 Mumtaz Maulana Hidayat
Mumtaz Maulana Hidayat Denny Agustiningsih
Denny Agustiningsih Rahmaningsih Mara Sabirin
Rahmaningsih Mara Sabirin Rakhmat Ari Wibowo
Rakhmat Ari Wibowo- Department of Physiology, Faculty of Medicine, Public Health and Nursing, Gadjah Mada University, Yogyakarta, Indonesia
Background: Global burden of hypertension among young people continues to increase. There have been many studies examining the effect of aerobic and muscle-strengthening physical activity on blood pressure, many of them didn't consider interdependence between them. Conflicting results of health-related fitness, particularly handgrip strength, as intermediate outcomes of muscle-strengthening physical activity on blood pressure also emerged. This research will carry out a mediation-moderation analysis to find out the relationship between muscle strengthening physical activity and blood pressure among young adults by considering health-related fitness and 24-hour movement behavior.
Methods: A cross-sectional study among 221 Indonesian young adults attending a physical activity intervention collected participant's muscle-strengthening physical activity, and 24 h movement behavior, including aerobic physical activity, sedentary and sleep behavior, and mental well-being using validated questionnaires. Mediation and moderation analyses were conducted using Process Macro model 10 on SPSS 25 to investigate the association of muscle-strengthening physical activity on blood pressure, with gender and blood pressure as moderator, mediators consist of handgrip strength, muscle mass percentage and cardiorespiratory fitness. A subgroup analysis was conducted based on participant's cardiorespiratory fitness level.
Results: Volume of muscle-strengthening physical activities in a week have a direct association with systolic blood pressure among prehypertensive male with an effect of 0,00989359 (95% CI 0,0046488 to 0,00336478). Considering its volume as mediator, the frequency of muscle-strengthening physical activity contributed to a significant direct effect on diastolic blood pressure in both genders, but the duration of MSPA has a significant direct effect on systolic blood pressure in male subjects. There is no component of physical fitness that provides a significant mediating effect. After a subgroup analysis, the relationship between MSPA Volume and blood pressure is not significant for individuals with a high level of cardiorespiratory fitness.
Conclusions: This study shows that increased participation in muscle strengthening physical activity, especially in subject with low cardiorespiratory fitness, could increase blood pressure in prehypertensive young adult male population without mediation by physical fitness. Further research is needed to investigate other mechanisms that influence this relationship.
1. Introduction
The prevalence of hypertension, a non-communicable condition, is quite high and is constantly rising. From 1990 to 2019, the number of persons with hypertension more than doubled, from 600 million to more than 1 billion (1). In just a few years, the prevalence of hypertension among Indonesian adults between the ages of 18 and 24 has nearly doubled (2). Given that hypertension, especially in young people, can continue to rise and constitute a major financial burden on the world's healthcare system. The average total costs of hypertension for all the studied countries, calculated per person, amounted to 630.14 USD, with direct costs of 1,497.36 USD and indirect costs of 282.34 USD (3). That should be a serious worry.
The high rate of hypertension at a young age is inseparable from the reluctance of young people to do physical activity (4, 5). Various studies have shown the benefits of physical activity in maintaining health and controlling non-communicable diseases such as hypertension. Aerobic physical activity and muscle strengthening physical activity are the most commonly associated with blood pressure. Muscle-strengthening physical activities (MSPA) deserve more attention because health surveys in various countries also show that only 10%–30% of adults do MSPA according to recommendations (6). MSPA are also rarely the focus of promoting physical activity for public health in various countries (7).
Although there have been many studies looking for a relationship between MSPA and blood pressure, many of them didn't consider the interdependence between them. While health- related fitness components such as muscle strength can be intermediates between MSE and blood pressure, some studies show inconsistent results. MSPA is generally associated with a lower risk of high blood pressure, but several studies have shown that higher blood pressure is associated with higher grip strength through mechanisms that are unclear. Therefore, it is necessary to do an analysis to assess the relationship between various factors (8, 9, 10).
In addition, various health-related factors that can affect blood pressure conditions, such as age, mental health, sleeping behavior, and sedentary behavior are also rarely considered. Age is globally known as one of the biggest risk factor in high blood pressure incidence, including in Indonesia (11). Mental health condition, such as anxiety or depression are also associated with the incidence of high blood pressure in young adults by unclear mechanism (12, 13). There is strong evidence of an association between sleep disturbance and increased risk of blood pressure, especially in young population (14, 15). Sedentary behavior in adult population is also associated with elevated blood pressure (16). The relationship between blood pressure and all the above factors encourages us to control them as covariates in this study.
Moreover, gender and abnormal blood pressure as potential moderators. There are several studies that show differences in response to physical exercise between men and women. Systolic Blood Pressure (SBP) and Diastolic Blood Pressure (DBP) reduction with muscle strengthening exercises differs statistically between men and women (17). Another study showed statistically significantly more pronounced DBP and mean arterial pressure (MAP) reductions from isometric resistance training among males than females (18). A meta-analysis also showed that the reduction in MAP due to muscle strengthening exercises was greater in subjects with hypertension than in subjects with normal blood pressure (19).
Given that there is still a knowledge gap where there are not many mediation analysis studies that link MSPA and blood pressure with consideration of the interdependence connection between them, this research will carry out a mediation-moderation analysis to find out the relationship between muscle strengthening physical activity and blood pressure by considering gender and abnormal blood pressure as moderator, muscle strength, muscle mass percentage and cardiorespiratory fitness as mediator and moderate-vigorous physical activity, age, sleep behavior, sedentary behaviour, mental wellbeing and BMI as covariates.
2. Material and methods
2.1. Study design and setting
We conducted a cross-sectional study taking place at Gadjah Mada University, Yogyakarta, Indonesia. This study was conducted to see the mediating role of physical fitness in the relationship between MSPA and its domain with blood pressure in the young adult population by considering moderate-vigorous physical activity, age, mental health, sleep behavior, and sedentary behavior. Data collection was carried out for 1 month in November-December 2022. The study protocol was approved by the medical and health research ethics committee of the Faculty of Medicine, Public Health, and Nursing at UGM (approval number: KE/FK/1382/EC/2022). This study is a sub-study of a quasi-experimental study entitled “Effectiveness of a virtual challenge with a social component in promoting physical activity, hydration, and fruit consumption among university students.” This study protocol has been registered with the Thai Clinical Registry with the registry number TCTR20230106003. We reported our current study following the strengthening the reporting of observational studies in epidemiology (STROBE) statement and A Guideline for Reporting Mediation Analyses of Randomized Trials and Observational (20, 21).
2.2. Participants and sample size
All Gadjah Mada University students, including those pursuing vocational, undergraduate, master, and doctoral degrees, were qualified to take part in the study. Subject age was limited to the range of 18–25. The study excluded participants who had experienced a heart attack within the previous three months, were recovering from surgery, and had physical or mental impairments that precluded them from taking part in all tests. Convenience sampling technique was adopted in this investigation. G*Power analysis was used to calculate the sample size to examine the link between the volume of muscle-strengthening activities and blood pressure (22). Using a power of 0.8, an alpha level of 0.05, and an effect size of 0.2, the minimal number of samples is 153 (23). Out of a total of 412 eligible prospective subjects, 155 did not give their consent to participate. 257 subjects were checked for eligibility, and 22 were excluded for not attending fitness checks. Six subjects had musculoskeletal problems that were contraindications for fitness checks. 231 subjects were confirmed as eligible for the study. After there were 10 missing and invalid data, 221 subjects were included in the analysis. The study flow diagram follows previous study.
2.3. Effect of interest
The primary aim of this study was examining the direct effect of volume of MSPA on blood pressure. In addition, the study also aimed to analyze the indirect effect of various physical fitness components as potential mediators in the relationship between them by considering the role of sex and abnormal blood pressure as moderators.
This study not only wants to see the direct effect of volume of MSPA on blood pressure but also the indirect effect of various physical fitness components as potential mediators in the relationship between them. This study also wants to see the role of sex and abnormal blood pressure as moderators.
2.4. Variables and causal assumption
We used a modeling framework to examine whether physical fitness mediates the relationship between MSPA volume and blood pressure (Figure 1). MSPA served as an independent variable, while systolic blood pressure, diastolic blood pressure, and mean arterial pressure served as dependent variables. We also included sedentary behavior, moderate-to-vigorous aerobic physical activity, and sleep behavior as covariates. The model is created with the assumption that independent variables have a significant correlation with the outcome, independent variables have a significant correlation with the mediator, and mediator has a significant correlation with the dependent variable. We investigated the total effect (path c) and direct effect (path c') in the figure above using linear regression with the Hayes model. Path a showed the correlation between the independent variables (MSPA) and the mediators (muscle mass, muscle strength, and CRF). Path b represents the correlation between the mediators (muscle mass, muscle strength, and CRF) and the dependent variable (BP). After adjustment for confounders, the a-b pathway represents the indirect effect of MSPA, which is mediated by muscle mass, muscle strength, and CRF. The mediated effect is a multiplication of effects a and b. Therefore, the direct effect c' represents the independent variable's effect after considering the mediated effect.
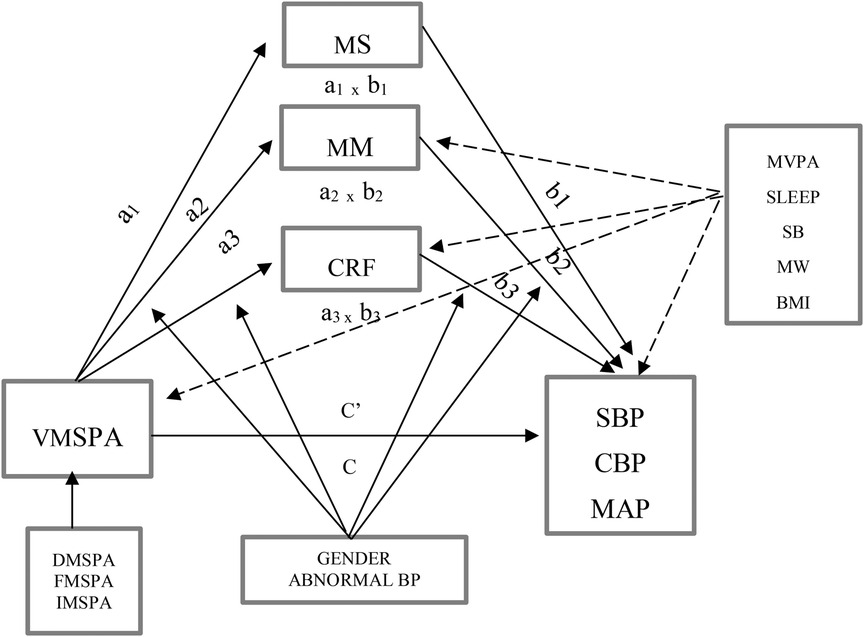
Figure 1. Causal model representing moderated-mediation analysis of association between muscle-strengthening physical activity with blood pressure considering covariates. a, effect of independent variable on mediator; b, effect of mediator on outcome; c’, direct effect of independent variable on outcome; c, total effect of independent variable on outcome; VMSPA, Volume of Muscle-Strengthening Physical Activity; DMSPA, Duration of Muscle-Strengthening Physical Activity; FMSPA, Frequency of Muscle-Strengthening Physical Activity; IMSPA, Intensity of Muscle-Strengthening Physical Activity; MVPA, Moderate-Vigorous Aerobic Physical Activity; MW, Mental Well-being; MS, Muscle Strength; MM, Muscle Mass Percentage; CRF, Cardiorespiratory Fitness; BMI, Body Mass Index; SLEEP, Sleep Quality and Quantity; SB, Sedentary Behavior; SBP, Systolic Blood Pressure; DBP, Diastolic Blood Pressure; MAP, Mean Arterial Pressure. - -, covariates; __, moderators.
2.5. Outcome measure
2.5.1. Main outcome: blood pressure
After a minimum of five minutes of rest, SBP and DBP were assessed in a sitting position using a certified digital instrument (Omron HEM 705CPINT, USA) (24). We measure twice, one minute apart, and then average the two results. Blood pressure measurements were obtained from 8 to 10 a.m. to minimize circadian effects.
2.5.2. Main predictor: volume of muscle strength physical activity
The volume of Muscle Strength Physical Activity (MSPA) for a week was measured by the Muscle Strengthening Exercise Questionnaire (MSEQ), which consists of questions about the duration, intensity, frequency, and domain of muscle strengthening exercises (24). MSPA is expressed in MET-minutes per week.
2.5.3. Potential mediator
2.5.3.1. Muscle strength
Muscle strength was assessed with a Camry handgrip dynamometer (Model EH101). All subjects were asked to sit down while holding the dynamometer in the dominant hand with their arms at a 90degree angle with the body without squeezing the arms against the body. Participants are allowed to do one trial. As in the previous study (10, 25), three trials were performed, resting 60 s between measurements on the same hand. The dynamometer was adjusted to the size of the participant's hand before measuring grip strength by turning the adjusting knob right or left to get an ideal grasp. All three scores are averaged for analysis. Grip strength is expressed in kilograms.
2.5.3.2. Muscle mass
Omron Karada Scan HBF 375 Body Fat Composition Monitor Used to measure body weight in kilograms (kg) and percentage of skeletal muscle mass.
2.5.3.3. Cardiorespiratory fitness
Cardiorespiratory fitness examined by the 6-Minute Walking Test (6MWT) method. The result of the 6MWT distance in meters is converted to an estimate of V˙O2max by the formula (26). V˙O2max is expressed in numbers, with units of ml/kg/minute. The Vo2max level is categorized as good if it is above 40 for women and above 50 for men. In the sensitivity analysis, we consider the VO2max category. All physical fitness examinations are carried out in the morning (08.00–12.00 am) to avoid the effects of circadian rhythms.
2.5.4. Covariate and other variables
Covariates consist of Moderate-Vigorous physical activity (MVPA), sedentary behavior, sleep behavior, mental wellbeing, and BMI. MVPA, sedentary behavior, and sleeping habits are measured from questions on a questionnaire that has been tested for reliability and validity in our unpublished study (27). MVPA is expressed in Met-Minutes per week. While sleep behavior is expressed in Score (28, 29) and sedentary behavior expressed in minutes per week. Mental wellbeing was measured using the shortened Warwick-Edinburgh Mental Well-being Scale (WEMWBS) which has been translated and validated in Bahasa Indonesia (28, 29). BMI is obtained from body weight in kg divided by height in m2 and expressed in number.
2.6. Statistical analysis
Data were displayed using descriptive statistics in the form of a mean and standard deviation. The distribution of categorical variables is presented using frequency and proportion. If data is normally distributed, then Pearson correlation was used to see the relationship between volume of muscle strengthening exercises, blood pressure, muscle strength, and percentage of muscle mass. If the data is not normally distributed, then an alternative is using Spearman's correlation. The percentile bootstrapping linear regression using Hayes model was used to assess the mediating effect of muscle strength and muscle mass percentage. We present the results of the mediation-moderation analysis with data that has been adjusted by the covariates and without adjustment. A sensitivity analysis was carried out by considering the level of cardiopulmonary fitness. All analyses were performed using the SPSS version 25 application with a significance level of 0.05.
3. Result
257 undergraduate students who were among the 412 participants in the virtual challenge decided to take part in the study and completed the questionnaire. Ninety percent of them (235) attended the health and fitness examination, but 4 of them had an absolute contraindication to fitness measurement, resulting in a total of 231 study subjects. After excluding 5 missing and 5 invalid data, a total of 221 subjects were finally included in the analysis. Based on Table 1, the mean age was 19.25 years old, the majority of subjects were 19 years old (121, or 54.8%), and the rest were in the age ranges of 18 years and 20–23 years. The majority of subjects were female, namely 143 people (64.7%) and the remaining 78 men (35.3%). The data in Table 1 show that the participants' average volume of muscle-strengthening physical activity per week is still below moderate-vigorous aerobic physical activity, where the ratio is three times. As many as 131 subjects (59.3%) had systolic and diastolic blood pressure within the normal range, while the remaining 90 people (40.7%) were in the high blood pressure category (systolic >120 and/or diastolic >80 mmHg).

Table 1. Participant characteristics.
According to the R2 of the unadjusted models (Figure 2), muscle-strengthening physical activity explains the variation in blood pressure readings in the population by 66.27% for systolic blood pressure, 48.72% for diastolic blood pressure, and 60.75% for MAP, MSPA, on the other hand, accounted for 69.16%, 49.79%, and 62.36% of the variation in the population's systolic, diastolic, and MAP blood pressure readings in the table. Therefore, tables were used in explaining the mediation-moderation analysis.
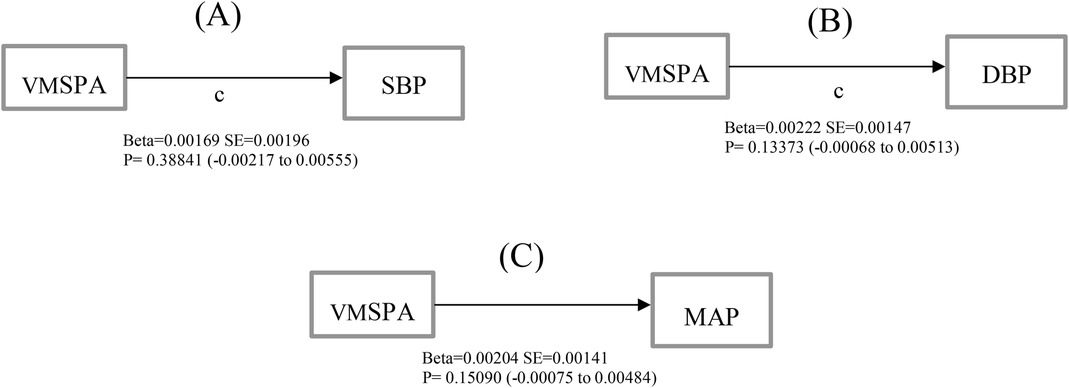
Figure 2. Total effect (path c) of muscle-strengthening physical activity volume on (A) systolic blood pressure (B) diastolic blood pressure (C) mean arterial pressure.
Looking at the results of the adjusted model that included covariates (Tables 2–5), it is clear that muscle-strengthening physical activity has a significant direct effect on systolic blood pressure in the male population with high blood pressure (β = 0.00191, 95% CI 0.00046 to 0.00335, t = 2.60425, p = 0.00987), but not in women (β = 0.00015, 95% CI −0.00339 to 0.00370, t = 0.08623, p = 0.93136). Looking at these data, it can be estimated that every 625 min of 4 MET (moderate intensity) muscle-strengthening physical activity in 1 week is associated with an increase in systolic blood pressure of 5 mmHg in the male population that has high blood pressure. Neither muscle mass, muscle strength nor cardiorespiratory fitness has a mediating effect on the relationship between MSPA volume and blood pressure.
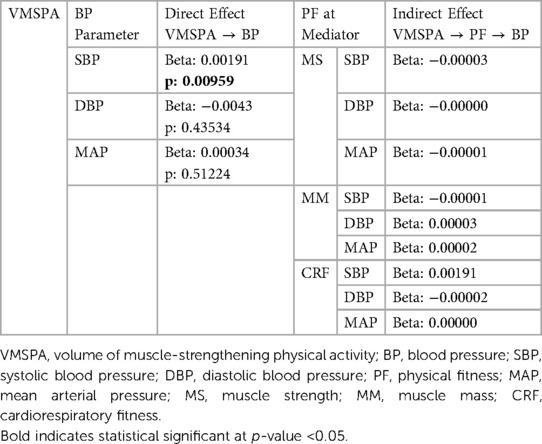
Table 2. Direct and indirect effect of muscle-strengthening physical activity volume (VMSPA) on BP parameter in male group with Abnormal blood pressure.

Table 3. Direct and indirect effect of muscle-strengthening physical activity volume (VMSPA) on BP parameter in male group with normal blood pressure.
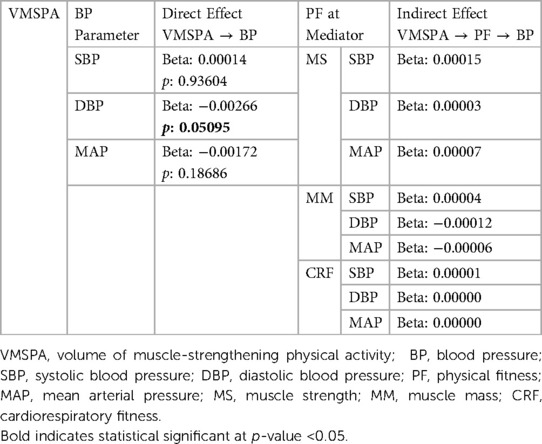
Table 4. Direct and indirect effect of muscle-strengthening physical activity volume (VMSPA) on BP parameter in female group with Abnormal blood pressure.
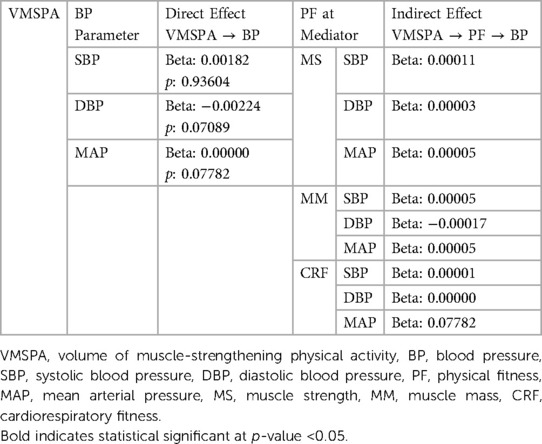
Table 5. Direct and indirect effect of muscle-strengthening physical activity volume (VMSPA) on BP parameter in female group with normal blood pressure.
Tables 6–8 show the effect and direct effect of MSPA components (which include MSPA duration, frequency, and intensity) on blood pressure outcome via MSPA volume mediation. Of the three components, the frequency of MSPA contributed to a significant direct effect on diastolic blood pressure in both genders (male p = 0.02064, 95% CI −1.63213 to −0.13681; female p = 0.03221, 95% CI −2.59071 to −0.11597). Meanwhile, the duration of MSPA has a significant direct effect on systolic blood pressure in male subjects (p = 0.02087, 95% CI 0.00446 to 0.05389). After looking at the direct and indirect effects in the model above, we conducted a sensitivity analysis by comparing the data on the relationship between VMSPA and blood pressure by grouping subjects based on their level of cardiopulmonary fitness, shown in Tables 9–11.
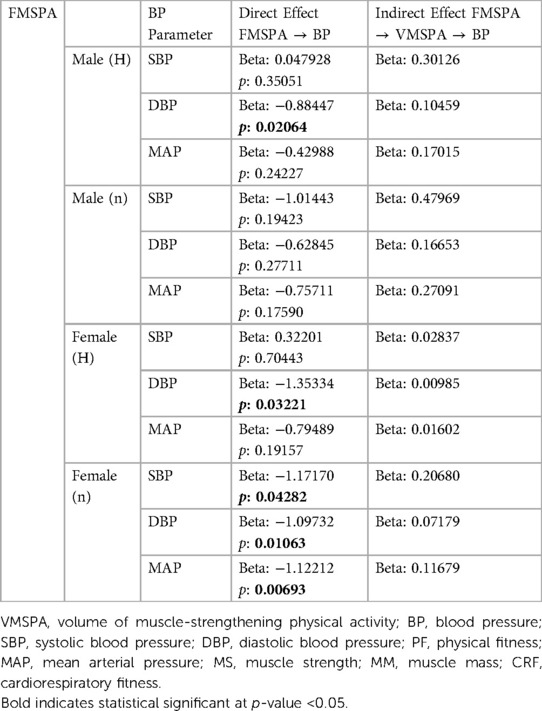
Table 6. Direct and indirect effect of muscle strength physical activity frequency (FMSPA) on BP parameter.
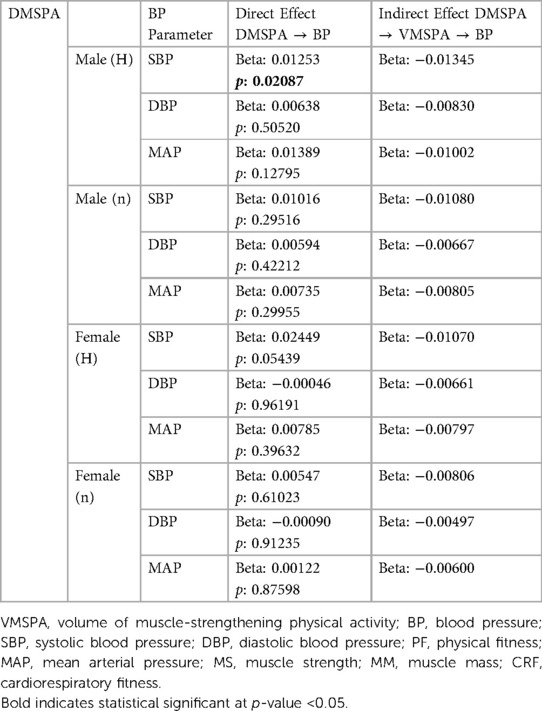
Table 7. Direct and indirect effect of muscle strength physical activity duration (DMSPA) on BP parameter.
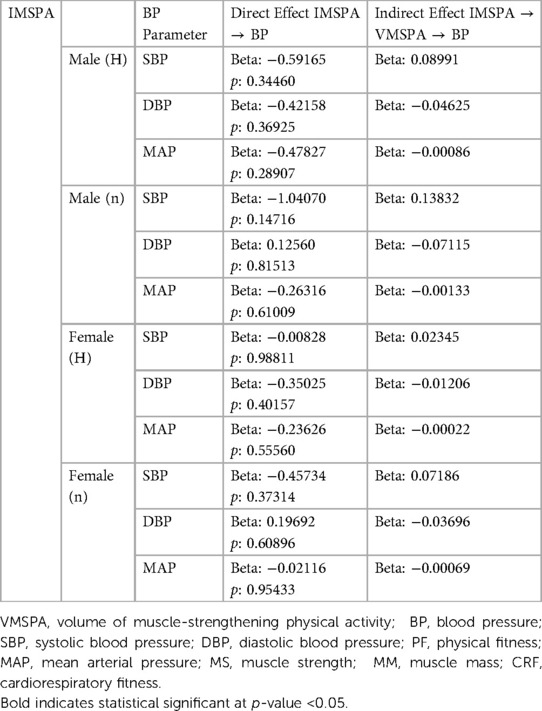
Table 8. Direct and indirect effect of intensity of muscle-strengthening physical activity (IMSPA) on BP parameter.
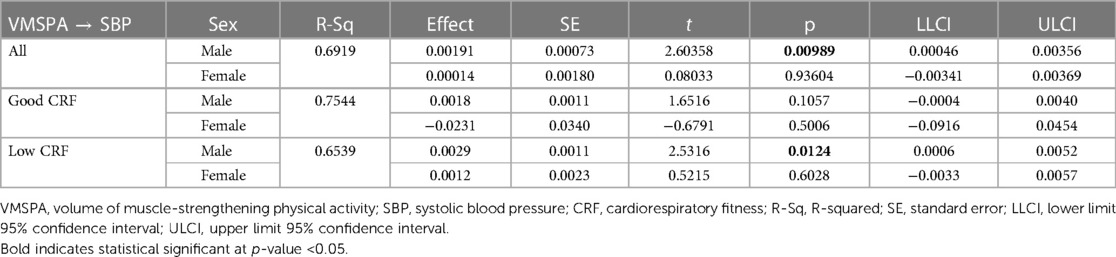
Table 9. Subgroup analysis with cardiorespiratory fitness classification parameters on the direct relationship between muscle strengthening physical activity volume and systolic blood pressure.
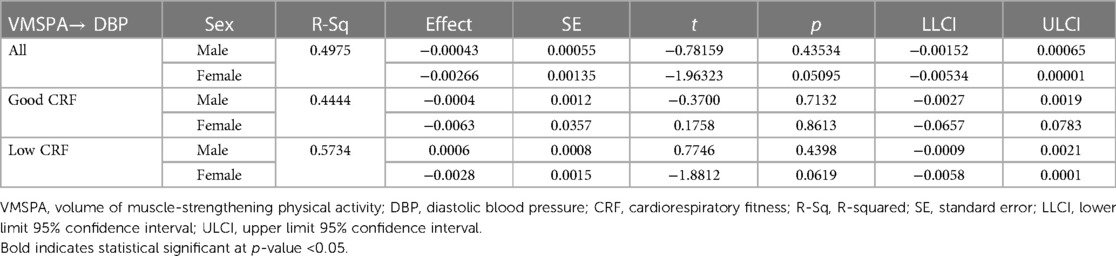
Table 10. Subgroup analysis with cardiorespiratory fitness classification parameters on the direct relationship between muscle strengthening physical activity volume and diastolic blood pressure.
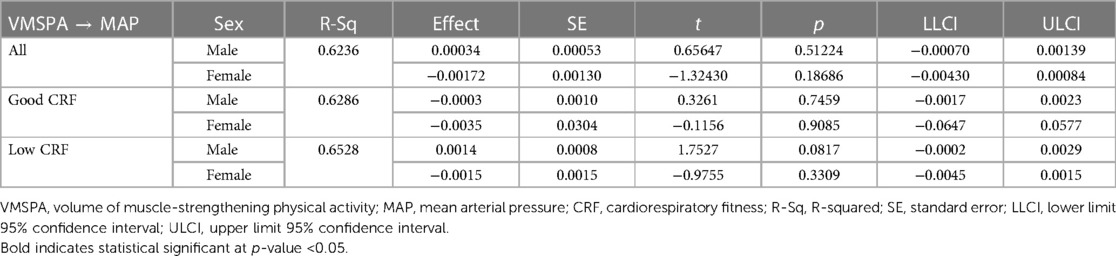
Table 11. Subgroup analysis with cardiorespiratory fitness classification parameters on the direct relationship between muscle strengthening physical activity volume and mean arterial pressure.
According to the Tables 9–11, among 221 subjects, there were 58 subjects with good cardiorespiratory fitness (≥40 ml/kg/minute) and 163 with low cardiorespiratory fitness (<40 ml/kg/minute). In Table 9, it can be seen that for male subjects in the good fitness group, the relationship between the volume of muscle strengthening exercises and systolic blood pressure was not significant (p: 0.1057, 95% CI −0.0004 to 0.0040), compared to the group of all fitness levels (p: 0.00989, 95% CI 0.00046 to 0.00356) and in the low fitness group (p: 0.0124, 95% CI 0.0006 to 0.0052), which is significant. Comparing R2 among the three groups, we can see the good fitness group explains the variation in systolic blood pressure readings in the population by 75.44%, compared with 69.16% in the all fitness group and 65.39% in the low fitness group. As a result, in people with a high level of cardiorespiratory fitness, the relationship between the volume of muscle-strengthening exercises and blood pressure is not significant.
4. Discussion
4.1. Key result and interpretation
This study shows statistically that there is a significant positive relationship between MSPA and blood pressure, after entering gender and abnormal blood pressure as moderators. Different results appear when the two variables are not considered, where there is no significant direct effect between MSPA and BP. This shows that sex and abnormal pressure function as moderator variables in the relationship between MSPA and BP.
In previous studies that investigated the relationship between muscle strength and BP, there was a positive relationship between MS and BP. However, in the present study, the relationship between MS and BP was not significant. This could be influenced by many things, seeing as the number of samples and the age range used in previous studies were different. However, MSPA has a direct effect on SBP. In the components and domains of MSPA, it turns out that free weight also has a direct effect on SBP in men.
However, there was no indirect effect from the mediators studied. This shows that there are other mechanisms or factors other than physical fitness that can mediate the relationship between MSPA and blood pressure. We suspect that there are three things that can explain why there are differences in the effects of MSPA on BP in men and women.
First, hormone and autonomic response differences between gender. In women, there is hormone secretion, such as estrogen, which has an effect on nitric oxide synthesis, and provides a relaxing effect on peripheral resistance of blood vessels (30). In addition, it is well known that testosterone levels in women are lower than in men. Meanwhile, higher testosterone levels are associated with higher blood pressure (31).
It is well known that blood pressure is the product of cardiac output and peripheral resistance. Cardiac output is the product of the heart rate and stroke volume, where the heart rate component is strongly influenced by the work of the sympathetic and parasympathetic nerves. While, in resting conditions, young women have lower muscle sympathetic activity to support blood pressure than men (32, 33). This condition is different in older women, especially in menopausal conditions, where there is an accelerated process of sympathetic activity. This explains why, in resting conditions, women's heart rates tend to be lower than men's (34).
Women typically have a poorer capacity for arterial bed vasoconstriction than males do under specific circumstances following physical activity. Following exercise, women's vascular resistance is lower than men's. This could be the reason why women's blood pressure tends to drop more quickly and effectively after exercise than men's does (35).
Second, differences in metabolism during conditions of abnormal blood pressure. Because of the cross-sectional design of this study, it is not possible to determine whether the association between blood pressure and the amount of muscle-strengthening exercise is causative or allows for a two-way relationship. The increase in blood pressure may be due to adaptation to muscle-building activities, or the individual may already have high blood pressure before beginning resistance training. Regarding the relationship between muscle strengthening exercises and blood pressure, there is some evidence indicating that there is a disturbance of skeletal muscle oxygenation during exercise in adult subjects with hypertension (34). When compared to persons without hypertension, the adult population with hypertension has diminished functional sympatholysis. It has been demonstrated that hypertension people had reduced blood flow and oxygen delivery to functioning skeletal muscles. These effects were assessed in response to lower body negative pressure both at rest and during moderately intense handgrip exercises (34).
In addition, acute weight training will have an impact on the activation of muscle fibers due to alterations in skeletal muscle metabolism that occur in people with high blood pressure. In individuals with high blood pressure, there is a shift from oxidative metabolism to predominantly glycolytic metabolism under hypoxic conditions in skeletal muscle during weight training This increased use of energy from glycolysis will change the recruitment of type II muscle fibers to be dominant over type I muscle fibers (36, 37, 38, 39). It is clearly known that the size of type II muscle fibers is relatively larger than type I. This may underlie muscle strengthening exercises associated with increased strength and muscle mass, which can also be associated with high blood pressure.
Third, resistance training reduces arterial compliance and exacerbates aortic wave reflection, especially in young subjects (40, 41). In one study, interventions in young adults showed a 20% reduction in central arterial compliance after 2 months of resistance training. The occurrence of arterial stiffness certainly plays a role in increasing blood pressure. Stiffness can occur due to an intermittent increase in arterial blood pressure. This can change the structure of the arteries, especially components that play a role in load-bearing conditions, such as connective tissue collagen and elastin. Although resistant exercise has not been shown to change intima-media thickness, it does have the potential to change the quality of the arterial wall by causing fractures of the elastic lamellae. In addition, high-intensity resistance training is a powerful stimulus to the sympathetic nervous system. Chronic increases in the sympathetic nervous system can decrease arterial compliance through chronic restraint on the arterial wall via the greater sympathetic adrenergic vasoconstrictor tone (40).
Fourth, there are non-biological factors that can affect a person's health, including how a person's reasons for doing physical activity and how a person's body responds to physical activity and produces blood pressure output (42). One of them is social appearance anxiety. Social appearance anxiety is a feeling of distress related to other people's judgments of one's physical appearance. A young population that is physically active with the aim of losing weight significantly shows greater anxiety than someone who just wants to keep fit (43). In this study, an examination was carried out related to the mental well-being of the subjects, using the WEMWBS questionnaire. Mental well-being is a condition of being happy and satisfied, with low stress levels, physically and mentally healthy, and having a good quality of life. The WEMWBS can assess mental well-being but does not assess mental disorders. In fact, both mental well-being and mental disorders can affect blood pressure (36). Given the existence of psychological factors (such as anxiety and depression) in the relationship between physical activity and health outcomes, particularly in the young adult population, it is necessary to conduct research that focuses on identifying neurobehavioral factors that investigate one's goals and perspectives in doing physical activity and their relationship to health outcomes.
In addition to these four mechanisms, this study found that cardiorespiratory fitness level played a role in the relationship between the volume of muscle-strengthening exercises and blood pressure. It is known that there is a significant positive relationship between the volume of muscle strengthening exercises and systolic blood pressure in male subjects with high blood pressure. The volume of muscle strengthening exercises and systolic blood pressure relationship was not significant in male subjects with good fitness (p: 0.1057, 95% CI: −0.0004 to 0.0040). From these results, it can be concluded that a good level of cardiorespiratory fitness has a protective effect on blood pressure in the young adult population, especially in male subjects with high blood pressure. Therefore, someone at a young age who does muscle strengthening exercises is advised to maintain cardiorespiratory fitness by doing aerobics activities as a companion to muscle strengthening exercises.
4.2. Limitation
There are two limitations to this study. First, we know that a person's cardio-metabolic state is influenced by hereditary factors. Because this study focuses on functional outcomes, especially aspects of fitness, we do not carry out tests that lead to biomarkers or genetic characteristics. Second, because this research is not an interventional study, the conclusions in this study cannot prove a definite causal relationship between the independent variable and the outcome. For future research, lab-based RCTs can be conducted to learn more about the mechanisms, or research in the form of mediation analysis of behavioral-based cluster interventions can be conducted to see a more in-depth dose-response in the population.
5. Conclusion
This study investigates the relationship between MSPA and blood pressure in a young adult population, taking into account mediators, moderators, and various covariate variables. The results show that MSPA has a significant positive direct effect on systolic blood pressure, especially in the male population with high blood pressure and low cardiorespiratory fitness. It can be estimated that every 625 min of 4 MET MSPA per week is associated with an increase in systolic blood pressure of 5 mmHg in the male population that has high blood pressure. Seeing this, when exercising, the community, especially fitness practitioners, must consider the dose of exercise that is in accordance with a person's premorbid conditions. Looking at the results of the sensitivity analysis, the possibility of a harmful effect of MSPA on blood pressure can be minimized by increasing cardiopulmonary fitness by also doing aerobic activity in addition to MSPA. In addition, functional parameters such as physical fitness do not have a mediating effect on the relationship between MSPA and blood pressure, so it is necessary to study the mechanism to explain other pathways that can explain the pathway of the relationship between MSPA volume and blood pressure.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving human participants were reviewed and approved by the medical and health research Ethics Committee of the Faculty of Medicine, Public Health, and Nursing at UGM. The patients/participants provided their written informed consent to participate in this study.
Author contributions
MMH: conceptualization, methodology, investigation, project administration, formal analysis, visualization and writing original draft, review and editing. DA: conceptualization, methodology, writing-review and supervision. RMS: conceptualization, methodology and writing-review. RAW: conceptualization, methodology, funding acquisition, writing-review. All authors contributed to the article and approved the submitted version.
Funding
This work was supported by Faculty of Medicine, Public Health and Nursing, Universitas Gadjah Mada (Grant agreement number: 324 /UN1/FKKMK/PPKE/PT/2022), Directorate of Community Services Gadjah Mada University, and The Health Promoting University Unit Gadjah Mada University.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. NCD Risk Factor Collaboration (NCD-RisC). Worldwide trends in hypertension prevalence and progress in treatment and control from 1990 to 2019: a pooled analysis of 1201 population-representative studies with 104 million participants. Lancet. (2021) 398(10304):957–80. doi: 10.1016/S0140-6736(21)01330-1
2. Tirtasari S, Kodim N. Prevalensi dan karakteristik hipertensi pada usia dewasa muda di Indonesia. Tarumanegara Med J. (2019) 1(2):395–402. doi: 10.24912/tmj.v1i2.3851
3. Wierzejska E, Giernaś B, Lipiak A, Karasiewicz M, Cofta M, Staszewski R. A global perspective on the costs of hypertension: a systematic review. Arch Med Sci. (2020) 16(5):1078–91. doi: 10.5114/aoms.2020.92689
4. Domaradzki J, Koźlenia D, Popowczak M. The mediation role of fatness in associations between cardiorespiratory fitness and blood pressure after high-intensity interval training in adolescents. Int J Environ Res Public Health. (2022) 19(3):1698. doi: 10.3390/ijerph19031698
5. Bairapareddy KC, Kamcheh MMS, Itani RJ, Mohamed M, Abdellatif ZHAE, Alaparthi GK, et al. Low physical activity levels are linked to early hypertension risk in college-going young adults. Healthcare (Basel). (2021) 9(10):1258. doi: 10.3390/healthcare9101258
6. Bennie JA, Shakespear-Druery J, De Cocker K. Muscle-strengthening exercise epidemiology: a new frontier in chronic disease prevention. Sports Medicine-Open. (2020) 6(1):1–8. doi: 10.1186/s40798-020-00271-w
7. Milton K, Varela AR, Strain T, Cavill N, Foster C, Mutrie N. A review of global surveillance on the muscle strengthening and balance elements of physical activity recommendations. J Frailty Sarcopenia Falls. (2018) 3(2):114. doi: 10.22540/JFSF-03-114
8. Dong B, Wang Z, Arnold L, Song Y, Wang HJ, Ma J. The association between blood pressure and grip strength in adolescents: does body mass index matter? Hypertens Res. (2016) 39(12):919–25. doi: 10.1038/hr.2016.84
9. Blanchard AR, Taylor BA, Thompson PD, Lepley LK, White CM, Corso LM, et al. The influence of resting blood pressure on muscle strength in healthy adults: resting blood pressure and muscle strength. Blood Press Monit. (2018) 23(4):185. doi: 10.1097/MBP.0000000000000325
10. Taekema DG, Maier AB, Westendorp RG, Craen AJ. Higher blood pressure is associated with higher handgrip strength in the oldest old. Am J Hypertens. (2011) 24(1):83–9. doi: 10.1038/ajh.2010.185
11. Hustrini NM, Susalit E, Rotmans JI. Older age is the strongest risk factors for hypertension in Indonesia: subgroup analysis of the national basic health survey 2018. J Hypertens. (2023) 41(Suppl 2):e14–5. doi: 10.1097/01.hjh.0000935624.29815.3f
12. Lim LF, Solmi M, Cortese S. Association between anxiety and hypertension in adults: a systematic review and meta-analysis. Neurosci Biobehav Rev. (2021) 131:96–119. doi: 10.1016/j.neubiorev.2021.08.031
13. Mucci N, Giorgi G, De Pasquale CS, Fiz-Pérez J, Mucci F, Arcangeli G. Anxiety, stress-related factors, and blood pressure in young adults. Front Psychol. (2016) 7:1682. doi: 10.3389/fpsyg.2016.01682
14. Fobian AD, Elliott L, Louie T. A systematic review of sleep, hypertension, and cardiovascular risk in children and adolescents. Curr Hypertens Rep. (2018) 20(5):42. doi: 10.1007/s11906-018-0841-7
15. Li C, Shang S. Relationship between sleep and hypertension: findings from the nhanes (2007-2014). Int J Environ Res Public Health. (2021) 18(15):7867. doi: 10.3390/ijerph18157867
16. Zhang K, Huang S, Feng D, Lang X, Wang Q, Liu Y. Sedentary behavioral studies of young and middle-aged adults with hypertension in the framework of behavioral epidemiology: a scoping review. Int J Environ Res Public Health. (2022) 19(24):16796. doi: 10.3390/ijerph192416796
17. Cornelissen V, Smart N. Exercise for blood pressure: a systematic review and meta-analysis. J Am Heart Assoc Cardiovasc Cerebrovasc Dis. (2013) 2(1):e004473. doi: 10.1161/jaha.112.004473
18. Lopez-Valenciano A, Ruiz-Perez I, Ayala F, Sanchez-Meca J, Vera-Garcia FJ. Updated systematic review and meta-analysis on the role of isometric resistance training for resting blood pressure management in adults. J Hypertens. (2019) 37(7):1320–33. doi: 10.1097/HJH.0000000000002022
19. Inder JD, Carlson DJ, Dieberg G, McFarlane JR, Hess NC, Smart NA. Isometric exercise training for blood pressure management: a systematic review and meta-analysis to optimize benefit. Hypertens Res. (2016) 39(2):88–94. doi: 10.1038/hr.2015.111
20. Von EE, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP. STROBE Initiative. The strengthening the reporting of observational studies in epidemiology (STROBE) statement: guidelines for reporting observational studies. J Clin Epidemiol. (2008) 61(4):344–9. doi: 10.1016/j.jclinepi.2007.11.008
21. Lee H, Cashin AG, Lamb SE, Hopewell S, Vansteelandt S, VanderWeele TJ, et al. A guideline for reporting mediation analyses of randomized trials and observational studies: the AGReMA statement. JAMA. (2021) 326(11):1045–56. doi: 10.1001/jama.2021.1407
22. Faul F, Erdfelder E, Lang AG, Buchner A. G* power 3: a flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav Res Methods. (2007) 39(2):175–91. doi: 10.3758/BF03193146
23. Maruf F, Odetunde M, Okonkwo P. Association between physical activity level and blood pressure: varied and graded mediating effects of obesity indices in schoolchildren. Cardiol Young. (2020) 30(1):82–8. doi: 10.1017/S1047951119003172
24. Shakespear-Druery J, De Cocker K, Biddle SJ, Bennie J. Muscle-strengthening exercise questionnaire (MSEQ): an assessment of concurrent validity and test-retest reliability. BMJ Open Sport Exerc Med. (2022) 8(1):e001225. doi: 10.1136/bmjsem-2021-001225
25. Ji C, Zheng L, Zhang R, Wu Q, Zhao Y. Handgrip strength is positively related to blood pressure and hypertension risk: results from the national health and nutrition examination survey. Lipids Health Dis. (2018) 17(1):1–7. doi: 10.1186/s12944-017-0646-8
26. Mänttäri A, Suni J, Sievänen H, Husu P, Vähä-Ypyä H, Valkeinen H, et al. Six-minute walk test: a tool for predicting maximal aerobic power (VO 2 max) in healthy adults. Clin Physiol Funct Imaging. (2018) 38(6):1038–45. doi: 10.1111/cpf.12525
27. Tsania ML, Wibowo RA, Sofyana M. (Unpublished). Development, validity and reliability of indonesian physical activity, sedentary behaviour and sleep (I-PASS) questionnaire among university students.
28. Stewart-Brown S, Tennant A, Tennant R, Platt S, Parkinson J, Weich S. Internal construct validity of the Warwick-Edinburgh mental well-being scale (WEMWBS): a rasch analysis using data from the Scottish health education population survey. Health Qual Life Outcomes. (2009) 7(1):15. doi: 10.1186/1477-7525-7-15
29. Rahman HA, Amornsriwatanakul A, Abdul-Mumin KH, Agustiningsih D, Chaiyasong S, Chia M, et al. Prevalence of health-risk behaviors and mental well-being of asean university students in COVID-19 pandemic. Int J Environ Res Public Health. (2022) 19(14):8528. doi: 10.3390/ijerph19148528
30. Penna C, Tullio F, Merlino A, Moro F, Raimondo S, Rastaldo R, et al. Postconditioning cardioprotection against infarct size and post-ischemic systolic dysfunction is influenced by gender. Basic Res Cardiol. (2009) 104(4):390–402. doi: 10.1007/s00395-008-0762-8
31. Batool AI, Rehman M, Unab S, Naveed N, Arshad M, Jabeen SH. Reproductive endocrinopathy among cardiovascular hypertensive patients. Saudi J Biomed Res. (2016) 1:13.
32. Christou DD, Jones PP, Jordan J, Diedrich A, Robertson D, Seals DR. Women have lower tonic autonomic support of arterial blood pressure and less effective baroreflex buffering than men. Circulation. (2005) 111(4):494–8. doi: 10.1161/01.CIR.0000153864.24034.A6
33. Schmitt JA, Joyner MJ, Charkoudian N, Wallin BG, Hart EC. Sex differences in α-adrenergic support of blood pressure. Clin Auton Res. (2010) 20(4):271–5. doi: 10.1007/s10286-010-0061-y
34. Vongpatanasin W. Autonomic regulation of blood pressure in menopause. Semin Reprod Med. (2009) 27(04):338–45. Thieme Medical Publishers. doi: 10.1055/s-0029-1225262
35. Bassareo PP, Crisafulli A. Gender differences in hemodynamic regulation and cardiovascular adaptations to dynamic exercise. Curr Cardiol Rev. (2020) 16(1):65–72. doi: 10.2174/18756557OTc0bOTciTcVY
36. Nyberg M, Gliemann L, Hellsten Y. Vascular function in health, hypertension, and diabetes: effect of physical activity on skeletal muscle microcirculation. Scand J Med Sci Sports. (2015) 25:60–73. doi: 10.1111/sms.12591
37. Gosker HR, Wouters EF, van der Vusse GJ, Schols AM. Skeletal muscle dysfunction in chronic obstructive pulmonary disease and chronic heart failure: underlying mechanisms and therapy perspectives. Am J Clin Nutr. (2000) 71(5):1033–47. doi: 10.1093/ajcn/71.5.1033
38. Jones AM, Ferguson SK, Bailey SJ, Vanhatalo A, Poole DC. Fiber type-specific effects of dietary nitrate. Exerc Sport Sci Rev. (2016) 44(2):53–60. doi: 10.1249/JES.0000000000000074
39. Boushel R. Muscle metaboreflex control of the circulation during exercise. Acta Physiol. (2010) 199(4):367–83. doi: 10.1111/j.1748-1716.2010.02133.x
40. Miyachi M, Kawano H, Sugawara J, Takahashi K, Hayashi K, Yamazaki K, et al. Unfavorable effects of resistance training on central arterial compliance: a randomized intervention study. Circulation. (2004) 110(18):2858–63. doi: 10.1161/01.CIR.0000146380.08401.99
41. Cortez-Cooper MY, DeVan AE, Anton MM, Farrar RP, Beckwith KA, Todd JS, et al. Effects of high intensity resistance training on arterial stiffness and wave reflection in women. Am J Hypertens. (2005) 18(7):930–4. doi: 10.1016/j.amjhyper.2005.01.008
42. Shahimi NH, Lim R, Mat S, Goh CH, Tan MP, Lim E. Association between mental illness and blood pressure variability: a systematic review. Biomed Eng Online. (2022) 21(1):19. doi: 10.1186/s12938-022-00985-w
Keywords: mediation analysis, physical fitness, muscle strengthening, physical activity, blood pressure, young adults
Citation: Hidayat MM, Agustiningsih D, Sabirin RM and Wibowo RA (2023) The mediation role of physical fitness in association between muscle-strengthening physical activities and its component with blood pressure among young adults: considering gender and abnormal blood pressure as moderators, moderate-vigorous physical activity, sleep behavior, sedentary behavior, mental wellbeing and BMI as covariates. Front. Cardiovasc. Med. 10:1158893. doi: 10.3389/fcvm.2023.1158893
Received: 4 February 2023; Accepted: 9 June 2023;
Published: 20 September 2023.
Edited by:
Guido Iaccarino, University of Naples Federico II, ItalyReviewed by:
Yusheng Pang, Guangxi Medical University, ChinaOyuntugs Byambasukh, Mongolian National University of Medical Sciences, Mongolia
© 2023 Hidayat, Agustiningsih, Sabirin and Wibowo. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Denny Agustiningsih ZGVubnlfYWd1c3RpbmluZ3NpaEB1Z20uYWMuaWQ=