 Julia Stehli
Julia Stehli Sarah Zaman2,3
Sarah Zaman2,3 Barbara E. Stähli
Barbara E. Stähli- 1Department of Cardiology, University Hospital Zurich, Zurich, Switzerland
- 2Westmead Applied Research Centre, Faculty of Medicine and Health, University of Sydney, Sydney, NSW, Australia
- 3Department of Cardiology, Westmead Hospital, Sydney, NSW, Australia
- 4Faculty of Medicine, University of Zurich, Zurich, Switzerland
This review gives an overview of sex-based differences in aortic valve stenosis, spanning from pathophysiological mechanisms and disease progression, clinical presentation, presence of comorbidities, and diagnostic assessment, to treatment and outcomes. In particular, sex-related differences in the degree of aortic valve calcification, the response of the left ventricle to pressure overload, as well as in the referral to procedures, with women being less frequently referred for surgical aortic valve replacement and experiencing longer waiting times for transcatheter procedures, will be discussed. Sex-related differences are also particularly evident in outcomes of patients with severe aortic stenosis undergoing surgical or transcatheter procedures. The apparent sex paradox seen in women undergoing transcatheter aortic valve implantation refers to the phenomenon of women experiencing higher rates of short-term mortality and bleeding events, but demonstrating improved long-term survival as compared to men. Women who undergo surgical aortic valve replacement have generally worse outcomes as compared to men, which is reflected by the inclusion of female sex in surgical risk calculation scores. Hence, a thorough understanding of sex-related differences in aortic valve stenosis is important to provide optimal and personalized patient care.
Introduction
Aortic stenosis (AS) is highly prevalent and known to increase in prevalence with age (1). In the elderly, severe AS is present in 3.4% of the population and any degree of AS in up to 12.4% (2). Interestingly, sex distribution differs across age subgroups. In younger patients there is a male predominance, primarily due to the prevalence of bicuspid aortic valve (AV) disease (3, 4). However, women represent the majority of patients with severe AS over 80 years of age (2, 5).
Pathophysiology
The development of AS shares several pathophysiological similarities with atherosclerosis. Endothelial damage sets off a cascade of processes involving lipid accumulation, inflammation, the development of fibrotic alterations, and finally calcification (6). Interestingly, it has been observed that women with similar hemodynamic AS severity show a lower degree of AV calcification than men (7). It is therefore of utmost importance to consider sex-specific threshold values for the definition of severe AS by means of computed tomography (CT) measurement of AV calcification. The [European Society of Cardiology (ESC)] guidelines suggest cutoffs of >3,000 AU in men and >1,600 AU in women as “highly likely” for severe AS. Calcium scoring of >2,000 AU in men and >1,200 AU in women “likely” represent severe AS, whereas values of <1,600 AU in men and <800 AU in women most likely do not represent severe AS (8). This discrepancy in the degree of AV calcification persists even after accounting for the smaller size (body, heart, and aorta) of women, with severe AV calcification relative to the aortic annulus area defined as ≥300 Agatston unit (AU)/cm2 in women and ≥500 AU/cm2 in men (9). When accounting for the lower CT calcium score at baseline, female sex has been identified as independent predictor of AV calcification progression (10). Notably, in patients undergoing transcatheter aortic valve implantation (TAVI), a significant increase in mortality risk was observed with higher AV calcium scores among women. Every 500 AU increase in AV calcium was associated with a 7% increase in mortality risk in women, while no significant association was observed in men (11).
The response of the left ventricle to pressure overload may also demonstrate sex-related differences, however, results are conflicting. In an analysis performed in patients waiting for surgical aortic valve replacement (SAVR), women more frequently exhibited left ventricular concentric remodeling as compared to men which more often displayed eccentric left ventricular remodeling (12). However, in a study enrolling elderly patients scheduled for TAVI, no differences between sexes were observed in left ventricular remodeling patterns as assessed by CT scans (13), although smaller left ventricular volumes and mass were observed for women, even after indexing to body surface area (13).
Another difference is the development of a more diffuse fibrosis pattern within the myocardium in women as compared to the higher level of focal fibrosis in men (14). This could be the reason that women exhibit more often reduced left ventricular compliance, higher left ventricular filling pressures, increased left atrial volume indexes, and consequentially more advanced left ventricular diastolic dysfunction and higher rates of heart failure with preserved left ventricular ejection fraction (12, 15). This remodeling pattern may promote the development of paradoxical low-flow AS in women and emphasizes the importance of considering sex-specific factors in the assessment and management of patients with AS and heart failure. Indeed, sex specific cut-off values for indexed stroke volume have been proposed (40 ml/m2 for men and 32 ml/m2 for women) (16). Alongside increased myocardial fibrosis, differences in ventricular remodeling may also be influenced by the higher prevalence of hypertension in women and possible interactions with sex hormones (17).
Symptoms and presentation
Women with severe AS tend to receive their diagnosis at later ages as compared to men (15), and they are less likely to have concomitant coronary artery disease, peripheral arterial disease, and amyloid cardiomyopathy (17, 18). When presenting with severe AS, even when the severity of AS is similar, women experience a greater symptom burden (15, 19). This includes a higher incidence of exertional dizziness and more pronounced dyspnea. Women also tend to have an increased level of frailty at the time of presentation, which is a known risk factor for worse outcomes in these patients (19–21).
Prognosis and treatment
Even the presence of mild stenotic AV changes is associated with a 50% higher risk of myocardial infarction and cardiovascular death (6). Once severe AS has developed and patients become symptomatic, rates of mortality rise to more than 30% per year if AS is left untreated (22). Similar mortality rates of women and men with untreated severe AS have been observed (22, 23).
There are data pointing towards an undertreatment of patients with severe AS. In a large US cohort of 43,000 patients diagnosed with severe AS between 2008 and 2016, only 28% of patients underwent SAVR or TAVI within one year of diagnosis (22). Even after adjusting for clinical characteristics, socioeconomic status, and access to healthcare, women were 20% less likely than men to undergo AV replacement, including both SAVR and TAVI (15). Further, women appear to be referred at a later stage of the disease compared to men (15).
Transcatheter aortic valve implantation
Current guidelines recommend TAVI as a Class I indication for patients over 65 year years of age (American College of Cardiology (ACC)/American Heart Association (AHA)) or over 75 years of age ESC who are at high or prohibitive risk for SAVR and suitable candidates for transfemoral TAVI (8, 24). Based on these guidelines, approximately 290,000 elderly individuals with severe AS may qualify as candidates for TAVI and yearly around 27,000 become eligible for TAVI (2). It needs to be taken into account that although females represent half of the patients included in registries (25, 26), women have consistently been underrepresented in large TAVI trials, with only 33%–47% of participants being females (27–29).
Among the women who underwent any kind of AV procedure, a higher proportion received TAVI as compared to men (22, 25). Women undergoing TAVI were mostly older and had higher levels of frailty than men, but fewer comorbidities (21). Further, longer waiting times to undergo TAVI, including longer work-up and procedural waiting times, were observed in women, even after adjustment for comorbidities and age (19). The lower referral rates of women for SAVR as well as the longer waiting times for TAVI may at least in part represent health care system-related delays. However, whilst it is possible that the risk of women with severe AS may be underestimated, as it has been documented in coronary artery disease (30, 31), it is also possible that women themselves contribute to prolonged waiting times due to potential misinterpretation of symptoms and their roles as caregivers in the society (32).
In terms of procedural outcomes, no differences in procedural success were observed between men and women undergoing TAVI (26). However, it is worth noting that female sex is associated with a higher incidence of major bleeding and major vascular access site complications (25, 33, 34). In a recently published post hoc analysis of the Antiplatelet Therapy for Patients Undergoing Transcatheter Aortic Valve Implantation (POPular TAVI) trial, the influence of sex on bleeding and ischemic complications following TAVI was examined, taking into account the specific antiplatelet and anticoagulation regimens used (35). This analysis showed that the overall incidence of bleeding events did not differ between women and men, but women exhibited a higher occurrence of major or life-threatening bleedings as compared to men. An interesting observation of this study was the differential effect of antithrombotic treatment on bleeding events in women and men. Specifically, women who received aspirin both before and after TAVI had a higher incidence of major or life-threatening bleeding as compared to men (35). Several mechanisms have been suggested to account for post-TAVI bleeding, encompassing intrinsic bleeding abnormalities that go beyond the platelet system (36). These mechanisms may differ from those observed in patients with coronary artery disease who undergo percutaneous coronary intervention, where bleeding issues are also more prevalent in women (37). Since coexistence of epicardial coronary artery disease among patients with AS is common and both pathologies lead to similar symptoms, decisions making regarding treatment of either AS or coronary artery disease or both remains a challenge. This is particularly true since treatment for coronary artery disease will require dual antiplatelet therapy, increasing the risk of bleeding in women undergoing TAVI (35). Further clarification on which patients are more susceptible to bleeding after TAVI might arise from subanalyses of data derived from the Global Study Comparing a Rivaroxaban-based Antithrombotic Strategy to an Antiplatelet-based Strategy after Transcatheter Aortic Valve Replacement to Optimize Clinical Outcomes (GALILEO) (38).
Following TAVI, more women than men were discharged to rehabilitation facilities, likely due to a higher level of frailty observed in women as compared to men (19, 21).
Short-term mortality and rates of readmission following TAVI have decreased over time across both women and men (34). Despite these improvements, women undergoing TAVI continue to have higher rates of in-hospital mortality and 90-day readmission as compared with men (39). The higher bleeding rates could explain at least in part the higher short-term mortality that was observed in women in multiple analyses (26, 33, 34). Despite increased rates of bleeding and vascular access site complications as well as an excess short-term mortality, multiple observational studies and meta-analyses pointed towards better mid- and long-term survival among women who undergo TAVI as compared to men (40). However, whether sex-related differences in long-term survival after TAVI do exist remains to be determined, as recent analyses of large randomized trials in high- and intermediate-risk patients undergoing TAVI with newer generation transcatheter heart valves have revealed no sex-related differences in survival (20). Changing demographics of enrolled patients, the utilization of newer-generation transcatheter heart valves with smaller delivery systems, more accurate valve sizing techniques, as well as increasing operator experience may have substantially impacted on outcomes in women and men after TAVI. Consistently, observational analyses confirmed a decrease in mortality rates following TAVI over time, however, mortality rates decreased to a greater extent in men than in women (60% vs. 50%) (34). The ongoing randomized controlled Randomized researcH in womEn All Comers With Aortic Stenosis (RHEIA) trial, comparing SAVR and TAVI specifically in women, will provide important insights into this topic (41).
Worse outcomes for women undergoing TAVI were observed in specific vulnerable subsets of patients, including those with low-gradient low-ejection fraction AS. In this patient cohort, women undergoing TAVI exhibited significantly higher rates of mortality as compared to men (17, 23). This disparity in long-term survival could be attributed to the distinct and sex-specific left ventricular remodeling pattern induced by pressure overload.
Other subgroups of patients in which women had an increased mortality were very elderly, frail patients as well as those with pulmonary hypertension (21, 42). The longer waiting times for TAVI observed in women were also associated with higher rates of mortality and hospitalizations for heart failure and reduced mobility (19).
A comparable symptomatic benefit after TAVI has been reported for women and men, with similar improvements in quality of life (evaluated by the Kansas City Cardiomyopathy Questionnaire) observed following TAVI, which is an interesting finding, given the increased age and the higher prevalence of frailty as well as reduced mobility observed in women (43).
Surgical aortic valve replacement
The impact of sex on outcomes following SAVR remains a subject of ongoing debate. Various analyses have reported worse outcomes for women undergoing SAVR, including an excess short-term mortality, an increased need for postoperative blood products, and a longer hospital stay (44, 45). However, women are also older and have more advanced disease at the time of surgery as compared to men, which is likely one of the causes for the increased mortality observed after SAVR in women (22). Other factors that may contribute to these sex-related differences are increased frailty, a higher prevalence of patient prosthesis mismatch due to smaller aortic annular dimensions, a higher incidence of paradoxical low-flow AS, and an increased need for permanent pacemaker implantation in women (23). In some analyses, female sex itself has been identified as independent predictor of mortality and morbidity following SAVR (46). Consequentially, female sex is included in the widely used Society of Thoracic Surgeons (STS) and EuroSCORE surgical risk prediction tools (47, 48).
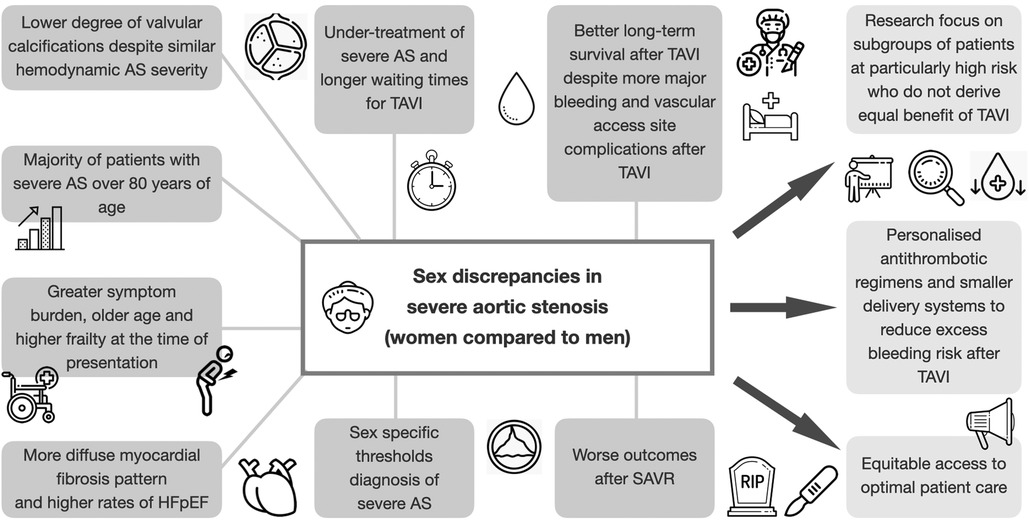
CENTRAL ILLUSTRATION. Sex-related discrepancies and future directions in severe aortic stenosis. AS, aortic stenosis; HFpEF, heart failure with preserved ejection fraction; SAVR, surgical aortic valve replacement; TAVI, transcatheter aortic valve implantation.
As discussed above, outcomes after TAVI seem to exhibit less mortality differences between women and men, suggesting that TAVI may mitigate some of the sex-specific disparities observed in SAVR.
Summary and future directions
In conclusion, sex-related differences are evident from the pathophysiology of AS to clinical presentation, treatment, and outcomes (Central illustration). Aortic stenosis in women is characterized by a lower degree of valvular calcifications and a more diffuse myocardial fibrosis pattern. TAVI has been proven to be an effective treatment option for women with severe AS, contributing to improved survival rates in the mid- to long-term, despite an increased risk of bleeding and procedural complications. However, not all subsets of women seem to derive equal benefit from TAVI. Research should focus on these specific subgroups of patients at particularly high risk, including those with low-gradient, low-ejection fraction AS or those with higher levels of frailty.
To improve outcomes of patients with severe AS, sex specific thresholds for earlier and improved AS diagnosis in women are necessary. Future research is warranted to advance our understanding of sex-specific AV calcification and left ventricular remodeling processes, as well as to develop personalized antithrombotic regimens aiming at reducing the excess bleeding risk of women. Differences in patient referral need to be investigated to ensure equitable access to optimal patient care for women and men with severe AS. Thereby, personalized treatment strategies for patients with severe AS can be developed and outcomes improved.
Author contributions
JS: Conceptualization, Methodology, Visualization, Writing—original draft, Writing—review & editing. SZ: Writing—review & editing. BS: Supervision, Writing—review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. GBD 2017 Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: a systematic analysis for the global burden of disease study 2017. Lancet. (2018) 392(10159):1789–858. doi: 10.1016/S0140-6736(18)32279-7
2. Osnabrugge RL, Mylotte D, Head SJ, Van Mieghem NM, Nkomo VT, LeReun CM, et al. Aortic stenosis in the elderly: disease prevalence and number of candidates for transcatheter aortic valve replacement: a meta-analysis and modeling study. J Am Coll Cardiol. (2013) 62(11):1002–12. doi: 10.1016/j.jacc.2013.05.015
3. Ren X, Li F, Wang C, Hou Z, Gao Y, Yin W, et al. Age- and sex-related aortic valve dysfunction and aortopathy difference in patients with bicuspid aortic valve. Int Heart J. (2019) 60(3):637–42. doi: 10.1536/ihj.18-363
4. Sillesen AS, Vøgg O, Pihl C, Raja AA, Sundberg K, Vedel C, et al. Prevalence of bicuspid aortic valve and associated aortopathy in newborns in Copenhagen, Denmark. JAMA. (2021) 325(6):561–7. doi: 10.1001/jama.2020.27205
5. Andell P, Li X, Martinsson A, Andersson C, Stagmo M, Zoller B, et al. Epidemiology of valvular heart disease in a Swedish nationwide hospital-based register study. Heart. (2017) 103(21):1696–703. doi: 10.1136/heartjnl-2016-310894
6. Otto CM. Calcific aortic stenosis — time to look more closely at the valve. N Engl J Med. (2008) 359(13):1395–8. doi: 10.1056/NEJMe0807001
7. Pawade T, Sheth T, Guzzetti E, Dweck MR, Clavel MA. Why and how to measure aortic valve calcification in patients with aortic stenosis. JACC Cardiovasc Imaging. (2019) 12(9):1835–48. doi: 10.1016/j.jcmg.2019.01.045
8. Vahanian A, Beyersdorf F, Praz F, Milojevic M, Baldus S, Bauersachs J, et al. 2021 ESC/EACTS guidelines for the management of valvular heart disease. Eur Heart J. (2022) 43(7):561–632. doi: 10.1093/eurheartj/ehab395
9. Clavel MA, Pibarot P, MessikaZeitoun D, Capoulade R, Malouf J, Aggarwal SR, et al. Impact of aortic valve calcification, as measured by MDCT, on survival in patients with aortic stenosis: results of an international registry study. J Am Coll Cardiol. (2014) 64(12):1202–13. doi: 10.1016/j.jacc.2014.05.066
10. Nguyen V, Mathieu T, Melissopoulou M, Cimadevilla C, Codogno I, Huart V, et al. Sex differences in the progression of aortic stenosis and prognostic implication: the COFRASA-GENERAC study. JACC Cardiovasc Imaging. (2016) 9(4):499–501. doi: 10.1016/j.jcmg.2016.02.006
11. Patel PP, El Sabbagh A, Johnson PW, Suliman R, Salwa N, MoralesLara AC, et al. Sex differences in the impact of aortic valve calcium score on mortality after transcatheter aortic valve replacement. Circ Cardiovasc Imaging. (2022) 15(8):e014034. doi: 10.1161/CIRCIMAGING.122.014034
12. Treibel TA, Kozor R, Fontana M, Torlasco C, Reant P, Badiani S, et al. Sex dimorphism in the myocardial response to aortic stenosis. JACC Cardiovasc Imaging. (2018) 11(7):962–73. doi: 10.1016/j.jcmg.2017.08.025
13. Kuneman JH, Singh GK, Milhorini Pio S, Hirasawa K, Hautemann D, van der Kley F, et al. Sex differences in left ventricular remodelling in patients with severe aortic valve stenosis. Eur Heart J Cardiovasc Imaging. (2021) 23(6):781–9. doi: 10.1093/ehjci/jeab174
14. Tastet L, Kwiecinski J, Pibarot P, Capoulade R, Everett RJ, Newby DE, et al. Sex-related differences in the extent of myocardial fibrosis in patients with aortic valve stenosis. Cardiovas Imaging. (2020) 13(3):699–711. doi: 10.1016/j.jcmg.2019.06.014
15. Tribouilloy C, Bohbot Y, Rusinaru D, Belkhir K, M Diouf, Altes A, et al. Excess mortality and undertreatment of women with severe aortic stenosis. J Am Heart Assoc. (2021) 10(1):e018816. doi: 10.1161/JAHA.120.018816
16. Guzzetti E, Poulin A, Annabi MS, Zhang B, Kalavrouziotis D, Couture C, et al. Transvalvular flow, sex, and survival after valve replacement surgery in patients with severe aortic stenosis. J Am Coll Cardiol. (2020) 75(16):1897–909. doi: 10.1016/j.jacc.2020.02.065
17. Bienjonetti-Boudreau D, Fleury MA, Voisine M, Paquin A, Chouinard I, Tailleur M, et al. Impact of sex on the management and outcome of aortic stenosis patients. Eur Heart J. (2021) 42(27):2683–91. doi: 10.1093/eurheartj/ehab242
18. Castaño A, Narotsky DL, Hamid N, Khalique OK, Morgenstern R, DeLuca A, et al. Unveiling transthyretin cardiac amyloidosis and its predictors among elderly patients with severe aortic stenosis undergoing transcatheter aortic valve replacement. Eur Heart J. (2017) 38(38):2879–87. doi: 10.1093/eurheartj/ehx350
19. Stehli J, Johnston R, Duffy SJ, Zaman S, Gusberti TDH, Dagan M, et al. Waiting times of women versus men undergoing transcatheter aortic valve implantation. Eur Heart J Qual Care Clin Outcomes. (2022). doi: 10.1093/ehjqcco/qcac081.
20. Szerlip M, Gualano S, Holper E, Squiers JJ, White JM, Doshi D, et al. Sex-specific outcomes of transcatheter aortic valve replacement with the SAPIEN 3 valve: insights from the PARTNER II S3 high-risk and intermediate-risk cohorts. JACC Cardiovasc Interv. (2018) 11(1):13–20. doi: 10.1016/j.jcin.2017.09.035
21. Pighi M, Piazza N, Martucci G, Lachapelle K, Perrault LP, Asgar AW, et al. Sex-Specific determinants of outcomes after transcatheter aortic valve replacement. Circ Cardiovasc Qual Outcomes. (2019) 12(3):e005363. doi: 10.1161/CIRCOUTCOMES.118.005363
22. Lowenstern A, Sheridan P, Wang TY, Boero I, Vemulapalli S, Thourani VH, et al. Sex disparities in patients with symptomatic severe aortic stenosis. Am Heart J. (2021) 237:116–26. doi: 10.1016/j.ahj.2021.01.021
23. Bartko PE, Clavel MA, Annabi MS, Dahou A, Ristl R, Goliasch G, et al. Sex-related differences in low-gradient, low–ejection fraction aortic stenosis: results from the multicenter TOPAS study. JACC Cardiovasc Imaging. (2019) 12(1):203–5. doi: 10.1016/j.jcmg.2018.11.003
24. Otto CM, Nishimura RA, Bonow RO, Carabello BA, Erwin JP 3rd, Gentile F, et al. 2020 ACC/AHA guideline for the management of patients with valvular heart disease: executive summary: a report of the American college of cardiology/American heart association joint committee on clinical practice guidelines. J Am Coll Cardiol. (2021) 77(4):450–500. doi: 10.1016/j.jacc.2020.11.035
25. Chandrasekhar J, Dangas G, Yu J, Vemulapalli S, Suchindran S, Vora AN, et al. Sex-based differences in outcomes with transcatheter aortic valve therapy: tVT registry from 2011 to 2014. J Am Coll Cardiol. (2016) 68(25):2733–44. doi: 10.1016/j.jacc.2016.10.041
26. O'Connor SA, Morice MC, Gilard M, Leon MB, Webb JG, Dvir D, et al. Revisiting sex equality with transcatheter aortic valve replacement outcomes: a collaborative, patient-level meta-analysis of 11,310 patients. J Am Coll Cardiol. (2015) 66(3):221–8. doi: 10.1016/j.jacc.2015.05.024
27. Mack MJ, Leon MB, Thourani VH, Makkar R, Kodali SK, Russo M, et al. Transcatheter aortic-valve replacement with a balloon-expandable valve in low-risk patients. N Engl J Med. (2019) 380(18):1695–705. doi: 10.1056/NEJMoa1814052
28. Popma JJ, Deeb GM, Yakubov SJ, Mumtaz M, Gada H, O'Hair D, et al. Transcatheter aortic-valve replacement with a self-expanding valve in low-risk patients. N Engl J Med. (2019) 380(18):1706–15. doi: 10.1056/NEJMoa1816885
29. Adams DH, Popma JJ, Reardon MJ. Transcatheter aortic-valve replacement with a self-expanding prosthesis. N Engl J Med. (2014) 371(10):967–8. doi: 10.1056/NEJMc1408396
30. Stehli J, Martin C, Brennan A, Dinh DT, Lefkovits J, Zaman S. Sex differences persist in time to presentation, revascularization, and mortality in myocardial infarction treated with percutaneous coronary intervention. J Am Heart Assoc. (2019) 8(10):e012161. doi: 10.1161/JAHA.119.012161
31. Stehli J, Duffy SJ, Burgess S, Kuhn L, Gulati M, Chow C, et al. Sex disparities in myocardial infarction: biology or bias? Heart Lung Circ. (2021) 30(1):18–26. doi: 10.1016/j.hlc.2020.06.025
32. Nguyen HL, Saczynski JS, Gore JM, Goldberg RJ. Age and sex differences in duration of prehospital delay in patients with acute myocardial infarction: a systematic review. Circ Cardiovasc Qual Outcomes. (2010) 3(1):82–92. doi: 10.1161/CIRCOUTCOMES.109.884361
33. Stehli J, Dagan M, Zaman S, Koh JQS, Quine E, Gouskova N, et al. Impact of gender on transcatheter aortic valve implantation outcomes. Am J Cardiol. (2020) 133:98–104. doi: 10.1016/j.amjcard.2020.07.052
34. Vlastra W, Chandrasekhar J, Del Blanco BG, Tchetche D, de Brito FS Jr, Barbanti M, et al. Gender differences in transfemoral transcatheter aortic valve replacement. J Am Coll Cardiol. (2019) 74(22):2758–67. doi: 10.1016/j.jacc.2019.09.015.31562908
35. Bergeijk KHv, Ginkel DJv, Brouwer J, Nijenhuis VJ, Werf HWvd, Heuvel AFMvd, et al. Sex differences in outcomes after transcatheter aortic valve replacement. JACC Cardiovasc Interv. (2023) 16(9):1095–102. doi: 10.1016/j.jcin.2023.02.039
36. Dauerman HL, DeStephan CM, Sommer HT, Kurchena KC, DeSarno M, Mendoza EG, et al. Prolonged clotting time among patients undergoing transcatheter aortic valve replacement. J Am Coll Cardiol. (2019) 74(6):820–1. doi: 10.1016/j.jacc.2019.06.022
37. Stehli J, Duffy SJ, Koh Y, Martin C, Brennan A, Dinh DT, et al. Sex differences in radial access for percutaneous coronary intervention in acute coronary syndrome are independent of body size. Heart Lung Circ. (2021) 30(1):108–14. doi: 10.1016/j.hlc.2020.06.023
38. Dangas GD, Tijssen JGP, Wöhrle J, Søndergaard L, Gilard M, Möllmann H, et al. A controlled trial of rivaroxaban after transcatheter aortic-valve replacement. N Engl J Med. (2020) 382(2):120–9. doi: 10.1056/NEJMoa1911425
39. Pajjuru VS, Thandra A, Guddeti RR, Walters RW, Jhand A, Andukuri VG, et al. Sex differences in mortality and 90-day readmission rates after transcatheter aortic valve replacement: a nationwide analysis from the USA. Eur Heart J Qual Care Clin Outcomes. (2021) 8(2):135–42. doi: 10.1093/ehjqcco/qcab012
40. Saad M, Nairooz R, Pothineni NVK, Almomani A, Kovelamudi S, Sardar P, et al. Long-term outcomes with transcatheter aortic valve replacement in women compared with men: evidence from a meta-analysis. JACC Cardiovasc Interv. (2018) 11(1):24–35. doi: 10.1016/j.jcin.2017.08.015
41. Eltchaninoff H, Tchétché D. RHEIA (Randomized researcH in womEn All Comers With Aortic Stenosis). 6.7.2023]; Available at: https://classic.clinicaltrials.gov/ct2/show/NCT04160130?cond=RHEIA&draw=2&rank=1.
42. Zhou C, Xia Z, Chen B, Song Y, Lian Z. Gender differences in age-stratified early outcomes in patients with transcatheter aortic valve implantation. Am J Cardiol. (2023) 187:100–9. doi: 10.1016/j.amjcard.2022.10.038
43. Arnold SV, Spertus JA, Vemulapalli S, Li Z, Matsouaka RA, Baron SJ, et al. Quality-of-life outcomes after transcatheter aortic valve replacement in an unselected population: a report from the STS/ACC transcatheter valve therapy registry. JAMA cardiology. (2017) 2(4):409–16. doi: 10.1001/jamacardio.2016.5302
44. Chaker Z, Badhwar V, Alqahtani F, Aljohani S, Zack CJ, Holmes DR, et al. Sex differences in the utilization and outcomes of surgical aortic valve replacement for severe aortic stenosis. J Am Heart Assoc. (2017) 6(9):e006370. doi: 10.1161/JAHA.117.006370
45. Cho IJ, Chang HJ, Cho I, Heo R, Lee SE, Shim CY, et al. Association of thoracic aorta calcium score with exercise blood pressure response and clinical outcomes in elderly individuals: differential impact of aorta calcification compared with coronary artery calcification. J Am Heart Assoc. (2016) 5(4):e003131. doi: 10.1161/JAHA.115.003131
46. Ryan CT, Almousa A, ZeaVera R, Zhang Q, Amos CI, Coselli JS, et al. Outcomes of aortic valve replacement for chronic aortic insufficiency: analysis of the society of thoracic surgeons database. Ann Thorac Surg. (2022) 113(3):763–72. doi: 10.1016/j.athoracsur.2021.04.027
47. O'Brien SM, Shahian DM, Filardo G, Ferraris VA, Haan CK, Rich JB, et al. The society of thoracic surgeons 2008 cardiac surgery risk models: part 2–isolated valve surgery. Ann Thorac Surg. (2009) 88(1 Suppl):S23–42. doi: 10.1016/j.athoracsur.2009.05.056
Keywords: female, sex, aortic stenosis, transcatheter aortic valve implantation (TAVI), surgical aortic valve replacement (SAVR)
Citation: Stehli J, Zaman S and Stähli BE (2023) Sex discrepancies in pathophysiology, presentation, treatment, and outcomes of severe aortic stenosis. Front. Cardiovasc. Med. 10:1256970. doi: 10.3389/fcvm.2023.1256970
Received: 12 July 2023; Accepted: 28 July 2023;
Published: 15 August 2023.
Edited by:
Edina Cenko, University of Bologna, ItalyReviewed by:
Henryk Dreger, Charité University Medicine Berlin, Germany© 2023 Stehli, Zaman and Stähli. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Julia Stehli anVsaWEuc3RlaGxpQHVzei5jaA==