
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Cardiovasc. Med. , 07 May 2024
Sec. Pediatric Cardiology
Volume 11 - 2024 | https://doi.org/10.3389/fcvm.2024.1341882
 Hoon Ko1
Hoon Ko1 Jinyoung Song2*
Jinyoung Song2* Sang Ah Chi3,4
Sang Ah Chi3,4 Sang-Yun Lee5Soo-Jin Kim6Chang-Ha Lee7Chun Soo Park8Eun Seok Choi8Hyo Soon An5
Sang-Yun Lee5Soo-Jin Kim6Chang-Ha Lee7Chun Soo Park8Eun Seok Choi8Hyo Soon An5 I. Seok Kang2Ja Kyoung Yoon6Jae-Suk Baek9Jae-Young Lee10
I. Seok Kang2Ja Kyoung Yoon6Jae-Suk Baek9Jae-Young Lee10 Joowon Lee11June Huh2Kyung-Jin Ahn12
Joowon Lee11June Huh2Kyung-Jin Ahn12 Se Yong Jung13Seul Gi Cha9Yeo-Hyang Kim14Young-Seok Lee15
Se Yong Jung13Seul Gi Cha9Yeo-Hyang Kim14Young-Seok Lee15
Introduction: The long-term effects of fenestration in patients with Fontan circulation remain unclear. We aim to evaluate the fenestration impact on early and late outcomes in patients with extracardiac Fontan (ECF) using a propensity score matching analysis.
Methods: We performed an extensive retrospective multicenter clinical data review of the Korean Fontan registry and included 1,233 patients with surgical ECF (779 fenestrated, 454 non-fenestrated). Demographics, baseline, and follow-up data were collected and comprehensively analyzed. Patients were divided into two groups according to the baseline presence or absence of surgical fenestration. Subsequently, patients were sub-divided according to the fenestration status at the last follow-up. Propensity-score matching was performed to account for collected data between the 2 groups using a multistep approach. The primary outcomes were survival and freedom from Fontan failure (FFF). We also looked at postoperative hemodynamics, cardiopulmonary exercise test results, oxygen saturations, and functional status.
Results: After propensity-score matching (454 matched pairs), there was no difference in survival or FFF between the 2 groups. However, ECF patients with baseline fenestration had significantly lower oxygen saturation (p = 0.001) and lower functional status (p < 0.001). Patients with fenestration had significantly longer bypass times, higher postoperative central venous pressure, higher postoperative left atrial pressure, and less prolonged pleural effusion in the early postoperative period. The propensity score matching according to the fenestration status at the last follow-up (148 matched pairs) showed that patients with a persistent fenestration had significantly lower oxygen saturation levels (p < 0.001). However there were no intergroup differences in the functional status, survival and FFF.
Conclusions: Our results showed no long-term benefits of the Fenestration in terms of survival and FFF. Patients with persistent fenestration showed oxygen desaturation but no difference in exercise intolerance was shown between the 2 groups.
The original Fontan operation was described by Francis Fontan in 1971 for a patient with tricuspid atresia (TA) (1); since then, some modifications have been developed for a functional single ventricular heart. Extracardiac conduit Fontan (ECF) can be fenestrated and not fenestrated, and fenestrated Fontan operations are now the most commonly used modifications. Owing to its simplicity and superior surgical outcomes (2–5), ECF has been accepted as the primary choice in Korea. However, controversy remains regarding fenestration. Fenestrated Fontan, which was first proposed for high-risk patients in 1990 (6), has demonstrated some benefits in terms of pleural drainage, hospital length of stay, and short-term morbidity (7, 8). However, it allows some degree of arterial desaturation and carries the possibility of systemic thromboembolism such as stroke (8). Thompson et al. concluded that fenestration was not necessary in all patients undergoing ECF (9). However, exercise intolerance in patients after ECF is well known (10, 11). Long-term Fontan-associated liver disease (FALD), a serious consequence after Fontan operation, has recently recognized after the Fontan operation (12–14). Fontan fenestration is expected to reduce pressure in the Fontan circuit and increase cardiac output by increasing the preload (9). These might be reasons why some still insist on fenestration in ECF. Previous studies assessing the necessity and impact of the fenestration were limited by their small number of patients and lack of randomization. The long-term effects of fenestration in patients with Fontan circulation remain unclear. Therefore, we aim to evaluate the fenestration impact on early and late outcomes in patients with ECF using a propensity score matching analysis.
For the study, we performed an extensive clinical data review of the Korean Fontan registry and included 1,233 patients with surgical ECF (779 fenestrated, 454 non-fenestrated). Demographics, baseline, and follow-up data were collected and comprehensively analyzed. The Korean Fontan registry is the first national multicenter registry for patients with congenital heart disease in Korea. The registry includes the medical records of all patients who underwent ECF surgeries between June 1988 and December 2019 in South Korea. The decision to fenestrate the ECF was made either systematically according to the institutional approach or by the team in charge according to each individual case. Patients were divided into two groups according to the baseline presence or absence of surgical fenestration. Subsequently, patients were sub-divided according to the fenestration status at the last follow-up. The primary outcomes were survival and freedom from Fontan failure (FFF). The study flow chart is summarized in patients who underwent ECF with or without surgical fenestration (Figure 1). We also looked at postoperative hemodynamics, cardiopulmonary exercise test results, oxygen saturations, and functional status at the last follow-up.
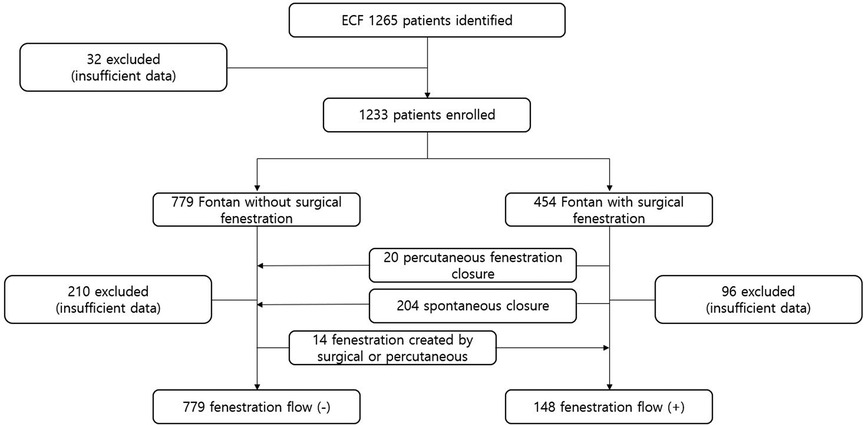
Figure 1. The study flow chart.
Transthoracic echocardiography (TTE) was used to evaluate the status of Fontan fenestration during follow-up. Early mortality was defined as death occurring within the first 30 postoperative days after Fontan surgery. Prolonged pleural drainage was defined as chest drainage for >14 days postoperative or readmission for pleural effusion. Fontan failure was defined as death, takedown, transplantation, or protein-losing enteropathy (PLE). Liver cirrhosis was defined as the advanced irreversible stage of progressive hepatic fibrosis characterized by distortion of hepatic architecture and formation of regenerative nodules (15). Clinically significant arrhythmia was defined as an arrhythmia requiring antiarrhythmic medication, cardioversion/defibrillation, or pacing devices. Heart failure was defined as presence of current or prior characteristic symptoms, such as dyspnea and fatigue, and evidence of ventricular dysfunction as a cause of these symptoms (16). Functional status was evaluated at every follow-up visit using the NYHA classification (17). Cardiopulmonary exercise test (CPET) was performed on a treadmill or on an ergometer cycle (18). Patients performed a symptom-limited maximal exercise test using an incremental protocol that allowed reaching exhaustion. Peak oxygen consumption (peak VO2) was defined as the maximal oxygen consumption.
All statistical analyses were performed using R statistical software (version 3.6.3; Foundation for Statistical Computing, Vienna, Austria). A two-sample t-test or Wilcoxon rank-sum test was used as appropriate to examine continuous variables. The χ2 test or Fisher's exact test was used to examine categorical variables. Categorical variables were reported as frequency and percentage and continuous variables were represented as median with interquartile range (IQR). Statistical analysis for continuous variables was conducted using the Mann–Whitney U-test. And for categorical variables, the χ2 test or Fisher's exact test was conducted. Statistical significance was set at a two-sided p-value < 0.05.
To reduce the effects of selection bias and confounding factors, we used propensity score matching to estimate the effects of baseline presence/absence of surgical fenestration and the fenestration status at the last follow-up using a multistep approach (19) (Supplementary Figure S1).
In first step, missing values were imputed using multiple imputation by chained equations to generate five imputed datasets (20). To predict each variable with missingness, the following variables were used in the imputation model: pre-Fontan pulmonary artery pressure, pre-Fontan transpulmonary pressure gradient (TPG), pre-Fontan pulmonary resistance (Rp). The distributions of these variables varied across the five imputed datasets.
Then, propensity score matching was applied within each imputed dataset using 1:1 nearest-neighbor matching without replacement in the second step (21). No caliper was applied. The propensity score was calculated using logistic regression with the following matching variables: gender, age at the time of the Fontan operation, TA, mitral atresia (MA), double-inlet left ventricle (DILV), unbalanced atrioventricular septal defect (AVSD), hypoplastic left heart syndrome (HLHS), prior shunt, prior banding, prior atrioventricular valve repair, prior total anomalous pulmonary venous return (TAPVR) repair, prior aortic arch repair, bilateral bidirectional cavopulmonary shunt (BCPS), pre-Fontan pulmonary artery pressure (PAP), pre-Fontan TPG, pre-Fontan Rp, and concomitant procedure during the Fontan operation. For each matched dataset, the absolute standard mean difference (ASMD) was computed to assess the balance of the variables used for matching and confirm whether the value of each variable was less than 0.2 with love plots. Group comparison was also compared using Wilcoxon signed-rank test for continuous variables and the McNemar test for categorical variables.
In third step, generalized linear models were used to determine the effect of having baseline fenestration or fenestration at the last follow-up in each matched dataset. Linear regression models, logistic regression models and cox regression models were used to calculate β estimates, odds ratios (ORs), and hazard ratios (HRs) with 95% confidence intervals (CIs) of having fenestration. Lastly, the results were pooled from five imputed datasets using Rubin's rules (22).
Among the enrolled cohort of Fontan survivors, the overall proportion of surgical fenestrations was 36.8% in 1988–2019 (Figure 2). After 2011, the proportion of Fontan procedures including surgical fenestration was approximately 40%. At the time of cross-sectional testing (median years after Fontan 12.8 years, IQR 5.4–18.1 years), the fenestration remained open in 41.3% (n = 148) of subjects.
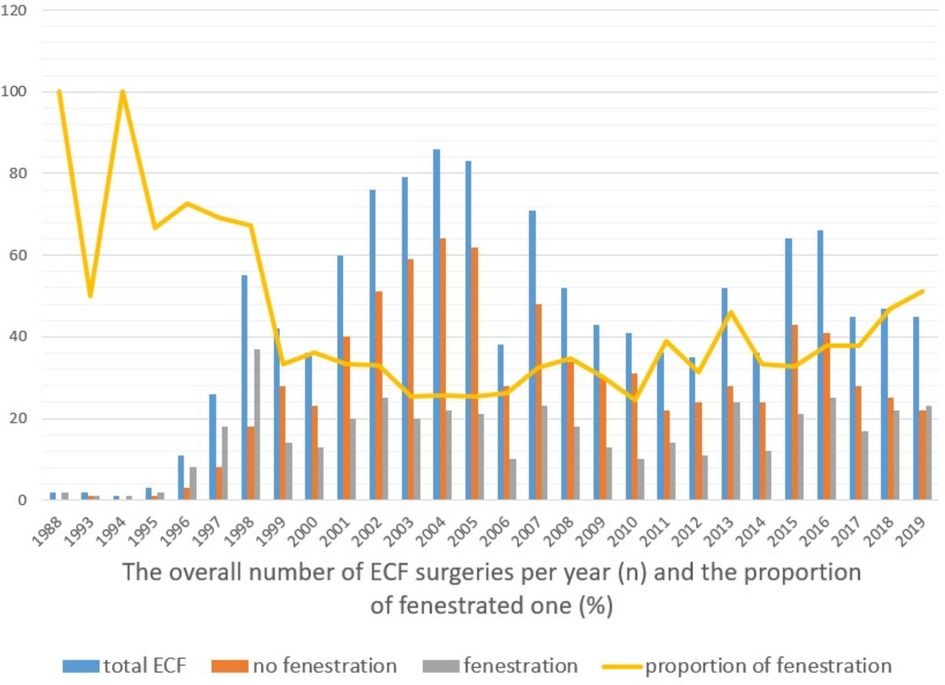
Figure 2. The overall number of ECF surgeries per year and the proportion of fenestrated one.
Among 1,233 patients with surgical ECF, there were 454 patients with baseline fenestration and 779 patients without baseline fenestration. The clinical, procedural, and follow-up characteristics in 1,233 patients were shown in Supplementary Tables S1–S3.
As there were 148 (12.0%), 339 (27.5%), and 313 (25.4%) missing values of the overall cohort for mean PAP, TPG, and Rp, respectively, we imputed these values by multiple imputation ad generated five imputed datasets. For each imputed dataset, 454 patients without baseline fenestration was matched with those with baseline fenestration (i.e., total of 908 patients in after-matched cohort). The 325 patients who were unmatched had significantly higher proportion of not having HLHS (p < 0.001), not having prior shunt (p < 0.001), and not having prior banding (p = 0.002) and not having concomitant procedure during Fontan operation (p < 0.001) and lower level of pre-Fontan PAP, pre-Fontan TPG, pre-Fontan Rp (all p < 0.001). The difference in these variables results into lower level of probability of getting baseline fenestration (i.e., propensity score), which would be a reason of being excluded from propensity score matching. After matching, all ASMDs for the matching variables were less than 0.2, which indicates well-balanced between two groups (Supplementary Figure S2).
The baseline demographics and clinical characteristics of the matched cohort are shown in Table 1. Among a total of 908 patients, there were 538 males (59.3%) with median age at Fontan of 3.2 years. Median duration from Fontan to last follow-up was 10.7 years (IQR 4.4–15.7 years). No significant difference in all variables were found between patients with and without fenestration.
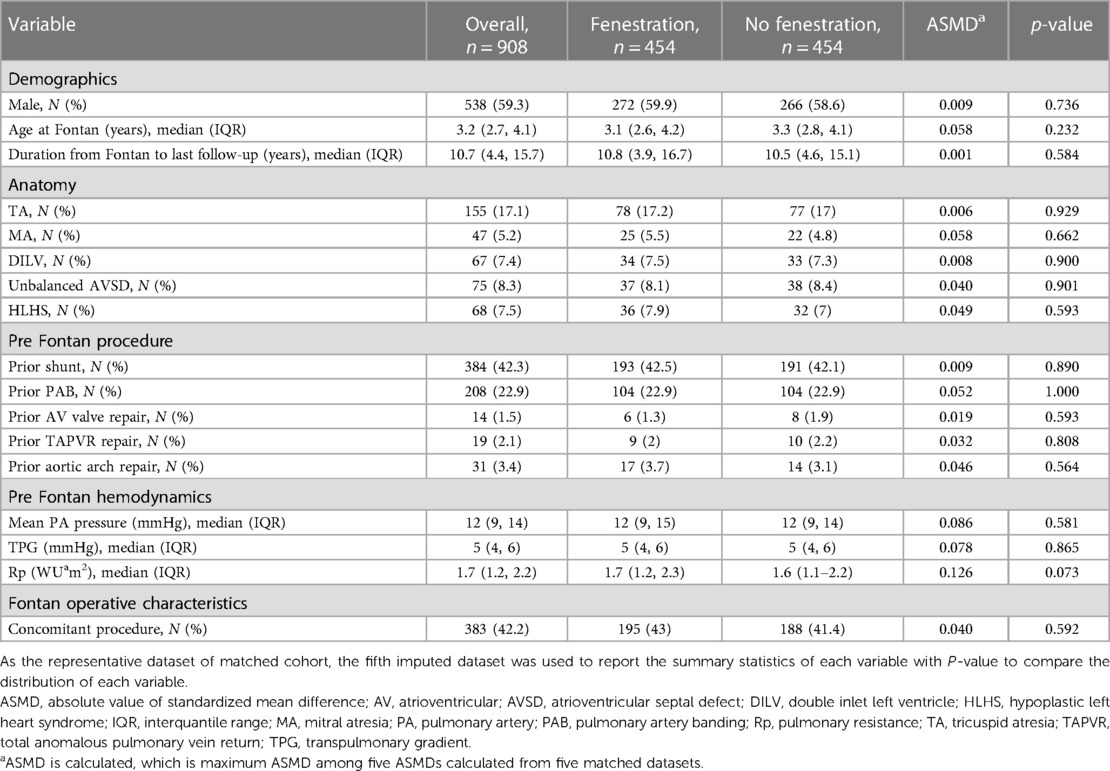
Table 1. Propensity score–matched 454 pairs according to baseline fenestration status.
Univariable and multivariable analyses for estimating the effect of baseline fenestration on operative, postoperative, follow-up outcomes were presented in Table 2. In univariable analyses, patients with fenestration had longer CPB time (β coefficient 25.592, 95% CI 16.962–34.222), higher post bypass CVP (β coefficient 0.733, 95% CI 0.221–1.244), higher post bypass LAP (β coefficient 3.119, 95% CI 0.68–5.558), less prolonged pleural effusion (OR 0.658, 95% CI 0.476–0.909) for operative and postoperative outcomes in the early postoperative period. For follow-up outcomes, higher NYHA class (OR 2.905, 95% CI 1.795–4.7 for 2 vs. 1 and OR 8.07, 95% CI 1.03–63.252 for 3 vs. 1) and lower oxygen saturation (β coefficient −2.379, 95% CI −3.451 to 1.307) were found to be significant in favor of ECF patients with fenestration. After adjusting all matching variables, having baseline fenestration was still significantly associated with these variables.
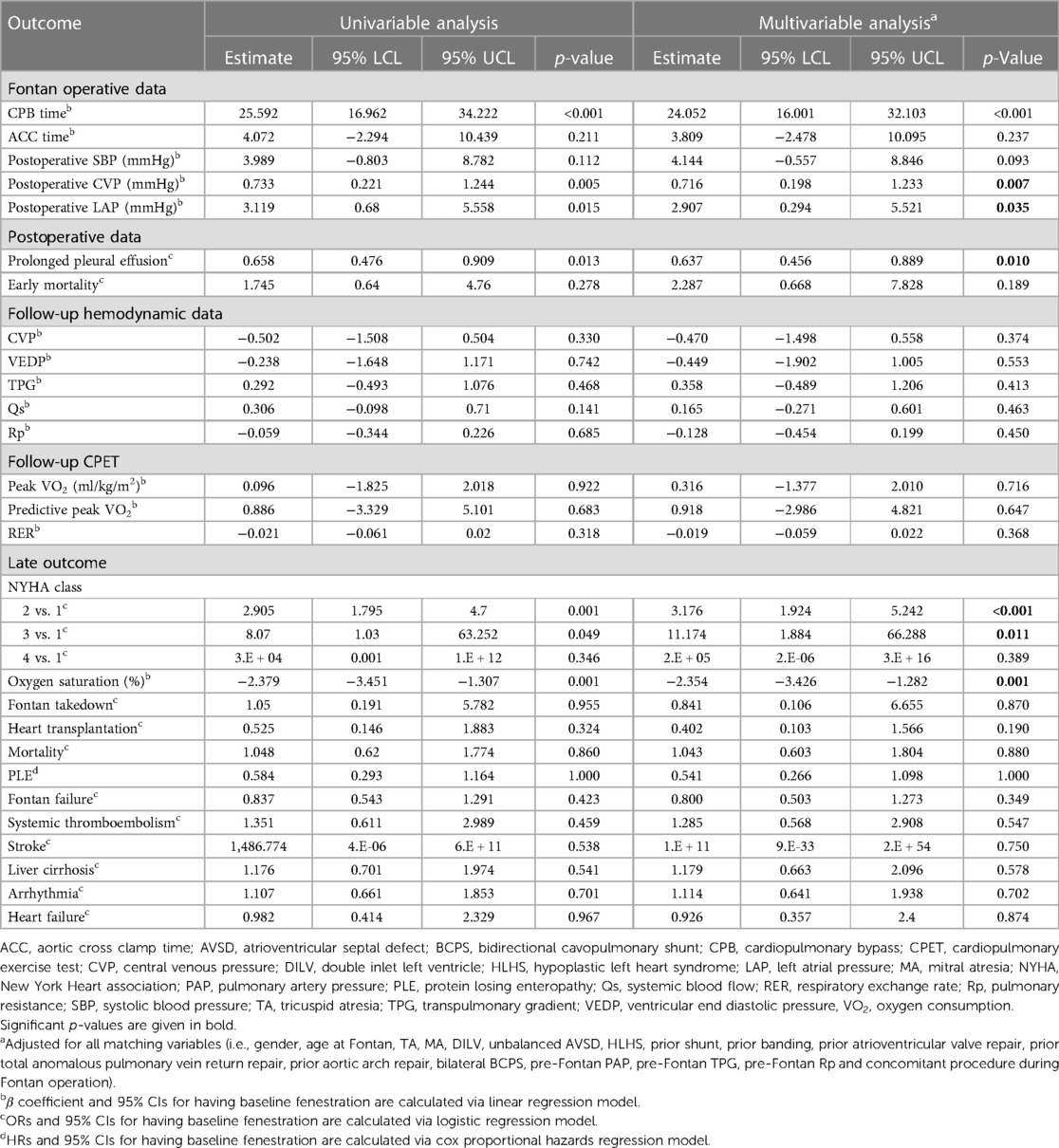
Table 2. The effect of baseline fenestration on various outcomes in the matched 454 pairs.
Out of 1,233 patients with 779 without surgical fenestration and 454 surgical fenestration, 210 and 96 patients were excluded for insufficiency of data. Then, 238 patients were also excluded from the analysis of fenestration status at last follow-up because of specific reasons below.
Among the patient underwent Fontan procedure with surgical fenestration (n = 454), excluding 96 patients with insufficient data, 5.6% (n = 20) underwent transcatheter fenestration closure with covered stents or closure devices. The following criteria were assessed to determine suitability for fenestration closure: an unobstructed Fontan pathway with no significant decompressing venovenous collaterals, baseline Fontan pressure <15 mmHg, baseline cardiac index >2l/min/m2, and decrease in cardiac index <20% with test occlusion of the fenestration (23).
If the parameters for closure suitability were met, the fenestration was closed. All children received prophylactic antibiotics and anticoagulant according to institutional protocol. After device closure, patients resumed routine anticoagulation or antiplatelet agent according to the primary cardiologist's preference.
Among the patient underwent Fontan procedure with surgical fenestration (n = 454), excluding 96 patients with insufficient data and 20 patient with transcatheter fenestration closure, 60.4% (n = 204) experienced apparent spontaneous closure at the last follow-up. As the current medications in patients who are being followed, most patients are taking anticoagulation and or antithrombotic regimen (overall cohort 94.7%, anticoagulation 38.3%, and antithrombotic regimen 59.6%).
Fourteen patients without initial surgical fenestration underwent surgical or percutaneous fenestration after the Fontan operation. Indications for recreated fenestration included severe chronic effusions or PLE.
With remained 927 patients with 148 patients (16%) for open fenestration, there were 102 (11.0%), 239 (25.8%), and 214 (23.1%) missing values of the overall cohort for mean PAP, TPG, and Rp, respectively. After multiple imputation for these missing values, 148 patients without fenestration at last follow-up were matched with those with fenestration with last follow-up for each imputed dataset (i.e., total of 296 patients in after-matched cohort). The 631 patients who were unmatched had significantly higher proportion of not having HLHS (p < 0.001), not having prior shunt (p < 0.001), not having prior banding (p = 0.002), not having prior TAPVR repair (p = 0.038) and not having concomitant procedure during Fontan operation (p < 0.001), and lower level of pre-Fontan TPG (p = 0.030) and pre-Fontan Rp (p < 0.001). The difference in these variables results into lower level of probability of getting fenestration at last follow-up (i.e., propensity score), which would be a reason of being excluded from propensity score matching. After matching, all ASMDs for the matching variables were less than 0.2, which indicates well-balanced between two groups (Supplementary Figure S3). The baseline demographics and clinical characteristics of the before-matched and after-matched cohorts are shown in Supplementary Table S4.
In before-matched group, there were significantly higher proportion of HLHS, prior shunt, and concomitant procedure and higher level of Rp in the open fenestration group. These results suggest that patients in the present fenestration flow group had higher disease severity at the time of the Fontan operation than those in the absent fenestration flow group. After propensity score matching, there were no significant difference in all variables including HLHS, prior shunt, Rp, and concomitant procedure. The follow-up characteristics for after-matched cohort were presented in Table 3. Only oxygen saturation level was significantly different between open fenestration and no fenestration groups.
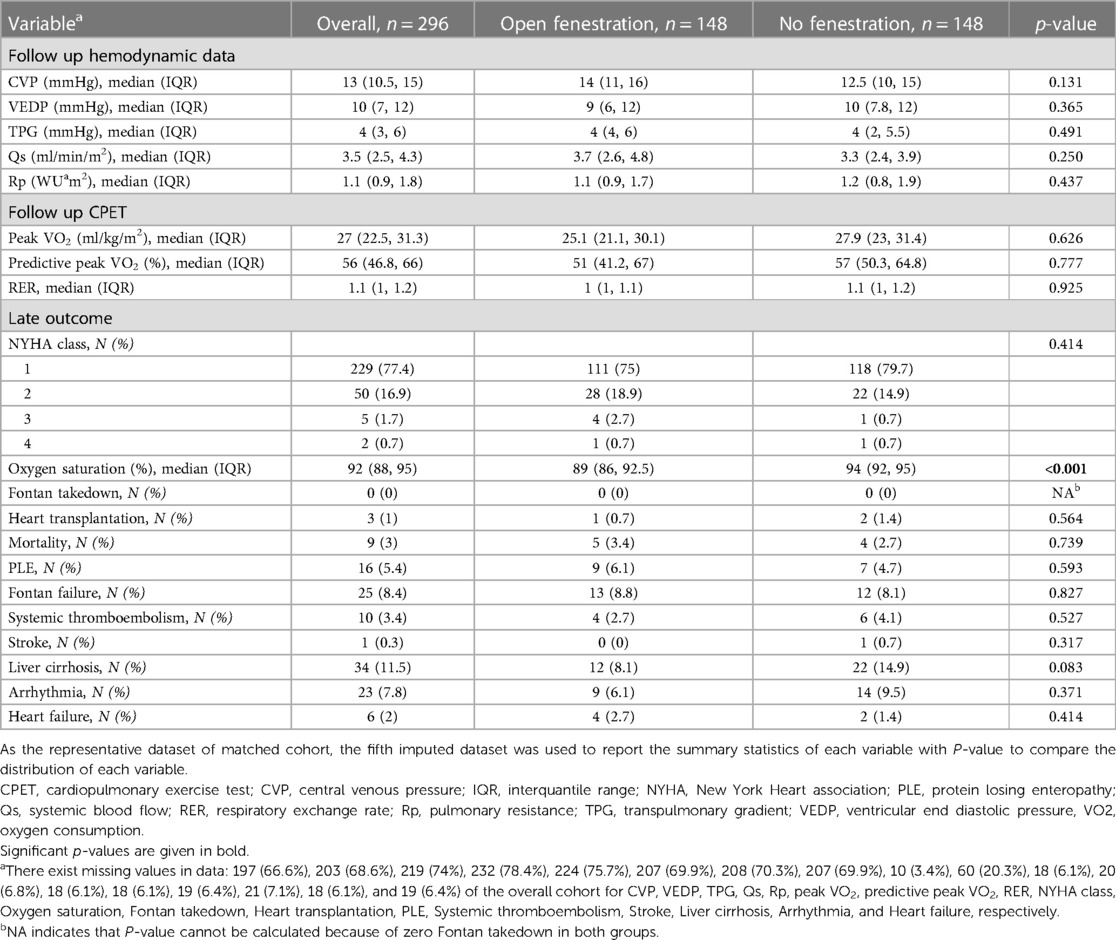
Table 3. Propensity score–matched 148 pairs according to fenestration status at last follow-up.
Univariable and multivariable analyses for estimating the effect of fenestration at last follow-up on follow-up outcomes were presented in Table 4. In univariable analyses, patients with fenestration at last follow-up had lower oxygen saturation level (β coefficient −4.073, 95% CI −5.311 to 2.836). After adjusting all matching variables, having fenestration at last follow-up was still significantly associated with lower oxygen saturation level (β coefficient −4.247, 95% CI −5.552 to 2.942). Other variables showed no significant association with fenestration at last follow-up.
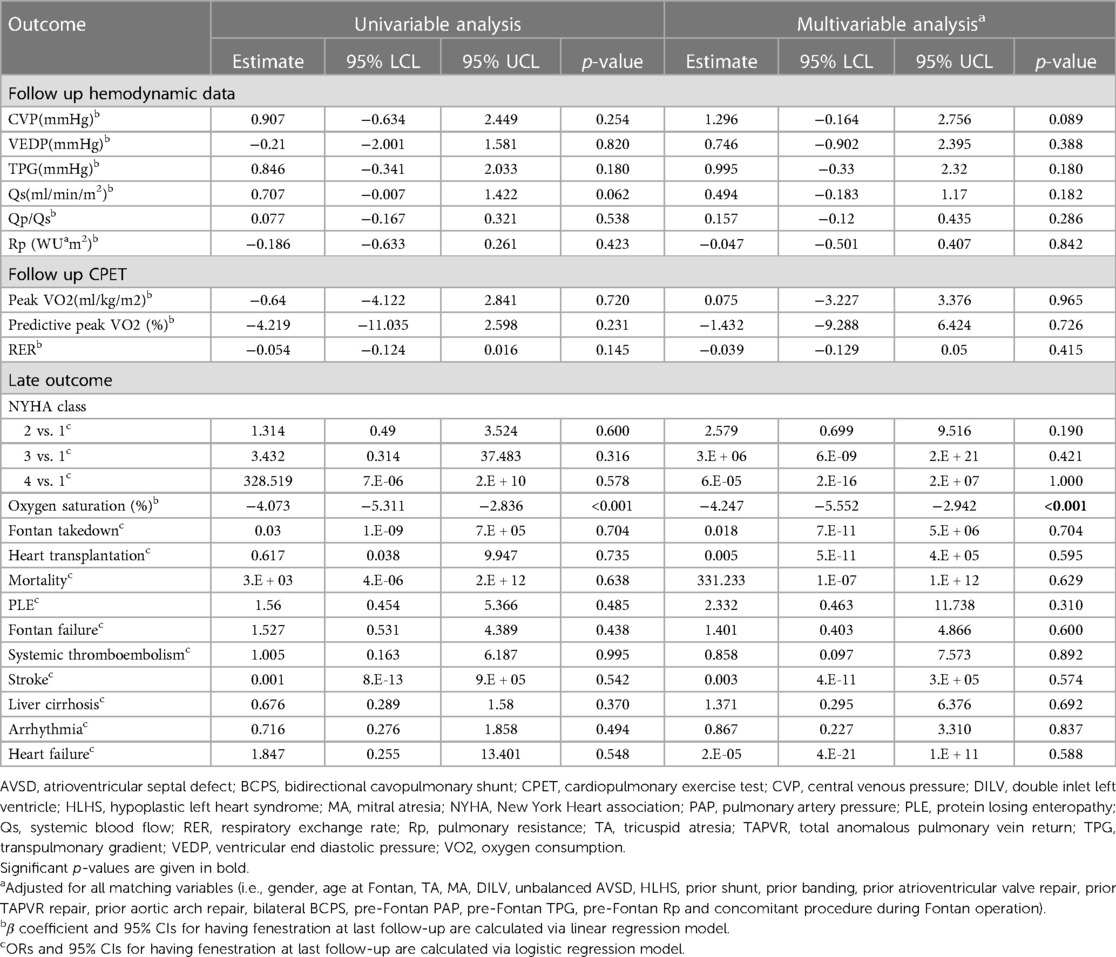
Table 4. The effect of fenestration at last follow-up on various outcomes in the matched 148 pairs.
The Korea Fontan registry is the first multicenter national registry of patients who underwent the Fontan operation in Korea. In our study, fenestration performed during ECF failed to provide any long-term benefits, including survival and Fontan failure, but led to systemic desaturation and a lower functional status. However, the benefits of early postoperative pleural drainage have been demonstrated. We observed that a considerable number of fenestrations closed spontaneously. Patients with persistent fenestration flow had no long-term benefits in terms of survival, FALD, exercise intolerance, and Fontan failure but had lower oxygen saturation than those without persistent fenestration flow.
Recently, a similar study of the Australia and New Zealand Fontan registry concluded that fenestration in the Fontan circulation had no early or long-term benefits but resulted in a higher incidence of thromboembolic events (24). In contrast to our study, the study of the ANZ Fontan registry included patients with lateral tunnel and ECF modifications, and it was unclear whether the fenestration represented persistent patent fenestration.
The early postoperative effect of fenestration reportedly reduces the length of hospital stay and duration of pleural drainage (8, 25–28). However, several studies demonstrated excellent outcomes without fenestration and improved oxygen saturation after fenestration (29–31). Therefore, fenestration should be limited to patients with high-risk Fontan circulation and enthusiastic transcatheter closure (9, 32). Still, there have been controversies on routine transcatheter closure of fenestration. Technically, transcatheter closure of fenestration in EC or lateral tunnel Fontan is not tricky. Not only various kinds of occlusive device but balloon expandable covered stent or self expanding graft stent have been used with good results (33–36). It has been reported improved systemic saturation and exercise capacity but no adverse events from several studies (29, 31, 37).
A few studies suggested that there may be some benefits to persistent fenestration. Saiki et al. demonstrated the chronic cardioprotective effect of persistent fenestration on long-term Fontan circulation (38). Greenleaf et al. reported a significant increase in Fontan pressure after fenestration closure (31), while Oka et al. reported that the absence of fenestration flow was a predictor of FALD (39).
A meta-analysis performed by Bouhout showed results very similar to those of our study, proving a shorter duration of pleural drainage but no long-term benefits (26). Unlike our study, another meta-analysis demonstrated no difference in oxygen saturation in patients with patent fenestration (40). Both analyses showed no long-term benefits or higher risk of stroke with fenestration (26, 40). Our patients with persistent fenestration had a lower oxygen saturation but no difference in exercise capacity and no history of stroke. Although the veno-venous collaterals (VVC) may affect systemic arterial desaturation, this study did not include an investigation into the prevalence and/or flow of the VVC.
There were changes in the tendency to perform fenestration during ECF. The lowest proportion of fenestrated ECF in Korea was 24.7% in 2004; this value gradually increased to 45.8% in 2018. The proportions of fenestrated ECF vs. non-fenestrated ECF differed among the participating institutes. There was only one institution performing routine Fontan perforations. The criteria for Fontan fenestration were not consistent as they differed according to the policies of each heart center. One of the main reasons for a consistent fenestrated ECF might be the concern of long-term Fontan failure, including FALD, although most studies to date failed to prove the long-term benefits of fenestration. Our data showed a 60.4% spontaneous closure rate of the initial fenestration. The spontaneous closure rate in our patients might be much higher than that reported by Gorla et al. (22%) (41) and hemodynamic data were not proven as significant factors for spontaneous closure in our analysis. However, fenestration type, size, and anticoagulation agents used are the most important factors. Owing to a lack of data, it was not possible to analyze these factors in our study.
The long-term incidence of systemic thromboembolic events in our analysis was lower than those in the ANZ Fontan registry (24). The definitions of systemic thromboembolic events differed between the two studies, and the lack of systemic screening for silent stroke in our study resulted in a lower stroke rate.
These retrospective studies including our study have their crucial limitations, so that a well-designed prospective study in homogenous group of patients should be conducted afterward. For a long-term effect, close observations with comprehensive evaluations for a long enough time are needed.
This study has limitations owing to its retrospective and multicenter design. The indication for Fontan fenestration, transcatheter fenestration closure and subsequent fenestration creation were not exactly consistent as they differed according to the policies of each heart center. The impact of a learning curve associated with surgical skills and postoperative care by individual surgeon and cardiologist may have affected the results of this study. This study is not an alternative to randomized control studies but is an important add-on to the literature.
Our results showed no long-term benefits of the Fenestration in terms of survival and FFF. Patients with persistent fenestration showed oxygen desaturation but no difference in exercise intolerance was shown between the 2 groups. ECF patients with baseline fenestration showed significantly reduced pleural drainage during the early postoperative period. Regarding the long-term effects of fenestrated ECF, our study showed similar findings to ECF patients with persistent fenestration but poorer functional class than those with baseline fenestration.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
HK: Writing – original draft, Investigation. JS: Conceptualization, Supervision, Writing – review & editing, Writing – original draft. SAC: Data curation, Formal Analysis, Methodology, Writing – original draft. S-YL: Investigation, Writing – review & editing. S-JK: Investigation, Writing – review & editing. C-HL: Investigation, Writing – review & editing. CP: Investigation, Writing – review & editing. EC: Investigation, Writing – review & editing. HA: Investigation, Writing – review & editing. IK: Investigation, Writing – review & editing. JY: Investigation, Writing – review & editing. J-SB: Investigation, Writing – review & editing. J-YL: Investigation, Writing – review & editing. JL: Investigation, Writing – review & editing. JH: Investigation, Writing – review & editing. K-JA: Investigation, Writing – review & editing. SJ: Investigation, Writing – review & editing. SGC: Investigation, Writing – review & editing. Y-HK: Investigation, Writing – review & editing. Y-SL: Investigation, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article.
This research was supported and funded by SNUH Lee Kun-hee Child Cancer & Rare Disease Project, Republic of Korea (grant number: 23C-030-00400).
We are grateful to all patients for their cooperation during the study and the collaborating investigators of Korean Fontan Registry for their contributions.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fcvm.2024.1341882/full#supplementary-material
1. Fontan F, Baudet E. Surgical repair of tricuspid atresia. Thorax. (1971) 26(3):240–8. doi: 10.1136/thx.26.3.240
2. Backer CL, Deal BJ, Kaushal S, Russell HM, Tsao S, Mavroudis C. Extracardiac versus intra-atrial lateral tunnel fontan: extracardiac is better. Semin Thorac Cardiovasc Surg Pediatr Card Surg Annu. (2011) 14(1):4–10. doi: 10.1053/j.pcsu.2011.01.019
3. Daley M, d'Udekem Y. The optimal Fontan operation: lateral tunnel or extracardiac conduit? J Thorac Cardiovasc Surg. (2021) 162(6):1825–34. doi: 10.1016/j.jtcvs.2020.11.179
4. Tireli E, Ugurlucan M, Basaran M, Kafali E, Harmandar B, Sayin OA, et al. Extracardiac Fontan operation without cardiopulmonary bypass. J Cardiovasc Surg (Torino). (2006) 47(6):699–704.17043618
5. Rajab TK, Jaggers J. Extracardiac Fontan operation: how I teach it. Ann Thorac Surg. (2020) 110(4):1119–22. doi: 10.1016/j.athoracsur.2020.06.014
6. Bridges ND, Lock JE, Castaneda AR. Baffle fenestration with subsequent transcatheter closure. Modification of the Fontan operation for patients at increased risk. Circulation. (1990) 82(5):1681–9. doi: 10.1161/01.CIR.82.5.1681
7. Bridges ND, Mayer JE Jr, Lock JE, Jonas RA, Hanley FL, Keane JF, et al. Effect of baffle fenestration on outcome of the modified Fontan operation. Circulation. (1992) 86(6):1762–9. doi: 10.1161/01.CIR.86.6.1762
8. Lemler MS, Scott WA, Leonard SR, Stromberg D, Ramaciotti C. Fenestration improves clinical outcome of the fontan procedure: a prospective, randomized study. Circulation. (2002) 105(2):207–12. doi: 10.1161/hc0202.102237
9. Thompson LD, Petrossian E, McElhinney DB, Abrikosova NA, Moore P, Reddy VM, et al. Is it necessary to routinely fenestrate an extracardiac fontan? J Am Coll Cardiol. (1999) 34(2):539–44. doi: 10.1016/S0735-1097(99)00228-4
10. Tran DL, Gibson H, Maiorana AJ, Verrall CE, Baker DW, Clode M, et al. Exercise intolerance, benefits, and prescription for people living with a fontan circulation: the Fontan fitness intervention trial (F-FIT)-rationale and design. Front Pediatr. (2021) 9:799125. doi: 10.3389/fped.2021.799125
11. Takken T, Tacken MH, Blank AC, Hulzebos EH, Strengers JL, Helders PJ. Exercise limitation in patients with Fontan circulation: a review. J Cardiovasc Med (Hagerstown). (2007) 8(10):775–81. doi: 10.2459/JCM.0b013e328011c999
12. Parada Blazquez MJ, Rodriguez Vargas D, Mohigefer Barrera J, Borrero Martin JJ, Vargas Serrano B. Fontan-associated liver disease. Radiologia (Engl Ed). (2021) 63(2):159–69. doi: 10.1016/j.rxeng.2020.10.007
13. Gordon-Walker TT, Bove K, Veldtman G. Fontan-associated liver disease: a review. J Cardiol. (2019) 74(3):223–32. doi: 10.1016/j.jjcc.2019.02.016
14. Tellez L, Rodriguez de Santiago E, Albillos A. Fontan-associated liver disease: pathophysiology, staging, and management. Semin Liver Dis. (2021) 41(4):538–50. doi: 10.1055/s-0041-1732355
15. Liu X, Tan SBM, Awiwi MO, Jang HJ, Chernyak V, Fowler KJ, et al. Imaging findings in cirrhotic liver: pearls and pitfalls for diagnosis of focal benign and malignant lesions. Radiographics. (2023) 43(9):e230043. doi: 10.1148/rg.230043
16. Kirk R, Dipchand AI, Rosenthal DN, Addonizio L, Burch M, Chrisant M, et al. The international society for heart and lung transplantation guidelines for the management of pediatric heart failure: executive summary. [corrected]. J Heart Lung Transplant. (2014) 33(9):888–909. doi: 10.1016/j.healun.2014.06.002
17. Heidenreich PA, Bozkurt B, Aguilar D, Allen LA, Byun JJ, Colvin MM, et al. 2022 AHA/ACC/HFSA guideline for the management of heart failure: executive summary: a report of the American College of Cardiology/American Heart Association Joint Committee on clinical practice guidelines. Circulation. (2022) 145(18):e876–e94. doi: 10.1161/CIR.0000000000001062
18. Glaab T, Taube C. Practical guide to cardiopulmonary exercise testing in adults. Respir Res. (2022) 23(1):9. doi: 10.1186/s12931-021-01895-6
19. Ling A, Montez-Rath M, Mathur M, Kapphahn K, Desai M. How to apply multiple imputation in propensity score matching with partially observed confounders: a simulation study and practical recommendations. J Mod Appl Stat Meth. (2020) 19(1):eP3439. doi: 10.22237/jmasm/1608552120
20. Schafer JL. Multiple imputation: a primer. Stat Methods Med Res. (1999) 8(1):3–15. doi: 10.1177/096228029900800102
21. Rosenbaum PR, Rubin DB. The central role of the propensity score in observational studies for causal effects. Biometrika. (1983) 70(1):41–55. doi: 10.1093/biomet/70.1.41
22. Pishgar F, Greifer N, Leyrat C, Stuart E. Matchthem:: matching and weighting after multiple imputation. R J. (2021) 13(2):292–305. doi: 10.32614/RJ-2021-073
23. Thatte N, Dimas V, Nugent A, Zellers T, Forbess J, Zabala L, et al. Use of institutional criteria for transcatheter device closure of Fontan fenestration—midterm outcomes. Ann Pediatr Cardiol. (2020) 13(4):327–33. doi: 10.4103/apc.APC_154_19
24. Daley M, Buratto E, King G, Grigg L, Iyengar A, Alphonso N, et al. Impact of Fontan fenestration on long-term outcomes: a propensity score-matched analysis. J Am Heart Assoc. (2022) 11(11):e026087. doi: 10.1161/JAHA.122.026087
25. Airan B, Sharma R, Choudhary SK, Mohanty SR, Bhan A, Chowdhari UK, et al. Univentricular repair: is routine fenestration justified? Ann Thorac Surg. (2000) 69(6):1900–6. doi: 10.1016/S0003-4975(00)01247-9
26. Bouhout I, Ben-Ali W, Khalaf D, Raboisson MJ, Poirier N. Effect of fenestration on Fontan procedure outcomes: a meta-analysis and review. Ann Thorac Surg. (2020) 109(5):1467–74. doi: 10.1016/j.athoracsur.2019.12.020
27. Atz AM, Travison TG, McCrindle BW, Mahony L, Quartermain M, Williams RV, et al. Late status of Fontan patients with persistent surgical fenestration. J Am Coll Cardiol. (2011) 57(24):2437–43. doi: 10.1016/j.jacc.2011.01.031
28. Luo Q, Zhao W, Su Z, Liu Y, Jia Y, Zhang L, et al. Risk factors for prolonged pleural effusion following total cavopulmonary connection surgery: 9 years’ experience at Fuwai Hospital. Front Pediatr. (2019) 7:456. doi: 10.3389/fped.2019.00456
29. Devanagondi R, Leonard G. Transcatheter Fontan fenestration closure: sustained improvements in oxygen saturation with minimal morbidity and mortality. Pediatr Cardiol. (2023) 44(4):922–6. doi: 10.1007/s00246-022-03077-7
30. Stephens EH, Talwar AA, Devlin PJ, Eltayeb O, Monge MC, Tsao S, et al. 24-year results of nonfenestrated extracardiac Fontan including Fontan conversions. Ann Thorac Surg. (2021) 112(2):619–25. doi: 10.1016/j.athoracsur.2020.06.019
31. Greenleaf CE, Lim ZN, Li W, LaPar DJ, Salazar JD, Corno AF. Impact on clinical outcomes from transcatheter closure of the Fontan fenestration: a systematic review and meta-analysis. Front Pediatr. (2022) 10:915045. doi: 10.3389/fped.2022.915045
32. Haddad RN, Bonnet D, Malekzadeh-Milani S. Transcatheter closure of extracardiac Fontan conduit fenestration using new promising materials. J Card Surg. (2021) 36(11):4381–5. doi: 10.1111/jocs.15916
33. Webb MK, Hunter LE, Kremer TR, Huddleston CB, Fiore AC, Danon S. Extracardiac Fontan fenestration device closure with amplatzer vascular plug II and septal occluder: procedure results and medium-term follow-up. Pediatr Cardiol. (2020) 41(4):703–8. doi: 10.1007/s00246-019-02283-0
34. Kim SH, Kang IS, Huh J, Lee HJ, Yang JH, Jun TG. Transcatheter closure of fenestration with detachable coils after the Fontan operation. J Korean Med Sci. (2006) 21(5):859–64. doi: 10.3346/jkms.2006.21.5.859
35. Chadalavada S, Boolkah S, Smith BG. Use of a self-expanding custom-made stent graft to treat lateral tunnel leak, stenosis, and fenestration in the Fontan pathway. Cardiol Young. (2012) 22(1):110–2. doi: 10.1017/S1047951111000886
36. Malekzadeh-Milani S, Ladouceur M, Bajolle F, Bonnet D, Boudjemline Y. Closure of Fontan fenestration with the use of covered stents: short- and mid-term results in a cohort of 50 patients. Cardiol Young. (2015) 25(5):868–73. doi: 10.1017/S1047951114000894
37. Momenah TS, Eltayb H, Oakley RE, Qethamy HA, Faraidi YA. Effects of transcatheter closure of Fontan fenestration on exercise tolerance.a2lkZWNob0B5YWhvby5jb20=. Pediatr Cardiol. (2008) 29(3):585–8. doi: 10.1007/s00246-007-9154-3
38. Saiki H, Kuwata S, Iwamoto Y, Ishido H, Taketazu M, Masutani S, et al. Fenestration in the fontan circulation as a strategy for chronic cardioprotection. Heart. (2019) 105(16):1266–72. doi: 10.1136/heartjnl-2018-314183
39. Oka N, Miyamoto T, Tomoyasu T, Hayashi H, Miyaji K. Risk factors for mid-term liver disease after the Fontan procedure. Int Heart J. (2020) 61(5):979–83. doi: 10.1536/ihj.20-059
40. Li D, Li M, Zhou X, An Q. Comparison of the fenestrated and non-fenestrated Fontan procedures: a meta-analysis. Medicine (Baltimore). (2019) 98(29):e16554. doi: 10.1097/MD.0000000000016554
Keywords: Fontan, fenestration, outcome, registries, propensity score
Citation: Ko H, Song J, Chi SA, Lee S-Y, Kim S-J, Lee C-H, Park CS, Choi ES, An HS, Kang I.S, Yoon JK, Baek J-S, Lee J-Y, Lee J, Huh J, Ahn K-J, Jung SY, Cha SG, Kim Y-H and Lee Y-S (2024) The long-term effects of the fenestration in patients with extracardiac Fontan circulation—a multicenter Korean cohort study based on national Fontan registry. Front. Cardiovasc. Med. 11:1341882. doi: 10.3389/fcvm.2024.1341882
Received: 21 November 2023; Accepted: 22 April 2024;
Published: 7 May 2024.
Edited by:
Petru Liuba, Lund University, SwedenReviewed by:
Hideo Ohuchi, National Cerebral and Cardiovascular Center, Japan© 2024 Ko, Song, Chi, Lee, Kim, Lee, Park, Choi, An, Kang, Yoon, Baek, Lee, Lee, Huh, Ahn, Jung, Cha, Kim and Lee. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jinyoung Song YW15anlzQG5hdmVyLmNvbQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.