
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Cardiovasc. Med. , 31 August 2023
Sec. Cardiovascular Pharmacology and Drug Discovery
Volume 10 - 2023 | https://doi.org/10.3389/fcvm.2023.1220017
This article is part of the Research Topic Therapeutic Strategies to Lower Residual Dyslipidemic CV Risk Beyond LDL-C and Statins View all 7 articles
 Peter P. Toth1,2*
Peter P. Toth1,2* Jean Ferrières3
Jean Ferrières3 Max Waters4Martin Bødtker Mortensen5
Max Waters4Martin Bødtker Mortensen5 Nick S. R. Lan6,7
Nick S. R. Lan6,7 Nathan D. Wong8
Nathan D. Wong8
Icosapent ethyl (IPE) is a purified eicosapentaenoic acid–only omega-3 fatty acid that significantly reduced cardiovascular (CV) events in patients receiving statins with established cardiovascular disease (CVD) and those with diabetes and additional risk factors in the pivotal REDUCE-IT trial. Since the publication of REDUCE-IT, there has been global interest in determining IPE eligibility in different patient populations, the proportion of patients who may benefit from IPE, and cost effectiveness of IPE in primary and secondary prevention settings. The aim of this review is to summarize information from eligibility and cost effectiveness studies of IPE to date. A total of sixteen studies were reviewed, involving 2,068,111 patients in the primary or secondary prevention settings worldwide. Up to forty-five percent of patients were eligible for IPE, depending on the selection criteria used (ie, REDUCE-IT criteria, US Food and Drug Administration label, Health Canada label, practice guidelines) and the population studied. Overall, eight cost-effectiveness studies across the United States, Canada, Germany, Israel, and Australia were included in this review and findings indicated that IPE is particularly cost effective in patients with established CVD.
Cardiovascular disease (CVD) is the most common cause of morbidity and mortality worldwide (1). Low-density lipoprotein cholesterol (LDL-C) continues to be the main treatment target for managing CVD risk (2), and statin therapy remains the cornerstone of preventive treatment for CVD. However, despite the effectiveness of statins, many patients receiving statin therapy continue to have a high residual cardiovascular (CV) risk (3). Consequently, research efforts are increasingly focused on discovering other therapeutic targets to help lower this persistent risk (4).
Mounting evidence from Mendelian and observational studies indicate that elevated triglyceride (TG) levels signal a substantial persistent residual risk for CVD (5). Nevertheless, until recently, no large, multinational, randomized trial in patients with elevated TG levels, including trials of niacin, fibrates, and mixed-omega-3 fatty acids comprising a combination of eicosapentaenoic acid (EPA) and docosahexaenoic acid, consistently showed improvement in CV outcomes in combination with statin therapy (6–9). This changed with the release of the pivotal REDUCE-IT study, a placebo-controlled, randomized, CV outcomes trial of the highly purified omega-3 stable ethyl ester of EPA, icosapent ethyl (IPE) in primary and secondary prevention settings (10, 11).
The REDUCE-IT trial included patients receiving statin therapy with fasting TG levels of 150 (with allowance for TG levels at or below 135 mg/dl due to intraindividual variability) to 499 mg/dl and LDL-C levels of 41 to 100 mg/dl who were aged forty-five years or older with established CVD or aged fifty years or older with diabetes mellitus and at least one additional risk factor (10). Select exclusion criteria were heart failure or renal impairment that was severe, severe active liver disease, glycated hemoglobin level higher than 10%, planned coronary surgery or intervention, history of chronic/acute pancreatitis, known hypersensitivity to shellfish or fish, or hypersensitivity to ingredients of icosapent ethyl or the placebo. The primary efficacy endpoint included a composite of CV death, nonfatal stroke, nonfatal myocardial infarction (MI), unstable angina, or coronary revascularization; the secondary endpoint was a composite of CV death, nonfatal stroke, or nonfatal MI (10).
After a median follow-up of 4.9 years, the primary efficacy endpoint occurred in 17.2% of patients in the IPE group vs. 22.0% of patients in the mineral oil placebo group (HR 0.75; P < 0.001), representing a twenty-five percent reduction in CV events with IPE. The key secondary endpoint occurred in 11.2% of patients receiving IPE vs. 14.8% receiving placebo (HR 0.74; P < 0.001) (10). With regard to safety, overall rates of adverse events were similar between IPE and placebo, albeit the rate of serious adverse bleeding events was nonsignificantly higher with IPE vs. placebo (2.7% vs. 2.1%, respectively; P = 0.06), and the rate of atrial fibrillation was significantly higher with IPE than with placebo (5.3% vs. 3.9%, respectively; P = 0.003). The US Food and Drug Administration (FDA) deemed that the benefits of IPE outweighed the potential risks. In secondary analysis, reductions in the primary and key secondary endpoints of REDUCE-IT were consistent across different statin background groups (12), suggesting that the type of statin used does not relevantly affect the efficacy of IPE.
Although IPE was first approved by the US FDA for lowering TG levels in patients with severe hypertriglyceridemia (11), the significant reduction in CV events reported in REDUCE-IT is unlikely to be attributed solely to lipid lowering because only a modest reduction in TG levels was observed (10). As such, other mechanisms of action of IPE are purported to be responsible for the significant reduction in CV events (10), including its effects on endothelial function, oxidative stress, foam-cell formation, inflammation/cytokines, plaque formation/progression, platelet aggregation, thrombus formation, and plaque rupture (13).
Since publication of the REDUCE-IT results, there has been much debate as to whether positive outcomes in REDUCE-IT can be attributed to the potential negative effects of mineral oil on lipid and inflammatory parameters in the placebo group (14, 15), namely increases in LDL-C (10.2%) and high-sensitivity C-reactive protein (29.9%; both P < 0.001). This controversy was particularly driven by a report that used data from the Copenhagen General Population Study to mimic lipid and high-sensitivity C-reactive protein trends of REDUCE-IT that found increased TG, LDL-C, and high-sensitivity C-reactive protein levels may be associated with increased risk of CVD in patients treated with mineral oil placebo (16). The assertion that changes in lipid levels and C-reactive protein were important contributors to the findings of REDUCE-IT has been independently investigated by multiple global regulatory authorities, including those in the United States and the European Union, both of which concluded that it is unlikely that mineral oil impacted CV outcomes in REDUCE-IT (17, 18), further adding that, even if it did have any effect, the effect was negligible, with EPA still providing at least a twenty-two percent incremental benefit over statin therapy alone (17). In addition, the JELIS trial, which assessed the efficacy of purified EPA 1.8 mg daily among 18,645 Japanese patients with hypercholesterolemia, did not use a mineral oil placebo, and yet reported similar reduction (nineteen percent) in CV events (19). Furthermore, mineral oil is a common agent used as a placebo in clinical trials due in part to its inert properties (20), and recent animal and in vitro data did not show significant changes in statin absorption when administered with mineral oil, nor any biologic properties of mineral oil (21, 22).
The positive CV outcomes in REDUCE-IT are further supported by findings in other trials that used EPA-only formulations (23), including JELIS (19), CHERRY (24), EVAPORATE (25), a Japanese study that reported reductions in CVD events after early initiation of EPA after percutaneous coronary intervention (PCI) in patients with acute coronary syndrome (26), and RESPECT-EPA (27–29).
Results from RESPECT-EPA were presented at the American Heart Association meeting in 2022 and the magnitude of the effect of EPA on its CV endpoints was consistent with the results of REDUCE-IT (27). The open-label trial included 2,460 Japanese patients treated with statins who were aged twenty to seventy-nine years with chronic coronary artery disease (CAD) and a low EPA-to-arachidonic acid ratio (<0.4); they were randomized in a one-to-one ratio to receive purified EPA 1.8 g/day plus statin therapy (n = 1,225) or statin monotherapy (n = 1,235). Purified EPA was associated with a borderline significant reduction of 21.5% in CV risk in the primary endpoint (P = 0.054) and a significant reduction of 26.6% in the secondary composite endpoint (P = 0.03) vs. statin monotherapy. Levels of EPA significantly increased from 48.5 at baseline to 140.5 µg/dl at the three-year follow-up in the EPA group vs. 46.6 to 51.5 µg/dl, respectively, in the statin monotherapy group (P < 0.05). Gastrointestinal disorders and new-onset atrial fibrillation occurred significantly (P < 0.001 and P = 0.017, respectively) more frequently in the EPA group than the statin monotherapy group (27). It is important to note here that CV clinical trials in Japan are open-label because blinding therapy is considered unethical (30).
In the United States, the results from REDUCE-IT led the US FDA to grant IPE a second indication as an adjunct to maximally tolerated statin therapy to reduce the risk of MI, stroke, coronary revascularization, and unstable angina requiring hospitalization in adults with elevated TG levels (≥150 mg/dl) and either established CVD or diabetes mellitus with at least two additional risk factors for CVD (11). Soon after this approval, regulatory authorities in the European Union, United Kingdom, Canada, Hong Kong, Australia, and certain regions in the Middle East also approved IPE for CVD risk reduction (31, 32). In light of the data from REDUCE-IT, international medical societies and professional associations published scientific statements and updated guidelines, recommending use of IPE for CVD risk reduction (31, 33–38). These recommendations highlighted a need for IPE to be available worldwide.
Since the approval of IPE for residual CVD risk reduction, global interest has been growing to investigate the proportion of patients who may be eligible for and benefit from treatment with IPE in a real-world setting as well as its cost effectiveness in primary and secondary prevention settings (39–42). The aim of this review is to provide a comprehensive, worldwide overview of published, real-world eligibility analyses. A secondary aim is to provide an overview of published global cost-effectiveness data.
After the publication of REDUCE-IT in January 2019, PubMed and Google Scholar were continuously monitored for publications relating to eligibility for or cost effectiveness of IPE.
One of the larger studies on IPE eligibility was conducted using the REACH registry, which involved more than 65,000 patients closely resembling the patient population in REDUCE-IT (10); patients were aged forty-five years or older with stable atherothrombosis (ie, CAD, peripheral arterial disease, cerebrovascular disease) or with at least three risk factors for atherothrombosis and from forty-four countries across Asia, Australia, Europe, North and Central Americas, and the Middle East (Table 1) (41–60). Select REDUCE-IT inclusion criteria were applied to all patients with diabetes or atherosclerotic cardiovascular disease (ASCVD) and available baseline TG and total cholesterol levels. Overall, 11.3% (n = 7,085) patients were eligible for IPE, of whom 12.3% (n = 1,036) were eligible for IPE for primary prevention (41). The most common reasons for not meeting REDUCE-IT criteria included LDL-C levels above 100 mg/dl (60.8%), TG levels below 135 mg/dl (58.2%), and not receiving statin treatment (34.5%). After applying secondary prevention REDUCE-IT inclusion criteria to 54,046 with established ASCVD, 11.2% (n = 6,049) of patients were eligible for IPE (41). As in the primary prevention group, most patients who did not meet REDUCE-IT criteria had LDL-C levels above 100 mg/dl (53.5%), TG levels below 135 mg/dl (70.2%), and were not receiving statin treatment (35.3%). Patients eligible for IPE were at increased risk for cardiac atherothrombotic events vs. noneligible patients, including PCI and coronary artery bypass graft (CABG) surgery, demonstrating that persistent risk exists despite statin therapy (41).
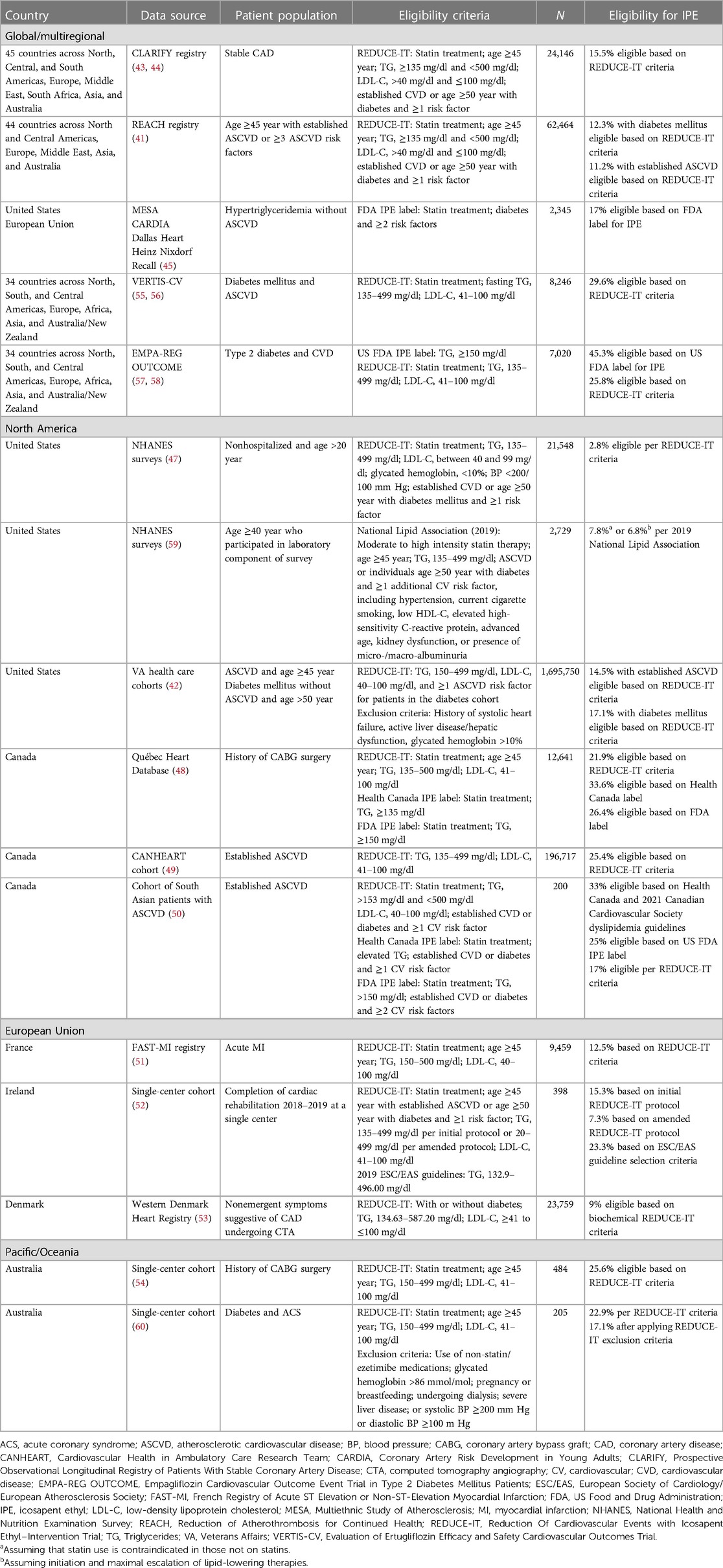
Table 1. Eligibility for IPE risk reduction from cohorts by region.
The CLARIFY registry included 32,703 patients with stable CAD (eg, documented MI/CABG surgery/PCI >3 months ago) in forty-five countries across Africa, Asia, Australia, Europe, the Middle East, and North, Central, and South Americas (43, 44). After applying REDUCE-IT inclusion criteria to 24,146 patients with complete baseline data, 15.5% (3,738) of patients were eligible to receive IPE. Similar to those in the REACH registry (41), most patients who did not meet REDUCE-IT eligibility criteria had TG levels below 135 mg/dl (57.1%) and LDL-C levels above 100 mg/dl (34.4%); other ineligible patients had LDL-C levels at or below 40 mg/dl (12.6%), were younger than forty-five years of age (3.8%), or had TG levels at or above 500 mg/dl (0.6%). Extrapolating these results to the global (111 million) and US populations (17 million) with CAD, an estimated 17.14 million and 2.56 million patients with CAD, respectively, may be eligible for and benefit from treatment with IPE (43). It is important to note that the CLARIFY registry did not include US patients, many of whom are more likely to be eligible for IPE given the greater prevalence of high TG levels and use of intensive statin treatment. In addition, the REDUCE-IT trial included a broader patient population vs. the CLARIFY registry, which included only patients with CAD (41).
Kim et al. (56) used the global VERTIS-CV trial of 8,246 patients with diabetes mellitus and ASCVD to assess eligibility for IPE across four subgroups of patients stratified by baseline TG and LDL-C levels (TG < 135 mg/dl and LDL-C < 70 mg/dl; TG < 135 mg/dl and LDL-C ≥ 70 mg/dl; TG ≥135 mg/dl and LDL-C < 70 mg/dl; and TG ≥135 mg/dl and LDL-C ≥ 70 mg/dl). Mean patient age was sixty-four years, with median TG and LDL-C levels of 153 and 82 mg/dl, respectively. After applying the REDUCE-IT criteria, 29.6% (n = 2,444) of patients were eligible to receive IPE. Overall, 18.2% of patients were not receiving statins, and 65.3% had LDL-C levels of 70 mg/dl or higher, highlighting the gap in statin use and lipid management. In addition, 30.3% (n = 2,500) did not fully meet REDUCE-IT eligibility criteria, but they had TG levels above 135 mg/dl, and 3,302 (40.0%) did not meet REDUCE-IT eligibility criteria but had TG levels at or below 135 mg/dl. Adding IPE could have been considered in sixty percent of patients based on the REDUCE-IT trial inclusion criteria or on TG levels alone (56).
Using IPE eligibility per the US FDA label, Cainzos-Achirica (45) evaluated whether the coronary artery calcium (CAC) score could enhance risk stratification among individuals with hypertriglyceridemia in the primary prevention setting. The study pooled data from 2,345 patients from four studies, including MESA, CARDIA, the Dallas Heart, and the Heinz Nixdorf Recall studies, and evaluated the incidence of ASCVD events in patients meeting IPE eligibility criteria per the US package insert and stratified by CAC scores (0, >1–100, >100). The outcome of this study was designed to simulate that of the composite ASCVD endpoint in REDUCE-IT, which included CV death, nonfatal MI, unstable angina, coronary revascularization, or nonfatal stroke. Overall, seventeen percent (n = 643) of patients were eligible for IPE per the US FDA IPE label. After stratifying patients eligible for IPE by CAC category, twenty-five percent had a CAC score of zero with a five-year incidence of ASCVD of 7.2%; thirty-seven percent had a CAC score of one to 100 with a five-year incidence of ASCVD of 10.9%; and thirty-eight percent had a CAC score higher than 100 with a five-year incidence of ASCVD of 15.9%. The number of patients ineligible for IPE with a CAC score higher than one hundred (17%) was similar to that of participants eligible for IPE therapy irrespective of CAC score (17%), suggesting that trial enrollment and pharmacotherapy allocation approaches using the presence of diabetes, various additional risk factors, or both may miss a large portion of individuals with hypertriglyceridemia at high risk for ASCVD events who may benefit from IPE. Importantly, the study showed that long-term residual CV risk is substantial despite high-intensity statin treatment, suggesting that other therapies are needed to reduce this risk (45).
Verma et al. (57) used data from the global EMPA-REG OUTCOME trial of empagliflozin in 7,020 patients with type 2 diabetes and established CVD. Eligibility for IPE was assessed using REDUCE-IT eligibility criteria and US package insert criteria. In addition, they investigated whether CV outcomes and efficacy of empagliflozin differed based on eligibility for IPE treatment. Overall, 1,810 (26%) patients (placebo, n = 608; empagliflozin, n = 1,202) fulfilled the REDUCE-IT criteria, and 3,182 (45%) patients (placebo, n = 1,043; empagliflozin, n = 2,139) fulfilled US FDA label requirements. Compared with those not fulfilling the criteria, these patients had generally comparable risk of CV outcomes, and the treatment effect of empagliflozin was comparable across all cohorts (57).
Using data from the National Health and Nutrition Examination Survey (NHANES) from 2017 to 2020, Shen et al. (59) investigated eligibility and use of lipid-lowering therapies, including statins, IPE, and proprotein convertase subtilisin/kexin type 9 inhibitors, among US adults. Eligibility criteria for IPE were based on the scientific statement from the National Lipid Association (33), which included patients treated with moderate- to high-intensity statins aged forty-five years or older with clinical ASCVD or aged fifty years or older with diabetes and at least one additional CV risk factor (eg, hypertension, current cigarette smoking, low high-density lipoprotein cholesterol, advanced age, residual TG 135–499 mg/dl even after statin treatment) (59). Of 2,729 sampled individuals (or 149.3 million US adults), forty-four percent (n = 1,376) had had an indication for statins (or 65.8 million US adults), but only forty-five percent of these had taken statins. Given that use of guideline-recommended lipid-lowering therapies such as statins is suboptimal, eligibility for IPE was assessed in two scenarios: (1) assuming existing lipid-lowering therapy as the maximum tolerated dose before evaluating eligibility and (2) assuming initiation and maximal escalation of preexisting lipid-lowering therapies and accounting for expected lipid improvements. Based on lipid profiles and existing therapies, 7.8% (11.6 million US adults) would benefit from IPE, including 29.2% (6.1 million US adults) of patients with ASCVD and 35.6% (8.9 million US adults) of patients with diabetes. Assuming maximal escalation of statins and addition of ezetimibe, 6.8% (10.2 million) of patients would benefit from IPE, including 26.0% (5.4 million) with ASCVD and 31.4% (7.8 million) with diabetes. Eligibility for IPE in this study was relatively higher than reported in other studies partly because the 2019 statement from the National Lipid Association did not include LDL-C criteria. Overall, the study underscored that use of lipid-lowering therapies is suboptimal (59).
Using the NHANES dataset from 1999 to 2016 involving 53,348 US adults, Wong et al. (47) applied IPE eligibility criteria per REDUCE-IT or the US package insert for IPE to estimate the proportion of US adults who may benefit from IPE and the number of potentially preventable ASCVD events with IPE therapy. The number of anticipated ASCVD events, including the REDUCE-IT primary composite endpoint, secondary composite endpoint, and individual secondary endpoints (CV-related death, revascularization, nonfatal MI, stroke, and total mortality), was estimated using the overall REDUCE-IT initial and total published event rates as well as event rates for initial events alone in the IPE and placebo groups. REDUCE-IT criteria were applied to 21,548 NHANES participants randomly assigned to morning sessions who fasted for at least 8.5 h. Overall, 319 participants (or projected 3,041,891 US adults) would be eligible to receive IPE, including 114 participants (n = 1,133,110) for primary prevention and 205 participants (n = 1,908,781) for secondary prevention. Ineligibility for IPE was most commonly due to age younger than forty-five years (n = 10,103) and TG levels below 135 mg/dl or 500 mg/dl or higher (n = 7,148). Treatment with IPE for more than 4.9 years could potentially prevent 71,391 primary and 31,660 secondary composite outcomes each year, with 29,798 and 22,349 accounting for first time events, respectively. The majority of estimated preventable events occurred in patients eligible for IPE in the secondary prevention setting vs. the primary prevention cohort (47).
After applying the US FDA IPE label inclusion criteria, 476 participants (or 4,564,056 US adults) were eligible to receive IPE, with 161 (n = 1,614,561) and 315 (n = 2,949,495) eligible in primary prevention and secondary prevention settings, respectively (47). The most common reasons for ineligibility included TG levels below 150 (n = 15,595), not receiving statins (n = 4,857), and not meeting criteria for primary prevention (n = 620). If these patients were given IPE for 4.9 years, then 60,544 and 41,915 primary and secondary composite endpoints, respectively, were estimated to be prevented each year (47).
Jia et al. (42) used primary (diabetes mellitus) and secondary prevention (prior MI, ischemic stroke, or peripheral artery disease) cohorts receiving care in the US Veterans Affairs Healthcare System between October 2013 and September 2014 to estimate the number of patients who may benefit from IPE per the REDUCE-IT eligibility criteria. Patients with available TG data, aged forty-five years or older with ASCVD (n = 1,011,558), or aged fifty years or older with diabetes mellitus (n = 684,192) were screened per REDUCE-IT inclusion and exclusion criteria. A total of 263,114 patients were eligible for IPE in the primary and secondary prevention settings: 17.1% (n = 116,925) of patients for primary prevention and 14.5% (n = 146,189) of patients for secondary prevention (42).
Kosmopoulos et al. (48) used REDUCE-IT-derived, US FDA IPE package insert, and Health Canada IPE label selection criteria to determine IPE eligibility in the secondary prevention setting among 12,641 patients from the Québec Heart Database who underwent CABG surgery between 2006 and 2016. Overall, 21.9% (n = 2,769) of patients were eligible for IPE per the REDUCE-IT criteria. Reasons for ineligibility included TG levels below 135 or higher than 500 mg/dl (n = 7,217), LDL-C levels below 41 or higher than 100 mg/dl (n = 1,396), not treated with statins (n = 1,230), and age younger than forty-five years (n = 29). After applying Health Canada label selection criteria, which included patients receiving statins with TG levels 135 mg/dl or higher, 33.6% (n = 4,253) were eligible for IPE. Reasons for ineligibility included TG levels below 135 mg/dl (n = 7,158) and not receiving statins (n = 1,230). Per the US label selection criteria, 26.4% (n = 3,337) of patients were eligible for IPE; reasons for ineligibility included TG levels less than 150 mg/dl (n = 8,074) and not receiving statins (n = 1,230). Regardless of whether the REDUCE-IT–derived, Health Canada label, or US label selection criteria were applied, this study showed that a considerable proportion of patients would be eligible for and benefit from use of IPE as an adjunct to secondary prevention therapies after CABG surgery (48).
Lawler et al. (49) used the CANHEART cohort of 9,403,853 patients across Ontario, Canada, to determine the real-world risk of ASCVD events in a secondary prevention setting involving patients with ASCVD and hypertriglyceridemia as well as to estimate the proportion of patients who may qualify for IPE therapy. Only patients with lipid panels, aged forty years or older, and a history of ASCVD but without major life-limiting conditions and those not living in a skilled nursing facility were screened for IPE eligibility per the REDUCE-IT criteria. Of 196,717 patients with established ASCVD, 25.4% (n = 49,886) were eligible for IPE. Over a median of three years, 24,097 composite ASCVD events occurred with a primary outcome (ie, unstable angina, first occurrence of MI, stroke, transient ischemic attack, coronary revascularization, CVD-related death) at a rate of 38.6 per 1,000 person-years. The event rate for patients with TG levels above 354.3 mg/dl was 52% higher than for patients with TG levels below 88.6 mg/dl, indicating that this patient population may benefit from therapies such as IPE that reduce residual CV risk (49).
South Asians are particularly prone to CVD and CVD-related mortality (61–63), and, given that an overwhelming majority of patients in REDUCE-IT were White, Krishnaraj et al. (50) sought to determine the generalizability of the REDUCE-IT results in the secondary prevention setting—using the Health Canada IPE label, the Canadian Cardiovascular Society dyslipidemia guidelines, the US FDA IPE label, and REDUCE-IT criteria—to 200 South Asian patients treated with statins aged forty-five years or older with ASCVD from community cardiology and family practice clinics living in Canada. Overall, ninety-five percent of patients had CAD, eighty-six percent underwent coronary revascularization, forty percent had a history of MI, and seventy-five percent were taking high-dose statins. Per the Health Canada IPE label (64), IPE is indicated for patients with elevated TG levels, with increased CV risk due to established CVD, or diabetes and at least one other CV risk factor. Although the Health Canada label did not denote a TG threshold (64), Krishnaraj et al. (50) specified a TG threshold of 135 mg/dl or higher to represent hypertriglyceridemia. The Canadian Cardiovascular Society dyslipidemia guidelines recommend IPE for patients with TG levels 135 to 499 m/dl (37). Regardless of the slight differences in specified TG levels between the Health Canada IPE label and Canadian guidelines, patients eligible for IPE using either selection criteria was similar, with approximately thirty-three percent of patients eligible for IPE. After applying the US FDA IPE label TG threshold of 150 mg/dl or higher and the REDUCE-IT criteria for TG levels (135–499 mg/dl) and LDL-C levels (41–100 mg/dl), 24.5% and 17.0% of patients, respectively, would be eligible for IPE.
Using the FAST-MI 2010 and FAST-MI 2015 registries comprising 9,459 patients with acute MI across France (65), Ferrières et al. (51) applied the REDUCE-IT selection criteria to 3,789 patients with a complete lipid panel; exclusion criteria were also applied. Overall, 12.5% (n = 472) of patients were eligible for IPE. Despite several differences between patients in the FAST-MI registries and REDUCE-IT trial, such as the prevalence of established ASCVD, cigarette smoking, hypertension, and statin use, their residual risk was similar with an event rate of 36.7 per 1,000 patient-years in the FAST-MI registry vs. 36.9 per 1,000 patient-years in REDUCE-IT. Overall, the proportion of patients eligible for IPE in this study was lower vs. other studies, in part because the FAST-MI registries only included patients hospitalized with acute MI rather than all patients with established CVD (51).
Using data from 23,759 patients aged eighteen years or older who presented with nonemergent symptoms suggestive of CAD and who underwent computed tomography angiography between January 2008 and December 2017 in the Western Denmark Heart Registry, Mortensen et al. (53) estimated ASCVD event rates (ie, MI, stroke, revascularization, all-cause mortality >90 days after testing), including hard ASCVD events (ASCVD events, excluding revascularization), and a five-year number need to treat (NNT) to prevent one ASCVD event in patients meeting IPE eligibility criteria, including patients with or without diabetes, TG levels 134.63 to 587.20 mg/dl, and LDL-C levels of at least 41 but no higher than 100 mg/dl. The ASCVD event rates were stratified by calcified plaque burden (CAC scores of 0, 1–299, and ≥300) and CAD severity defined by computed tomography angiography (no CAD, nonobstructive CAD, and obstructive CAD); patients with prior MI or revascularization were excluded. Overall, nine percent (n = 2,146) of patients were eligible for IPE: 523 patients with obstructive CAD, 738 patients with nonobstructive CAD, and 885 with no CAD. A considerable difference was observed in the estimated five-year NNT to prevent one event across increasing CAC scores among REDUCE-IT–eligible patients, ranging from eighty-seven in patients with a CAC score of zero to seventeen in patients with a CAC score above 300. In addition, the NNT for hard ASCVD events was lower in patients with extensive nonobstructive CAD vs. patients with obstructive CAD and lower plaque burden. Overall, the study found that REDUCE-IT-eligible patients with high plaque burden but nonobstructive CAD may benefit more from IPE than patients with obstructive CAD and less plaque burden (53).
Using a single-center cardiac rehabilitation cohort population in Ireland, Gaine et al. (52) applied REDUCE-IT selection criteria (initial and amended) and the 2019 European Society of Cardiology/European Atherosclerosis Society guideline selection criteria to 275 patients with available LDL-C and TG data. The initial REDUCE-IT criteria for TG levels were 150 mg/dl or higher (with allowance for ≥135 mg/dl due to intraindividual variability), a value that was later amended to 200 mg/dl or higher (10). After applying the REDUCE-IT criteria, 15.3% (n = 42) and 7.3% (n = 20) of patients were eligible for IPE per the initial and amended REDUCE-IT criteria, respectively (52). According to the 2019 European Society of Cardiology/European Atherosclerosis Society guideline selection criteria for IPE (TG 132.86–496.00 mg/dl, no LDL-C or age limits), 23.3% (n = 64) of patients were eligible for IPE (52).
Using data from 1,676 patients who underwent CABG surgery in a western Australian tertiary hospital from February 2015 until August 2020, Lan et al. (54) applied REDUCE-IT inclusion criteria to 484 patients with available follow-up lipid profiles. Patients not eligible for IPE were those not prescribed statin therapy or taking a fibrate. Only some REDUCE-IT exclusion criteria were applied due to limitations in data availability and retrospective analysis. In total, 25.6% (n = 124) of patients were eligible for IPE. Results from this study demonstrate that a substantial proportion of patients may benefit from therapy with IPE following CABG surgery (54).
Lan et al. (60) applied secondary prevention REDUCE-IT eligibility criteria in 205 patients with diabetes and acute coronary syndrome in a western Australian tertiary hospital. Several exclusion criteria were also applied, some of which included use of nonstatin or nonezetimibe medications, undergoing dialysis, severe liver disease or poorly controlled hypertension. Overall, 22.9% (n = 47) and 17.1% (n = 35) of patients were eligible for IPE based on REDUCE-IT inclusion only and after applying exclusion criteria, respectively. Importantly, the study found that nearly two-thirds of patients with diabetes who would be eligible for IPE had a prior history of ASCD, suggesting that targeting LDL-C alone for prevention is not sufficient (60).
Cost-effective, add-on therapies to statins are needed for primary and secondary CVD prevention to help reduce the incidence of CV events and the costs associated with these events. REDUCE-IT was the first and only trial to demonstrate a cardiovascular mortality benefit over and above a statin. However, providing IPE therapy to all eligible patients necessitates a substantial investment (66).
Although generic formulations of IPE are available and it is well established that generic drugs cost less than branded drugs, these formulations are not approved for the same indications as their branded counterparts. In the United States, generic IPE is approved for only one indication, ie, as an adjunct to diet to reduce TG levels in adults with severe (≥500 mg/dl) hypertriglyceridemia. Only branded IPE is approved for reducing TG levels and reducing CV events in primary and secondary prevention settings (11).
At the net annual price of $1,625 for IPE, approximately four percent of eligible patients could be treated in a year before exceeding the Institute for Clinical and Economic Review (ICER) budget impact threshold of $819 million (67). As, such, concerns regarding potential lack of access to IPE prompted the ICER to issue an access and affordability alert for IPE, signaling to stakeholders and policymakers “that the amount of added health care costs associated with a new service may be difficult for the health care system to absorb over the short term without displacing other needed services or contributing to rapid growth in health care insurance costs” that threaten sustainable access to high-value care for all patients (67). Thus, it is important to understand the value of IPE treatment in different populations so that health benefit from treatment can be maximized.
Since the approval of IPE by various regulatory agencies, interest has been growing to understand the value of IPE as a treatment option, and multiple studies worldwide have investigated the cost effectiveness of IPE vs. standard of care in primary and secondary prevention settings (Table 2; Figure 1) (39, 40, 66, 68–72).
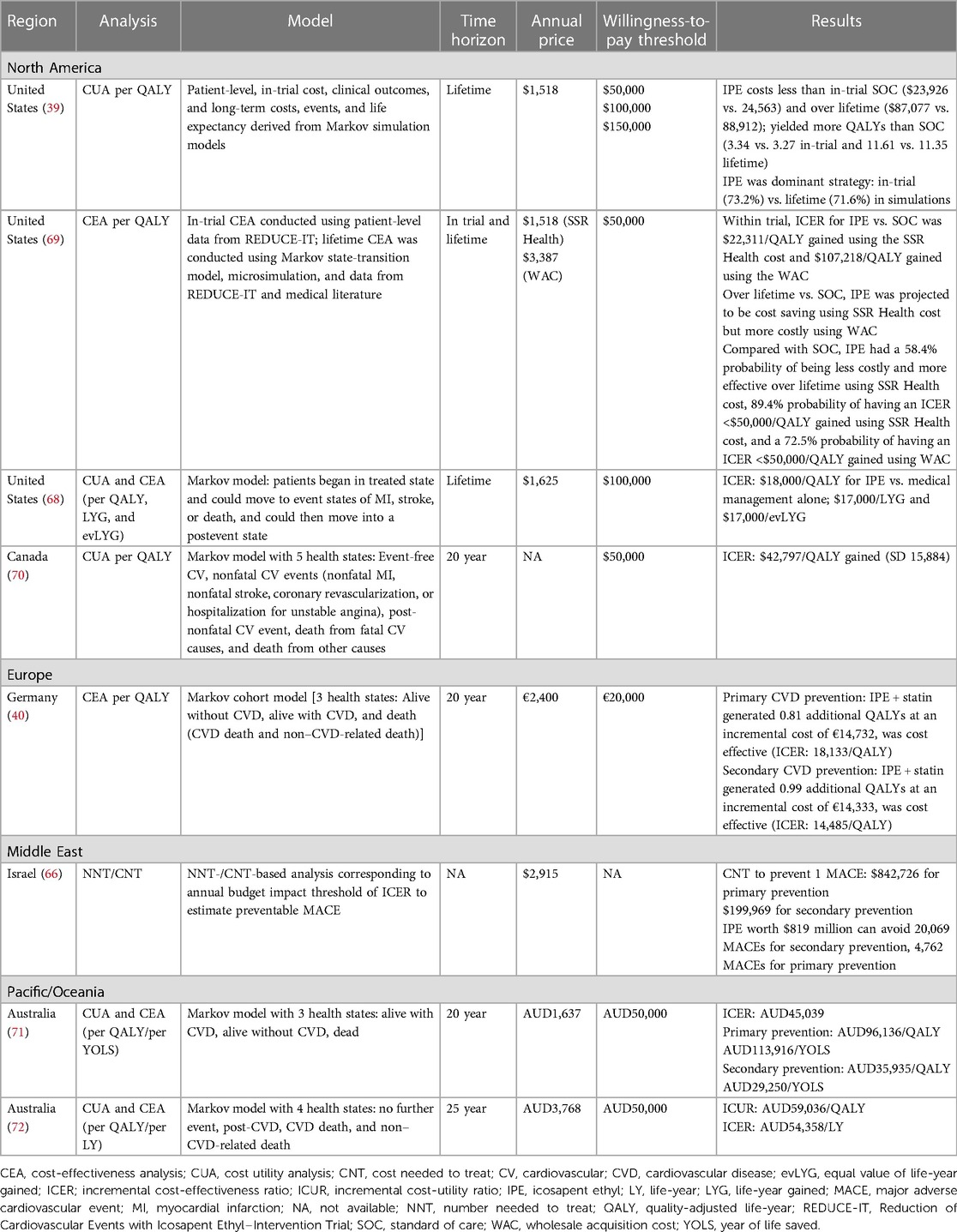
Table 2. Cost-effectiveness studies of IPE risk reduction by region.
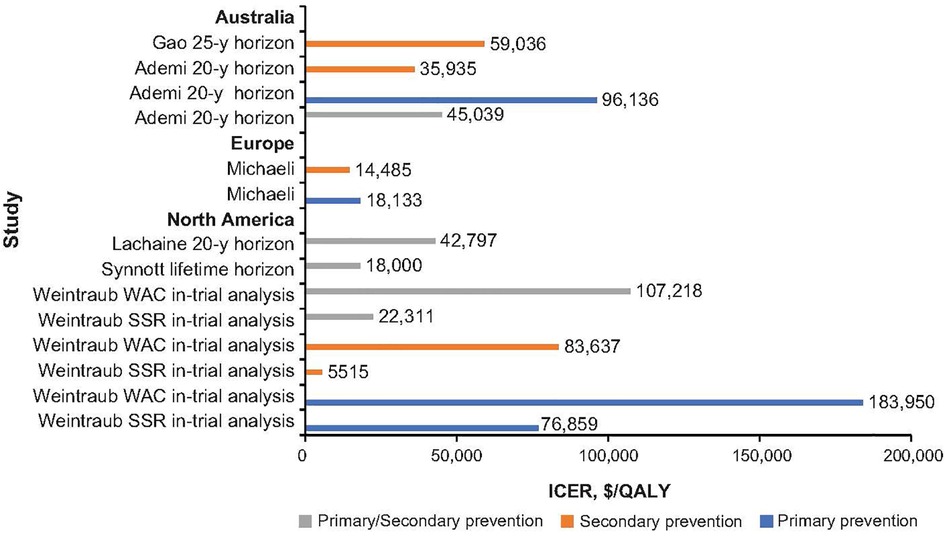
Figure 1. Incremental cost-effective ratio with icosapent ethyl across world regions. ICER, incremental cost-effectiveness ratio; QALY, quality-adjusted life-year; WAC, wholesale acquisition cost (40, 68–72).
From US and Canadian health care perspectives, IPE is a cost-effective therapeutic option, falling at or below the willingness-to-pay threshold of $50,000 or 100,000, depending on the study (39, 68–70). Several studies indicate that IPE is cost effective for both primary and secondary prevention settings, but IPE consistently offers more value for secondary prevention (68, 70, 73). A US study by Weintraub et al. showed that probability of cost effectiveness of IPE over a lifetime, below a willingness-to-pay threshold of $50,000, was 89% and 72% depending on different cost used for IPE in the model (69).
Cost effectiveness of IPE from a German health care perspective was consistent with those of the United States and Canada (68–70); namely, Michaeli et al. (40) demonstrated that IPE was cost effective in primary and secondary prevention settings, but it offered more value in secondary prevention, with ICER of €18,133/QALY in patients without CVD vs. €14,485/QALY in patients with existing CVD over a 20-year time horizon. Importantly the number needed to treat was below six for nonfatal MI, nonfatal stroke, hospitalization for unstable angina, coronary revascularization, and CVD death in both primary and secondary prevention settings. In addition, the study showed that early lipid management with IPE starting at fifty-five years over twenty-five years could reduce ICER for primary prevention by nearly fifty percent to €9,381/QALY (40).
The Israeli health care perspective echoed that of the United States, Canada, and Germany, showing that prioritizing IPE therapy for patients with established CVD over primary prevention avoids fourfold higher rates of major adverse CV events for resources spent (66).
The cost effectiveness of IPE from an Australian health care perspective was dependent on the drug cost utilized and model inputs. Gao et al. (72) found that IPE for secondary prevention was not cost effective at a willingness-to-pay threshold of AUD50,000. However, Ademi et al. (71) found that it was cost effective for secondary prevention alone and prevented 270.8 MIs, strokes, or both; 295.8 coronary revascularizations; and 57.8 deaths overall vs. a statin alone. Differences in these study results were attributed to variation in annual cost of IPE (AUD3,768 vs. 1,637) and discount rate (3% vs. 5%) (71). Discrete patient-level data from REDUCE-IT were not used for either study, as was done in the primary cost-effectiveness analysis from REDUCE-IT (69).
Studies of IPE eligibility across geographies demonstrate that a considerable portion of patients with residual persistent CV risk could benefit from treatment with IPE in primary and secondary prevention settings, ranging from 2.8% to 45.3% (47, 48). Variation in IPE eligibility largely depended on whether studies used highly selected patient populations (eg, history of CABG) vs. broader populations (eg, general adult population); which and how many of the REDUCE-IT, regulatory label, or guideline criteria were used; and whether studies assessed IPE eligibility in primary, secondary, or both prevention settings. Importantly, some of the most common reasons for IPE ineligibility were that patients did not meet TG and LDL-C criteria (41, 47, 48), suggesting that existing lipid-lowering therapies such as statins remain underused (59).
Studies assessing cost effectiveness worldwide found that IPE was generally most cost effective for secondary prevention. Several studies found that IPE is cost effective in both settings. Variations in the cost effectiveness of IPE across studies are largely attributed to differences in regional drug pricing and modeling assumptions. A majority of studies used a willingness-to-pay threshold of $50,000, whereas several used $100,000. Identifying which populations may benefit more from IPE and in whom IPE would be a more cost-effective treatment are important considerations given health care budget constraints (39, 40, 68–72).
Bolstered by the regulatory approval of IPE and widespread adoption of IPE recommendations into international medical society scientific statements and guidelines (31, 33–38), global findings from IPE eligibility and cost-effectiveness studies further underscore that IPE is a feasible add-on treatment to statins, especially in the secondary prevention setting. Importantly, the benefits of IPE cannot be generalized to other formulations of EPA. This is important because IPE is not available in some countries.
Review conception: PT, JF, MW, MM, NL, NW. Collection and assembly of data: PT, JF, MW, MM, NL, NW. Data interpretation: PT, JF, MW, MM, NL, NW. Manuscript preparation: PT, JF, MW, MM, NL, NW. All authors participated in the critical review and revision of this manuscript and provided approval of the manuscript for submission. All authors contributed to the article and approved the submitted version.
This analysis was sponsored by Amarin Pharma, Inc.
Medical writing and editorial support were provided by Lilly Shelomyanov, MS, Noud van Helmond, MD, PhD, and Sherri Damlo, MS, ELS, at Peloton Advantage, LLC, an OPEN Health company (Parsippany, NJ), and were funded by Amarin Pharma, Inc. (Bridgewater, NJ).
PT: speakers bureau Amgen and Novo-Nordisk; consultant to Novartis. JF: has received grants and personal fees from Akcea, Amarin, Amgen, Merck Sharp and Dohme, Sanofi, and Servier. NW: research support from Novartis, Novo Nordisk, and Lilly and consultant of Novartis. MM: has received speaker fees from Amarin, Novo Nordisk, Amgen, and Sanofi. MW: stock shareholder Watershed Group. NL: has received research funding from Sanofi as part of a Clinical Fellowship in Endocrinology and Diabetes, education support from Amgen, Bayer, Boehringer Ingelheim, and Eli Lilly, and speaker honoraria from Sanofi, Boehringer Ingelheim, and Eli Lilly.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Amini M, Zayeri F, Salehi M. Trend analysis of cardiovascular disease mortality, incidence, and mortality-to-incidence ratio: results from global burden of disease study 2017. BMC Public Health. (2021) 21:401. doi: 10.1186/s12889-021-10429-0
2. Baigent C, Keech A, Kearney PM, Blackwell L, Buck G, Pollicino C, et al. Efficacy and safety of cholesterol-lowering treatment: prospective meta-analysis of data from 90,056 participants in 14 randomised trials of statins. Lancet. (2005) 366:1267–78. doi: 10.1016/S0140-6736(05)67394-1
3. Wong ND, Zhao Y, Quek RGW, Blumenthal RS, Budoff MJ, Cushman M, et al. Residual atherosclerotic cardiovascular disease risk in statin-treated adults: the multi-ethnic study of atherosclerosis. J Clin Lipidol. (2017) 11:1223–33. doi: 10.1016/j.jacl.2017.06.015
4. Kaasenbrood L, Boekholdt SM, van der Graaf Y, Ray KK, Peters RJ, Kastelein JJ, et al. Distribution of estimated 10-year risk of recurrent vascular events and residual risk in a secondary prevention population. Circulation. (2016) 134:1419–29. doi: 10.1161/CIRCULATIONAHA.116.021314
5. Jorgensen AB, Frikke-Schmidt R, West AS, Grande P, Nordestgaard BG, Tybjaerg-Hansen A. Genetically elevated non-fasting triglycerides and calculated remnant cholesterol as causal risk factors for myocardial infarction. Eur Heart J. (2013) 34:1826–33. doi: 10.1093/eurheartj/ehs431
6. The HPS2-THRIVE Collaborative Group. Effects of extended-release niacin with laropiprant in high-risk patients. N Engl J Med (2014) 371:203–12. doi: 10.1056/NEJMoa1300955
7. The ACCORD Study Group, Ginsberg HN, Elam MB, Lovato LC, Crouse IIIJR, Leiter LA, et al. Effects of combination lipid therapy in type 2 diabetes mellitus. N Engl J Med. (2010) 362:1563–74. doi: 10.1056/NEJMoa1001282
8. Pradhan A D, Glynn RJ, Fruchart JC, MacFadyen JG, Zaharris ES, Everett BM, et al. Triglyceride lowering with pemafibrate to reduce cardiovascular risk. N Engl J Med. (2022) 387:1923–34. doi: 10.1056/NEJMoa2210645
9. Aung T, Halsey J, Kromhout D, Gerstein HC, Marchioli R, Tavazzi L, et al. Associations of omega-3 fatty acid supplement use with cardiovascular disease risks: meta-analysis of 10 trials involving 77917 individuals. JAMA Cardiol. (2018) 3:225–34. doi: 10.1001/jamacardio.2017.5205
10. Bhatt DL, Steg G, Miller M, Brinton EA, Jacobson TA, Ketchum SB, et al. Cardiovascular risk reduction with icosapent ethyl for hypertriglyceridemia. N Engl J Med. (2019) 380:11–22. doi: 10.1056/NEJMoa1812792
12. Singh N, Bhatt DL, Miller M, Steg PG, Brinton EA, Jacobson TA, et al. Consistency of benefit of icosapent ethyl by background statin type in REDUCE-IT. J Am Coll Cardiol. (2022) 79:220–2. doi: 10.1016/j.jacc.2021.11.005
13. Nelson JR, Budoff MJ, Wani OR, Le V, Patel DK, Nelson A, et al. EPA's pleiotropic mechanisms of action: a narrative review. Postgrad Med. (2021) 133:651–64. doi: 10.1080/00325481.2021.1921491
14. Wilkins JT, Lloyd-Jones DM. Icosapent ethyl supplementation and cardiovascular prevention-implications of evolving data. JAMA Cardiol. (2022) 7(12):1185–6. doi: 10.1001/jamacardio.2022.3701
15. Nissen SE. When is a placebo not a placebo. JAMA Cardiol. (2022) 7(12):1183–84. doi: 10.1001/jamacardio.2022.3698
16. Doi T, Langsted A, Nordestgaard BG. A possible explanation for the contrasting results of REDUCE-IT vs. STRENGTH: cohort study mimicking trial designs. Eur Heart J. (2021) 42:4807–17. doi: 10.1093/eurheartj/ehab555
17. FDA Briefing Document Endocrinologic and Metabolic Drugs Advisory Committee Meeting, Food and Drug Administration (2019).
18. Committee for Medicinal Products for Human Use. Assessment report: Vazkepa. Amsterdam: European Medicines Agency (2021).
19. Yokoyama M, Origasa H, Matsuzaki M, Matsuzawa Y, Saito Y, Ishikawa Y, et al. Effects of eicosapentaenoic acid on major coronary events in hypercholesterolaemic patients (JELIS): a randomised open-label, blinded endpoint analysis. Lancet. (2007) 369:1090–8. doi: 10.1016/S0140-6736(07)60527-3
20. Olshansky B, Chung MK, Budoff MJ, Philip S, Jiao L, Doyle RT Jr., et al. Mineral oil: safety and use as placebo in REDUCE-IT and other clinical studies. Eur Heart J Suppl. (2020) 22(suppl J):J32–48. doi: 10.1093/eurheartj/suaa117
21. Gopaul VS, Pieterman EJ, Princen HMG, Bergenholm L, Lundborg E, Cavallin A, et al. Effects of mineral oil administration on the pharmacokinetics, metabolism and pharmacodynamics of atorvastatin and pravastatin in mice and dogs. Eur J Pharm Sci. (2021) 161:105776. doi: 10.1016/j.ejps.2021.105776
22. Sherratt SCR, Libby P, Bhatt DL, Mason RP. Comparative effects of mineral oil, corn oil, eicosapentaenoic acid, and docosahexaenoic acid in an in vitro atherosclerosis model. J Am Heart Assoc. (2023) 12:e029109. doi: 10.1161/JAHA.122.029109
23. Sheppard JP JP, Lakshmanan S, Dahal S, Roy SK, Bhatt DL, Budoff MJ, et al. EPA Versus mixed EPA/DHA plus statin for coronary atherosclerosis: meta-analysis of prospective imaging trials. JACC Cardiovasc Imaging. (2022) 15:1825–8. doi: 10.1016/j.jcmg.2022.04.014
24. Watanabe T, Ando K, Daidoji H, Otaki Y, Sugawara S, Matsui M, et al. A randomized controlled trial of eicosapentaenoic acid in patients with coronary heart disease on statins. J Cardiol. (2017) 70:537–44. doi: 10.1016/j.jjcc.2017.07.007
25. Budoff MJ, Bhatt DL, Kinninger A, Lakshmanan S, Muhlestein JB, Le VT, et al. Effect of icosapent ethyl on progression of coronary atherosclerosis in patients with elevated triglycerides on statin therapy: final results of the EVAPORATE trial. Eur Heart J. (2020) 41:3925–32. doi: 10.1093/eurheartj/ehaa652
26. Nosaka K, Miyoshi T, Iwamoto M, Kajiya M, Okawa K, Tsukuda S, et al. Early initiation of eicosapentaenoic acid and statin treatment is associated with better clinical outcomes than statin alone in patients with acute coronary syndromes: 1-year outcomes of a randomized controlled study. Int J Cardiol. (2017) 228:173–9. doi: 10.1016/j.ijcard.2016.11.105
27. Daida H, Nishizaki Y, Iwata H, Inoue T, Hirayama A, Kimura K, et al. Randomized trial for evaluation in secondary prevention efficacy of combination therapy—statin and eicosapentaenoic acid (RESPECT-EPA) [oral presentation]. Chicago, IL: Annual Scientific Sessions of the American Heart Association (2022).
28. Nishizaki Y, Miyauchi K, Iwata H, Inoue T, Hirayama A, Kimura K, et al. Study protocol and baseline characteristics of randomized trial for evaluation in secondary prevention efficacy of combination therapy-statin and eicosapentaenoic acid: RESPECT-EPA, the combination of a randomized control trial and an observational biomarker study. Am Heart J. (2022) 257:1–8. doi: 10.1016/j.ahj.2022.11.008
29. Nelson JR, Budoff MJ. Fourth study to show consistent benefit of highly purified eicosapentaenoic acid on cardiovascular outcomes: Results from RESPECT-EPA. Cardiol News. (2023) (suppl). Available at: https://cdn.mdedge.com/files/s3fs-public/v2.0_aha_respect-epa_brief_comm_return_to_journal_from_frontline_12-13-22.pdf (Accessed August 14, 2023).
30. Kohro T, Yamazaki T. Cardiovascular clinical trials in Japan and controversies regarding prospective randomized open-label blinded end-point design. Hypertens Res. (2009) 32:109–14. doi: 10.1038/hr.2008.26
31. Miller M, Tokgozoglu L, Parhofer KG, Handelsman Y, Leiter LA, Landmesser U, et al. Icosapent ethyl for reduction of persistent cardiovascular risk: a critical review of major medical society guidelines and statements. Expert Rev Cardiovasc Ther. (2022) 20:609–25. doi: 10.1080/14779072.2022.2103541
32. Amarin Announces VAZKEPA® (icosapent ethyl) Approved by the Therapeutic Goods Administration (TGA) in Australia [press release], Amarin Corporation. (2022).
33. Orringer CE, Jacobson TA, Maki KC. National lipid association scientific statement on the use of icosapent ethyl in statin-treated patients with elevated triglycerides and high or very-high ASCVD risk. J Clin Lipidol. (2019) 13:860–72. doi: 10.1016/j.jacl.2019.10.014
34. Kimura K, Kimura T, Ishihara M, Nakagawa Y, Nakao K, Miyauchi K, et al. JCS 2018 Guideline on diagnosis and treatment of acute coronary syndrome. Circ J. (2019) 83:1085–196. doi: 10.1253/circj.CJ-19-0133
35. Cosentino F, Grant PJ, Aboyans V, Bailey CJ, Ceriello A, Delgado V, et al. 2019 ESC guidelines on diabetes, pre-diabetes, and cardiovascular diseases developed in collaboration with the EASD: the task force for diabetes, pre-diabetes, and cardiovascular diseases of the European society of cardiology (ESC) and the European association for the study of diabetes (EASD). Eur Heart J. (2020) 41:255–323. doi: 10.1093/eurheartj/ehz486
36. Precoma D, De Oliveira JM, Simao A, Dutra O, Coelho O, Izar M, et al. Updated cardiovascular prevention guideline of the Brazilian society of cardiology—2019. Arq Bras Cardiol. (2019) 113:787–891. doi: 10.5935/abc.20190204
37. Pearson GJ, Thanassoulis G, Anderson TJ, Barry AR, Couture P, Dayan N, et al. 2021 Canadian cardiovascular society guidelines for the management of dyslipidemia for the prevention of cardiovascular disease in the adult. Can J Cardiol. (2021) 37:1129–50. doi: 10.1016/j.cjca.2021.03.016
38. Virani SS, Morris PB, Agarwala A, Ballantyne CM, Birtcher KK, Kris-Etherton PM, et al. 2021 ACC expert consensus decision pathway on the management of ASCVD risk reduction in patients with persistent hypertriglyceridemia: a report of the American college of cardiology solution set oversight committee. J Am Coll Cardiol. (2021) 78:960–93. doi: 10.1016/j.jacc.2021.06.011
39. Zhang Z, Bhatt DL, Zhang C, Dolman S, Boden WE, Steg P, et al. Scenario analyses of lifetime cost-effectiveness of icosapent ethyl in REDUCE-IT [abstract]. Circ Cardiovasc Qual Outcomes. (2020) 13(suppl 1):A26. doi: 10.1161/hcq.13.suppl_1.26
40. Michaeli DT, Michaeli JC, Boch T, Michaeli T. Cost-effectiveness of lipid-lowering therapies for cardiovascular prevention in Germany. Cardiovasc Drugs Ther. (2023) 37(4):683–94. doi: 10.1007/s10557-021-07310-y
41. Picard F, Bhatt DL, Ducrocq G, Ohman EM, Goto S, Eagle KA, et al. Generalizability of the REDUCE-IT trial and cardiovascular outcomes associated with hypertriglyceridemia among patients potentially eligible for icosapent ethyl therapy: an analysis of the REduction of atherothrombosis for continued health (REACH) registry. Int J Cardiol. (2021) 340:96–104. doi: 10.1016/j.ijcard.2021.08.031
42. Jia X, Akeroyd JM, Nasir K, Nambi V, Ballantyne CM, Petersen LA, et al. Eligibility and cost for icosapent ethyl based on the REDUCE-IT trial. Insight from the veterans affairs healthcare system. Circulation. (2019) 139:1341–3. doi: 10.1161/CIRCULATIONAHA.118.038691
43. Picard F, Bhatt DL, Ducrocq G, Elbez Y, Ferrari R, Ford I, et al. Generalizability of the REDUCE-IT trial in patients with stable coronary artery disease. J Am Coll Cardiol. (2019) 73:1362–4. doi: 10.1016/j.jacc.2019.01.016
44. Sorbets E, Greenlaw N, Ferrari R, Ford I, Fox KM, Tardif JC, et al. Rationale, design, and baseline characteristics of the CLARIFY registry of outpatients with stable coronary artery disease. Clin Cardiol. (2017) 40:797–806. doi: 10.1002/clc.22730
45. Cainzos-Achirica M, Quispe R, Dudum R, Greenland P, Lloyd-Jones D, Rana JS, et al. CAC for risk stratification among individuals with hypertriglyceridemia free of clinical atherosclerotic cardiovascular disease. JACC Cardiovasc Imaging. (2022) 15(4):641–51. doi: 10.1016/j.jcmg.2021.10.017
46. Kim JM, Bhatt DL, Dagogo-Jack S, Cherney D, Cosentino F, Mcguire DK, et al. Eligibility for icosapent ethyl in patients with type 2 diabetes and atherosclerotic cardiovascular disease: an analysis of VERTIS CV [abstract]. Diabetes. (2022) 71(suppl 1):481-P. doi: 10.2337/db22-481-P
47. Wong ND, Fan W, Philip S, Granowitz C, Toth PP. REDUCE-IT eligibility and preventable cardiovascular events in the US population (from the national health and nutrition examination survey [NHANES]). Am J Cardiol. (2020) 134:62–8. doi: 10.1016/j.amjcard.2020.08.015
48. Kosmopoulos A, Verma S, Meglis G, Bhatt DL, Verma R, Mazer CD, et al. Generalizability of reduction of cardiovascular events with icosapent ethyl-intervention trial in patients with a history of coronary artery bypass graft surgery. Curr Opin Cardiol. (2021) 36:172–8. doi: 10.1097/HCO.0000000000000800
49. Lawler PR, Kotrri G, Koh M, Goodman SG, Farkouh ME, Lee DS, et al. Real-world risk of cardiovascular outcomes associated with hypertriglyceridaemia among individuals with atherosclerotic cardiovascular disease and potential eligibility for emerging therapies. Eur Heart J. (2020) 41:86–94. doi: 10.1093/eurheartj/ehz767
50. Krishnaraj A, Bakbak E, Teoh H, Bhatt DL, Quan A, Puar P, et al. Generalizability of the REDUCE-IT trial to south Asians with cardiovascular disease. Med. (2023) 4(2):130–138.e1. doi: 10.1016/j.medj.2022.12.008
51. Ferrières J, Bataille V, Puymirat E, Schiele F, Simon T, Danchin N. Applicability of the REDUCE-IT trial to the FAST-MI registry. Are the results of randomized trials relevant in routine clinical practice? Clin Cardiol. (2020) 43:1260–5. doi: 10.1002/clc.23437
52. Gaine S, Coughlan JJ, Maher V, Waters M. Residual risk in cardiac rehab: can we reduce-it more? Eligibility for icosapent ethyl in patients attending cardiac rehabilitation [abstract 54]. Heart. (2020) 106(suppl 4):A34–5.
53. Mortensen MB, Dzaye O, Razavi AC, Jensen JM, Steffensen FH, Bøtker HE, et al. Association between REDUCE-IT criteria, coronary artery disease severity and cardiovascular events: the western Denmark heart registry. Eur J Prev Cardiol. (2022) 29(13):1802–10. doi: 10.1093/eurjpc/zwac104
54. Lan NSR, Ali US, Larbalestier R, Dwivedi G, Bell DA. An opportunity to improve secondary prevention with icosapent ethyl in patients who have undergone coronary artery bypass graft surgery. Cardiovasc Revasc Med. (2022) 41:170–2. doi: 10.1016/j.carrev.2021.12.025
55. Cannon CP, McGuire DK, Pratley R, Dagogo-Jack S, Mancuso J, Huyck S, et al. Design and baseline characteristics of the eValuation of ERTugliflozin effIcacy and safety cardiovascular outcomes trial (VERTIS-CV). Am Heart J. (2018) 206:11–23. doi: 10.1016/j.ahj.2018.08.016
56. Kim JM, Bhatt DL, Dagogo-Jack S, Cherney DZI, Cosentino F, McGuire DK, et al. Potential for residual cardiovascular risk reduction: eligibility for icosapent ethyl in the VERTIS CV population with type 2 diabetes and atherosclerotic cardiovascular disease. Diabetes Obes Metab. (2023) 25(5):1398–402. doi: 10.1111/dom.14965
57. Verma S, Kosmopoulos A, Bhatt DL, Fitchett D, Ofstad AP, Wanner C, et al. Generalizability of REDUCE-IT eligibility criteria in a large diabetes cardiovascular outcomes trial: a post hoc subgroup analysis of EMPA-REG outcome: analysis of EMPA-REG OUTCOME using REDUCE-IT criteria. Am J Prevent Cardiol. (2023) 15:100510. doi: 10.1016/j.ajpc.2023.100510
58. Zinman B, Wanner C, Lachin JM, Fitchett D, Bluhmki E, Hantel S, et al. Empagliflozin, cardiovascular outcomes, and mortality in type 2 diabetes. N Engl J Med. (2015) 373:2117–28. doi: 10.1056/NEJMoa1504720
59. Shen M, Aghajani Nargesi A, Nasir K, Bhatt DL, Khera R. Contemporary national patterns of eligibility and use of novel lipid-lowering therapies in the United States. J Am Heart Assoc. (2022) 11:e026075. doi: 10.1161/JAHA.122.026075
60. Lan NSR, Fegan PG, Yeap BB, Rankin JM, Watts GF. Icosapent ethyl for dyslipidaemia in patients with diabetes and coronary artery disease: act now to reduce it. Diabetes Obes Metab. (2019) 21:1734–6. doi: 10.1111/dom.13689
61. Volgman AS, Palaniappan LS, Aggarwal NT, Gupta M, Khandelwal A, Krishnan AV, et al. Atherosclerotic cardiovascular disease in south asians in the United States: epidemiology, risk factors, and treatments: a scientific statement from the American heart association. Circulation. (2018) 138:e1–e34. doi: 10.1161/CIR.0000000000000580
62. Patel M, Abatcha S, Uthman O. Ethnic differences between south Asians and white caucasians in cardiovascular disease-related mortality in developed countries: a systematic literature review. Syst Rev. (2022) 11:207. doi: 10.1186/s13643-022-02079-z
63. Rana A, de Souza RJ, Kandasamy S, Lear SA, Anand SS. Cardiovascular risk among south Asians living in Canada: a systematic review and meta-analysis. CMAJ Open. (2014) 2:E183–91. doi: 10.9778/cmajo.20130064
65. Bouisset F, Gerbaud E, Bataille V, Coste P, Puymirat E, Belle L, et al. Percutaneous myocardial revascularization in late-presenting patients with STEMI. J Am Coll Cardiol. (2021) 78:1291–305. doi: 10.1016/j.jacc.2021.07.039
66. Arbel R, Aboalhasan E, Hammerman A, Azuri J. Icosapent ethyl for primary versus secondary prevention of major adverse cardiovascular events in hypertriglyceridemia-value for money analysis. Am J Med. (2021) 134:e415–9. doi: 10.1016/j.amjmed.2020.12.023
67. Ollendorf D, McQueen R, Fazioli K, Synnott P, Campbell J, Quinlan T, et al. Additive therapies for cardiovascular disease: Effectiveness and value, Institute for Clinical and Economic Review. Boston, MA: Institute for Clinical and Economic Review (2019).
68. Synnott PG, McQueen RB, Ollendorf DA, Campbell JD, Pearson SD. The effectiveness and value of rivaroxaban and icosapent ethyl as additive therapies for cardiovascular disease. J Manag Care Spec Pharm. (2020) 26(6):782–5. doi: 10.18553/jmcp.2020.26.6.782
69. Weintraub WS, Bhatt DL, Zhang Z, Dolman S, Boden WE, Bress AP, et al. Cost-effectiveness of icosapent ethyl for high-risk patients with hypertriglyceridemia despite statin treatment. JAMA Netw Open. (2022) 5:e2148172. doi: 10.1001/jamanetworkopen.2021.48172
70. Lachaine J, Charron JN, Gregoire JC, Hegele RA, Leiter LA. Cost-effectiveness of icosapent ethyl (IPE) for the reduction of the risk of ischemic cardiovascular events in Canada [abstract PCV55]. Value Health. (2020) 23(suppl 3):S496. doi: 10.1016/j.jval.2020.08.546
71. Ademi Z, Ofori-Asenso R, Zomer E, Owen A, Liew D. The cost-effectiveness of icosapent ethyl in combination with statin therapy compared with statin alone for cardiovascular risk reduction. Eur J Prev Cardiol. (2021) 28:897–904. doi: 10.1177/2047487319896648
72. Gao L, Moodie M, Li SC. The cost-effectiveness of omega-3 polyunsaturated fatty acids—the Australian healthcare perspective. Eur J Intern Med. (2019) 67:70–6. doi: 10.1016/j.ejim.2019.07.001
Keywords: eicosapentaenoic acid, cardiovascular disease, cost effectiveness, icosapent ethyl, eligibility
Citation: Toth PP, Ferrières J, Waters M, Mortensen MB, Lan NSR and Wong ND (2023) Global eligibility and cost effectiveness of icosapent ethyl in primary and secondary cardiovascular prevention. Front. Cardiovasc. Med. 10:1220017. doi: 10.3389/fcvm.2023.1220017
Received: 9 May 2023; Accepted: 8 August 2023;
Published: 31 August 2023.
Edited by:
Raffaele De Caterina, University of Pisa, ItalyReviewed by:
Federica Fogacci, University of Bologna, Italy© 2023 Toth, Ferrières, Waters, Mortensen, Lan and Wong. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Peter P. Toth cGV0ZXIudG90aEBjZ2htYy5jb20=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.