (19). Conversely, experiences and psychological well-being of patients participating in cardiac rehabilitation during the pandemic have been less thoroughly addressed (20, 21).
The information about COVID-19 pandemic effects on patient psychological well-being, personal experience, and trust in the health-care system during cardiac rehabilitation is insufficient. We concieved the mixed-methods study to quantitatively assess stress, anxiety and obsessive thinking related to COVID-19 and qualitatively appraise perceptions in patients attending centre-based cardiac rehabilitation during the COVID-19 pandemic.
The study was conducted from February 2021 to April 2021, with pandemic in Slovenia in its third wave, with restrictive measures at its peak and with vaccination in its infancy (available as of December 2020, primarily reserved for persons at higher risk of infection). We used mixed-methods approach — i.e., a quantitative prospective design with dedicated instruments (for COVID-19-related anxiety, obsessive thinking, stress, generalized anxiety and depression), and qualitative descriptive design (to examine participants' perceptions of their experiences with cardiac rehabilitation during the COVID-19 pandemic).
Participants were recruited from two cardiac rehabilitation centres in Slovenia (one university and one regional hospital), which provided uninterrupted cardiac rehabilitation throughout the pandemic. Referral to cardiac rehabilitation after acute myocardial infarction followed international and national recommendations and referral pathways. Eligible patients were adults (over 18 years), who had attended at least 5 cardiac rehabilitation sessions between January 2021 and April 2021.
Cardiac rehabilitation was provided through a structured and comprehensive program with 36 sessions adhering to pertinent guidelines. During the pandemic, the programs were adapted to contain the risk of COVID-19 infection in line with national public health guidance, governmental regulations and professional recommendations. Adapted provision included: limiting number of participants per session (maximal 3, at least 30 m3 per patient), intensified hygienic provision, mandatory ventilation and/or opening of windows, mask mandates as per government regulations, regular testing when available (at no cost for patients), regular informing of patients on COVID-19 related issues (including promotion of public health recommendations).
We collected basic demographic, socioeconomic, risk factors, comorbidities, and pharmacotherapy information. Additionally, patients completed three COVID-19 related questionnaires and the Hospital Anxiety and Depression Scale (HADS).
The Coronavirus Anxiety Scale (CAS) is a reliable instrument (αs >.90) with solid factorial and construct validity, which captures the frequency of dysfunctional anxiety associated with the COVID-19 pandemic through 5 items scored on a 5-point Likert scale from 0 (“Not at all”) to 4 (“Almost every day over the last two weeks”); the total score ranges from 0 to 20 (with the cut-off ≥9 providing 90% sensitivity and 85% specificity). Internal consistency for the scale in the present study was α = .83 (22).
The Obsession with COVID-19 Scale (OCS) is a reliable instrument (αs >.83) with solid factorial and construct validity, which captures the frequency of obsessive thinking about COVID-19. Four items are scored on a 5-point Likert scale from 0 (“Not at all”) to 4 (“Almost every day over the last two weeks”); the total score ranges from 0 to 16 (with the cut-off ≥7 providing 81%–93% sensitivity and 73%–76% specificity). Internal consistency for the scale in the present study was α = .88 (23).
A dedicated COVID-19 Stress Scale (CSS) was constructed examining the relevant literature and existing COVID-19-related scales (24); with 19 items, various kinds of concerns about the virus over the past month are investigated and scored on a 5-point scale from 0 (“Not at all”/“Never”) to 4 (“Extremely”/“Almost always”). Following the factor structure of the standard COVID-19 Stress Scale (25), items capturing COVID-19 related fears of becoming infected (4 items), perceived risk of infection when coming into contact with possibly contaminated objects or surfaces (4 items), compulsive checking and reassurance regarding possible pandemic related threats (6 items) pertinent to patients undergoing cardiac rehabilitation were selected. Additionally, 5 items capturing COVID-19 related health-care consequences were constructed. The total score ranges from 0 to 76. The current study yielded acceptable to good reliability coefficients for each of the three subscales (Danger/Contamination fears, α = .92; Checking/Reassurance seeking, α = .76; Health-care consequences, α = .73) and the overall scale (α = .91). Confirmatory factor analysis in the Mplus 6 program (26) using the WLSMV estimator indicated that the proposed 3-factor model (Danger/Contamination fears, Checking/Reassurance seeking, Health-care consequences) fits better than the 1-factor model. All factor loadings for the model were greater than 0.50 (see Appendix 1).
HADS is a valid and reliable instrument, which captures symptoms relating to generalised anxiety (HADS-A subscale) and anhedonia, central aspect of depression (HADS-D) (28, 29). Fourteen items (7 for each subscale) are scored on a 4-point Likert scale from 0 to 3, with each subscale score ranging from 0 to 21. Values 8–10 and ≥11 indicate possible and probable mood disorder, respectively; the minimal clinically important difference for cardiac patients is estimated at 1.7 points (30).
We aimed to interview 15%–20% of included patients, with sample size determined by data saturation criteria (ie. no new categories obtained in the last two interviews). Two investigators (D.S., N.S.) conducted 30–60 min in-person interviews with patients attending cardiac rehabilitation. A semi-structured interview used a priori questions (Table 1) and probing (31) to identify perceptions of cardiac rehabilitation during pandemic.

Table 1 Interview sample questions.
Data were appraised for normality of distribution visually and formally (Shapiro Wilk test). Summary descriptive statistics are expressed as means [with standard deviation (SD)] or medians [with interquartile range (IQR)] for normally and non-normally distributed continuous variables, respectively, and as total numbers (with proportions) for categorical variables. Comparisons were assessed by t-test, Mann–Whitney U-test or Chi-square tests, as appropriate.
Possible predictors of COVID-19 scales scores (i.e., CAS, OCS and CSS) were analysed using ordered logistic regression models given the ordered non-interval responses scorings on individual items and assuming proportional odds (formally tested with the Brant test). Ordered regression null mixed-model was fit for interclass coefficient appraisal of possible significant difference between centres, suggesting <2% variation in COVID-19 scales scores was attributable to recruitment centre. COVID-19 multivariate ordered logistic regression model was then fitted with data for the overall population to assess the impact of the total number of comorbidities and social characteristics, and HADS scores on the total CAS, OCS and CSS scores. Statistical significance was set at two-tailed p < 0.05. Statistical analyses were performed with Stata/IC 14.2 for Mac (StataCorp, College Station, TX, USA).
Interviews were audiotaped and transcribed verbatim. The transcripts were analysed using content analysis (32, 33) as previously described (31), consisting of line-by-line coding and grouping codes into larger categories. Transcripts were independently reviewed by 3 investigators (D.S., N.S., J.F.). After an initial reading of all available transcripts, relevant parts were extracted and preliminarily coded (i.e., given descriptive labels). According to similarities and differences the codes were grouped into the higher order meaning units (subcategories) and named using words that characterize their content. These were organized into core categories. Identification of new contents and inconsistencies in the coding scheme were discussed by a research team and the coding scheme was adapted accordingly. Double-coding of some interviews (n = 7) was used to test interrater agreement.
In total, 109 patients after AMI, all after percutaneous coronary intervention with stenting, were included in a quantitative cross-sectional study during their attendance of cardiac rehabilitation program (49 in General Hospital Murska Sobota and 60 in University Medical Centre Ljubljana, mean age 59 ± 10 years, 20% women) – Table 2. There were no significant differences between the two centers, except in some socioeconomic determinants of health and prevalence of reported comorbidity. All patients were vaccinated during the cardiac rehabilitation unless there were medical or personal constraints against it.
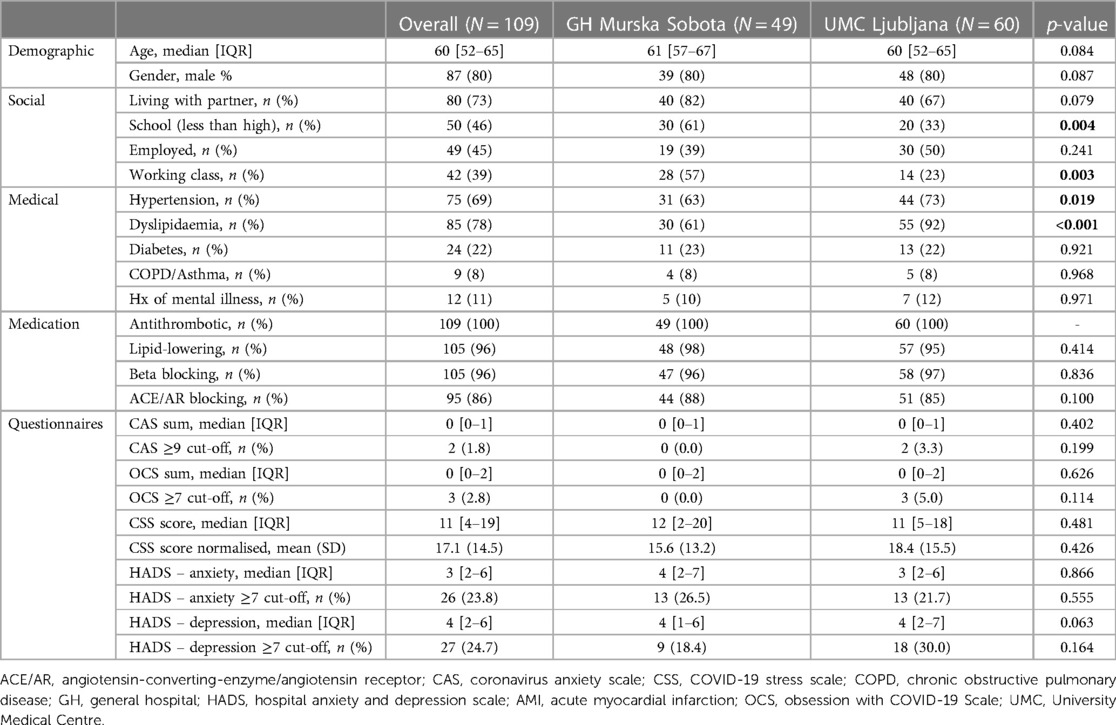
Table 2 Characteristics of study participants.
Twentyseven (25%) and twentysix (24%) patients reached the value that more likely indicates depression or anxiety on the HADS questionnaire. An OCS total score of ≥7 was observed in 3 patients (3%) to indicate probable dysfunctional thinking about COVID-19; a CAS total score of ≥9 was observed in 2 patients (2%) to indicate probable dysfunctional coronavirus-related anxiety.
Based on CSS questionnaire results, the level of stress about the COVID-19 among patients attending cardiac rehabilitation program was not high (Figure 1). Patients were most often afraid of getting infected (60%) and had worries about COVID-19 vaccines safety (60%).
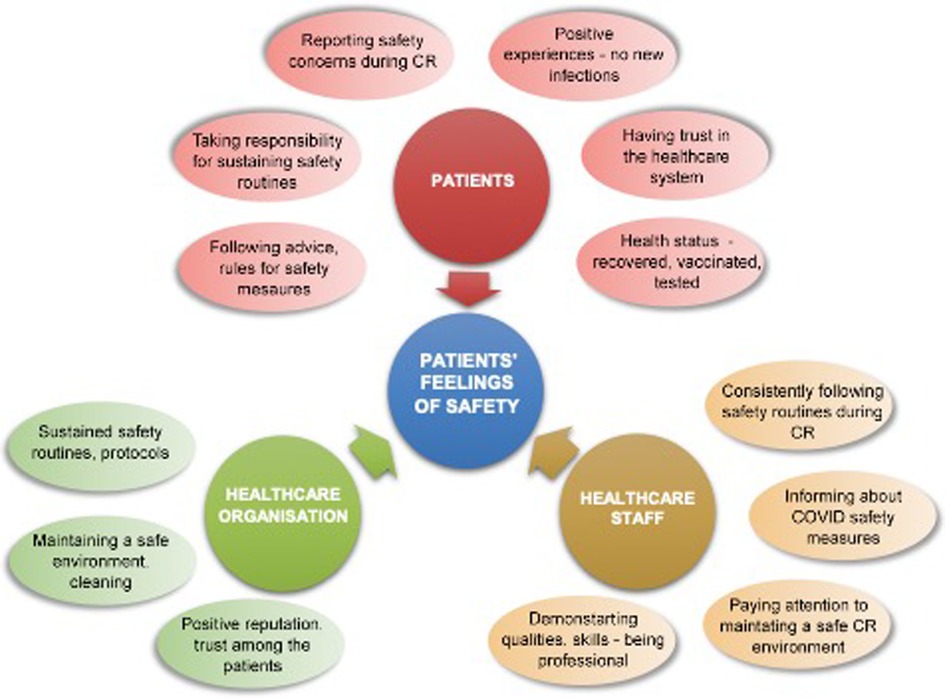
Figure 1 The COVID-19 stress scale (CSS). For items 1–13: How often have you experience following kinds of worries during the last month? 0 (Not at all), 1 (Slightly), 2 (Moderately), 3 (Extremely), 4 (Very often).For items 14–19: During the past month, how much have you done the following because of concerns about COVID-19? 0 (Never), 1 (Rarely), 2 (Sometimes), 3 (Often), 4 (Almost always).
CAS and OCS scale results (Figures 2, 3) show that patients most often expressed fear of meeting an infected person (30%) and reported sleep problems due to thinking about the coronavirus (15%).
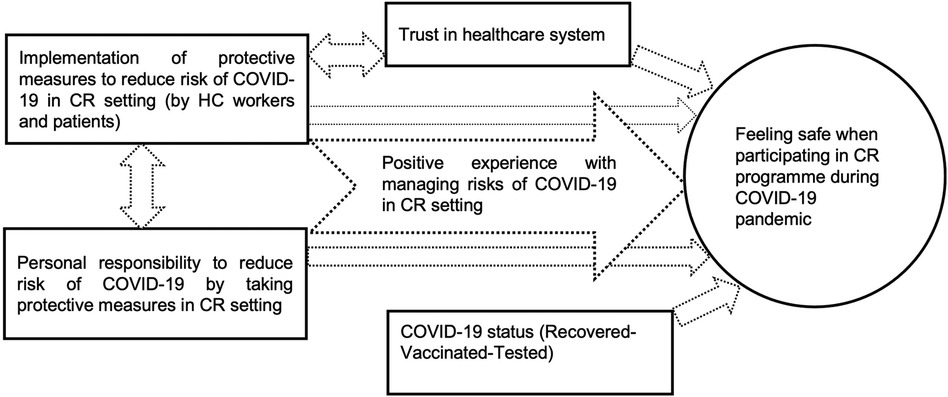
Figure 2 The coronavirus anxiety scale (CAS). How often have you experienced the following activities over the last 2 weeks? 0 (Not at all), 1 (Rare, less than a day or two), 2 (Several days), 3 (More than 7 days), 4 (Nearly every day over the last 2 weeks).
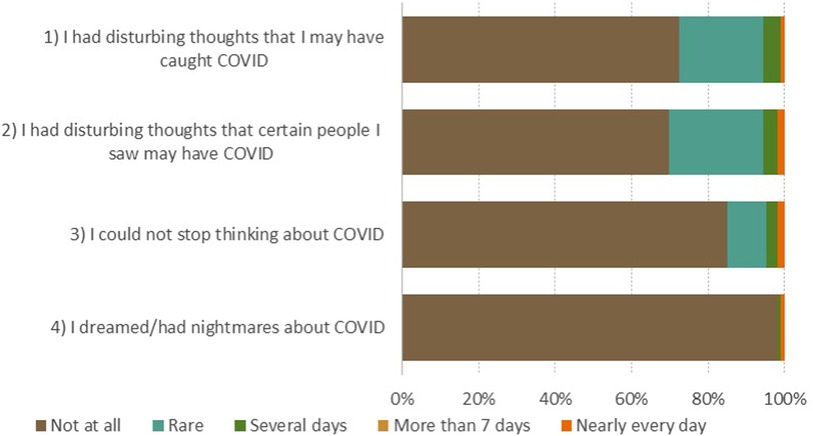
Figure 3 The obsession with COVID-19 scale (OCS). How often have you experienced the following activities over the last 2 weeks? 0 (Not at all), 1 (Rare, less than a day or two), 2 (Several days), 3 (More than 7 days), 4 (Nearly every day over the last 2 weeks).
Thirty patients after AMI (15 in General Hospital Murska Sobota and 15 in University Medical Centre Ljubljana) were interviewed in qualitative study of the project. Patients were 59 ± 12 years old, 30% women, 40% employed, majority were living with partner (67%) and 60% had less than high school education (Table 3).
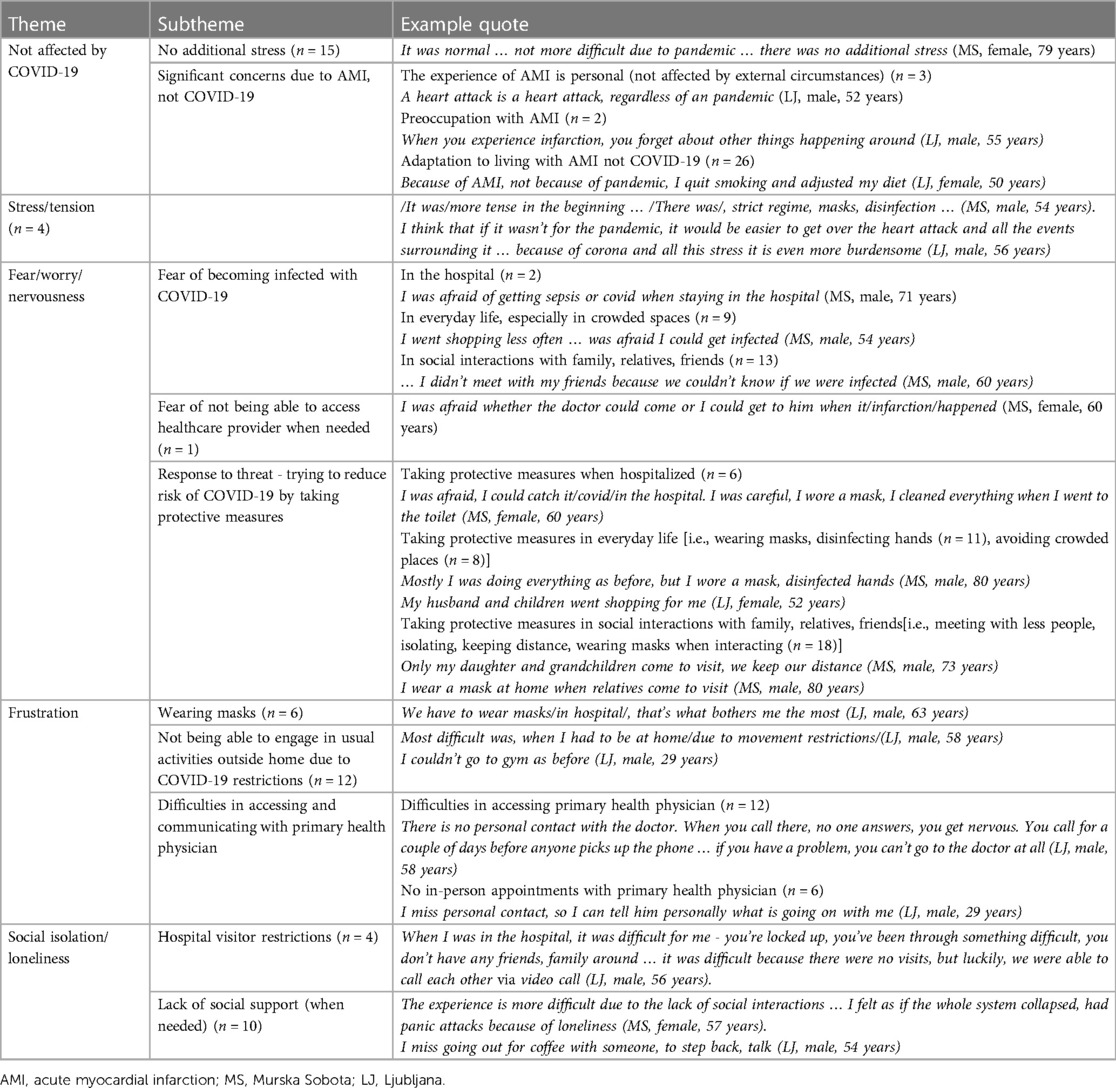
Table 3 Psychological experience of COVID-19 pandemic on acute myocardial infarction experience.
Generally seen, patients attending the interview were similar to others (p > 0.1) in all characteristics except for diagnosed hypertension (53% vs. 75%, p = 0.032) and dyslipidemia (90% vs. 73%, p = 0.063) – see Supplementary Table S1. There were also no differences when comparing CAS, OCS, CSS scores and HADS questionnaire. However, more patients who were not interviewed had HADS score indicative of anxiety and depression.
The interviews yielded two overarching domains: general psychological experience of AMI during the pandemic and psychological experience when visiting cardiac rehabilitation during the pandemic.
Five major themes, capturing general psychological experience of AMI during the pandemic, emerged from the analysis of interviews: Not affected by COVID-19, Stress/tension, Fear/worry/nervousness, Frustration, Social isolation/loneliness (see Table 3 for themes, subthemes and example quotes).
Patients generally expressed they were not affected by COVID-19. However, emotions that were most experienced during the COVID-19 pandemic were fear, worry, nervousness; participants worried about being infected with COVID-19 and of not being able to access healthcare provider when needed. In response to the threat of COVID-19 infection they tried to reduce its risk by taking protective measures. Some noted that COVID-19 pandemic presented and additional stress during their AMI experience. Frustration due to mandatory masks, limitations due to COVID-19 restrictions and difficulties in assessing primary health physicians was also mentioned. Another negative aspect during patients' AMI experience was feeling of social isolation in the hospital due to hospital visitor restrictions and lack of social support.
When asked about their experience in cardiac rehabilitation program during COVID-19 pandemic majority of patients (n = 28) reported they had little or no health-related concerns when participating in the program. Some of them noted (n = 6) they experienced some fear of COVID-19 infection before or at the beginning of the program.
Content analysis of interviews revealed five major themes of factors, contributing to patients' feeling of safety when participating in cardiac rehabilitation program during COVID-19 pandemic: Implementation of protective measures to reduce risk of COVID-19 by healthcare workers and patients in cardiac rehabilitation setting, Personal responsibility to reduce risk of COVID-19 by taking protective measures in cardiac rehabilitation setting, Positive experience with managing risks of COVID-19 in cardiac rehabilitation setting, Trust in healthcare system/workers, COVID-19 status (Recovered-Vaccinated-Tested) (see Table 4, Figure 4).
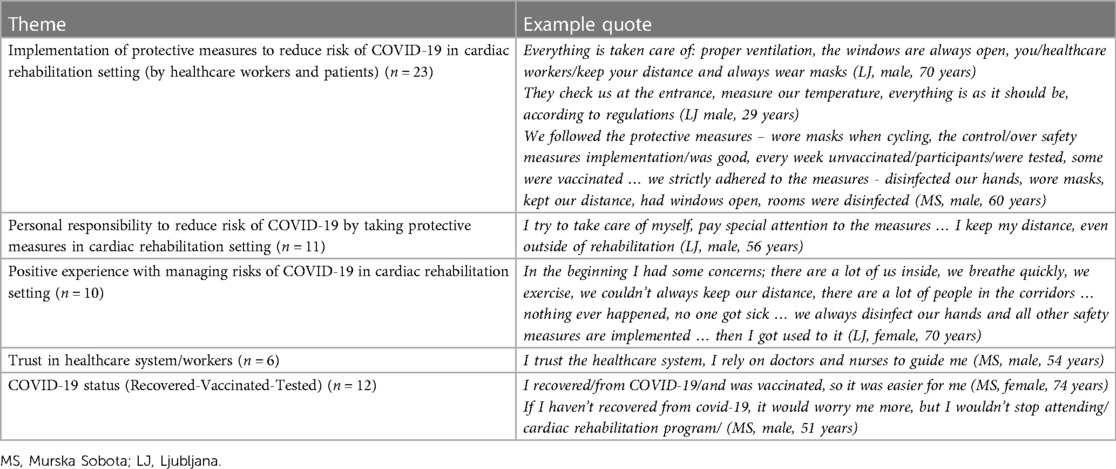
Table 4 Exploring COVID-19 related factors contributing to patients’ feeling of safety when participating in cardiac rehabilitation program during COVID-19 pandemic.
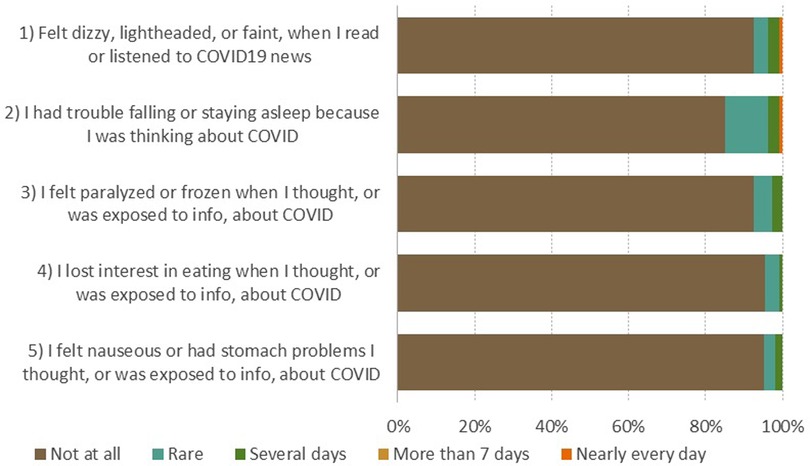
Figure 4 Factors contributing to patients’ feeling of safety when participating in cardiac rehabilitation programme during COVID-19 pandemic identified in the qualitative analysis.
Figure 4 shows the importance of positive experience with managing risks of COVID-19 in cardiac rehabilitation setting that can be established through the implementation of effective infection protective measures (by healthcare workers and participants) and supporting personal responsibility of patients to reduce risk of COVID-19.
Figure 5 organizes experiences that contributed to patients' feelings of safety when attending cardiac rehabilitation programme during COVID-19 pandemic into characteristics of patients, healthcare staff and healthcare organisations.
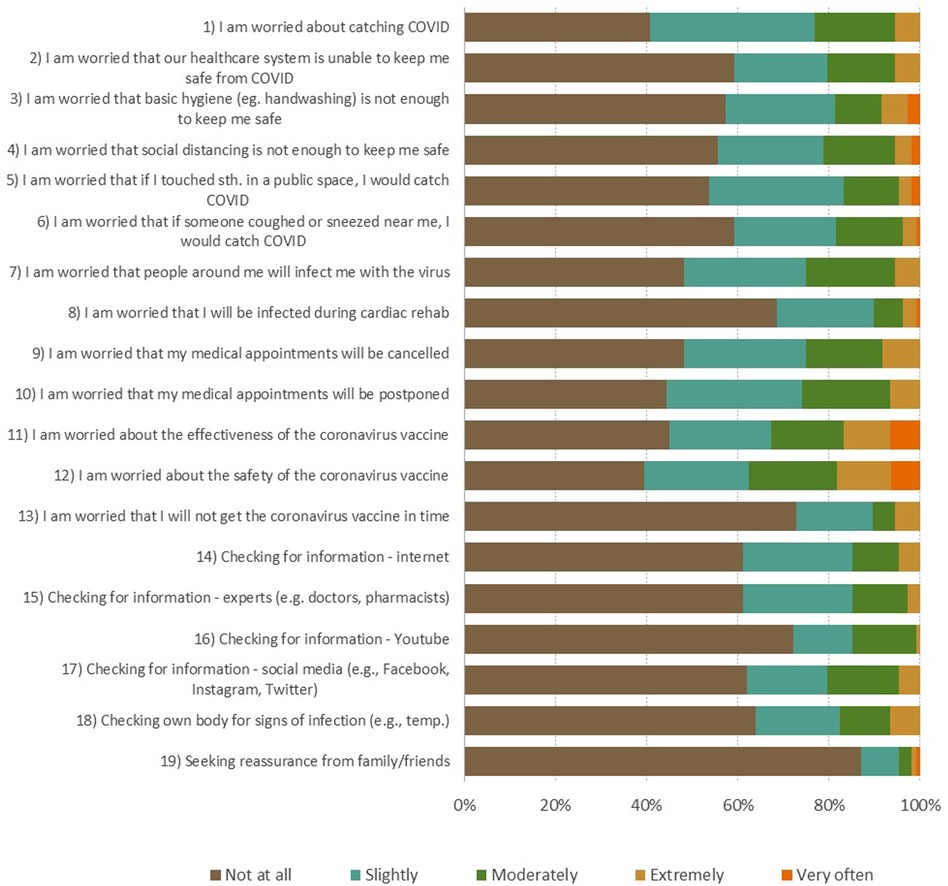
Figure 5 Characteristics of patients, healthcare staff and healthcare organisations that made cardiac rehabilitation patients feel safe during COVID pandemic.
In our quantitative and qualitative study about patient psychological well-being, personal experience, and trust in the health-care system in patients after myocardial infarction who attended the outpatient cardiac rehabilitation during COVID-19 pandemic at its peak and lockdown, the reported levels of pandemic related discomfort were relatively low and mostly related to fear of infection and vaccine safety. When analysed in-depth during structured interviews, patients perceived the cardiac rehabilitation program itself as well as health care provider delivery of care as safe, trustworthy and with enough support to avoid or manage COVID-19 health risks.
COVID-19 pandemic and lockdown reduced the delivery of healthcare services in Europe, including access to cardiac rehabilitation (9). In Slovenia, severe restrictions at large as elsewhere were adopted thus only 2 out of 8 cardiac rehabilitation centres were able to meet the required standards and had no interruption in their service. Although the number of patients receiving cardiac rehabilitation was strikingly reduced, the general characteristics were comparable to previous years in Slovenia (8). Both patients and health care providers needed to follow several restrictions in a strict manner that were implemented through medical and governmental authorities. Such restrictions in daily life can result in negative connotation and experience related to healthcare service. As global pandemic started abruptly, there were no specific instruments to address patient needs, experiences and attitudes. The general instruments were initially used while specific instruments were developed at different pace and with different scientific scrutiny. When we conceived this study, only few specific instruments for general population or patients were available therefore we used them along with some established ones to assess these aspects (22–24). As used instruments render quantitative data only, we have additionally performed the interviews in a qualitative study to gain further insights into specific individual characteristics and needs that are beyond the quantitative research. Similar approaches were used previously and also during the COVID-19 pandemics.
To best of our knowledge, the CAS, CSS and OCS were not used in cardiac patients. In fact, only few studies investigated depression and anxiety in cardiac rehabilitation setting during COVID-19 pandemic. According to REACH-HF investigators who focused on heart failure (34), COVID-19 apparently resulted in more anxiety and depression symptoms as assessed by HADS questionnaire. When compared to our results, the average scores in REACH-HF were higher which could also be related to previous observations that patients with heart failure generally have more anxiety and depression than those post myocardial infarction (35). When our findings are compared to previous studies in acute myocardial infarction (36), the psychosocial stress levels were higher than in control subjects but remarkably similar to ours which may reflect that myocardial infarction remained primary patient concern even under COVID-19 pandemic related measures.
With several questionnaires used, we are able to complement the current literature. In our study, patients after AMI expressed low levels of COVID-19 related stress, anxiety and/or obsessive thinking. All measures were associated with general anxiety scores on the HADS-anxiety sub-score domain, but not with demographic, clinical, or socioeconomic characteristics. Regardless, we must highlight those concerns that patients most often reported in connection to COVID-19. On CSS questionnaire, almost two thirds of patients reported worries about COVID-19 vaccines safety and fear of getting infected. Similarly, on OCS questionnaire 30% of patients reported that they had disturbing thoughts that certain people they saw may have the coronavirus. Based on that, it is not surprising that on CAS questionnaire 15% of patients indicated to had trouble falling or staying asleep because they were thinking about the coronavirus. To further appraise perceptions and experiences in patients undergoing centre-based cardiac rehabilitation during the COVID-19 pandemic, we conducted a qualitative study. Results offered insight into psychological experience when visiting cardiac rehabilitation during the COVID-19 pandemic as well as into more general psychological experience of AMI during the COVID-19 pandemic.
As individual experience and perception is relevant when exposed to new situation, the mixed-method with interviews enables us to get in-depth information about patient perception. Others also have used interviews in patients attending cardiac rehabilitation during COVID-19 pandemic yet they focused more on barriers against attendance, which generally were same as prior to pandemic (19, 37, 38). These studies specifically focused on alternatives to institution based cardiac rehabilitation as home based rehabilitation. Patients generally were supportive of this transfer yet additional support to keep motivation at adequate level (e.g., video conferencing, professional supervision) was needed to complete the rehabilitation programme, which can definitely be part of telerehabilitation during pandemics or as a regular service (39).
In our study, we did not have these challenges and patients generally did not report many COVID-19 related issues. A strong theme that however emerged from the data, were changes in psychological experience and lifestyle in relation to experienced myocardial infarction, regardless of COVID-19 pandemic. Similar significant impact of cardiovascular disease on psychosocial outcomes has also been widely noted in literature (40). However, participants in qualitative study noted the impact of their health situation and COVID-19 on fear of becoming infected, resulting in protective behaviour. Similarly, Mejdahl et al. (41) reported that chronic patients who felt they belonged to a particularly vulnerable high-risk group took many precautions with consequences for their everyday life and emotional well-being. We were able to identify factors arising from patients, healthcare staff and healthcare organisations, contributing to patients' feelings of safety when visiting cardiac rehabilitation during COVID-19 pandemic. This is of particular importance as patients needed to visit group rehabilitation sessions amid uncertainty in relation to COVID-19 regularly over a longer period. Sustained safety routines and protocols that are consistently followed by healthcare staff and patients, their mutual efforts to maintain a safe environment, including patients' possibility to report safety concerns, professionalism of healthcare workers, general trust in healthcare system, were identified. Similar safety-related factors arising from a range of care experiences in healthcare setting have been acknowledged by Barrow et al. (42). Our findings could form a basis for future healthcare in uncertain circumstances during pandemics, especially for chronic patients that need regular contact with healthcare system.
Our findings deserve to be interpreted with some caution. Firstly, the sample size may be considered as rather small but when compared to other studies in the field, we are well off in particular in qualitative aspect as our sample was larger than in others. Also, it needs to be pointed out that the study was conducted in all national cardiac rehabilitation centres that were open during the COVID-19 pandemic, which means that we have captured the maximum possible number of patients during pandemic. Secondly, the interviews were conducted between the second and third wave, when the number of patients with COVID-19 was relatively low, and we already had first experience with COVID-19 that might have had affected patient and healthcare professionals' behaviours during next waves. Thirdly, we have included only patients after AMI, which was due to limited cardiac rehabilitation network capacity and need to prioritize patients as per level of guideline recommendation (4, 43). Finally, the clinical diagnosis of anxiety or depression was not confirmed in full.
Patients reported that the acute myocardial infarction affected their lives more than the COVID-19 pandemic. Patients attending cardiac rehabilitation showed relatively low levels of stress and anxiety due to the COVID-19 pandemic. A higher level of stress, anxiety and obsessive thinking due to the coronavirus was detected in patients with a more pronounced level of anxiety, but not in connection with somatic indicators of cardiovascular disease. It was shown that the consistent implementation of measures to prevent infection in the medical institution, the participants' own concern for the implementation of preventive measures and positive experiences in managing the risks of infection significantly contributed to the feeling of safety when attending the cardiac rehabilitation program during the COVID-19 pandemic.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The study protocol was evaluated and approved by the National Medical Ethics Committee, no. KME 0120-557/2021/3, and the study was conducted in accordance with the Declaration of Helsinki. All participants gave their written informed consent for participation in the study prior to any study related procedure.
BJ: Conceptualization, Data curation, Investigation, Methodology, Supervision, Writing – original draft, Writing – review & editing. NK: Conceptualization, Investigation, Software, Writing – review & editing. DS: Data curation, Investigation, Methodology, Writing – review & editing. ML: Conceptualization, Data curation, Writing – original draft, Writing – review & editing. JF: Conceptualization, Investigation, Supervision, Validation, Writing – original draft, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article.
This study was supported by the Slovenian Research and Innovation Agency and Republic of Slovenia Ministry of Health Grant V3-2104 “Secondary prevention and quality of care of myocardial infarction in Slovenian hospitals, and the impact of the COVID-19 pandemic on the management of atherosclerotic vascular disease”.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fcvm.2024.1373684/full#supplementary-material
Supplementary Table S1
Characteristics of participants.
1. Richardson C, Franklin B, Moy M, Jackson E. Advances in rehabilitation for chronic diseases: improving health outcomes and function. Br Med J. (2019) 365:I219131208954.
2. Ambrosetti M, Abreu A, Corrà U, Davos C, Hansen D, Frederix I, et al. Secondary prevention through comprehensive cardiovascular rehabilitation: from knowledge to implementation. 2020 update. A position paper from the secondary prevention and rehabilitation section of the European association of preventive cardiology. Eur J Prev Cardiol. (2021) 28(5):460–95.33611446
3. Taylor R, Dalal H, McDonagh S. The role of cardiac rehabilitation in improving cardiovascular outcomes. Nat Rev Cardiol. (2022) 19(3):180–94. doi: 10.1038/s41569-021-00611-7
4. Visseren F, Mach F, Smulders Y, Carballo D, Koskinas KC, Bäck M, et al. 2021 ESC guidelines on cardiovascular disease prevention in clinical practice: developed by the task force for cardiovascular disease prevention in clinical practice with representatives of the European Society of Cardiology and 12 medical societies with the special contribution of the European association of preventive cardiology (EAPC). Eur Heart J. (2021) 42(34):3227–337. doi: 10.1093/eurheartj/ehab484
5. Redfern J, Gallagher R, O’Neil A, Grace S, Bauman A, Jennings G, et al. Historical context of cardiac rehabilitation: learning from the past to move to the future. Front Cardiovasc Med. (2022) 9:842567. doi: 10.3389/fcvm.2022.842567
6. van Halewijn G, Deckers J, Yong Tay H, van Domburg R, Kotseva K, Wood D. Lessons from contemporary trials of cardiovascular prevention and rehabilitation: a systematic review and meta-analysis. Int J Cardiol. (2017) 232:294–303. doi: 10.1016/j.ijcard.2016.12.125
7. Kambic T, Šarabon N, Hadžić V, Lainscak M. Effects of high- and low-load resistance training in patients with coronary artery disease: a randomized controlled clinical trial. Eur J Prev Cardiol. (2022) 29(15):e338–42. doi: 10.1093/eurjpc/zwac063
8. Novaković M, Novak T, Vižintin Cuderman T, Krevel B, Tasič J, Rajkovič U, et al. Exercise capacity improvement after cardiac rehabilitation following myocardial infarction and its association with long-term cardiovascular events. Eur J Cardiovasc Nurs. (2022) 21(1):76–84. doi: 10.1093/eurjcn/zvab015
9. Ghisi G, Xu Z, Liu X, Mola A, Gallagher R, Babu A, et al. Impacts of the COVID-19 pandemic on cardiac rehabilitation delivery around the world. Glob Heart. (2021) 16(1):43. doi: 10.5334/gh.939
10. Ambrosetti M, Abreu A, Cornelissen V, Hansen D, Iliou MC, Kemps H, et al. Delphi consensus recommendations on how to provide cardiovascular rehabilitation in the COVID-19 era. Eur J Prev Cardiol. (2021) 28(5):541–57. doi: 10.1093/eurjpc/zwaa080
11. Kirwan R, de Heredia FP, McCullough D, Butler T, Davies IG. Impact of COVID-19 lockdown restrictions on cardiac rehabilitation participation and behaviours in the United Kingdom. BMC Sports Sci Med Rehabil. (2022) 14(1):67. doi: 10.1186/s13102-022-00459-5
12. Lindsey Anderson L, Sharp G, Norton RJ, Dalal H, Dean SG, Jolly K, et al. Home-based versus centre-based cardiac rehabilitation. Cochrane Database Syst Rev. (2017) 6(6):CD007130.28665511
13. O'Doherty AF, Humphreys H, Dawkes S, Cowie A, Hinton S, Brubaker P, et al. How has technology been used to deliver cardiac rehabilitation during the COVID-19 pandemic? An international cross-sectional survey of healthcare professionals conducted by the BACPR. BMJ Open. (2021) 11(4):e046051. doi: 10.1136/bmjopen-2020-046051
14. Secondary Prevention and Rehabilitation Section of the European Association of Preventive Cardiology. Recommendations on how to provide cardiac rehabilitation activities during the COVID-19 pandemic. In: Cardiology SPaRSotEAoP, editor. ESC Practice Tools. European Society of Cardiology (2020). Available online at: https://www.escardio.org/Education/Practice-Tools/CVD-prevention-toolbox
15. Howarth A, Munro M, Theodorou A, Mills P. Trends in healthcare utilisation during COVID-19: a longitudinal study from the UK. BMJ Open. (2021) 11:e048151.34330859
16. Khubchandani J, Kandiah J, Saiki D. The COVID-19 pandemic, stress, and eating practices in the United States. Eur J Investig Health Psychol Educ. (2020) 10(4):950–6.34542428
17. Flanagan EW, Beyl RA, Fearnbach SN, Altazan AD, Martin CK, Redman LM. The impact of COVID-19 stay-at-home orders on health behaviors in adults. Obesity. (2021) 29(2):438–45. doi: 10.1002/oby.23066
18. Mulugeta W, Desalegn H, Solomon S. Impact of the COVID-19 pandemic lockdown on weight status and factors associated with weight gain among adults in Massachusetts. Clin Obes. (2021) 11(4):e12453. doi: 10.1111/cob.12453
19. Kulnik S, Sareban M, Höppchen I, Droese S, Egger A, Gutenberg J, et al. Outpatient cardiac rehabilitation closure and home-based exercise training during the first COVID-19 lockdown in Austria: a mixed-methods study. Front Psychol. (2022) 13:817912. doi: 10.3389/fpsyg.2022.817912
20. Van Iterson E, Laffin L, Crawford M, Mc Mahan D, Cho C, Khot U. Cardiac rehabilitation is essential in the COVID-19 era: delivering uninterrupted heart care based on the Cleveland clinic experience. J Cardiopulm Rehabil Prev. (2021) 41(2):88–92. doi: 10.1097/HCR.0000000000000585
22. Lee S. Coronavirus anxiety scale: a brief mental health screener for COVID-19 related anxiety. Death Stud. (2020) 44(7):393–401. doi: 10.1080/07481187.2020.1748481
23. Lee S. How much “thinking” about COVID-19 is clinically dysfunctional? Brain Behav Immun. (2020) 67:97–8. doi: 10.1016/j.bbi.2020.04.067
24. Chaitanya Chandu V, Marella Y, Panga GS, Pachava S, Vadapalli V. Measuring the impact of COVID-19 on mental health: a scoping review of the existing scales. Indian J Psych Med. (2020) 42(5):421–7. doi: 10.1177/0253717620946439
25. Taylor S, Landry C, Paluszek M, Fergus T, McKay D, Asmundson G. Development and initial validation of the COVID stress scales. J Anxiety Disord. (2022) 7w:102232–9.32408047
27. Hu L, Bentler PM. Cutoff criteria for fit indexes in covariance structure analysis: conventional criteria versus new alternatives. Struct Eq Mod. (1999) 6:1–55.
28. Vučko Miklavčič I, Snoj Z, Mlakar J, Pregelj P. Validation of the Slovenian version of hospital anxiety and depression scale in female cancer patients. Psychiatr Danub. (2008) 20(2):148–5218587282.
29. Cosco T, Doyle F, Ward M, McGee H. Latent structure of the hospital anxiety and depression scale: a 10-year systematic review. J Psychosom Res. (2012) 72:180–4. doi: 10.1016/j.jpsychores.2011.06.008
30. Lemay K, Tulloch H, Pipe A, Reed J. Establishing the minimal clinically important difference for the hospital anxiety and depression scale in patients with cardiovascular disease. J Cardiopulm Rehabil Prev. (2019) 39(6):E9–11. doi: 10.1097/HCR.0000000000000379
31. Jamshed S. Qualitative research method-interviewing and observation. J Basic Clin Pharm. (2014) 5:87–8. doi: 10.4103/0976-0105.141942
32. Elo S, Kyngäs H. The qualitative content analysis process. J Adv Nurs. (2008) 62:107–15. doi: 10.1111/j.1365-2648.2007.04569.x
33. Hsieh H, Shannon S. Three approaches to qualitative content analysis. Qual Health Res. (2005) 15:1277–88. doi: 10.1177/1049732305276687
34. Daw P, Harrison A, Doherty PJ, van Zanten JJCSV, Dalal HM, Taylor RS, et al. A pragmatic effectiveness-implementation study comparing trial evidence with routinely collected outcome data for patients receiving the REACH-HF home-based cardiac rehabilitation programme. BMC Cardiovasc Disord. (2022) 22(1):270. doi: 10.1186/s12872-022-02707-5
35. Stauber S, Schmid JP, Saner H, Saner G, Grolimund J, von Känel R. A comparison of psychosocial risk factors between 3 groups of cardiovascular disease patients referred for outpatient cardiac rehabilitation. J Cardiopulm Rehabil Prev. (2012) 32(4):175–81. doi: 10.1097/HCR.0b013e31824cc1f7
36. Rosengren A, Hawken S, Ounpuu S, Sliwa K, Zubaid M, Almahmeed WA, et al. Association of psychosocial risk factors with risk of acute myocardial infarction in 11119 cases and 13648 controls from 52 countries (the INTERHEART study): case-control study. Lancet. (2004) 364:953–62. doi: 10.1016/S0140-6736(04)17019-0
37. Xie X, Chen Q, Liu H. Barriers to hospital-based phase 2 cardiac rehabilitation among patients with coronary heart disease in China: a mixed-methods study. BMC Nurs. (2022) 21(1):333. doi: 10.1186/s12912-022-01115-6
38. Vanzella LM, Ghisi GLM, Colella TJF, Larkin J, Vanderlei LCM, Marzolini S, et al. Physical activity level and perspectives of participants transitioning from onsite to virtual cardiac rehabilitation during the early COVID-19 pandemic: a mixed-method study. J Clin Med. (2022) 11:4838. doi: 10.3390/jcm11164838
39. Scherrenberg M, Wilhelm M, Hansen D, Voeller H, Cornelissen V, Frederix I, et al. The future is now: a call for action for cardiac telerehabilitation in the COVID-19 pandemic from the secondary prevention and rehabilitation section of the European association of preventive cardiology. Eur J Prev Cardiol. (2021) 28:524–40. doi: 10.1177/2047487320939671
40. Nwosu WO, Rajani R, Mcdonagh T, Driscoll E, Hughes LD. Patients’ and carers’ perspective of the impact of heart failure on quality of life: a qualitative study. Psychol Health Med. (2022) 27:1381–96. doi: 10.1080/13548506.2021.1922719
41. Mejdahl CT, Nielsen PB, Nielsen LA, Christensen AF, Nielsen BK. Experiences of being at high-risk during the COVID-19 pandemic and its impact on emotional well-being and daily life in people with chronic conditions: a qualitative study. J Patient Rep Outcomes. (2023) 7:62. doi: 10.1186/s41687-023-00607-6
42. Barrow E, Lear RA, Morbi A, Long S, Darzi A, Mayer E, et al. How do hospital inpatients conceptualise patient safety? A qualitative interview study using constructivist grounded theory. BMJ Qual Saf. (2023) 32:383–93. doi: 10.1136/bmjqs-2022-014695
43. McDonagh T, Metra M, Adamo M, Gardner RS, Baumbach A, Böhm M, et al. 2021 ESC guidelines for the diagnosis and treatment of acute and chronic heart failure: developed by the task force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). With the special contribution of the heart failure association (HFA) of the ESC. Eur J Heart Fail. (2022) 24:4–131. doi: 10.1002/ejhf.2333
Confirmatory factor analysis (CFA) was conducted to confirm the scale's factor structure in the Mplus 6 program22 using the WLSMV estimator. The following model fit indices were used besides the chi-square statistic (the approximate cut-off values and value-related references are in parentheses): RMSEA [<.06; (27)]; CFI [>.95, (27)], TLI [>.95; (27)], WRMR [<.90; (26)].
The proposed 3-factor model (danger/contamination fears, checking/reassurance seeking, health-care consequences) had a better model fit [χ2(149) = 424.7, P < .001; RMSEA = .13, 90% CI: .12–.15; CFI = .93; TLI = .92; WRMR = 1.40] compared with the unidimensional model (i.e., all 19 items loading on a single factor) and [χ2(152) = 658.9, P < .001; RMSEA = .18, 90% CI: .16–.19; CFI = .86; TLI = .85; WRMR = 1.87], with reliability coefficients alpha of the scales.92,.76 and.73, respectively. All factor loadings for the 3-factor model were greater than 0.50. However, in terms of goodness-of-fit indices the original 5-factor model (25) performed better (RMSEA = .05, 90% CI: .05–.05; SMRM = .04; CFI = .93).
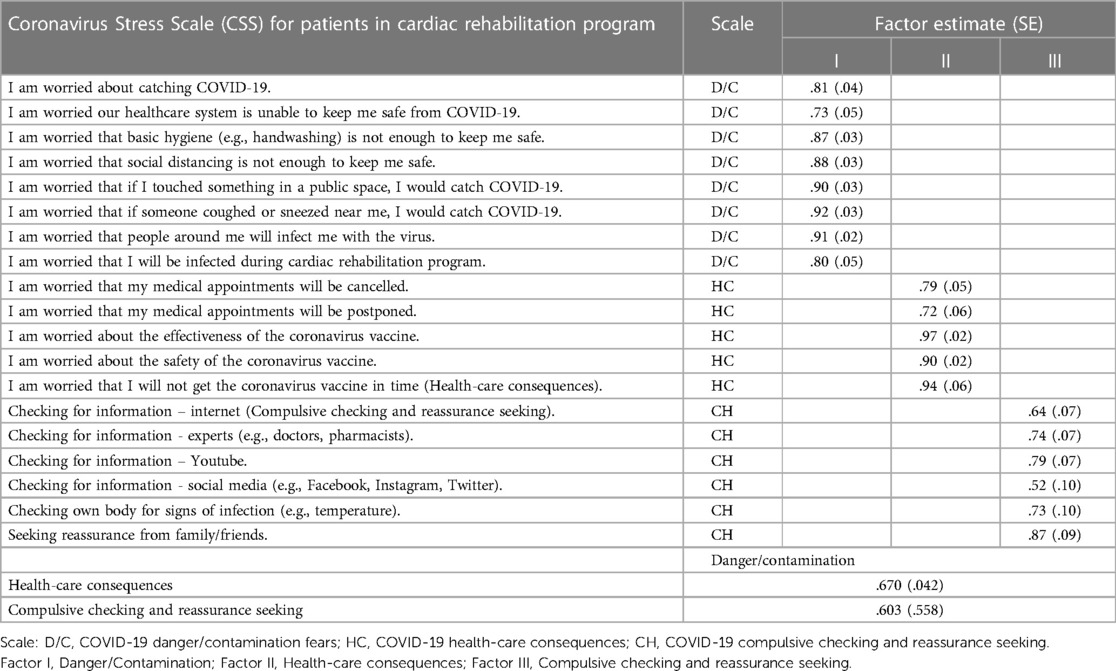
Table 1A Confirmatory factor analysis factor loading of the proposed CSS model.
Keywords: acute myocardial infarction, patients, cardiac rehabilitation, coronavirus disease, pandemic, psychological experience
Citation: Jug B, Sedlar Kobe N, Stojinic D, Lainscak M and Farkas J (2024) Cardiac rehabilitation patient perspectives during COVID-19 pandemic: quantitative and qualitative study. Front. Cardiovasc. Med. 11: 1373684. doi: 10.3389/fcvm.2024.1373684
Received: 20 January 2024; Accepted: 11 July 2024;
Published: 30 July 2024.
Edited by:
Otto Alexander Sanchez, Minneapolis Heart Institute Foundation (MHIF), United StatesReviewed by:
Tatjana Miljkovic, University of Novi Sad, Serbia© 2024 Jug, Sedlar Kobe, Stojnic, Lainscak and Farkas. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Borut Jug, Ym9ydXQuanVnQGtjbGouc2k=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.