 Yuping Xiang
Yuping Xiang Qin Zhao
Qin Zhao- Department of Critical Care Medicine, West China Hospital, Sichuan University/West China School of Nursing, Sichuan University, Chengdu, China
Background: Pulmonary complications occur in a substantial proportion of patients who undergo coronary artery bypass grafting. Inspiratory muscle training (IMT), a simple, well-tolerated physical therapy, has been proposed to reduce the risk of complications, but its efficacy remains controversial.
Method: Randomized controlled trials (RCTs) examining the influence of IMT on the risk of pulmonary complications after coronary artery bypass grafting were identified from PubMed, Embase, CENTRAL, CINAL, and Web of Science through March 2023. Data were meta-analyzed for the primary outcomes of pulmonary complications, defined as pneumonia, pleural effusion, and atelectasis; and in terms of the secondary outcomes of maximum inspiratory pressure, maximum expiratory pressure, length of hospitalization, 6 min walk test, and peak expiratory flow and other outcomes. Risk of bias and quality of evidence assessments were carried out using the RoB 2.0 and Grading of Recommendations Assessment, Development and Evaluation (GRADE) applied to primary outcomes of pulmonary complications.
Results: Data from eight RCTs involving 755 patients were meta-analyzed. IMT was associated with a significantly lower risk of postoperative pneumonia [relative risk (RR) 0.39, 95% confidence interval (CI) 0.25–0.62, P < 0.0001] and atelectasis (RR 0.43, 95% CI 0.27–0.67, P = 0.0002), but not pleural effusion (RR 1.09, 95% CI 0.62–1.93, P = 0.76). IMT was associated with significantly better maximum inspiratory pressure (preoperative: mean difference (MD) 16.55 cmH2O, 95% CI 13.86–19.24, P < 0.00001; postoperative: mean difference (MD) 8.99 cmH2O, 95% CI 2.39–15.60, P = 0.008) and maximum expiratory pressure (MD 7.15 cmH2O, 95% CI: 1.52–12.79, P = 0.01), and with significantly shorter hospitalization (MD −1.71 days, 95% CI −2.56 to −0.87, P < 0.001). IMT did not significantly affect peak expiratory flow or distance traveled during the 6 min walk test.
Conclusions: The available evidence from medium and high quality trials suggests that IMT can significantly decrease the risk of pneumonia and atelectasis after coronary artery bypass grafting while shortening hospitalization and improving the strength of respiratory muscles.
Systematic Review Registration: https://www.crd.york.ac.uk/prospero/, identifier: CRD42023415817.
Introduction
Cardiovascular disease, which is fast becoming the leading cause of death and disability worldwide (1) and caused 17.8 million deaths globally in 2017 (2), is a major health concern together with coronary heart disease, which has a prevalence of 6%–7% in North America, Europe, and Asia (3). Common forms of these diseases are stenosis of the left main coronary artery and multivessel disease, which are typically treated through surgery involving coronary artery bypass grafting (CABG) (4). Such grafting involves substantial risk of pulmonary complications including pneumonia, atelectasis, respiratory failure, pleural effusion, acute respiratory distress syndrome, and pneumothorax (5, 6). These complications can lead to hypoxemia, which affects 11%–40% of patients who undergo CABG (7), and they can prolong hospitalization and increase healthcare costs (8).
Numerous factors appear to contribute to postoperative pulmonary complications after CABG, and a major one is inadequate respiratory muscle function (9). One quarter of patients awaiting elective cardiac surgery show inspiratory muscle weakness (10), which reduces vital capacity, tidal volume, and total lung capacity. It leads to insufficient cough, increasing risk of atelectasis, and pneumonia. Risk of pulmonary complications after CABG can be reduced through respiratory physiotherapy, epidural analgesia, and enhanced recovery protocols (11). Several meta-analyses have concluded that inspiratory muscle training (IMT) can strengthen respiratory muscles and prevent muscle fatigue (12–16). In addition, some scholars have reported that IMT can reduce the incidence of postoperative pulmonary complications (PPCs) (17–19) and short hospitalization (20), but these previous analyses were not comprised of only CABG patients.
A meta-analysis confirmed that IMT had a reduced risk of postoperative pneumonia for CABG patients, which included four studies, and the cutoff time for inclusion was 2017 (21). In recent years, several randomized controlled trials (RCTs) have examined the effects of IMT on PPCs (including pneumonia, atelectasis, and pleural effusion) after CABG. Therefore, we systematically reviewed the literature to identify such RCTs and meta-analyzed their data in order to provide a rigorous assessment of available evidence.
Methods
This systematic review and meta-analysis were conducted in accordance with the “Preferred Reporting Items for Systematic Reviews and Meta-Analyses” (PRISMA) guidelines and were registered with the identifier CRD42023415817.
Literature search and study inclusion
We systematically searched the following databases for RCTs indexed through March 2023: PubMed, Embase, Cochrane Library (CENTRAL), CINAL (via EBSCO), and Web of Science. Search strings contained the terms coronary artery bypass [as Medical Subject Heading], coronary artery bypass*, coronary artery bypass surgery, aortocoronary bypass*, coronary artery bypass grafting, CABG, myocardial revascularization, vascular grafting, coronary artery bypass graft; AND breathing exercises [as Medical Subject Heading], breathing exercise*, respiratory muscle training, inspiratory muscle training, expiratory muscle training, inspiratory muscle strength, respiratory exercise, inspiratory muscle train*, respiratory train, ventilatory train, breathing train, respiratory therapy, IMT, RMT (Supplementary Appendix 1). In addition, we manually searched the reference lists of relevant studies.
To be included in this review and meta-analysis, studies had to (1) examine patients at least 18 years old who underwent CABG either pre- or postoperatively; (2) apply a randomized controlled design in which the IMT arm was compared to an arm that received sham IMT, physical therapy, or usual care; (3) report data on at least one of pneumonia, pleural effusion, or atelectasis; and (4) the language of the publication was not limited. Studies were excluded if the full text was unavailable or if they were reviews or observational studies.
Data extraction and outcomes
Two authors independently extracted the following data using a data extraction form developed a priori: (1) study characteristics, including author name, title, comparison arms, and year of publication; (2) population characteristics, including age, sex, and sample size; (3) details of interventions, including training type, frequency, session duration, and intensity; and (4) outcomes. Primary outcomes were rates of pneumonia, pleural effusion, and atelectasis. Secondary outcomes were maximum inspiratory pressure (MIP), maximum expiratory pressure (MEP), Pmpeak/Pimax, and length of hospitalization (LOS). Other outcomes such as exercise capacity were meta-analyzed when relevant data were reported. If outcome data were unclear or not reported, we contacted the authors in an attempt to obtain missing data.
Assessment of study quality
Two authors independently assessed the risk of bias for included studies using the RoB 2.0 tools for randomized trials and included the following domains: randomization/allocation process, deviation from intended intervention, missing outcome data, outcome measurement, and selective outcome reporting. Visualization of RoB 2.0 was produced using robvis. Studies were judged to be at low, high, or unclear risk of bias. Similarly, discordance was dealt with by adjudication among the authors until consensus was reached by following the appropriate algorithms.
Statistical analysis
Statistical analyses were conducted using RevMan 5.3 software. Statistical heterogeneity in pooled results was assessed using the chi-squared test, Cochran's Q-test, and the inconsistency I2 test, in which I2 values of 25%, 50%, or 75% were considered cut-offs to indicate low, moderate, or high heterogeneity, respectively (22). We performed random-effect heterogeneity in the event of moderate or high heterogeneity. Where appropriate, results were reported as relative risk (RR) and associated 95% confidence interval (CI). The mean difference (MD) was used as the effect size if studies used the same tool to measure the outcome. We used the Grading of Recommendations Assessment, Development and Evaluation (GRADE) system to assess the quality of the body of evidence associated with the following specific outcomes in our review and constructed a summary of findings for the main outcomes: pneumonia, atelectasis, and pleural effusion. This assessment considers the study methodological quality, directness of the evidence, heterogeneity of the data, precision of the effect estimates, and the risk of publication bias.
Results
Study selection
Database search yielded 1,390 potentially eligible articles, while manual searching of reference lists did not identify additional studies. After excluding 440 duplicates and 926 studies based on their titles and abstracts, the full text of 24 publications was examined, leading to the exclusion of 16 studies (Figure 1). In the end, a total of eight studies (23–30) met the inclusion criteria and were utilized for meta-analysis (Table 1).
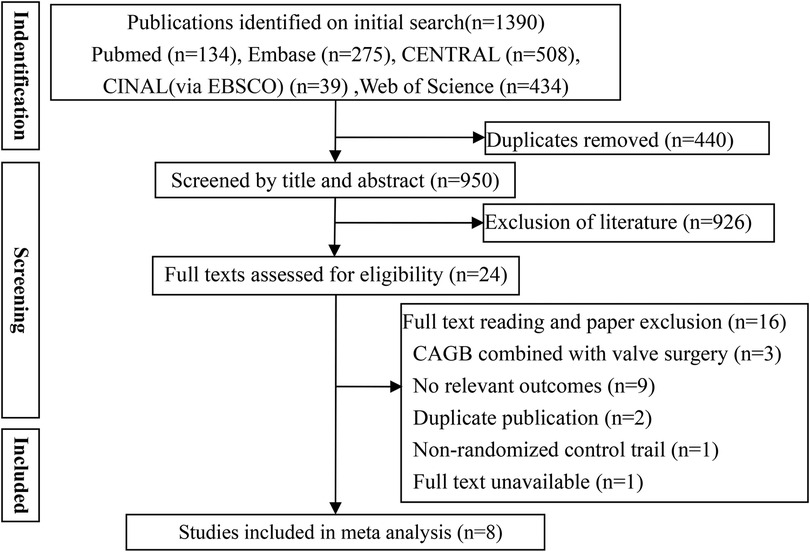
Figure 1. Flowchart of study selection.
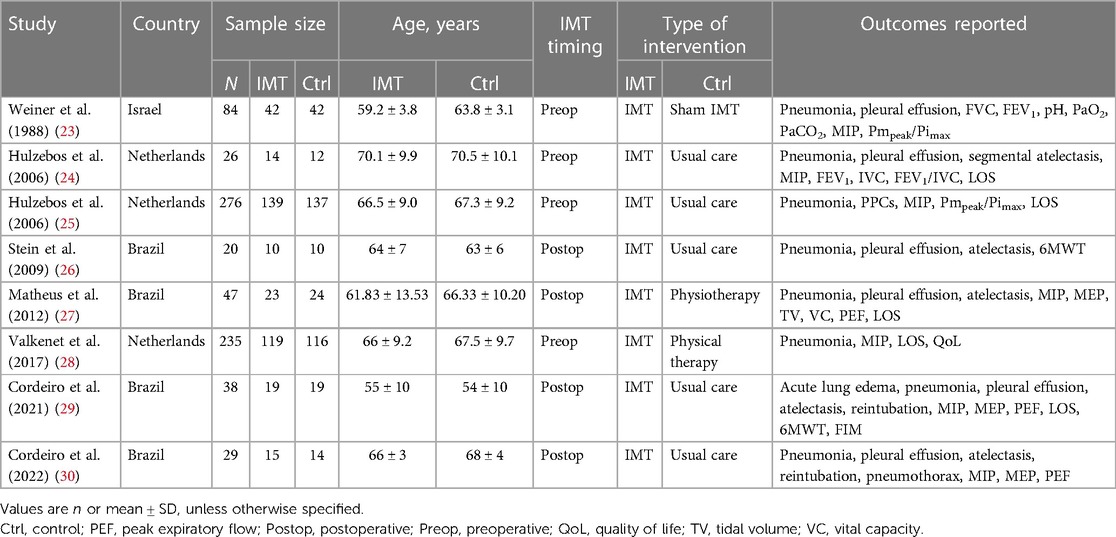
Table 1. Characteristics of included studies.
Study characteristics
These studies, each of which enrolled 20–276 patients, involved a total of 755 patients. Studies examined pre- and postoperative IMT, which usually involved the threshold IMT, and involved an intensity at 30%–60% of MIP once to twice daily for durations ranging from 3 days to 4 weeks (Table 2). Most studies described the details of random sequence generation, blinding during outcome assessment, incomplete outcome data, selective reporting, and other biases (Figure 2). However, few studies described details of allocation concealment or blinding of participants and investigators.
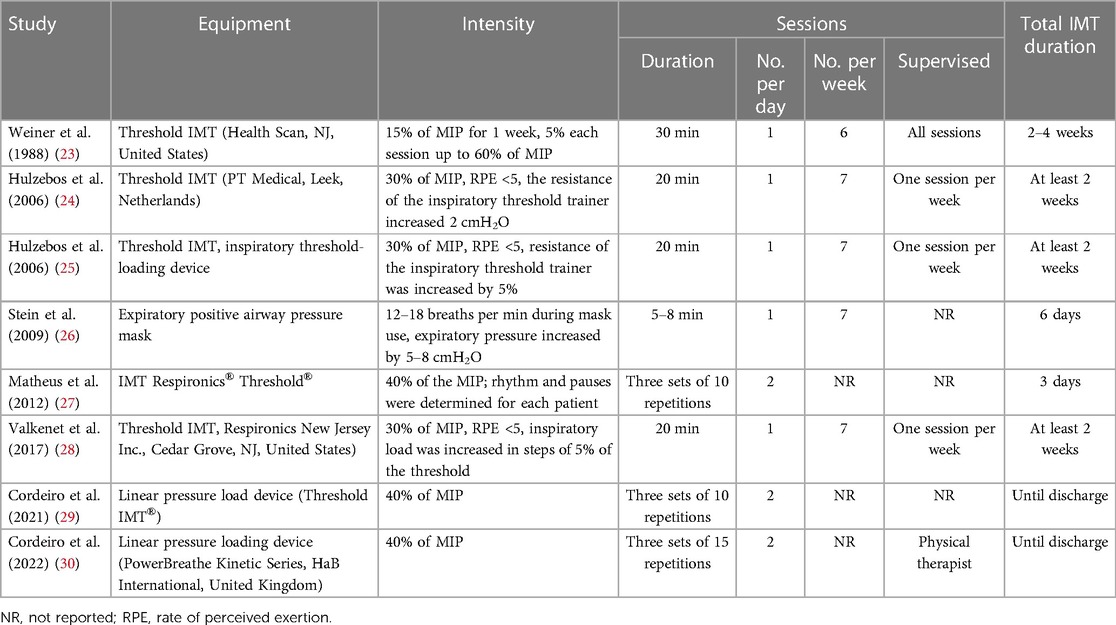
Table 2. Details of IMT training in included studies.
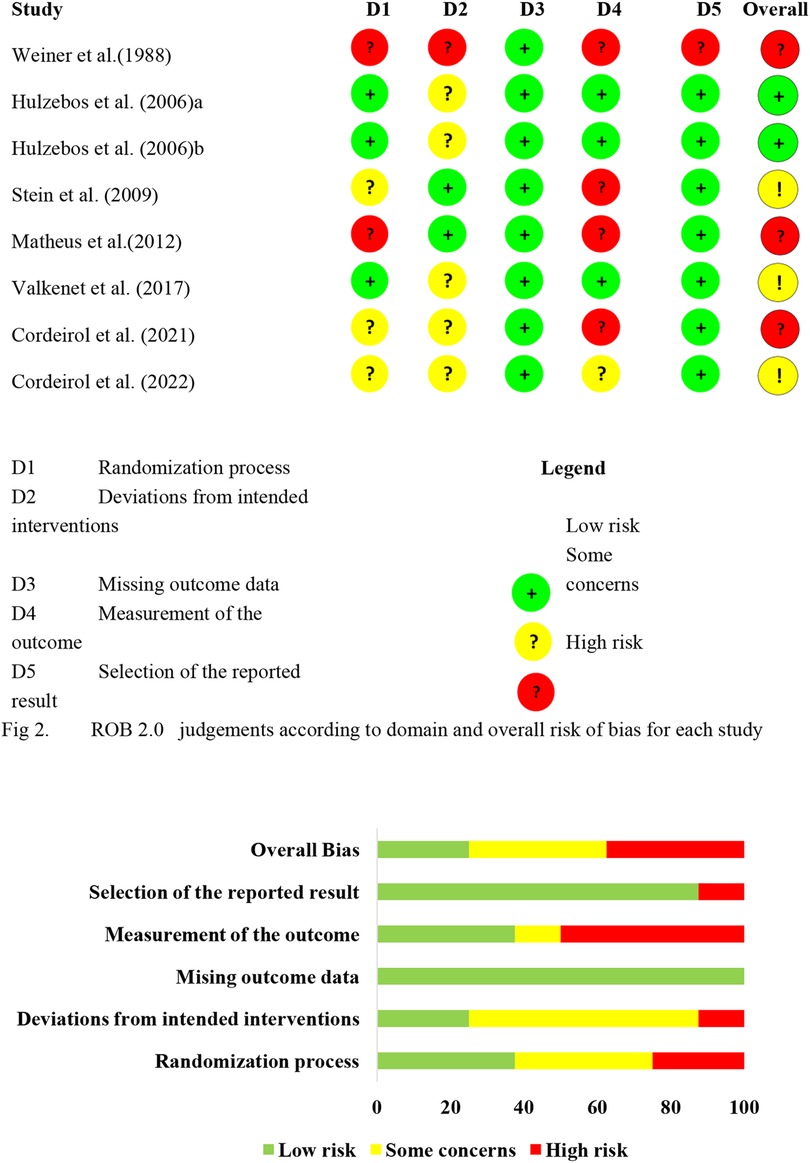
Figure 2. Risk of bias summary. ROB 2.0 judgements according to domain and overall risk of bias for each study.
Methodological quality
Figure 2 shows the results of the risk of bias assessment.
Postoperative pulmonary complications
(1) All eight studies (23–30) involving 755 participants reported on postoperative pneumonia, the risk of which was significantly lower in the IMT group (RR 0.39, 95% CI 0.25–0.62, P < 0.0001; Figure 3A). Although we noted no heterogeneity in the included studies, small-study effects may be present. We downgraded the outcome for risk of bias and publication bias, but upgraded it for large effect (RR < 0.5). As a result, we rated the quality of evidence as moderate quality.
(2) Six trials (23, 24, 26, 27, 29, 30) involving 244 participants reported on postoperative atelectasis, the risk of which was significantly lower in the IMT group (RR 0.43, 95% CI 0.27–0.67, P = 0.0002; Figure 3B). Although we noted no heterogeneity in the included studies, small-study effects may be present. We therefore downgraded the outcome for risk of bias and publication bias. As a result, we rated the quality of evidence as low quality.
(3) Six trials (23, 24, 26, 27, 29, 30) reported on postoperative pleural effusion, the risk of which was not significantly different between the IMT and control groups (RR 1.09, 95% CI 0.62–1.93, P = 0.76; Figure 3C). The three outcomes were meta-analyzed using a fixed-effect model because of low heterogeneity.
We noted a low heterogeneity between the trials, and small-study effects may be present. So we downgraded this outcome for inconsistency and publication bias. Eventually, we rated the quality of evidence as very low quality and the effect is uncertain.
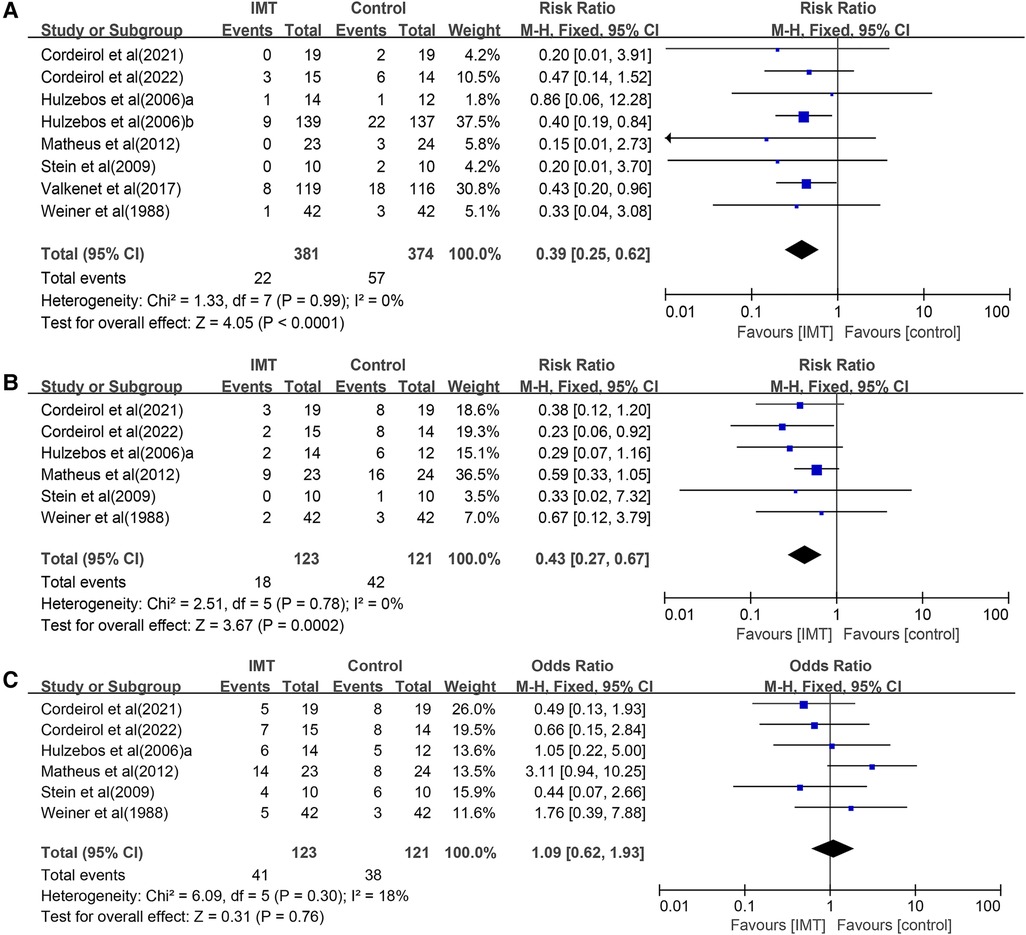
Figure 3. Forest plots of the association between IMT and risk of the postoperative pulmonary complications: (A) pneumonia, (B) atelectasis, and (C) pleural effusion.
Strength and endurance of respiratory muscles
Seven studies involving 738 participants evaluated the effect of IMT on MIP (23–25, 27–30), and it was significantly better in the IMT group. Similar results were obtained in separate meta-analyses of the four studies involving preoperative IMT (MD 16.55 cmH2O, 95% CI 13.86–19.24, P < 0.00001); or the remaining three studies involving postoperative IMT (MD 8.99 cmH2O, 95% CI: 2.39–15.60, P = 0.008) (Figure 4A).
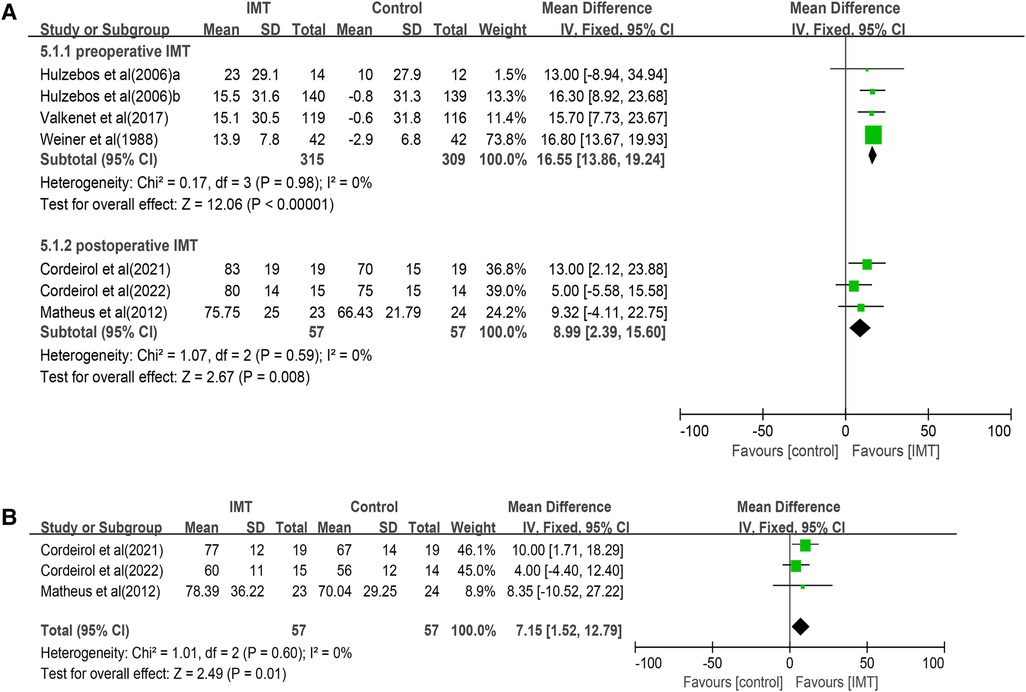
Figure 4. Forrest plot of the effect of IMT on respiratory muscle strength: (A) the change of MIP and (B) the change of MEP.
Meta-analysis of three studies (27, 29, 30) involving 144 patients associated postoperative IMT with significantly better MEP (MD 7.15 cmH2O, 95% CI 1.52–12.79, P = 0.01; Figure 4B). Both meta-analyses were performed with fixed-effect models because heterogeneity was negligible (I2 = 0%). Two trials (23, 25) reported the data about respiratory muscle endurance, which they assessed in terms of the ratio of Pmpeak to Pimax (Table 3), but data heterogeneity were too high to permit meta-analysis (I2 = 90%, P = 0.018).
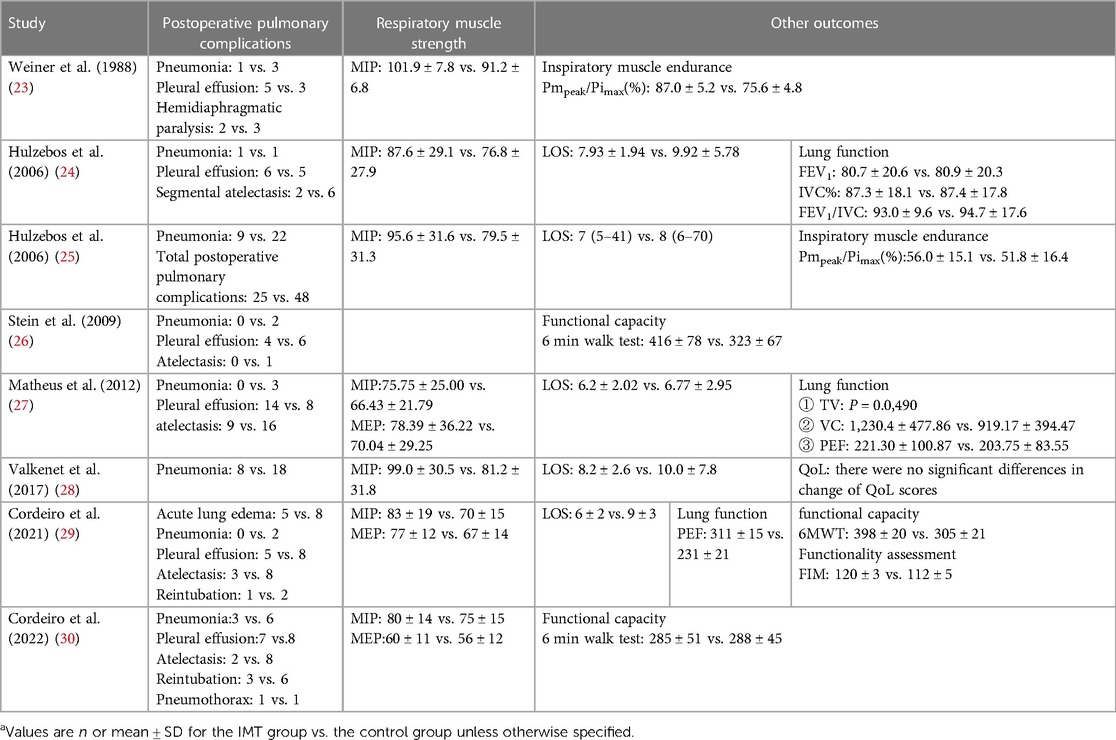
Table 3. Summary of outcomes in included studiesa.
Length of hospitalization
Five studies (24, 25, 27–29) compared length of hospitalization between the IMT and control groups, but one (25) of them reported respective median and ranges [7 (5–41) vs. 8 (6–70) days], which we could not pool with the means and standard deviations reported in the other four trials. Meta-analysis of those four trials associated IMT with significantly shorter hospitalization (−1.71 days, 95% CI −2.56 to −0.87 days, P < 0.0001; Figure 5).
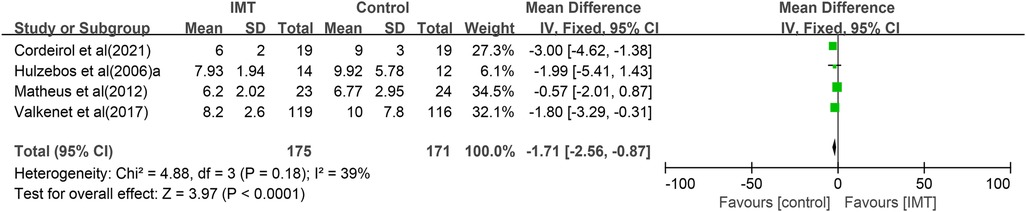
Figure 5. Forest plot of the association between IMT and length of hospitalization.
Exercise capacity
Three studies (26, 29, 30) examined the impact of IMT on performance in the 6 min walk test (6MWT). Due to the high heterogeneity (I2 = 92%, P < 0.00001), a random effects model was used for pooled analysis. The results showed that IMT was not associated with significantly longer distance traveled (MD 60.03 m, 95% CI −9.01 to 129.08, P = 0.09; Figure 6). Due to the small sample size, subgroup analysis and meta-regression cannot be conducted.
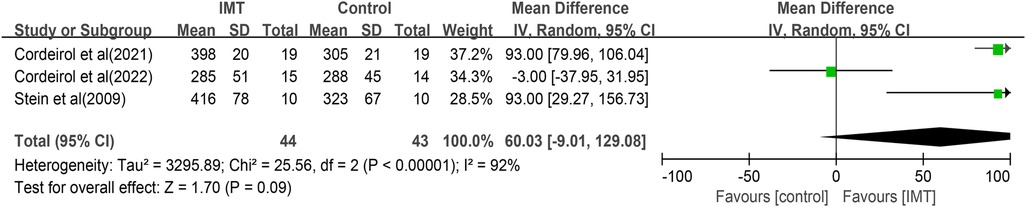
Figure 6. Forest plot of the association between IMT and distance traveled in the 6 min walk test.
Other outcomes
Subsets of the eight RCTs reported on additional secondary outcomes. One trial (28) with 235 participants found no significant difference in postoperative quality of life between IMT and control groups, as measured using the Form 36 questionnaire or the EuroQol questionnaire with five dimensions and three levels. One trial (28) reported no significant difference between IMT and control groups in how much percentage of inspiratory vital capacity (IVC%), forced vital capacity (FVC%), and forced expiration volume in 1 s (FEV1%) changed as a result of CABG (Table 3). Similarly, another study (27) reported improvement between IMT and control groups in tidal volume (P = 0.049) and vital capacity (P = 0.022). Meta-analysis of two studies (27, 29) involving 85 patients found that IMT did not significantly affect the peak expiratory flow (MD 54.36 L/min, 95% CI −5.85 to 114.58, P = 0.08; Figure 7).

Figure 7. Forest plot of the association between IMT and peak expiratory flow.
Discussion
This review of high-quality RCTs suggests that IMT can significantly decrease the risk of pulmonary complications like pneumonia and atelectasis after CABG, although not necessarily a risk of pleural effusion. In addition, IMT can significantly shorten hospitalization and strengthen respiratory muscles. Conclusions should be interpreted with caution in light of the apparent risk of overestimating the benefits of IMT, given the lack of adequate blinding, small samples, and publication bias in the available evidence.
Previous systematic reviews did show evidence that IMT can reduce PPCs in patients undergoing cardiac surgery. The meta-analysis by Ge et al. (19) showed that preoperative IMT resulted in significantly improved MIP and was associated with decreased PPCs, for patients undergoing cardiac, upper abdominal, and thoracic surgery. Gomes Neto et al. (13) showed that preoperative IMT reduced the risk of PPCs in patients undergoing cardiac surgery, which included three trials with 386 patients, and improved the MIP and reduced the length of hospital stay. A Cochrane meta-analysis (18) showed that preoperative IMT was associated with a reduction of postoperative atelectasis, pneumonia, and length of hospital stay in adults undergoing cardiac and major abdominal surgery, which included 12 trials with 695 participants. In addition, Thybo Karanfil and Møller (17) confirmed that preoperative IMT may reduce the risk of pneumonia and atelectasis after cardiac surgery, which included five trials with 348 patients. Thus, above-mentioned studies have focused on patients after cardiac surgery, and the definition of PPCs is inconsistent. Recently, the meta-analysis by Zhang et al. (21) revealed that IMT can improve the inspiratory muscle strength and endurance, pulmonary function, and 6MWT, and decrease PPCs and the LOS, which included 12 trials with 918 patients. However, only four studies that reported postoperative pneumonia were pooled analysis, and the cutoff time for inclusion was 2017, which is in accordance with our findings.
Limitations
The limitations of our systematic review and meta-analysis should also be noted. First, although the overall analysis suggests that IMT can reduce pneumonia and atelectasis, further studies are needed to examine IMT on different types of PPCs, including pleural effusion, mechanical ventilation more than 48 h, and pneumothorax. Additionally, preoperative and postoperative intervention period were included, and subgroup analysis was not performed, except MIP. Second, in the secondary outcome, the quality of life and pulmonary function (FVC, FEV1) data cannot be completely extracted. Thus, meta-analysis was not done. Third, this review did not cover cost–benefit and safety analyses. Fourth, due to the intervention equipment, sessions and intensity were inconsistent, and subgroup analysis was not performed. More well-designed large research studies are still needed.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Author contributions
YX contributed to the conception and design of the work, searched the literature, and drafted the manuscript, which YX, TL, and LZ revised. YX, TL, and QZ selected studies and extracted data. YX, TL, and LZ performed statistical analysis. All authors contributed to the article and approved the submitted version.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fcvm.2023.1223619/full#supplementary-material
References
1. Virani SS, Alonso A, Aparicio HJ, Benjamin EJ, Bittencourt MS, Callaway CW, et al. Heart disease and stroke statistics—2021 update: a report from the American Heart Association. Circulation. (2021) 143(8):e254–743. doi: 10.1161/CIR.0000000000000950
2. GBD 2016 Causes of Death Collaborators. Global, regional, and national age-sex specific mortality for 264 causes of death, 1980–2016: a systematic analysis for the global burden of disease study 2016. Lancet. (2017) 390(10100):1151–210. doi: 10.1016/S0140-6736(17)32152-9
3. Zhu KF, Wang YM, Zhu JZ, Zhou QY, Wang NF. National prevalence of coronary heart disease and its relationship with human development index: a systematic review. Eur J Prev Cardiol. (2016) 23(5):530–43. doi: 10.1177/2047487315587402
4. Hillis LD, Smith PK, Anderson JL, Bittl JA, Bridges CR, Byrne JG, et al. 2011 ACCF/AHA guideline for coronary artery bypass graft surgery: executive summary: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Thorac Cardiovasc Surg. (2012) 143(1):4–34. doi: 10.1016/j.jtcvs.2011.10.015
5. Mullen-Fortino M, O'Brien N, Jones M. Critical care of a patient after CABG surgery. Nurs Crit Care. (2009) 4(4):46–53. doi: 10.1097/01.CCN.0000357491.92428.71
6. Jammer I, Wickboldt N, Sander M, Smith A, Schultz MJ, Pelosi P, et al. Standards for definitions and use of outcome measures for clinical effectiveness research in perioperative medicine: European Perioperative Clinical Outcome (EPCO) definitions: a statement from the ESA-ESICM joint taskforce on perioperative outcome measures. Eur J Anaesthesiol. (2015) 32(2):88–105. doi: 10.1097/EJA.0000000000000118
7. Xiang Y, Zeng L, Luo T, Huang KQ. Risk factors for hypoxemia after coronary artery bypass grafting: a systematic review and meta-analysis. Chin J Clin Thoracic Cardiovasc Surg. (2020) 27(08):926–32. doi: 10.7507/1007-4848.202001074
8. Miskovic A, Lumb AB. Postoperative pulmonary complications. Br J Anaesth. (2017) 118(3):317–34. doi: 10.1093/bja/aex002
9. Rodrigues AJ, Mendes V, Ferreira PE, Xavier MA, Augusto VS, Bassetto S, et al. Preoperative respiratory muscle dysfunction is a predictor of prolonged invasive mechanical ventilation in cardiorespiratory complications after heart valve surgery. Eur J Cardiothorac Surg. (2011) 39(5):662–6. doi: 10.1016/j.ejcts.2010.08.021
10. D'Arx A, Freene N, Bowen S, Bissaker P, McKay G, Bissett B. What is the prevalence of inspiratory muscle weakness in preoperative cardiac surgery patients? An observational study. Heart Lung. (2020) 49(6):909–14. doi: 10.1016/j.hrtlng.2020.06.012
11. Odor PM, Bampoe S, Gilhooly D, Creagh-Brown B, Moonesinghe SR. Perioperative interventions for prevention of postoperative pulmonary complications: systematic review and meta-analysis. Br Med J. (2020) 368:m540. doi: 10.1136/bmj.m540
12. Dsouza FV, Amaravadi SK, Samuel SR, Raghavan H, Ravishankar N. Effectiveness of inspiratory muscle training on respiratory muscle strength in patients undergoing cardiac surgeries: a systematic review with meta-analysis. Ann Rehabil Med. (2021) 45(4):264–73. doi: 10.5535/arm.21027
13. Gomes Neto M, Martinez BP, Reis HF, Carvalho VO. Pre- and postoperative inspiratory muscle training in patients undergoing cardiac surgery: systematic review and meta-analysis. Clin Rehabil. (2017) 31(4):454–64. doi: 10.1177/0269215516648754
14. Luo Z, Qian H, Zhang X, Wang Y, Wang J, Yu P. Effectiveness and safety of inspiratory muscle training in patients with pulmonary hypertension: a systematic review and meta-analysis. Front Cardiovasc Med. (2022) 9:999422. doi: 10.3389/fcvm.2022.999422
15. Elkins M, Dentice R. Inspiratory muscle training facilitates weaning from mechanical ventilation among patients in the intensive care unit: a systematic review. J Physiother. (2015) 61(3):125–34. doi: 10.1016/j.jphys.2015.05.016
16. Menezes KK, Nascimento LR, Ada L, Polese JC, Avelino PR, Teixeira-Salmela LF. Respiratory muscle training increases respiratory muscle strength and reduces respiratory complications after stroke: a systematic review. J Physiother. (2016) 62(3):138–44. doi: 10.1016/j.jphys.2016.05.014
17. Thybo Karanfil EO, Møller AM. Preoperative inspiratory muscle training prevents pulmonary complications after cardiac surgery-a systematic review. Dan Med J. (2018) 65(3):A5450.29510803
18. Katsura M, Kuriyama A, Takeshima T, Fukuhara S, Furukawa TA. Preoperative inspiratory muscle training for postoperative pulmonary complications in adults undergoing cardiac and major abdominal surgery. Cochrane Database Syst Rev. (2015) 10:CD010356. doi: 10.1002/14651858.CD010356.pub2
19. Ge X, Wang W, Hou L, Yang K, Fa X. Inspiratory muscle training is associated with decreased postoperative pulmonary complications: evidence from randomized trials. J Thorac Cardiovasc Surg. (2018) 156(3):1290–300.e5. doi: 10.1016/j.jtcvs.2018.02.105
20. Cook A, Smith L, Anderson C, Ewing N, Gammack A, Pecover M, et al. The effect of preoperative threshold inspiratory muscle training in adults undergoing cardiac surgery on postoperative hospital stay: a systematic review. Physiother Theory Pract. (2023) 39(4):690–703. doi: 10.1080/09593985.2022.2025548
21. Zhang S, Li B, Meng X, Zuo H, Hu D. The effects of inspiratory muscle training (IMT) on patients undergoing coronary artery bypass graft (CABG) surgery: a systematic review and meta-analysis. Rev Cardiovasc Med. (2023) 24(1):16. doi: 10.31083/j.rcm2401016
22. Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. Br Med J. (2003) 327(7414):557–60. doi: 10.1136/bmj.327.7414.557
23. Weiner P, Zeidan F, Zamir D, Pelled B, Waizman J, Beckerman M, et al. Prophylactic inspiratory muscle training in patients undergoing coronary artery bypass graft. World J Surg. (1998) 22(5):427–31. doi: 10.1007/s002689900410
24. Hulzebos EH, van Meeteren NL, van den Buijs BJ, de Bie RA, Brutel de la Rivière A, Helders PJ. Feasibility of preoperative inspiratory muscle training in patients undergoing coronary artery bypass surgery with a high risk of postoperative pulmonary complications: a randomized controlled pilot study. Clin Rehabil. (2006) 20(11):949–59. doi: 10.1177/0269215506070691
25. Hulzebos EH, Helders PJ, Favié NJ, De Bie RA, Brutel de la Riviere A, Van Meeteren NL. Preoperative intensive inspiratory muscle training to prevent postoperative pulmonary complications in high-risk patients undergoing CABG surgery: a randomized clinical trial. JAMA. (2006) 296(15):1851–7. doi: 10.1001/jama.296.15.1851
26. Stein R, Maia CP, Silveira AD, Chiappa GR, Myers J, Ribeiro JP. Inspiratory muscle strength as a determinant of functional capacity early after coronary artery bypass graft surgery. Arch Phys Med Rehabil. (2009) 90(10):1685–91. doi: 10.1016/j.apmr.2009.05.010
27. Matheus GB, Dragosavac D, Trevisan P, Costa CE, Lopes MM, Ribeiro GC. Inspiratory muscle training improves tidal volume and vital capacity after CABG surgery. Rev Bras Cir Cardiovasc. (2012) 27(3):362–9. doi: 10.5935/1678-9741
28. Valkenet K, Trappenburg JCA, Hulzebos EH, van Meeteren NLU, Backx FJG. Effects of a pre-operative home-based inspiratory muscle training programme on perceived health-related quality of life in patients undergoing coronary artery bypass graft surgery. Physiotherapy. (2017) 103(3):276–82. doi: 10.1016/j.physio.2016.02.007
29. Cordeiro ALL, Soares LO, Vasconcelos MLL, Correia TR, Souza AS, Guimarães ARF, et al. Dois tipos de treinamento muscular inspiratório sobre a força muscular de pacientes após revascularização do miocárdio: ensaio clínico. Fisioterapia Brasil. (2021) 22(3):290–305. doi: 10.33233/fb.v22i3.4796
30. Cordeiro ALL, Carvalho BSC, Silva EGD, Santos NDS, de Melo TA, Guimarães ARF, et al. Inspiratory muscle training and functional capacity following coronary artery bypass grafting in high-risk patients: a pilot randomized and controlled trial. J Clin Transl Res. (2022) 8(4):266–71. doi: 10.18053/jctres.08.202204.001
Keywords: inspiratory muscle training, postoperative pulmonary complications, coronary artery bypass grafting, meta-analysis, randomized controlled trials
Citation: Xiang Y, Zhao Q, Luo T and Zeng L (2023) Inspiratory muscle training to reduce risk of pulmonary complications after coronary artery bypass grafting: a systematic review and meta-analysis. Front. Cardiovasc. Med. 10:1223619. doi: 10.3389/fcvm.2023.1223619
Received: 16 May 2023; Accepted: 27 June 2023;
Published: 24 July 2023.
Edited by:
Hiroki Teragawa, JR Hiroshima Hospital, JapanReviewed by:
Ada Gastaldi, University of São Paulo, BrazilRodrigo Antonini Ribeiro, HTAnalyze Consultoria e Treinamento, Brazil
© 2023 Xiang, Zhao, Luo and Zeng. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ling Zeng emVuZ2xpbmc1MTBAMTYzLmNvbQ==