 Maximillian A. Rogers
Maximillian A. Rogers Giuseppe Tarantini
Giuseppe Tarantini Verena Veulemans
Verena Veulemans
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
EDITORIAL article
Front. Cardiovasc. Med. , 02 August 2023
Sec. Heart Valve Disease
Volume 10 - 2023 | https://doi.org/10.3389/fcvm.2023.1260522
This article is part of the Research Topic Case Reports in Heart Valve Disease: 2022 View all 11 articles
Editorial on the Research Topic
Case reports in heart valve disease: 2022
Heart valve disease affects tens of millions of people worldwide (1), greatly impacting loss of function, quality of life, and mortality. Each year we learn more about conditions impacting patients with the aim of better identifying, treating, and reducing this significant global health burden. 2022 continued this aim, with 10 interesting case reports being published that enhanced our knowledge of these areas, summarized in Table 1. Heart valve disease can originate from bacterial infections as well as valve functional and degenerative causes. In low- and middle-income countries, rheumatic heart disease that results from damage to heart valves caused by rheumatic fever incidents is the most common form of heart valve disease. Whereas functional and degenerative valvular diseases predominate in high-income countries (1). The case reports in this collection span these conditions, giving a large array of heart valve disease causes, identification, and treatment recommendations relevant to heart valve clinicians and scientists around the world. A high impact was reached by this collection with thousands of article views and downloads in the past year.
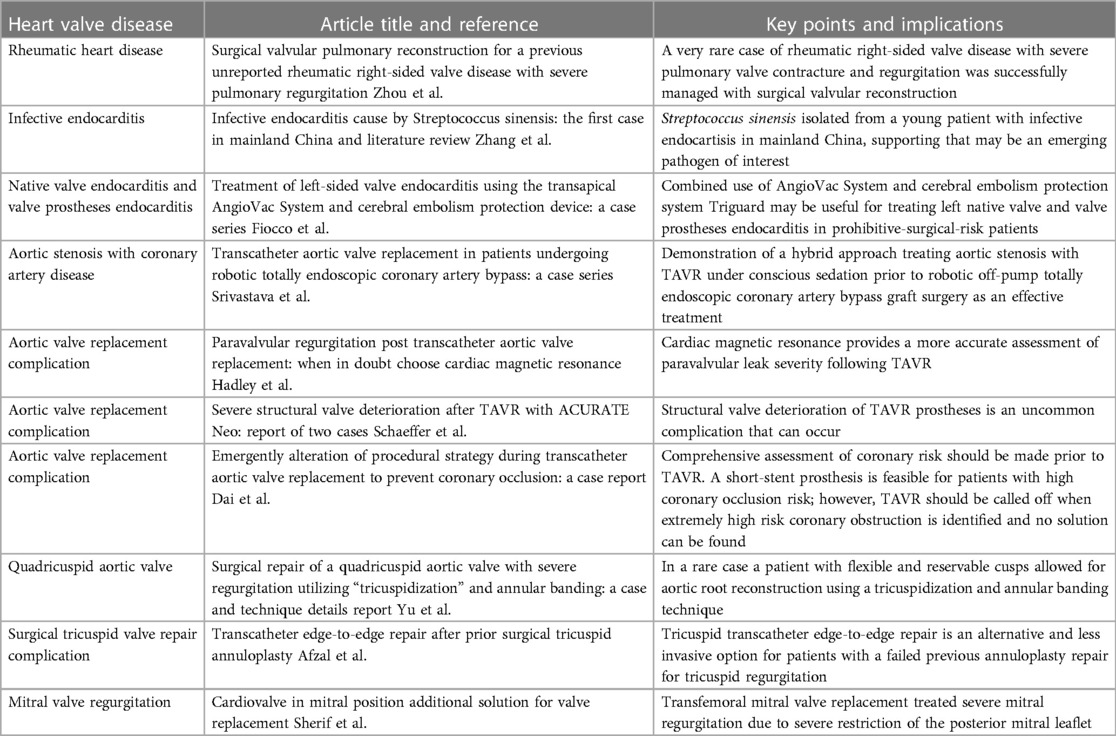
Table 1. Summary of 2022 case reports in heart valve disease.
Understanding emerging causes, effective treatments as well as gaps enables the clinical and research communities to best address heart valve disease originating from bacterial infections. Rheumatic heart disease, an autoimmune inflammatory reaction with streptococci has been almost eradicated in several parts of the world. However, it remains the most common cardiovascular disease in children and young people worldwide, impacting vulnerable communities in sub-Saharan Africa, the Middle East, South-East Asia, and Western Pacific. Despite declining rheumatic heart disease burden, the 2015 Global Burden of Disease study estimated 29.7–43.1 million cases and about 300,000 associated deaths (2). Early diagnosis through means like echocardiography when prophylaxis is most likely to be effective in treating patients is a major strategy in managing this disease (3). Beyond early prevention, knowing treatment options likely to benefit patients, particular with less commonly observed complications is of importance. In this collection, Zhou et al. report a successfully managed case of rheumatic right-sided valve disease, a rarely affected tissue that may result in severe rheumatic pulmonary regurgitation, by surgical valvular reconstruction.
Infective endocarditis occurs by infection of the endocardial surfaces of the heart and can be fatal if not treated. The annual incidence is estimated at 3–10/100,000 and has a mortality of up to 30%, with Staphylococcus aureus being the most prevalent cause followed by streptococci infection (4). Zhang et al. report a case of infective endocarditis in mainland China associated with streptococcus sinensis, contributing to an increasing number of cases reported with this emerging pathogen. Surgery is used in acute heart failure following large vegetations, but a substantial number of patients have high surgical risk necessitating alternatives that have low or acceptable risk for patients. One alternative is the AngioVac System for mass removal. Also in this collection of case reports, Fiocco et al. present a case series with AngioVac System utilization and the cerebral embolism protective system Triguard. These authors validate this hybrid approach by treating prohibitive-surgical-risk patients in a way that reduces cerebral embolization risk stemming from this mass removal system.
Transcatheter aortic valve replacement (TAVR) is a minimally invasive procedure used frequently in high-income countries to treat aortic stenosis patients who are at risk for death from surgery. TAVR has also been suggested to be noninferior to surgery in low-surgical-risk patients (5). TAVR may also be combined with other procedures, as exemplified by Srivastava et al., who report a case series in which TAVR was safely completed prior to coronary revascularization for patients with coronary artery disease and aortic stenosis. Although highly effective, TAVR is not entirely without risk. Paravalvular leak is a complication that can follow TAVR, and one with which Hadley et al. provide support of using cardiac magnetic resonance to more accurately assess. While uncommon, structural valve deterioration of TAVR prostheses is another concern, as shown in the cases reported by Schaeffer et al. in this collection. Coronary occlusion is another uncommon but fatal complication of TAVR, which Dai et al. highlight the importance of performing a comprehensive coronary risk assessment to avoid. The management of coronary artery disease with severe aortic stenosis is particularly important with extension of transcatheter aortic valve implantation to younger and lower-risk patients, discussed in detail in a consensus statement on this topic (6). Quadricuspid aortic valve is a rare congenital disease, in which most patients are treated with aortic valve replacement. However, valve reconstruction can be an alternative to replacement. In this collection, Yu et al. report a case in which tricuspidization and annular banding technique was applied in a patient with cusps that allowed for corrective reconstruction. In addition to the aortic valve, both surgical and minimally invasive procedures are used to treat patients with other forms of heart valve disease. Surgical tricuspid valve repair is another lifesaving procedure but is also with risk. Tricuspid regurgitation may occur following surgical tricuspid valve repair, and Afzal et al. report a case where tricuspid transcatheter edge-to-edge repair was successfully used in a patient with massive tricuspid regurgitation after surgery. Mitral regurgitation is similarly a risk factor for mortality, and Sherif et al. support minimally invasive transcatheter mitral valve replacement to correct this condition.
Knowing the major and emerging causes of heart valve disease, and how to effectively treat them with minimal risk to patients is paramount to achieving declines in patient mortality. While the reports here represent a single or in some instances a small series of cases, they add to that larger goal by providing the heart valve community with greater knowledge on rare conditions as well as best practices to reduce patient treatment risks.
MR: Writing – original draft, Writing – review & editing. GT: Writing – review & editing. VV: Writing – review & editing.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The handling editor EA declared a past collaboration with the author MR.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Coffey S, Roberts-Thomson R, Brown A, Carapetis J, Chen M, Enriquez-Sarano M, et al. Global epidemiology of valvular heart disease. Nat Rev Cardiol. (2021) 18:853–64. doi: 10.1038/s41569-021-00570-z
2. Watkins DA, Johnson CO, Colquhoun SM, Karthikeyan G, Beaton A, Bukhman G, et al. Global, regional, and national burden of rheumatic heart disease, 1990–2015. N Engl J Med. (2017) 377:713–22. doi: 10.1056/NEJMoa1603693
3. Kumar RK, Antunes MJ, Beaton A, Mirabel M, Nkomo VT, Okello E, et al. Contemporary diagnosis and management of rheumatic heart disease: implications for closing the gap: a scientific statement from the American heart association. Circulation. (2020) 142:e337–57 doi: 10.1161/CIR.0000000000000921
4. Rajani R, Klein JL. Infective endocarditis: a contemporary update. Clin Med (Lond). (2020) 20:31–5 doi: 10.7861/clinmed.cme.20.1.1
5. Popma JJ, Deeb GM, Yakubov SJ, Mumtaz M, Gada H, O’Hair D, et al. Transcatheter aortic-valve replacement with a self-expanding valve in low-risk patients. N Engl J Med. (2019) 380:1706–15 doi: 10.1056/NEJMoa1816885
6. Tarantini G, Tang G, Fovino LN, Blackman D, Van Mieghem NM, Kim WK, et al. Management of coronary artery disease in patients undergoing transcatheter aortic valve implantation. A clinical consensus statement from the European association of percutaneous cardiovascular interventions in collaboration with the ESC working group on cardiovascular surgery. EuroIntervention. (2023) 19:37–52. doi: 10.4244/EIJ-D-22-00958
Keywords: aortic valve disease, TAVR, infective endocarditis, rheumatic heart diease, mitral valve, aortic stenosis, coronary artery disease
Citation: Rogers MA, Tarantini G and Veulemans V (2023) Editorial: Case reports in heart valve disease: 2022. Front. Cardiovasc. Med. 10:1260522. doi: 10.3389/fcvm.2023.1260522
Received: 18 July 2023; Accepted: 24 July 2023;
Published: 2 August 2023.
Edited and Reviewed by: Elena Aikawa, Harvard Medical School, United States
© 2023 Rogers, Tarantini and Veulemans. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Maximillian A. Rogers bWF4YXJvZ2Vyc0BnbWFpbC5jb20=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.