 Changjian He1,†
Changjian He1,† Wenchang Zhang1,†Lei Yin2,†Mingzhuang Sun1Zihan Zhao1Guojie Ye1Tengfei Liu1Wence Shi1Da Zhang1
Wenchang Zhang1,†Lei Yin2,†Mingzhuang Sun1Zihan Zhao1Guojie Ye1Tengfei Liu1Wence Shi1Da Zhang1 Feng Li3*
Feng Li3* Chunhua Ding1*
Chunhua Ding1*
- 1Cardiac Department, Aerospace Center Hospital (Peking University Aerospace School of Clinical Medicine), Beijing, China
- 2Department of Cardiology, The Second Hospital of Hebei Medical University, Shijiazhuang, China
- 3Department of Cardiology, The Second Affiliated Hospital of Soochow University, Suzhou, China
Background: Although there are many freezing protocols available, the optimal freezing dose is still not determined. We aimed to evaluate the effectiveness and safety of different freeze strategies of CBA in the treatment of AF.
Methods: PubMed, Cochrane Library, Web of Science, and Embase were searched up to 1st December 2022. Studies comparing the outcomes between single-shot technique and standard technique of cryoablation were included. Subgroup analysis identified potential determinants for single-shot technique procedure.
Results: Our search resulted in 3407 records after deduplication. A total of 17 qualified studies met our inclusion criteria. Compared with standard technique, single-shot technique of cryoablation has a comparable rate of freedom from AF/AT(RR 1.00; P = 0.968), a trend for lower rate of procedure complications (RR 0.80; P = 0.069), a lower rate in transient phrenic paralysis (t-PNP) (RR 0.67; P = 0.038), a similar rate in persistent phrenic paralysis (per-PNP) (RR 1.15; P = 0.645), as well as a comparable procedure parameters. Importantly, potentially significant treatment covariable interactions in procedure complications were found in freeze strategy subgroup, male proportion subgroup and age subgroup, including single-shot freeze (RR 1.02; P = 0.915) and TTI-guided (RR 0.63; P = 0.007) with interaction P = 0.051, high male proportion (RR 0.54; P = 0.005) and a low male proportion (RR 0.94; P = 0.759) with interaction P = 0.074, as well as age ≥ 65 (RR0.91; P = 0.642) and age <65 (RR 0.54; P = 0.006),interaction P = 0.090. Meanwhile, only one significant treatment covariable interactions in procedure complications was found in the hypertension subgroup, including HT > 60% (RR 0.89; P = 0.549) and HT ≤ 60% (RR 0. 46; P < 0.01) with interaction P = 0.043.
Conclusions: Our study suggested that single-shot technique of cryoablation has comparable effective and safety outcomes for AF ablation compared to standard technique.
1. Introduction
Pulmonary vein isolation (PVI) is the cornerstone of catheter ablation in patients with atrial fibrillation (AF). Cryo-balloon ablation (CBA) has been widely used for AF treatment worldwide. Whether in patients with paroxysmal atrial fibrillation (PFA) or persistent atrial fibrillation (per-AF), PVI alone has achieved satisfactory curative effects (1–3), which is superior to drug therapy and not inferior to radiofrequency ablation(RFA). CBA is characterized by less procedural complexity and a shorter learning curve. Different center and operator experience had a weaker impact on program success in CBA than in RFA procedure (4). Recently, several studies have demonstrated high acute efficacy and low complication rates using CBA for PVI in paroxysmal or persistent AF in both low-volume and high-volume centers (5, 6).
Due to the cumbersome nature of RFA to achieve PVI, CBA was developed to further simplify the PVI procedure by homogenizing the results of operators with different experience. However, the ideal energy dose has not yet been standardized, and preclinical and clinical studies have been trying to find the optimal cryo-energy dose that results in durable PVI with the shortest effective cryo-duration. The current CBA protocol are varied, including fixed cycle single ablation or double ablation, cryo-dose guided by TTI, and cryo-dose based on temperature monitoring (7, 8). This may hinder its application and promotion, and often confuses beginners, thus affecting the safety and effectiveness of CBA. The latest CB−2 ablation studies have demonstrated high single-procedure success rates for PVI, with good long-term clinical outcomes even when “no addition” cryo-protocols or shorter cryo-cycles were applied (9–15). Moreover, the rate of persistent PVI was high in patients who underwent re-acceptance of atrial tachyarrhythmias ablation after CB-2 ablation (16, 17). In addition, recent studies have shown that time-to-isolation (TTI) has the potential to be the best indicator for cryo-dose monitoring and a strong marker for predicting acute and durable PVI (18, 19). However, the current ability to monitor TTI needs to be further improved, and the TTI protocol has not yet formed a standardized unified scheme.
Therefore, in this study, we aimed to evaluate the effectiveness and safety of different administration strategies of CBA in the treatment of AF.
2. Methods
2.1. Search strategy
We conducted this systematic review according to the Preferred Reporting Items for Reviews and Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) guidelines (20). The study protocol was registered in the PROSPERO database (Registration ID: CRD42022382336).
A comprehensive literature search was conducted with four online search engines, including PubMed, Cochrane Library, Web of Science, and Embase, by two independent reviewers (C.J.H and F.L) from the establishment of the databases up to 1st December 2022. Search keywords included “cryoballon”, “cryoablation”, “ablation”, and “atrial fibrillation”. Trials comparing the therapeutic effects between single-shot technique of cryoablation and standard technique in patients with AF were included. In addition, the reference list of review literature and retrieved eligible literature were hand-searched for potential publications not being identified previously.
2.2. Study design
A clinical study was eligible if it met the following inclusion criteria: (1) randomized controlled trials and cohorts, observational studies, and case controls. (2) studies comparing the results of different freezing strategies, including long-term freedom of atrial fibrillation / AT, phrenic paralysis, pericardial effusion, stroke / transient ischemic attack (TIA) and surgery-related death. Phrenic nerve palsy (PNP)was classified as either transient or persistent. Transient phrenic nerve palsies (t- PNP), defined as palsy resolution by the end of the cryo-balloon procedure or before discharge, whereas persistent phrenic nerve palsy (per-PNP) was characterized by continued loss of phrenic nerve function that persisted during follow-up. (3) full-text studies published in English in peer-reviewed journals. (4) for multiple publications of the same trial or cohort, only the research containing the most data is included. Meanwhile, single-arm study, studies without original data, review articles, case reports, letters, editorials, and animal studies were excluded. Two independent reviewers (C.J.H and F.L) searched and reviewed the titles, abstracts, and full texts to determine the eligible study. Any disagreements about eligibility were resolved by consulting a third reviewer (C.H.D).
The intervention evaluated was CBA for AF. In this study, the single-shot technique was defined as the AF patients underwent single-shot freeze or TTI-guided single freeze. The standard technique was defined as the AF patients underwent double freeze or bonus freeze. Moreover, single-shot technique was allowed for additional freeze to reduce the concerns about lesion durability when sensory isolation was not achieved or achieved lately in the freezing process.
2.3. Data extraction
For each eligible study, data were extracted by two independent researchers (C.J.H and F.L), and any differences were resolved through discussion with a third researcher (C.H.D). We first recorded the eligible characteristics of the study, including the first author, year of publication, study design, number of patients, and follow-up time. At the same time, the demographic and clinical characteristics of the patients and the indicators related to the procedure were also recorded.
2.4. Quality assessment
Given the heterogeneity of the eligible studies, the quality of each study was assessed using two different critical appraisal tools by two independent researchers. For randomized clinical trial included in our review, the Cochrane risk of bias assessment tool was used. The Newcastle-Ottawa Quality Assessment Scale (NOS) was used to assess observational studies. We also assessed the potential publication using Egger's and Begg's test.
2.5. Statistical analysis
Categorical variables were presented as frequencies or percentages, and continuous variables were presented as means ± standard deviations, or median with interquartile range, as appropriate. The Stata version 16.0 (College Station, Texas 77845 USA, StataCorp LP) was used for all statistical analyses, and P < 0.05 was considered statistically significant.
We used I2 to quantify the proportion of variance derived from between-study heterogeneity (21) and I2 values of 0, <25%, 25%–49%, and >50% were considered as no, low, moderate, and high heterogeneity, respectively. If I2 value was more than 50%, a random effect model was adopted. Otherwise, a fixed effect model was used. Meanwhile, when significant heterogeneity was presented, we performed a sensitivity analysis to examine the effect of a single study on the overall risk estimate by sequentially omitting one study at a time. We also assessed the potential publication bias using Egger's tests.
In addition, subgroup analysis was performed to screen sources of heterogeneity and potential determinants of AF ablation outcomes between single-shot technique of cryoablation and standard technique. According to the characteristics of eligible studies, some potential factors, and previously reported factors, a total of nine subgroup factors were identified, including study design, follow-up time, sample size, age cutoff, male proportion, hypertension (HT) proportion, paroxysmal atrial fibrillation (PAF) proportion, left atrial diameter (LAD) and freeze strategy. If the study design included only one center, it was defined as a single-center subgroup; otherwise, it was defined as a multicenter subgroup. Follow-up time was divided into two subgroups (>12 months and ≤12 months). According to the cutoff value 100 and 65, the group sample size and the age cutoff were divided into two subgroups, respectively. According to cutoff values of 60%, the male proportion and HT proportion were divided into two subgroups, respectively. According to the cutoff value 100% and 40, the PAF proportion and LAD were divided into two subgroups, respectively. Based on the freeze strategy, single-shot and TTI-guided subgroups were defined.
3. Results
3.1. Study selection and quality assessment
The research selection flow chart is shown in Figure 1. Our search resulted in 3,407 records after deduplication. Abstracts were independently screened by two investigators. Finally, a total of 17 qualified studies met our inclusion criteria, including 6 prospective studies (15, 22–26) and 11 retrospective studies (8, 13, 14, 17, 27–33), including 4,688 patients with AF (2,526 in single-shot technique group and 2,162 in standard technique group). In two multicenter studies (17, 29), the only two subgroups, including bonus-freeze protocol group and the time-to-effect protocol group, were extracted due to their comparability. The demographic and clinical characteristics was presented in Table 1. Details of cryoablation are shown in Table 2.
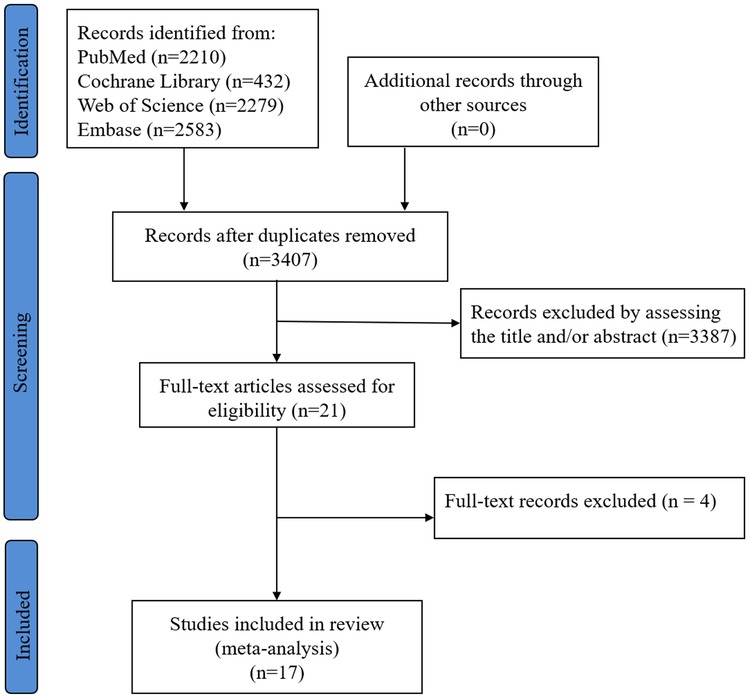
Figure 1. Flow diagram of the study selection.
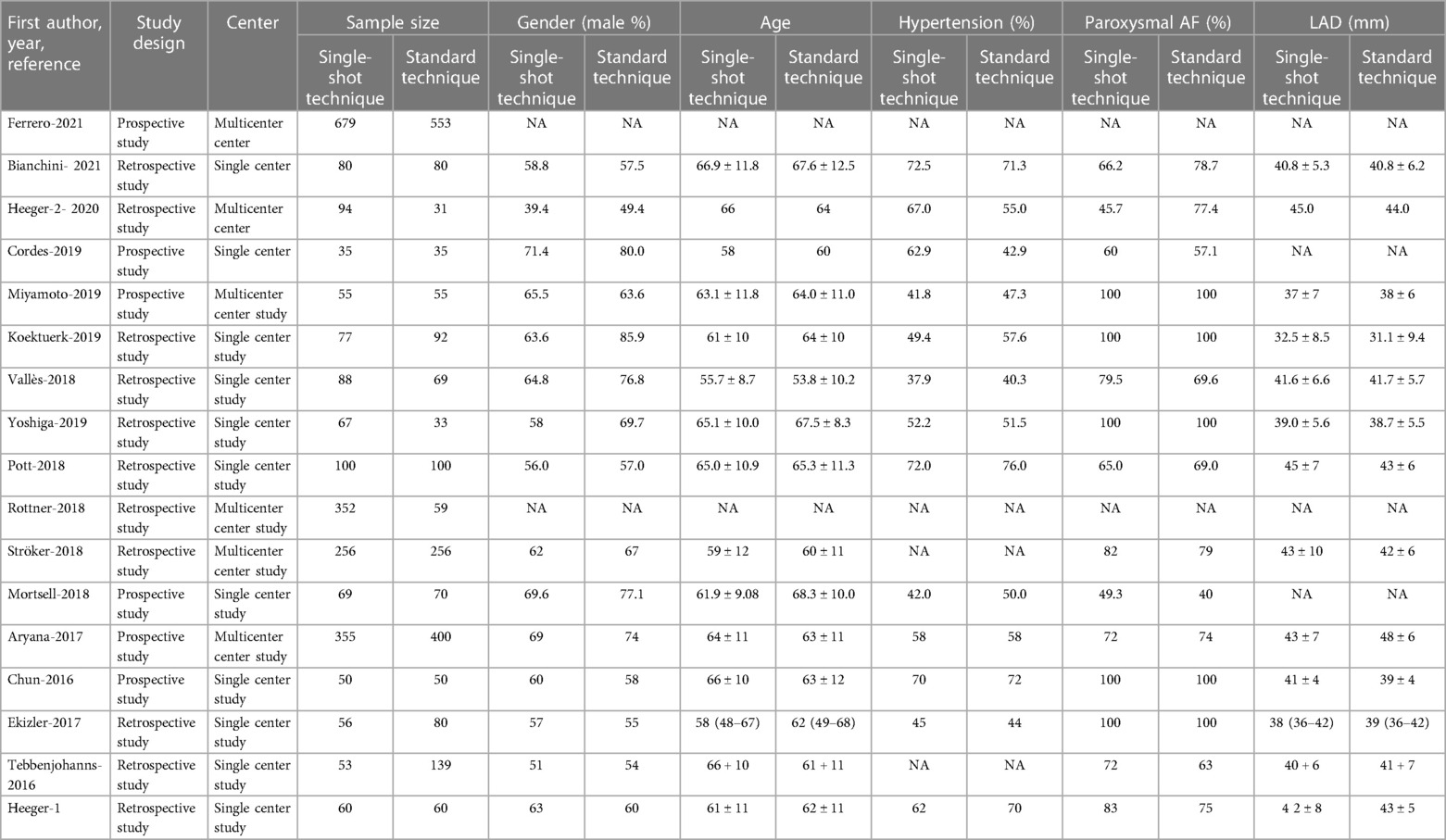
Table 1. The demographic and clinical characteristics.
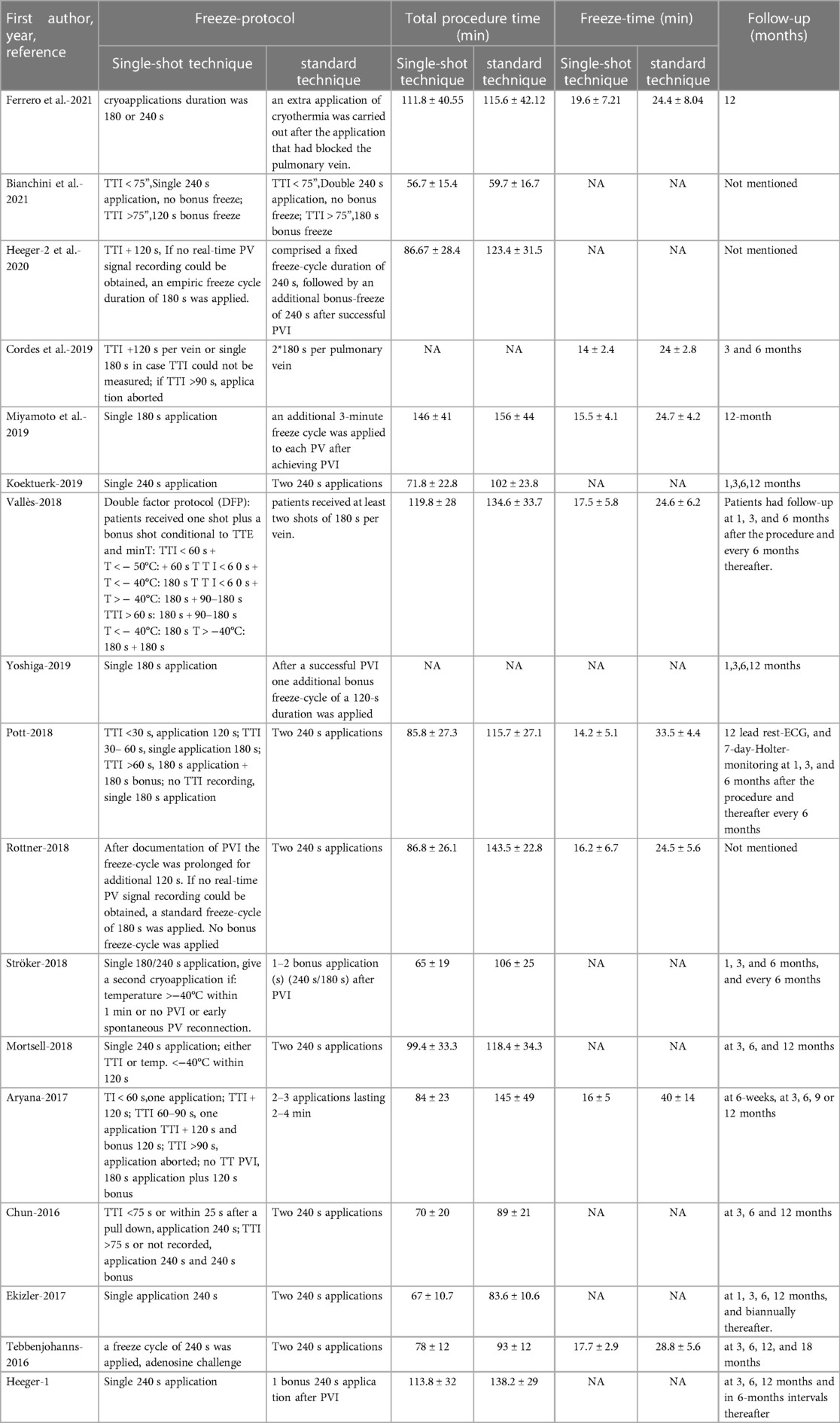
Table 2. Details of CBA.
3.2. Efficacy between single-shot technique and standard technique
A total of 14 studies (8, 13, 14, 15, 17, 22–33) reported 3,971 patients getting rid of AF/atrial tachycardia (AT), including 1990 in the single-shot technique group and 1981 in the standard technique group. Using the random effect model, the recurrence rate of AF/AT in the single-shot technique group was similar to that in the standard technique group (RR, 1.00; 95%CI, 0.97–1.03; P = 0.968; I2 = 0.0%; Figure 2).
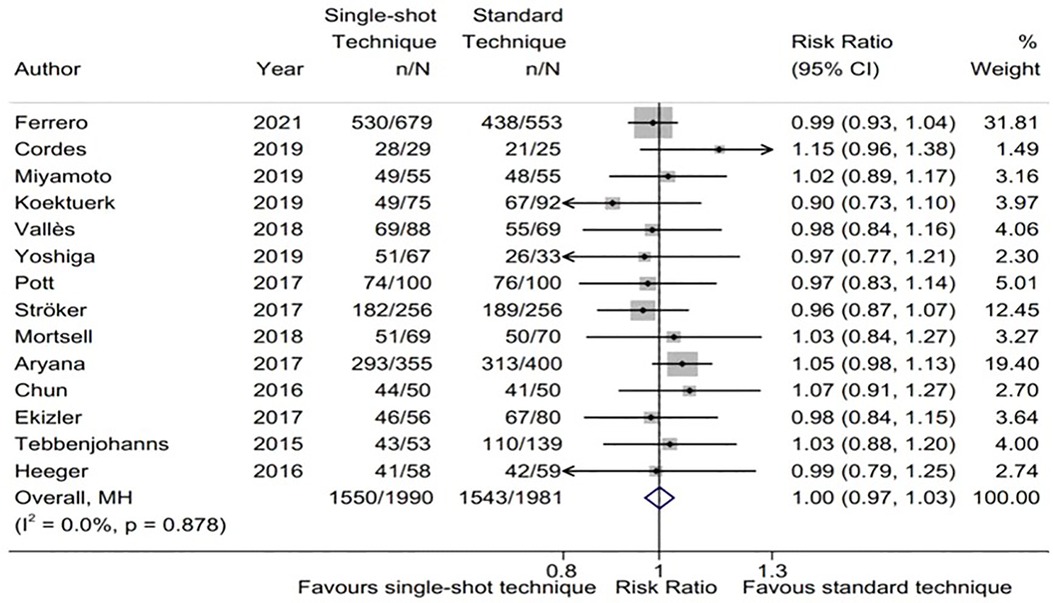
Figure 2. Forest plot of the freedom from atrial fibrillation (AF)/atrial tachycardia (AT). Comparison of the rate of freedom from AF/AT between single-shot technique and standard technique. AF, atrial fibrillation; AT, atrial tachycardia.
A total of nine subgroup factors of the freedom of AF were analyzed, and the results were shown in Figure 3 and Supplementary Table S1. There was no significant statistical difference among the subgroups. Interestingly, we found that in the predetermined subgroups, the success rates of ablation in single-shot freeze and TTI-guided groups were the same, and both were comparable to those in standard technique.
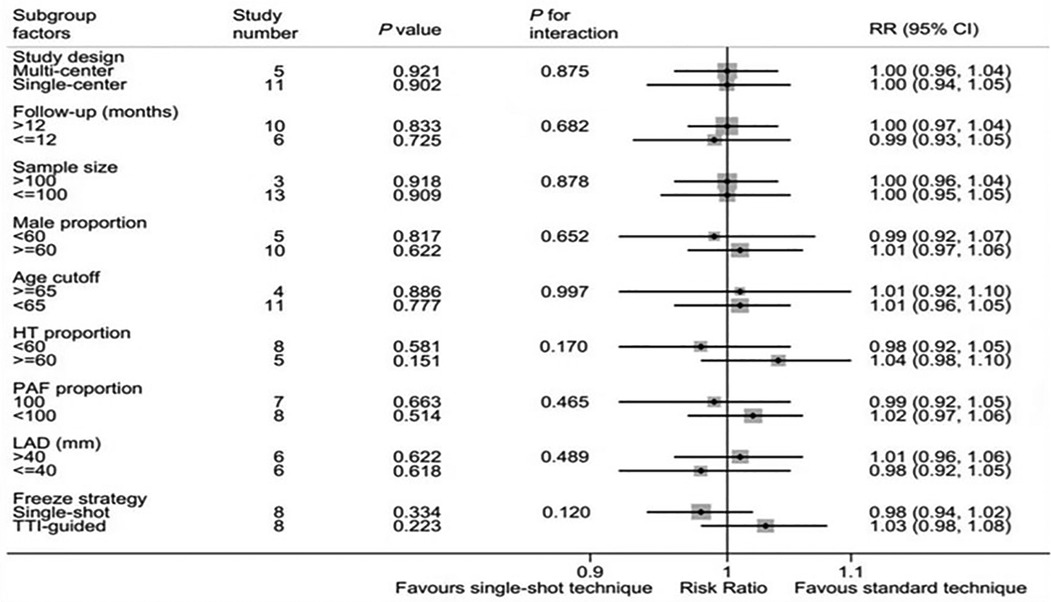
Figure 3. Forest plot of subgroup analysis for freedom from AF. Subgroup analysis of the rate of freedom from AF/AT between single-shot technique and standard technique.
Moreover, the sensitivity analysis show that there was no significant change for the pooled proportion, ranging from 0.99 (0.95–1.03) to 1.01 (0.97–1.05). Meanwhile, there was no publication bias with Egger's test (P = 0.94). These results suggested that our pooled results were robust.
3.3. Safety between single-shot technique and standard technique
14 studies reported procedure complications, 13 reported transient phrenic paralysis (t-PNP), and 11 reported per-PNP. The risk of complications in single-shot technique group showed a trend for lower rate than that in standard technique group. (RR, 0.80; 95%CI, 0.63–1.02; P = 0.069; I2 = 36.9%; Figure 4). Moreover, the sensitivity analysis show that there was no significant change for the pooled proportion, ranging from 0.69 (0.52–0.91) to 0.85 (0.67–1.09). Meanwhile, there was no publication bias with Egger's test (P = 0.18). These results suggested that our pooled results were robust.
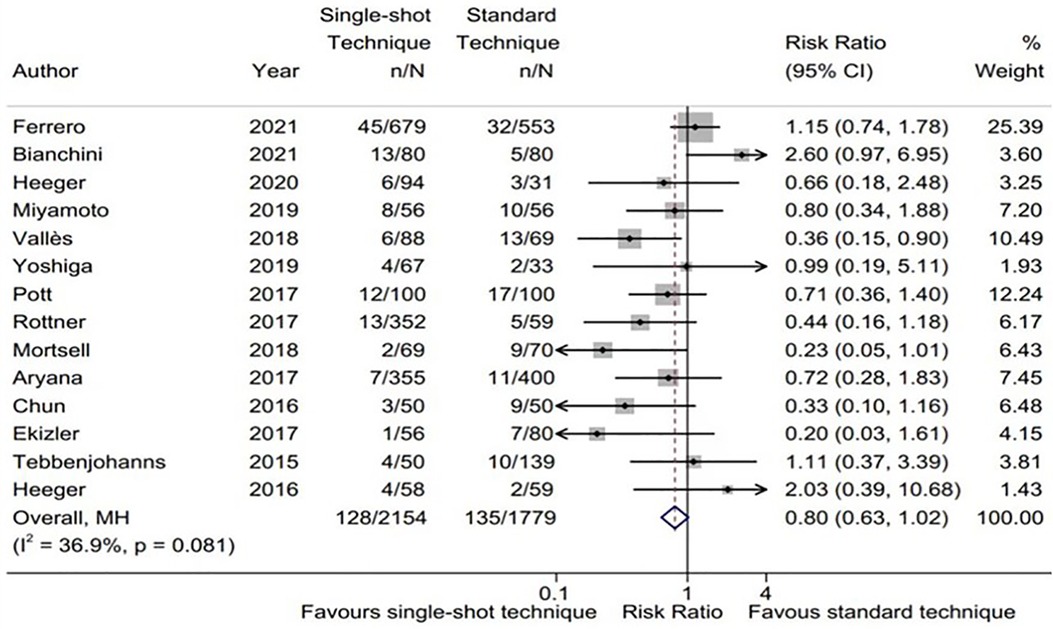
Figure 4. Forest plot of the procedure complications. Comparison of the procedure complications between single-shot technique and standard technique.
In our meta-analysis, the subgroup analysis results are shown in Figure 5 and Supplementary Table S2. The single center subgroup (RR, 0.70; 95%CI, 0.49–0.99; P = 0.042; I2 = 50.6%), sample size <100 subgroup (RR, 0.71; 95%CI, 0.52–0.97; P = 0.030; I2 = 38.5%), high male proportion subgroup (RR, 0.54; 95%CI, 0.35–0.83; P = 0.005; I2 = 19.9%), age <65 subgroup (RR, 0.54; 95%CI, 0.35–0.84; P = 0.006; I2 = 23.3%), low proportion of HT subgroup (RR, 0.46; 95%CI, 0.27–0.76; P = 0.003; I2 = 4.6%), simple paroxysmal atrial fibrillation subgroup (RR, 0.54; 95%CI, 0.30–0.99; P = 0.045; I2 = 0.0%), and TTI-guided subgroup (RR, 0.63; 95%CI, 0.45–0.88; P = 0.007; I2 = 45.8%) are significant statistical differences. There was no significant difference in left atrial diameter subgroup and follow-up time subgroup. Importantly, potentially significant treatment covariable interactions in the risk of complications were found in freeze strategy subgroup, male proportion subgroup and age subgroup, including single-shot freeze (RR 1.02; 95%CI, 0.72–1.43; P = 0.915) and TTI-guided(RR 0.63; 95%CI, 0.45–0.88; P = 0.007), interaction P = 0.051; high male proportion (RR 0.54; 95%CI, 0.35–0.83; P = 0.005) and a low male proportion (RR 0.94; 95%CI, 0.61–1.43; P = 0.759), interaction P = 0.074; age ≥ 65 (RR0.91; 95%CI, 0.61–1.36; P = 0.642) and age <65 (RR 0.54; 95%CI, 0.35–0.84; P = 0.006), interaction P = 0.090. In addition, significant treatment covariable interactions in the risk of complications were found in the hypertension subgroup, including HT > 60% (RR 0.89; 95%CI, 0.60–1.31; P = 0.549) and HT ≤ 60% (RR 0.46; 95%CI, 0.27–0.76; P < 0.01), interaction P = 0.043.
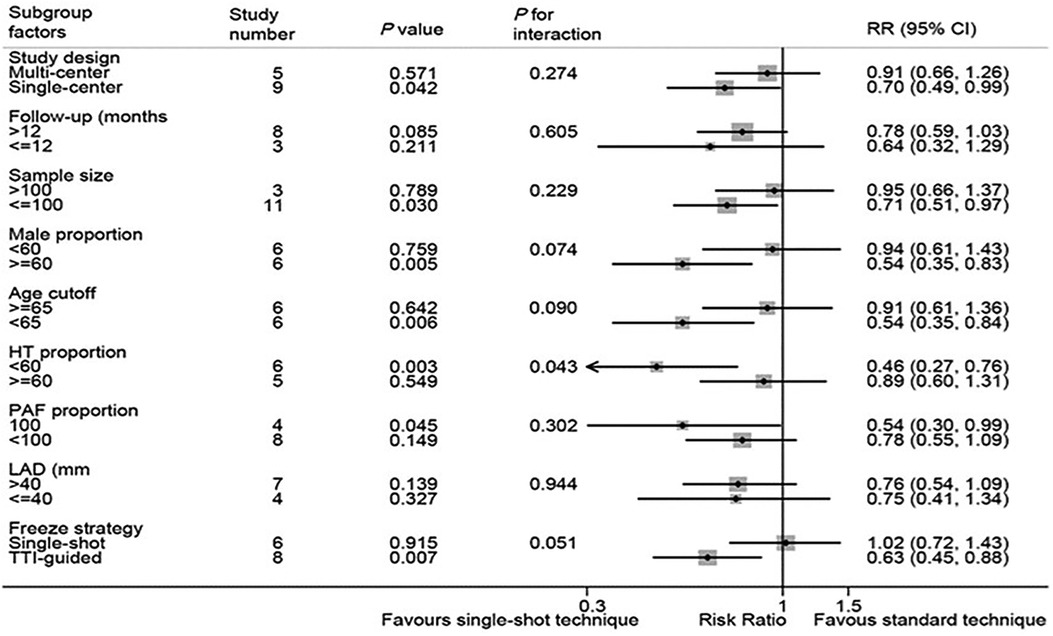
Figure 5. Forest plot of subgroup analysis for procedure complications. Subgroup analysis of the procedure complications between single-shot technique and standard technique.
Compared with standard technique group, single-shot technique group had a lower incidence of t-PNP (RR, 0.67; 95%CI, 0.45–0.96; P = 0.038; I2 = 0.0%). The sensitivity analysis show that there was no significant change for the pooled proportion, ranging from 0.57 (0.38–0.87) to 0.71 (0.48–1.07). No publication bias was presented with Egger's test (P = 0.06). These results suggested that our pooled results were robust. In addition, a similar risk of per-PNP was showed between standard technique group and single-shot technique group (RR, 1.15; 95%CI, 0.63–2.10; P = 0.645; I2 = 0.0%). The sensitivity analysis, ranging from 1.00 (0.54–1.86) to 1.37 (0.71–2.65), as well as Egger's test (P = 0.96) also showed that our pooled results were robust.
3.4. Procedure parameters
Total operation time was reported in 15 studies(8, 13–17, 22–25, 27, 29–32), freeze time in 8 studies(8, 13, 15, 22, 24, 26, 29, 31), and fluoroscopy time in 14 studies(8, 13–15, 17, 22–25, 27, 30–33). The results showed that the total operation time of single-shot technique group was significantly shorter than that of standard technique group. (SMD: −25.2; 95%CI: −35.25, −15.80; I2 = 97.5%, P < 0.001),and the freezing application time is significantly reduced (SMD: −11.73; 95%CI: −16.33, −7.2; I2 = 99.0%, P < 0.001). In terms of fluoroscopy time, the single-shot technique group decreased slightly (SMD: −3.3; 95%CI: −6.03,−0.58; I2 = 96.9%, P < 0.001).
3.5. Risk of bias
Of the seventeen studies, three were randomized clinical trials (RCT) studies and the remaining fourteen were Non-RCT studies. The Quality of the eligible studies was moderate to good (Tables 3, 4). All the three RCTs lacked blinding of participants and personnel to the intervention, and all observational studies had control groups and obtained their data directly from medical records. The NOS score varied between 8 and 9 which means they were high-quality observational studies.

Table 3. Quality assessment for randomized clinical trials according to the cochrane risk of bias assessment tool.
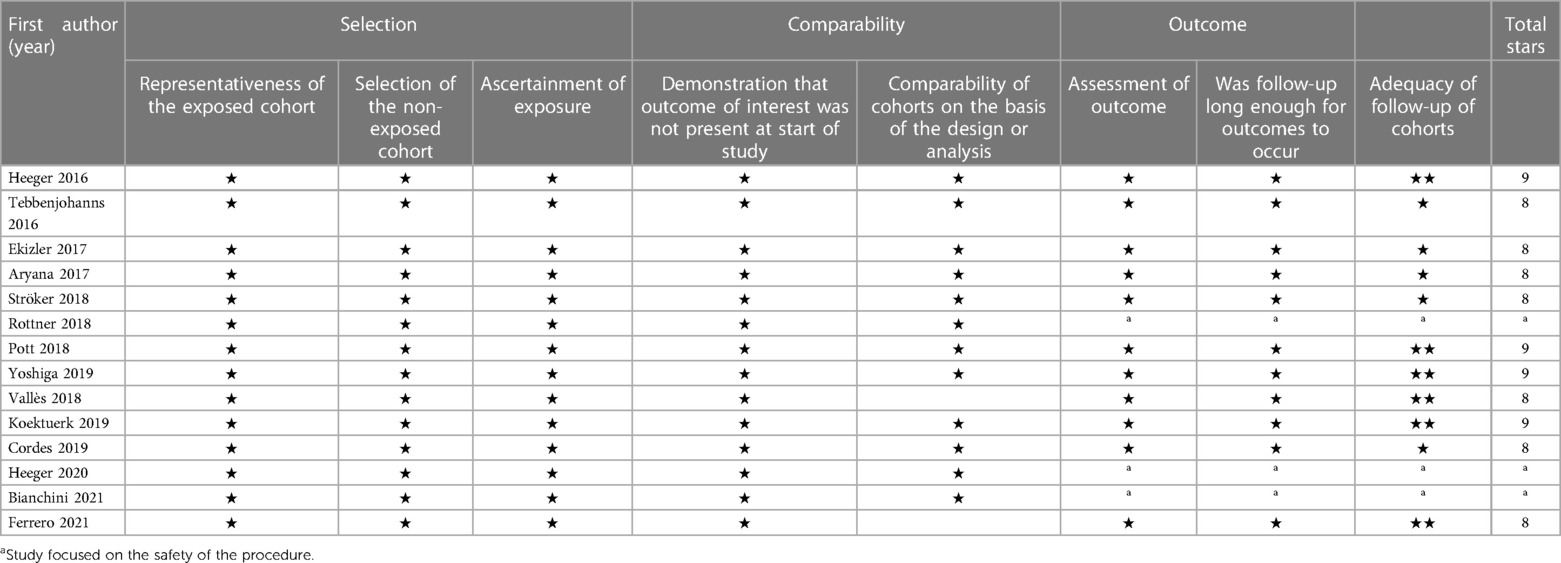
Table 4. Quality assessment of enrolled studies according to the Newcastle-Ottawa quality Assessment scale (NOS).
3.6. Sensitivity analysis for RCT and Non-RCT studies
Sensitivity analysis was performed for RCT and Non-RCT studies, and the method was to recalculate the pooled OR/SMD estimates of the remaining studies after excluding each trial item by item. The results showed that there was no individual study having a significant impact on the overall estimation of any outcome expect for the sensitivity results of the procedural complications in terms of RCT (Supplementary Table S3).
4. Discussion
We systematically evaluated 4,688 AF patients (2,526 in single-shot technique group and 2,162 in standard technique group) derived from a total of 17 original articles. To our knowledge, this registered study had the relatively large samples to explore the ablation results of AF with different freezing strategies. The main results included (1) single-shot technique of cryoablation for AF has comparable effective and safety outcomes compared to standard technique; (2) compared with the standard technique group, the single-shot technique group showed an extent advantage in terms of the total operation time and freeze time and fluoroscopy time.
At present, there is no accepted opinion on the dose strategy for CBA. The scope of the ablation protocol has developed from a rather conservative fixed freeze cycle to an empirical bonus freeze, following with a more tailored and personalized ablation strategy to implement “time-to-isolation”. Previous studies have revealed that the single freeze showed a similar efficacy and better safety compared to the double/bonus freeze (22, 23, 27–30). Similarly, a recent meta-analysis has indicated that the single freeze strategy was as effective as the empirical double /bonus freeze strategy for CBA, while it was likely to be safer and faster (34). Unsimilar with previous studies, our registered study had the relatively large samples to explore the ablation results of AF, as well as potential determinants of AF ablation outcomes, between single-shot technique of cryoablation and standard technique. Additionally, a meta-analysis performed by Tsiachris et al. (35) showed that the personalized TTI-guided strategy based on TTI and the prolonging the duration of CBA (more than two minutes after TTI) is associated with less AF recurrence after ablation, which did not affect the safety of AF ablation and shorten the duration of ablation.
TTI, an acute biophysical indicator of PVI reflecting the transmural cold transmission, was considered as a significantly valuable and quantifiable index to evaluate the success of operation (24). Preliminary studies indicated that Cryo-application based on TTI may be significantly associated with the better long-term results (25). Recently, the INDI-FREEZE trial further reported that compared to the fixed protocol, the TTI-guided individualized approach provides a similar safety profile and clinical outcome, while reducing the total freezing time (36). It appears reasonable to implement TTI into individualized energy dosing protocols. However, the high incidence of real-time pulmonary vein potential recording is a necessary condition for the personalized PVI based on TTI. The tip length of the CB2 is 13.5 mm, which limits its real-time monitoring of TTI, and the new CB4 is characterized by a shorter tip, which may facilitate to better TTI monitoring. Although the ability of TTI monitoring had been significantly improved with the emergence of CB4, the overall capacity failed to completely satisfactory, with the success monitoring rate ranging from 70% to 86.2%. Therefore, it seemed necessary to further improve the CB system to improve the ability of TTI monitoring (37, 38). Since TTI is not acquired in each individual application, single-shot freeze still has its significance and value.
In this study, our results showed that the similar success rates of ablation were displayed in in single-shot freeze and TTI-guided group, both of which were comparable to standard technique. In relatively inexperienced centers, or even large centers with rich experience, when TTI is difficult to be recording, single-shot freeze might achieve a satisfactory success rate for AF ablation without significant increase of complications. It is worth noting that although the efficacy in single-shot freeze group and TTI-guided group was similar, the risk of complications in the TTI-guided group was significantly lower than that in the single-shot freeze group and shorten the freezing time, suggesting that personalization and optimal freeze dose are still our ultimate goals. In addition, efforts should be made to develop tools to guide ablation techniques as accurately as possible to achieve irreversible targeted myocardial tissue injury. Studies based on animal models have shown that impedance measurements of annular electrodes may provide valuable data on ice propagation. This real-time measurement may be used to guide cryopreservation applications and further reduce the risk of extracardiac injury while ensuring that PVI (39).
The confounder of gender played a significant role on CBA is still controversial. Recently, Hermida et al. (40) found that the success rate of single freeze for PVI in female patients with PAF was significantly lower than that in male patients, and the incidence of complications in female patients was higher than that in male patients. In another study, the efficacy of CBA was similar in men and women, but the risk of complications was higher in women (41). In this study, our subgroup analysis showed that there was no significant difference in the effect of sex on CBA. However, in the high male proportion subgroup, there were fewer complications in the Single-shot technique group than in standard technique group.
Our subgroup analysis showed that age had no significant effect on the efficacy of cryotherapy. Interestingly, in the age <65 subgroup, there were fewer complications in the single-shot technique group than in the standard technique group. CBA is a relatively simple procedure that can be easily applied to elderly patients. Short operation time is very important for elderly patients and can minimize the incidence of complications. Moreover, another advantage of single application over double applications is that it may reduce pain, and older patients are better tolerated. Age should not be the only factor excluding elderly patients receiving CBA for AF. As an effective and safe procedure, CBA on elderly AF patients has similar success rate and complication rate compared with young ones (42, 43). In a multi-center study for the long-term efficacy and safety of CBA in octogenarian individuals, the results showed that CBA was effective even in patients over 80 years old, with a seemingly acceptable risk profile and a lower risk of complications (44). In a large all-comer study, they found that CBA was effective in all age groups. Although more recurrence was observed in the elderly in the late stage of follow up, age was not an independent predictor of recurrence. And the incidence of perioperative adverse events is very low, and age has nothing to do with increased risk (45).
Ablation strategies with additional freeze cycles require longer freeze time, which may be associated with an increased risk of collateral damage to extracardiac structures such as phrenic nerve (PN), esophagus, and bronchial trees. In a prospective study on the endoscopic examination of mediastinal and esophageal changes caused by frozen balloon PVI, the results showed that compared with conventional protocol, TTI-guided with CB2 reduced the incidence and size of mediastinal and esophageal lesions and had a similar effect in the treatment of AF (26). Previous studies have found that less freeze application may be associated with a lower incidence of complications. Our subgroup analysis shows that single-shot technique appears to be safer for the safety of ablation, and complications of TTI-guided groups are significantly lower than those in single-shot freeze and standard technique groups. In addition, consistent with previous studies (29, 31, 32), we also found that the single-shot technique group significantly shortened the total operation time, freeze time and fluoroscopy time without increase of the procedure risk, which was beneficial to accelerate the turnover of the operating room. Interestingly, Heeger et al. (46) found that in patients with premature CB application abortion due to PNP, a high rate of persistent PVI was found at repeat procedures. It is expected to further shorten the application of freezing without affecting the success rate of ablation.
PNP is a typical complication of PVI with CBA. In the case of phrenic nerve injury, the movement of the diaphragm can be limited or even cancelled, resulting in severe dyspnea, which may counteract the clinical benefits of restoring sinus rhythm. The reported incidence of PNP is ranged from 1.1% to 6.2%. In the latest multicenter, multinational retrospective registration study, the incidence of PNP during CBA was approximately 4.2%. Overall, 97% of PNP was likely to recover within 12 months. Symptomatic and per-PNP is very rare after CBA based PVI (0.06%) (47). The recovery rate of PNP is high, and clinically related perioperative PNP seems to be rare in CBA-based PVI. Some studies had shown that there was no difference in the average numbers of freeze times between patients without PNP and patients with pers-PNP during right superior pulmonary vein isolation, suggesting that PNP had nothing to do with more cryo-application times (48). Moreover, Bianchini et al. (33) found that the number of double 120 s freeze strategy seems to be significantly less than that of a single 240 s PNP event, and only shows a short-term form of damage. However, another study showed that PNP patients had shorter freeze times and total freeze time than non-PNP patients. The authors speculate that the reason may be due to the result of the operator's emergency termination of the freeze application in the event of compound muscle action potential (CMAP) reduction or PN capture loss (49). Our meta-analysis found that compared with standard technique group, single-shot technique group had a lower incidence of t-PNP, both have a similar risk of per-PNP. We speculate that this may be due to the shorter freezing time and the more individual freezing application in the single-shot technique group. And one of the reasons for this result is the high clinical recovery rate of persistent phrenic nerve paralysis. This also indicated that the single-shot technique group reduced the incidence of phrenic nerve paralysis while shortening the operation time. Although both the left and right phrenic nerves may theoretically be injured, the right phrenic nerves are most likely to be injured during cryoablation of the right pulmonary vein because they are close to each other. Studies have shown that the use of near-end sealing technology and avoiding deeper balloon position, combined with CMAP detection is helpful to reduce the number of PNP (50).
Sensitivity analysis of effective and safety outcomes between single-shot technique vs. standard technique was performed for RCT and Non-RCT studies. The sensitivity analysis results verified the robustness of our meta-analysis results, expect the results of the procedural complications in RCT. This suggested that procedural complications between single-shot technique of cryoablation and standard technique should be interpreted with caution, and more RCTs will be needed to further confirm our results.
5. Limitations
Three studies focused on the safety of surgery without mentioning further follow-up, and none of the studies were achieved with five- or ten-year follow-up, making it a challenge to objectively evaluate the long-term efficacy and safety of the single-shot technique group compared with the standard technique group. The results of subgroup analysis may be limited by a limited number of available studies, which leads to the need for careful interpretation of subgroup results. Therefore, large cohort randomized controlled trials and longer follow-up are needed to further confirm the clinical results. The included study could not rule out the potential effects of different freezing duration on cryoablation (such as 240 and 180 s).
6. Conclusions
Our study suggested that single-shot technique of cryoablation has comparable effective and safety outcomes for AF ablation compared to standard technique.
Author contributions
CD developed the concept of the study. CH, WZ, and LY designed this study and carried out the data analysis. CH wrote the manuscript with help from CD and FL. MS, ZZ, GY, TL, WS, DZ, and CD provided critical reviews of the paper. All authors have read and approved the final manuscript. All author contributed to the article and approved the submitted version.
Acknowledgments
We would like show our sincere appreciation to the reviewers for critical comments on this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fcvm.2023.1195492/full#supplementary-material
References
1. Sawhney V, Schilling RJ, Providencia R, Cadd M, Perera D, Chatha S, et al. Cryoablation for persistent and longstanding persistent atrial fibrillation: results from a multicentre European registry. Europace. (2020) 22(3):375–81. doi: 10.1093/europace/euz313
2. Su WW, Reddy VY, Bhasin K, Champagne J, Sangrigoli RM, Braegelmann KM, et al. Cryoballoon ablation of pulmonary veins for persistent atrial fibrillation: results from the multicenter STOP persistent AF trial. Heart Rhythm. (2020) 17(11):1841–7. doi: 10.1016/j.hrthm.2020.06.020
3. Reissmann B, Plenge T, Heeger CH, Schlüter M, Wohlmuth P, Fink T, et al. Predictors of freedom from atrial arrhythmia recurrence after cryoballoon ablation for persistent atrial fibrillation: a multicenter study. J Cardiovasc Electrophysiol. (2019) 30(9):1436–42. doi: 10.1111/jce.14023
4. Providencia R, Defaye P, Lambiase PD, Pavin D, Cebron JP, Halimi F, et al. Results from a multicentre comparison of cryoballoon vs. radiofrequency ablation for paroxysmal atrial fibrillation: is cryoablation more reproducible. Europace. (2017) 19(1):48–57. doi: 10.1093/europace/euw080
5. Hoffmann R, Parade U, Bauerle H, Winter KD, Rauschenbach U, Mischke K, et al. Safety and acute efficacy of cryoballoon ablation for atrial fibrillation at community hospitals. Europace. (2021) 23(11):1744–50. doi: 10.1093/europace/euab132
6. Bordignon S, Chen S, Bologna F, Thohoku S, Urbanek L, Willems F, et al. Optimizing cryoballoon pulmonary vein isolation: lessons from >1000 procedures- the Frankfurt approach. Europace. (2021) 23(6):868–77. doi: 10.1093/europace/euaa406
7. Paparella G, Iacopino S, Osório TG, de Torres JPA, Ströker E, Sieira J, et al. Temperature-guided ablation with the second-generation cryoballoon for paroxysmal atrial fibrillation: 3-year follow-up in a multicenter experience. J Interv Card Electrophysiol. (2021) 61(1):95–104. doi: 10.1007/s10840-020-00770-6
8. Vallès E, Benito B, Jiménez J, Cabrera S, Alcalde O, Altaba C, et al. Double factor single shot to diminish complications in cryoballoon ablation procedures for atrial fibrillation. J Interv Card Electrophysiol. (2019) 55(1):17–26. doi: 10.1007/s10840-018-0483-3
9. Heeger CH, Subin B, Wissner E, Fink T, Mathew S, Maurer T, et al. Second-generation cryoballoon-based pulmonary vein isolation: lessons from a five-year follow-up. Int J Cardiol. (2020) 312:73–80. doi: 10.1016/j.ijcard.2020.03.062
10. Hara S, Miyazaki S, Hachiya H, Kajiyama T, Watanabe T, Nakamura H, et al. Long-term outcomes after second-generation cryoballoon ablation of paroxysmal atrial fibrillation—feasibility of a single short freeze strategy without bonus applications. Int J Cardiol. (2020) 306:90–4. doi: 10.1016/j.ijcard.2020.02.032
11. Chen S, Schmidt B, Bordignon S, Tohoku S, Urbanek L, Plank K, et al. Cryoballoon pulmonary vein isolation in treating atrial fibrillation using different freeze protocols: the “ICE-T 4 minutes vs. 3 minutes” propensity-matched study (Frankfurt ICE-T 4 vs. 3). J Cardiovasc Electrophysiol. (2020) 31(8):1923–31. doi: 10.1111/jce.14602
12. Canpolat U, Kocyigit D, Yalcin MU, Coteli C, Sener YZ, Oksul M, et al. Long-term outcomes of pulmonary vein isolation using second-generation cryoballoon during atrial fibrillation ablation. Pacing Clin Electrophysiol. (2019) 42(7):910–21. doi: 10.1111/pace.13721
13. Tebbenjohanns J, Höfer C, Bergmann L, Dedroogh M, Gaudin D, von Werder A, et al. Shortening of freezing cycles provides equal outcome to standard ablation procedure using second-generation 28 mm cryoballoon after 15-month follow-up. Europace. (2016) 18(2):206–10. doi: 10.1093/europace/euv189
14. Heeger CH, Wissner E, Wohlmuth P, Mathew S, Hayashi K, Sohns C, et al. Bonus-freeze: benefit or risk? Two-year outcome and procedural comparison of a “bonus-freeze” and “no bonus-freeze” protocol using the second-generation cryoballoon for pulmonary vein isolation. Clin Res Cardiol. (2016) 105(9):774–82. doi: 10.1007/s00392-016-0987-8
15. De Loma Osorio Ángel F, Rocío C, Arcadio GA, Ermengol V, Alberto B, Jorge T, et al. Primary results of the Spanish Cryoballoon Ablation Registry: acute and long-term outcomes of the RECABA study. Sci Rep. (2021) 11(1):17628. doi: 10.1038/s41598-021-96655-3
16. Miyazaki S, Kajiyama T, Watanabe T, Nakamura H, Hachiya H, Tada H, et al. Can the durability of pulmonary vein isolation be predicted by the time-to-isolation in second-generation cryoballoon ablation?: insight from the results of repeat procedures. Circ Arrhythm Electrophysiol. (2020) 13(1):e008076. doi: 10.1161/CIRCEP.119.008076
17. Heeger CH, Rexha E, Maack S, Rottner L, Fink T, Mathew S, et al. Reconduction after second-generation cryoballoon-based pulmonary vein isolation- impact of different ablation strategies. Circ J. (2020) 84(6):902–10. doi: 10.1253/circj.CJ-19-1144
18. Getman MK, Wissner E, Ranjan R, Lalonde JP. Relationship between time-to-isolation and freeze duration: computational modeling of dosing for Arctic front advance and arctic front advance pro cryoballoons. J Cardiovasc Electrophysiol. (2019) 30(11):2274–82. doi: 10.1111/jce.14150
19. Aryana A, Mugnai G, Singh SM, Pujara DK, de Asmundis C, Singh SK, et al. Procedural and biophysical indicators of durable pulmonary vein isolation during cryoballoon ablation of atrial fibrillation. Heart Rhythm. (2016) 13(2):424–32. doi: 10.1016/j.hrthm.2015.10.033
20. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Int J Surg. (2021) 88:105906. doi: 10.1016/j.ijsu.2021.105906
21. Higgins JP, Thompson SG. Quantifying heterogeneity in a meta-analysis. Stat Med. (2002) 21(11):1539–58. doi: 10.1002/sim.1186
22. Miyamoto K, Doi A, Hasegawa K, Morita Y, Mishima T, Suzuki I, et al. Multicenter study of the validity of additional freeze cycles for cryoballoon ablation in patients with paroxysmal atrial fibrillation: the AD-balloon study. Circ Arrhythm Electrophysiol. (2019) 12(1):e006989. doi: 10.1161/CIRCEP.118.006989
23. Mörtsell D, Malmborg H, Lönnerholm S, Jansson V, Blomström-Lundqvist C. Acute and long-term efficacy and safety with a single cryoballoon application as compared with the standard dual application strategy: a prospective randomized study using the second-generation cryoballoon for pulmonary vein isolation in patients with symptomatic atrial fibrillation. Europace. (2018) 20(10):1598–605. doi: 10.1093/europace/euy014
24. Aryana A, Kenigsberg DN, Kowalski M, Koo CH, Lim HW, O'Neill PG, et al. Verification of a novel atrial fibrillation cryoablation dosing algorithm guided by time-to-pulmonary vein isolation: results from the cryo-DOSING study (cryoballoon-ablation DOSING based on the assessment of time-to-effect and pulmonary vein isolation guidance). Heart Rhythm. (2017) 14(9):1319–25. doi: 10.1016/j.hrthm.2017.06.020
25. Chun KR, Stich M, Fürnkranz A, et al. Individualized cryoballoon energy pulmonary vein isolation guided by real-time pulmonary vein recordings, the randomized ICE-T trial. Heart Rhythm. (2017) 14(4):495–500. doi: 10.1016/j.hrthm.2016.12.014
26. Cordes F, Ellermann C, Dechering DG, Frommeyer G, Kochhäuser S, Lange PS, et al. Time-to-isolation-guided cryoballoon ablation reduces oesophageal and mediastinal alterations detected by endoscopic ultrasound: results of the MADE-PVI trial. Europace. (2019) 21(9):1325–33. doi: 10.1093/europace/euz142
27. Koektuerk B, Koektuerk O, Yorgun H, Guelker JE, Turan C, Gorr E, et al. Long-term impact of a bonus freeze on clinical outcome: analysis of effective and non-effective bonus freezes in cryoballoon ablation. PLoS One. (2019) 14(5):e0214231. doi: 10.1371/journal.pone.0214231
28. Yoshiga Y, Okamoto T, Shimizu A, Ueyama T, Ono M, Mito T, et al. Correlation between asymptomatic gastroesophageal excessive transmural injury after pulmonary vein isolation and a bonus freeze protocol using the second-generation 28-mm cryoballoon for paroxysmal atrial fibrillation. J Cardiol. (2019) 74(6):494–500. doi: 10.1016/j.jjcc.2019.05.008
29. Rottner L, Fink T, Heeger CH, Schlüter M, Goldmann B, Lemes C, et al. Is less more? Impact of different ablation protocols on periprocedural complications in second-generation cryoballoon based pulmonary vein isolation. Europace. (2018) 20(9):1459–67. doi: 10.1093/europace/eux219
30. Ekizler A, Aras D, Cay S, Ozeke O, Ozcan F, Topaloglu S. Bonus vs. no bonus cryoballoon isolation for paroxysmal atrial fibrillation ablation. J Atr Fibrillation. (2017) 9(5):1513. doi: 10.4022/jafib.1513
31. Pott A, Kraft C, Stephan T, Petscher K, Rottbauer W, Dahme T. Time-to-isolation guided titration of freeze duration in 3rd generation short-tip cryoballoon pulmonary vein isolation—comparable clinical outcome and shorter procedure duration. Int J Cardiol. (2018) 255:80–4. doi: 10.1016/j.ijcard.2017.11.039
32. Ströker E, Kupics K, de Asmundis C, Mugnai G, de Regibus V, De Cocker J, et al. Atrial fibrillation ablation with the second generation cryoballoon: multicenter propensity score matched comparison between freezing strategies. Int J Cardiol. (2018) 253:78–81. doi: 10.1016/j.ijcard.2017.11.069
33. Bianchini L, Bordignon S, Chen S, Zanchi S, Tohoku S, Bologna F, et al. Increased procedural safety of cryoballoon pulmonary vein isolation with a double 120 s freeze protocol. Pacing Clin Electrophysiol. (2021) 44(8):1371–9. doi: 10.1111/pace.14299
34. Farkowski MM, Karlinski M, Barra S, Providencia R, Golicki D, Pytkowski M, et al. Effectiveness and safety of a single freeze strategy of cryoballoon ablation of atrial fibrillation: an EHRA systematic review and meta-analysis. Europace. (2022) 24(1):58–69. doi: 10.1093/europace/euab133
35. Tsiachris D, Doundoulakis I, Antoniou CK, Pagkalidou E, Zafeiropoulos S, Kordalis A, et al. Effectiveness and safety of a time to isolation strategy of cryoballoon ablation of atrial fibrillation: a systematic review and meta-analysis. J Cardiovasc Electrophysiol. (2022) 33(12):2640–8. doi: 10.1111/jce.15697
36. Heeger CH, Popescu SS, Saraei R, Kirstein B, Hatahet S, Samara O, et al. Individualized or fixed approach to pulmonary vein isolation utilizing the fourth-generation cryoballoon in patients with paroxysmal atrial fibrillation: the randomized INDI-FREEZE trial. Europace. (2022) 24(6):921–7. doi: 10.1093/europace/euab305
37. Miyazaki S, Hasegawa K, Mukai M, Aoyama D, Nodera M, Shiomi Y, et al. The advantages and disadvantages of the novel fourth-generation cryoballoon as compared to the second-generation cryoballoon in the current short freeze strategy. J Interv Card Electrophysiol. (2022) 63(1):143–52. doi: 10.1007/s10840-021-00957-5
38. Manfrin M, Verlato R, Arena G, Pieragnoli P, Molon G, Tondo C, et al. Second versus fourth generation of cryoballoon catheters: the 1STOP real-world multicenter experience. Pacing Clin Electrophysiol. (2022) 45(8):968–74. doi: 10.1111/pace.14494
39. Avitall B, Kalinski A, Kocheril GS, Lizama KS, Coulombe N, Laske T. Characteristics of ice impedance recorded from a ring electrode placed at the anterior surface of the cryoballoon: novel approach to define ice formation and pulmonary vein isolation. Circ Arrhythm Electrophysiol. (2018) 11(4):e005949. doi: 10.1161/CIRCEP.117.005949
40. Hermida A, Burtin J, Kubala M, Fay F, Lallemand PM, Buiciuc O, et al. Sex differences in the outcomes of cryoablation for atrial fibrillation. Front Cardiovasc Med. (2022) 9:893553. doi: 10.3389/fcvm.2022.893553
41. Ekrami NK, Magni FT, Dayalani V, van Gelder IC, Groenveld HF, Tieleman RG, et al. Assessment of sex-related differences and outcome in patients who underwent cryoballoon pulmonary vein isolation for atrial fibrillation: an observational cohort study. BMJ Open. (2022) 12(11):e063359. doi: 10.1136/bmjopen-2022-063359
42. Abdin A, Yalin K, Lyan E, Sawan N, Liosis S, Meyer-Saraei R, et al. Safety and efficacy of cryoballoon ablation for the treatment of atrial fibrillation in elderly patients. Clin Res Cardiol. (2019) 108(2):167–74. doi: 10.1007/s00392-018-1336-x
43. Kanda T, Masuda M, Kurata N, Asai M, Iida O, Okamoto S, et al. Efficacy and safety of the cryoballoon-based atrial fibrillation ablation in patients aged ≥80 years. J Cardiovasc Electrophysiol. (2019) 30(11):2242–7. doi: 10.1111/jce.14166
44. Cecchini F, Mugnai G, Iacopino S, Abugattas JP, Adriaenssens B, Al-Housari M, et al. Safety and long-term efficacy of cryoballoon ablation for atrial fibrillation in octogenarians: a multicenter experience. J Interv Card Electrophysiol. (2022) 65(2):559–71. doi: 10.1007/s10840-022-01313-x
45. Hartl S, Dorwarth U, Pongratz J, Aurich F, Brück B, Tesche C, et al. Impact of age on the outcome of cryoballoon ablation as the primary approach in the interventional treatment of atrial fibrillation: insights from a large all-comer study. J Cardiovasc Electrophysiol. (2021) 32(4):949–57. doi: 10.1111/jce.14972
46. Heeger CH, Popescu SȘ, Sohns C, Pott A, Metzner A, Inaba O, et al. Impact of cryoballoon application abortion due to phrenic nerve injury on reconnection rates: a YETI subgroup analysis. Europace. (2023) 25(2):374–81. doi: 10.1093/europace/euac212
47. Heeger CH, Sohns C, Pott A, Metzner A, Inaba O, Straube F, et al. Phrenic nerve injury during cryoballoon-based pulmonary vein isolation: results of the worldwide YETI registry. Circ Arrhythm Electrophysiol. (2022) 15(1):e010516. doi: 10.1161/CIRCEP.121.010516
48. Pott A, Wirth H, Teumer Y, Weinmann K, Baumhardt M, Schweizer C, et al. Predicting phrenic nerve palsy in patients undergoing atrial fibrillation ablation with the cryoballoon-does sex matter. Front Cardiovasc Med. (2021) 8:746820. doi: 10.3389/fcvm.2021.746820
49. Tokuda M, Yamashita S, Sato H, Oseto H, Ikewaki H, Yokoyama M, et al. Long-term course of phrenic nerve injury after cryoballoon ablation of atrial fibrillation. Sci Rep. (2021) 11(1):6226. doi: 10.1038/s41598-021-85618-3
50. Anwar O, Gunawardene MA, Dickow J, Scherschel K, Jungen C, Münkler P, et al. Contemporary analysis of phrenic nerve injuries following cryoballoon-based pulmonary vein isolation: a single-centre experience with the systematic use of compound motor action potential monitoring. PLoS One. (2020) 15(6):e0235132. doi: 10.1371/journal.pone.0235132
Keywords: atrial fibrillation, cryo-balloon ablation, single-shot technique, meta-analysis, time to isolation
Citation: He C, Zhang W, Yin L, Sun M, Zhao Z, Ye G, Liu T, Shi W, Zhang D, Li F and Ding C (2023) Single-shot technique of cryoablation for atrial fibrillation has comparable effective and safety outcomes compared to standard technique: insights from multiple clinical studies. Front. Cardiovasc. Med. 10:1195492. doi: 10.3389/fcvm.2023.1195492
Received: 28 March 2023; Accepted: 14 August 2023;
Published: 7 September 2023.
Edited by:
Teresa Strisciuglio, University of Naples Federico II, ItalyReviewed by:
Christian Hendrik Heeger, University Heart Center Luebeck, GermanyRui Providência, Institute of Health Informatics Research—University College London, United Kingdom
© 2023 He, Zhang, Yin, Sun, Zhao, Ye, Liu, Shi, Zhang, Li and Ding. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Chunhua Ding dingmd@gmail.com Feng Li m17512576836@163.com
†These authors have contributed equally to this work