
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
BRIEF RESEARCH REPORT article
Front. Cardiovasc. Med. , 08 January 2024
Sec. Heart Failure and Transplantation
Volume 10 - 2023 | https://doi.org/10.3389/fcvm.2023.1297900
This article is part of the Research Topic Insights in Heart Failure and Transplantation: 2023 View all 9 articles
 Jiří Plášek1,2*
Jiří Plášek1,2* Jozef Dodulík1Marie Lazárová1
Jozef Dodulík1Marie Lazárová1 David Stejskal3,4Zdeněk Švagera3,4
David Stejskal3,4Zdeněk Švagera3,4 Nela Chobolová3Patrik Šulc1Lukáš Evin1,2
Nela Chobolová3Patrik Šulc1Lukáš Evin1,2 Dana Purová5Jan Václavík1,2
Dana Purová5Jan Václavík1,2
Background: Secretoneurin (SN) is a neuropeptide with potential utility as a biomarker of cardiovascular episodes. The main effect of SN is mediated through its inhibition of calmodulin-dependent kinase II (CaMKII), which influences calcium handling. We aimed to associate the levels of SN in plasma with different causes of heart failure.
Methods: We prospectively enrolled consecutive patients with ischaemic (ICM) and dilated (DCM) cardiomyopathy from the outpatient heart failure clinic and healthy individuals. SN was analysed from venous blood by use of the ELISA method. SN plasma levels were compared in DCM, ICM and healthy individuals with non-parametric tests.
Results: A total of 53 patients (81.1% male, 18.9% female; mean age 67.9 ± 12.6 years) and 34 healthy individuals (38% male, 62% female) were included in the analysis. Plasma SN levels were significantly higher in the dilated cardiomyopathy (38.8 ± 27 pmol/L) as compared with the ischaemic cardiomyopathy (19.7 ± 22.6 pmol/L) group (P = 0.006). There was no significant difference between females vs. males (27.1 ± 23 vs. 25.5 ± 26.2 pmol/L, P = NS). Plasma SN levels allowed DCM and ICM to be differentiated with 88% sensitivity and 61% specificity (P = 0.007), the cut of value is 13.3 pmol/L. Plasma SN levels differed significantly between healthy volunteers and both ICM (P < 0.0001) and DCM (P = 0.049). Plasma SN levels did not differ according to age and were not associated with comorbidities, left ventricular ejection fraction, heart failure medication, troponin, creatinine, or natriuretic peptide plasma levels.
Conclusion: Plasma secretoneurin levels differed significantly in DCM vs. ICM, being higher in the former. Based on plasma SN levels, discrimination between DCM and ICM might be possible. Healthy individuals produce higher SN plasma levels than stable HFrEF patients.
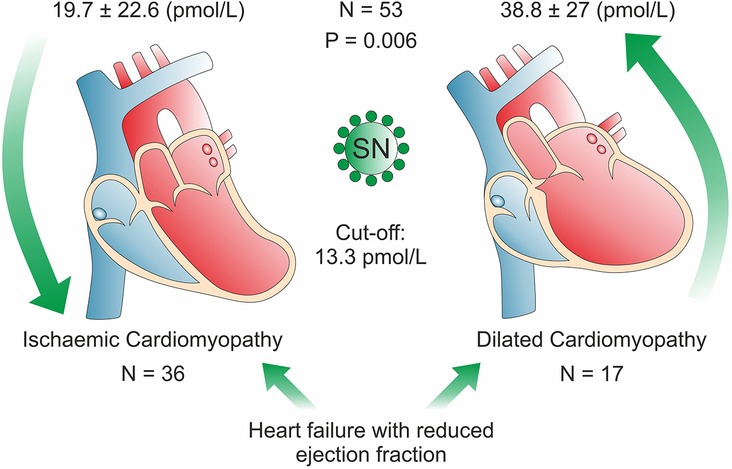
Graphical Abstract.
Secretoneurin (SN) is a 33–amino acid neuropeptide from the chromogranin peptide family. SN may be a novel biomarker with potential use in cardiovascular medicine (1). Its pathway differs from those of the most often measured natriuretic peptides and troponin. SN's main effects are most likely transmitted by calmodulin-dependent kinase II (CaMKII). However, other cellular pathways may play a role (2). Since CaMKII is one of the regulators of calcium handling in the cell, it may enhance protective effects of SN in the diseased myocardium (3). CaMKII inhibition in the myocardium improves contraction and suppresses proneness to arrhythmia by diminishing calcium leakage from the sarcoplasmic reticulum (3). Calcium is crucial to myocardial excitation-contraction coupling and intracellular signalling. Since in heart failure patients, the calcium handling is known to be disrupted, the SN plasma levels may entail prognostic information (4).
Of note, in the recent sub-analysis of the GISSI-HF trial in patients with chronic heart failure, SN concentrations were associated with mortality, even after adjusting for multiple factors (5). SN levels were also weakly associated with admission to the hospital for cardiovascular reasons (5).
We already know that SN levels may contain prognostic information in heart failure (HF) patients. Therefore, we aim to address possible differences in the SN levels associated mainly with the HF aetiology.
For this study, we prospectively enrolled 53 consecutive patients from the heart failure outpatient clinic of University Hospital Ostrava from August 2022 to January 2023 and 34 heathy volunteers in October 2023. The study sample comprised only patients with a reduced ejection fraction of two causes (ischaemic cardiomyopathy, dilated cardiomyopathy). All patients were in stabilized condition without recent heart failure decompensation. All patients with dilated cardiomyopathy have no coronary artery disease (no coronary artery stenosis ≥ 70% or 50% of the common trunk of the left coronary artery). Acute myocardial infarction and/or coronary artery by-pass grafting surgery within three months before enrolment were exclusion criteria.
The healthy volunteers were without any treated disease. Most importantly, no cardiac disease was present, defined by the absence of clinical symptoms, normal echocardiography, and normal plasma levels of markers of cardiac injury at the time of blood sampling. This study was approved by the Institutional Review Board of University Hospital Ostrava (Nr. 526/2022) and conducted in accordance with the Helsinki Declaration. All patients have signed informed consent.
Blood sampling was performed in patients with chronic stable heart failure during outpatient visits. SN was analysed from venous blood by use of the ELISA method (CardiNor AS, Oslo, Norway) (6). The blood was drawn into the lithium-heparin tubes, plasma was separated and frozen to −70°C, only one defrosting cycle was allowed. The intra-assay coefficients of variation for SN were lower than 5% and inter-assay coefficient lower than 10%. The level of determination (LoD) for the CardiNor SN is 5,1 pmol/L, The level of quantification (LoQ) is 7,6 pmol/L. Analytical range is 11,8–299,2 pmol/L.
Continuous variables are expressed as mean ± standard deviation or as median and interquartile range when indicated and compared by the Mann–Whitney U test since the data were non-normally distributed according to both the Kolmogorov-Smirnov and Levene's tests. Categorical variables are expressed as percentages and compared by the chi-square test, Fisher's exact test, or logistic regression, as appropriate. Correlations between SN levels and other biomarkers were examined by Spearman correlation. The difference between plasma SN levels in ICM vs. DCM or healthy individuals was examined by Kruskal-Wallis or Mann–Whitney U tests. Receiver operating characteristics analysis was performed for SN discriminative abilities related to the cause of heart failure. A two-tailed α < 0.05 was considered statistically significant. All analyses were performed using IBM SPSS for Mac version 23 (IBM, Armonk, USA).
A total of 53 HFrEF patients (81.1% male, 18.9% female) aged 67.9 ± 12.6 with a BMI of 27.7 ± 4.4 and 34 healthy individuals (38% male, 62% female) were included in the analysis. Mean SN values (pmol/L) according to the cause of heart failure were 19.7 ± 22.6 for ischaemic cardiomyopathy (N = 36), 38.8 ± 27 for dilated cardiomyopathy (N = 17) (7); the median and IQR were as follows ICM: 13.3(29.6), DCM: 34.4 (27.2) pmol/L. Mean SN values for health individuals were 50.7 ± 15.3 pmol/L. The mean left ventricular ejection fraction (LV EF) in HFrEF patients was 29.7 ± 6.6. Comorbidities, anthropometric factors, medication, mean levels of biomarkers and plasma electrolytes are depicted in Table 1.
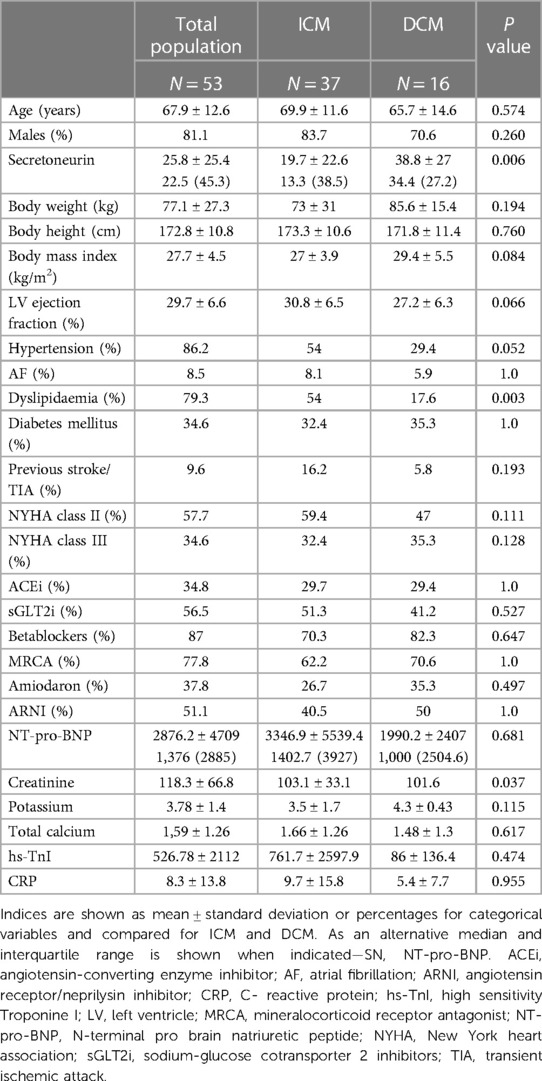
Table 1. Baseline characteristics of the study population, ischemic (ICM) vs. Dilated cardiomyopathy (DCM).
SN plasma levels differed significantly in the dilated cardiomyopathy (DCM) as compared with the ischemic cardiomyopathy (ICM) group (P = 0.006, Figure 1), irrespective of NYHA class, heart failure pharmacotherapy and LV EF. In the multivariable analysis, SN still differed significantly between ICM and DCM, even after entering LV EF, age, heart failure treatment and hypertension/gender as covariates in the regression model. On the contrary, LV EF did not differ significantly between the DCM and the ICM group (27.2 ± 6.3 vs. 30.8 ± 6.5, P = NS). The presence/absence of outliers in both groups did not change the test result, what means that the significance or non-significance of the test was not different; the outliers stayed in the analysis. Coronary artery by-pass grafting surgery was done 24.1% of the ICM patients, all of them more than one year before the SN plasma levels sampling. There was no difference between SN plasma levels in females and males, respectively (27.1 ± 23 vs. 25.5 ± 26.2 pmol/L, P = NS); the median and IQR for females/males 26.8 (49.8), 22.4 (41.3) pmol/L, respectively. The ICM vs. DCM group differ in Dyslipidaemia (P = 0.003) and creatinine level (P = 0.036). The groups did not differ in age, anthropometric factors, diabetes, cerebrovascular accidents, NYHA class, LV EF, analytes, or HF medication (Table 1). Moreover, SN levels were able to discriminate dilated cardiomyopathy from ischemic cardiomyopathy as causation with 88% sensitivity and 61% specificity (AUC 0.73, 95% CI 0.58–0.87, P = 0.007, Figure 2), the cut-off value is 13.3 pmol/L. Of note, plasma SN did not vary according to age and was not associated with comorbidities, left ventricular ejection fraction, troponin, creatinine, or natriuretic peptide levels in plasma. There were also no significant correlations between SN and N-terminal pro natriuretic peptide (NT-pro-BNP), high-sensitivity troponin (hs-TnI), creatinine, natrium, total calcium or potassium plasma levels.
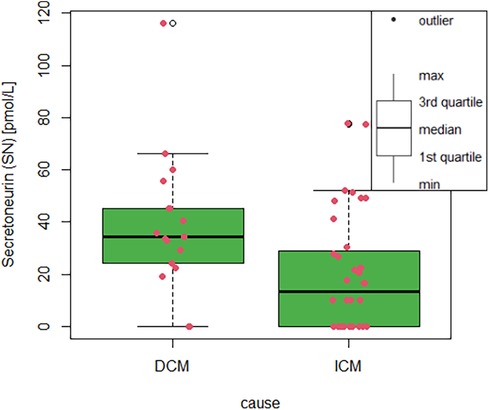
Figure 1. Box-plot with whiskers displaying differences in SN plasma level between ICM and DCM. The red dots stand for individual measurement value. Secretoneurin (SN) plasma levels in pmol/L according to the cause of heart failure; ICM, ischaemic cardiomyopathy; DCM, dilated cardiomyopathy.
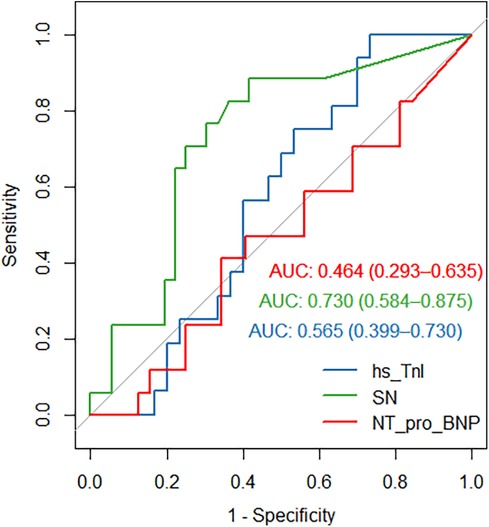
Figure 2. Receiver operating curve (ROC) for secretoneurin (SN, green curve), high-sensitivity troponin I (hs-TnI, blue curve) and N-terminal-pro natriuretic peptide (NT-pro-BNP, red curve) differentiating dilated cardiomyopathy from ischaemic cardiomyopathy (SN, AUC 0.73, 95% CI 0.58–0.87, P = 0.007; TnI, AUC 0.56, 95% CI 0.4–0.73, P = NS;NT-pro-BNP, AUC 0.44, 95% CI 0.27–0.62, P = NS).
There is also no significant difference between total calcium between ICM and DCM (Table 1). However, there is a significant difference in calcium levels between the whole HFrEF group and the healthy individuals (P = 0.0001).
Our healthy volunteers (N = 34, 62% females, Table 2) have SN plasma levels of 50.7 ± 15.3 pmol/L, which was significantly higher than in both DCM (P = 0.049) and ICM (P < 0.0001) or HFrEF (ICM/DCM combined), P < 0.0001. Males and females in the healthy individuals' group did not differ in any parameters (Table 2). We have not observed myocardial injury in any of the healthy individuals (Table 2). Our healthy volunteers were also significantly younger (P < 0.0001) and differed in the BMI (P < 0.0001), being lower in the healthy individuals as compared to the HFrEF group.
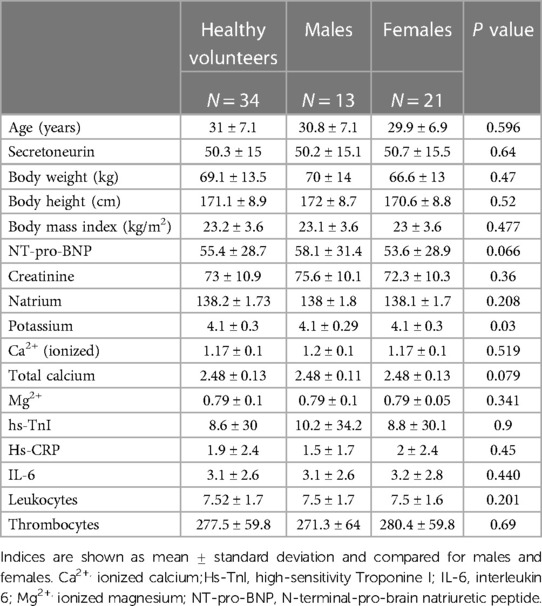
Table 2. Baseline characteristics of the healthy volunteers
SN plasma levels in healthy individuals were not associated with total or ionized calcium, hs-CRP, IL-6, pH, hs-TnI, NT-pro-BNP, or albumin level. Plasma levels of SN did not vary according to the age, sex, anthropometric parameters, thrombocytes, haemoglobin, or leukocytes in the healthy individuals (P = NS). Potassium and ionized magnesium levels were borderline non-significant when associated to the SN plasma levels (P = 0.064, P = 0.065, respectively).
The main findings of our preliminary analysis can be summarized as follows:
(1) We found plasma SN levels to be significantly higher in patients with dilated cardiomyopathy than in patients with ischaemic cardiomyopathy.
(2) Plasma SN levels were able to differentiate between DCM and ICM with 88% sensitivity and 61% specificity with a cut-off value 13.3 pmol/L.
(3) Plasma SN levels differed significantly in healthy volunteers as compared to ICM or DCM, healthy volunteers produced higher plasma SN.
(4) Plasma SN levels did not differ according to age or sex and were not associated with comorbidities, left ventricular ejection fraction, troponin, creatinine, or natriuretic peptide levels in plasma.
SN takes part in many processes, namely: apoptosis, immune response, inflammation/chemotaxis, endothelium relaxation, calcium handling, arrhythmogenesis, and cell cycle regulation (2). The broad range of biological effects, independent from classical overload markers such as N-terminal pro-brain natriuretic peptide (NT-pro-BNP) or troponin, suggests that SN is a potentially useful biomarker in cardiology (8). SN has been studied in catecholaminergic polymorphic ventricular arrhythmia, in which it was moderately elevated irrespective of arrhythmogenic episodes (8). SN seems to be a marker reflecting particular cellular mechanism of specific disease than the clinical episodes itself. This pattern of differentiating a type of a disease (ICM vs. DCM), we have observed also in our analysis.
In patients after coronary artery bypass graft (CABG) surgery, SN levels were significantly higher in non-survivors as compared with survivors (173 vs. 143 pmol/L) (9).
The cut-off value for increased mortality risk is >204 pmol/L in patients with aortic stenosis (10). Moreover, in critically ill patients in the intensive care unit, SN was able to predict mortality on top of classical risk factors (11).
In our study, SN levels were somewhat lower than those observed in patients with CABG, critically ill patients, or patients with aortic stenosis before replacement, most of whom were in advanced heart failure or dying (9–11). The reason for lower SN levels in our trial might be the stable state of most of our heart failure patients, who are not comparable to critically ill patients, patients after coronary bypass surgery or younger healthy individuals. On the contrary, in the stable condition of the ICM and/or DCM HFrEF patients are producing even significantly less SN than the healthy individuals in our analysis. Of note, our healthy volunteers were significantly younger but with comparable body size to the HF group.
Moreover, all the previous studies predicted hard clinical endpoints as all-cause or cardiovascular mortality in severe disease states in a completely different patient population compared to our study, differentiating the cause of the disease in stable heart failure.
There are two trials from the same study group evaluating SN in acute and chronic heart failure. In acute heart failure, SN levels were closely associated with mortality. Moreover, SN reclassified patients to their correct risk strata on top of other predictors of mortality (3). In more recent trial in patients with chronic heart failure, SN concentrations were also able to stratify the patients to favourable and poor prognosis on multivariable analysis (5, 12). The SN levels in the chronic HF trial (42;35–62.8 pmol/L) were also very close to our own observations (5, 12).
None of these trials however analysed different SN levels according to the aetiology of HF, ischemic aetiology was only used as an adjusting factor to predict mortality in chronic HF (5, 12). In addition, these trials did not include their own healthy individual subgroup to compare the SN plasma levels with the HF population. Consequently, it is more complicated to draw any conclusion on basal SN secretion patterns in a particular disease specific subgroup of patients. The common denominator of SN elevation in critically ill patients (3, 8–11) is probably tissue ischemia since the studied population otherwise differed in multiple factors. On the contrary, the basal secretion in the fully compensated state may be specific to the underlying disease.
The discriminative capacity of SN with AUC around 0.7 may seem low, though the confidence interval is quite narrow (0.5–0.8). We also must keep in mind that our whole cohort constituted of patients with HFrEF, and no other biomarker has been able to discriminate between the causes of heart failure (ROC curve for hs-TnI and NT-pro BNP are shown in Figure 2). In general, the main goal of biomarkers in heart failure is to provide information regarding the magnitude of risk, and they can also be used to monitor the effects of changes in treatment and detect subclinical disease (13). Although in many of these applications is the utility of SN not clear at the present time, we hope to provide information in the near future on the development of plasma SN levels through time and in response to changes in heart failure treatment. It is becoming clearer, that SN has the capacity to risk stratify and predict the mortality risk in patients with acute and chronic heart failure (3, 5, 12). It is less evident however, whether SN will be able to reflect treatment changes in HF or HF progression. Based on our results SN may also differentiate the ICM vs. DCM cause of heart failure.
We may only speculate that the higher plasma SN levels in DCM, as compared with those in ICM represent more molecularly advanced heart failure and/or impaired calcium handling. Whether higher plasma levels in our study will also predict higher mortality or more frequent heart failure hospitalizations will be revealed in the follow-up. The other, somewhat contradictory, explanation may be that higher plasma SN levels in DCM may be a surrogate for cardiomyocyte's regenerative activity.
Potentially, the SN discriminative capacity (ICM vs. DCM) may be used in the initial heart failure differential diagnosis if confirmed by more extensive trials from different investigator groups.
However, up to now, every elevation of plasma SN levels has led to a worse prognosis in different disease states (8–12). Though all the predictive capacity was limited to acute or critical patient status.
The possible explanation for different SN plasma levels will probably be at the cellular and subcellular levels. In a study with patients with advanced heart failure, ICM and DCM have significantly different molecular profiles (14). DCM (non-ischemic) samples have 32 differentially expressed profiles, and ICM samples have 185 differentially expressed proteins compared to non-failing heart samples (14). The most enriched proteins in ICM are serum amyloid A1, lipopolysaccharide-binding protein, and activated protein C, which are biomarkers associated with coronary artery disease (15, 16). Conversely, non-ischemic enriched proteins are primarily involved in the mitochondrial membrane respiratory chain (14). Also, the extracellular matrix (ECM), a critical component interacting with cells and modulating tissue functions, is different in ICM and DCM (non-ischemic) (14). In DCM, ECM has predominantly interstitial collagen deposition; in ICM, fibrotic replacement is more likely (17). Most interestingly, specific abnormalities in calcium handling have been demonstrated depending on the etiology of HF. ICM is associated with a decreased rate of calcium uptake into the sarcoplasmic reticulum (SR), while DCM is associated with a decreased rate of calcium release from the SR (18).
In our trial, there was no difference in calcium levels between ICM and DCM. However, both groups were hypocalcaemic as compared to healthy individuals. Severe hypocalcaemia may even be the sole cause of heart failure (19). Moreover, in patients after myocardial infarction, low serum calcium may result in a higher mortality rate (20). Extracellular calcium levels may, however not reflect the cytosolic free calcium and related calcium handling in the sarcoplasmic reticulum (21).
All these factors and many unknowns may influence the plasmatic levels of SN in DCM vs. ICM.
Also, our trial confirmed the independence of plasma SN levels from troponin I and NT-pro-BNP levels in plasma, both in HFrEF ICM/DCM patients and healthy individuals. Our results are, at this point, hypothesis-generating at best. Plasma SN levels must be associated with clinical events to show its predictive capacity. Since we have not collected enough clinical events yet, we cannot state whether SN has or has not the prognostic capacity in HFrEF patients. To capture the relationship between calcium handling and SN, the association of ionized calcium plasma levels may be sampled and correlated with SN plasma levels in future trials.
Our sample was small and unbalanced for sex, with male predominance in the heart failure group and female predominance in the healthy volunteer group. Moreover, there were more patients with ischemic cardiomyopathy than with dilated cardiomyopathy. These results cannot be extrapolated to different patient population (different cardiomyopathies) or acute state of the heart failure.
Plasma secretoneurin levels differed significantly in DCM vs. ICM, being higher in the former. Moreover, discrimination between DCM and ICM might be possible based on plasma SN levels. Healthy individuals produce higher SN plasma levels than stable HFrEF patients.
The raw data supporting the conclusions of this article will be made available by the authors upon reasonable request and in compliance with the General Data Protection Rule (GDPR).
The studies involving humans were approved by Etická komise FN Ostrava (eticka.komise@fno.cz). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
JP: Conceptualization, Data curation, Formal analysis, Supervision, Writing – original draft, Writing – review & editing. JD: Conceptualization, Investigation, Methodology, Resources, Writing – review & editing. ML: Conceptualization, Investigation, Methodology, Project administration, Resources, Writing – review & editing. DS: Methodology, Project administration, Supervision, Validation, Writing – review & editing. ZŠ: Conceptualization, Funding acquisition, Methodology, Project administration, Writing – review & editing. NC: Investigation, Methodology, Project administration, Resources, Writing – review & editing. PŠ: Investigation, Methodology, Writing – review & editing. LE: Investigation, Methodology, Validation, Writing – review & editing. DP: Data curation, Formal analysis, Visualization, Writing – review & editing. JV: Project administration, Supervision, Validation, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article.
The study was supported by the Ministry of Health, Czech Republic, for the conceptual development of a research organization (FNOs/2022).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Anderson ME. Will secretoneurin be the next big thing. J Am Coll Cardiol. (2015) 65(4):352–4. doi: 10.1016/j.jacc.2014.11.028
2. Plášek J, Lazárová M, Dodulík J, Šulc P, Stejskal D, Švagera Z, et al. Secretoneurin as a novel biomarker of cardiovascular episodes: are we there yet? A narrative review. J Clin Med. (2022) 11(23):7191. doi: 10.3390/jcm11237191
3. Ottesen AH, Louch WE, Carlson CR, Landsverk OJB, Kurola J, Johansen RF, et al. Secretoneurin is a novel prognostic cardiovascular biomarker associated with cardiomyocyte calcium handling. J Am Coll Cardiol. (2015) 65:339–51. doi: 10.1016/j.jacc.2014.10.065
4. Luo M, Anderson ME. Mechanisms of altered Ca2+ handling in heart failure. Circ Res. (2013) 113(6):690–708. doi: 10.1161/CIRCRESAHA.113.301651
5. Røsjø H, Meessen J, Ottesen AH, Latini R, Omland T, GISSI HF investigators. Prognostic value of secretoneurin in chronic heart failure. Data from the GISSI-heart failure trial. Clin Biochem. (2023) 118:110595. doi: 10.1016/j.clinbiochem.2023.110595
6. Aakre KM, Ottesen AH, Strand H, Faaren AL, Alaour B, Torsvik J, et al. Biologial variation of secretoneurin; a novel cardiovascular biomarker implicated in arrhythmogenesis. Clin Biochem. (2021) 98:74–7. doi: 10.1016/j.clinbiochem.2021.09.014
7. Dodulík J, Václavík J, Lazarová M, Šulc P, Evin L, Stejskal D, et al. Secretoneurin plasma levels in patients with different etiologies of heart failure: preliminary data—abstracts of the heart failure 2023 and the world congress on acute heart failure, 20–23 May 2023, Prague, Czechia. Eur J Heart Fail. (2023) 25(S2):144. doi: 10.1002/ejhf.2927
8. Ottesen AH, Carlson CR, Eken OS, Sadredini M, Myhre PL, Shen X, et al. Secretoneurin is an endogenous CaMKII inhibitor that attenuates Ca2+-dependent arrhythmia. Circ Arrhythm Electrophysiol. (2019) 12:007045. doi: 10.1161/CIRCEP.118.007045
9. Brynildsen J, Petäjä L, Myhre PL, Lyngbakken MN, Nygård S, Stridsberg M, et al. Circulating secretoneurin concentrations after cardiac surgery: data from the FINNish acute kidney injury heart study. Crit Care med. (2019) 47(5):e412–9. doi: 10.1097/CCM.0000000000003670
10. Brynildsen J, Myhre PL, Lynbakken MN, Klaeboe LG, Sridsberg M, Christensen G, et al. Circulating secretoneurin concentrations in patients with moderate to severe aortic stenosis. Clin Biochem. (2019) 71:17–23. doi: 10.1016/j.clinbiochem.2019.06.008
11. Røsjø H, Stridsberg M, Ottesen AH, Nygård S, Christensen G, Pettilä V, et al. Prognostic value of secretoneurin in critically ill patients with infections. Crit Care. (2016) 44(10):1882–90. doi: 10.1097/CCM.0000000000001832
12. Rosjo H, Meessen J, Ottesen AH, Omland H, GISSI-HF study. Circulating secretoneurin concentrations provide independent prognostic information to established risk indices in patients with chronic heart failure. Eur Heart J. (2022) 43(2):ehac544.912. doi: 10.1093/eurheartj/ehac544.912
13. Miller WL, Jaffe AS. Biomarkers in heart failure: the importance of inconvenient details. ESC Heart Fail. (2016) 3(1):3–10. doi: 10.1002/ehf2.12071
14. Zhao Y, Godier-Furnemont A, Bax NAM, Bouten CVC, Brown LM, Vunjak-Novakonic G. Changes in extracellular matrix in failing human non-ischemic nad ischemic hearts with mechanical unloading. J Mol Cell Cardiol. (2022) 166:137–51. doi: 10.1016/j.yjmcc.2022.02.003
15. Kosuge M, Ebina T, Ishikawa T, Hibi K, Tsukara K, Okuda J, et al. Serum amyloid A is a better predictor of clinical outcomes than C-reative protein in non-ST-segment elevation acute coronary syndromes. Circ J. (2007) 71(2):186–90. doi: 10.1253/circj.71.186
16. Lepper PM, Kleber ME, Grammer TB, Hoffmann K, Dietz S, Winkelmann BR, et al. Lipopolysaccharide-binding protein (LBP) is associated with total and cardiovascular mortality in individuals with or without stable coronary artery disease—results from the ludwigshafen risk and cardiovascular health study (LURIC). Atherosclerosis. (2011) 219(1):291–7. doi: 10.1016/j.atherosclerosis.2011.06.001
17. Frangogiannis NG. The extracellular matrix in ischemic and nonischemic heart failure. Circ Res. (2019) 125(1):117–46. doi: 10.1161/CIRCRESAHA.119.311148
18. Sen L, Cui G, Fonarow GS, Laks H. Differences in mechanisms of SR dysfunction in ischemic vs. idiopathic dilated cardiomyopathy. Am J Physiol Heart Circ Physiol. (2000) 279(2):H709–18. doi: 10.1152/ajpheart.2000.279.2.H709
19. Baqi DH, Ahmed SF, Baba HO, Fattah FH, Salih AM, Ali RM, et al. Hypocalcemia as a cause of reversible heart failure: a case report and review of the literature. Ann Med Surg. (2022) 77:103572. doi: 10.1016/j.amsu.2022.103572
20. Schmitz T, Thilo Ch, Linseisen J, Heier M, Peters A, Kuch B, et al. Low serum calcium is associated with higher long-term mortality in myocardial infarction patients from a population-based registry. Sci Rep. (2021) 11(1):2476. doi: 10.1038/s41598-021-81929-7
Keywords: secretoneurin, heart failure, CaMKII, dilated cardiomyopathy, ischaemic cardiomyopathy
Citation: Plášek J, Dodulík J, Lazárová M, Stejskal D, Švagera Z, Chobolová N, Šulc P, Evin L, Purová D and Václavík J (2024) Secretoneurin levels are higher in dilated cardiomyopathy than in ischaemic cardiomyopathy: preliminary results. Front. Cardiovasc. Med. 10:1297900. doi: 10.3389/fcvm.2023.1297900
Received: 20 September 2023; Accepted: 14 December 2023;
Published: 8 January 2024.
Edited by:
Matteo Cameli, University of Siena, ItalyReviewed by:
Elena Revuelta-López, Germans Trias i Pujol Health Science Research Institute (IGTP), Spain© 2024 Plášek, Dodulík, Lazárová, Stejskal, Švagera, Chobolová, Šulc, Evin, Purová and Václavík. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jiří Plášek amlyaS5wbGFzZWtAZm5vLmN6
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.