
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
CLINICAL TRIAL article
Front. Cardiovasc. Med., 05 September 2023
Sec. Heart Failure and Transplantation
Volume 10 - 2023 | https://doi.org/10.3389/fcvm.2023.1167738
This article is part of the Research TopicPathophysiological and Clinical Insights for Atrial Fibrillation/Flutter or Heart Failure, Volume IIView all 8 articles
 Miloud Cherbi1,2
Miloud Cherbi1,2 Eric Bonnefoy3Nicolas Lamblin4
Eric Bonnefoy3Nicolas Lamblin4 Edouard Gerbaud5,6Laurent Bonello7,8,9
Edouard Gerbaud5,6Laurent Bonello7,8,9 François Roubille10Bruno Levy11Sebastien Champion12Pascal Lim13,14
François Roubille10Bruno Levy11Sebastien Champion12Pascal Lim13,14 Francis Schneider15Meyer Elbaz1,2Hadi Khachab16
Francis Schneider15Meyer Elbaz1,2Hadi Khachab16 Jeremy Bourenne17Marie-France Seronde18Guillaume Schurtz4Brahim Harbaoui19,20Gerald Vanzetto21
Jeremy Bourenne17Marie-France Seronde18Guillaume Schurtz4Brahim Harbaoui19,20Gerald Vanzetto21 Nicolas Combaret22Vincent Labbe23Benjamin Marchandot24Benoit Lattuca25Caroline Biendel-Picquet1,2Guillaume Leurent26Etienne Puymirat27,28Philippe Maury1,2
Nicolas Combaret22Vincent Labbe23Benjamin Marchandot24Benoit Lattuca25Caroline Biendel-Picquet1,2Guillaume Leurent26Etienne Puymirat27,28Philippe Maury1,2 Clément Delmas1,2,29*
Clément Delmas1,2,29*
Background: Cardiogenic shock (CS) is the most severe form of heart failure (HF), resulting in high early and long-term mortality. Characteristics of CS secondary to supraventricular tachycardia (SVT) are poorly reported. Based on a large registry of unselected CS, we aimed to compare 1-year outcomes between SVT-triggered and non-SVT-triggered CS.
Methods: FRENSHOCK is a French prospective registry including 772 CS patients from 49 centers. For each patient, the investigator could report 1–3 CS triggers from a pre-established list (ischemic, mechanical complications, ventricular/supraventricular arrhythmia, bradycardia, iatrogenesis, infection, non-compliance, and others). In this study, 1-year outcomes [rehospitalizations, mortality, heart transplantation (HTx), ventricular assist devices (VAD)] were analyzed and adjusted for independent predictive factors.
Results: Among 769 CS patients included, 100 were SVT-triggered (13%), of which 65 had SVT as an exclusive trigger (8.5%). SVT-triggered CS patients exhibited a higher proportion of male individuals with a more frequent history of cardiomyopathy or chronic kidney disease and more profound CS (biventricular failure and multiorgan failure). At 1 year, there was no difference in all-cause mortality (43% vs. 45.3%, adjusted HR 0.9 (95% CI 0.59–1.39), p = 0.64), need for HTx or VAD [10% vs. 10%, aOR 0.88 (0.41–1.88), p = 0.74], or rehospitalizations [49.4% vs. 44.4%, aOR 1.24 (0.78–1.98), p = 0.36]. Patients with SVT as an exclusive trigger presented more 1-year rehospitalizations [52.8% vs. 43.3%, aOR 3.74 (1.05–10.5), p = 0.01].
Conclusion: SVT is a frequent trigger of CS alone or in association in more than 10% of miscellaneous CS cases. Although SVT-triggered CS patients were more comorbid with more pre-existing cardiomyopathies and HF incidences, they presented similar rates of mortality, HTx, and VAD at 1 year, arguing for a better overall prognosis.
Clinical Trial Registration: https://clinicaltrials.gov, identifier: NCT02703038.
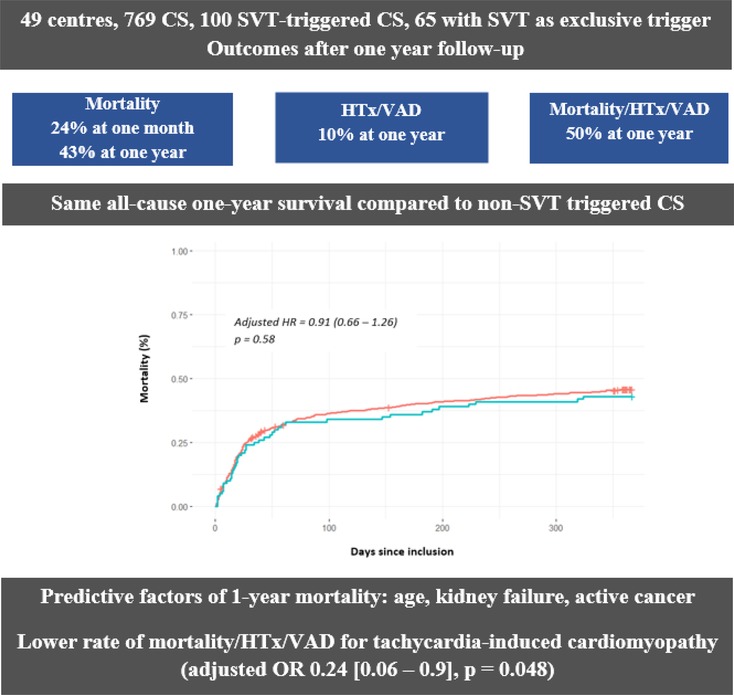
Graphical Abstract. The FRENSHOCK registry—1-year outcomes in cardiogenic shock triggered by supraventricular arrhythmia. CS, cardiogenic shock; HR, hazards ratio; HTx, heart transplantation; OR, odds ratio; SVT, supraventricular tachycardia; VAD, ventricular assist device
Cardiogenic shock (CS) is the most severe form of heart failure (HF), resulting in a life-threatening state of tissue hypoperfusion, which can lead to multiorgan failure and death (1). Despite recent improvements, the mortality rate remains extremely high, close to 50% in 1 year (2), depending on the underlying trigger (3).
The relationship between supraventricular tachycardia (SVT) and HF remains challenging. First, there is strong evidence suggesting that SVT is a poor prognostic factor in cases of chronic HF (4) or acute myocardial infarction (AMI) without CS (5).
Nevertheless, outside the context of CS (6, 7), (1) SVT is considered a negative prognostic marker in patients with altered ejection fraction and (2) the independent effect of SVT on mortality seems inversely related to the severity of HF, suggesting a potential role as a marker of advanced HF. In addition, the prognosis appears less affected for non-ischemic than ischemic heart disease in the case of new onset of SVT (8, 9). On the other hand, there are little available data regarding the short- and long-term outcomes of SVT-triggered CS, especially when it occurs without an acute ischemic trigger.
Hence, this study aimed to compare 1-year outcomes between SVT-triggered CS and non-SVT-triggered CS based on the multicenter prospective FRENSHOCK registry.
As previously reported (10), FRENSHOCK is a prospective, observational, and multicenter registry including 772 patients admitted between April and October 2016 for CS in the intensive care unit (ICU)/intensive cardiac care unit (ICCU) in France, coming from all types of institutions (primary to tertiary centers, university and non-university, and public and private hospitals).
All adult patients (≥18 years old) with CS were prospectively included in this registry if they met at least one criterion of each of the following three components: (1) low cardiac output: low systolic blood pressure (SBP) <90 mmHg, the need for maintenance with vasopressors/inotropes, or a low cardiac index <2.2 L/min/m²; (2) left and/or right heart filling pressure elevation, defined by clinical signs, radiology, blood tests, echocardiography, or signs of invasive hemodynamic overload; and (3) signs of organ malperfusion, which could be clinical (oliguria, confusion, pale and/or cold extremities, mottled skin) or biological (lactate > 2 mmol/L, metabolic acidosis, renal failure, liver insufficiency).
For each patient, the investigator could report 1–3 CS triggers from a pre-established list including ischemic (type 1 or 2 AMI), mechanical complications (valvular injury, ventricular septal defect), ventricular arrhythmia, supraventricular tachycardia, severe bradycardia, iatrogenesis (medication induced), infections, non-observance, or others. Hence, the SVT could be reported by the managing physician as the sole and exclusive trigger of CS (CS with SVT as an exclusive trigger) or be associated with one or two other coexisting triggers (CS with SVT as a non-exclusive trigger).
As previously described (3, 10), past medical history, ongoing treatments, and clinical, biological, and echocardiographic data were collected at admission and at 24 h. In-hospital CS management [especially inotropes/vasopressors, mechanical ventilation, renal replacement therapy, and short-term mechanical circulatory support (MCS)] was reported, as well as medication at admission, at discharge, and at 1 year. Precise mechanisms of SVT could not be retrieved from the database nor the evolution of SVT after adapted management.
All-cause mortality, heart transplantation (HTx), and ventricular assist devices (VADs) were assessed at 1 month and 1 year. The primary endpoint was 1-year all-cause mortality. Secondary endpoints included 1-month all-cause mortality, 1-year need for HTx or VAD, the 1-year rate of cardiovascular rehospitalizations, and the composite of death, HTx, or VAD at 1 year. When done, SVT catheter ablation (11) and myocardial revascularization (12) were performed according to the current techniques.
The study was conducted in accordance with the Helsinki Declaration and French law. Written consent was obtained for all patients. Recorded data and their storage were approved by the CCTIRS (French Health Research Data Processing Advisory Committee) (no. 15.897) and the CNIL (French Data Protection Agency) (no. DR-2016-109).
Continuous variables are reported as means ± SDs or medians and interquartile ranges (IQRs) when appropriate. Categorical variables are reported as frequencies and percentages. Comparisons were made using the Mann–Whitney non-parametric test for continuous variables and the chi-square test or Fisher's exact test for categorical variables. Paired data were analyzed with the Wilcoxon signed-rank test. Multivariate stepwise logistic regression analysis was performed to determine independent predictors for each primary and secondary outcome. First, the association of all baseline characteristics and each outcome of interest was assessed using univariable logistic regression analyses. Thereafter, all significant independent predictors were integrated into multivariable analyses for each outcome and backward reduced to only significant characteristics (p ≤ 0.05). Finally, these significant characteristics were incorporated in multivariable models as fixed covariates for each adjusted outcome analysis. The significant risk factors were reported with their respective odds ratios (ORs) and 95% confidence intervals (CIs). The variance inflation factor (VIF) was used to rule out multicollinearity among the variables. The primary outcome of all-cause mortality was assessed using Kaplan–Meier time-to-event analysis, and the adjusted hazard ratios (HRs), 95% CIs, and p-values were determined by Cox proportional hazards models. Secondary outcomes (HTx, VAD, and further composites) are reported as their adjusted ORs and 95% CIs.
The main analysis was a comparison between SVT-triggered and non-SVT-triggered CS. Further analyses were conducted about the primary and secondary endpoints in the SVT-triggered group between patients with SVT as an exclusive trigger and those with other coexisting triggers, as well as between CS with SVT as exclusive trigger without a history of cardiomyopathy (CM) and other SVT-triggered CS.
Analyses were performed using R software [version 4.1.2 (2021-11-01)]. All tests were two-tailed. A value of p ≤ 0.05 was considered statistically significant.
After the exclusion of three patients for missing data, 769 patients were included in 49 centers (Figure 1). Table 1 reports the initial characteristics of included patients. Patients were predominantly men (71.4%) with a mean age of 65.8 ± 14.8 years. Previously known heart disease was reported for 56% (29.9% ischemic, 10% dilated, and 8.5% valvular) patients, most of whom had a New York Heart Association (NYHA) stage II or III (26% or 26.4%, respectively), consistent with a substantial rate of chronic heart failure treatments (41.1%, 37.9%, and 13.8% for beta blockers, ACEi/ARB, and aldosterone antagonists, respectively). Table 2 summarizes the initial clinical, biological, and echocardiographic data. The mean MBP was 74.9 ± 18.4 mmHg, with initial cardiac arrest for 78 patients (10.2%). The mean left ventricle ejection fraction (LVEF) was 26.3 ± 13.4%, with a median tricuspid annular plane systolic excursion (TAPSE) of 13 mm (10–16) and a median peak systolic velocity tissue Doppler imaging (PSVtdi) of 8 cm/s (6–11).
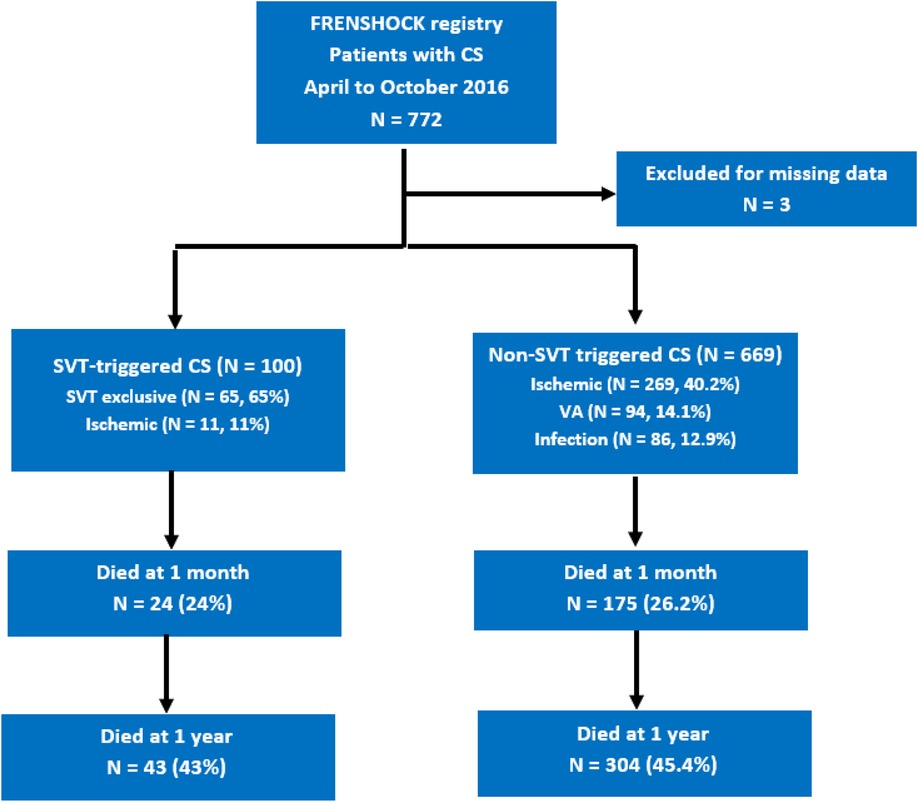
Figure 1. Flowchart of the study. CS, cardiogenic shock; SVT, supraventricular tachycardia; VA, ventricular arrythmias.

Table 1. Baseline characteristics at admission according to cardiogenic shock triggers (SVT vs. non-SVT).
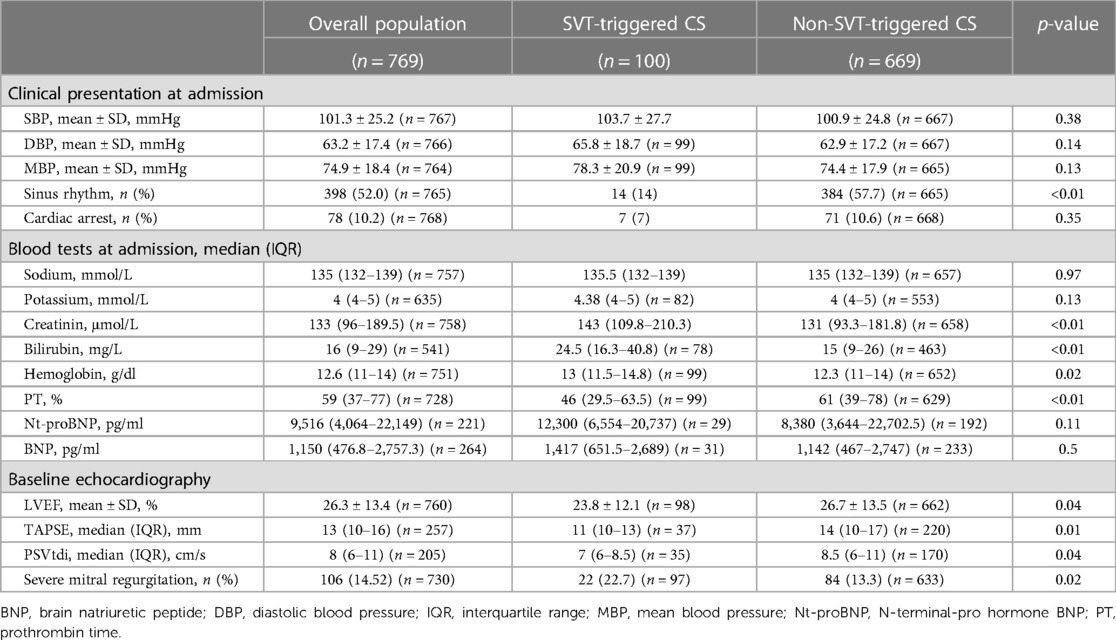
Table 2. Clinical, echocardiographic, and laboratory parameters according to cardiogenic shock triggers (SVT vs non-SVT).
Among the 769 CS patients, 100 were SVT-triggered (13%), of which 65 (8.5%) were exclusively triggered by SVT. Associated triggers reported in the SVT-CS group were ischemic (11%), iatrogenesis (7%), and infectious disease (6%) (Table 3). By contrast, among the 669 non-SVT-triggered CS patients, the main triggers were ischemic (40.2%), ventricular arrhythmia (14.1%), and infectious disease (12.9%).
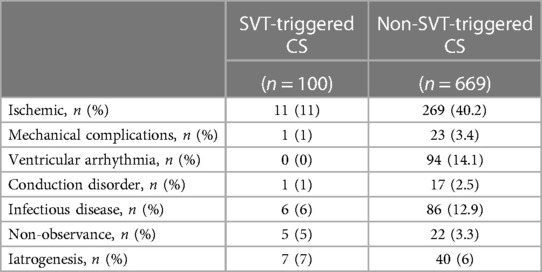
Table 3. Distribution of cardiogenic shock triggers between groups.
As reported in Table 1, initially, SVT-triggered CS patients exhibited higher proportions of male individuals (81% vs. 70%, p = 0.03), chronic kidney disease (32% vs. 19.6%, p < 0.01), and a history of previous heart disease (77% vs. 52.8%, p < 0.01), with an emphasis on ischemia (39% vs. 28.6%, p = 0.045) and valvular heart disease (15% vs. 7.5%, p = 0.02). Treatments with loop diuretics (65% vs. 46.2%, p < 0.01), aldosterone antagonists (26% vs. 12%, p < 0.01), amiodarone (35.4% vs. 14.6%, p < 0.01), vitamin K antagonist (VKA) (32% vs. 19.6%, p < 0.01), and direct oral anticoagulant (DOAC) (22% vs. 5.1%, p < 0.01) were significantly more commonly used in the SVT group.
SVT-triggered CS patients presented initially with higher initial creatinine and bilirubin levels, lower prothrombin time, lower LVEF, TAPSE, and PSVtdi, and more frequent severe mitral regurgitation (Table 2). After 24 h of management, the recovery was significantly better and more complete in the non-SVT group, as illustrated by a significant improvement in blood pressure, creatinine, bilirubin, lactate, and left ventricular ejection fraction parameters (Supplementary Table S1). At the time of initial care, 14% of patients in the SVT-triggered group presented with sinus rhythm against 57.7% of patients in the non-SVT group (p < 0.01).
As summarized in Table 4, inotropes were used in 89.8% of the overall population, with more frequent use of norepinephrine in the non-SVT group (42% vs. 55.2%, p = 0.02) and levosimendan in the SVT-triggered group (13% vs. 6.6%, p = 0.04). No between-group difference was found for ventilation, renal replacement therapy, and mechanical circulatory support.
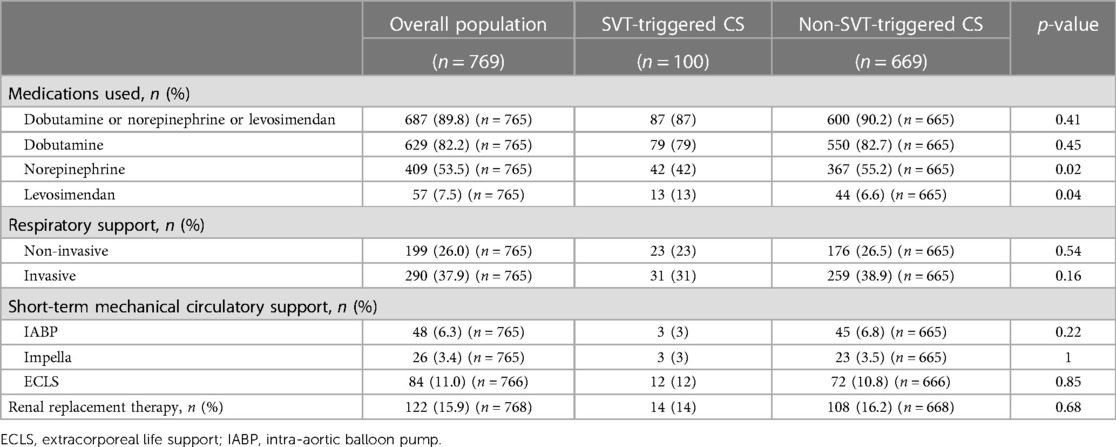
Table 4. In-hospital management according to cardiogenic shock triggers (SVT vs non-SVT).
Table 5 describes the antiarrhythmic therapy used in our population. Beta blockers and amiodarone were more frequently used in the SVT-triggered group at initial care (51% vs. 40%, p = 0.04 and 35.4% vs. 14.6%, p < 0.01), although at 24 h at discharge, only amiodarone was more frequently used in the SVT-triggered group (54% vs. 29.5%, p < 0.01, and 47.1% vs. 22.7%, p < 0.01).
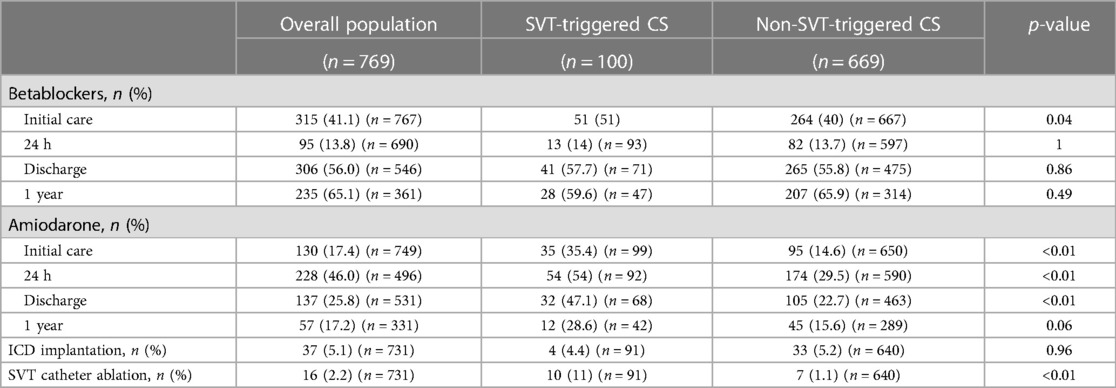
Table 5. Antiarrhythmic therapies according to cardiogenic shock triggers (SVT vs non-SVT).
SVT catheter ablation was performed in 10 patients of the SVT group vs. seven patients of the non-SVT group during initial CS hospitalization (11% vs. 1.1%, p < 0.01) because of the occurrence of SVT after inclusion in this group.
Figure 2 shows the absence of a 1-year all-cause mortality difference between SVT- and non-SVT-triggered CS [43% vs. 45.3%, adjusted HR of 0.9 (95% CI 0.59–1.39), p = 0.64]. The same results were found for 1-month all-cause mortality [24% vs. 26.2%, adjusted HR of 0.91 (95% CI 0.66–1.26), p = 0.58] (Figure 1). As reported in Figure 3, no difference was found in any secondary outcomes for cardiovascular rehospitalization, HTx, and VAD.
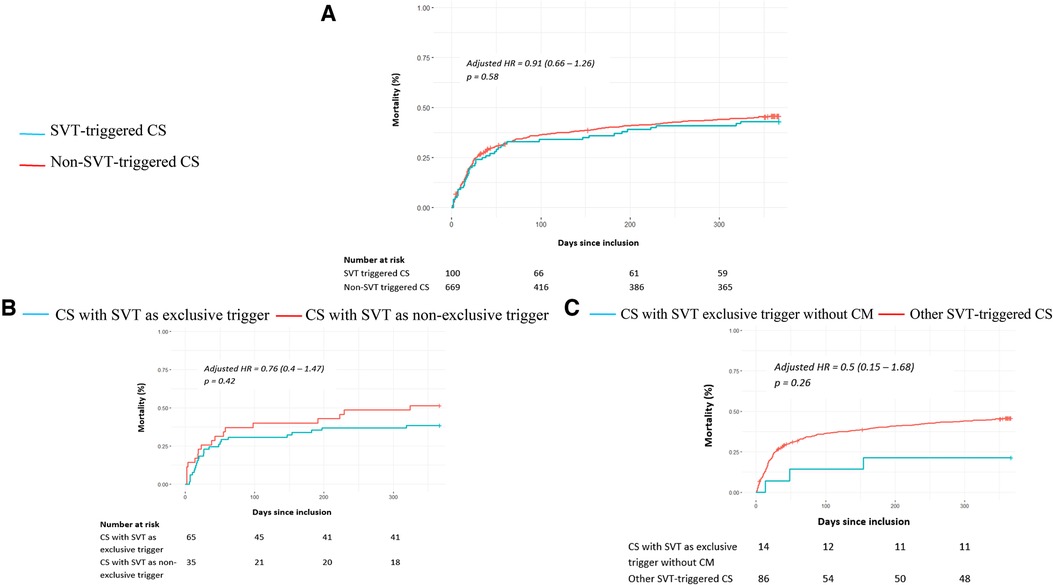
Figure 2. One-year all-cause mortality in patients with cardiogenic shock according to a supraventricular tachycardia trigger. The primary outcome of 1-year overall mortality is presented for SVT- and non-SVT-triggered CS patients (A), for CS patients with SVT as an exclusive trigger and CS patients with SVT and coexisting triggers (B), and for tachycardia-induced cardiomyopathy (CS with SVT as exclusive trigger and without previous cardiomyopathy) and other SVT-triggered CS patients (C). The cumulative incidences of 1-year and 1-month mortality were estimated using the Kaplan–Meier method; hazard ratios and 95% confidence intervals were estimated using Cox regression models. For all panels, 1-year all-cause mortality was adjusted for age, chronic kidney failure, and active cancer according to significant characteristics found as independent predictive factors in multivariable analyses.
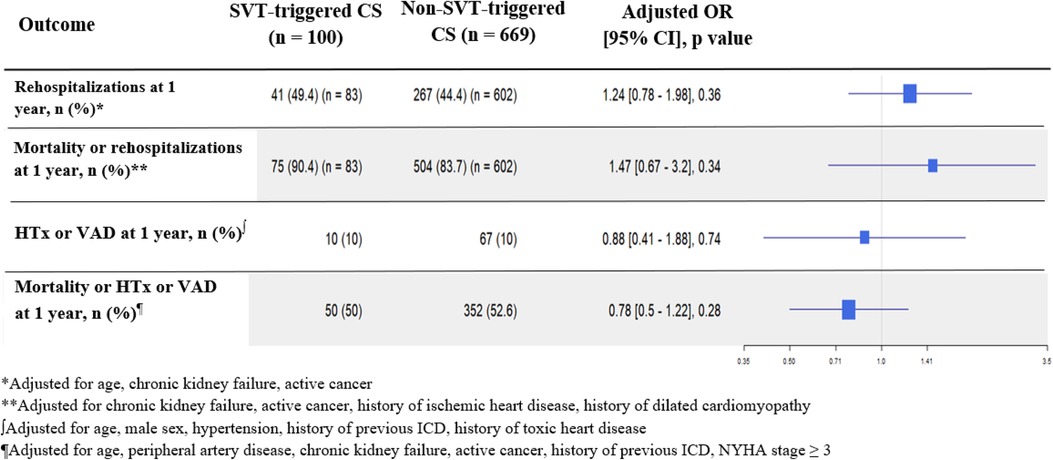
Figure 3. Secondary outcomes of rehospitalizations, heart transplantation, and ventricular assist devices in the overall population. Each adjusted outcome analysis included significant characteristics found as independent predictive factors in multivariable analyses and used as fixed covariates.
Among the 100 SVT-triggered CS patients, 65 presented initially with SVT as an exclusive trigger (distribution reported in Table 3), with balanced baseline characteristics between groups (Supplementary Table S2), except for higher rates of active cancers in the non-SVT-exclusive group (0% vs. 14.3%, p < 0.01), and aspirin treatment, more frequent in the SVT-exclusive group (46.2% vs. 20%, p = 0.02). The SVT-exclusive group presented with higher diastolic and mean blood pressure, with no difference in any biological or echocardiographic parameters except for higher sodium in the SVT-exclusive group (Supplementary Table S3). After 24 h, the exclusive SVT group showed a faster onset of LVEF recovery, while the non-SVT-exclusive group exhibited a more rapid decrease in lactate levels. In both groups, no substantial improvement was observed in blood pressure or renal and hepatic functions (Supplementary Table S4). Significant associations between baseline characteristics and each outcome of interest can be found in Supplementary Table S5.
Survival analyses did not show a difference in all-cause mortality at 1 month [adjusted HR 0.72 (95% CI 0.3–1.69), p = 0.45] and 1 year [adjusted HR 0.76 (95% CI 0.4–1.47), p = 0.42] (Figure 2) between SVT-exclusive and non-SVT-exclusive groups. As reported in Figure 4, no difference was observed for all secondary outcomes except for a higher rate of 1-year cardiovascular rehospitalizations in the SVT-exclusive group with an adjusted OR of 3.74 (95% CI 1.05–10.5, p = 0.01).
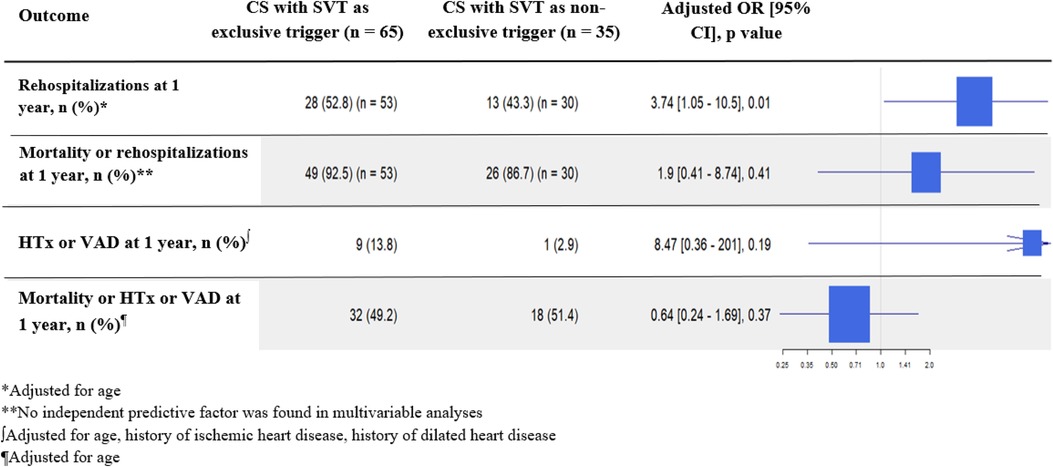
Figure 4. Secondary outcomes of rehospitalizations, heart transplantation, and ventricular assist devices in the SVT-triggered group. Each adjusted outcome analysis included significant characteristics found as independent predictive factors in multivariable analyses and used as fixed covariates.
All data relating to in-hospital management are reported in Supplementary Table S6. No difference was found in using any antiarrhythmic drug, neither at admission nor at 24 h, at discharge, or at 1 year (Supplementary Table S7).
Fourteen of the 100 SVT-triggered CS patients met this definition. As reported in Figure 2 and Supplementary Figure S1, overall composite criteria combining 1-year rates of mortality or HTx or VAD revealed a better outcome in this group with an adjusted OR of 0.23 (95% CI 0.04–0.95, p = 0.048).
To date, FRENSHOCK is the largest European prospective, observational, multicenter registry on CS, representing a real-world cohort from a broad spectrum of etiologies, including a relevant number of SVT-triggered CS patients, mostly non-ischemic, differing from previous surveys.
Analysis of the relationship between arrhythmia triggers and outcomes in unselected CS is scarce in the literature. We previously reported that ventricular arrhythmia is a common trigger of CS (12% in the FRENSHOCK population) associated with similar high mortality to other etiologies of CS but resulted in more heart transplantation and VAD cases at 1 year, especially in non-ischemic cardiomyopathy, suggesting the need for earlier evaluation by advanced heart failure specialized teams for a possible indication of mechanical circulatory support or heart transplantation (11).
Based on the FRENSHOCK registry, we would like to address the relationship between SVT and CS presentation, management, and outcomes.
Outside the setting of CS, several studies demonstrated that the presence of SVT (symptomatic or not) in patients with HF is associated with an increased risk for all-cause mortality, explained mainly by an increased risk for pump-failure death, suggesting that SVT may have a role in accelerating myocardial decline (7). By contrast, other studies, including, on average, patients with more severe HF, agreed not to support the concept that the presence of SVT in patients with advanced chronic HF is independently related to an adverse outcome during a long-term follow-up, considering SVT as a marker of advanced HF (6).
In this study, despite an initial presentation marked by more acute kidney and hepatic injuries and more severe biventricular dysfunction, SVT-triggered CS presented a similar 1-month rate of all-cause mortality to non-SVT-triggered CS. In addition, after 1 year of follow-up, no difference was observed in mortality, HTx or VAD, and rehospitalizations, suggesting a faster recovery in the medium and long term once the acute phase is resolved, indicative of an overall better prognosis.
Notwithstanding the high prevalence of SVT in CS, little has been reported about how they influence short- and long-term prognosis. Primary available data dealing with SVT and CS refer to the occurrence of arrhythmia in the case of CS complicating AMI, representing a minority in our cohort (11% of the 100 SVT-triggered CS patients), with no increase in 1-month and 1-year mortality (12, 13). A recent single-center retrospective study, including 222 patients with CS [of which 40 presented atrial fibrillation (AF)], focused on new-onset AF, indicating that although the presence of this arrhythmia can have a hemodynamic impact, it does not influence mortality rates (14), consistent with our results. As the relationship between SVT and ischemic heart disease is now well documented, further studies could focus on the influence of SVT-triggered CS in specific non-ischemic cardiomyopathies (e.g., dilated, hypertrophic, restrictive).
In comparison to the set of all CS triggers, pejorative independent predictive factors for 1-year all-cause mortality in the SVT-triggered CS population were age, chronic kidney failure, and active cancer, with variable correlation with other CS surveys such as the FAST-MI registry, which also highlighted age and history of kidney disease (15) or the CardShock study (16), underlying AMI, age, previous myocardial infarction, or prior coronary artery bypass as short-term mortality predictors. Yet, several studies found a higher mortality rate in non-ischemic heart disease (17). In our SVT-triggered CS group, coexisting ischemic trigger was not an independent pejorative predictive factor for mortality.
When exclusively triggered by SVT, the post-CS 1-year follow-up revealed a higher rate of cardiovascular rehospitalizations, consistent with many previous publications showing strong evidence for a high 30-day rate of rehospitalizations in the case of SVT and HF (18, 19). Even if no difference was found in mortality, HTx, or VAD, this trend should be highlighted, given the economic burden of rehospitalizations for SVT, which is probably underestimated (20). This trend leads us to assume that SVT can sometimes be considered a marker of myocardial decline, indicating a progression through the cascade of disease severity. Nonetheless, in our study, rehospitalizations were recorded globally from all cardiovascular causes without information on the possible recurrence of SVT.
To avoid the risk of misclassification, further analyses were made focusing on CS when exclusively triggered by SVT, without any additional trigger, as well as when occurring without a history of heart disease. Fourteen patients had an exclusively SVT-triggered CS occurring without previous heart disease and were associated with a significantly lower rate of the overall composite criteria combining 1-year mortality, HTx, and VAD. Even though we did not have enough data to sort them clearly, it might be in this part of the population that patients with tachycardia-induced cardiomyopathy (TIC), a clinical condition in which a persistent tachyarrhythmia or frequent ectopy contributes to ventricular dysfunction leading to systolic heart failure (21), are found. In addition, even if it should be taken with caution given the low number of patients, better outcome of 1-year mortality, HTx, or VAD seems consistent with previous studies, emphasizing restoration of LV function and reversal of LV remodeling with successful elimination of tachycardia in the majority of patients (22), even in emergency cases (23).
The relationship between SVT and advanced HF remains challenging, sometimes leading to iterative recurrences of CS because of inefficient maintenance of sinus rhythm, possibly requiring circulatory support and/or heart transplantation (24). Further studies could focus on patients with extremely severe SVT-triggered CS fulfilling the criteria for urgent indication of HTx and the prospect of escaping it through the restoration of sinus rhythm by efficient ablation.
First, from available data, we were not able to distinguish between different subtypes of atrial arrhythmia (e.g., atrial fibrillation, flutter, focal tachycardia) and their classification (first diagnosed, permanent, persistent, paroxysmal), although they fall under different management practices and could lead to different outcomes (25). Another main limitation was the assessment of return to sinus rhythm, which was only available during initial care and at discharge, limiting specific considerations, while long-term maintenance of sinus rhythm appears associated with better outcomes (26, 27). However, within the SVT-triggered group, we found the same rates of pharmacological and invasive antiarrhythmic treatments, suggesting that whatever the arrhythmia subtype and its curative strategy were, we achieved a good balance between groups. Furthermore, we had no information about SVT duration before CS, which might be a determining criterion for management strategy. Indeed, there is a singular difference between recent new-onset SVT, for which treatment should be to terminate SVT and prevent future recurrences using antiarrhythmic drugs and/or electrical cardioversion, followed by catheter ablation if needed, and chronic permanent SVT with high ventricular rate, less likely to be successfully converted and maintained in sinus rhythm, with a similar profile to that of end-stage heart failure. Future work on this topic should highlight this nuance, which was not detailed enough in this study.
While the crucial role of catheter ablation of SVT in heart failure is currently accepted (26, 28), only 11% of patients from the SVT-triggered CS benefited from such a procedure in our survey. Indeed, on top of including general hospitals with fewer facilities for carrying out an ablation, the cohort was conducted in 2016, when this type of procedure was less commonly performed than today. Ideally, this analysis should be done again with current data, and probably better outcomes would be observed in SVT-triggered CS.
Although considering all-cause mortality as the primary outcome was an intentional choice, since it represents the daily reality of the numerous comorbidities of patients suffering heart failure, future studies could also focus on specific cardiovascular outcomes and figure out a difference with all-cause mortality.
As previously reported (3), the FRENSHOCK registry involves risks of selection bias related to non-consecutive inclusions or exclusion of the most severe cases, with specific inclusion and exclusion criteria limiting the applicability to all patients with CS. We were not able to use the SCAI SHOCK Stage Classification, given that it was not yet available at the time of our study.
SVT is a frequent trigger of CS alone or in association. Although SVT-triggered CS patients were more comorbid with more pre-existing cardiomyopathies and HF incidences, they presented similar rates of mortality, HTx, and VAD at 1 year, arguing for a better overall prognosis. Nevertheless, limitations in the description of the SVT type, history, and long-term management in our registry justify pursuing research on this topic.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by CCTIRS (French Health Research Data Processing Advisory Committee) (no. 15.897) and the CNIL (French Data Protection Agency) (no. DR-2016-109. The patients/participants provided their written informed consent to participate in this study.
Design of the registry: EB, FR, GL, ME, EP, and CD; design of the analysis: MC, PM, and CD; statistics: MC; writing of the manuscript: MC, PM, and CD; substantial revision of the manuscript: MC, EB, EG, FR, NC, PM, and CD; data collection: all authors; review and acceptance of the manuscript: all authors. All authors contributed to the article and approved the submitted version.
The study was sponsored by the Fédération Française de Cardiologie and was funded by unrestricted grants from Daiichi-Sankyo and Maquet SAS.
FRENSHOCK is a registry of the French Society of Cardiology, managed by its Emergency and Acute Cardiovascular Care Working Group. The authors thank all the devoted personnel of Société Française de Cardiologie who participate in the upkeep of the registry. The authors are deeply indebted to all the physicians who took care of the patients at the participating institutions.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fcvm.2023.1167738/full#supplementary-material
1. McDonagh TA, Metra M, Adamo M, Gardner RS, Baumbach A, Böhm M, et al. 2021 ESC guidelines for the diagnosis and treatment of acute and chronic heart failure: developed by the task force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur Heart J. (2021) 42(36):3599–726. doi: 10.1093/eurheartj/ehab368
2. Chioncel O, Parissis J, Mebazaa A, Thiele H, Desch S, Bauersachs J, et al. Epidemiology, pathophysiology and contemporary management of cardiogenic shock—a position statement from the Heart Failure Association of the European Society of Cardiology. Eur J Heart Fail. (2020) 22:1315–41. doi: 10.1002/ejhf.1922
3. Delmas C, Roubille F, Lamblin N, Bonello L, Leurent G, Levy B, et al. Baseline characteristics, management, and predictors of early mortality in cardiogenic shock: insights from the FRENSHOCK registry. ESC Heart Fail. (2022) 9(1):408–19. doi: 10.1002/ehf2.13734
4. Wang TJ, Larson MG, Levy D, Vasan RS, Leip EP, Wolf PA, et al. Temporal relations of atrial fibrillation and congestive heart failure and their joint influence on mortality: the Framingham Heart Study. Circulation. (2003) 107(23):2920–5. doi: 10.1161/01.CIR.0000072767.89944.6E
5. Jabre P, Roger VL, Murad MH, Chamberlain AM, Prokop L, Adnet F, et al. Mortality associated with atrial fibrillation in patients with myocardial infarction: a systematic review and meta-analysis. Circulation. (2011) 123(15):1587–93. doi: 10.1161/CIRCULATIONAHA.110.986661
6. Crijns HJ, Tjeerdsma G, de Kam PJ, Boomsma F, van Gelder IC, van den Berg MP, et al. Prognostic value of the presence and development of atrial fibrillation in patients with advanced chronic heart failure. Eur Heart J. (2000) 21(15):1238–45. doi: 10.1053/euhj.1999.2107
7. Dries DL, Exner DV, Gersh BJ, Domanski MJ, Waclawiw MA, Stevenson LW. Atrial fibrillation is associated with an increased risk for mortality and heart failure progression in patients with asymptomatic and symptomatic left ventricular systolic dysfunction: a retrospective analysis of the SOLVD trials. Studies of left ventricular dysfunction. J Am Coll Cardiol. (1998) 32(3):695–703. doi: 10.1016/S0735-1097(98)00297-6
8. Raunsø J, Pedersen OD, Dominguez H, Hansen ML, Møller JE, Kjaergaard J, et al. Echocardiography and heart outcome study investigators. Atrial fibrillation in heart failure is associated with an increased risk of death only in patients with ischaemic heart disease. Eur J Heart Fail. (2010) 12(7):692–77. doi: 10.1093/eurjhf/hfq052
9. Pedersen OD, Søndergaard P, Nielsen T, Nielsen SJ, Nielsen ES, Falstie-Jensen N, et al. Atrial fibrillation, ischaemic heart disease, and the risk of death in patients with heart failure. Eur Heart J. (2006) 27(23):2866–70. doi: 10.1093/eurheartj/ehl359
10. Delmas C, Puymirat E, Leurent G, Elbaz M, Manzo-Silberman S, Bonello L, et al. Design and preliminary results of FRENSHOCK 2016: a prospective nationwide multicentre registry on cardiogenic shock. Arch Cardiovasc Dis. (2019) c112:343–53. doi: 10.1016/j.acvd.2019.02.001
11. Cherbi M, Roubille F, Lamblin N, Bonello L, Leurent G, Levy B, et al. One-year outcomes in cardiogenic shock triggered by ventricular arrhythmia: an analysis of the FRENSHOCK multicenter prospective registry. Front Cardiovasc Med. (2023) 10:1092904. doi: 10.3389/fcvm.2023.1092904
12. Neumann F-J, Sousa-Uva M, Ahlsson A, Alfonso F, Banning AP, Benedetto U, et al. 2018 ESC/EACTS guidelines on myocardial revascularization. Eur Heart J. (2019) 40(2):87–165. doi: 10.1093/eurheartj/ehy394
13. de Waha S, Schoene K, Fuernau G, Desch S, Eitel I, Pöss J, et al. Prognostic impact of atrial fibrillation in cardiogenic shock complicating acute myocardial infarction: a substudy of the IABP-SHOCK II trial. Clin Res Cardiol. (2018) 107(3):233–40. doi: 10.1007/s00392-017-1175-1
14. Santos H, Vieira T, Fernandes J, Ferreira AR, Rios M, Honrado T. New onset of atrial fibrillation in cardiogenic shock. Eur Heart J Acute Cardiovasc Care. (2021) 10(Supplement_1).
15. Aissaoui N, Puymirat E, Simon T, Bonnefoy-Cudraz E, Angoulvant D, Schiele F, et al. Long-term outcome in early survivors of cardiogenic shock at the acute stage of myocardial infarction: a landmark analysis from the French registry of acute ST-elevation and non-ST-elevation myocardial infarction (FAST-MI) registry. Crit Care. (2014) 18(5):516. doi: 10.1186/s13054-014-0516-y
16. Harjola VP, Lassus J, Sionis A, Køber L, Tarvasmäki T, Spinar J, et al. Clinical picture and risk prediction of short-term mortality in cardiogenic shock. Eur J Heart Fail. (2015) 17:501–9. doi: 10.1002/ejhf.260
17. Schrage B, Weimann J, Dabboura S, Yan I, Hilal R, Becher PM, et al. Patient characteristics, treatment, and outcome in non-ischemic vs. ischemic cardiogenic shock. J Clin Med. (2020) 9:931. doi: 10.3390/jcm9040931
18. Tripathi B, Atti V, Kumar V, Naraparaju V, Sharma P, Arora S, et al. Outcomes and resource utilization associated with readmissions after atrial fibrillation hospitalizations. J Am Heart Assoc. (2019) 8:e013026. doi: 10.1161/JAHA.119.013026
19. Munir MB, Sharbaugh MS, Ahmad S, Patil S, Mehta K, Althouse AD, et al. Causes and predictors of 30-day readmissions in atrial fibrillation (from the nationwide readmissions database). Am J Cardiol. (2017) 120(3):399–403. doi: 10.1016/j.amjcard.2017.04.040
20. Ericson L, Bergfeldt L, Björholt I. Atrial fibrillation: the cost of illness in Sweden. Eur J Health Econ. (2011) 12(5):479–87. doi: 10.1007/s10198-010-0261-3
21. Huizar JF, Ellenbogen KA, Tan AY, Kaszala K. Arrhythmia-Induced cardiomyopathy: JACC state-of-the-art review. J Am Coll Cardiol. (2019) 73:2328–44. doi: 10.1016/j.jacc.2019.02.045
22. Donghua Z, Jian P, Zhongbo X, Feifei Z, Xinhui P, Hao Y, et al. Reversal of cardiomyopathy in patients with congestive heart failure secondary to tachycardia. J Interv Card Electrophysiol. (2013) 36(1):27–32; discussion 32. doi: 10.1007/s10840-012-9727-9
23. Volle K, Delmas C, Rollin A, Voglimacci-Stephanopoli Q, Mondoly P, Cariou E, et al. Successful reversal of severe tachycardia-induced cardiomyopathy with cardiogenic shock by urgent rhythm or rate control: only rhythm and rate matter. J Clin Med. (2021) 10(19):4504. doi: 10.3390/jcm10194504
24. Hékimian G, Paulo N, Waintraub X, Bréchot N, Schmidt M, Lebreton G, et al. Arrhythmia-induced cardiomyopathy: a potentially reversible cause of refractory cardiogenic shock requiring venoarterial extracorporeal membrane oxygenation. Heart Rhythm. (2021) 18(7):1106–12. doi: 10.1016/j.hrthm.2021.03.014
25. Hindricks G, Potpara T, Dagres N, Arbelo E, Bax JJ, Blomström-Lundqvist C, et al. 2020 ESC guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS): the task force for the diagnosis and management of atrial fibrillation of the European Society of Cardiology (ESC) developed with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC. Eur Heart J. (2021) 42(5):373–498. doi: 10.1093/eurheartj/ehaa612
26. Hsu L-F, Jaïs P, Sanders P, Garrigue S, Hocini M, Sacher F, et al. Catheter ablation for atrial fibrillation in congestive heart failure. N Engl J Med. (2004) 351:2373–83. doi: 10.1056/NEJMoa041018
27. Mark DB, Anstrom KJ, Sheng S, Piccini JP, Baloch KN, Monahan KH, et al. Effect of catheter ablation vs. medical therapy on quality of life among patients with atrial fibrillation. The CABANA randomized clinical trial. JAMA. (2019) 321(13):1275–85. doi: 10.1001/jama.2019.0692
28. Marrouche NF, Brachmann J, Andresen D, Siebels J, Boersma L, Jordaens L, et al. Catheter ablation for atrial fibrillation with heart failure. N Engl J Med. (2018) 378:417–27. doi: 10.1056/NEJMoa1707855
ACE, angiotensin-converting enzyme; ACEi, angiotensin-converting enzyme inhibitor; AF, atrial fibrillation; ARB, angiotensin receptor blocker; ALAT, alanine aminotransferase; AMI, acute myocardial infarction; ASAT, aspartate aminotransferase; BNP, brain natriuretic peptide; CCTIRS, Comité Consultatif sur le Traitement de l’Information en matière de Recherche dans le domaine de la Santé; CI, confidence interval; CM, cardiomyopathy; CNIL, Commission nationale de l'informatique et des libertés; COPD, chronic obstructive pulmonary disease; CRP, C-reactive protein; CS, cardiogenic shock; DBP, diastolic blood pressure; DOAC, direct oral anticoagulant; ECLS, extracorporeal life support; HF, heart failure; HR, hazard ratio; HTx, heart transplantation; IABP, intra-aortic balloon pump; ICU, intensive care unit; ICCU, intensive cardiac care unit; ICD, implantable cardioverter-defibrillator; IQR, interquartile range MRA, mineralocorticoid receptor antagonist; LVEF, left ventricle ejection fraction; MBP, mean blood pressure; Nt-proBNP, N-terminal-pro hormone BNP; NYHA, New York Heart Association; PSVtdi, peak systolic velocity tissue Doppler imaging; PT, prothrombin time; SBP, systolic blood pressure; SD, standard deviation; STEMI, ST-segment elevation myocardial infarction; SVT, supraventricular tachycardia; TAPSE, tricuspid annular plane systolic excursion; TIC, tachycardia-induced cardiomyopathy; VA, ventricular arrythmias; VAD, ventricular assist device; VIF, variance inflation factor
Keywords: cardiogenic shock, supraventricular tachycardia, epidemiology, prognosis, mortality
Citation: Cherbi M, Bonnefoy E, Lamblin N, Gerbaud E, Bonello L, Roubille F, Levy B, Champion S, Lim P, Schneider F, Elbaz M, Khachab H, Bourenne J, Seronde M-F, Schurtz G, Harbaoui B, Vanzetto G, Combaret N, Labbe V, Marchandot B, Lattuca B, Biendel-Picquet C, Leurent G, Puymirat E, Maury P and Delmas C (2023) One-year outcomes in cardiogenic shock triggered by supraventricular tachycardia: an analysis of the FRENSHOCK multicenter prospective registry. Front. Cardiovasc. Med. 10:1167738. doi: 10.3389/fcvm.2023.1167738
Received: 16 February 2023; Accepted: 11 August 2023;
Published: 5 September 2023.
Edited by:
Matteo Cameli, University of Siena, ItalyReviewed by:
David Zweiker, Klinik Ottakring, Austria© 2023 Cherbi, Bonnefoy, Lamblin, Gerbaud, Bonello, Roubille, Levy, Champion, Lim, Schneider, Elbaz, Khachab, Bourenne, Seronde, Schurtz, Harbaoui, Vanzetto, Combaret, Labbe, Marchandot, Lattuca, Biendel-Picquet, Leurent, Puymirat, Maury and Delmas. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Clément Delmas ZGVsbWFzLmNsZW1lbnRAY2h1LXRvdWxvdXNlLmZy; Y2xlbWVudDIzMTg1QGhvdG1haWwuZnI=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.