
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
MINI REVIEW article
Front. Cardiovasc. Med. , 08 January 2024
Sec. Cardiovascular Epidemiology and Prevention
Volume 10 - 2023 | https://doi.org/10.3389/fcvm.2023.1301383
This article is part of the Research Topic Reviews in Takotsubo Syndrome View all 5 articles
 Giacomo Tini1*
Giacomo Tini1* Luca Arcari2,3
Luca Arcari2,3 Raffaella Mistrulli1
Raffaella Mistrulli1 Federico Follesa1
Federico Follesa1 Alessandro Cianca1Matteo Sclafani1
Alessandro Cianca1Matteo Sclafani1 Giuliano Tocci1
Giuliano Tocci1 Paolo Spallarossa4
Paolo Spallarossa4 Allegra Battistoni1Luca Cacciotti2
Allegra Battistoni1Luca Cacciotti2 Beatrice Musumeci1Emanuele Barbato1
Beatrice Musumeci1Emanuele Barbato1
Takotsubo syndrome (TTS) is characterized by a transient left ventricular systolic dysfunction, burdened by significant acute and long-term mortality and morbidity. The prognosis of TTS, especially in the long-term, is influenced by both non-cardiovascular (non-CV) and CV comorbidities, among which cancer is one of the most common. The presence of a malignancy is proven to be associated with higher mortality in TTS. Moreover, a number of anticancer treatments has been reported to possibly cause TTS as a form of cardiotoxicity, even though clearcut associations are lacking. The aim of this narrative review is to sum up contemporary knowledge on the association of cancer and TTS, addressing unmet needs and practical implications. The importance of a close collaboration between cardiologists and oncologists is herein highlighted, both to allow an adequate management of the acute TTS phase, and to actively and safely return to the oncologic management once the acute setting is resolved.
Takotsubo syndrome (TTS) is an acute heart failure (HF) condition, characterized by transient left ventricular (LV) systolic dysfunction (1). Alongside the classic “apical ballooning” presentation with mid-to-apical LV akinesia and basal iperkinesia (2), some “atypical” variants have been described: mid-ventricular, basal, and focal (3–5). The clinical presentation of TTS frequently resembles acute myocardial infarction (AMI), with chest pain, electrocardiographic (ECG) abnormalities and increased troponin values. Despite specific non-invasive diagnostic criteria have been proposed (6, 7), a final diagnosis of TTS is typically confirmed after coronary angiography excludes obstructive coronary artery disease as the underlying cause of the regional LV wall motion abnormalities (1, 2, 6). TTS pathophysiology has not been completely disentangled: a multifactorial genesis is likely to be accounted for its development, including catecholamine surge (i.e., an excessive sympathetic activation due to stressors), brain-heart axis alterations, acquired and genetic predisposition (1, 2, 8). At the clinical level, an identifiable trigger is often found as a precipitating factor, either as emotional or physical (i.e., surgery, infection).
Contrary to what initially thought (9–11), TTS is not a benign condition. In the acute phase it can be associated with a significant in-hospital mortality and morbidity. In the long-term, mortality risk has been shown to be similar to that of AMI (1, 12). Notably, this excess in mortality is mostly due to non-cardiovascular (non-CV) causes (2, 13–15). Indeed, the clinical course of TTS is significantly influenced by both non-CV and CV comorbidities. These are not only “contributors” of the clinical picture of vulnerable HF patients typical of TTS, but, most importantly, are prognostic factors (8, 12, 14, 16). Accordingly, TTS secondary to an emotional trigger has a relatively good prognosis, while physically triggered TTS has higher prevalence of non-CV comorbidities (17) and therefore is associated with worse outcomes (11, 17).
Cancer is one of the most common comorbidities in TTS, and a well-defined predictor of mortality (2, 12, 18). It is interesting to note that cancer can underlie both types of triggers, impacting on the emotional-psychological state and causing several physical pathological alterations (i.e., oxidative stress, inflammatory milieu, altered metabolism) (19). Moreover, a number of anticancer treatments have been reported to possibly cause TTS as a form of cardiotoxicity (20, 21). In the broader setting of HF, cancer has received large attention because of both the possible shared mechanisms and risk factors between CV diseases and malignancies, and its impact on tolerability of CV therapies and on prognosis (22, 23).
In this era of precision medicine, during which great improvements in CV and oncologic treatments and better prognosis have been recorded, an integrated approach caring for patients’ bidirectional needs appears fundamental (24, 25). In the case of a comorbid HF and oncologic patient, as each disease influences the management of the other, cooperation of clinicians must be pursued. However, the scientific community mostly focused on prevalence and prognostic impact of cancer in TTS. Reports of TTS in cancer patients are anectodical (i.e., case reports) or retrieved from large databases. The two aspects (cancer in TTS vs. TTS in cancer) are almost always kept separate, and data on optimal management of these cases are lacking. The aim of this narrative review is to sum up contemporary knowledge on these issues, focusing on unmet needs and practical implications.
A systematic revision of 1,109 TTS cases published in 2014 found a 10% mean prevalence of cancer in TTS, ranging from 4% to 29% (16). Similar frequencies were found in subsequent meta-analyses (18, 26, 27). In the three largest international TTS registries, cancer prevalence ranges from about 12% to 17% (17, 28, 29). Overall, cancer in TTS appears more common as compared to the general population, as well as to patients with AMI and HF (27, 30–33). Table 1 shows prevalence of cancer in the main TTS registries published to date. Notably, the definition of cancer may vary from one study to another (i.e., any cancer vs. active cancer).
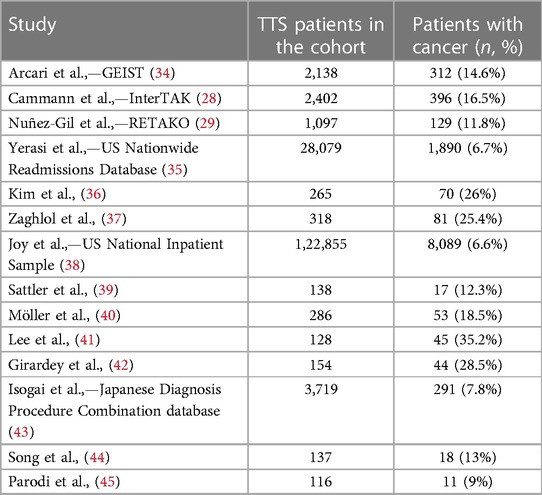
Table 1. Prevalence of cancer in the main TTS registries published to date.
Non-CV and CV comorbidities are the main determinants of outcome in TTS, especially in the long-term (12). Among these, cancer has been evaluated (specifically or among other variables) in several studies, and always resulted as a predictor of mortality at follow-up. In an analysis from the Mayo Clinic, cancer was the single leading cause of death in a cohort of 265 TTS patients (36). Some reports also highlighted the association of cancer with worse in-hospital outcome, further emphasizing how the presence of a malignancy reflects a particularly vulnerable status. Table 2 reports the main studies specifically evaluating the impact of cancer on TTS prognosis. Notably, these studies—with diverse follow-up times—mostly evaluated all-cause mortality or all-cause adverse events. Indeed, CV mortality does not appear to be influenced by cancer (40). Only two studies showed an association between cancer and both all-cause and CV mortality (42, 47).
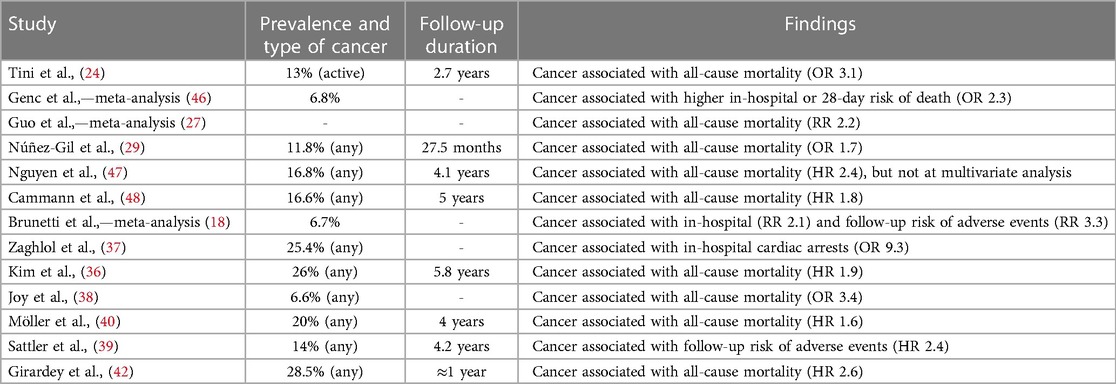
Table 2. Main studies evaluating the impact of cancer on TTS prognosis.
CV management of an oncologic subject suffering TTS may be challenging. Pharmacologic treatment of TTS involves HF drugs (in particular beta blockers and renin-angiotensin system inhibitors), which could be associated with better outcomes (12, 49), but may also be poorly tolerated in cancer (21, 22, 50, 51). Moreover, it has been reported that cancer patients are frequently under-treated in the CV setting (21, 25, 52–54). On the other hand, from an oncologic perspective, chronic CV comorbidities or acute events (as TTS) may be perceived as debilitating when pertaining a cancer patient, possibly impacting delivery of optimal treatments (22, 24, 50). This latter aspect may be alarming when one considers how mortality in TTS is typically comorbidity-related (i.e., cancer-related), and thus it might be enhanced by an oncologic undertreatment due to the acute CV event. Nonetheless, the only analysis to date, though from a small cohort, comparing TTS patients with cancer to a non-TTS matched cancer counterpart, showed similar prognosis in the two groups, suggesting that mortality is unrelated to the TTS event (24).
CV adverse events related to anticancer treatments are defined as “cardiotoxicity”. This term represents a heterogeneous group of conditions, including LV dysfunction and HF, venous thromboembolism, arterial thrombotic events, arrhythmias, myocarditis (20, 55). TTS has been included among this long list of adverse events, due to a range of cancer therapies. The most commonly associated agents are pyrimidines (19, 20), but TTS in patients treated with anti-VEGF agents, cisplatinum, gemcitabine, trastuzumab or anthracyclines has also been reported. Nevertheless, a specific underlying mechanism by which each of such treatments might cause TTS is not known. Moreover, there is a paucity of data concerning dosages and time frame in which TTS develops (19).
In a report from the US National Inpatient Sample database including 1,067,977 patients hospitalized with chemotherapy-related admissions between 2010 and 2014, the incidence of TTS was 53 per 100,000 cases (56). Those developing TTS were more commonly females and had a significantly higher risk of in-hospital mortality as compared to the group that did not develop TTS. This study did not report information regarding the type of treatments received by patients developing TTS.
In a recent meta-summary of 41 case reports of TTS occurring during diverse anticancer treatments, 5-fluorouracil was the most commonly reported drug, in more than one third of cases (57). Patients usually developed TTS a few days after the delivery of the anticancer treatment (median time: 2 days). TTS caused cardiogenic shock in one quarter of cases; at follow-up a complete recovery of LV function was reported in 89% of cases. In another study evaluating 27 cases, 5-fluorouracil was again the anticancer treatment most commonly associated with TTS (41% of cases) (58). TTS tended to develop shortly after the administration of chemotherapy, even hours, and most commonly occurred in women.
The pathogenetic mechanism of pyrimidine-associated TTS is unknown, likewise the overall mechanisms of pyrimidine-associated cardiotoxicity have not been completely elucidated. Coronary vasospasm and microvascular dysfunction have been proposed as putative mechanisms contributing to its pathophysiology, overall and specifically for TTS (59–62). However, few case reports described absence of overt or induced vasospasm during acute episodes of pyrimidine-associated angina or TTS (60, 63). In other cases, either the presence of not hemodynamically significant coronary artery disease was reported, or a history of previous coronary artery disease resulted as a predictor of cardiotoxicity development. In such scenarios plaque instability or vasospasm causing a narrowing of the coronary lumen on top of a pre-existing plaque might not be excluded (19, 64, 65). Finally, recent findings suggest that the main mechanisms of pyrimidine-associated cardiotoxicity are direct vascular (endothelial) and myocardial damage (59, 61). In summary, despite many reports suggest pyrimidines to possibly cause TTS, this association remains hypothetical, as “pure” coronary events cannot be ruled out with certainty.
Discontinuation of the “culprit” treatment is suggested when TTS occurs during anticancer therapy (20). This holds true for pyrimidines; however, a successful rechallenge after a cardiotoxic event has been reported in some cases (62).
In recent years the indications for immune checkpoint inhibitors (ICI) therapy widened, and concurrently there was an exponential increase in reports of ICI-associated cardiotoxicity (66). Outside of the well-known issue of myocarditis, other cardiac adverse events due to ICI have been reported, including atrial fibrillation, myocardial infarction, pericardial effusion and TTS. Through the World Health Organization (WHO) global database of individual case safety reports VigiBase®, 13 reports of TTS in patients receiving ICI drugs emerged (all with ICI monotherapy). Data on clinical evolution was available in eight of the reported cases: one patient died, four recovered LV systolic function, while three others did not (67). ICI-related TTS was observed in seven other case reports (68–74).
As for pyrimidines, a clear mechanism underlying the development of TTS in ICI is unknown. In several cases, an interesting overlap between TTS and myocarditis was described (75). In a registry of 30 ICI-related myocarditis, a “TTS–like appearance” occurred in 14% (76). Bearing in mind that myocarditis is a well-known differential diagnosis of TTS (1), the association of ICI with TTS remains difficult to be clearly confirmed.
After a cardiac adverse event, ICI are usually discontinued, and rechallenge is not recommended. However, this approach is strongly suggested for myocarditis, but there are no clear indications for other types of cardiotoxicities (20, 77). Re-challenge of ICI after cardiotoxicity have been proposed, but few data are available in this regard (78).
TTS due to anticancer treatments is a relatively rare event. However, it may have significant implications. Its occurrence may prompt discontinuation of the oncologic treatment, which may be even definitively halted, given the absence of clear recommendations. However, understanding the true association of a given anticancer treatment with a TTS event may be challenging, considering that the oncologic status itself may be causing TTS, or that TTS might not be diagnosed with certainty (i.e., difficulties in performing a thorough differential diagnosis with other conditions). Indeed, a clearcut association of anticancer drugs with TTS is frequently absent, and in some case reports, LV systolic function recovery is not always present. These diagnostic and nosologic issues appear difficult to overcome. Nevertheless, in clinical practice, the most important aspect remains that of an optimal management of the patient. A close collaboration between cardiologists and oncologists is needed, both to deliver an adequate CV management in the acute phase, and to actively and safely return to the oncologic management once the acute HF setting is overcome. Two aspects are very important and must be considered. First, as oncologists have the task to decide if, when and how to restart an anticancer treatment, cardiologists should be supportive in giving their perspective. Even in the case of a supposed association between TTS and the anticancer treatment, TTS recurrencies are uncommon (79) and should not be the only reason for a treatment to be permanently discontinued (80). Secondly, as for other CV risk factors or prior events, rather than to evaluate their presence vs. absence, it should be considered whether a condition is stable and well-treated, and which was its clinical course (54, 81). This is very important in Cardio-Oncology, where specific CV comorbidities may significantly influence the oncologic management. In a certain way, after the acute TTS phase, the cardiologic perspective should be of reassurance and cooperation toward the oncologist and the oncologic management (24).
The presence of cancer in a TTS patient should be recognized by clinicians as a proxy of a frail status, predisposing to a worse outcome, especially in the long-term. Although this concept might appear easy to understand, it is not as straightforward to translate it into clinical practice and holds significant implications.
Following the resolution of the acute phase, the management of TTS entails a shift from a single specialist (i.e., cardiologist) approach, to a comprehensive, inter- and multi-disciplinary management (82). An integrated treatment of each comorbidity appears fundamental, yet in everyday clinical practice this may not be easy to be pursued. It is worth noting that the high prevalence of cancer in TTS has prompted some Authors to suggest an oncologic screening of these patients (48). However, no clear data have been provided in this regard, and to date, there is no clear indication for performing such a screening.
When TTS occurs in a patient with a malignancy actively treated, the goal of the management after the acute CV phase should be to allow a safe return-to-therapy in the oncologic setting. A close follow-up in the first 3 to 6 months after the acute event, a period during which LV systolic function and ECG completely recover in most cases, must be performed, and a tailored HF therapy (i.e., according to patients' tolerability) must be delivered. During this period, a strict interaction with the oncologist should be maintained to allow initiation or re-initiation of the anticancer treatment. Given the paucity of data on this regard, and the uncertainties on clearcut association of specific anticancer treatments with TTS occurrence, we suggest that (re-)initiation of the oncologic therapy is discussed case-by-case in a multi-disciplinary setting. This means that not only aspects related to the TTS events should be considered, but also those related to the oncologic treatment. Clinicians should face the following questions: has the anticancer treatment possibly caused TTS? What was the clinical course of TTS and has LV systolic function recovered in the short-term? What is the oncologic risk of the patient? Is it feasible for the patient to pause the anticancer treatment (either it is associated with TTS or not) and to possibly re-start it in a few months or is it preferable not to stop the oncologic treatment? Coming up with the best solution to all these issues should be the priority of patient's management once the acute TTS phase has resolved. In most cases, and when the anticancer treatment may be safely paused, initiation or re-initiation of the oncologic therapy may be done after 3 months from the TTS event. With careful management, a re-challenge of the anticancer treatment used before the TTS event may be tested. Once again, the oncologic aspect is crucial in this decision (i.e., is that the best treatment for the patient and the one with the highest expected efficacy or are there any comparable solutions?). On the contrary, observing an uncomplete recovery of LV systolic function should raise concern. Since this is quite unusual in TTS (1), suspicion that myocardial injury (and not TTS) has occurred should be considered. Therefore, in such cases, a modification of the oncologic treatment is more reasonable.
In conclusion, a “holistic” Cardio-Oncology approach (25), dedicated to a multi-disciplinary patient's management (and not limited to the evaluation of cardiotoxicity) appears as the best method to care for TTS patients with cancer.
GT: Conceptualization, Data curation, Methodology, Writing – original draft, Writing – review & editing. LA: Conceptualization, Supervision, Writing – review & editing. RM: Data curation, Writing – review & editing. FF: Data curation, Writing – review & editing. AC: Writing – review & editing. MS: Supervision, Writing – review & editing. GT: Writing – review & editing. PS: Supervision, Writing – review & editing. AB: Writing – review & editing. LC: Supervision, Writing – review & editing. BM: Supervision, Writing – review & editing. EB: Supervision, Writing – review & editing.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Lyon AR, Bossone E, Schneider B, Sechtem U, Citro R, Underwood SR, et al. Current state of knowledge on takotsubo syndrome: a position statement from the taskforce on takotsubo syndrome of the heart failure association of the European society of cardiology: current state of knowledge on takotsubo syndrome. Eur J Heart Fail. (2016) 18:8–27. doi: 10.1002/ejhf.424
2. Medina de Chazal H, Del Buono MG, Keyser-Marcus L, Ma L, Moeller FG, Berrocal D, et al. Stress cardiomyopathy diagnosis and treatment. J Am Coll Cardiol. (2018) 72:1955–71. doi: 10.1016/j.jacc.2018.07.072
3. Cacciotti L, Camastra GS, Beni S, Giannantoni P, Musarò S, Proietti I, et al. A new variant of tako-tsubo cardiomyopathy: transient mid-ventricular ballooning. J Cardiovasc Med. (2007) 8:1052–4. doi: 10.2459/JCM.0b013e32803cab4a
4. Cacciotti L, Camastra GS, Musarò S, Proietti I, Semeraro R, Martina C, et al. Stress cardiomyopathy: transient basal ballooning. J Cardiovasc Med. (2010) 11:764–7. doi: 10.2459/JCM.0b013e328334466c
5. Tini G, Limite LR, Arcari L, Cacciotti L, Russo D, Sclafani M, et al. A systematic review on focal takotsubo syndrome: a not-so-small matter. Heart Fail Rev. (2020) 27:271–80. doi: 10.1007/s10741-020-09988-y
6. Ghadri J-R, Wittstein IS, Prasad A, Sharkey S, Dote K, Akashi YJ, et al. International expert consensus document on takotsubo syndrome (part I): clinical characteristics, diagnostic criteria, and pathophysiology. Eur Heart J. (2018) 39:2032–46. doi: 10.1093/eurheartj/ehy076
7. Prasad A, Lerman A, Rihal CS. Apical ballooning syndrome (tako-tsubo or stress cardiomyopathy): a mimic of acute myocardial infarction. Am Heart J. (2008) 155:408–17. doi: 10.1016/j.ahj.2007.11.008
8. Arcari L, Limite LR, Adduci C, Sclafani M, Tini G, Palano F, et al. Novel imaging and genetic risk markers in takotsubo syndrome. Front Cardiovasc Med. (2021) 8:703418. doi: 10.3389/fcvm.2021.703418
9. Elesber AA, Prasad A, Lennon RJ, Wright RS, Lerman A, Rihal CS. Four-year recurrence rate and prognosis of the apical ballooning syndrome. J Am Coll Cardiol. (2007) 50:448–52. doi: 10.1016/j.jacc.2007.03.050
10. Cacciotti L, Passaseo I, Marazzi G, Camastra G, Campolongo G, Beni S, et al. Observational study on takotsubo-like cardiomyopathy: clinical features, diagnosis, prognosis and follow-up. BMJ Open. (2012) 2. doi: 10.1136/bmjopen-2012-001165
11. Looi J-L, Verryt T, McLeod P, Chan C, Pemberton J, Webster M, et al. Type of stressor and medium-term outcomes after takotsubo syndrome: what becomes of the broken hearted? (ANZACS-QI 59). Heart Lung Circ. (2022) 31:499–507. doi: 10.1016/j.hlc.2021.09.021
12. Sclafani M, Arcari L, Russo D, Tini G, Limite LR, Cacciotti L, et al. Long-term management of takotsubo syndrome: a not-so-benign condition. Rev Cardiovasc Med. (2021) 22:597–611. doi: 10.31083/j.rcm2203071
13. Limite LR, Arcari L, Cacciotti L, Russo D, Musumeci MB. Cardiogenic shock in takotsubo syndrome: a clue to unravel what hides behind the curtain? JACC Heart Fail. (2019) 7:175–6. doi: 10.1016/j.jchf.2018.11.003
14. Rosa GM, Tini G, Porto I. Takotsubo syndrome: lonely hearts. Pol Arch Intern Med. (2020) 130:6–7. doi: 10.20452/pamw.15166
15. Scudiero F, Arcari L, Cacciotti L, De Vito E, Marcucci R, Passaseo I, et al. Prognostic relevance of GRACE risk score in takotsubo syndrome. Eur Heart J Acute Cardiovasc Care. (2020) 9:721–8. doi: 10.1177/2048872619882363
16. Pelliccia F, Parodi G, Greco C, Antoniucci D, Brenner R, Bossone E, et al. Comorbidities frequency in takotsubo syndrome: an international collaborative systematic review including 1109 patients. Am J Med. (2015) 128:654.e11–19. doi: 10.1016/j.amjmed.2015.01.016
17. Pätz T, Santoro F, Cetera R, Ragnatela I, El-Battrawy I, Mezger M, et al. Trigger-associated clinical implications and outcomes in takotsubo syndrome: results from the multicenter GEIST registry. J Am Heart Assoc. (2023) 12:e028511. doi: 10.1161/JAHA.122.028511
18. Brunetti ND, Tarantino N, Guastafierro F, De Gennaro L, Correale M, Stiermaier T, et al. Malignancies and outcome in takotsubo syndrome: a meta-analysis study on cancer and stress cardiomyopathy. Heart Fail Rev. (2019) 24:481–8. doi: 10.1007/s10741-019-09773-6
19. Desai A, Noor A, Joshi S, Kim AS. Takotsubo cardiomyopathy in cancer patients. Cardio-Oncol Lond Engl. (2019) 5:7. doi: 10.1186/s40959-019-0042-9
20. Lyon AR, López-Fernández T, Couch LS, Asteggiano R, Aznar MC, Bergler-Klein J, et al. 2022 ESC guidelines on cardio-oncology developed in collaboration with the European hematology association (EHA), the European society for therapeutic radiology and oncology (ESTRO) and the international cardio-oncology society (IC-OS). Eur Heart J. (2022) 43:4229–361. doi: 10.1093/eurheartj/ehac244
21. Keramida K, Farmakis D, Filippatos G. Cancer and takotsubo syndrome: from rarity to clinical practice. ESC Heart Fail. (2021) 8:4365–9. doi: 10.1002/ehf2.13741
22. Ameri P, Canepa M, Anker MS, Belenkov Y, Bergler-Klein J, Cohen-Solal A, et al. Cancer diagnosis in patients with heart failure: epidemiology, clinical implications and gaps in knowledge. Eur J Heart Fail. (2018) 20:879–87. doi: 10.1002/ejhf.1165
23. Bertero E, Canepa M, Maack C, Ameri P. Linking heart failure to cancer. Circulation. (2018) 138:735–42. doi: 10.1161/CIRCULATIONAHA.118.033603
24. Tini G, Arcari L, Sclafani M, Spallarossa P, Camastra G, Battistoni A, et al. Exploring the influence of takotsubo syndrome on oncologic patients’ mortality. Front Cardiovasc Med. (2022) 9:1020078. doi: 10.3389/fcvm.2022.1020078
25. Tini G, Ameri P, Buzzatti G, Sarocchi M, Murialdo R, Guglielmi G, et al. Diversity of cardiologic issues in a contemporary cohort of women with breast cancer. Front Cardiovasc Med. (2021) 8:654728. doi: 10.3389/fcvm.2021.654728
26. Lu X, Li P, Teng C, Cai P, Jin L, Li C, et al. Prognostic factors of takotsubo cardiomyopathy: a systematic review. ESC Heart Fail. (2021) 8:3663–89. doi: 10.1002/ehf2.13531
27. Guo S, Xie B, Tse G, Roever L, Xia Y, Li G, et al. Malignancy predicts outcome of takotsubo syndrome: a systematic review and meta-analysis. Heart Fail Rev. (2020) 25:513–22. doi: 10.1007/s10741-020-09917-z
28. Cammann VL, Scheitz JF, von Rennenberg R, Jäncke L, Nolte CH, Szawan KA, et al. Clinical correlates and prognostic impact of neurologic disorders in takotsubo syndrome. Sci Rep. (2021) 11:23555. doi: 10.1038/s41598-021-01496-9
29. Núñez-Gil IJ, Vedia O, Almendro-Delia M, Raposeiras-Roubín S, Sionis A, Martin-García AC, et al. Takotsubo syndrome and cancer, clinical and prognostic implications, insights of RETAKO. Med Clin (Barc). (2020) 155:521–8. doi: 10.1016/j.medcli.2020.01.033
30. El-Sayed AM, Brinjikji W, Salka S. Demographic and co-morbid predictors of stress (takotsubo) cardiomyopathy. Am J Cardiol. (2012) 110:1368–72. doi: 10.1016/j.amjcard.2012.06.041
31. Tornvall P, Collste O, Pettersson H. Prevalence and cumulative incidence of cancer, and mortality in patients with takotsubo syndrome with focus on the index event. QJM Mon J Assoc Physicians. (2019) 112:861–7. doi: 10.1093/qjmed/hcz186
32. Iorio A, Senni M, Barbati G, Greene SJ, Poli S, Zambon E, et al. Prevalence and prognostic impact of non-cardiac co-morbidities in heart failure outpatients with preserved and reduced ejection fraction: a community-based study. Eur J Heart Fail. (2018) 20:1257–66. doi: 10.1002/ejhf.1202
33. Khan MS, Samman Tahhan A, Vaduganathan M, Greene SJ, Alrohaibani A, Anker SD, et al. Trends in prevalence of comorbidities in heart failure clinical trials: comorbidities in HF clinical trials. Eur J Heart Fail. (2020) 22:1032–42. doi: 10.1002/ejhf.1818
34. Arcari L, Núñez-Gil IJ, Stiermaier T, El-Battrawy I, Guerra F, Novo G, et al. Gender differences in takotsubo syndrome. J Am Coll Cardiol. (2022) 79:2085–93. doi: 10.1016/j.jacc.2022.03.366
35. Yerasi C, Tripathi B, Banga S, McNown C, Jonnalagadda AK, Al-Qaisi S, et al. Predictors of 90-day readmission and in-hospital mortality in takotsubo cardiomyopathy: an analysis of 28,079 index admissions. Cardiovasc Revasc Med Mol Interv. (2019) 20:973–9. doi: 10.1016/j.carrev.2019.08.004
36. Kim H, Senecal C, Lewis B, Prasad A, Rajiv G, Lerman LO, et al. Natural history and predictors of mortality of patients with takotsubo syndrome. Int J Cardiol. (2018) 267:22–7. doi: 10.1016/j.ijcard.2018.04.139
37. Zaghlol R, Kashyap K-, Al-Shbool G, Basyal B, Desale S, Campia U, et al. Usefulness of malignancy as a predictor of WorseIn-hospital outcomes in patients with takotsubo cardiomyopathy. Am J Cardiol. (2019) 123:995–1001. doi: 10.1016/j.amjcard.2018.11.054
38. Joy PS, Guddati AK, Shapira I. Outcomes of takotsubo cardiomyopathy in hospitalized cancer patients. J Cancer Res Clin Oncol. (2018) 144:1539–45. doi: 10.1007/s00432-018-2661-1
39. Sattler K, El-Battrawy I, Lang S, Zhou X, Schramm K, Tülümen E, et al. Prevalence of cancer in takotsubo cardiomyopathy: short and long-term outcome. Int J Cardiol. (2017) 238:159–65. doi: 10.1016/j.ijcard.2017.02.093
40. Möller C, Stiermaier T, Graf T, Eitel C, Thiele H, Burgdorf C, et al. Prevalence and long-term prognostic impact of malignancy in patients with takotsubo syndrome. Eur J Heart Fail. (2018) 20:816–8. doi: 10.1002/ejhf.868
41. Lee J-H, Uhm J-S, Shin DG, Joung B, Pak H-N, Ko Y-G, et al. Clinical significance of changes in the corrected QT interval in stress-induced cardiomyopathy. Korean J Intern Med. (2016) 31:507–16. doi: 10.3904/kjim.2015.330
42. Girardey M, Jesel L, Campia U, Messas N, Hess S, Imperiale A, et al. Impact of malignancies in the early and late time course of takotsubo cardiomyopathy. Circ J Off J Jpn Circ Soc. (2016) 80:2192–8. doi: 10.1253/circj.CJ-16-0388
43. Isogai T, Yasunaga H, Matsui H, Tanaka H, Ueda T, Horiguchi H, et al. Out-of-hospital versus in-hospital takotsubo cardiomyopathy: analysis of 3719 patients in the diagnosis procedure combination database in Japan. Int J Cardiol. (2014) 176:413–7. doi: 10.1016/j.ijcard.2014.07.110
44. Song BG, Yang HS, Hwang HK, Kang GH, Park YH, Chun WJ, et al. The impact of stressor patterns on clinical features in patients with tako-tsubo cardiomyopathy: experiences of two tertiary cardiovascular centers. Clin Cardiol. (2012) 35:E6–13. doi: 10.1002/clc.22053
45. Parodi G, Bellandi B, Del Pace S, Barchielli A, Zampini L, Velluzzi S, et al. Natural history of tako-tsubo cardiomyopathy. Chest. (2011) 139:887–92. doi: 10.1378/chest.10-1041
46. Genc A, Gilis-Malinowska N, Kasprzyk P, Gasecka A, Perdyan A, Kacperczyk J, et al. Malignancy predicts short-term mortality in takotsubo: insights from a meta-analysis of 125 359 patients. ESC Heart Fail. (2021) 8:4357–9. doi: 10.1002/ehf2.13428
47. Nguyen TH, Stansborough J, Ong GJ, Surikow S, Price TJ, Horowitz JD. Antecedent cancer in takotsubo syndrome predicts both cardiovascular and long-term mortality. Cardio-Oncol Lond Engl. (2019) 5:20. doi: 10.1186/s40959-019-0053-6
48. Cammann VL, Sarcon A, Ding KJ, Seifert B, Kato K, Di Vece D, et al. Clinical features and outcomes of patients with malignancy and takotsubo syndrome: observations from the international takotsubo registry. J Am Heart Assoc. (2019) 8:e010881. doi: 10.1161/JAHA.118.010881
49. Silverio A, Parodi G, Scudiero F, Bossone E, Di Maio M, Vriz O, et al. Beta-blockers are associated with better long-term survival in patients with takotsubo syndrome. Heart. (2022) 108:1369–76. doi: 10.1136/heartjnl-2021-320543
50. Tini G, Sarocchi M, Tocci G, Arboscello E, Ghigliotti G, Novo G, et al. Arterial hypertension in cancer: the elephant in the room. Int J Cardiol. (2019) 281:133–9. doi: 10.1016/j.ijcard.2019.01.082
51. Gevaert SA, Halvorsen S, Sinnaeve PR, Sambola A, Gulati G, Lancellotti P, et al. Evaluation and management of cancer patients presenting with acute cardiovascular disease: a clinical consensus statement of the acute CardioVascular care association (ACVC) and the ESC council of cardio-oncology-part 2: acute heart failure, acute myocardial diseases, acute venous thromboembolic diseases, and acute arrhythmias. Eur Heart J Acute Cardiovasc Care. (2022) 11:865–74. doi: 10.1093/ehjacc/zuac107
52. Teece L, Sweeting MJ, Hall M, Coles B, Oliver-Williams C, Welch CA, et al. Impact of a prior cancer diagnosis on quality of care and survival following acute myocardial infarction: retrospective population-based cohort study in England. Circ Cardiovasc Qual Outcomes. (2023) 16:383–97. doi: 10.1161/CIRCOUTCOMES.122.009236
53. Chow YW, Pietranico R, Mukerji A. Studies of oxygen binding energy to hemoglobin molecule. Biochem Biophys Res Commun. (1975) 66:1424–31. doi: 10.1016/0006-291x(75)90518-5
54. Tini G, Sarocchi M, Ameri P, Arboscello E, Spallarossa P. The need for cardiovascular risk factor prevention in cardio-oncology. JACC Heart Fail. (2019) 7:367–8. doi: 10.1016/j.jchf.2019.01.002
55. Tini G, Tocci G, Battistoni A, Sarocchi M, Pietrantoni C, Russo D, et al. Role of arterial hypertension and hypertension-mediated organ damage in cardiotoxicity of anticancer therapies. Curr Heart Fail Rep. (2023) 20:56–62. doi: 10.1007/s11897-023-00590-5
56. Desai R, Abbas SA, Goyal H, Durairaj A, Fong HK, Hung O, et al. Frequency of takotsubo cardiomyopathy in adult patients receiving chemotherapy (from a 5-year nationwide inpatient study). Am J Cardiol. (2019) 123:667–73. doi: 10.1016/j.amjcard.2018.11.006
57. Carbone A, Bottino R, Russo V, D’Andrea A, Liccardo B, Maurea N, et al. Takotsubo cardiomyopathy as epiphenomenon of cardiotoxicity in patients with cancer: a meta-summary of case reports. J Cardiovasc Pharmacol. (2021) 78:e20–9. doi: 10.1097/FJC.0000000000001026
58. Coen M, Rigamonti F, Roth A, Koessler T. Chemotherapy-induced takotsubo cardiomyopathy, a case report and review of the literature. BMC Cancer. (2017) 17:394. doi: 10.1186/s12885-017-3384-4
59. Yuan C, Parekh H, Allegra C, George TJ, Starr JS. 5-FU Induced cardiotoxicity: case series and review of the literature. Cardio-Oncol Lond Engl. (2019) 5:13. doi: 10.1186/s40959-019-0048-3
60. Grunwald MR, Howie L, Diaz LA. Takotsubo cardiomyopathy and fluorouracil: case report and review of the literature. J Clin Oncol Off J Am Soc Clin Oncol. (2012) 30:e11–14. doi: 10.1200/JCO.2011.38.5278
61. Focaccetti C, Bruno A, Magnani E, Bartolini D, Principi E, Dallaglio K, et al. Effects of 5-fluorouracil on morphology, cell cycle, proliferation, apoptosis, autophagy and ROS production in endothelial cells and cardiomyocytes. PloS One. (2015) 10:e0115686. doi: 10.1371/journal.pone.0115686
62. Padegimas A, Carver JR. How to diagnose and manage patients with fluoropyrimidine-induced chest pain: a single center approach. JACC CardioOncology. (2020) 2:650–4. doi: 10.1016/j.jaccao.2020.06.012
63. Y-Hassan S, Tornvall P, Törnerud M, Henareh L. Capecitabine caused cardiogenic shock through induction of global takotsubo syndrome. Cardiovasc Revasc Med Mol Interv. (2013) 14:57–61. doi: 10.1016/j.carrev.2012.10.001
64. Aleksova A, Gagno G, Pierri A, Todaro C, Fluca AL, Orlando V, et al. What the cardiologist needs to consider in the management of oncologic patients with STEMI-like syndrome: a case report and literature review. Pharm Basel Switz. (2021) 14:563. doi: 10.3390/ph14060563
65. Chong JH, Ghosh AK. Coronary artery vasospasm induced by 5-fluorouracil: proposed mechanisms, existing management options and future directions. Interv Cardiol Lond Engl. (2019) 14:89–94. doi: 10.15420/icr.2019.12
66. Spallarossa P, Sarocchi M, Tini G, Arboscello E, Toma M, Ameri P, et al. How to monitor cardiac complications of immune checkpoint inhibitor therapy. Front Pharmacol. (2020) 11:972. doi: 10.3389/fphar.2020.00972
67. Ederhy S, Dolladille C, Thuny F, Alexandre J, Cohen A. Takotsubo syndrome in patients with cancer treated with immune checkpoint inhibitors: a new adverse cardiac complication. Eur J Heart Fail. (2019) 21:945–7. doi: 10.1002/ejhf.1497
68. Anderson RD, Brooks M. Apical takotsubo syndrome in a patient with metastatic breast carcinoma on novel immunotherapy. Int J Cardiol. (2016) 222:760–1. doi: 10.1016/j.ijcard.2016.07.291
69. Geisler BP, Raad RA, Esaian D, Sharon E, Schwartz DR. Apical ballooning and cardiomyopathy in a melanoma patient treated with ipilimumab: a case of takotsubo-like syndrome. J Immunother Cancer. (2015) 3:4. doi: 10.1186/s40425-015-0048-2
70. Airò G, Maffezzoli M, Lazzarin A, Bianconcini M, Greco A, Buti S, et al. Takotsubo syndrome in a patient with metastatic renal cell carcinoma treated with pembrolizumab plus axitinib. Immunotherapy. (2022) 14:1297–305. doi: 10.2217/imt-2022-0013
71. Monti M, Cortesi P, Vespignani R, Bronico I, Gallio C, Flospergher M, et al. Takotsubo syndrome (TTS) in onco-hematologic patients: retrospective analysis and focus on the correlation or not with anticancer drugs. Case reports and review of the literature. Front Oncol. (2022) 12:875391. doi: 10.3389/fonc.2022.875391
72. Tan NYL, Anavekar NS, Wiley BM. Concomitant myopericarditis and takotsubo syndrome following immune checkpoint inhibitor therapy. BMJ Case Rep. (2020) 13:e235265. doi: 10.1136/bcr-2020-235265
73. Khan NAJ, Pacioles T, Alsharedi M. Atypical takotsubo cardiomyopathy secondary to combination of chemo-immunotherapy in a patient with non-small cell lung cancer. Cureus. (2020) 12:e9429. doi: 10.7759/cureus.9429
74. Camastra G, Arcari L, Ciolina F, Danti M, Cacciotti L. Cardiac magnetic resonance imaging of transient myocardial dysfunction in a patient treated with checkpoint-targeted immunotherapy. Eur J Cancer. (2021) 144:389–91. doi: 10.1016/j.ejca.2020.11.026
75. Arcari L, Tini G, Camastra G, Ciolina F, De Santis D, Russo D, et al. Cardiac magnetic resonance imaging in immune check-point inhibitor myocarditis: a systematic review. J Imaging. (2022) 8:99. doi: 10.3390/jimaging8040099
76. Escudier M, Cautela J, Malissen N, Ancedy Y, Orabona M, Pinto J, et al. Clinical features, management, and outcomes of immune checkpoint inhibitor–related cardiotoxicity. Circulation. (2017) 136:2085–7. doi: 10.1161/CIRCULATIONAHA.117.030571
77. Schneider BJ, Naidoo J, Santomasso BD, Lacchetti C, Adkins S, Anadkat M, et al. Management of immune-related adverse events in patients treated with immune checkpoint inhibitor therapy: ASCO guideline update. J Clin Oncol. (2021) 39:4073–126. doi: 10.1200/JCO.21.01440
78. Park R, Lopes L, Saeed A. Outcomes following immunotherapy re-challenge after immune-related adverse event: systematic review and meta-analysis. Immunotherapy. (2020) 12:1183–93. doi: 10.2217/imt-2020-0103
79. Arcari L, Cacciotti L, Limite LR, Russo D, Sclafani M, Semeraro R, et al. Clinical characteristics of patients with takotsubo syndrome recurrence: an observational study with long-term follow-up. Int J Cardiol. (2021) 329:23–7. doi: 10.1016/j.ijcard.2020.12.047
80. Giza DE, Lopez-Mattei J, Vejpongsa P, Munoz E, Iliescu G, Kitkungvan D, et al. Stress-induced cardiomyopathy in cancer patients. Am J Cardiol. (2017) 120:2284–8. doi: 10.1016/j.amjcard.2017.09.009
81. Tini G, Sarocchi M, Sirello D, Murialdo R, Fornarini G, Buzzatti G, et al. Cardiovascular risk profile and events before and after treatment with anti-VEGF drugs in the setting of a structured cardio-oncologic program. Eur J Prev Cardiol. (2020) 28(9):e38–40. doi: 10.1177/2047487320923056
Keywords: takotsubo syndrome, cancer, cardiotoxicity, anticancer treatments, Cardio-Oncology
Citation: Tini G, Arcari L, Mistrulli R, Follesa F, Cianca A, Sclafani M, Tocci G, Spallarossa P, Battistoni A, Cacciotti L, Musumeci B and Barbato E (2024) A contemporary update on cancer and takotsubo syndrome. Front. Cardiovasc. Med. 10:1301383. doi: 10.3389/fcvm.2023.1301383
Received: 24 September 2023; Accepted: 18 December 2023;
Published: 8 January 2024.
Edited by:
Tomohiro Hayashi, Kobe University, JapanReviewed by:
Agnes S. Kim, UCONN Health, United States© 2024 Tini, Arcari, Mistrulli, Follesa, Cianca, Sclafani, Tocci, Spallarossa, Battistoni, Cacciotti, Musumeci and Barbato. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Giacomo Tini Z2lhY29tby50aW5pbWVsYXRvQHVuaXJvbWExLml0
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.