
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Cardiovasc. Med., 13 September 2023
Sec. Hypertension
Volume 10 - 2023 | https://doi.org/10.3389/fcvm.2023.1247146
This article is part of the Research TopicGlobal Excellence in Cardiovascular Medicine: Central and South AmericaView all 10 articles
 Gilberto Campos Guimarães Filho1
Gilberto Campos Guimarães Filho1 Priscila Valverde de Oliveira Vitorino2Sayuri Inuzuka1Adriana Sebba Barroso1Robson Pierre Pacífico Alves Filho1Victoria Alves Melo1Luiz Fernando de Oliveira Urzeda1
Priscila Valverde de Oliveira Vitorino2Sayuri Inuzuka1Adriana Sebba Barroso1Robson Pierre Pacífico Alves Filho1Victoria Alves Melo1Luiz Fernando de Oliveira Urzeda1 Ana Luiza Lima Sousa1
Ana Luiza Lima Sousa1 Antonio Coca3Paulo César Brandão Veiga Jardim1
Antonio Coca3Paulo César Brandão Veiga Jardim1 Weimar Kunz Sebba Barroso1*†
Weimar Kunz Sebba Barroso1*†
Background: Arterial hypertension treatment guided by central blood pressures (CPB) rather than peripheral blood pressures (PBP) measurement has the potential to show greater effectiveness in preventing or even regressing stiffness and target organ damage (TOD).
Objective: This study aimed to compare the parameters of CBP and PBP measurements, arterial stiffness, TOD and renal profile in patients with anti-hypertensive treatment guided by CBP or PBP targets.
Methods: A randomized clinical trial was conducted in central group (CG) and peripheral group (PG). Patients were randomized, evaluated every 3 months for BP and antihypertensive adjustments during a one-year follow up. The procedures in V1 and V5: anthropometric assessment; CBP/PBP measurements, carotid ultrasound; echocardiography; laboratory tests. Paired and unpaired t-tests and the χ2 were used (significance level: 5%).
Results: The study evaluated 59 participants (30CG/29PG). The augmentation index (AIx) was higher in the CG (27.3% vs. 20.3%, p = 0.041). Intergroup analysis has found central diastolic BP lower in the CG (78.9 vs. 84.3 mmHg, p = 0.024) and the Alx difference between groups ceased to exist after a one-year follow-up. Intragroup comparisons, after intervention, showed a lower frequency of changed PWV (p < 0.001) and LVMI (p = 0.018) in the CG. The PG showed a higher frequency of changed PWV (p < 0.001) and LVMI (p = 0.003).
Conclusion: The intervention guided by central BP reduced the central diastolic BP and AIx compared to the PG. There was a reduction in the frequency of changed PWV and LVMI in the CG.
Arterial hypertension (AH) is the main modifiable risk factor for cardiovascular disease (CVD) and premature mortality worldwide. It is traditionally diagnosed and treated based on peripheral blood pressure (BP) measurements (1–3).
The incorporation of arterial stiffness measurements into traditional scores for cardiovascular (CV) risk stratification and the early identification of vascular damage significantly improves the prediction of CV events. Pulse wave velocity (PWV) is a well-established measurement, an excellent biomarker that can identify subclinical target organ damage (TOD), and, when increased, is associated with a considerable increased CV mortality in hypertensive patients (1, 2, 4, 5).
The implementation of simplified technology and research on new low-cost methods to measure or estimate aortic stiffness have increased its use in clinical practice. Currently, different validated devices to measure central BP and PWV are available for clinical use (6) and can improve the prediction of a ten-year risk of CVD by 13% in intermediate risk patients (7).
Moreover, the presence of residual CV risk in the hypertensive population, delayed identification of subclinical damage, and implementation of optimized therapeutic strategies may be associated with difficulties in the absolute reduction of CV outcomes. The association of therapeutic strategies based only on peripheral BP measurements with these difficulties has been debated (3, 5, 8).
The hypothesis that the treatment guided by central BP reduction goals may present advantages over the conventional treatment strategy in reducing intermediate outcomes has biological plausibility (9–12). Few studies have tested this hypothesis, but the superiority of central BP parameters over peripheral ones in predicting CV risk highlights the importance of evaluating the possible behavior of some biomarkers such as PWV as risk factors (13–17).
Therefore, AH treatment guided by central BP parameters has the potential to show greater effectiveness in preventing or even regressing stiffness and TOD when compared to the conventional strategy (18, 19).
Thus, the objectives of this study were: (1) to verify if the treatment guided by central BP values has better effects on central BP values, carotid ultrasound, and Doppler echocardiography compared to the treatment guided by peripheral BP values; (2) to compare central BP values, carotid ultrasound, and Doppler echocardiography before and after the study in each of the groups; and (3) to compare inter- and intragroup frequency of changed PWV, left ventricular LVMI, and creatinine clearance.
This study is an open-label, randomized, clinical trial conducted in two AH reference services. The study protocol was approved by the Research Ethics Committee under opinion no. 2.746.523, and all participants signed the informed consent form before study procedures.
The inclusion criteria were patients with AH, aged 18 years or more, using or not using antihypertensive drugs, and with an indication for pharmacological treatment based on casual BP measurements (1).
The exclusion criteria were patients with end-stage chronic diseases or previous CVD, including coronary artery disease (acute myocardial infarction, angina, coronary artery bypass graft surgery, or angioplasty) or stroke (ischemic and hemorrhagic stroke or transient ischemic attack) less than six months before the study. These criteria were defined by information obtained directly from the patients or from complementary tests.
Study participants answered a sociodemographic questionnaire, had their body mass and height measured to calculate the body mass index (BMI) (20, 21), had their peripheral and central BP measured, and underwent Doppler echocardiography, carotid ultrasound, and laboratory tests.
Peripheral BP was measured in the office, in a quiet and silent environment, using an HEM-1100 OMRON® automatic device and following the recommended guidelines (1, 5). Central BP measurement was performed, under the same conditions, using the Cardios Dyna MAPA AOP® device with the ARV Solver algorithm (three consecutive measurement protocol and C1 calibration) to verify the central BP, PWV, total vascular resistance (TVR), and augmentation index (AIx).
Cardiac and vascular structural damage was assessed by Doppler echocardiography and carotid ultrasound using a TOSHIBA Xsario ultrasound device. The parameters analyzed included the interventricular septum and left ventricular posterior wall, LVMI, and left atrial volume measurement on Doppler echocardiography, and carotid intima-media thickness (cIMT) measurement and carotid plaque search on carotid ultrasound. All tests were performed by the same observer in each of the services.
The definition of cardiac and vascular damage was established using the following biomarkers: IMT >0.9 mm or presence of atherosclerotic plaques in carotid arteries (22, 23), left atrial diameter greater than 38 mm for women and 40 mm for men, LVMI >95 mg/m2 for women and >115 mg/m2 for men, and PWV ≥10 m/s (1, 5).
Creatinine was tested for the subsequent calculation of the glomerular filtration rate (GFR) using the Modification of Diet in Renal Disease (MDRD) formula and considering values ≤60 ml/min/1.73 m2 as reduced (24).
Treatment strategies were similar regarding the drugs used for both groups, and level adjustment was at the investigating physician's discretion to achieve the goals in both groups: level 1—Losartan 50 mg/day; level 2—Losartan 50 mg 12/12 hs; level 3—Losartan 50 mg 12/12 hs + Amlodipine 5 mg/day; level 4—Losartan 50 mg 12/12 hs + Amlodipine 10 mg/day; level 5—Losartan 50 mg 12/12 hs + Amlodipine 10 mg/day + Hydrochlorothiazide 12.5 mg/day; level 6—Losartan 50 mg 12/12 hs + Amlodipine 10 mg/day + Hydrochlorothiazide 25 mg/day; level 7—Losartan 50 mg 12/12 hs + Amlodipine 10 mg/day + Hydrochlorothiazide 25 mg/day + Spironolactone 25 mg/day.
There was no wash-out before randomization (1, 5, 6, 25). It is noteworthy that the use of the same antihypertensive drug strategy for both groups aimed to ensure that the only difference between them would be related to the goal guided by central or peripheral parameters.
After the initial visit, the participants were evaluated every 90 days to adjust the drug level. For the CG, the goal was to maintain central systolic BP below the values established with reference to sex and age group (25) (Table 1). For safety, the minimum limit for peripheral BP reduction was 110/70 mmHg.
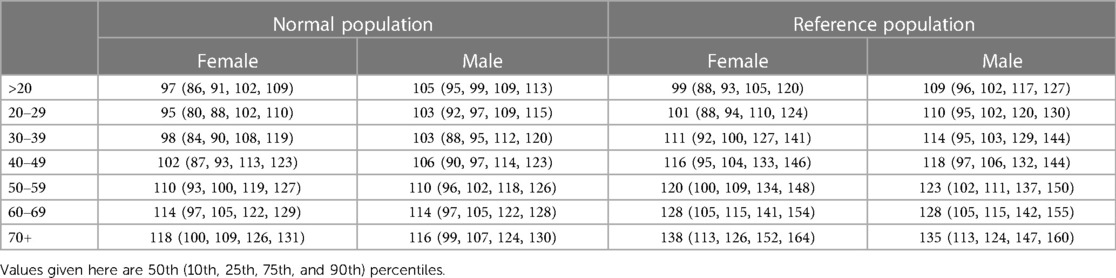
Table 1. Central systolic blood pressure values according to age categories, for males and females, in the normal and reference populations (25).
For the PG, the goal was a peripheral BP value lower than 140/90 mmHg for low and medium risk and lower than 130/80 mmHg for high risk such as European Society of Cardiology and the European Society of Hypertension Guidelines (1, 5).
If the patient did not meet the defined goals in the return visits, the drug level was increased at medical discretion. Patients who did not show up for a visit after at least two contact attempts were considered lost to follow-up.
Statistical analysis was performed with the Stata software version 14.0. The Shapiro Wilk test was used to verify the normality of data distribution. Quantitative variable values and deltas were compared between groups at the beginning and end of the study using the unpaired t-test for quantitative variables with normal distribution and the Mann–Whitney U-test for quantitative variables with non-normal distribution. The χ2 or Fisher's tests were used to compare qualitative sociodemographic, BP, and complementary test variables; drug level used at each visit; and the frequency of intragroup PWV, ventricular mass index, and creatinine clearance changes at the initial and final visits. The significance level was set at 5% for all tests.
The initial sample consisted of 130 participants, of whom 59 (30 CG and 29 PG) completed the study, with no deaths or serious adverse events. The 71 losses to follow-up (54.6%) occurred due to the coronavirus disease 2019 (COVID-19) pandemic.
At the initial visit, the groups were similar in terms of sociodemographic characteristics, BMI, cardiovascular risk factors, central and peripheral BP measurements, variables obtained by carotid ultrasound and Doppler echocardiography, and GFR. Only the AIx was higher in the CG (Table 2).
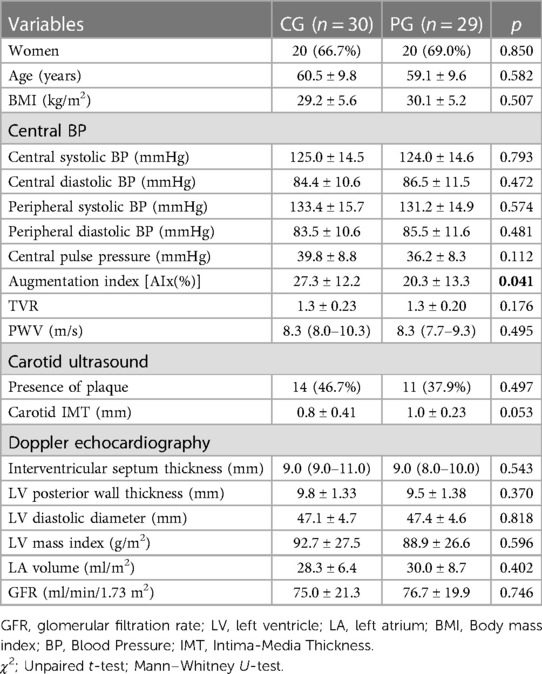
Table 2. Comparison between the central and peripheral groups before intervention regarding sociodemographic variables, body mass index, central blood pressure measurements, carotid ultrasound, Doppler echocardiography, and glomerular filtration rate, n = 59, 2018–2020.
No differences were identified in peripheral BP, carotid ultrasound and Doppler echocardiography variables, and in GFR after the 12-month follow-up. Central diastolic BP was lower in the CG than in the PG. The delta also showed a greater AIx and TVR reduction in the CG than in the PG (Table 3).
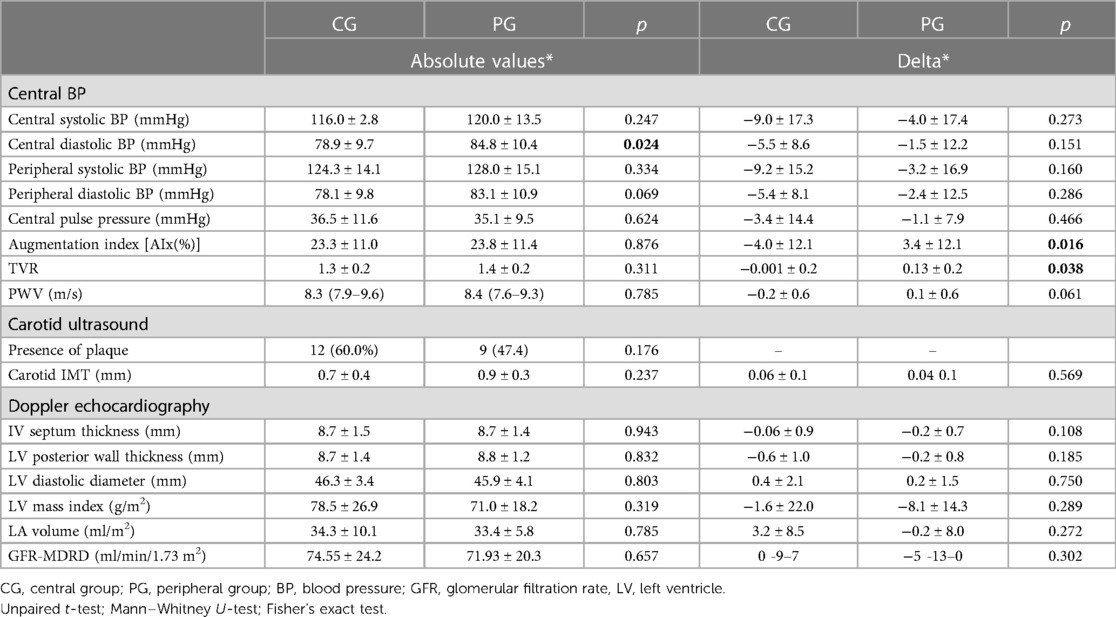
Table 3. Comparison of absolute values and deltas between the central and peripheral groups after the 12-month intervention regarding central blood pressure measurements, carotid ultrasound, Doppler echocardiography, and GFR, n = 59, 2018–2020.
Central diastolic pressure and AIx were reduced in the CG and AIx was increased in the PG at the end of the one-year follow-up (Figure 1).
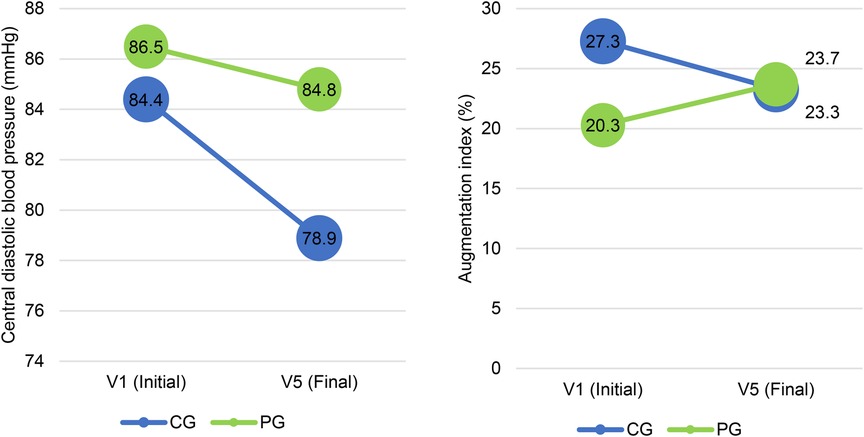
Figure 1. Central diastolic pressure and augmentation index values at V1 (initial) and V5 (final) in the CG and PG, n = 59. CG, central group; PG, peripheral group.
The use of three antihypertensive drugs showed a higher frequency than monotherapy and dual combination in both the CG and PG at the initial and final visits. There was no inter- or intragroup drug level difference before and after the follow-up (Table 4).
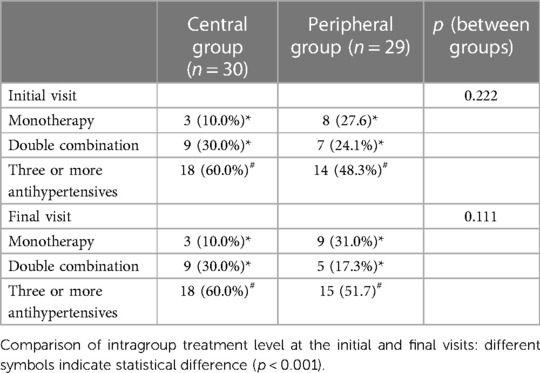
Table 4. Comparison of the number of drugs used before and after the intervention in the central (n = 30) and peripheral (n = 29) groups.
There was no difference between the CG and PG regarding the frequency of changed PWV values (≥10 m/s), LVMI (>95 mg/m2 for women and >115 mg/m2 for men), and GFR (≤60 ml/min/1.73 m2) at the initial and final visits (Table 5).
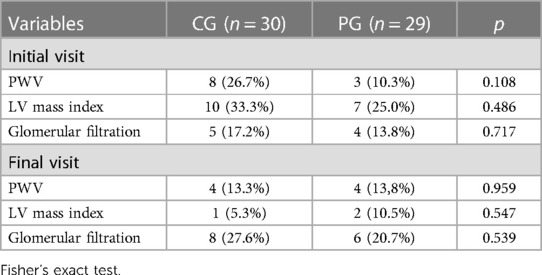
Table 5. Comparison of the frequency of pulse wave velocity, left ventricular mass index, and glomerular filtration rate changes between the CG and PG before and after the study.
When intragroup comparisons were made before and after the intervention, the CG showed a reduced frequency of participants with changed PWV (p < 0.001) and LVMI (p = 0.018). In the PG, the frequency of participants with changed PWV (p < 0.001) increased and of those with changed LVMI reduced (p = 0.003). The CG (p = 0.004) and PG (p = 0.004) showed increased frequency of changed GFR (Table 6).
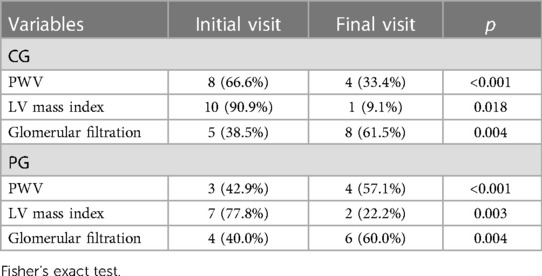
Table 6. Comparison of the frequency of pulse wave velocity, left ventricular mass index, and glomerular filtration rate changes before and after the follow-up.
Our study shows that the intervention guided by central BP reduced central diastolic BP but not central systolic BP, and corrected the AIx parameter after a one-year follow-up compared to the group guided by peripheral BP. Intragroup analysis showed a significantly reduced frequency of changed PWV and LVMI in the group of intervention guided by central BP.
This sample included hypertensive patients with a mean age of 60 years and mean BMI of 30 kg/m2 with well-controlled BP levels in the initial phase of the study. In addition, the comparative analysis in relation to the baseline characteristics showed that the groups randomized to treatment guided by central or peripheral pressure were similar, except for the AIx parameter, which was higher in the CG. As for the antihypertensive drugs used in our clinical trial, all patients used the same strategy in both groups to eliminate potential confounding factors that could occur in the case of different drugs. A recently published clinical trial randomized hypertensive patients to groups guided by the goal of PWV or peripheral BP reduction but used different classes and drugs in the follow-up phase (26).
PWV is considered an independent biomarker of subclinical TOD (27). To date, only the SPARTE study evaluated the strategy of AH treatment guided by PWV reduction compared with the strategy guided by peripheral BP and no significant differences were found to significantly CV outcomes, peripheral arterial disease, hospitalization for heart failure, aortic dissection, chronic kidney disease, and sudden death. However, the PWV guided treatment intensified the antihypertensive treatment with vascular aging prevention characterized by PWV behavior compared to the conventional treatment (26).
In our study treatment was guided with central or peripheral BP to achieve goals and considered PWV as an outcome variable. Although we found no significant difference between groups, the CG showed a significant reduction in changed PWV (≥10 m/s) over the 12-month follow-up. This finding corroborates the results of the SPARTE study and others that evaluated strategies to reduce vascular aging velocity (26–28).
In addition to PWV, our study also analyzed AIx, central BP, TVR, and central pulse pressure (CPP). We found a difference in central diastolic BP after a 12-month follow-up between the two randomized groups. Several studies evaluated these biomarkers, mainly as attempted surrogate outcome, and observed no significant association between central and peripheral BP measurements (29–32). However, a systematic review showed greater predictive power of central BP and CPP for TOD and CV outcomes (32). AIx was higher in the CG and reversed this behavior after the one-year follow-up.
Currently, evidence shows a stronger association between the central component of BP and increased LVMI and carotid IMT (33). Increased arterial stiffness is believed to be an intermediate stage between aging and CV damages, such as left ventricular and carotid dysfunction (34, 35). Our study showed no benefit in reducing CV outcomes such as left ventricular hypertrophy (LVH) and carotid vascular damage when treating hypertensive patients based on central BP compared with peripheral BP, and the frequency of subjects with changed LVMI reduced in both groups at the end of follow-up.
Two other studies that used the electrocardiogram as a measure of LVH showed a good association between central BP and LVH, but similar to that observed between peripheral systolic BP and LVH (36, 37). Another study reported the better predictive value of central BP compared to peripheral BP for cardiac damage such as LVH (38). A possible explanation is that arterial stiffness increases systolic BP, causing an early return of pulse waves during the systolic period and increased left ventricle afterload that causes cardiac hypertrophy and consequent LVH (39–41).
In our study, central BP had no better association with renal impairment than peripheral BP, a finding that corroborates with those of previous outpatient studies (42, 43). This may be justified by the fact that central BP is associated with macrovascular damage, but is not so closely related to microvascular injury, typical of renal injury (9). Another hypothesis suggests that in the early stages of kidney disease, the association between BP and kidney damage may be weak (44). We believe that longer follow-up and/or a larger sample size may detect greater CV protection with targets guided by central BP reduction.
The limitations of our study were mainly related to the loss of follow-up due to the COVID-19 pandemic, which may have impacted the statistical power to demonstrate differences between groups. Another limitation is related to a sample with well-controlled BP levels at the beginning of the study, which hinders differences in outcomes closely related to BP control. However, this is an unprecedented clinical trial in the comparison of goals guided by different strategies and with results that raise the need for further studies to provide the desired answers.
This clinical trial tested a hypothesis that is still under construction. Nevertheless, the intergroup difference in the behavior of AIx, central diastolic BP, and intragroup difference regarding the frequency of changed PWV and LVMI makes it plausible to consider the benefits of the treatment guided by central parameters.
The treatment of hypertensive disease guided by central pressure reduction goals was not able to demonstrate differences in outcomes related to PWV, LVMI, IMT, and renal function compared to the traditional strategy, but showed superiority in reducing central diastolic pressure and AIx behavior at the end of a one-year follow-up. Intragroup analysis found a lower frequency of PWV ≥10 m/s in the CG, raising the hypothesis that longer follow-ups and greater sampling power may demonstrate the benefits of this treatment strategy.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving humans were approved by Comitê de ética em pesquisa do Hospital das Clínicas da Universidade Federal de Goiás, Brasil. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
WB: Conceived and designed the analysis; Collected the data; Contributed data or analysis tools; Performed the analysis; Wrote the paper. GG: Collected the data; Contributed data or analysis tools; Wrote the paper. PO: Conceived and designed the analysis; Collected the data; Contributed data or analysis tools; Performed the analysis; Wrote the paper. SI: Collected the data; Contributed data or analysis tools; Performed the analysis; Wrote the paper. AB: Collected the data; Contributed data or analysis tools. RP: Collected the data; Contributed data or analysis tools. VM: Collected the data; Contributed data or analysis tools. LO: Collected the data; Contributed data or analysis tools. AS: Conceived and designed the analysis; Collected the data; Contributed data or analysis tools; Performed the analysis. AC: Conceived and designed the analysis; Contributed data or analysis tools; Wrote the paper. PV: Conceived and designed the analysis; Contributed data or analysis tools; Wrote the paper. All author contributed to the article and approved the submitted version.
The study was supported by the Brazilian National Council for Scientific and Technological Development (Conselho Nacional de Desenvolvimento Científico e Tecnológico – CNPQ) (grant 313481/2020-2) for Dr. Barroso.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Barroso WKS, Rodrigues CIS, Bortolotto LA, Mota-Gomes MA, Brandão AA, Feitosa ADdM, et al. Diretrizes Brasileiras de Hipertensão Arterial–2020. Arq Bras Cardiol. (2021) 116:516–658. doi: 10.36660/abc.20201238
2. Chirinos JA, Segers P, Hughes T, Townsend R. Large-artery stiffness in health and disease: JACC state-of-the-art review. J Am Coll Cardiol. (2019) 74(9):1237–63. doi: 10.1016/j.jacc.2019.07.012
3. Barroso WKS, Barbosa ECD, Mota-Gomes MA. Rigidez arterial e hemodinâmica central: do endotélio à camada média. Atha Mais Editora. (2020). 146p.
4. Kario K, Kanegae H, Oikawa T, Suzuki K. Hypertension is predicted by both large and small artery disease: a large population-based study in normotensive adults. Hypertension. (2019) 73(1):75–83. doi: 10.1161/HYPERTENSIONAHA.118.11800
5. Williams B, Mancia G, Spiering W, Agabiti Rosei E, Azizi M, Burnier M, et al. 2018 ESC/ESH guidelines for the management of arterial hypertension: the task force for the management of arterial hypertension of the European society of cardiology (ESC) and the European society of hypertension (ESH). Eur Heart J. (2018) 39(33):3021–104. doi: 10.1093/eurheartj/ehy339
6. McEniery CM, Cockcroft JR, Roman MJ, Franklin SS, Wilkinson IB. Central blood pressure: current evidence and clinical importance. Eur Heart J. (2014) 35(26):1719–25. doi: 10.1093/eurheartj/eht565
7. Ben-Shlomo Y, Spears M, Boustred C, May M, Anderson SG, Benjamin EJ, et al. Aortic pulse wave velocity improves cardiovascular event prediction: an individual participant meta-analysis of prospective observational data from 17,635 subjects. J Am Coll Cardiol. (2014) 63(7):636–46. doi: 10.1016/j.jacc.2013.09.063
8. Kohlmann O Jr, Gus M, Ribeiro AB, Vianna D, Coelho EB, Barbosa E, et al. Tratamento medicamentoso. J Bras Nefrol. (2010) 32:29–43. doi: 10.1590/S0101-28002010000500008
9. Omboni S, Posokhov IN, Rogoza AN. Relationships between 24-h blood pressure variability and 24-h central arterial pressure, pulse wave velocity and augmentation index in hypertensive patients. Hypertens Res. (2017) 40(4):385–91. doi: 10.1038/hr.2016.156
10. Liu Y, Yan Y, Yang X, Li S, Bazzano L, He J, et al. Long-term burden of higher body mass index and adult arterial stiffness are linked predominantly through elevated blood pressure. Hypertension. (2019) 73(1):229–34. doi: 10.1161/HYPERTENSIONAHA.118.12106
11. Haraguchi N, Koyama T, Kuriyama N, Ozaki E, Matsui D, Watanabe I, et al. Assessment of anthropometric indices other than BMI to evaluate arterial stiffness. Hypertens Res. (2019) 42(10):1599–605. doi: 10.1038/s41440-019-0264-0
12. Lopes-Vicente WR, Rodrigues S, Cepeda FX, Jordão CP, Costa-Hong V, Dutra-Marques AC, et al. Arterial stiffness and its association with clustering of metabolic syndrome risk factors. Diabetol Metab Syndr. (2017) 9(1):1–8. doi: 10.1186/s13098-016-0201-1
13. Lu Y, Pechlaner R, Cai J, Yuan H, Huang Z, Yang G, et al. Trajectories of age-related arterial stiffness in Chinese men and women. J Am Coll Cardiol. (2020) 75(8):870–80. doi: 10.1016/j.jacc.2019.12.039
14. Zhan B, Huang X, Wang J, Qin X, Zhang J, Cao J, et al. Association between lipid profiles and arterial stiffness in Chinese patients with hypertension: insights from the CSPPT. Angiology. (2019) 70(6):515–22. doi: 10.1177/0003319718823341
15. Coca A, Burnier M. Editorial: Hypertension in the Elderly. Front Cardiovasc Med. (2021) 8:645580. doi: 10.3389/fcvm.2021.645580
16. Prenner SB, Chirinos JA. Arterial stiffness in diabetes mellitus. Atherosclerosis. (2015) 238(2):370–9. doi: 10.1016/j.atherosclerosis.2014.12.023
17. Gottsäter M, Östling G, Persson M, Engström G, Melander O, Nilsson PM. Non-hemodynamic predictors of arterial stiffness after 17 years of follow-up: the malmö diet and cancer study. J Hypertens. (2015) 33(5):957. doi: 10.1097/HJH.0000000000000520
18. Fagundes RR, Vitorino PVO, Lelis ES, Jardim PCBV, Souza ALL, Jardim TdSV, et al. Relationship between pulse wave velocity and cardiovascular biomarkers in patients with risk factors. Arq Bras Cardiol. (2021) 115:1125–32. doi: 10.36660/abc.20190348
19. Hamczyk MR, Nevado RM, Barettino A, Fuster V, Andres V. Biological versus chronological aging: JACC focus seminar. J Am Coll Cardiol. (2020) 75(8):919–30. doi: 10.1016/j.jacc.2019.11.062
20. Quetelet A. Anthropométrie ou mesure des différentes facultés de l'Homme bruxelles. Muquardt éd. (1870). 479p.
21. World Health Organization. Physical status: the use and interpretation of anthropometry. WHO Tech Rep Ser. (1995) 854(9):463.
22. Nambi V, Chambless L, Folsom AR, He M, Hu Y, Mosley T, et al. Carotid intima-media thickness and presence or absence of plaque improves prediction of coronary heart disease risk: the ARIC (atherosclerosis risk in communities) study. J Am Coll Cardiol. (2010) 55(15):1600–7. doi: 10.1016/j.jacc.2009.11.075
23. Polak JF, Szklo M, O'Leary DH. Carotid intima-media thickness score, positive coronary artery calcium score, and incident coronary heart disease: the multi-ethnic study of atherosclerosis. J Am Coll Cardiol. (2017) 6(1):e004612. doi: 10.1161/JAHA.116.004612
24. Levey AS, Coresh J, Greene T, Stevens LA, Zhang Y, Hendriksen S, et al. Using standardized serum creatinine values in the modification of diet in renal disease study equation for estimating glomerular filtration rate. Ann Intern Med Clin Cases. (2006) 145(4):247–54. doi: 10.7326/0003-4819-145-4-200608150-00004
25. Herbert A, Cruickshank JK, Laurent S, Boutouyrie P. Establishing reference values for central blood pressure and its amplification in a general healthy population and according to cardiovascular risk factors. Eur Heart J. (2014) 35(44):3122–33. doi: 10.1093/eurheartj/ehu293
26. Laurent S, Chatellier G, Azizi M, Calvet D, Choukroun G, Danchin N, et al. SPARTE Study: normalization of arterial stiffness and cardiovascular events in patients with hypertension at medium to very high risk. Hypertension. (2021) 78(4):983–95. doi: 10.1161/HYPERTENSIONAHA.121.17579
27. Mitchell GF. Does measurement of central blood pressure have treatment consequences in the clinical praxis? Curr Hypertens Rep. (2015) 17(8):1–8. doi: 10.1007/s11906-015-0573-x
28. Niiranen TJ, Kalesan B, Hamburg NM, Benjamin EJ, Mitchell GF, Vasan RS. Relative contributions of arterial stiffness and hypertension to cardiovascular disease: the framingham heart study. J Am Coll Cardiol. (2016) 5(11):e004271. doi: 10.1161/JAHA.116.004271
29. Vlachopoulos C, Xaplanteris P, Aboyans V, Brodmann M, Cífková R, Cosentino F, et al. The role of vascular biomarkers for primary and secondary prevention. A position paper from the European society of cardiology working group on peripheral circulation: endorsed by the association for research into arterial structure and physiology (ARTERY) society. Atherosclerosis. (2015) 241(2):507–32. doi: 10.1016/j.atherosclerosis.2015.05.007
30. Chi C, Yu S, Auckle R, Argyris A, Nasothimiou E, Tountas C, et al. Association of left ventricular structural and functional abnormalities with aortic and brachial blood pressure variability in hypertensive patients: the SAFAR study. J Hum Hypertens. (2017) 31(10):633–9. doi: 10.1038/jhh.2017.37
31. de la Sierra A, Pareja J, Yun S, Acosta E, Aiello F, Oliveras A, et al. Central blood pressure variability is increased in hypertensive patients with target organ damage. J Clin Hypertens. (2018) 20(2):266–72. doi: 10.1111/jch.13172
32. Yu S, Chi C, Protogerou AD, Safar ME, Blacher J, Argyris AA, et al. 24-hour Aortic blood pressure variability showed a stronger association with carotid damage than 24-hour brachial blood pressure variability: the SAFAR study. J Clin Hypertens. (2018) 20(3):499–507. doi: 10.1111/jch.13226
33. Kollias A, Lagou S, Zeniodi ME, Boubouchairopoulou N, Stergiou GS. Association of central versus brachial blood pressure with target-organ damage: systematic review and meta-analysis. Hypertension. (2016) 67(1):183–90. doi: 10.1161/HYPERTENSIONAHA.115.06066
34. Fernandes VRS, Polak JF, Cheng S, Rosen BD, Carvalho B, Nasir K, et al. Arterial stiffness is associated with regional ventricular systolic and diastolic dysfunction: the multi-ethnic study of atherosclerosis. Arterioscler Thromb Vasc Biol. (2008) 28(1):194–201. doi: 10.1161/ATVBAHA.107.156950
35. Libhaber E, Woodiwiss AJ, Libhaber C, Maseko M, Majane OH, Makaula S, et al. Gender-specific brachial artery blood pressure-independent relationship between pulse wave velocity and left ventricular mass index in a group of African ancestry. J Hypertens. (2008) 26(8):1619–28. doi: 10.1097/HJH.0b013e328302ca27
36. Blanch P, Armario P, Oliveras A, Fernández-Llama P, Vázquez S, Pareja J, et al. Association of either left ventricular hypertrophy or diastolic dysfunction with 24-hour central and peripheral blood pressure. Am J Hypertens. (2018) 31(12):1293–9. doi: 10.1093/ajh/hpy123
37. Yang WY, Mujaj B, Efremov L, Zhang ZY, Thijs L, Wei FF, et al. ECG Voltage in relation to peripheral and central ambulatory blood pressure. Am J Hypertens. (2018) 31(2):178–87. doi: 10.1093/ajh/hpx157
38. Terentes-Printzios D, Gardikioti V, Vlachopoulos C. Central over peripheral blood pressure: an emerging issue in hypertension research. Heart Lung Circ. (2021) 30(11):1667–74. doi: 10.1016/j.hlc.2021.07.019
39. Chung CM, Lin YS, Chang ST, Cheng HW, Yang TY, Hsiao JF, et al. Arterial stiffness is the independent factor of left ventricular hypertrophy determined by electrocardiogram. Am J Med Sci. (2012) 344(3):190–3. doi: 10.1097/MAJ.0b013e318242a354
40. Yucel C, Demir S, Demir M, Tufenk M, Nas K, Molnar F, et al. Left ventricular hypertrophy and arterial stiffness in essential hypertension. Bratisl Lek Listy. (2015) 116(12):714–8. doi: 10.4149/bll_2015_140
41. Townsend RR, Wilkinson IB, Schiffrin EL, Avolio AP, Chirinos JA, Cockcroft JR, et al. Recommendations for improving and standardizing vascular research on arterial stiffness: a scientific statement from the American heart association. Hypertension. (2015) 66(3):698–722. doi: 10.1161/HYP.0000000000000033
42. Fernández-Llama P, Pareja J, Yun S, Vázquez S, Oliveras A, Armario P, et al. Cuff-based oscillometric central and brachial blood pressures obtained through ABPM are similarly associated with renal organ damage in arterial hypertension. Kidney Blood Press Res. (2017) 42(6):1068–77. doi: 10.1159/000485595
43. Theilade S, Lajer M, Hansen TW, Joergensen C, Persson F, Andrésdottir G, et al. 24-hour Central aortic systolic pressure and 24-hour central pulse pressure are related to diabetic complications in type 1 diabetes–a cross-sectional study. Cardiovasc Diabetol. (2013) 12(1):1–12. doi: 10.1186/1475-2840-12-122
Keywords: arterial stiffness, central blood pressure, clinical trial, hypertension, pulse wave velocity
Citation: Guimarães Filho GC, de Oliveira Vitorino PV, Inuzuka S, Barroso AS, Pacífico Alves Filho RP, Melo VA, de Oliveira Urzeda LF, Lima Sousa AL, Coca A, Veiga Jardim PCB and Barroso WKS (2023) Pharmacological treatment of hypertension guided by peripheral or central blood pressure: a comparison between the two strategies. Front. Cardiovasc. Med. 10:1247146. doi: 10.3389/fcvm.2023.1247146
Received: 25 June 2023; Accepted: 28 August 2023;
Published: 13 September 2023.
Edited by:
Patricio López-Jaramillo, Universidad de Santander, ColombiaReviewed by:
Miguel Urina-Triana, Simón Bolívar University, Colombia© 2023 Guimarães Filho, de Oliveira Vitorino, Inuzuka, Barroso, Pacífico Alves Filho, Melo, de Oliveira Urzeda, Lima Sousa, Coca, Veiga Jardim and Barroso. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Weimar Kunz Sebba Barroso c2ViYmFiYXJyb3NvQGdtYWlsLmNvbQ==
†Senior author
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.