
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Cardiovasc. Med. , 23 February 2024
Sec. Coronary Artery Disease
Volume 11 - 2024 | https://doi.org/10.3389/fcvm.2024.1305162
 Óscar González-Lorenzo1*
Óscar González-Lorenzo1* Juan A. Franco Pelaez1Andrea Kallmeyer1Luis Nieto1Laura Esteban1Ana Pello1
Juan A. Franco Pelaez1Andrea Kallmeyer1Luis Nieto1Laura Esteban1Ana Pello1 Álvaro Aceña1,2Gonzalo Aldamiz3José Tuñón1,2,4,5
Álvaro Aceña1,2Gonzalo Aldamiz3José Tuñón1,2,4,5
Introduction: The presence of non-coronary atherosclerosis (NCA) in patients with coronary artery disease is associated with a poor prognosis. We have studied whether NCA is also a predictor of poorer outcomes in patients undergoing coronary artery bypass grafting (CABG).
Materials and methods: This is an observational study involving 567 consecutive patients who underwent CABG. Variables and prognosis were analysed based on the presence or absence of NCA, defined as previous stroke, transient ischaemic attack (TIA), or peripheral artery disease (PAD) [lower extremity artery disease (LEAD), carotid disease, previous lower limb vascular surgery, or abdominal aortic aneurysm (AAA)]. The primary outcome was a combination of TIA/stroke, acute myocardial infarction, new revascularization procedure, or death. The secondary outcome added the need for LEAD revascularization or AAA surgery.
Results: One-hundred thirty-eight patients (24%) had NCA. Among them, traditional cardiovascular risk factors and older age were more frequently present. At multivariate analysis, NCA [hazard ratio (HR) = 1.84, 95% confidence interval (CI) 1.27–2.69], age (HR = 1.35, 95% CI 1.09–1.67, p = 0.004), and diabetes mellitus (HR = 1.50, 95% CI 1.05–2.15, p = 0.025), were positively associated with the development of the primary outcome, while estimated glomerular filtration rate (HR = 0.86, 95% CI 0.80–0.93, p = 0.001) and use of left internal mammary artery (HR = 0.36, 95% CI 0.15–0.82, p = 0.035), were inversely associated with this outcome. NCA was also an independent predictor of the secondary outcome. Mortality was also higher in NCA patients (27.5% vs. 9%, p < 0.001).
Conclusions: Among patients undergoing CABG, the presence of NCA doubled the risk of developing cardiovascular events, and it was associated with higher mortality.
High blood pressure, dyslipidaemia, smoking, diabetes, obesity, and a sedentary lifestyle are well-known risk factors for the development of atherosclerosis, and their prevalence is also related to aging. The association between the burden of these risk factors and the vascular territory affected by atherosclerosis is still under debate. However, there is consensus that once atherosclerosis is established in one vascular territory, the risk of ischaemic events increases in all vascular beds, leading to excess mortality (1).
It has been demonstrated that multiple artery disease results in a worse prognosis (2–4). However, to date, only one clinical trial (5) has been designed to systematically assess the existence of poly-vascular disease among coronary patients, with no clinical benefit of this approach demonstrated.
Notwithstanding this fact, it is beyond doubt that the coexistence of non-coronary atherosclerosis (NCA) worsens the prognosis of CAD patients, even when the first event is not clinically overt. The presence of lower extremity artery disease (LEAD) is known to be an independent risk factor since, after adjusting the analysis for smoking habit, age, diabetes, and gender, it still multiplies by four the risk of death (6, 7). This association appears less clear in patients with carotid artery disease (8).
On the other hand, patients with established CAD are at high risk for cardiac and cerebral ischaemic events, such as acute myocardial infarction (AMI), stroke/transient ischaemic attack (TIA), or even death (9). Furthermore, the presence of CAD is associated with an increased risk of subclinical abdominal aortic aneurysms (AAAs) and future AAA-related adverse events (10, 11). The existence of NCA is known to be associated with poor outcomes in patients with CAD, as it indicates the presence of extensive atherosclerosis (12). The aim of the present study is to analyse whether the presence of NCA among coronary patients undergoing coronary artery bypass graft (CABG) is associated with a poor outcome.
The design was a retrospective, observational, single-centre study. The study was carried out in a tertiary-level university hospital. Patients who underwent CABG between 2010 and 2018 were included on a consecutive basis, excluding those with concomitant valve or aortic surgery.
Clinical data were reviewed to obtain a wide range of variables concerning demographics, clinical characteristics, blood tests, and surgery-related data. After this, the cohort was divided into two groups, depending on the presence or absence of NCA, defined as previous stroke, TIA, or PAD [lower extremity artery disease (LEAD), carotid disease, previous lower limb vascular surgery, or AAA].
This study conforms to the ethical guidelines of the 1975 Declaration of Helsinki as reflected in a priori approval by the human research committee of Fundación Jiménez Díaz Hospital Ethics Board for Research (register number: EO077-19_FJD).
Follow-up was conducted by a review of the clinical history, during which adverse events were registered. We considered the date of surgery as the beginning of the follow-up. The primary outcome included the combination of TIA/stroke, AMI, new revascularization procedure, or death. The secondary outcome added the need for lower extremity revascularization or AAA surgery to the primary outcome.
Quantitative data are presented as medians and interquartile ranges. Comparisons between groups were performed by Student's t-test for variables that met the assumption of normality and by a non-parametric test (Mann–Whitney U-test) for those that did not. Normality was assessed by the Kolmogorov–Smirnov test, where p < 0.05 indicated that the variable did not meet the assumption of normality. Qualitative variables are displayed as percentages, and groups were compared using the chi-squared test (or Fisher's exact test when appropriate).
To find prognostic factors of primary and secondary endpoints, all relevant clinical and analytical variables, including NCA, were tested in a univariate Cox proportional hazards regression analysis. After that, all variables with a significance level of p < 0.2 in univariate analysis were included in a multivariate model. This multivariate analysis was performed using the backward step method, keeping only those variables with a significance level of p < 0.05 as calculated by the likelihood ratio method. The effect of every independent predictor variable is presented as a hazard ratio (HR) and its 95% confidence interval (CI). Kaplan–Meier curves were plotted to compare the intervals of survival free of the primary and secondary outcomes in patients with or without NCA at baseline, and groups were compared using the log-rank test.
Analyses were performed with IBM SPSS Statistics for Windows (version 20.0; Armonk, NY, IBM Corp), and statistical significance was considered when the “p” value was lower than 0.05 (two-tailed).
A total of 567 patients were included. Baseline characteristics are presented in Table 1. Of the total, 138 patients (24%) met the study criteria for NCA before the surgery date. Among these patients, the most frequent conditions were lower limb vascular disease, accounting for 72% of the cases, and stroke/TIA, accounting for 34%.
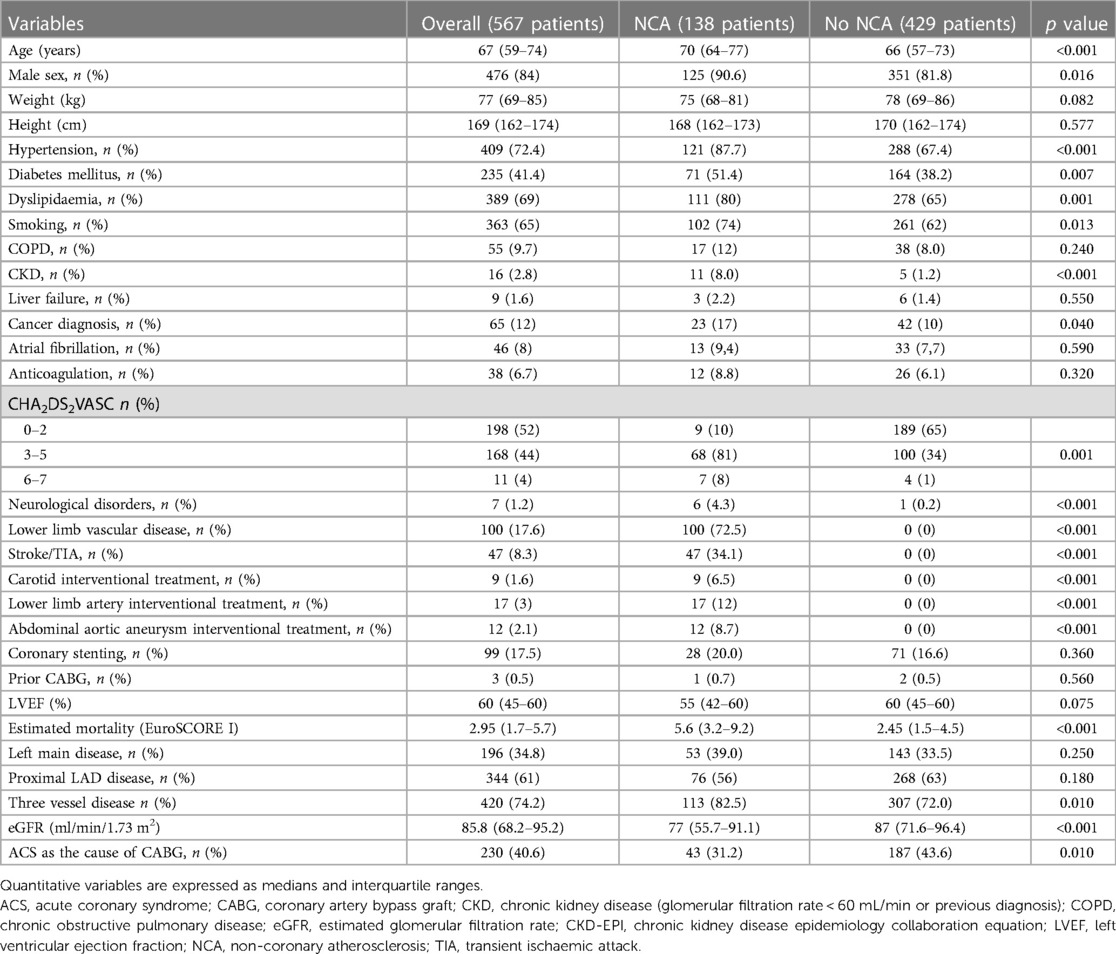
Table 1. Baseline characteristics prior to surgery.
Patients in the NCA group were older, predominantly male, and had a higher burden of traditional cardiovascular risk factors, as well as a high prevalence of kidney failure and oncological disease. In addition, patients with NCA had a higher EuroSCORE I than those without NCA. Of the total, 17.5% of patients had undergone a previous percutaneous revascularization procedure and three patients had undergone a previous CABG, with no significant differences between groups.
Moreover, acute coronary syndromes (ACS) accounted for around 41% of CABG procedures, being more frequent in the group without NCA. A total of 33% of patients had left main disease, and 66% had left anterior descendent artery (LAD) stenosis, with no differences between groups. Three-vessel disease was more frequent in the NCA group (82.5% vs. 72%).
Regarding technical issues of surgery, on-pump CABG was more frequently performed in the non-NCA group (82.2% vs. 71.7%). In approximately 98% of cases, a left internal mammary artery (LIMA) graft was used, with no differences between groups, whereas complete revascularization was more frequently achieved in non-NCA patients (76.5% vs. 68.0%) (Table 2).
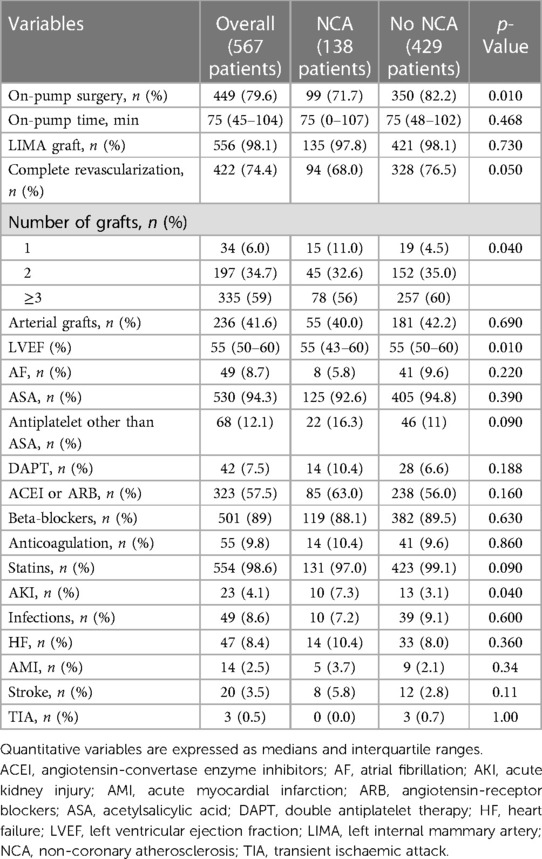
Table 2. Surgical features and postoperative characteristics and complications.
Complications before discharge are also detailed in Table 2. No differences were observed among groups, except for acute kidney injury (AKI), which occurred more frequently in the NCA group (7.3% vs. 3.1%).
There were no differences in medications at discharge nor in the rates of double antiplatelet therapy, which reached only 7% of patients.
Although the incidence of atrial fibrillation (AF) prior to surgery did not differ between groups, CHA2DS2VASc was significantly higher in the NCA group (Table 1). Moreover, there were no differences in the occurrence of AF after surgery. Seventy-two percent of patients who developed postoperative AF did not receive anticoagulation treatment on discharge, as arrhythmia was considered an immediate side effect of surgery. Chronic anticoagulation therapy at discharge was similar between both groups.
After a median follow-up of 4.2 (2.3–6.9) years, 122 patients reached the primary outcome, with 73 patients (17%) in the non-NCA group compared to 49 patients (35.5%) in the NCA group (p < 0.001) (Table 3).
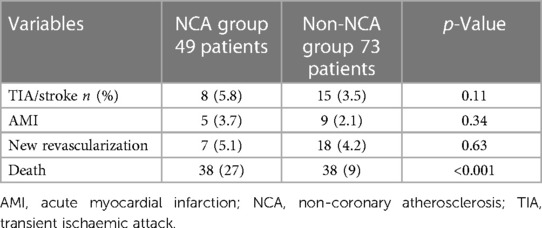
Table 3. Variables of the primary outcome.
The association of clinically relevant variables with the occurrence of the primary outcome in univariate Cox analysis is presented in Table 4.
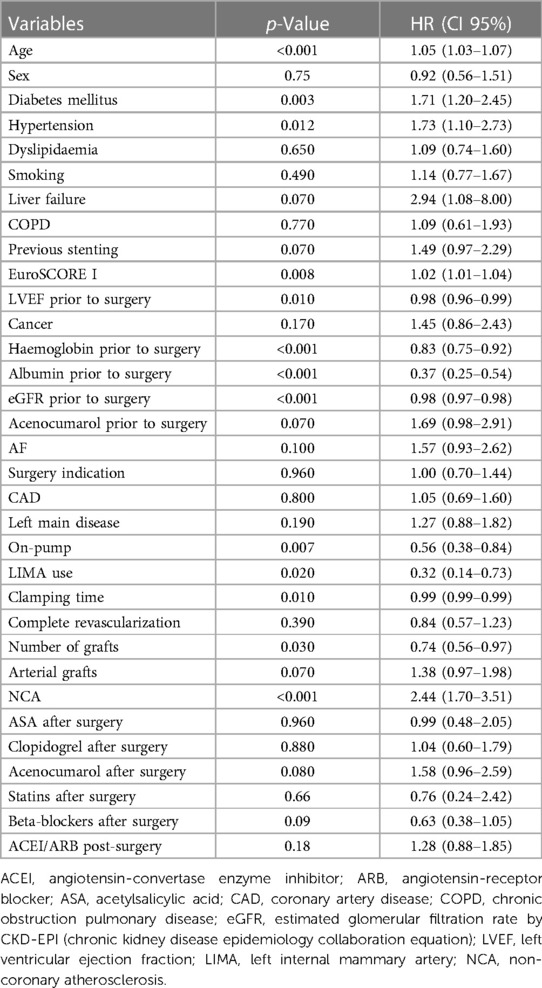
Table 4. Univariate Cox regression analysis for the primary outcome.
In multivariate analysis, NCA, older age, diabetes mellitus, worse eGFR, and non-use of LIMA at surgery were independent predictors of the primary outcome (Figure 1).
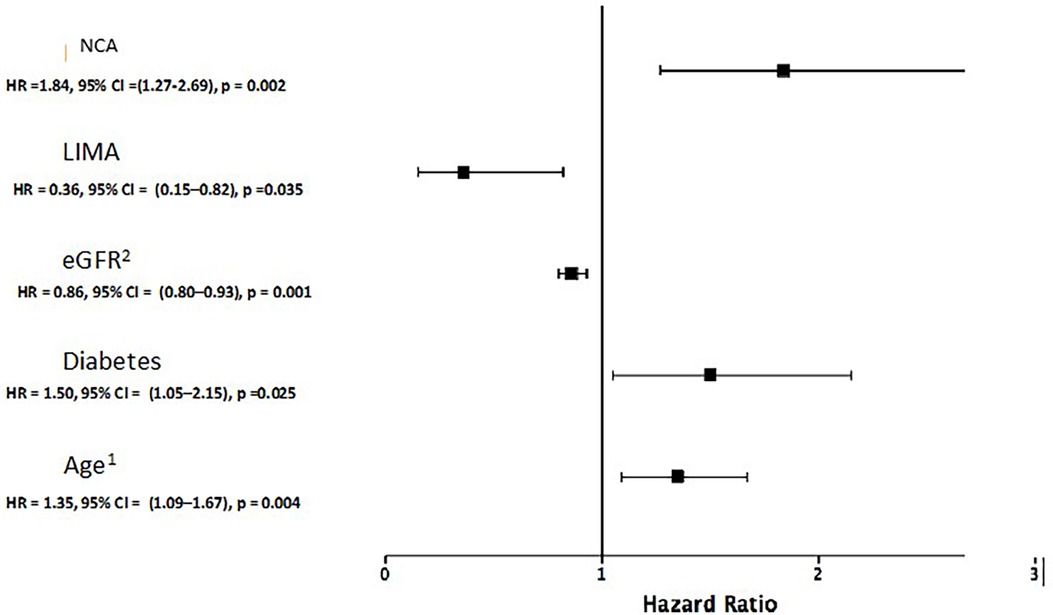
Figure 1. Final Cox regression multivariate model for the occurrence of the primary outcome. 1For each 10 years increase. 2For each 10 ml/min/1.73 m2 increase. eGFR: Estimated glomerular filtration rate by CKD-EPI (Chronic Kidney Disease Epidemiology Collaboration equation). LIMA, left internal mammary artery; NCA, non-coronary atherosclerosis.
Figure 2 shows the Kaplan–Meier curves for the occurrence of the primary outcome in both groups.
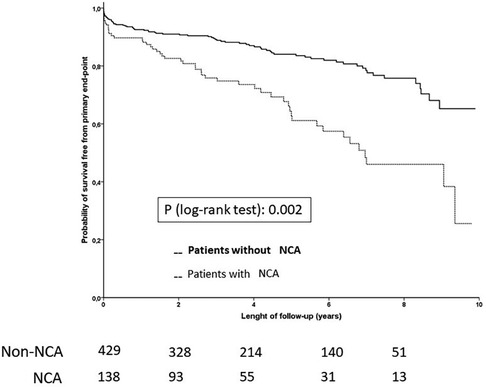
Figure 2. Kaplan-Meier curves for the primary outcome. NCA, non-coronary atherosclerosis.
A total of 135 patients reached the secondary outcome, with 18.6% of patients in the non-NCA group (80 patients) compared to 40% of patients in the NCA group (55 patients). Lower extremity revascularization occurred in 11.4% of patients in the NCA group (16 patients) after follow-up compared to 0.9% of patients (4 patients) in the non-NCA group (p < 0.001), and AAA surgery was performed in 5 patients (3.7%) in the NCA group compared to 4 patients (0.9%) in the non-NCA group (p = 0.04).
The association of clinically relevant variables with the occurrence of the secondary outcome in univariate Cox analysis is detailed in the Supplemental Material.
In multivariate analysis, NCA and non-use of LIMA were independent predictors of the secondary outcome. Moreover, for each 10 mL/min worsening of the estimated glomerular filtration rate, the risk increased by 15% (Table 5).
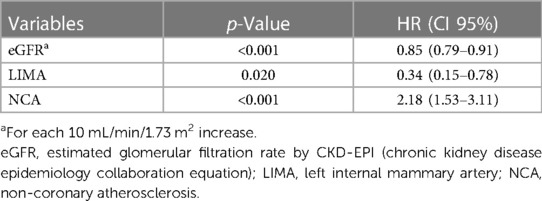
Table 5. Multivariate analysis for the secondary outcome.
Figure 3 shows the Kaplan–Meier curves for the occurrence of the secondary outcome in both groups.
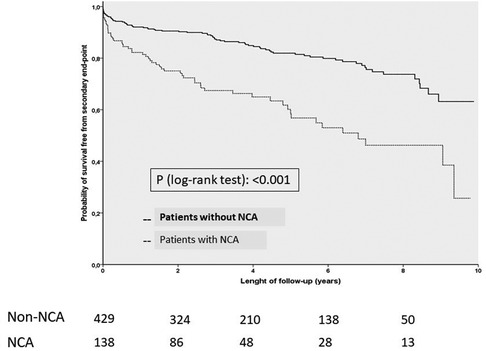
Figure 3. Kaplan-Meier curves for the secondary outcome. NCA, Non-coronary atherosclerosis.
The median follow-up was 3.6 years (IQR 1.9–6.4) in the NCA group and 4.4 years (IQR 2.5–7.0) in the non-PAD group. Mortality was higher in the NCA group (27% vs. 9%, p < 0.001) (Table 6). On the other hand, mortality within the first 30 days after surgery was similar in both groups (2.9% in the NCA group and 1.2% in the non-NCA group, p = 0.23).
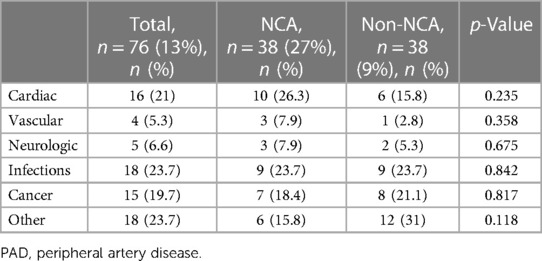
Table 6. Causes of death.
The main finding of our study was the confirmation that NCA is a strong predictor of worse prognosis in CAD patients undergoing CABG as a revascularization therapy. Thus, its presence increases the risk of TIA/stroke, AMI, new revascularization procedure, or death by 84% compared to patients without NCA.
In our study, NCA, older age, and diabetes mellitus were independent predictors of the primary outcome, while estimated glomerular filtration rate and use of LIMA were inversely associated with this outcome. Secondary outcome added the need for lower extremity revascularization or AAA surgery, with NCA once again emerging as a clearly determining factor, alongside impaired kidney function.
Traditional cardiovascular risk factors (smoking, hypertension, diabetes mellitus, and dyslipidaemia) and the ageing of the population are recognized as important determinants of NCA in all countries (13–15).
The BARI study previously demonstrated that searching for NCA, even when clinically silent, in CAD patients could be crucial for early detection of underlying conditions, and it could lead to more aggressive cardiovascular preventive treatment strategies (12, 16, 17).
When comparing our results with those from other studies, caution must be exercised due to the heterogeneous definitions of NCA. Some studies refer to PAD when diagnosing lower limb arterial disease (13, 18), while others include the existence of AAA and its repair treatments in the definition (12, 19, 20). Moreover, there have been studies (8, 21) that considered previous stroke/TIA as a form of PAD. As we aimed to include stroke and TIA as forms of previous peripheral atherosclerosis, we used the term NCA, including stroke and TIA on the one hand, along with the classical concept of PAD on the other hand, defined as LEAD, carotid disease, previous lower limb vascular surgery, or AAA.
The prevalence of NCA among our population was 24.3%, which was similar to other studies (17% in Nakamura et al., 26% in Birkmeyer et al., and 21% in Harskamp et al.). All these series described a similar incidence of older age, impaired renal function, and a higher frequency of cardiovascular risk factors in the PAD group (6, 8, 18, 21) compared with non-PAD patients.
Complications after CABG surgery were greater in previous studies in the PAD group (Harskamp et al.; Bonacchi et al.), with kidney failure up to 8.9% and a stroke rate of 2.7% (20, 21). In our study, the proportion of acute kidney injury after surgery was also higher in patients with NCA (7.3% vs. 3.1%), but there were no differences in terms of stroke. On the other hand, Chu et al. found no differences in the complication rate in the NCA group (13).
Considering mortality, the group of NCA patients may represent a subset of patients with a more aggressive form of CAD that progresses much faster, thus contributing to the increased late mortality observed in the NCA patients. It is important to differentiate between early (within 30 days after surgery) and long-term mortality. Birkmeyer et al. found a 2.4 times higher in-hospital mortality in patients with PAD (8). Our results, just like those of Harskamp et al. (21), Nakamura et al. (18), or van Straten et al. (19), did not show any significant difference in early mortality. However, in the long term, better survival was noted among the participants in the non-NCA group (survival was 90% vs. 72%).
Concerning causes of death, cardiovascular disease accounted for 34% in the NCA group vs. 18% in the non-NCA group, although it did not reach statistical significance. Birkmeyer et al. showed an excess of deaths due to heart failure and arrhythmia in the NCA group (8). Meanwhile, the BARI study highlighted that the main cause of mortality among PAD patients was cardiac, although the percentages of deaths from other causes were also more frequent (16).
Thus, with this body of evidence, it seems reasonable to recommend strategies to assess for the presence of NCA among patients with established CAD or in patients with high cardiovascular risk features. These findings suggest that NCA continues to identify a subgroup at particularly high risk for adverse cardiovascular outcomes that might benefit from more intensive secondary prevention. However, up to date, the single study that addressed this topic has failed to reach significance, although it had important limitations, such as the inclusion of high-risk patients in both arms (5).
On the other hand, PAD has been described as a treatment modifier in terms of the duration of dual antiplatelet therapy in patients undergoing percutaneous coronary intervention, with a prolonged regimen (up to 24 months) associated with a significantly lower risk of death and atherothrombotic events and unaffected risk of bleeding (22). Nevertheless, although clinical practice guidelines still recommend double antiplatelet therapy in ACS (9), irrespective of the revascularization strategy, there have been contradictory data about it among studies. This could be due to heterogeneous designs related to on-pump use and indication of surgery, among other factors (23). In our study, we did not find significant differences, probably due to the small sample size of patients discharged with double antiplatelet therapy.
This was a retrospective observational analysis, and thus, patients with subclinical NCA were not identified. The inclusion and exclusion criteria of this study may limit the possibility of extending our findings to other populations. The type of major adverse limb events was not available, so we could only include vascular limb intervention. Finally, the limited sample size precluded us from obtaining information about other interesting aspects, such as potential interactions between NCA and the use of dual antiplatelet therapy.
Among patients treated with CABG surgery, the presence of NCA confers a higher risk of death and doubles the incidence of the combined outcome of TIA/stroke, AMI, new revascularization therapy, lower limb or AAA surgery, and death.
The original contributions presented in the study are included in the article/Supplementary Material; further inquiries can be directed to the corresponding author.
The studies involving humans were approved by the human research committee of Fundación Jiménez Díaz Hospital Ethic Board for investigation (register number: EO077-19_FJD). The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participants’ legal guardians/next of kin because the design was a retrospective, observational study.
ÓG-L: Writing – original draft, Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Project administration. JF: Writing – review & editing, Conceptualization, Formal Analysis, Investigation, Methodology, Software, Supervision, Validation. AK: Writing – review & editing, Data curation, Formal Analysis, Supervision. LN: Investigation, Writing – original draft, Data curation. LE: Writing – original draft, Data curation, Investigation. AP: Conceptualization, Data curation, Investigation, Writing – review & editing. ÁA: Conceptualization, Data curation, Formal Analysis, Investigation, Writing – review & editing. GA: Conceptualization, Investigation, Writing – original draft. JT: Conceptualization, Methodology, Supervision, Writing – original draft.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fcvm.2024.1305162/full#supplementary-material
1. Aboyans V, Ricco JB, Bartelink MLEL, Björck M, Brodmann M, Cohnert T, et al. 2017 ESC guidelines on the diagnosis and treatment of peripheral arterial diseases, in collaboration with the European Society for Vascular Surgery (ESVS). Eur Heart J. (2018) 39(9):763–816. doi: 10.1093/eurheartj/ehx095
2. Mukherjee D, Eagle KA, Kline-Rogers E, Feldman LJ, Juliard JM, Agnelli G, et al. Impact of prior peripheral arterial disease and stroke on outcomes of acute coronary syndromes and effect of evidence-based therapies (from the Global Registry of Acute Coronary Events). Am J Cardiol. (2007) 100(1):1–6. doi: 10.1016/j.amjcard.2007.02.046
3. Saw J, Bhatt DL, Moliterno DJ, Brener SJ, Steinhubl SR, Lincoff AM, et al. The influence of peripheral arterial disease on outcomes: a pooled analysis of mortality in eight large randomized percutaneous coronary intervention trials. J Am Coll Cardiol. (2006) 48(8):1567–72. doi: 10.1016/j.jacc.2006.03.067
4. Manfrini O, Amaduzzi PL, Cenko E, Bugiardini R. Prognostic implications of peripheral artery disease in coronary artery disease. Curr Opin Pharmacol. (2018) 39:121–8. doi: 10.1016/j.coph.2018.04.005
5. Collet JP, Cayla G, Ennezat PV, Leclercq F, Cuisset T, Elhadad S, et al. Systematic detection of polyvascular disease combined with aggressive secondary prevention in patients presenting with severe coronary artery disease: the randomized AMERICA study. Int J Cardiol. (2018) 254:36–42. doi: 10.1016/j.ijcard.2017.11.081
6. Criqui MH, Langer RD, Fronek A, Feigelson HS, Klauber MR, McCann TJ, et al. Mortality over a period of 10 years in patients with peripheral arterial disease. N Engl J Med. (1992) 326(6):381–6. doi: 10.1056/NEJM199202063260605
7. Grenon SM, Vittinghoff E, Owens CD, Conte MS, Whooley M, Cohen BE. Peripheral artery disease and risk of cardiovascular events in patients with coronary artery disease: insights from the Heart and Soul Study. Vasc Med. (2013) 18(4):176–84. doi: 10.1177/1358863X13493825
8. Birkmeyer JD, Quinton HB, O'Connor NJ, McDaniel MD, Leavitt BJ, Charlesworth DC, et al. The effect of peripheral vascular disease on in-hospital mortality rates with coronary artery bypass surgery. Northern New England Cardiovascular Disease Study Group. J Vasc Surg. (1995) 21(3):445–52. doi: 10.1016/S0741-5214(95)70286-5
9. Neumann FJ, Sousa-Uva M, Ahlsson A, Alfonso F, Banning AP, Benedetto U, et al. 2018 ESC/EACTS guidelines on myocardial revascularization. Eur Heart J. (2019) 40(2):87–165. doi: 10.1093/eurheartj/ehy394
10. Hernesniemi JA, Vänni V, Hakala T. The prevalence of abdominal aortic aneurysm is consistently high among patients with coronary artery disease. J Vasc Surg. (2015) 62(1):232–40.e3. doi: 10.1016/j.jvs.2015.02.037
11. Erbel R, Aboyans V, Boileau C, Bossone E, Bartolomeo RD, Eggebrecht H, et al. 2014 ESC guidelines on the diagnosis and treatment of aortic diseases. Eur Heart J. (2014) 35(41):2873–926. doi: 10.1093/eurheartj/ehu281
12. Burek KA, Sutton-Tyrrell K, Brooks MM, Naydeck B, Keller N, Sellers MA, et al. Prognostic importance of lower extremity arterial disease in patients undergoing coronary revascularization in the Bypass Angioplasty Revascularization Investigation (BARI). J Am Coll Cardiol. (1999) 34(3):716–21. doi: 10.1016/S0735-1097(99)00262-4
13. Chu D, Bakaeen FG, Wang XL, Dao TK, LeMaire SA, Coselli JS, et al. The impact of peripheral vascular disease on long-term survival after coronary artery bypass graft surgery. Ann Thorac Surg. (2008) 86(4):1175–80. doi: 10.1016/j.athoracsur.2008.06.024
14. Criqui MH, Aboyans V. Epidemiology of peripheral artery disease. Circ Res. (2015) 116(9):1509–26. doi: 10.1161/CIRCRESAHA.116.303849
15. Savji N, Rockman CB, Skolnick AH, Guo Y, Adelman MA, Riles T, et al. Association between advanced age and vascular disease in different arterial territories: a population database of over 3.6 million subjects. J Am Coll Cardiol. (2013) 61(16):1736–43. doi: 10.1016/j.jacc.2013.01.054
16. Sutton-Tyrrell K, Rihal C, Sellers MA, Burek K, Trudel J, Roubin G, Brooks MM, et al. Long-term prognostic value of clinically evident noncoronary vascular disease in patients undergoing coronary revascularization in the Bypass Angioplasty Revascularization Investigation (BARI). Am J Cardiol. (1998) 81(4):375–81. doi: 10.1016/S0002-9149(97)00934-X
17. Rihal CS, Sutton-Tyrrell K, Guo P, Keller NM, Jandova R, Sellers MA, Schaff HV, et al. Increased incidence of periprocedural complications among patients with peripheral vascular disease undergoing myocardial revascularization in the bypass angioplasty revascularization investigation. Circulation. (1999) 100(2):171–7. doi: 10.1161/01.CIR.100.2.171
18. Nakamura T, Toda K, Miyagawa S, Yoshikawa Y, Fukushima S, Saito S, et al. Symptomatic peripheral artery disease is associated with decreased long-term survival after coronary artery bypass: a contemporary retrospective analysis. Surg Today. (2016) 46(11):1334–40. doi: 10.1007/s00595-016-1379-4
19. van Straten AHM, Firanescu C, Soliman Hamad MA, Tan MESH, ter Woorst JFJ, Martens EJ, et al. Peripheral vascular disease as a predictor of survival after coronary artery bypass grafting: comparison with a matched general population. Ann Thorac Surg. (2010) 89(2):414–20. doi: 10.1016/j.athoracsur.2009.11.036
20. Bonacchi M, Parise O, Matteucci F, Tetta C, Moula AI, Micali LR, et al. Is peripheral artery disease an independent predictor of isolated coronary artery bypass outcome? Heart Lung Circ. (2020) 29(10):1502–10. doi: 10.1016/j.hlc.2020.01.013
21. Harskamp RE, Alexander JH, Schulte PJ, Schuyler Jones W, Williams JB, Mack MJ, et al. Impact of extracardiac vascular disease on vein graft failure and outcomes after coronary artery bypass surgery. Ann Thorac Surg. (2014) 97(3):824–30. doi: 10.1016/j.athoracsur.2013.09.099
22. Franzone A, Piccolo R, Gargiulo G, Ariotti S, Marino M, Santucci A, et al. Prolonged vs. short duration of dual antiplatelet therapy after percutaneous coronary intervention in patients with or without peripheral arterial disease: a subgroup analysis of the PRODIGY randomized clinical trial. JAMA Cardiol. (2016) 1(7):795–803. doi: 10.1001/jamacardio.2016.2811
23. Willemsen LM, Janssen PWA, Peper J, Soliman-Hamad MA, van Straten AHM, Klein P, et al. Effect of adding ticagrelor to standard aspirin on saphenous vein graft patency in patients undergoing coronary artery bypass grafting (POPular CABG): a randomized, double-blind, placebo-controlled trial. Circulation. (2020) 142(19):1799–807. doi: 10.1161/CIRCULATIONAHA.120.050749
Keywords: peripheral artery disease (PAD), stroke, transient ischaemic attack (TIA), coronary artery bypass grafting (CABG), cardiovascular risk factors
Citation: González-Lorenzo Ó, Franco Pelaez JA, Kallmeyer A, Nieto L, Esteban L, Pello A, Aceña Á, Aldamiz G and Tuñón J (2024) Non-coronary atherosclerosis: a marker of poor prognosis in patients undergoing coronary artery bypass surgery. Front. Cardiovasc. Med. 11:1305162. doi: 10.3389/fcvm.2024.1305162
Received: 2 October 2023; Accepted: 2 February 2024;
Published: 23 February 2024.
Edited by:
Lars Norgren, Örebro University, SwedenReviewed by:
Chenggang Li, Xuzhou Medical University, China© 2024 González-Lorenzo, Franco Pelaez, Kallmeyer, Nieto, Esteban, Pello, Aceña, Aldamiz and Tuñón. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Óscar González-Lorenzo b2dvbnphbGV6QHF1aXJvbnNhbHVkLmVz
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.