 Javier Segovia-Cubero1,2*Lorena Ruiz-Bautista1Luis Maiz-Carro3Rosa M. Girón-Moreno4M. Concepción Prados-Sánchez5M. Teresa Martínez-Martínez6Montserrat González-Estecha7Susana Mingo-Santos1Manuel Gómez-Bueno1,2Clara Salas-Antón8Miguel A. Cavero-Gibanel1Miguel Pastrana-Ledesma9Pablo García-Pavía1,2Rosalía Laporta-Hernández10David Sánchez-Ortiz1Luis Alonso-Pulpón1,2
Javier Segovia-Cubero1,2*Lorena Ruiz-Bautista1Luis Maiz-Carro3Rosa M. Girón-Moreno4M. Concepción Prados-Sánchez5M. Teresa Martínez-Martínez6Montserrat González-Estecha7Susana Mingo-Santos1Manuel Gómez-Bueno1,2Clara Salas-Antón8Miguel A. Cavero-Gibanel1Miguel Pastrana-Ledesma9Pablo García-Pavía1,2Rosalía Laporta-Hernández10David Sánchez-Ortiz1Luis Alonso-Pulpón1,2
- 1Cardiolology Dept., Hospital Universitario Puerta de Hierro, Madrid, Spain
- 2Centro de Investigación Biomédica en Red en Enfermedades Cardiovasculares (CIBERCV), Madrid, Spain
- 3Cystic Fibrosis Unit, Pneumology Dept., Hospital Universitario Ramon y Cajal, Madrid, Spain
- 4Cystic Fibrosis Unit, Pneumology Dept., Hospital Universitario La Princesa, Madrid, Spain
- 5Cystic Fibrosis Unit, Pneumology Dept., Hospital Universitario La Paz, Madrid, Spain
- 6Cystic Fibrosis Unit, Pneumology Dept., Hospital Universitario Doce de Octubre, Madrid, Spain
- 7Trace Element Laboratory, Biochemistry Dept., Hosp. Universitario San Carlos, Madrid, Spain
- 8Pathology Dept., Hospital Universitario Puerta de Hierro, Madrid, Spain
- 9Radiology Dept., Hospital Universitario Puerta de Hierro, Madrid, Spain
- 10Pneumology Dept., Hospital Universitario Puerta de Hierro, Madrid, Spain
Introduction: We conducted a study to determine the prevalence of structural heart disease in patients with CF, the characteristics of a cardiomyopathy not previously described in this population, and its possible relationship with nutritional deficiencies in CF.
Methods: We studied 3 CMP CF patients referred for heart-lung transplantation and a prospective series of 120 adult CF patients. All patients underwent a clinical examination, blood tests including levels of vitamins and trace elements, and echocardiography with evaluation of myocardial strain. Cardiac magnetic resonance imaging (CMR) was performed in patients with CMP and in a control group. Histopathological study was performed on hearts obtained in transplant or necropsy.
Results: We found a prevalence of 10% (CI 4.6%–15.4%) of left ventricular (LV) dysfunction in the prospective cohort. Myocardial strain parameters were already altered in CF patients with otherwise normal hearts. Histopathological examination of 4 hearts from CF CMP patients showed a unique histological pattern of multifocal myocardial fibrosis similar to Keshan disease. Four of the five CF CMP patients undergoing CMR showed late gadolinium uptake, with a characteristic patchy pattern in 3 cases (p < 0.001 vs. CF controls). Selenium deficiency (Se < 60 µg/L) was associated with more severe LV dysfunction, higher prevalence of CF CMP, higher NTproBNP levels, and more severe pulmonary and digestive involvement.
Conclusion: 10% of adults with CF showed significant cardiac involvement, with histological and imaging features resembling Keshan disease. Selenium deficiency was associated with the presence and severity of LV dysfunction in these patients.
1 Introduction
Cystic fibrosis (CF) represents the most common lethal hereditary disorder in individuals of Caucasian descent, with an incidence ranging from 1 in 2,000 to 1 in 5,000 live births. The condition arises from mutations in the CFTR gene, which codes for the Cystic Fibrosis Transmembrane Conductance Regulator—a key protein facilitating the movement of chloride ions and other electrolytes across cellular membranes (1). Prior to the substantial progress in treatment over the past two decades, most individuals with CF succumbed to the disease in their youth. However, recent advancements have markedly prolonged the life span of those affected, now potentially surpassing 40 years (2, 3). Continuous development in targeted therapies is expected to yield further enhancements in patient outcomes shortly (1, 3).
Historically, cardiac involvement has not been predominantly recognized within the spectrum of CF pathology. Although cor pulmonale due to chronic hypoxemia was once suggested to be present in advanced stages of CF lung disease, this has not been substantiated by rigorous research (3–5). Nonetheless, comprehensive autopsies of young CF patients have documented pronounced cardiac abnormalities, including left ventricular enlargement and a distinctive histological presentation termed multifocal myocardial fibrosis (MMF) (6, 7). Similar cardiac histological patterns have been observed in individuals with severe malabsorption disorders (8), and intriguingly, in cases of Keshan disease (9) —a region-specific cardiomyopathy in parts of China predominantly affecting children and pregnant females, linked to selenium deficiency, and largely eradicated following Se supplementation in at-risk groups (10–12).
Prompted by the identification of Se deficiency in a CF patient evaluated for heart-lung transplantation, we structured a prospective study aimed at assessing the incidence of structural heart disease within the CF demographic. This research also uncovers the features of a previously unidentified cardiac condition and explores its potential association with the nutritional complications inherent to CF. The importance of this work lies in the need to clarify the existence of this entity and its manifestations, establish the appropriate diagnostic tools and suggest pathophysiological hypotheses that could help improve the prevention of its appearance and treatment in the future.
2 Materials and methods
We recruited a series of adult CF patients without known cardiac disease from all of the four specific CF outpatient clinics in our health area. We also analyzed the characteristics of the patients referred for HLTx who motivated the project. We obtained the approval of the Research Ethics Committees of the five participating institutions. Informed consent was obtained from patients and controls.
Clinical data were obtained by structured interview. Patients were grouped according to the presence of homozygous or heterozygous F508del mutation of CFTR gene or other mutations. Pancreatic insufficiency was stratified by dose of pancreatic enzyme supplements (thresholds 1,000 and 2,000 UI). For pulmonary involvement, the presence and type of pulmonary colonization were recorded, as well as the severity of pulmonary disease expressed as % of FEV1 and other spirometry parameters.
Blood tests: Blood samples were collected after an 8 h overnight fasting period and were processed at the same laboratory. Trace element samples were processed in accordance with the Guideline of the Clinical and Laboratory Standards Institute, as shown in Supplementary Appendix I of Supplementary Material.
Cardiac evaluation: Twelve-lead surface EKG and an echocardiographic study (IE33 digital ultrasound system®, Philips Medical Systems, Amsterdam, Holland) were performed. Echocardiographic evaluation was performed according to the American Society of Echocardiography (ASE) recommendations as shown in Supplementary Appendix II (13).
Established CF cardiomyopathy was defined by the presence of a left ventricular ejection fraction (LVEF) ≤ 50% (systolic dysfunction) without other obvious cause in cardiac study. LV dysfunction was diagnosed in the presence of either systolic or diastolic dysfunction. LV longitudinal and circumferential strain measurements were performed by speckle tracking technique according to the EACVI/ASE recommendations (14). A series of 21 healthy adults matched for age and gender served as a control group for strain and strain-rate data comparisons. A reproducibility analysis of myocardial deformation measures was performed and is available in Supplementary Appendix II.
In order to define the characteristics of CF cardiomyopathy we studied a group of 8 patients including 3 patients referred to our center for HLTx and 5 patients with cardiomyopathy (systolic dysfunction) detected in the prospective cohort. Cardiac magnetic resonance (CMR) and histology when possible (organs explanted at HLTx) were carried out in this group. CMR was performed with a 1.5 T equipment, (Philips Intera CV, Best, The Netherlands®). A subgroup of 20 volunteer CF individuals without cardiac dysfunction served as control. CMR protocol is described in Supplementary Appendix III of Supplemental Material.
Statistical analysis: Shapiro-Wilk test was used to confirm the normal distribution hypothesis. Comparison between groups was performed with the Student's t test for independent samples with a normal distribution and the Mann-Whitney test for non-normally distributed variables. The strain values were contrasted by the one-way ANOVA test and the post-hoc multiple comparison Tukey test. The comparison of two proportions in independent samples was performed using the χ2 test and Fisher's exact test as appropriate. Risk was estimated with the OR and 95% CI. A two-sided p-value less than 0.05 was considered statistically significant. All analyses were performed with SPSS® v21 (SPSS Inc., Chicago, IL, USA).
3 Results
3.1 Cardiomyopathy associated with CF
In this study, we delineate a cohort of 8 patients presenting with a distinct form of cardiomyopathy, which we propose to term “Cardiomyopathy of Cystic Fibrosis” (CF CMP) henceforth. Among these individuals, 3 were referred to our institution for heart-lung transplantation (HLTx), while the remaining 5 were identified through our prospective study, exhibiting a left ventricular ejection fraction (LVEF) below 50%. Table 1A shows the clinical attributes of CF in these subjects, comparing them with CF patients who do not present with CMP. Overall, those with CMP demonstrated exacerbated respiratory and gastrointestinal manifestations of CF, in addition to lower body mass indices, frequently registering as underweight. Genetic analysis of patients disclosed the following mutations in the CFTR gene: three subjects possessed a homozygous F508del mutation, one a heterozygous F508del mutation, one a homozygous G542X mutation, one a homozygous S549R mutation, and two exhibited no identifiable mutations.
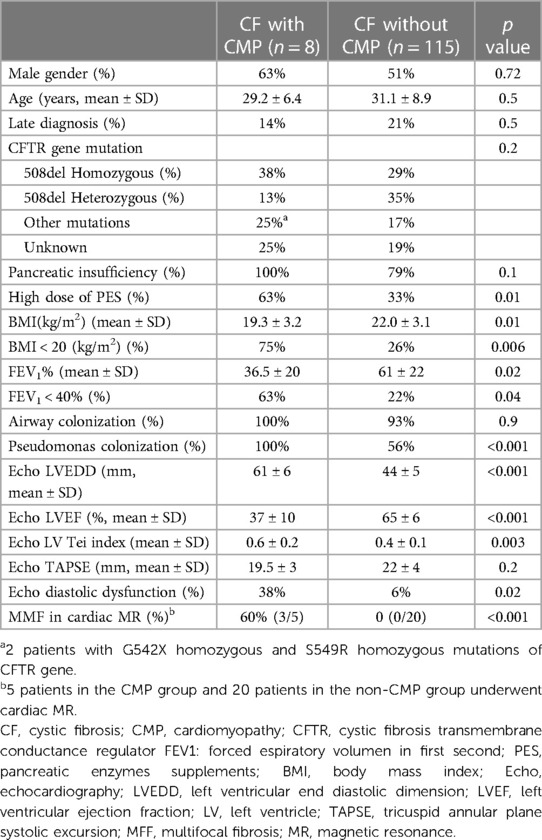
Table 1A. Comparison of the characteristics of CF patients with cardiomyopathy with those of CF patients with normal hearts.
Laboratory findings, as delineated in Table 1B, revealed salient disparities such as elevated NT-proBNP levels and a pronounced occurrence of selenium (Se) deficiency within the CF CMP cohort, though aggregate Se concentrations remained analogous across both patient groups.
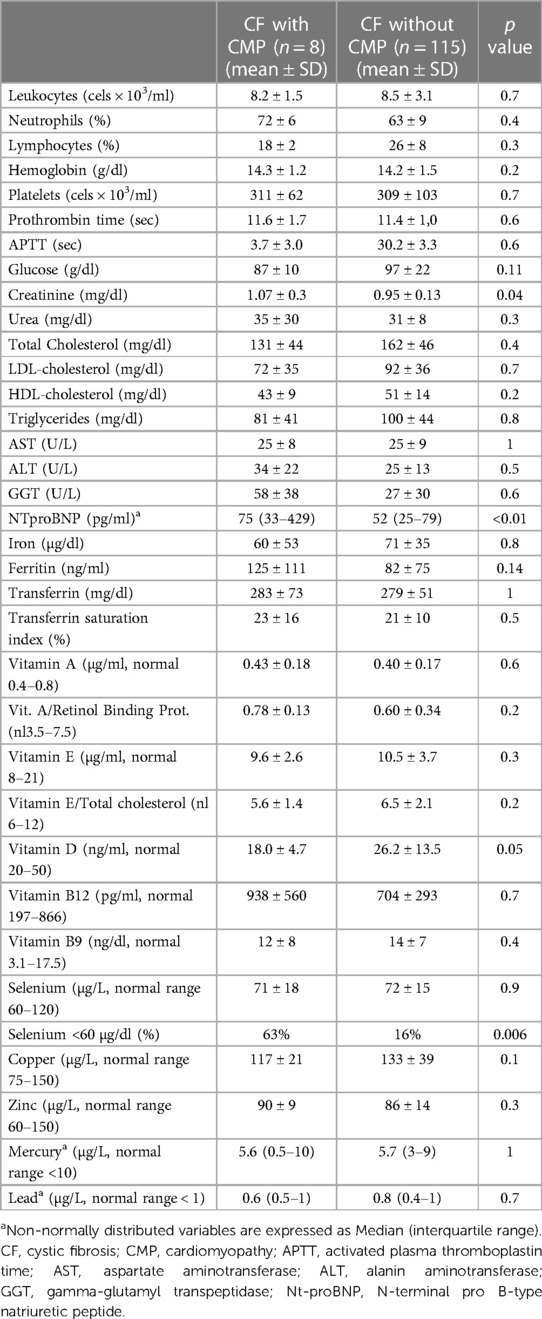
Table 1B. Selected laboratory values of CF patients with cardiomyopathy as compared with those without it.
Electrocardiography in patients with CMP uniformly showed normal sinus rhythm with standard PR and QTc intervals. Two EKG showed signs of left atrial enlargement, two displayed intraventricular conduction delays, and five presented repolarization anomalies suggestive of LV overload. Chest radiography consistently confirmed signs of CF-related pulmonary involvement in all cases, yet an augmented cardiothoracic index, devoid of associated pulmonary congestion, was visible in only two of the eight patients.
Echocardiographic measures for the CF CMP subjects (Table 1A), principally highlighted notable discrepancies in LV function relative to CF patients without CMP, while parameters of right ventricular function, such as Tricuspid Annular Plane Systolic Excursion (TAPSE), were comparable between both groups. Moreover, a substantial decrease in longitudinal strain values was observed (−13 ± 6 for CF CMP vs. −20 ± 5 for CF patients without CMP, p = 0.04). Within the CMP subset, only a singular patient exhibited mitral regurgitation of a moderate degree. Fundamentally, echocardiographic findings from the CF CMP population resembled those associated with other dilated cardiomyopathy variants.
Cardiac MRI, conducted on five CMP subjects (all CMP patients excluding the 3 who received HLTx), revealed late gadolinium enhancement in four patients, with three demonstrating a patchy myocardial uptake dispersed arbitrarily across the LV walls (Figure 1). Another patient displayed marginal linear subepicardial gadolinium uptake, while the one with a higher LVEF (48%) showed no detectable enhancement. In contrast, gadolinium uptake was absent in CMR studies of 20 CF patients with an unremarkable echocardiogram (p < 0.001 by comparison).
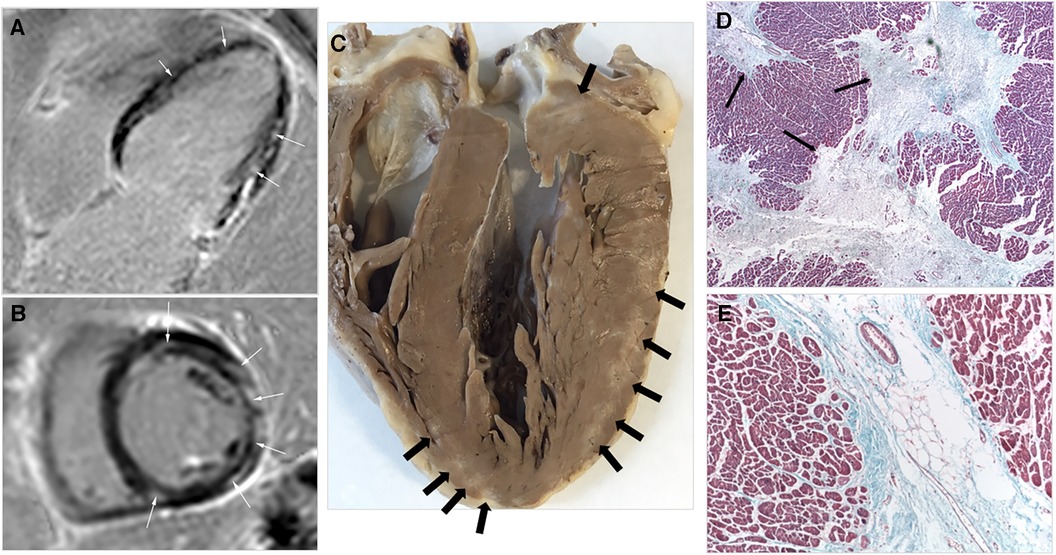
Figure 1. (A,B) CMR imaging in a patient with CF cardiomyopathy. Late gadolinium enhancement PSIR (phase sensitive inversion recovery) sequences seen on (A) long axis four-chamber view and (B) short axis view. Multiple patchy fibrotic areas of late gadolinium enhancement are evident, with a fibrosis pattern that is neither transmural nor subendocardial (small arrows). (C–E) Pathology of CF CMP. (C) Macroscopic view of a four-chamber section of the entire heart explanted during cardiopulmonary transplantation. Whitish areas of patchy fibrosis are evident within the myocardium of the free wall of the LV and the apical region of the interventricular septum (arrows). (D) Myocardium from LV wall showing multifocal myocardial fibrosis (MMF): large bands of lax fibrotic tissue are interspersed with areas of myocardium. (Masson trichrome staining, original magnification 40×). (E) Increased magnification (original 200×), showing lack of inflammatory cells at the grossly preserved myocardial areas, with atrophic myocardial fibers encroached by surrounding fibrotic tissue at the edges.
Pathologically, the four hearts available for examination (three explanted during HLTx and one necropsy from a CMP patient who succumbed to pulmonary infection) showcased congruent findings: Macroscopic inspection of sections of LV walls revealed patchy, whitish scars interspersed within otherwise normal myocardium (Figure 2A). Histological scrutiny identified the distinctive patterns of multifocal myocardial fibrosis (MMF), characterized by bands of fibrosis weaving through largely intact myocardial territories (Figures 2B,C). It is imperative to note the absence of inflammatory cellular infiltration or disruption of the myocardial architecture. The collagen within the fibrotic strands presented a characteristic lax appearance, distinctly differing from scarring consequent to ischemic necrosis. Coronary arteries were normal in all inspected cases.
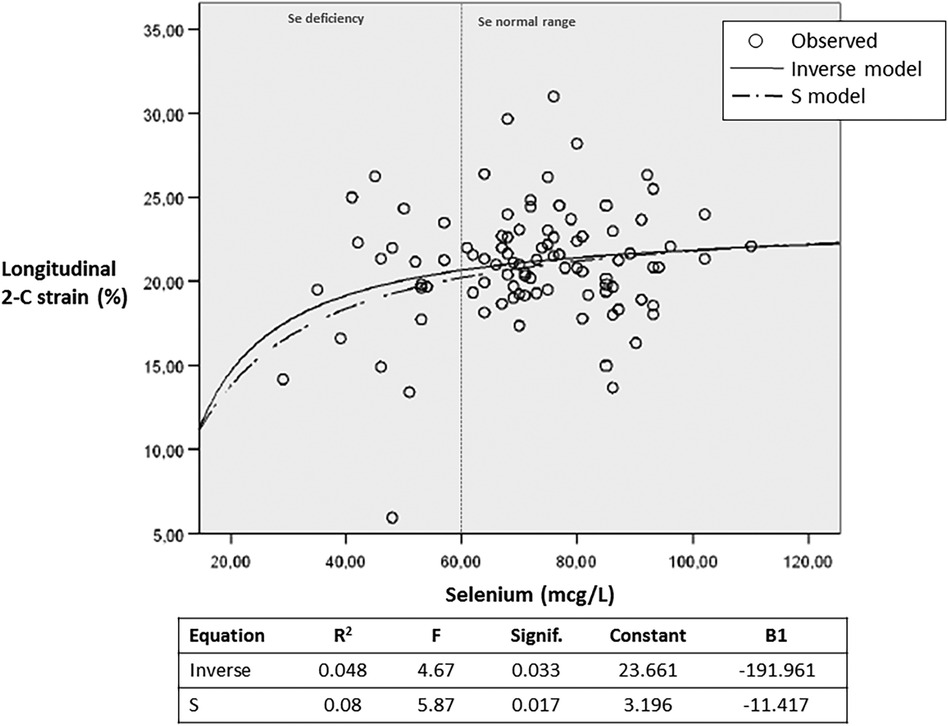
Figure 2. Non-linear models (inverse and S) of correlation between Se levels and longitudinal 2-chamber strain values. The models reflect stability of LV contractility values when Se levels are >60 mcg/L, and a tendency to progressively lower values below this cut-off Se level. Equations: Inverse: y = b0 + (b1/t) and S: y = eE(b0 + b1/t), where y = strain 2C; b0 = constant; b1 = B1; t = Se level.
3.2 Prevalence of left ventricular dysfunction in adults with cystic fibrosis
Out of 320 adults attending four specialized cystic fibrosis outpatient clinics, 135 agreed to participate in our prospective study and provided informed consent. Fifteen of these participants were unable to complete the necessary evaluations and were subsequently excluded from the analysis, resulting in a cohort of 120 consecutively enrolled, unselected adult CF patients devoid of any known cardiac pathologies. It is noteworthy to mention that none of the patients were receiving CF transmembrane conductance regulator modulator therapies, including lumacaftor, ivacaftor, tezacaftor, or elexacaftor, as the data collection predated the introduction of these treatments in our country.
Echocardiographic assessments identified left ventricular (LV) dysfunction in 12 individuals [10%; 95% Confidence Interval (CI): 4.6%–15.4%]. Among these, five (4.2%, CI: 0.6%–7.8%) were found to have significant systolic LV dysfunction: two (1.7%) exhibited isolated systolic impairment, while three (2.5%) presented with concurrent systolic and diastolic dysfunction. An additional seven participants (5.8%, CI: 1.6%–10%) were diagnosed with isolated diastolic LV dysfunction. Comprehensive clinical, laboratory, and echocardiographic parameters for the total study population and its respective subgroups are organized in Tables 2A,B.
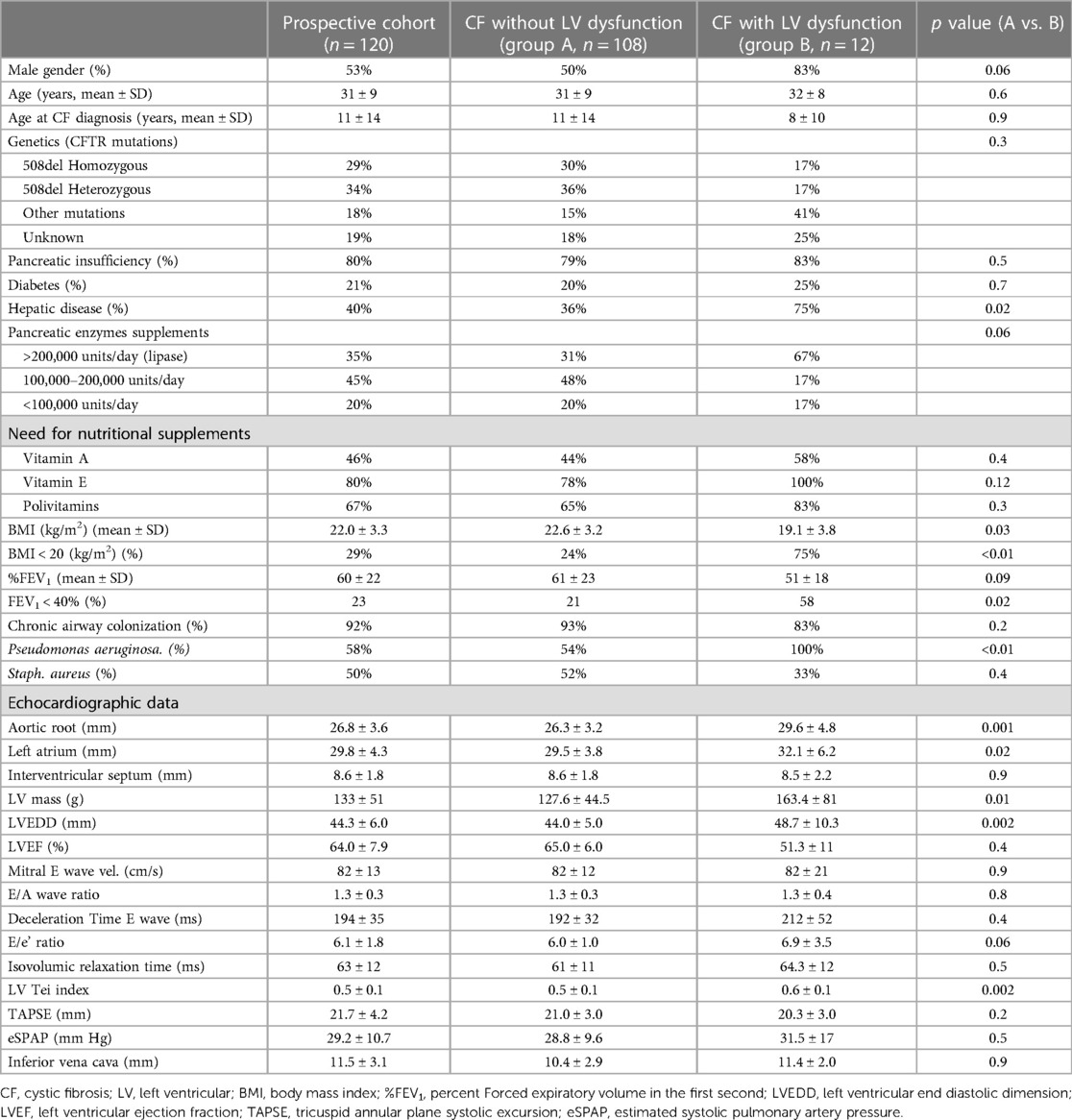
Table 2A. Clinical and cardiac and echocardiographic data of patients in the prospective cohort and its subgroups.
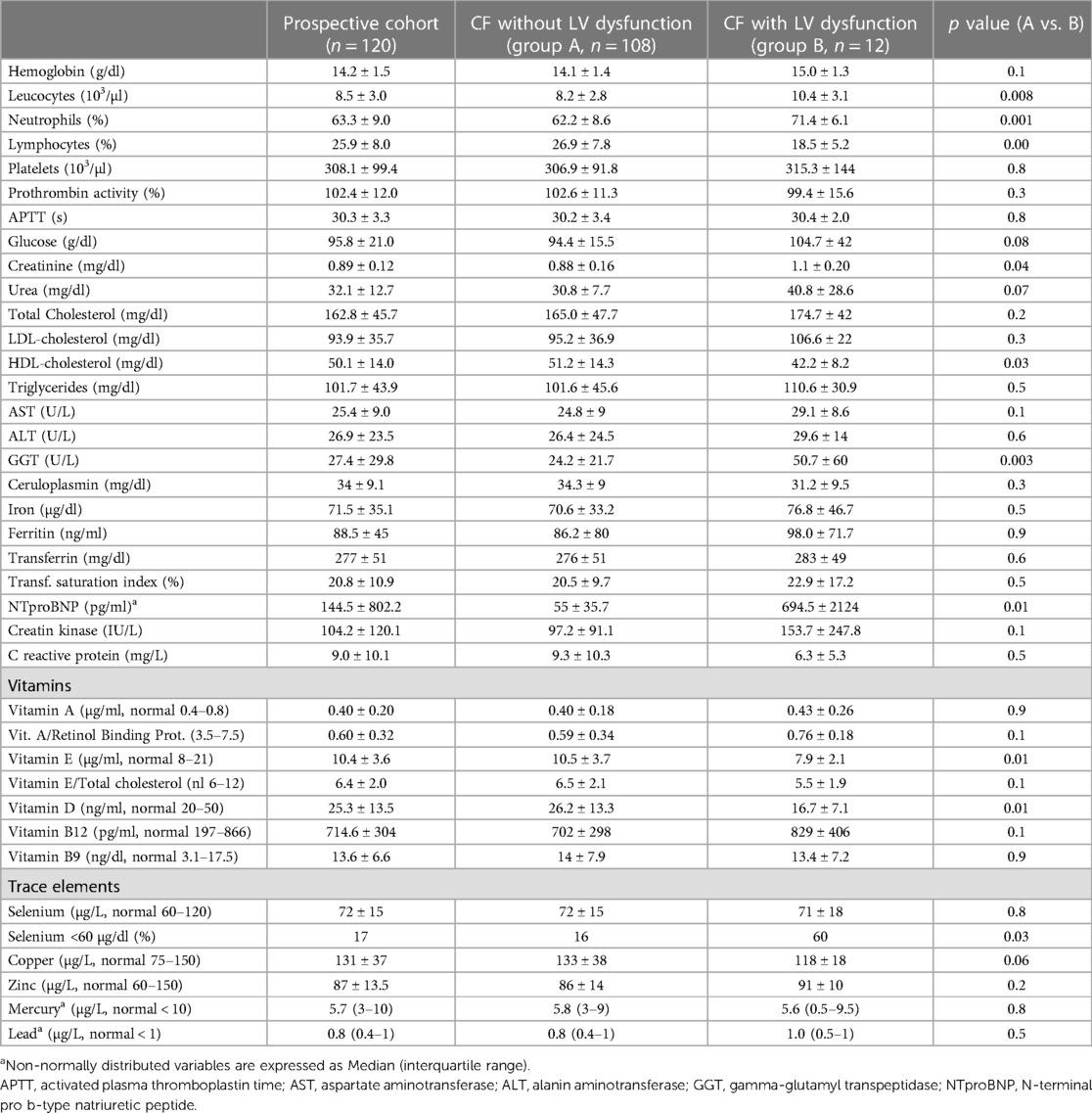
Table 2B. General laboratory results, vitamin and trace elements of patients in the prospective cohort and its subgroups.
Table 3 details the assessment of myocardial deformation parameters. Imaging quality impeded the deformation analysis of six patients, all pertaining to the subgroup with no LV dysfunction, thus reducing our sample to 114. The collective myocardial deformation measures among the CF patient cohort generally resided within normal parameters. Nonetheless, these figures were significantly inferior to those of a control group consisting of 21 healthy volunteers, suggesting that even CF patients with a standard cardiac evaluation may present subtly compromised myocardial mechanics.
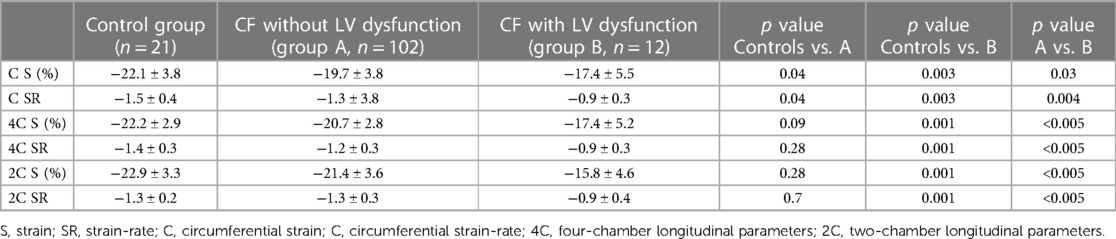
Table 3. Myocardial deformation analysis in the prospective series. Comparison of average strain and strain-rate values between normal controls, CF patients with normal LV function and CF patients with LV dysfunction of any type.
When focusing on CF patients with LV dysfunction, the myocardial deformation indices were substantially below normative values, showing significant reductions compared to both healthy controls and CF patients without LV impairment. Further analysis within the LV dysfunction classification revealed the most pronounced anomalies in patients with systolic dysfunction; comparative examination against those with solely diastolic dysfunction approached statistical significance in the case of longitudinal strain (−14.7 ± 4.2% vs. −19.5 ± 5.1%, p = 0.05).
3.3 Nutritional factors associated with cystic fibrosis cardiomyopathy
Vitamin levels in the prospective cohort and in CMP patients are shown in Table 2B. As anticipated within a population receiving tailored oral supplementation, average vitamin levels were predominantly in the normal range. However, trends toward lower concentrations of vitamins E and D were observed in CMP patients (p = 0.09 and p = 0.05, respectively). Vitamin D deficiency was more prevalent in the CMP subset (38%) compared to the broader CF cohort (17%), though this did not reach statistical significance (p = 0.17). Notably, we found no substantial correlations between vitamin levels and indices of left ventricular function.
The trace element profiles are summarized in Table 2B, with Cadmium levels excluded due to most (>80%) patients having measurements below detectable thresholds. Overall, trace element values in CF patients fell within acceptable ranges. Although the mean selenium (Se) levels did not differ significantly between those with and without LV dysfunction, Se deficiency (Se < 60 µg/L, identified in 17.5% of the prospective series) was linked to lower LVEF, an increased prevalence of LV dysfunction and CMP (14% among Se-deficient patients vs. 2% in the remainder, p = 0.037), as well as heightened NT-proBNP concentrations (Table 4). Furthermore, Se deficiency was associated with deleterious myocardial deformation metrics, higher instances of undernourishment indicated by BMI < 20 kg/m2, and more severe pulmonary disease manifestations. No relationships were found between LVEF and other trace elements.
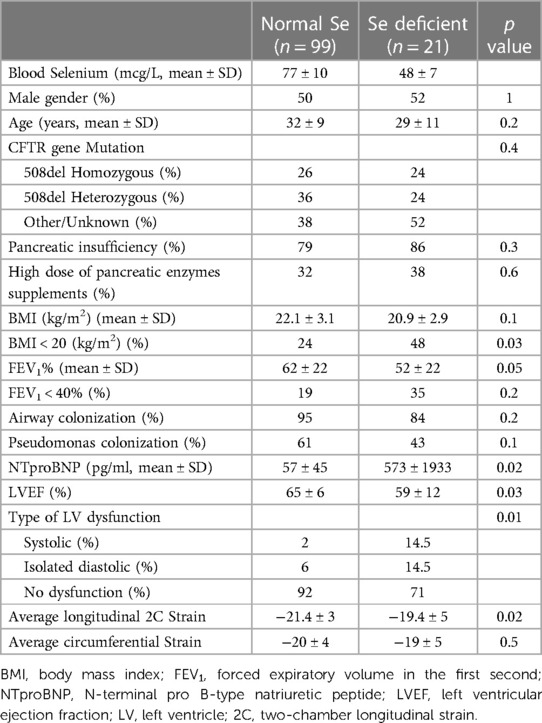
Table 4. Comparison of selected clinical, laboratory and echocardiographic values between Se-deficient CF patients and CF patients with normal Se blood levels.
4 Discussion
Our investigation delineates a unique subset of cardiomyopathy in adult patients with cystic fibrosis, characterized by a distinct pattern of multifocal myocardial fibrosis marked by characteristic histological findings and corroborating CMR imaging, with an observed association with selenium deficiency. In our CF population, the incidence of left ventricular dysfunction of any form is approximately 10%, with overt CMP presenting in about 4% of cases, usually associated with more severe pulmonary and nutritional manifestations of CF. These outcomes are summarized in Figure 3.
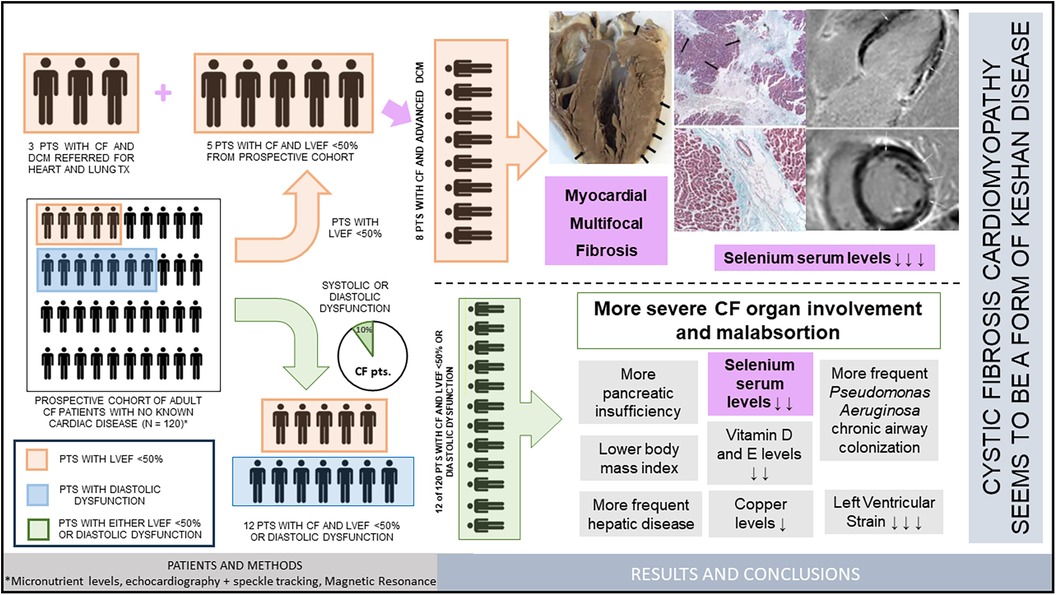
Figure 3. The coincidence of severe cystic fibrosis and cardiomyopathy in 3 patients referred to us for heart and lung transplantation suggested the existence of a specific type of cardiomyopathy related to cystic fibrosis. We recruited a prospective cohort of 120 patients with cystic fibrosis who were studied with echocardiogram and laboratory tests. Patients with LVEF < 50% (5 from the prospective cohort plus the 3 initial patients) underwent cardiac magnetic resonance, where a patchy pattern of late gadolinium enhancement was identified. Selenium deficiency was more frequent among these patients. Pathologic study of the explanted hearts from the 3 transplanted patients showed a distinct pattern of multifocal myocardial fibrosis similar to that of Keshan disease and other entities with nutrient malabsorption. Within the prospective cohort, we compared the clinical and laboratory findings of patients with significant diastolic or systolic dysfunction (n = 12) with those of cystic fibrosis patients with normal myocardial function (n = 108). Patients with cardiac dysfunction showed more severe organ involvement and lower levels of Selenium, other trace elements and several nutritional parameters. We conclude that a distinct type of cardiomyopathy similar to that of Keshan disease is present in a small percentage of patients with cystic fibrosis, and is associated with lower selenium levels, poorer nutritional status and more severe organ involvement.
Historically, the exploration into cardiac manifestations in CF traces back to the 1980s when cor pulmonale was frequently cited as a cause of mortality within this demographic, and non-invasive diagnostic options remained equivocal. There exists a paucity of contemporary data delineating the prevalence and characteristics of cardiac involvement in CF, partly because earlier studies emerged from an era when the clinical prognosis was graver and long-term survival past adolescence was rare (15–18).
The cohort of CF patients with cardiomyopathy in our study exhibited clinical, electrocardiographic, radiological, and echocardiographic features commonly associated with other forms of dilated cardiomyopathy. Nonetheless, histological analyses in all four patients where such data were attainable consistently revealed the distinctive presentation of patchy myocardial fibrosis (MMF). This discovery bears a connection to necropsy findings from the 1970s in children with CF. Notably, Oppenheimer and colleagues flagged a prevalence of MMF, then referred to as multifocal myocardial necrosis, at 4% among 143 autopsies of children with CF who had succumbed to various etiologies, including acute heart failure (6).
The observation of late gadolinium enhancement in four out of the five CF CMP cases subject to CMR imaging suggests substantial myocardial fibrosis. Particularly notable is the patchy intramyocardial distribution of this uptake in three instances, which diverges from patterns characteristic of ischemic and other cardiomyopathies. This distribution may indeed be reflective of the histological findings we observed. Such CMR findings have not been previously documented in CF patients and could potentially serve as a non-invasive marker for the diagnosis of this specific cardiomyopathy variant.
Nezelof et al. (8) previously identified MMF in 16 instances from an extensive collection of necropsy studies in children younger than two years. Over two decades later, the same researchers noted a resemblance between this fibrosis pattern and Keshan disease, suggesting a shared nutritional deficit as the etiological basis (9). More recently, selenium deficiency has been linked to Keshan disease, and dietary selenium supplements have proven instrumental in its mitigation and prevention (11, 12). In 2000, Zebrak et al. (7) conducted research on a cohort of 18 children with CF who experienced sudden fatality, finding the defining MMF pattern in the vast majority (89%). Here, the possibility of the F508del CFTR gene mutation as a predisposing factor was contemplated. Collectively, these studies have hypothesized a potential nutritional deficiency as a contributory factor in cardiac involvement, although subsequent research to substantiate this postulation has been lacking.
Prior surveys of cardiac function in CF patients have reported a wide range of incidences for right and left ventricular dysfunction, from nonexistent to more than 40% (5, 15–18) The investigation of diastolic LV dysfunction by Johnson et al. (17) and Koelling et al. (18) highlighted a common observation — the absence of a correlation between LV dysfunction and right ventricular complications, poised alongside a correlation of LV dysfunction with the severity of pulmonary disease and clinical CF evaluations.
The diagnostic methods for detecting LV dysfunction have seen significant advancements in recent times (5, 18–23). Concurrently, substantial enhancements in CF treatment have resulted in improved survival rates and elevated quality of life for patients (2). Accordingly, the prominence of cardiovascular symptoms associated with CF is likely to become increasingly salient in the foreseeable future (3, 22).
Myocardial deformation analysis, utilizing echocardiographic speckle-tracking techniques, has earned validation as an effective screening modality for subclinical cardiomyopathy across diverse etiologies. The detection of reduced strain and strain-rate values among CF patients with standard echocardiographic results dates back to 2011 and is corroborated by our research (19–21, 24). Thus, our data supports the growing consensus regarding the utility of myocardial deformation analysis as a sensitive method for uncovering incipient cardiac conditions within the CF population (20, 21, 24–26).
Out of the numerous vitamins and trace elements analyzed in our study, selenium (Se) deficiency has consistently emerged as the singular nutritional deficiency notably linked with various facets of myocardial dysfunction. This deficiency is not only associated to a 14.5% occurrence of CMP but is also identified as a factor contributing to diminished global left ventricular ejection fraction, altered myocardial deformation indices, and heightened levels of NT-proBNP. These relationships appear to follow a non-linear trend, analogous to what is observed in essential element-deficiency disorders, where damage typically manifests only below a cut-off (deficiency) value. The presence of normal Se levels in three out of eight CF patients diagnosed with CMP in this series could be attributed to delayed CF diagnosis in two of the individuals, positing that prolonged malnutrition—resulting from untreated CF-related digestive issues—may have led to exposure to Se deficiency and subsequent myocardial injury. Additionally, genetic variables may exert a significant role in determining the impact of selenium deficiency among patients. Future investigations are anticipated to elucidate the reparative potential of selenium supplementation in CF patients afflicted by low selenium-associated cardiomyopathy.
In 2012, Frustaci et al. documented a group of patients who developed dilated CMP subsequent to intestinal bypass surgery. Notably, after six months of intravenous selenium (Se) supplementation, the majority demonstrated a marked improvement in myocardial contractility (27).
Antioxidants play a crucial role in mitigating the harmful impacts of cellular oxidation resulting from free oxygen radicals (28–30). Selenium is an integral component of selenoproteins, such as glutathione peroxidases, and confers protection against oxidative stress-induced damage (22, 28, 30, 31–33). Moreover, particular signaling pathways and their interaction with microRNAs, as well as autophagy processes, contribute to the antioxidative effects of these proteins (34, 35). Deficiencies in micronutrients can profoundly affect mitochondrial energy production, endothelial function regulation, skeletal muscle protection, and thyroid metabolism (36–38). The link between selenium deficiency and cardiomyopathy has been established in humans, as seen in Keshan disease, and among animals, as illustrated by the condition known as “white muscle disease” (30, 31).
CF is characterized by a pronounced chronic inflammatory response and elevated levels of oxidative stress (22). Proper function of the CF transmembrane conductance regulator (CFTR) appears to shield myocytes from ischemia/reperfusion injury (39). Contemporary studies reveal adult CF patients still exhibit total selenium levels, both organic (Se-cysteine) and cationic forms of the element, that are significantly lower compared to healthy individuals (40). Case reports linking CF, CMP, and selenium deficiency corroborate this finding, lending support to the hypothesis of a relationship between these conditions (41).
A recent meta-analysis on the effect of supplementation with antioxidant principles in patients with CF suggested a relationship between serum selenium levels and respiratory function parameters such as FEV1. The different studies confirmed the positive correlation between serum selenium levels and antioxidant status described in the literature. The effect of supplementation on clinical variables is more controversial. The lack of efficacy of supplementation could be due to short treatment and follow-up periods in an entity with poorly understood pathophysiology (42, 43).
There is a growing consensus that even CF patients who adhere to current nutritional guidelines may experience micronutrient shortfalls that are associated with poorer clinical outcomes (44). Selenium supplementation must be judiciously administered, as elevated levels are linked to adverse consequences (45, 46). Future research is essential for elucidating the underlying mechanisms of cardiomyopathy tied to selenium deficits.
Limitations of the present study warrant careful interpretation when applying these findings across different populations and periods. As a cross-sectional analysis, it cannot establish causative links.
In conclusion, our investigation identified a particular form of cardiomyopathy in CF adults, which may be considered a variant analogous to Keshan disease. Diagnosis of this cardiomyopathy is attainable via non-invasive methods, and proactive screening using myocardial deformation echocardiographic techniques is viable. We observed that significant cardiac impairment occurs in 10% of a non-selected adult CF cohort, with half exhibiting systolic dysfunction. Notably, a correlation between CF CMP and reduced selenium levels was determined, highlighting a potential avenue for preventative measures and therapeutic intervention. Continued research is required to further elucidate the pathophysiological relationship between cardiomyopathy and selenium deficiency.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Comité Ético de Investigación del Hospital Universitario Puerta de Hierro Majadahonda de Madrid, Spain. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
JS: Conceptualization, Formal Analysis, Funding acquisition, Investigation, Methodology, Supervision, Validation, Writing – original draft. LR: Conceptualization, Data curation, Formal Analysis, Writing – review & editing. LM: Data curation, Investigation, Validation, Writing – review & editing. RG: Data curation, Investigation, Validation, Writing – review & editing. MP: Data curation, Investigation, Validation, Writing – review & editing. MM: Data curation, Investigation, Validation, Writing – review & editing. MG: Data curation, Formal Analysis, Methodology, Writing – review & editing. SM: Data curation, Investigation, Methodology, Writing – review & editing. MG: Data curation, Investigation, Validation, Writing – review & editing. CS: Data curation, Investigation, Methodology, Validation, Writing – review & editing. MC: Data curation, Methodology, Validation, Writing – review & editing. MP: Data curation, Methodology, Validation, Writing – review & editing. PG: Data curation, Validation, Writing – review & editing. RL: Data curation, Validation, Writing – review & editing. DS: Investigation, Methodology, Validation, Writing – original draft. LA: Conceptualization, Funding acquisition, Investigation, Methodology, Validation, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article.
This project received partial funding through a Pablo Motos grant from the Federación Española de Fibrosis Quística, located in Madrid, Spain. We also received logistic and administrative support from the Fundación Interhospitalaria para la Investigación Cardiovascular, located in Madrid, Spain.
Acknowledgments
We want to express our gratitude to the patients who agreed to take part in this study, to Isabel Millan Santos, PhD, for her help in the statistical analysis, and to Mrs. Ana Briceño, Ariadna G. Segovia, Isabel Molina and Dulce San Juan for their help in the handling of blood samples.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fcvm.2024.1285223/full#supplementary-material
References
1. Stoltz DA, Meyerholz DK, Welsh MJ. Origins of cystic fibrosis lung disease. N Engl J Med. (2015) 372:351–62. doi: 10.1056/NEJMra1300109
2. MacKenzie T, Gifford AH, Sabadosa KA, Quinton HB, Knapp EA, Goss CH, et al. Longevity of patients with cystic fibrosis in 2000 to 2010 and beyond: survival analysis of the cystic fibrosis foundation patient registry. Ann Intern Med. (2014) 161:233–41. doi: 10.7326/M13-0636
3. Plant BJ, Goss CH, Plant WD, Bell SC. Management of comorbidities in older patients with cystic fibrosis. Lancet Respir Med. (2013) 1:164–74. doi: 10.1016/S2213-2600(13)70025-0
4. Bright-Thomas RJ, Webb AK. The heart in cystic fibrosis. J R Soc Med. (2002) 95(41):2–10. 12216270.12216270
5. Florea VG, Florea ND, Sharma R, Coats AJ, Gibson DG, Hodson ME, et al. Right ventricular dysfunction in adult severe cystic fibrosis. Chest. (2000) 118:1063–8. doi: 10.1378/chest.118.4.1063
6. Oppenheimer EH, Esterly JR. Myocardial lesions in patients with cystic fibrosis of the pancreas. Johns Hopkins Med J. (1973) 133:252–61. 4759704.4759704
7. Zebrak J, Skuza B, Pogorzelski A, Ligarska R, Kopytko E, Pawlik J, et al. Partial CFTR genotyping and characterisation of cystic fibrosis patients with myocardial fibrosis and necrosis. Clin Genet. (2000) 57:56–60. doi: 10.1034/j.1399-0004.2000.570108.x
8. Nezelof C, LeSec G. Multifocal myocardial necrosis and fibrosis in pancreatic diseases of children. Pediatrics. (1979) 63:361–8. doi: 10.1542/peds.63.3.361
9. Nezelof C, Bouvier R, Dijoud F. Multifocal myocardial necrosis: a distinctive cardiac lesion in cystic fibrosis, lipomatous pancreatic atrophy, and Keshan disease. Pediatr Pathol Mol Med. (2002) 21:343–52. doi: 10.1080/pdp.21.3.343.352
10. Chen J. An original discovery: selenium deficiency and Keshan disease (an endemic heart disease). Asia Pac J Clin Nutr. (2012) 21:320–6. 22705420.22705420
11. Hou J, Zhu L, Chen C, Feng H, Li D, Sun S, et al. Association of selenium levels with the prevention and control of Keshan disease: a cross-sectional study. J Trace Elem Med Biol. (2021) 68:126832. doi: 10.1016/j.jtemb.2021.126832
12. Zhou H, Wang T, Li Q, Li D. Prevention of Keshan disease by selenium supplementation: a systematic review and meta-analysis. Biol Trace Elem Res. (2018) 186:98–105. doi: 10.1007/s12011-018-1302-5
13. Lang RM, Badano LP, Mor-Avi V, Afilalo J, Armstrong A, Ernande L, et al. Recommendations for cardiac chamber quantification by echocardiography in adults: an update from the American society of echocardiography and the European association of cardiovascular imaging. J Am Soc Echocardiogr. (2015) 28:1–39. doi: 10.1016/j.echo.2014.10.003
14. Voigt JU, Pedrizzetti G, Lysyansky P, Marwick TH, Houle H, Baumann R, et al. Definitions for a common standard for 2D speckle tracking echocardiography: consensus document of the EACVI/ASE/industry task force to standardize deformation imaging. J Am Soc Echocardiogr. (2015) 28:183–93. doi: 10.1016/j.echo.2014.11.003
15. Panidis IP, Ren JF, Holsclaw DS, Kotler MN, Mintz GS, Ross J. Cardiac function in patients with cystic fibrosis: evaluation by two-dimensional and Doppler echocardiography. J Am Coll Cardiol. (1985) 6:701–6. doi: 10.1016/S0735-1097(85)80134-0
16. Chipps BE, Alderson PO, Roland JM, Yang S, van AA, Martinez CR, et al. Noninvasive evaluation of ventricular function in cystic fibrosis. J Pediatr. (1979) 95:379–84. doi: 10.1016/S0022-3476(79)80510-7
17. Johnson GL, Kanga JF, Moffett CB, Noonan JA. Changes in left ventricular diastolic filling patterns by Doppler echocardiography in cystic fibrosis. Chest. (1991) 99:646–50. doi: 10.1378/chest.99.3.646
18. Koelling TM, Dec GW, Ginns LC, Semigran MJ. Left ventricular diastolic function in patients with advanced cystic fibrosis. Chest. (2003) 123:1488–94. doi: 10.1378/chest.123.5.1488
19. Labombarda F, Pellissier A, Ellafi M, Creveuil C, Ribault V, Laurans M, et al. Myocardial strain assessment in cystic fibrosis. J Am Soc Echocardiogr. (2011) 24:1037–45. doi: 10.1016/j.echo.2011.06.004
20. Sellers ZM, McGlocklin L, Brasch A. Strain rate echocardiography uncovers subclinical left ventricular dysfunction in cystic fibrosis. J Cyst Fibros. (2015) 14:654–60. doi: 10.1016/j.jcf.2015.03.010
21. Labombarda F, Saloux E, Brouard J, Bergot E, Milliez P. Heart involvement in cystic fibrosis: a specific cystic fibrosis-related myocardial changes? Respir Med. (2016) 118:31–8. doi: 10.1016/j.rmed.2016.07.011
22. Reverri EJ, Morrissey BM, Cross CE, Steinberg FM. Inflammation, oxidative stress, and cardiovascular disease risk factors in adults with cystic fibrosis. Free Radic Biol Med. (2014) 76:261–77. doi: 10.1016/j.freeradbiomed.2014.08.005
23. Ambrosi P, Chazalettes JP, Viard L, Raynaud M, Faugere G, Noirclerc M, et al. Left ventricular involvement in mucoviscidosis after 2 years of age. Arch Fr Pediatr. (1993) 50:653–6. 8002738.
24. Sayyid ZN, Sellers ZM. Technological advances shed light on left ventricular cardiac disturbances in cystic fibrosis. J Cyst Fibros. (2017) 16:454–64. doi: 10.1016/j.jcf.2017.02.013
25. Eising JB, van der Ent CK, Teske AJ, Vanderschuren MM, Uiterwaal CSPM, Meijboom FJ. Young patients with cystic fibrosis demonstrate subtle alterations of the cardiovascular system. J Cyst Fibros. (2018) 17:643–49. doi: 10.1016/j.jcf.2017.12.009
26. Sciatti E, Vizzardi E, Bonadei I, Valentini F, Menotti E, Prati F, et al. Focus on echocardiographic right ventricular strain analysis in cystic fibrosis adults without cardiovascular risk factors: a case-control study. Intern Emerg Med. (2019) 14:1279–85. doi: 10.1007/s11739-019-02104-5
27. Frustaci A, Sabbioni E, Fortaner S, Farina M, del Torchio R, Tafani M, et al. Selenium- and zinc-deficient cardiomyopathy in human intestinal malabsorption: preliminary results of selenium/zinc infusion. Eur J Heart Fail. (2012) 14:202–10. doi: 10.1093/eurjhf/hfr167
28. Loscalzo J. Keshan disease, selenium deficiency, and the selenoproteome. N Engl J Med. (2014) 370:1756–60. doi: 10.1056/NEJMcibr1402199
29. Bomer N, Grote Beverborg N, Hoes MF, Streng KW, Vermeer M, Dokter MM, et al. Selenium and outcome in heart failure. Eur J Heart Fail. (2020) 22:1415–23. doi: 10.1002/ejhf.1644
30. Tanguy S, Grauzam S, de Leiris J, Boucher F. Impact of dietary selenium intake on cardiac health: experimental approaches and human studies. Mol Nutr Food Res. (2012) 56:1106–21. doi: 10.1002/mnfr.201100766
31. Oropeza-Moe M, Wisløff H, Bernhoft A. Selenium deficiency associated porcine and human cardiomyopathies. J Trace Elem Med Biol. (2015) 31:148–56. doi: 10.1016/j.jtemb.2014.09.011
32. Bjørklund G, Shanaida M, Lysiuk R, Antonyak H, Klishch I, Shanaida V, et al. Selenium: an antioxidant with a critical role in anti-aging. Molecules. (2022) 27:6613. doi: 10.3390/molecules27196613
33. Zheng Y, Xie T, Li S, Wang W, Wang Y, Cao Z, et al. Effects of selenium as a dietary source on performance, inflammation, cell damage, and reproduction of livestock induced by heat stress: a review. Front Immunol. (2022) 12:820853. doi: 10.3389/fimmu.2021.820853
34. Ilhan I, Asci H, Tepebasi MY, Imeci OB, Sevuk MA, Temel EN, et al. Selenium exerts protective effects on inflammatory cardiovascular damage: molecular aspects via SIRT1/p53 and Cyt- c/Cas-3 pathways. Mol Biol Rep. (2023) 50:1627–37. doi: 10.1007/s11033-022-08192-5
35. Shalihat A, Hasanah AN, Mutakin M, Lesmana R, Budiman A, Gozali D. The role of selenium in cell survival and its correlation with protective effects against cardiovascular disease: a literature review. Biomed Pharmacother. (2021) 134(1–8):111125. doi: 10.1016/j.biopha.2020.111125
36. Bomer N, Pavez-Giani MG, Grote Beverborg N, Cleland JGF, van Veldhuisen DJ, van der Meer P. Micronutrient deficiencies in heart failure: mitochondrial dysfunction as a common pathophysiological mechanism? J Intern Med. (2022) 291:713–31. doi: 10.1111/joim.13456
37. Al-Mubarak AA, van der Meer P, Bomer N. Selenium, selenoproteins, and heart failure: current knowledge and future perspective. Curr Heart Fail Rep. (2021) 18:122–31. doi: 10.1007/s11897-021-00511-4
38. Shimada BK, Alfulaij N, Seale LA. The impact of selenium deficiency on cardiovascular function. Int J Mol Sci. (2021) 22:10713. doi: 10.3390/ijms221910713
39. Chen H, Liu LL, Ye LL, McGuckin C, Tamowski S, Scowen P, et al. Targeted inactivation of cystic fibrosis transmembrane conductance regulator chloride channel gene prevents ischemic preconditioning in isolated mouse heart. Circulation. (2004) 110:700–4. doi: 10.1161/01.CIR.0000138110.84758.BB
40. Michalke B. Selenium speciation in human serum of cystic fibrosis patients compared to serum from healthy persons. J Chromatogr A. (2004) 1058:203–8. doi: 10.1016/S0021-9673(04)01416-5
41. Volk DM, Cutliff SA. Selenium deficiency and cardiomyopathy in a patient with cystic fibrosis. J Ky Med Assoc. (1986) 84:222–4. 3722990.3722990
42. Ciofu O, Smith S, Lykkesfeldt J. Antioxidant supplementation for lung disease in cystic fibrosis. Cochrane Database Syst Rev. (2019) 10:CD 007020. doi: 10.1002/14651858.CD007020.pub4
43. Wood LG, Fitzgerald DA, Lee AK, Garg ML. Improved antioxidant and fatty acid status of patients with cystic fibrosis after antioxidant supplementation is linked to improved lung function. Am J Clin Nutr. (2003) 77:150–9. doi: 10.1093/ajcn/77.1.150
44. Li L, Somerset S. Dietary intake and nutritional status of micronutrients in adults with cystic fibrosis in relation to current recommendations. Clin Nutr. (2016) 35:775–82. doi: 10.1016/j.clnu.2015.06.004
Keywords: cystic fibrosis, cardiomyopathy, selenium deficiency, Keshan disease, heart failure
Citation: Segovia-Cubero J, Ruiz-Bautista L, Maiz-Carro L, Girón-Moreno RM, Prados-Sánchez MC, Martínez-Martínez MT, González-Estecha M, Mingo-Santos S, Gómez-Bueno M, Salas-Antón C, Cavero-Gibanel MA, Pastrana-Ledesma M, García-Pavía P, Laporta-Hernández R, Sánchez-Ortiz D and Alonso-Pulpón L (2024) The cardiomyopathy of cystic fibrosis: a modern form of Keshan disease. Front. Cardiovasc. Med. 11:1285223. doi: 10.3389/fcvm.2024.1285223
Received: 29 August 2023; Accepted: 18 January 2024;
Published: 1 February 2024.
Edited by:
Harry Boardman, Milton Keynes University Hosptal, United Kingdom© 2024 Segovia-Cubero, Ruiz-Bautista, Maiz-Carro, Girón-Moreno, Prados-Sánchez, Martínez-Martínez, González-Estecha, Mingo-Santos, Gómez-Bueno, Salas-Antón, Cavero-Gibanel, Pastrana-Ledesma, García-Pavía, Laporta-Hernández, Sánchez-Ortiz and Alonso-Pulpón. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Javier Segovia-Cubero jsecu@telefonica.net