 Ae-Young Her1,†
Ae-Young Her1,† Dominic Dischl
Dominic Dischl Yong Hoon Kim
Yong Hoon Kim Eun-Seok Shin
Eun-Seok Shin
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
MINI REVIEW article
Front. Cardiovasc. Med. , 07 July 2023
Sec. General Cardiovascular Medicine
Volume 10 - 2023 | https://doi.org/10.3389/fcvm.2023.1242215
This article is part of the Research Topic Current Proceedings in Magnetocardiology View all 8 articles
Ischemic heart disease (IHD) continues to be a significant global public health concern and ranks among the leading causes of mortality worldwide. However, the identification of myocardial ischemia in patients suspected of having coronary artery disease (CAD) remains a challenging issue. Functional or stress testing is widely recognized as the gold standard method for diagnosing myocardial ischemia, but it is hindered by low diagnostic accuracy and limitations such as radiation exposure. Magnetocardiography (MCG) is a non-contact, non-invasive method that records magnetic fields produced by the electrical activity of the heart. Unlike electrocardiography (EKG) and other functional or stress testing, MCG offers numerous advantages. It is highly sensitive and can detect early signs of myocardial ischemia that may be missed by other diagnostic tools. This review aims to provide an extensive overview of the available evidence that establishes the utility of MCG as a valuable diagnostic tool for identifying myocardial ischemia, accompanied by a discussion of potential future research directions in this domain.
Ischemic heart disease (IHD) remains a significant global public health issue, and its prevalence has been increasing over the years. According to the 2023 report from the National Center for Biotechnology Information (NCBI), IHD is responsible for 17.8 million deaths annually, positioning it as the third most common cause of mortality worldwide (1). However, identifying myocardial ischemia in patients with suspected coronary artery disease (CAD) remains a challenging aspect of routine cardiological diagnostics with its diverse manifestation and the complexities involved in distinguishing non-IHD. Functional or stress testing, which aims to detect inducible myocardial ischemia, has traditionally been considered the “gold standard” and is the most commonly used as a non-invasive method for diagnosing CAD (2). However, a non-invasive evaluation is performed on less than half of the patients before percutaneous coronary intervention (PCI) (3, 4). This is primarily due to limitations in testing, which include low diagnostic accuracy and the potential radiation risks associated with coronary computed tomography (CT) or single-photon emission computed tomography (SPECT) (5).
Magnetocardiography (MCG) is a non-contact, non-invasive, radiation and contrast-free method that enables the recording of magnetic fields generated by the electrical activity of the heart (6–9). Although electrocardiography (EKG) and MCG provide information about the same electrical activities of the heart, MCG presents several advantages. Cardiac magnetic fields remain unaffected by variations in the conductivity of body tissues or fluids, without attenuation or distortion (10). Additionally, its high sensitivity and non-invasive, contactless procedure make it a valuable tool for early diagnosis of myocardial ischemia that may otherwise go undetected by EKG (11). Several clinical studies have already demonstrated the superior sensitivity of MCG compared to EKG in detecting ischemic myocardium both at rest and during stress (11–17). The remarkable ability of MCG to identify patients with CAD has been widely recognized (5, 17–20). Various MCG investigations have employed a variety of devices, including cryogenic superconducting quantum interference devices (SQUIDs) (21, 22). These devices have primarily been utilized in magnetically shielded rooms (MSR) to eliminate background environmental noise, for instance, noise emanating from nearby instruments. However, they can also yield reliable outcomes in unshielded environments by incorporating a second (or higher order) gradiometer configuration of the pick-up coils and/or utilizing real-time electronic noise subtraction (10). Recently, advancements have been made in non-cryogenic MCG devices, offering alternative options (23). Furthermore, a variety of quantitative methods and computer algorithms have been devised to facilitate the interpretation of diverse magnetic field patterns (24–27).
This review will provide an overview of the evidence supporting the utility of MCG, a valuable tool for diagnosing myocardial ischemia that is currently available, and discuss the potential impact of these findings on the future integration of MCG into clinical practice.
Previous studies have explored the application of MCG for the diagnosis or ruling out of stable CAD in Table 1. Other studies have investigated its use for the detection or ruling out of acute coronary syndrome (ACS) in Table 2. These studies have utilized a range of techniques to qualitatively and quantitatively analyze the magnetic field throughout the cardiac cycle. In most of the studies, the quantitative analysis has been focused on evaluating changes in the magnetic field during ventricular repolarization, typically occurring at the end of the ST segment (prior to the T wave) and/or the T wave. These methods encompass the analysis of various aspects, such as the extrema and dynamics of the magnetic field angle, as well as the dynamics of distance and ratio involving the minimum and maximum poles. These measurements are typically taken during the ascending T wave, specifically from one-third of the peak intensity (Tmax/3) to the peak intensity (Tmax) (6, 28–32, 42, 49). Additionally, other studies have also investigated different parameters related to the ST segment and T wave, particularly during or after exercise (13, 33). Due to the typically higher magnetic field and signal-to-noise (S/N) ratio during rest, many subsequent studies have focused on utilizing variations of parameters measured during the T wave, initially described by Park et al. (42). Additionally, other MCG parameters have been investigated during the QT and QRS intervals (23, 34–39), and there have been reports on the application of machine-learning approaches for interpreting MCG signals (24–26).
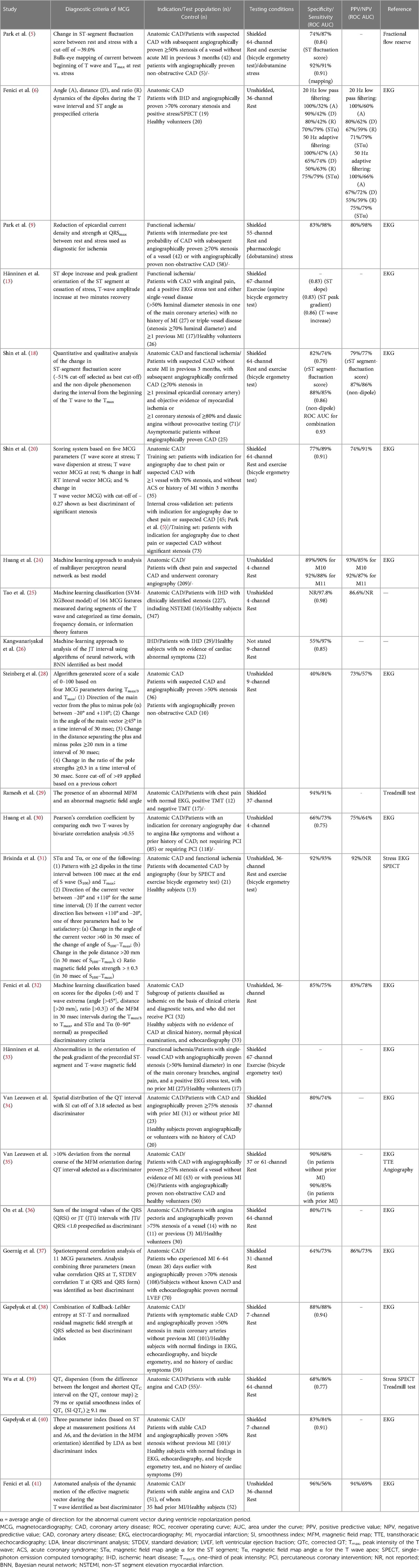
Table 1. Studies of MCG in patients with stable CAD.
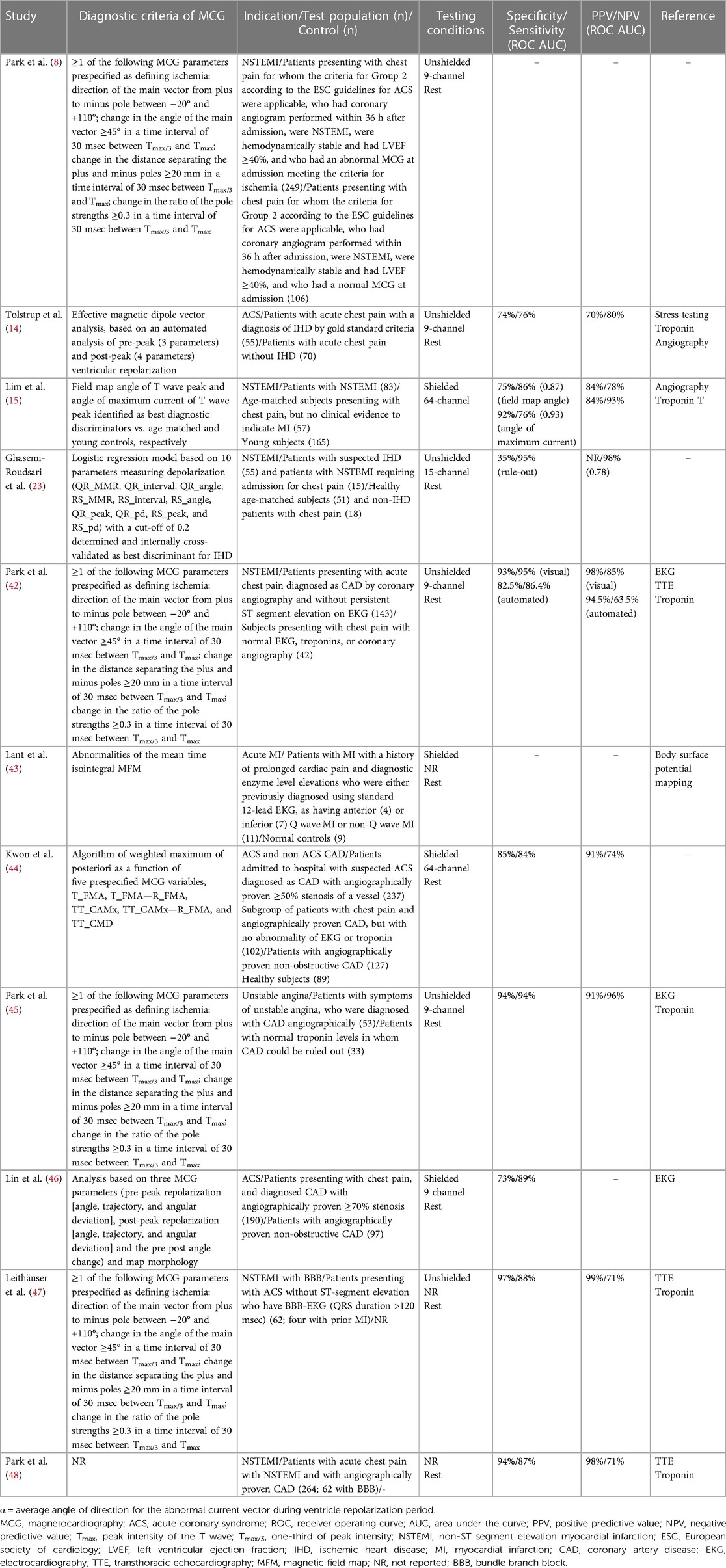
Table 2. Studies of MCG in patients with ACS.
Numerous studies have provided evidence that MCG, whether conducted in a shielded or unshielded environment, at rest, or under conditions of exercise or pharmacologic stress, can effectively differentiate between patients with angiographically confirmed stable CAD and healthy individuals (13, 25, 26, 34, 36–38, 40, 41). Additionally, MCG has shown potential in distinguishing patients with chest pain but without evidence of CAD on angiography or other diagnostic tests (5, 9, 18, 20, 28, 35, 39). However, it is important to proceed with caution when interpreting these results, as many of the studies enrolled small populations and included highly selected patient cohorts with or without the disease, which may not fully represent the broader population encountered in clinical practice.
Several studies have subsequently examined the patterns of resting magnetic fields in individuals with CAD. These studies have evaluated different parameters of MCG and have endeavored to enhance diagnostic accuracy and minimize background noise by employing various analytical approaches and algorithms. The earlier study revealed significant differences in multiple MCG parameters such as ST slope, ST shift, T peak amplitude, ST-T integral, and magnetic field map (MFM) orientation between patients with CAD (n = 101) and a control group of healthy subjects (n = 59) (40). They yielded a specificity and sensitivity of 83% and 84% respectively [with an area under the curve (AUC) of 91.2% for the receiver operating curve (ROC)], and the accuracy of CAD classification at 84% remained consistent regardless of the number of affected vessels or the severity of stenosis. In addition, various quantitative methods have been employed to differentiate CAD. These methods include binary classification approaches utilizing threshold values for MCG indices (5, 28, 35, 36), integrated indices derived from MCG parameter values (20, 50–52), the assessment of the number of abnormal MCG parameters (31), spatial distribution analysis of the QT interval (34), and the utilization of automated machine learning algorithms (25–27). In a recent study, a combination of quantitative (change in ST-segment fluctuation score) and qualitative (non-dipole phenomenon) parameters was utilized to improve the diagnostic accuracy of shielded MCG in distinguishing patients with stable angina from asymptomatic individuals without CAD (18). The inclusion of the non-dipole phenomenon resulted in an increased AUC of the ROC curve, elevating it from 0.79 to 0.93.
Initial investigations on MCG in patients with CAD demonstrated its capacity to identify alterations in multiple MCG parameters during stress induced by exercise or drugs. The analysis indicated that ST segment MCG parameters exhibited greater sensitivity to exercise-induced ischemia in patients without a history of MI (n = 27), whereas T wave MCG parameters were most sensitive to changes in patients with prior MI (n = 17) (13). For the assessment of 42 patients with CAD following a dobutamine-stress test, an analytical approach centered on the epicardial current distribution at the point of maximum amplitude of the QRS complex (QRSmax) was employed (9). MCG demonstrated a sensitivity of over 90% for detecting CAD, irrespective of the location of stenosis or the number of affected vessels.
Several studies have directly compared the diagnostic efficacy of MCG with other tests. In a study by Park et al., MCG exhibited superior sensitivity compared to 12-lead EKG in detecting CAD using a conventional dobutamine stress protocol (9). Another study demonstrated higher sensitivity, along with comparable specificity, and similar positive predictive value (PPV) and negative predictive value (NPV) for MCG compared to EKG in the diagnosis of stable angina (41). In another study, MCG showed higher specificity and comparable sensitivity, PPV, and NPV when compared to single photon emission computed tomography (SPECT) for discriminating patients with angina (39).
In studies involving patients experiencing acute chest pain and suspected ACS, the analysis of MCG data, measured either at rest or after exercise, in shielded or unshielded environments, has revealed qualitative and quantitative distinctions that facilitate differentiation between patients with ACS and healthy individuals (15, 16, 23, 43, 44, 53, 54). Moreover, MCG has been successful in distinguishing patients without definitive evidence of ACS or CAD in diagnostic examinations (7, 8, 14, 15, 42, 44–46, 55, 56). A previous study utilizing a shielded, 64-channel MCG system showed the capability of 15 MCG parameters to discriminate between patients diagnosed with non-ST segment elevation myocardial infarction (NSTEMI) (n = 83) and age-matched individuals presenting with chest pain but without clinical indications of CAD (15). Among these parameters, the field map angle of the T wave peak exhibited the highest diagnostic accuracy, with a sensitivity of 86% and a specificity of 75%. In a prospective study involving 402 patients experiencing acute chest pain without ST-segment elevation in the EKG, it was observed that abnormalities in the MFM between the onset and peak of the T wave at admission were predictive of an elevated risk of mortality over a 3-year period. The relative risk for MCG abnormalities was 4.58, compared to 1.69 for EKG, and 2.58 for elevated troponin levels (8). Another study found that MCG has the potential to differentiate patients with ACS and bundle branch block, a condition that can complicate the diagnosis of ACS when using EKG (47, 48). MCG has also shown promise in discriminating patients with reduced left ventricular ejection fraction (37) and those with a history of previous MI (57). However, further studies with larger patient populations are necessary to explore the full potential of MCG in these particular conditions. Additionally, a direct comparison between MCG, utilizing either visual or automated analysis, and other diagnostic tests such as EKG, cardiac troponin I, and echocardiography, revealed that MCG showed higher sensitivity, comparable specificity, comparable positive predictive value (PPV), and higher negative predictive value (NPV) in distinguishing patients with CAD and acute chest pain from patients with chest pain but normal results on diagnostic tests (42).
Previous studies evaluated various MCG parameters to improve the detection of stable CAD or ACS in patients with different clinical presentations. MCG proved effective in identifying ischemia, even in patients with normal EKG and cardiac biomarker results. Initial evidence suggests acceptable sensitivity and specificity for detecting IHD in selected cohorts with stable CAD or ACS, with MCG outperforming EKG, echocardiography, and cardiac troponin assays. MCG could be a valuable initial test for suspected CAD or ACS, but more research is needed to determine the best parameters and validate its diagnostic performance across diverse patient populations. Further studies should focus on integrating MCG into clinical practice and assessing its incremental value in existing diagnostic pathways, potentially leading to the development of MCG criteria for early exclusion of non-ischemic or non-CAD patients, reducing unnecessary testing and hospital resource utilization. In addition, to address the challenges posed by the evolving nature of MCG technology and diagnostic criteria in CAD studies conducted over several decades, a meta-analysis of current data or the following approaches are needed. Although significant progress has been made in MCG device technology and machine-learning analysis techniques, further validation of potential diagnostic parameters is necessary, particularly in large patient cohorts that represent a diverse range of cases.
The use of MCG has the potential to benefit the assessment of patients with suspected ACS, particularly in the field of emergency medicine. Chest pain is a common reason for emergency department visits, but a significant portion of patients (60%–90%) do not have an acute cardiac cause for their pain. Current diagnosis of ACS in patients with acute undifferentiated chest pain involves a resting 12-lead EKG, multiple measurements of cardiac troponin levels over several hours, and clinical judgment. Integrating MCG into the diagnostic pathway could help reduce the time to diagnosis and the costs associated with serial troponin testing. Another challenge in emergency medicine is the risk of missed diagnoses of patients with NSTEMI or unstable angina, which can lead to adverse outcomes after discharge. MCG has the potential to decrease the likelihood of missed diagnoses and improve clinical outcomes. The benefits of early identification of patients with non-cardiac chest pain have been demonstrated through accelerated risk algorithms that incorporate high-sensitivity cardiac troponin assays, resulting in significant improvements in time to discharge, cardiac outcomes, and hospital resource utilization. Further evaluation through prospective observational studies involving unselected cohorts of patients presenting to the emergency department with acute chest pain will provide insights into whether MCG could be used prior to cardiac troponin testing to expedite patient assessment. Most of the original multichannel MCG devices have specific operational requirements and high running costs, primarily due to the need for external electromagnetic shielding (EMS) or liquid helium cooling. However, the recent development of portable MCG devices holds the potential for bedside assessment of patients with acute chest pain upon their initial presentation to the emergency department (23, 58). Enhancements in the practical aspects of MCG devices such as device footprint, ease of use, operator training requirements, and the need for a shielded operating environment will play a crucial role in determining their ease of implementation in clinical practice.
Finally, validation studies are necessary to determine the diagnostic accuracy of MCG parameters compared to current diagnostic pathways in undifferentiated patient populations. Validated MCG diagnostic criteria should be evaluated in well-defined cohorts including patients with stable CAD, ACS, inducible ischemia, and non-ischemic chest pain. Furthermore, there are indications in the literature that MCG may have broader clinical applications in CAD beyond diagnosis. For instance, its use in stress testing to detect functional ischemia could provide valuable prognostic information for risk stratification. Future clinical studies should explore other endpoints such as infarction location and severity, as well as the prediction of major adverse cardiac events and post-MI arrhythmias.
MCG presents a non-invasive and non-contact imaging modality that is free from emissions, offering potential improvements in the management of patients with CAD. It has demonstrated the ability to detect myocardial ischemia in patients with stable CAD and ACS. However, further clinical studies are necessary to evaluate the use of MCG in undifferentiated patient cohorts. It is also important to validate and standardize MCG analytical techniques and parameters. Prospective, multicenter observational studies are currently needed to investigate the effectiveness of MCG in ruling out ACS in emergency settings. These studies will help determine the utility of newer MCG devices and their potential integration into routine clinical practice as complementary diagnostic tools.
Conceptualization: AH, YK, and ES. Supervision: YK, SK, and ES. Visualization: AH, DD, YK, SK, and ES. Writing-original draft: AH. Writing-review & editing: AH, DD, YK, SK, and ES. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The handling editor JP declared a shared affiliation with the author DD at the time of review.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Tsao CW, Aday AW, Almarzooq ZI, Anderson CAM, Arora P, Avery CL, et al. Heart disease and stroke statistics-2023 update: a report from the American heart association. Circulation. (2023) 147(8):e93–e621. doi: 10.1161/cir.0000000000001123
2. Levine GN, Bates ER, Bittl JA, Brindis RG, Fihn SD, Fleisher LA, et al. 2016 ACC/AHA guideline focused update on duration of dual antiplatelet therapy in patients with coronary artery disease: a report of the American college of cardiology/American heart association task force on clinical practice guidelines: an update of the 2011 ACCF/AHA/SCAI guideline for percutaneous coronary intervention, 2011 ACCF/AHA guideline for coronary artery bypass graft surgery, 2012 ACC/AHA/ACP/AATS/PCNA/SCAI/STS guideline for the diagnosis and management of patients with stable ischemic heart disease, 2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction, 2014 AHA/ACC guideline for the management of patients with non-ST-elevation acute coronary syndromes, and 2014 ACC/AHA guideline on perioperative cardiovascular evaluation and management of patients undergoing noncardiac surgery. Circulation. (2016) 134:e123–55. doi: 10.1161/cir.0000000000000404
3. Lin GA, Dudley RA, Lucas FL, Malenka DJ, Vittinghoff E, Redberg RF. Frequency of stress testing to document ischemia prior to elective percutaneous coronary intervention. JAMA. (2008) 300:1765–73. doi: 10.1001/jama.300.15.1765
4. Lin GA, Lucas FL, Malenka DJ, Skinner J, Redberg RF. Mortality in medicare patients undergoing elective percutaneous coronary intervention with or without antecedent stress testing. Circ Cardiovasc Qual Outcomes. (2013) 6:309–14. doi: 10.1161/circoutcomes.113.000138
5. Park JW, Shin ES, Ann SH, Gödde M, Park LS, Brachmann J, et al. Validation of magnetocardiography versus fractional flow reserve for detection of coronary artery disease. Clin Hemorheol Microcirc. (2015) 59:267–81. doi: 10.3233/ch-141912
6. Fenici R, Brisinda D, Meloni AM. Effects of filtering on computer-aided analysis for detection of chronic ischemic heart disease with unshielded rest magnetocardiographic mapping. Neurol Clin Neurophysiol. (2004) 2004:7.16012666
7. Kyoon Lim H, Kim K, Lee YH, Chung N. Detection of non-ST-elevation myocardial infarction using magnetocardiogram: new information from spatiotemporal electrical activation map. Ann Med. (2009) 41:533–46. doi: 10.1080/07853890903107883
8. Park JW, Leithäuser B, Hill P, Jung F. Resting magnetocardiography predicts 3-year mortality in patients presenting with acute chest pain without ST segment elevation. Ann Noninvasive Electrocardiol. (2008) 13:171–9. doi: 10.1111/j.1542-474X.2008.00217.x
9. Park JW, Leithäuser B, Vrsansky M, Jung F. Dobutamine stress magnetocardiography for the detection of significant coronary artery stenoses—a prospective study in comparison with simultaneous 12-lead electrocardiography. Clin Hemorheol Microcirc. (2008) 39:21–32. doi: 10.3233/CH-2008-1064
10. Fenici R, Brisinda D, Meloni AM. Clinical application of magnetocardiography. Expert Rev Mol Diagn. (2005) 5:291–313. doi: 10.1586/14737159.5.3.291
11. Her AY, Park JW. Repolarization heterogeneity of magnetocardiography predicts long-term prognosis in patients with acute myocardial infarction. Yonsei Med J. (2016) 57:1305–6. doi: 10.3349/ymj.2016.57.6.1305
12. Hänninen H, Takala P, Mäkijärvi M, Montonen J, Korhonen P, Oikarinen L, et al. Recording locations in multichannel magnetocardiography and body surface potential mapping sensitive for regional exercise-induced myocardial ischemia. Basic Res Cardiol. (2001) 96:405–14. doi: 10.1007/s003950170049
13. Hänninen H, Takala P, Korhonen P, Oikarinen L, Mäkijärvi M, Nenonen J, et al. Features of ST segment and T-wave in exercise-induced myocardial ischemia evaluated with multichannel magnetocardiography. Ann Med. (2002) 34:120–9. doi: 10.1080/07853890252953518
14. Tolstrup K, Madsen BE, Ruiz JA, Greenwood SD, Camacho J, Siegel RJ, et al. Non-invasive resting magnetocardiographic imaging for the rapid detection of ischemia in subjects presenting with chest pain. Cardiology. (2006) 106:270–6. doi: 10.1159/000093490
15. Lim HK, Chung N, Kim K, Ko YG, Kwon H, Lee YH, et al. Can magnetocardiography detect patients with non-ST-segment elevation myocardial infarction? Ann Med. (2007) 39:617–27. doi: 10.1080/07853890701538040
16. Lim HK, Kwon H, Chung N, Ko YG, Kim JM, Kim IS, et al. Usefulness of magnetocardiogram to detect unstable angina pectoris and non-ST elevation myocardial infarction. Am J Cardiol. (2009) 103:448–54. doi: 10.1016/j.amjcard.2008.10.013
17. Shin ES, Chung JH, Park SG, Saleh A, Lam YY, Bhak J, et al. Comparison of exercise electrocardiography and magnetocardiography for detection of coronary artery disease using ST-segment fluctuation score. Clin Hemorheol Microcirc. (2019) 73:283–91. doi: 10.3233/ch-180485
18. Shin ES, Lam YY, Her AY, Brachmann J, Jung F, Park JW. Incremental diagnostic value of combined quantitative and qualitative parameters of magnetocardiography to detect coronary artery disease. Int J Cardiol. (2017) 228:948–52. doi: 10.1016/j.ijcard.2016.11.165
19. Shin ES, Park JW, Lim DS. Magnetocardiography for the diagnosis of non-obstructive coronary artery disease1. Clin Hemorheol Microcirc. (2018) 69:9–11. doi: 10.3233/ch-189106
20. Shin ES, Park SG, Saleh A, Lam YY, Bhak J, Jung F, et al. Magnetocardiography scoring system to predict the presence of obstructive coronary artery disease. Clin Hemorheol Microcirc. (2018) 70:365–73. doi: 10.3233/ch-189301
21. Kobayashi T, Kuriki S. Principal component elimination method for the improvement of S/N in evoked neuromagnetic field measurements. IEEE Trans Biomed Eng. (1999) 46:951–8. doi: 10.1109/10.775405
22. Yang HC, Hung SY, Wu CH, Chen JC, Hsu SJ, Liao SH, et al. High-Tc SQUID magnetocardiography imaging system. Neurol Clin Neurophysiol. (2004) 2004:23.16012658
23. Ghasemi-Roudsari S, Al-Shimary A, Varcoe B, Byrom R, Kearney L, Kearney M. A portable prototype magnetometer to differentiate ischemic and non-ischemic heart disease in patients with chest pain. PLoS One. (2018) 13:e0191241. doi: 10.1371/journal.pone.0191241
24. Huang X, Chen P, Tang F, Hua N. Detection of coronary artery disease in patients with chest pain: a machine learning model based on magnetocardiography parameters. Clin Hemorheol Microcirc. (2021) 78:227–36. doi: 10.3233/ch-200905
25. Rong T, Shulin Z, Xiao H, Minfang T, Jian M, Shixin M, et al. Magnetocardiography-Based ischemic heart disease detection and localization using machine learning methods. IEEE Trans Biomed Eng. (2019) 66:1658–67. doi: 10.1109/tbme.2018.2877649
26. Kangwanariyakul Y, Nantasenamat C, Tantimongcolwat T, Naenna T. Data mining of magnetocardiograms for prediction of ischemic heart disease. Excli J. (2010) 9:82–95.29255391
27. Tantimongcolwat T, Naenna T, Isarankura-Na-Ayudhya C, Embrechts MJ, Prachayasittikul V. Identification of ischemic heart disease via machine learning analysis on magnetocardiograms. Comput Biol Med. (2008) 38:817–25. doi: 10.1016/j.compbiomed.2008.04.009
28. Steinberg BA, Roguin A, Watkins SP 3rd, Hill P, Fernando D, Resar JR. Magnetocardiogram recordings in a nonshielded environment–reproducibility and ischemia detection. Ann Noninvasive Electrocardiol. (2005) 10:152–60. doi: 10.1111/j.1542-474X.2005.05611.x
29. Ramesh R, Senthilnathan S, Satheesh S, Swain PP, Patel R, Ananthakrishna Pillai A, et al. Magnetocardiography for identification of coronary ischemia in patients with chest pain and normal resting 12-lead electrocardiogram. Ann Noninvasive Electrocardiol. (2020) 25:e12715. doi: 10.1111/anec.12715
30. Huang X, Hua N, Tang F, Zhang S. Effectiveness of magnetocardiography to identify patients in need of coronary artery revascularization: a cross-sectional study. Cardiovasc Diagn Ther. (2020) 10:831–40. doi: 10.21037/cdt-20-121
31. Brisinda D, Meloni AM, Fenici R, editors. First 36-channel magnetocardiographic study of CAD patients in an unshielded laboratory for interventional and intensive cardiac care. Functional imaging and modeling of the heart. Berlin, Heidelberg: Springer Berlin Heidelberg (2003). p. 122–31.
32. Fenici R, Brisinda D, Meloni AM, Sternickel K, Fenici P, editors. Clinical validation of machine learning for automatic analysis of multichannel magnetocardiography. Functional imaging and modeling of the heart. Berlin, Heidelberg: Springer Berlin Heidelberg (2005). p. 143–52.
33. Hänninen H, Takala P, Mäkijärvi M, Montonen J, Korhonen P, Oikarinen L, et al. Detection of exercise-induced myocardial ischemia by multichannel magnetocardiography in single vessel coronary artery disease. Ann Noninvasive Electrocardiol. (2000) 5:147–57. doi: 10.1111/j.1542-474X.2000.tb00380.x
34. Van Leeuwen P, Hailer B, Lange S, Grönemeyer D. Spatial distribution of repolarization times in patients with coronary artery disease. Pacing Clin Electrophysiol. (2003) 26:1706–14. doi: 10.1046/j.1460-9592.2003.t01-1-00256.x
35. Van Leeuwen P, Hailer B, Lange S, Grönemeyer DH. Identification of patients with coronary artery disease using magnetocardiographic signal analysis. Biomed Tech. (2006) 51:83–8. doi: 10.1515/bmt.2006.015
36. On K, Watanabe S, Yamada S, Takeyasu N, Nakagawa Y, Nishina H, et al. Integral value of JT interval in magnetocardiography is sensitive to coronary stenosis and improves soon after coronary revascularization. Circ J. (2007) 71:1586–92. doi: 10.1253/circj.71.1586
37. Goernig M, Liehr M, Tute C, Schlosser M, Haueisen J, Figulla HR, et al. Magnetocardiography based spatiotemporal correlation analysis is superior to conventional ECG analysis for identifying myocardial injury. Ann Biomed Eng. (2009) 37:107–11. doi: 10.1007/s10439-008-9598-5
38. Gapelyuk A, Schirdewan A, Fischer R, Wessel N. Cardiac magnetic field mapping quantified by kullback-leibler entropy detects patients with coronary artery disease. Physiol Meas. (2010) 31:1345–54. doi: 10.1088/0967-3334/31/10/004
39. Wu YW, Lin LC, Tseng WK, Liu YB, Kao HL, Lin MS, et al. QTc heterogeneity in rest magnetocardiography is sensitive to detect coronary artery disease: in comparison with stress myocardial perfusion imaging. Acta Cardiol Sin. (2014) 30:445–54.27122818
40. Gapelyuk A, Wessel N, Fischer R, Zacharzowsky U, Koch L, Selbig D, et al. Detection of patients with coronary artery disease using cardiac magnetic field mapping at rest. J Electrocardiol. (2007) 40:401–7. doi: 10.1016/j.jelectrocard.2007.03.013
41. Fenici R, Brisinda D. Predictive value of rest magnetocardiography in patients with stable angina. Int Congr Ser. (2007) 1300:737–40. doi: 10.1016/j.ics.2007.02.022
42. Park JW, Hill PM, Chung N, Hugenholtz PG, Jung F. Magnetocardiography predicts coronary artery disease in patients with acute chest pain. Ann Noninvasive Electrocardiol. (2005) 10:312–23. doi: 10.1111/j.1542-474X.2005.00634.x
43. Lant J, Stroink G, ten Voorde B, Horacek BM, Montague TJ. Complementary nature of electrocardiographic and magnetocardiographic data in patients with ischemic heart disease. J Electrocardiol. (1990) 23:315–22. doi: 10.1016/0022-0736(90)90121-h
44. Kwon H, Kim K, Lee YH, Kim JM, Yu KK, Chung N, et al. Non-invasive magnetocardiography for the early diagnosis of coronary artery disease in patients presenting with acute chest pain. Circ J. (2010) 74:1424–30. doi: 10.1253/circj.cj-09-0975
45. Park JW, Jung F. Qualitative and quantitative description of myocardial ischemia by means of magnetocardiography. Biomed Tech. (2004) 49:267–73. doi: 10.1515/bmt.2004.050
46. Lin LJ, Tang FK, Hua N, Lu H, editors. Contrast between magnetocardiography and electrocardiography for the early diagnosis of coronary artery disease in patients with acute chest pain. 2011 computing in cardiology. (2011). p. 641–3.
47. Leithäuser B, Park JW, Hill P, Lam YY, Jung F. Magnetocardiography in patients with acute chest pain and bundle branch block. Int J Cardiol. (2013) 168:582–3. doi: 10.1016/j.ijcard.2013.01.254
48. Park J-W, Leithäuser B, Jung F. Magnetocardiography predicts coronary artery disease in bundle-branch block patients with acute chest pain. J Electrocardiol. (2007) 40(1):S53. doi: 10.1016/j.jelectrocard.2006.10.033
49. Brisinda D, Meloni AM, Fenici R. Clinical multichannel MCG in unshielded hospital environment. Neurol Clin Neurophysiol. (2004) 2004:8.16015715
50. Van Leeuwen P, Hailer B, Lange S, Klein A, Geue D, Seybold K, et al. Quantification of cardiac magnetic field orientation during ventricular de- and repolarization. Phys Med Biol. (2008) 53:2291–301. doi: 10.1088/0031-9155/53/9/006
51. Chaikovsky I, Hailer B, Sosnytskyy V, Lutay M, Mjasnikov G, Kazmirchuk A, et al. Predictive value of the complex magnetocardiographic index in patients with intermediate pretest probability of chronic coronary artery disease: results of a two-center study. Coron Artery Dis. (2014) 25:474–84. doi: 10.1097/mca.0000000000000107
52. Ogata K, Kandori A, Watanabe Y, Suzuki A, Tanaka K, Oka Y, et al. Repolarization spatial-time current abnormalities in patients with coronary heart disease. Pacing Clin Electrophysiol. (2009) 32:516–24. doi: 10.1111/j.1540-8159.2009.02313.x
53. Budnyk MM, Kozlovsky VI, Stadnyuk LA, Zahrabova OM, Ryzhenko TM, Getman TV. Evaluation of magnetocardiography indices in patients with cardiac diseases. Neurol Clin Neurophysiol. (2004) 2004:111.16012664
54. Sosnytskyy V, Chaikovsky I, Stadnyuk L, Miasnykov G, Kazmirchyk A, Sosnytska T, et al. Magnetocardiography capabilities in myocardium injuries diagnosis. World J Cardiovasc Dis. (2013) 3(5):9. doi: 10.4236/wjcd.2013.35059
55. Goodacre S, Walters SJ, Qayyum H, Coffey F, Carlton E, Coats T, et al. Diagnostic accuracy of the magnetocardiograph for patients with suspected acute coronary syndrome. Emerg Med J. (2021) 38:47–52. doi: 10.1136/emermed-2020-210396
56. Koivisto T, Lahdenoja O, Hurnanen T, Vasankari T, Jaakkola S, Kiviniemi T, et al. Mechanocardiography in the detection of acute ST elevation myocardial infarction: the MECHANO-STEMI study. Sensors. (2022) 22(12):4384. doi: 10.3390/s22124384
57. Korhonen P, Husa T, Tierala I, Väänänen H, Mäkijärvi M, Katila T, et al. QRS Duration in high-resolution methods and standard ECG in risk assessment after first and recurrent myocardial infarctions. Pacing Clin Electrophysiol. (2006) 29:830–6. doi: 10.1111/j.1540-8159.2006.00448.x
Keywords: magnetocardiography, myocardial ischemia, coronary artery disease, electrocardiography, acute coronary syndrome
Citation: Her A-Y, Dischl D, Kim YH, Kim S-W and Shin E-S (2023) Magnetocardiography for the detection of myocardial ischemia. Front. Cardiovasc. Med. 10:1242215. doi: 10.3389/fcvm.2023.1242215
Received: 18 June 2023; Accepted: 28 June 2023;
Published: 7 July 2023.
Edited by:
Jai-Wun Park, Charité University Medicine Berlin, GermanyReviewed by:
Friedrich Jung, Helmholtz Centre for Materials and Coastal Research (HZG), Germany© 2023 Her, Dischl, Kim, Kim and Shin. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Eun-Seok Shin c2VzaW0xOTg5QGdtYWlsLmNvbQ==
†ORCID Ae-Young Her orcid.org/0000-0002-9990-6843 Dominic Dischl orcid.org/0000-0001-8382-765X Yong Hoon Kim orcid.org/0000-0002-9669-3598 Sang-Wook Kim orcid.org/0000-0002-7208-8596 Eun-Seok Shin orcid.org/0000-0002-9169-6968
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.