 Reine Sam Shi Ni
Reine Sam Shi Ni Hanis Qarissa Mohamed Raffi
Hanis Qarissa Mohamed Raffi Yanhong Dong
Yanhong Dong
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Cardiovasc. Med., 23 May 2023
Sec. Cardioneurology
Volume 10 - 2023 | https://doi.org/10.3389/fcvm.2023.1181979
This article is part of the Research TopicSpotlights On CardioneurologyView all 5 articles
Introduction: Heart Failure and Cognitive Impairment are both on the rise and shown to be interlinked. Despite existing reviews delineating a relationship between heart failure and cognitive impairment, the underlying pathophysiology is not researched in great depth. Current literature proposed varying pathophysiological mechanisms and focused heavily on the prevalence of cognitive impairment and treatment interventions such as cardiac rehabilitation. In view of the limitations of previous reviews, this systematic review summarized the best existing evidence concerning different pathophysiological mechanisms behind cognitive impairment in individuals with heart failure.
Methods: Eight electronic databases including PubMed, Cochrane Library and EMBASE etc., two grey literatures (ProQuest Theses and Dissertations and Mednar) and hand-searching of references were performed using specific criteria regarding population, exposures and outcomes, before duplicate removal and screening using Endnote and Rayyan respectively. JBI critical appraisal tools for non-randomized studies were used for appraisal. Data extraction was performed using two modified forms from JBI Manual for Evidence Synthesis.
Results: Narrative synthesis was performed to summarize the data from 32 studies. There were three main themes—cognitive impairment due to changes in the brain: brain atrophy, alterations in grey matter and white matter, cerebral alterations, pathway or axis changes, neuroinflammation and hippocampal gene changes; cognitive impairment due to changes in the heart or systemic circulation: inflammation, oxidative stress and changes in serum biomarkers or proteins and the riser rhythm; cognitive impairment due to changes in both the brain and the heart, with seven studies obtaining negative results. There are some limitations such as having non-human studies and large numbers of cross-sectional studies etc.
Discussion: Considering the findings, future research should examine the bi-directional relationship between the brain and the heart as most of the existing research is about the effect of the heart on the brain. By understanding the different pathophysiological mechanisms, the management and prognosis of heart failure patients will be ameliorated. Interventions that slow down or even reverse cognitive impairment can be explored so that these two common issues will not add to the already aggravating disease burden.
Systematic Review Registration: This review is registered under PROSPERO. Identifier: CRD42022381359.
Heart Failure (HF) is an illness with structural and functional defects in the myocardium, resulting in failure to perform ventricular filling or ejection. HF can be acute or chronic. There are two major types of HF, namely Heart Failure with preserved ejection fraction (HFpEF) and Heart Failure with reduced ejection fraction (HFrEF). In HFpEF, the EF is usually above 50% with the left-ventricular (LV) cavity volume being normal. In HFrEF, the EF is below 40% and LV cavity is dilated (1). There are four HF classes according to the New York Heart Association (NYHA) (2), which would be discussed later. Around 64.3 million people are diagnosed with HF worldwide, with a surge in the younger population (3). HF brings about many co-morbidities. Common ones include chronic kidney disease, diabetes, and obesity, especially in HFpEF (4). Others include hypertension, atrial fibrillation, and ischemic heart disease (3).
The comorbidity discussed in this review is Cognitive Impairment (CI), which is present in around 40% of HF. Patients with HF typically exhibit CI in domains of memory, attention, processing speed, and executive function. They face issues with self-management and medication adherence (5). They have difficulties learning and concentrating. In HF, CI usually ranges from mild cognitive impairments (MCI) to dementia (6). MCI does not fully disrupt patients' daily activities, but it is an important stage before transiting to dementia, which is a bigger health burden. It is crucial to prevent MCI and the development of dementia (7). Common cognitive tools used includes Mini-Mental State Examination (MMSE) and Montreal Cognitive Assessment (MoCA) (8).
Pathophysiology refers to the study of changes in bodily functions which lead to the development of diseases. It usually involves studying biological processes related to the diseases, such as identifying biological markers and mechanisms that can explain the progress of the disease (9).
Two of the existing systematic reviews were more pertinent to this review. The first one included 66 studies and found that cognitive decline was related to medial temporal lobe atrophy (MTA), reduced cerebral blood flow (CBF) and decrease of grey matter (GM). Some other factors included increased B-type natriuretic peptide (NT-proBNP) and the aforementioned comorbidities—Diabetes Mellitus, obesity and atrial fibrillation. However, it concentrated heavily on imaging, which might have restricted the exploration of other pathophysiological mechanisms, albeit being published recently (10). The second one included 148 studies and reported similar findings—brain atrophy, GM, white matter (WM) and poor CBF. Additionally, it included infarcts and microemboli, which influenced cardiac output (11). However, it only utilized PubMed and was published in 2015 hence the data would not be as extensive and updated. Moreover, it extended to all types of CI but this review restricted to MCI, dementia and Alzheimer's Disease (AD) since they are the common CI linked to HF.
Most systematic reviews did not include grey literature. Despite delineating a relationship between HF and CI, the underlying pathophysiology was not researched in great depth. Current literature proposed varying pathophysiological mechanisms but focused heavily on the prevalence of CI in HF and treatment interventions such as cardiac rehabilitation. In light of the limitations, this review summarized the best existing evidence concerning the different pathophysiological mechanisms behind CI in individuals with Heart Failure. The following question was addressed: What is the pathophysiology of Cognitive Impairment in individuals with Heart Failure? The gaps were addressed in this review to provide an updated overview of all the available literature. As CI has negative impacts on the trajectory of HF patients, it is important to understand the mechanisms that correlate them together.
The methodology was referenced from Joanna Briggs Institute (JBI) Reviewer's Manual on systematic reviews of etiology and risk (12). This review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Protocols (PRISMA) guidelines and statement (13) and was registered under PROSPERO CRD42022381359. The PRISMA checklist is attached in Supplementary Appendix S1.
The inclusion criteria were as follows: (1) human individual with HF diagnosis or animal HF model; (2) minimally one cognitive tool or diagnosis of cognitive problem(s) including dementia, AD and MCI for human studies; (3) in peer-reviewed journals; (4) published in English or Chinese; (5) quantitative studies—observational studies which encompass cross-sectional, case-control and cohort studies; 6) published from 1 January 2013 to 31 December 2022. This was set as filter whenever possible. If the full date could not be set, it would be set with the year minimally. The limit of 10 years ensured sufficient data whilst not being outdated. Meanwhile, for the other inclusion criteria, they would come into play during screening. The inclusion of animal models was necessary to avoid missing important results as animals especially mice, have more than 95% of homologous genes as humans and were used in numerous research studies (14).
The exclusion criteria were as follows. Firstly, the study was excluded if CI occurred before HF as it would not illustrate the pathophysiology of CI in HF. Secondly, studies that focused heavily on non-HF conditions were excluded, unless they included sufficient data on HF and the pathophysiology of CI on it. This was to prevent missing out on significant studies that could answer the research question and aim. Thirdly, all non-primary papers such as reviews, reports, commentaries, letters, protocols, clinical guidelines, and case reports were excluded.
Eight electronic databases, namely PubMed, Cochrane Library, EMBASE, ProQuest Social Science Premium Collection, Scopus, Web of Science Core Collection, CINAHL Complete and PsycINFO were used. The grey literature databases included ProQuest Theses and Dissertations and Mednar. Hand-searching of the reference list and journals was performed.
The three-step search strategy was adopted (12). The first step was an initial search of PubMed and Embase alongside the analysis of the keywords and subject headings contained in the title and abstract. A second search using those keywords and subject headings was conducted across the databases. The third step was examining the reference lists of selected sources to broaden the search results. We developed the search strategy iteratively and sought the assistance of a medical librarian for refinement. The strategies included keywords and subject headings in relation to Heart Failure, Cognitive Impairment, and pathophysiology, though there were variations between databases in terms of the MESH terms, Emtree terms and specific database subject headings. An example of the PubMed search strategy is illustrated in Table 1 by concepts. The full search strategy is included in Supplementary Appendix S2.
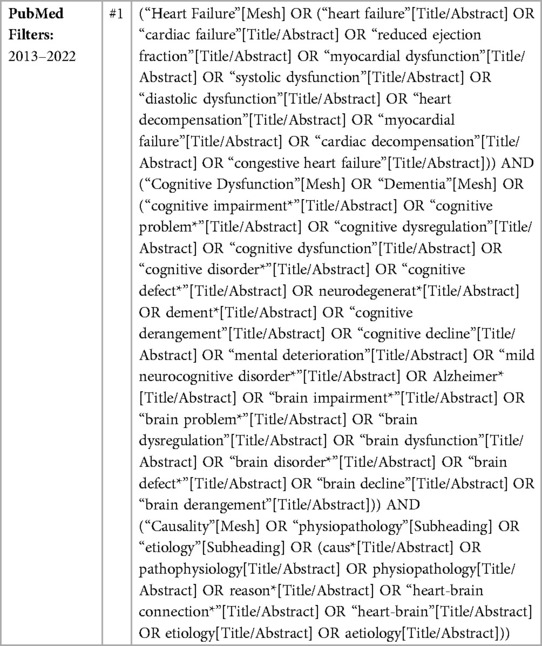
Table 1. Pubmed search strategy.
Endnote was used to manage the citations. It processes papers and citations in line with PRISMA (15, 16). The exported records were inclusive of a pre-searched filter—year of publication. Duplicates were removed before exporting to Rayyan. Rayyan allows for proper labelling and independent screening with other reviewers (16). Duplicates were removed again in Rayyan. Citation, title, and abstract screening were performed followed by full-text screening. The selection process and results were reported in the PRISMA chart. The search strategy and study selection were conducted independently by two reviewers (RS and HQ) with a consensus reached among them. The screening tool was piloted for five records to ensure mutual understanding of the criteria. The tool is attached in Supplementary Appendix S3.
For citation, title, and abstract screening, these eligibility criteria were used: (1) related to HF and CI; (2) from January 2013 to December 2022; (3) primary studies; (4) in English or Chinese; (5) non-intervention type [e.g., not randomized controlled trials (RCTs)]; (6) discuss the pathophysiology of CI in HF; (7) quantitative designs. For full-text screening, these eligibility criteria were used: (1) studies that fully fit aforementioned eligibility criteria; (2) access to the full-text. The excluded reports were tagged with the following reasons: (1) non primary study—study is related to HF and CI but is non primary; (2) intervention type study—study is related to HF and CI but is focused on intervention(s) or screening tools; (3) not HF and CI—study is not related to both HF and CI; (4) language—study is not in English or Chinese; (5) HF occurred after CI—different from the eligibility criteria required which was for individuals to have HF before CI; (6) not related to pathophysiology—study is related to both HF and CI but not on pathophysiological mechanisms; (7) year—study is published in a different year compared to the criteria; (8) no access—full-text cannot be accessed, the reports under this tag were included under “Reports not retrieved” in the PRISMA chart.
As Rayyan has “Excluded”, “Maybe” and “Included” labels, the records that passed the citation, title, and abstract screening stage were placed under “Maybe” and assessed subsequently during full-text screening. Besides Rayyan, an excel sheet was used to include the papers that were “Excluded” and “Maybe” during citation, title, and abstract screening. Details such as the title, database and reasons for exclusion were input. This acted as a backup record to prevent missing data. The reports in the excel sheet were indicated as “Excluded” or “Included” eventually after full-text screening.
The JBI checklists were used to appraise the studies by assessing the trustworthiness, relevance, and results. There are three different checklists for case-control, cohort, and cross-sectional studies respectively. They were answered using Yes, No, Unclear and Not Applicable. Eventually, a conclusion was made on the quality of the report and whether to include, exclude or to seek further information (17). The entire assessment was done by two reviewers (RS and HQ) with discussions performed for disagreements. The checklists are attached in Supplementary Appendix S4.
Two independent reviewers (RS and HQ) conducted data extraction for the included studies independently. In the event of disagreements, discussions were done. The data were extracted using forms modified from the guidelines of the JBI Manual for Evidence Synthesis, which were piloted on five studies before usage (12). There were two forms, one for human and one for animal studies since different forms of data would be extracted. These are attached in Supplementary Appendix S5.
For human studies, there were seven main sections to fill up in the form, namely General study details, Participant characteristics, Methods, Study result(s) or outcome(s), Data analysis methods, Others and Reviewer's comments. For animal studies, these seven sections were included with minor alterations. For Participant Characteristics, the age range, type of HF and cardiac function grades were omitted since these were mostly unavailable. For Methods, setting and preparation done were used instead of recruitment methods.
For data analysis, narrative summary was performed whereby the studies were discussed in textual form individually and in groups when there were similarities between the studies (18). This was due to unstandardized cognitive tools used and plenty of varying mechanisms. The studies were first placed in the main themes to discuss as a group due to similarities and those that did not fit were discussed separately.
A total of 7,815 records were identified from all databases. After duplicate removal, 5,151 records were set for screening. After citation, title, and abstract screening, there were 81 reports, with 39 being unretrievable. Out of the 39 reports, 37 reports were conference abstracts. Two were not conference abstracts and hence, their full texts were requested. However, one had the abstract only while the other received no response. The remaining 42 reports underwent full-text screening, with 32 studies being eligible. The final studies included 4,630 humans, 452 animals and six datasets. The PRISMA chart is illustrated in Figure 1.
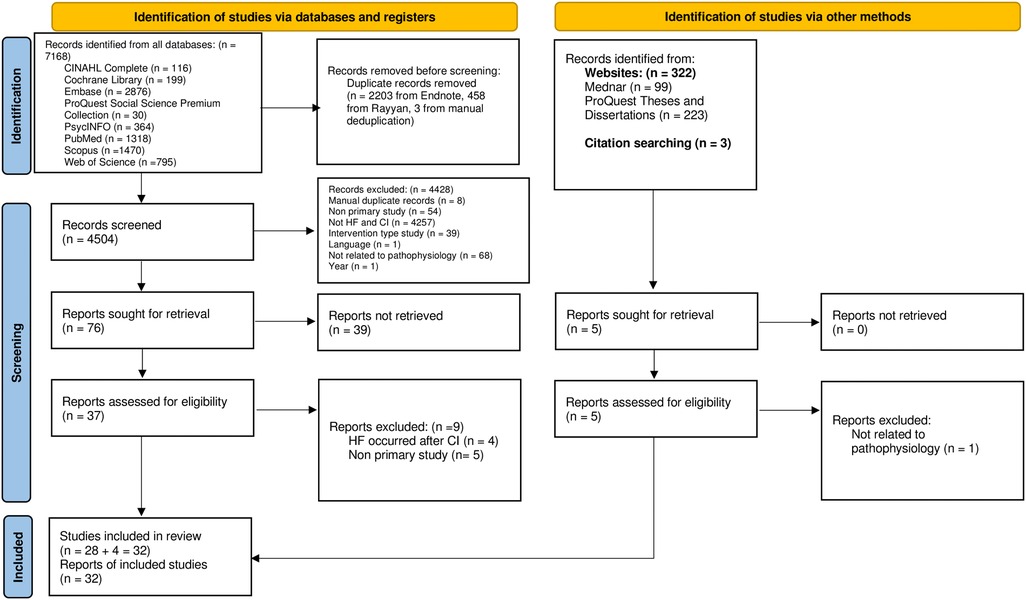
Figure 1. PRISMA chart.
The study characteristics are described in Tables 2–5. The study sizes ranged from 37 to 939 for human and nine to 209 for animal studies. The age ranged from 51.4 to 85 years for human and 10 weeks to 10 months for animal studies, with almost all studies reporting in mean and standard deviation. All human studies had more males than females except one cohort study measuring NT-proBNP. Likewise, seven animal studies had male models or more males compared to three with female models or more females involved (19). For human studies, nine studies indicated the type of HF recruited, with the majority being chronic HF (n = 9). More studies had non-ischemic causes of HF as opposed to ischemic causes. Some studies included the EF, with a few of them mentioning the mean only whilst the rest mentioning the percentage of HFrEF and HFpEF respectively. Out of those that mentioned the specific type of EF, most of them included more HFrEF than HFpEF, except one study that included more HFpEF instead. The NYHA class were mostly class II with 14 studies, followed by class III with 13 studies and classes I and IV with six studies each. Most studies recruited HF patients in more than one NYHA class, except one that only included class II. Seven studies did not limit the class type. For the case-control human studies, seven studies included healthy controls. Meanwhile, for animal studies, sham groups were used more often than control groups. One human study investigated different illnesses besides HF, namely vascular cognitive impairment (VCI) and carotid occlusive disease (COD), but still focused on HF hence it was included (20). The studies were grouped into three main themes—CI due to changes in the brain in HF: brain atrophy, alterations in GM and WM, cerebral alterations, pathway or axis changes, neuroinflammation and hippocampal gene changes; CI due to changes in the heart or systemic circulation in HF: inflammation, oxidative stress and changes in serum biomarkers or proteins and the riser rhythm; CI due to changes in both the brain and the heart in HF: combination of mechanisms from the previous two sections, with six studies obtaining negative results. The last study with negative results revealed the lack of relationship between AD and HF.
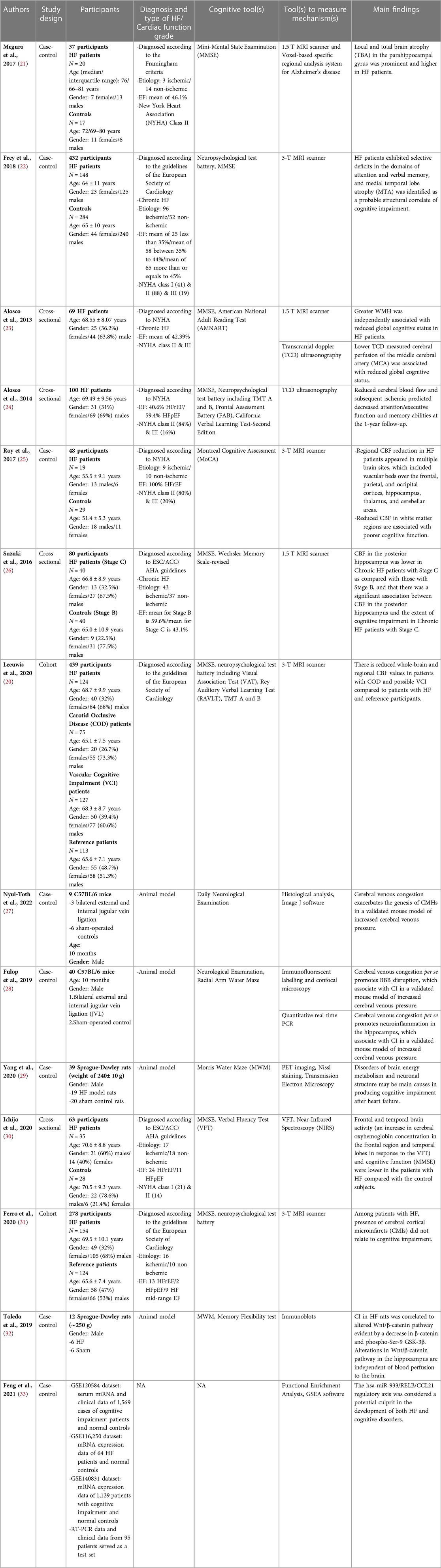
Table 2. CI due to changes in the brain in HF.
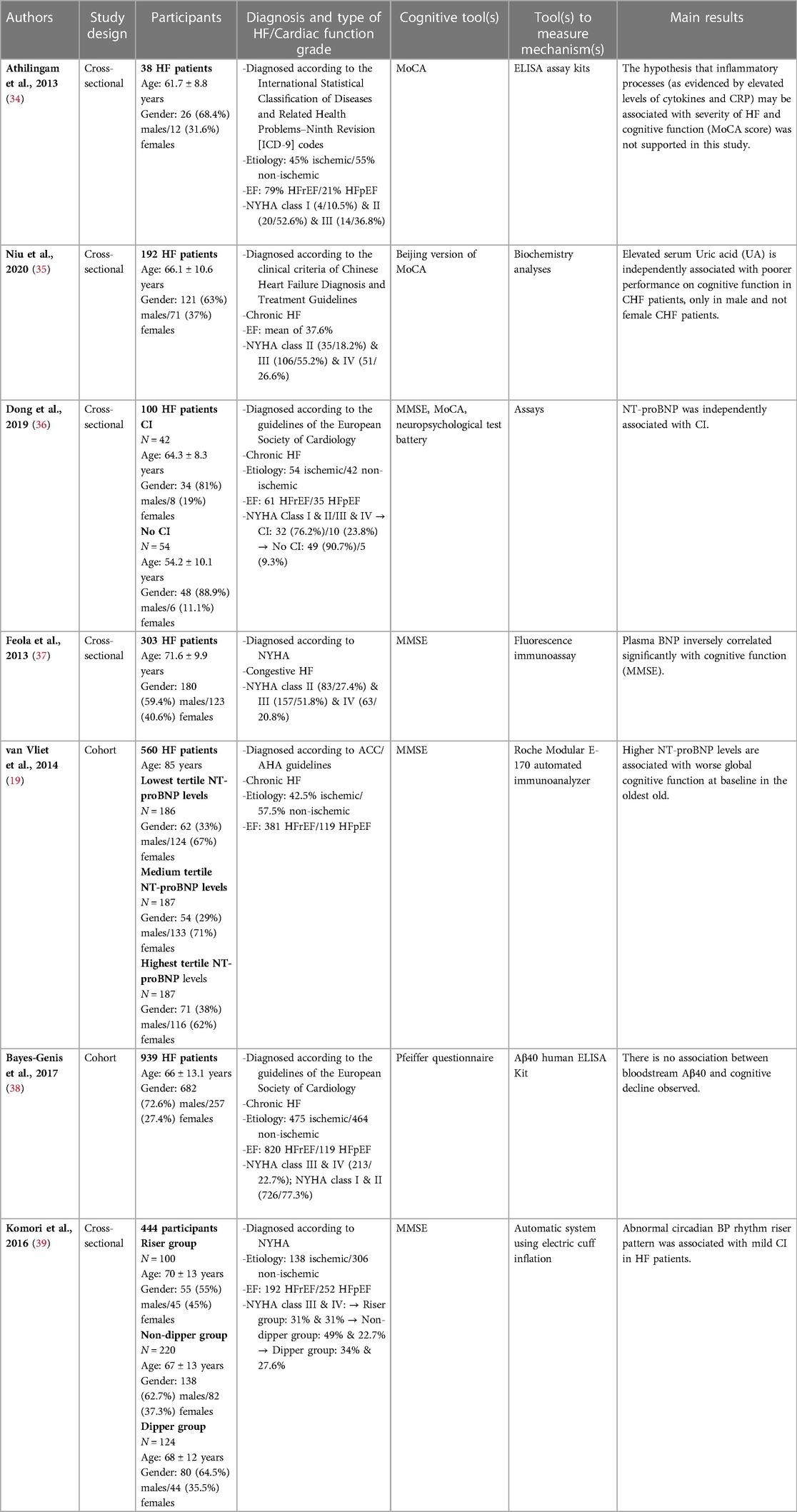
Table 3. CI due to changes in the heart or systemic circulation in HF.
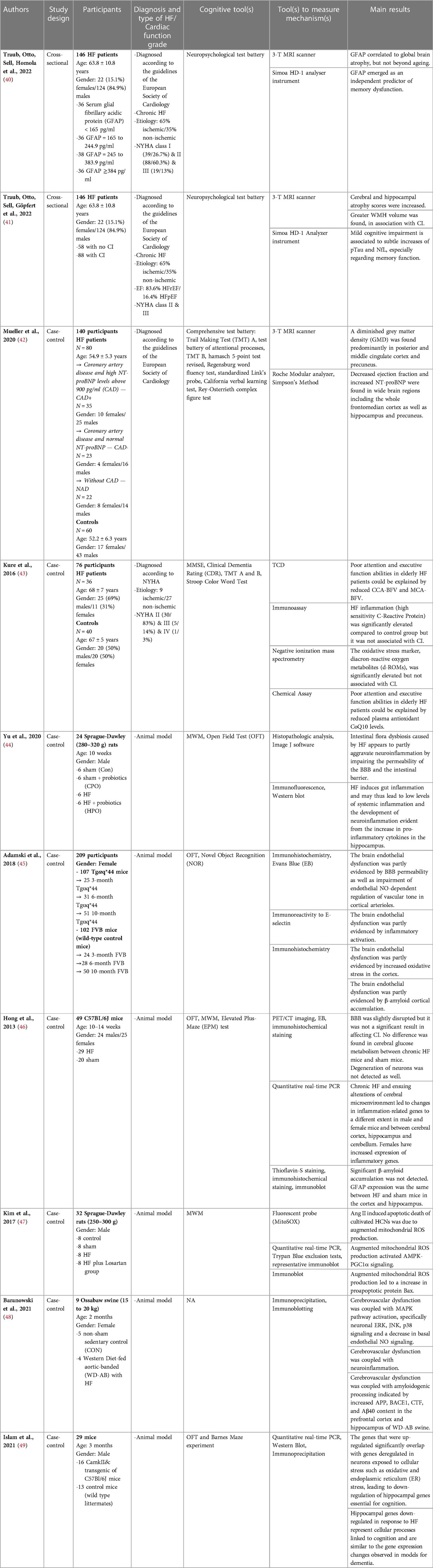
Table 4. CI due to changes in both the brain and the heart in HF.
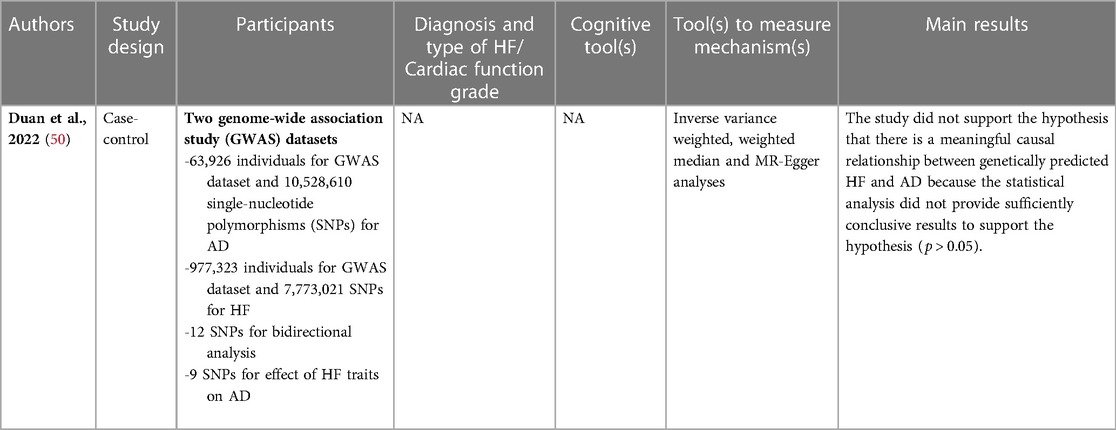
Table 5. Relationship between AD and HF.
This review included 32 studies—17 case-control, 11 cross-sectional and four cohort. The summarized appraisal is shown in Supplementary Appendix S6. The results were decided by two reviewers (RS and HQ). All the studies were eventually included though there were studies that had some “No” and “Unclear”, indicating compromised quality. For case-control studies, three studies had no “No” or “Unclear”. The remaining studies had 0–4 “Unclear” and 0–2 “No”, but all studies had minimally six “Yes” out of 10 questions. For cross-sectional studies, three studies had no “No” or “Unclear”. The remaining studies had 0–2 “Unclear” and 0–2 “No”, with all studies having minimally five “Yes” out of eight questions. For cohort studies, all studies had 1–4 “Unclear” and 0–2 “No”, with minimally five “Yes” out of 11 questions.
Two studies reported on the relationship between CI and brain atrophy. These studies are illustrated in Table 2. One study illustrated local and total brain atrophy (TBA) in the parahippocampal gyrus of HF patients as compared to the controls. Though the severity of TBA was similar between HF and control group, the averaged Z-score which measured the severity of atrophy in parahippocampal gyrus was much higher in HF than control group (21). The other study illustrated more severe MTA and worse attention and memory in HF compared to control group (22). Both utilized magnetic resonance imaging (MRI) to demonstrate the atrophy.
One study reported on the relationship between CI and GM and WM changes, specifically increased white matter hyperintensities (WMH) (23). It is illustrated in Table 2. Besides the use of MRI, it utilized the Transcranial Doppler (TCD) which allow effective measuring of perfusion. The mean EF was 42.39% which is a mid-range EF, suggesting that of the inclusion of HF with both HFrEF and HFpEF participants.
10 studies reported on the relationship between CI and cerebral changes. These studies are illustrated in Table 2. Five studies illustrated the relationship between CI and CBF, albeit in different regions. One study reported that reduced CBF velocity (CBFV) of middle cerebral artery (MCA) was related to increased WMH and as aforementioned, increased WMH was related to poorer cognitive function (23). Another study reported reduced CBFV in the posterior cerebral artery (PCA) and middle cerebral artery after a year of follow-up (24). One study reported reduced CBF over the frontal, parietal, and occipital cortices, hippocampus, thalamus, and cerebellar area, with more decline on the right side in cortical and diencephalic areas, indicating laterality in CBF reduction. It was the only study that included fully HFrEF, which might thus illustrate reduced CBF is one of the more definite causes of CI in HF (25). The above three studies all involved NYHA classes II & III. Another study reported reduced CBF in posterior hippocampus for chronic HF participants (26). The last study did not report any association for both whole-brain or regional CBF in HF participants (20). TCD and MRI were the two main tools used to detect CBFV. Two studies illustrated the relationship between CI and cerebral venous congestion. One study reported that cerebral venous congestion led to cerebral microhemorrhages (CMHs) (27) whilst the other stated it caused blood-brain barrier (BBB) disruption instead, leading to CI (28). One study reported that issues with glucose metabolism and structure of neurons contributed to CI (29). The above three studies were all animal models. One other study reported increase in frontal and temporal brain activity, particularly increase in oxyhemoglobin concentration, contributed to CI. There were more participants with non-ischemic causes of HF and HFrEF, it focused more on NYHA classes I and II as well (30). One study reported no association between CI and cerebral cortical microinfarcts (CMI), despite including participants with both ischemic and non-ischemic causes of HF and all ranges of EF (31).
Two studies reported on the relationship between CI and pathway or axis changes. These studies are illustrated in Table 2. One study reported the changes in Wnt/β-catenin pathway in the hippocampus as a contributor (32), whilst the other reported the hsa-miR-933/RELB/CCL21 axis as another contributor (33). They were both case-control studies though one utilized an animal model while the othere was using datasets.
One study reported on the relationship between CI and neuroinflammation, specifically evident from increased pro-inflammatory cytokines found in the hippocampus of the animal model (28). It is illustrated in Table 2.
One study reported the lack of association between inflammation and CI, despite including participants with both ischemic and non-ischemic causes of HF, all ranges of EF and almost all classes of NYHA. This was the only study that was diagnosed using the International Statistical Classification of Diseases and Related Health Problems–Ninth Revision (34). It is illustrated in Table 3.
Five studies reported on the relationship between CI and biomarkers or proteins. These studies are illustrated in Table 3. One study reported that increased uric acid (UA) was related to poorer cognition only in male patients. This was the only study that utilized the Beijing version of MoCA and was diagnosed using the Chinese Heart Failure Diagnosis and Treatment Guidelines. It focused on chronic HF but included all forms of etiology of HF and had a mean of 37.6% EF, meaning that most participants were of HFrEF (35). Three studies reported higher NT-proBNP was associated with CI (19, 36, 37). Two studies focused on chronic HF, with one on congestive HF. All three studies included more HFrEF participants and used MMSE as one of the tools to measure cognitive function. One study reported no association between Aβ40 and CI. It included more participants with ischemic etiology, HFrEF and all classes of NYHA. It is the only study to utilize the Pfeiffer questionnaire for cognitive function (38).
One study reported irregular circadian blood pressure (BP) rhythm being related to MCI. it included more participants with non-ichemic etiology and HFpEF (39). It is illustrated in Table 3. It is a relatively specific mechanism, being the only study that discussed about this. Hence, it requires further research to validate it.
10 studies reported varying mechanisms involving both the brain and the heart or systemic circulation. Some of the major mechanisms have been mentioned previously, with oxidative stress and hippocampal gene changes being new ones. These are illustrated in Table 4. Four studies were human studies with the remaining six being animal models. The first study illustrated increase in global cerebral atrophy scores in relation to serum glial fibrillary acidic protein (GFAP), which were independently associated with CI (40).
The second study reported increased cerebral and hippocampal atrophy scores. It also illustrated increased WMH, phosphorylated Tau protein (pTau) and neurofilament light chain (NfL), which are key biomarkers of AD (41). These two studies focused on chronic HF, with more participants having ischemic etiology. They both used MRI and the Simoa Analyzer instrument as tools for cognitive function.
The third study reported reduced GM density in specific regions. Additionally, there was reduced EF and increased NT-proBNP in the cortex, hippocampus and precuneus. These were linked to CI (42). The above three studies utilized MRI as a tool for measuring cognitive function.
The fourth study reported that out of the four main outcomes, two were shown to contribute to CI — reduced CBF in middle cerebral artery and common carotid artery (CCA) and reduced antioxidant CoQ10. For the other two outcomes, despite illustrating increase in both oxidative stress and inflammatory markers such as C-Reactive Protein, they were not associated with CI (43)..
The fifth study reported that impaired blood-brain barrier permeability was due to intestinal flora dysbiosis. The gut inflammation led to neuroinflammation as well, evident from increased pro-inflammatory cytokines in the hippocampus. These were contributors to CI (44).
The sixth study reported that four different causes, namely oxidative stress, β-amyloid accumulation, impaired endothelial NO-dependent regulation and inflammation caused endothelial damage, which was linked to CI (45).
The seventh study reported neuroinflammation as a contributor, albeit difference found between gender and brain regions. However, there was slight but insignificant disruption of blood-brain barrier, with glucose metabolism and degeneration of neurons not being contributors of CI. β-amyloid accumulation was not found and GFAP did not contribute to CI as well (46).
The eighth study reported that Angiotensin II induced apoptosis of hippocampal neural stem cells (HCNs) was caused by AMPK-PGC1α signaling. This was due to the increase in reactive oxygen species (ROS) which led to concomitant increase of pro-apoptotic Bax protein (47).
The ninth study reported the activation of MAPK pathway and reduced NO signaling as contributors to CI. Other contributors include amyloidogenic processing and thus increased β-amyloid in the prefrontal cortex and hippocampus and neuroinflammation evident from increased ERK, JNK and p38 (48).
The last study reported that hippocampal gene changes led to down-regulation of genes responsible for cognition, which were similar to those observed in animal models with dementia. This was caused by cellular stress such as oxidative and endoplasmic reticulum stress (49).
One study reported a lack of association between HF and AD, due to lack of conclusive statistical analysis results (50). This is illustrated in Table 5. It is a case-control study that utilized datasets, similar to another study mentioned previously.
With the aim of summarizing the best available evidence concerning different pathophysiological mechanisms behind CI in individuals with Heart Failure, three main themes—CI due to changes in the brain: brain atrophy, alterations in GM and WM, cerebral alterations, pathway or axis changes, neuroinflammation and hippocampal gene changes; CI due to changes in the heart or systemic circulation: inflammation, oxidative stress and changes in serum biomarkers or proteins and the riser rhythm; CI due to changes in both the brain and the heart: combination of some mechanisms from the previous two sections, were identified. Our findings corroborated with both Jiang et al. (10) and Ampadu and Morley (11) as 11 different studies discussed about the same findings in terms of changes in the brain—brain atrophy, changes in GM and WM and decreased CBF. One study produced negative results in terms of atrophy. Possible reasons include some participants using anti-hypertensive medications which might affect the CBF and the delay in transit time during the usage of arterial spin labeling technique. It did not include all potential confounders as well (20). Four studies discussed about NT-proBNP, like Jiang et al. (10). Akin to Ampadu and Morley (11), 10 studies mentioned about oxidative stress, infarcts, and inflammatory cytokines. Ferro et al. (31) concluded that cerebral cortical microinfarcts had no influence on CI, which could be explained by the recruitment of clinically stable HF patients only. Kure et al. (43) concluded that both inflammation and oxidative stress were not statistically significant, possibly due to the small sample size of 36 HF patients, milder HF as 83% were NYHA class II and the exclusion of demented individuals based on MMSE scores. Athilingam et al. (34) proposed negative results on inflammation, possibly due to recruitment of stable HF patients. Being a pilot and cross-sectional study, it might not delineate the causal association well and there was no reference group. Nevertheless, there were new mechanisms that surfaced, such as pathways, genes, antioxidant, electrolyte and protein changes, blood-brain barrier and glucose metabolism issues. Three other reviews done previously had similar findings regarding reduced CBF and inflammation, with Toledo & Andrade et al. (51) discussing about oxidative stress and Wnt signaling as well, Xu et al. (52) on oxidative stress, GFAP and β-amyloid and Goh et al. (53) on atrophy, GM and WM changes. Some of these mechanisms are interlinked and the summary is demonstrated in Figure 2. The yellow coded boxes illustrate the initial causes of CI, with the orange coded boxes being the linkages leading to the green coded CI. Despite the presence of many causes, many pathways are eventually linked to neuroinflammation, oxidative stress, atrophy and increase in β-amyloid.
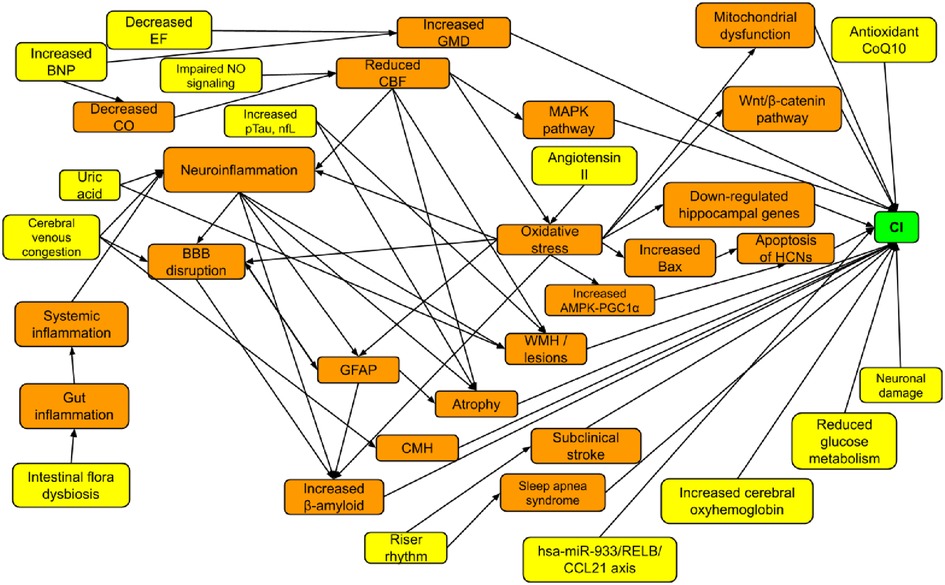
Figure 2. Summarized pathophysiological mechanisms.
Besides the aforementioned studies, there were three more studies with negative results. Hong et al. (46) concluded that GFAP, β-amyloid, blood-brain barrier, glucose metabolism and neurodegeneration were insignificant in contributing to CI. This might be attributed to it being an animal study and modeling of mice with myocardial infarction and congestive HF, which was a more specific population type. Bayes-genis et al. (38) concluded that Aβ40 was irrelevant in contributing to CI, possibly due to the usage of a less common cognitive tool—Pfeiffer questionnaire and the loss of nearly half the participants due to death, albeit the study focusing on mortality as an outcome as well. Duan et al. (50) concluded that there was no association between AD and HF, possibly due to restricting to European populations and lack of test set to evaluate the model objectively.
There are both strengths and limitations to this review. For the strengths, they include having two reviewers which helped to reduce inclusion bias. The results were more updated than previous systematic reviews and included grey literature to minimize publication bias, which was lacking in previous systematic reviews. Studies with contradictory results were included to ensure fair representation instead of purely portraying one side and minimized selection bias. Additionally, eight databases were utilized, ensuring more comprehensive search results. There were more variety of study types instead of mostly cross-sectional ones by Jiang et al. (10). For the limitations, this review included non-human studies which might not be fully replicable of the human system and thus there might be information bias. More than a quarter of the studies were cross-sectional hence the causal relationship might not be identifiable and observational studies in general, might bring about more confounders. Additionally, only English and Chinese language publications were included due to reviewers’ inability to understand other languages, leading to publication bias, albeit only one exclusion due to language. A few of the included studies had compromised quality based on the quality appraisal performed, which made the study results less credible.
These findings will be important in informing the healthcare staff on better ways to deal with this comorbidity of HF and to put more focus on it by monitoring and advising HF patients about it. Moving on, more brain imaging can be performed in HF patients as numerous mechanisms involve the changes in CBF and brain structure such as atrophy, amyloid plaques and apoptosis of cells etc. In conjunction with brain imaging, standardized cognitive screening tools can be used as well for more accurate and prompt diagnosis and management plans to be conceived. There are currently many varying tools whereby some may be less effective in the detection of potential CI. Routine blood samplings may involve the testing of significant biomarkers such as UA, NT-proBNP, CRP, phosphorylated Tau protein and ROS metabolites etc. This was noted in Ampadu and Morley (11) as well that there should be screenings to check for CI and rise in NT-proBNP. These increase the probability of noticing any cognitive changes before they develop to irreversible cognitive impairments as these are not checked for routinely. Timely interventions can then be put in place after recognizing the signs of disease progression to prevent further deterioration.
The studies included varying NYHA classes—NYHA classes I to IV. Most of the studies included classes II and III which are the more moderate HF classes. Hence, the pathophysiological mechanisms summarized may be more relevant to those with moderate severity of HF as opposed to the extreme ends. The studies did not specifically illustrate the mechanisms for different classes but discussed as a whole. Most studies included more HFrEF participants, which might suggest that the mechanisms are more relevant to this form of HF. Nevertheless, as the studies still varied in terms of other aspects such as diagnostic tool or etiology or class of HF etc, there were no obvious linkages between these differences and the different pathophysiological mechanisms proposed. Hence, this can be explored further for future studies, to determine the precise mechanisms for different groups of HF participants. More research must be performed to determine suitable tools and treatments for different severity of HF and thus, different severity of CI.
Additionally, an estimated 3.4%–6.7% of hospitalized patients have HF in Asia and around one million people have HF in Japan. HF patients in Asia are mostly younger than in Western countries. However, the youngest in this review was 51.4 years old, thus there was no focus on the younger population per se. Hence, future studies can focus on them to determine if there are any differences in the mechanisms depending on age. Thereafter, different tools can be utilized to detect the mechanisms at different ages. In the elderly population, HF conditions are more likely to reduce appetite, decrease muscle mass and physical activity, resulting in malnutrition, frailty and poorer prognosis of HF (54). Groenewegen et al. (3) purported that compared to men, women have lower incidence of HF, albeit them still occupying around half of the prevalent cases. HFpEF is more prevalent in women as they are often more obese than men. In terms of CI, Hong et al. (46) reported worse outcomes in females. However, Niu et al. (35) reported otherwise—increased UA affected only males' cognition.
Future primary research can continue to validate and postulate further pathophysiological mechanisms, especially on those that had contradictory results, albeit being the minority. Understanding the pathophysiology of diseases will allow the effective evaluation of health status and development of suitable treatments and plans (9). Furthermore, the mechanisms are mostly interlinked, hence realizing these linkages can help to prevent further advancement and thereafter deterioration of CI in HF individuals.
In conclusion, from 32 studies, it is evident that HF and CI are interlinked through the various mechanisms, in terms of changes in the brain and or heart. Future primary research can continue to validate and postulate further pathophysiological mechanisms, especially on those that had contradictory results, albeit being the minority. Larger longitudinal studies will better describe the causal relationship and development of CI in HF, potentially leading to more discovery. Being aware of the pathophysiological mechanisms allows for more pharmacological and non-pharmacological methods to be established by stopping the mechanisms etc., instead of focusing solely on certain treatments such as cardiac rehabilitation. Medications can be created to hinder the mechanisms directly which is more effective than slowing down the cognitive impairments via the overt symptoms. Moreover, prompt detection of CI will bring about better clinical outcomes in HF patients.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
RSNS designed and conceptualized the manuscript, with the help of YD. RSNS searched the databases, screened, critically appraised and extracted the data of included studies, with HQMR as the other independent reviewer. RSNS wrote the manuscript, with YD reviewing the manuscript critically. All authors contributed to the article and approved the submitted version.
YD is supported by Singapore NMRC Transition Award (NMRC/TA/0060/2017).
The authors would like to acknowledge the editing support from Ms Xinyao Wu and Mr Kang Wei Wong.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fcvm.2023.1181979/full#supplementary-material.
Supplementary Table 1
PRISMA checklist.
Supplementary Table 2
Search strategy.
Supplementary Table 3
Screening tool.
Supplementary Table 4
Critical appraisal checklists.
Supplementary Table 5
Data extraction forms.
Supplementary Table 6
Summary of quality appraisal.
1. Simmonds SJ, Cuijpers I, Heymans S, Jones EAV. Cellular and molecular differences between HFpEF and HFrEF: a step ahead in an improved pathological understanding. Cells. (2020) 9(1):242. doi: 10.3390/cells9010242
2. Inamdar A, Inamdar A. Heart failure: diagnosis, management and utilization. J Clin Med. (2016) 5(7):62. doi: 10.3390/jcm5070062
3. Groenewegen A, Rutten FH, Mosterd A, Hoes AW. Epidemiology of heart failure. Eur J Heart Fail. (2020) 22(8):1342–56. doi: 10.1002/ejhf.1858
4. Streng KW, Nauta JF, Hillege HL, Anker SD, Cleland JG, Dickstein K, et al. Non-cardiac comorbidities in heart failure with reduced, mid-range and preserved ejection fraction. Int J Cardiol. (2018) 271:132–9. doi: 10.1016/j.ijcard.2018.04.001
5. Yang MX, Sun D, Wang Y, Yan MW, Zheng JA, Ren JY. Cognitive impairment in heart failure: landscape, challenges, and future directions. Front Cardiovasc Med. (2022) 8:2–4. doi: 10.3389/fcvm.2021.831734
6. Pais R, Ruano LP, Carvalho O, Barros H. Global cognitive impairment prevalence and incidence in community dwelling older adults—a systematic review. Geriatrics. (2020) 5(4):84. doi: 10.3390/geriatrics5040084
7. Eshkoor SA, Hamid TA, Mun CY, Ng CK. Mild cognitive impairment and its management older people. Clin Interv Aging. (2015) 10:687–93. doi: 10.2147/CIA.S73922
8. Pan C-W, Wang X, Ma Q, Sun H-P, Xu Y, Wang P. Cognitive dysfunction and health-related quality of life among older Chinese. Sci Rep. (2015) 5(1):17301. doi: 10.1038/srep17301
9. Witthöft M. Pathophysiology. In: Gellman MD, Turner JR, editors. Encyclopedia of behavioral medicine. New York, NY: Springer New York (2013). p. 1443–5.
10. Jiang Y, Wang L, Lu Z, Chen S, Teng Y, Li T, et al. Brain imaging changes and related risk factors of cognitive impairment in patients with heart failure. Front Cardiovasc Med. (2022) 8:838680. doi: 10.3389/fcvm.2021.838680
11. Ampadu J, Morley JE. Heart failure and cognitive dysfunction. Int J Cardiol. (2015) 178:12–23. doi: 10.1016/j.ijcard.2014.10.087
12. Moola S, Munn Z, Tufanaru C, Aromataris E, Sears K, Sfetc R, et al. Chapter 7: systematic reviews of etiology and risk. JBI. (2020). doi: 10.46658/JBIMES-20-08
13. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Br Med J. (2021) 372:n71. doi: 10.1136/bmj.n71
14. Barré-Sinoussi F, Montagutelli X. Animal models are essential to biological research: issues and perspectives. Future Sci OA. (2015) 1(4). doi: 10.4155/fso.15.63
15. EndNote. EndNote. https://endnote.com/ (Accessed September 19, 2022).
16. Ouzzani M, Hammady H, Fedorowicz Z, Elmagarmid A. Rayyan—a web and mobile app for systematic reviews. Syst Rev. (2016) 5(1):3. doi: 10.1186/s13643-016-0384-4
17. JBI. Critical Appraisal Tools. https://jbi.global/critical-appraisal-tools (Accessed September 18, 2022).
18. Moola S, Munn Z, Sears K, Sfetcu R, Currie M, Lisy K, et al. Conducting systematic reviews of association (etiology): the joanna briggs institute’s approach. JBI Evid Implement. (2015) 13(3):163–9. doi: 10.1097/xeb.0000000000000064
19. van Vliet P, Sabayan B, Wijsman LW, Poortvliet RK, Mooijaart SP, de Ruijter W, et al. NT-proBNP, blood pressure, and cognitive decline in the oldest old: the Leiden 85-plus study. Neurology. (2014) 83(13):1192–9. doi: 10.1212/wnl.0000000000000820
20. Leeuwis AE, Hooghiemstra AM, Bron EE, Kuipers S, Oudeman EA, Kalay T, et al. Cerebral blood flow and cognitive functioning in patients with disorders along the heart–brain axis: cerebral blood flow and the heart–brain axis. Alzheimers Dement. (2020) 6(1):e12034. doi: 10.1002/trc2.12034
21. Meguro T, Meguro Y, Kunieda T. Atrophy of the parahippocampal gyrus is prominent in heart failure patients without dementia. ESC Heart Fail. (2017) 4(4):632–40. doi: 10.1002/ehf2.12192
22. Frey A, Sell R, Homola GA, Malsch C, Kraft P, Gunreben I, et al. Cognitive deficits and related brain lesions in patients with chronic heart failure. JACC Heart Fail. (2018) 6(7):583–92. doi: 10.1016/j.jchf.2018.03.010
23. Alosco ML, Brickman AM, Spitznagel MB, Garcia SL, Narkhede A, Griffith EY, et al. Cerebral perfusion is associated with white matter hyperintensities in older adults with heart failure. Congest Heart Fail. (2013) 19(4):E29–34. doi: 10.1111/chf.12025
24. Alosco ML, Spitznagel MB, Cohen R, Raz N, Sweet LH, Josephson R, et al. Reduced cerebral perfusion predicts greater depressive symptoms and cognitive dysfunction at a 1-year follow-up in patients with heart failure. Int J Geriatr Psychiatry. (2014) 29(4):428–36. doi: 10.1002/gps.4023
25. Roy B, Woo MA, Wang DJJ, Fonarow GC, Harper RM, Kumar R. Reduced regional cerebral blood flow in patients with heart failure. Eur J Heart Fail. (2017) 19(10):1294–302. doi: 10.1002/ejhf.874
26. Suzuki H, Matsumoto Y, Ota H, Sugimura K, Takahashi J, Ito K, et al. Hippocampal blood flow abnormality associated with depressive symptoms and cognitive impairment in patients with chronic heart failure. Circ J. (2016) 80(8):1773–80. doi: 10.1253/circj.CJ-16-0367
27. Nyul-Toth A, Fulop GA, Tarantini S, Kiss T, Ahire C, Faakye JA, et al. Cerebral venous congestion exacerbates cerebral microhemorrhages in mice. Geroscience. (2022) 44(2):805–16. doi: 10.1007/s11357-021-00504-0
28. Fulop GA, Ahire C, Csipo T, Tarantini S, Kiss T, Balasubramanian P, et al. Cerebral venous congestion promotes blood-brain barrier disruption and neuroinflammation, impairing cognitive function in mice. Geroscience. (2019) 41(5):575–89. doi: 10.1007/s11357-019-00110-1
29. Yang T, Lu Z, Wang L, Zhao Y, Nie B, Xu Q, et al. Dynamic changes in brain glucose metabolism and neuronal structure in rats with heart failure. Neuroscience. (2020) 424:34–44. doi: 10.1016/j.neuroscience.2019.10.008
30. Ichijo Y, Kono S, Yoshihisa A, Misaka T, Kaneshiro T, Oikawa M, et al. Impaired frontal brain activity in patients with heart failure assessed by near-infrared spectroscopy. J Am Heart Assoc. (2020) 9(3):e014564. doi: 10.1161/jaha.119.014564
31. Ferro D, van den Brink H, Amier R, van Buchem M, de Bresser J, Bron E, et al. Cerebral cortical microinfarcts: a novel MRI marker of vascular brain injury in patients with heart failure. Int J Cardiol. (2020) 310:96–102. doi: 10.1016/j.ijcard.2020.04.032
32. Toledo C, Lucero C, Andrade DC, Díaz HS, Schwarz KG, Pereyra KV, et al. Cognitive impairment in heart failure is associated with altered Wnt signaling in the hippocampus. Aging (Albany NY). (2019) 11(16):5924–42. doi: 10.18632/aging.102150
33. Feng W, Yang J, Song W, Xue Y. Crosstalk between heart failure and cognitive impairment via hsa-miR-933/RELB/CCL21 pathway. BioMed Res Int. (2021) 2021:2291899. doi: 10.1155/2021/2291899
34. Athilingam P, Moynihan J, Chen L, D’Aoust R, Groer M, Kip K. Elevated levels of interleukin 6 and C-reactive protein associated with cognitive impairment in heart failure. Congest Heart Fail. (2013) 19(2):92–8. doi: 10.1111/chf.12007
35. Niu W, Yang H, Lu C. The relationship between serum uric acid and cognitive function in patients with chronic heart failure. BMC Cardiovasc Disord. (2020) 20(1):381. doi: 10.1186/s12872-020-01666-z
36. Dong Y, Teo SY, Kang K, Tan M, Ling LH, Yeo PSD, et al. Cognitive impairment in Asian patients with heart failure: prevalence, biomarkers, clinical correlates, and outcomes. Eur J Heart Fail. (2019) 21(5):688–90. doi: 10.1002/ejhf.1442
37. Feola M, Garnero S, Vallauri P, Salvatico L, Vado A, Leto L, et al. Relationship between cognitive function, depression/anxiety and functional parameters in patients admitted for congestive heart failure. Open Cardiovasc Med J. (2013) 7:54–60. doi: 10.2174/1874192401307010054
38. Bayes-Genis A, Barallat J, de Antonio M, Domingo M, Zamora E, Vila J, et al. Bloodstream amyloid-beta (1-40) peptide, cognition, and outcomes in heart failure. Rev Esp Cardiol. (2017) 70(11):924–32. doi: 10.1016/j.rec.2017.02.021
39. Komori T, Eguchi K, Saito T, Nishimura Y, Hoshide S, Kario K. Riser blood pressure pattern is associated with mild cognitive impairment in heart failure patients. Am J Hypertens. (2016) 29(2):194–201. doi: 10.1093/ajh/hpv086
40. Traub J, Otto M, Sell R, Homola GA, Steinacker P, Oeckl P, et al. Serum glial fibrillary acidic protein indicates memory impairment in patients with chronic heart failure. ESC Heart Fail. (2022) 9(4):2626–34. doi: 10.1002/ehf2.13986
41. Traub J, Otto M, Sell R, Göpfert D, Homola G, Steinacker P, et al. Serum phosphorylated tau protein 181 and neurofilament light chain in cognitively impaired heart failure patients. Alzheimers Res Ther. (2022) 14(1):149. doi: 10.1186/s13195-022-01087-4
42. Mueller K, Thiel F, Beutner F, Teren A, Frisch S, Ballarini T, et al. Brain damage with heart failure: cardiac biomarker alterations and gray matter decline. Circ Res. (2020) 126(6):750–64. doi: 10.1161/circresaha.119.315813
43. Kure CE, Rosenfeldt FL, Scholey AB, Pipingas A, Kaye DM, Bergin PJ, et al. Relationships among cognitive function and cerebral blood flow, oxidative stress, and inflammation in older heart failure patients. J Card Fail. (2016) 22(7):548–59. doi: 10.1016/j.cardfail.2016.03.006
44. Yu W, Gao DP, Jin W, Wang ZJ, Li Y, Peng XW, et al. Intestinal flora dysbiosis aggravates cognitive dysfunction associated with neuroinflammation in heart failure. J Card Fail. (2020) 26(10):885–94. doi: 10.1016/j.cardfail.2020.02.002
45. Adamski MG, Sternak M, Mohaissen T, Kaczor D, Wierońska JM, Malinowska M, et al. Vascular cognitive impairment linked to brain endothelium inflammation in early stages of heart failure in mice. J Am Heart Assoc. (2018) 7(7):3–17. doi: 10.1161/JAHA.117.007694
46. Hong X, Bu L, Wang Y, Xu J, Wu J, Huang Y, et al. Increases in the risk of cognitive impairment and alterations of cerebral beta-amyloid metabolism in mouse model of heart failure. PLoS ONE. (2013) 8(5):e63829. doi: 10.1371/journal.pone.0063829
47. Kim MS, Lee GH, Kim YM, Lee BW, Nam HY, Sim UC, et al. Angiotensin II causes apoptosis of adult hippocampal neural stem cells and memory impairment through the action on AMPK-PGC1 alpha signaling in heart failure. Stem Cells Transl Med. (2017) 6(6):1491–503. doi: 10.1002/sctm.16-0382
48. Baranowski BJ, Allen MD, Nyarko JN, Rector RS, Padilla J, Mousseau DD, et al. Cerebrovascular insufficiency and amyloidogenic signaling in Ossabaw swine with cardiometabolic heart failure. JCI Insight. (2021) 6(10):2–11. doi: 10.1172/jci.insight.143141
49. Islam MR, Lbik D, Sakib MS, Maximilian Hofmann R, Berulava T, Jiménez Mausbach M, et al. Epigenetic gene expression links heart failure to memory impairment. EMBO Mol Med. (2021) 13(3):e11900. doi: 10.15252/emmm.201911900
50. Duan CL, Shi JJ, Yuan GZ, Shou XT, Chen T, Zhu XP, et al. Causal association between heart failure and Alzheimer’s disease: a two-sample bidirectional mendelian randomization study. Front Genet. (2022) 12:3–5. doi: 10.3389/fgene.2021.772343
51. Toledo C, Andrade DC, Díaz HS, Inestrosa NC, Del Rio R. Neurocognitive disorders in heart failure: novel pathophysiological mechanisms underpinning memory loss and learning impairment. Mol Neurobiol. (2019) 56(12):8035–51. doi: 10.1007/s12035-019-01655-0
52. Xu C, Tao X, Ma X, Zhao R, Cao Z. Cognitive dysfunction after heart disease: a manifestation of the heart-brain axis. Oxid Med Cell Longevity. (2021) 2021:4899688. doi: 10.1155/2021/4899688
53. Goh FQ, Kong WKF, Wong RCC, Chong YF, Chew NWS, Yeo TC, et al. Cognitive impairment in heart failure-A review. Biology (Basel). (2022) 11(2):179. doi: 10.3390/biology11020179
Keywords: heart failure, cognitive impairment, pathophysiology, systematic review, dementia
Citation: Sam RSN, Mohamed Raffi HQ and Dong Y (2023) The pathophysiology of cognitive impairment in individuals with heart failure: a systematic review. Front. Cardiovasc. Med. 10:1181979. doi: 10.3389/fcvm.2023.1181979
Received: 8 March 2023; Accepted: 28 April 2023;
Published: 23 May 2023.
Edited by:
Constantina Aggeli, National and Kapodistrian University of Athens, GreeceReviewed by:
Maria Kariori, Hippokration General Hospital, Greece© 2023 Sam, Mohamed Raffi and Dong. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yanhong Dong bnVyZHlAbnVzLmVkdS5zZw==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.