 Jan D. Schmitto1
Jan D. Schmitto1 Aleksi Kuuva
Aleksi Kuuva Kai Kronström
Kai Kronström Esko Kankuri
Esko Kankuri
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
BRIEF RESEARCH REPORT article
Front. Cardiovasc. Med. , 28 April 2023
Sec. Heart Failure and Transplantation
Volume 10 - 2023 | https://doi.org/10.3389/fcvm.2023.1143886
This article is part of the Research Topic Methods in Treating Heart Failure - Device and Surgery Approach View all 16 articles
We report here the first clinical use of the left atrial appendage (LAA) for epicardial micrograft transplantation during left ventricular assist device (LVAD) implantation. Previously, a sample from the right atrial appendage (RAA) has been available for processing and administering micrograft therapy in cardiac surgery. Both LAA and RAA are rich sources of various types of myocardial cells and are capable of providing both paracrine and cellular support to the failing myocardium. The surgical approach of LAA micrografting facilitates epicardial micrograft therapy dose escalation and treatment of larger myocardial areas than done previously. Moreover, as collection of treated vs. untreated tissues from the recipient heart is possible following LVAD implantation at the time of heart transplantation, the evaluation of the therapy's mechanism of action can be further deciphered at cellular and molecular levels. This LAA modification of the epicardial micrografting technique has the overall potential to facilitate the adoption of cardiac cell therapy during heart surgery.
Myocardial recovery and device explantation are achieved in 3% of patients receiving mechanical circulatory support by left ventricular assist device (LVAD). It is considered that LVAD-induced cardiac unloading induces reverse cardiac remodeling, which contributes to myocardial recovery (1–4). Further possibilities for inducing structural and functional improvements in the myocardium are offered by cellular therapies, which have been under evaluation for the treatment of heart failure over two decades (5, 6). Despite controversies, cellular therapies remain under investigation for their numerous potential beneficial effects on the heart (7, 8). Theoretically, inducing myocardial regeneration at the cellular level can improve myocardial recovery after LVAD implantation. The high costs of cell therapy manufacturing, extensive culturing, dedicated facilities required, and concerns of mutations due to prolonged extensive expansion and in vitro manipulations have attracted the search for alternative possibilities to cell therapy production and administration. During LVAD implantation surgery, autologous cardiac tissue can be harvested for the purpose of cell therapy generation from, for example, atrial appendages and left ventricular tissue. Recent data have shown that epicardial transplantation of autologous right atrial appendage (RAA) micrografts is clinically safe and feasible and is associated with beneficial structural and functional effects on ischemic myocardium (9–11).
As compared to the limited amount of tissue that can be harvested from the RAA for therapy preparation, the left atrial appendage (12, 13) allows for harvesting of a substantially greater amount of tissue and thus serves as a scalable tissue source for autologous therapeutic applications. We provide here the first clinical insight into the feasibility and safety of autologous left atrial appendage (LAA) harvesting, processing, and epicardial micrograft transplantation during LVAD implantation.
A 61-year-old male patient with dilated cardiomyopathy underwent LVAD implantation as destination therapy. Prior to surgery, the patient was provided with information regarding the implantation procedure. The patient provided written informed consent for the procedure and follow-up. For the procedure, a HeartMate 3 LVAD (Abbott, Green Oaks, IL, United States) was implanted via full sternotomy. The LAA was then closed (Atriclip, Atricure Inc., Mason, OH, United States), removed, and forwarded for mechanical disaggregation and epicardial graft composition. A set of instrumentation for micrografting including a tissue processing station (EpiHeart Oy, Helsinki, Finland) and micrografting tool (HBW srl, Turin, Italy) were used.
Figure 1 illustrates LAA processing and epicardial LAA micrograft patch application. The harvested LAA tissue (∼5 g) was first cut into smaller pieces. Processing into micrografts was carried out from 1 g of LAA tissue with the micrografting tool in four 1-min cycles. Each cycle was followed by micrograft harvesting in 4 ml of cardioplegia into a 50-ml centrifugation tube. To ensure washing in an ample buffer solution volume, fresh cardioplegia was added to the tube to reach a total volume of 25 ml. After centrifugation and removal of the cardioplegia supernatant, the LAA micrograft pellet was suspended in saline-diluted (1:1) fibrinogen component of the Tisseel fibrin sealant (Tisseel, Baxter Healthcare Corp., Westlake Village, CA, United States). The micrografts were then applied onto a decellularized equine pericardium matrix sheet (Auto Tissue Berlin GmbH, Berlin, Germany) spread on a dedicated transplant holder (EpiHeart Oy). The completed transplant was placed on a cooling plate (EpiHeart Oy) on the transplant holder to minimize micrograft metabolic activity before transplantation and to allow for controlled fibrin mesh formation. Saline-diluted (1:30) thrombin component of the fibrin sealant was then used to induce the formation of a fibrin mesh gel to support and fix the LAA micrografts to the matrix sheet. At the end of surgery, the autologous LAA micrograft transplant was fixed onto the epicardial surface with four sutures.
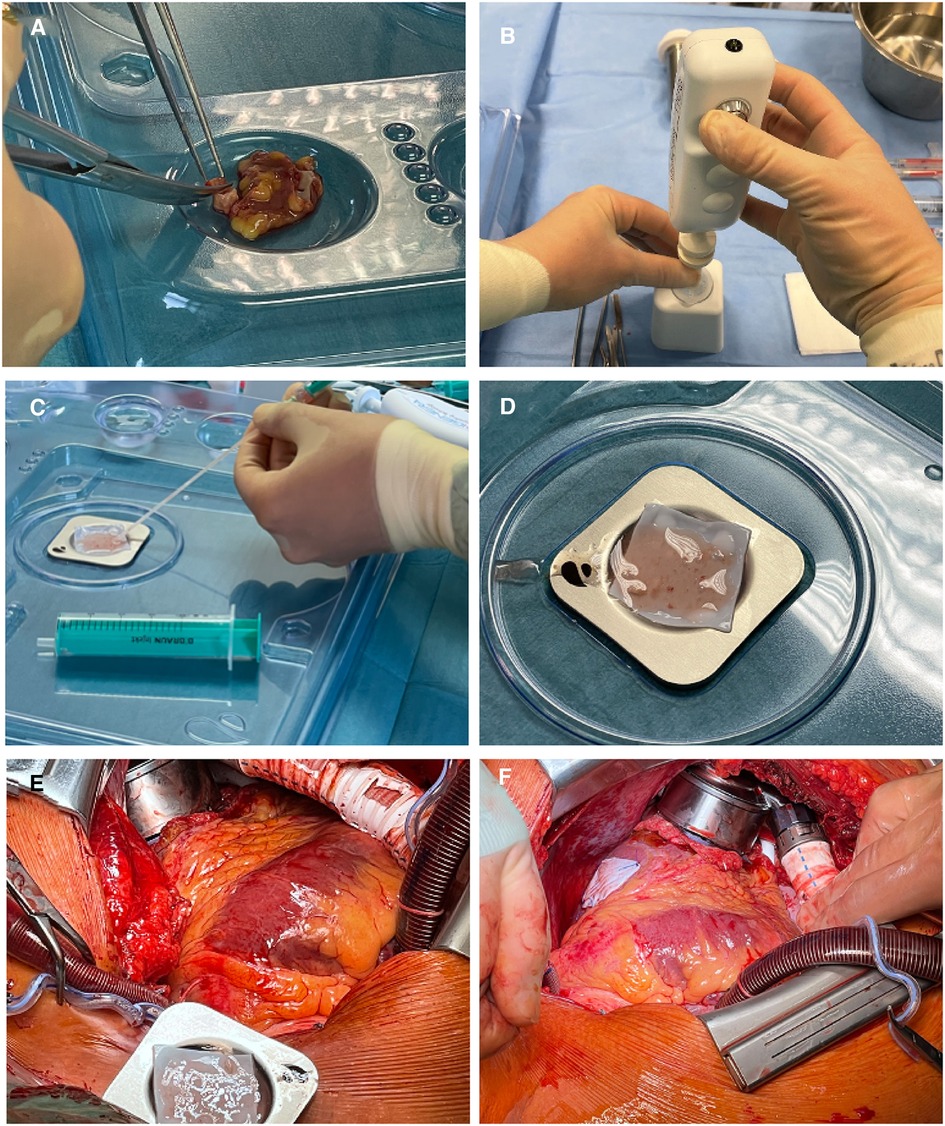
Figure 1. Left atrial appendage processing and epicardial transplantation. (A) Pieces of LAA are cut for processing. (B) Mechanical processing of LAA pieces to micrografts. (C) Application of LAA micrografts to the ECM sheet. (D) ECM sheet with LAA micrografts waiting for transplantation. (E) Transplant in transplant holder for flipping onto the epicardial surface. (F) Epicardially applied LAA micrograft patch in place on the left ventricle. LAA, left atrial appendage; ECM, extracellular matrix.
The harvesting, mechanical tissue disaggregation, and preparation of the epicardial graft was carried out in a total of 35 min. Impact of the process on the duration of surgery was an increase of 6 min: 2 min for collecting the atrial appendage and 4 min for fixing and suturing the graft in place on the epicardial surface. The postoperative course was uneventful, and the patient was discharged home on postoperative day 33 with regular outpatient follow-up after approximately 3 months.
We report here the first clinical application of intraoperative cardiac tissue micrografting using the LAA. The LAA micrograft transplant was successfully applied epicardially in conjunction with LVAD implantation. In addition to potential therapeutic benefits, this approach facilitates obtaining mechanistic proof of remodeling efficacy at functional, molecular, and structural levels using clinical imaging tools. Importantly, this protocol enables in-depth analytical comparisons of a baseline myocardial sample (available from the apical myocardium removed for LVAD implantation) with samples from treated and untreated myocardial areas available from the discarded host heart at heart transplantation. Such analyses can provide unique insights into intriguing new paracrine and cellular mechanisms of action of epicardial cellular therapies and increase our understanding on the nonthrombogenic roles of the LAA (14). Interestingly, graft-to-myocardium migration of tissue-resident macrophages was associated with myocardial healing after epicardial transplantation of LAA in a mouse model of acute myocardial infarction and heart failure (15). The contribution of graft-to-myocardium cell migration to myocardial healing will be an exciting topic for further research the autologous atrial appendage micrografts.
Similar therapy utilizing a small piece of the RAA has already been evaluated in conjunction with coronary artery bypass grafting (CABG) surgeries (9, 11). With increased amounts of tissue, for example from the LAA, available for processing, larger areas can be treated, and increased doses can be administered. Moreover, additional tissues utilizable for cell therapy are also available from cardiac surgeries. In addition to atrial appendage tissues, even leftover parts of vascular grafts at CABG surgery and apical myocardial tissue removed for the LVAD inlet at LVAD implantation are available for rapid mechanical processing to micrografts and subsequent epicardial transplantation intraoperatively. Such hybrid-tissue micrograft transplants may offer unprecedented therapeutic advances.
The adaptation of epicardial micrografting and the utilization of LAA, as presented here, offer a relatively ample autologous cardiac tissue source for surgical cell therapy. Straightforward mechanical disaggregation and available regulatory-approved devices are expected to facilitate the adoption of this cardiac cell therapy approach. This, in turn, enables further therapy optimization and provides possibilities to obtain advanced mechanistic understanding of therapy efficacy.
The original contributions presented in the study are included in the article, further inquiries can be directed to the corresponding author.
Ethical review and approval was not required for the study on human participants in accordance with the local legislation and institutional requirements. The patient/participant provided his written informed consent to participate in this study.
JDS: Conceptualization, methodology, validation, formal analysis, investigation, resources, writing—review and editing, supervision, and project administration. AK: Methodology, validation, formal analysis, investigation, data curation, writing—original draft, writing—review and editing, and visualization. KK: Conceptualization, methodology, validation, investigation, resources, writing—Original Draft, writing—review and editing, visualization, and project administration. JSH: Validation, investigation, formal analysis, data curation, and writing—review and editing. EK: Conceptualization, methodology, validation, formal analysis, writing—original draft, writing—review and editing, visualization, supervision, and project administration. All authors contributed to the article and approved the submitted version.
EpiHeart Oy and HBW srl contributed materials to this study. Open access funding was received from EpiHeart Oy. EpiHeart Oy were not involved in the study design, collection, analysis, interpretation of data, the writing of the article or the decision to submit it for publication.
EK, AK, and KK are stakeholders of EpiHeart Oy. EK is a scientific advisor for HBW srl.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
CABG, coronary artery bypass grafting; LVAD, left ventricular assist device.
1. Birks EJ. Molecular changes after left ventricular assist device support for heart failure. Circ Res. (2013) 113:777–91. doi: 10.1161/CIRCRESAHA.113.301413
2. Birks EJ, Drakos SG, Patel SR, Lowes BD, Selzman CH, Starling RC, et al. Prospective multicenter study of myocardial recovery using left ventricular assist devices (RESTAGE-HF [remission from stage D heart failure]): medium-term and primary end point results. Circulation. (2020) 142:2016–28. doi: 10.1161/CIRCULATIONAHA.120.046415
3. Topkara VK, Garan AR, Fine B, Godier-Furnémont AF, Breskin A, Cagliostro B, et al. Myocardial recovery in patients receiving contemporary left ventricular assist devices: results from the interagency registry for mechanically assisted circulatory support (INTERMACS). Circ Heart Fail. (2016) 9:e003157. doi: 10.1161/CIRCHEARTFAILURE.116.003157
4. Varshney AS, DeFilippis EM, Cowger JA, Netuka I, Pinney SP, Givertz MM. Trends and outcomes of left ventricular assist device therapy: JACC focus seminar. J Am Coll Cardiol. (2022) 79:1092–107. doi: 10.1016/j.jacc.2022.01.017
5. Lampinen M, Vento A, Laurikka J, Nystedt J, Mervaala E, Harjula A, et al. Rational autologous cell sources for therapy of heart failure—vehicles and targets for gene and RNA therapies. Curr Gene Ther. (2016) 16:21–33. doi: 10.2174/1566523216666160104141809
6. Bolli R, Solankhi M, Tang XL, Kahlon A. Cell therapy in patients with heart failure: a comprehensive review and emerging concepts. Cardiovasc Res. (2022) 118:951–76. doi: 10.1093/cvr/cvab135
7. Kankuri E, Lampinen M, Harjula A. Cellular cardiomyoplasty—challenges of a new era. Curr Tissue Eng. (2015) 4:41–6. doi: 10.2174/2211542004666150305235238
8. Marbán E. A phoenix rises from the ashes of cardiac cell therapy. Nat Rev Cardiol. (2021) 18:743–4. doi: 10.1038/s41569-021-00625-1
9. Nummi A, Mulari S, Stewart JA, Kivistö S, Teittinen K, Nieminen T, et al. Epicardial transplantation of autologous cardiac micrografts during coronary artery bypass surgery. Front Cardiovasc Med. (2021) 8:726889. doi: 10.3389/fcvm.2021.726889
10. Xie Y, Lampinen M, Takala J, Sikorski V, Soliymani R, Tarkia M, et al. Epicardial transplantation of atrial appendage micrograft patch salvages myocardium after infarction. J Heart Lung Transplant. (2020) 39:707–18. doi: 10.1016/j.healun.2020.03.023
11. Lampinen M, Nummi A, Nieminen T, Harjula A, Kankuri E. Intraoperative processing and epicardial transplantation of autologous atrial tissue for cardiac repair. J Heart Lung Transplant. (2017) 36:1020–2. doi: 10.1016/j.healun.2017.06.002
12. Verma S, Bhatt DL, Tseng EE. Time to remove the left atrial appendage at surgery: LAAOS III in perspective. Circulation. (2021) 144:1088–90. doi: 10.1161/CIRCULATIONAHA.121.055825
13. Johnson WD, Ganjoo AK, Stone CD, Srivyas RC, Howard M. The left atrial appendage: our most lethal human attachment! Surgical implications. Eur J Cardiothorac Surg. (2000) 17:718–22. doi: 10.1016/s1010-7940(00)00419-x
14. Alkhouli M, Di Biase L, Natale A, Rihal CS, Holmes DR, Asirvatham S, et al. Nonthrombogenic roles of the left atrial appendage: JACC review topic of the week. J Am Coll Cardiol. (2023) 81:1063–75. doi: 10.1016/j.jacc.2023.01.017
Keywords: autologous cardiac micrografts, cell therapy, epicardial transplantation, left ventricular assist device (LVAD), left atrial appendage (LAA), heart failure
Citation: Schmitto JD, Kuuva A, Kronström K, Hanke JS and Kankuri E (2023) Use of left atrial appendage as an autologous tissue source for epicardial micrograft transplantation during LVAD implantation. Front. Cardiovasc. Med. 10:1143886. doi: 10.3389/fcvm.2023.1143886
Received: 13 January 2023; Accepted: 10 April 2023;
Published: 28 April 2023.
Edited by:
Tomasz Zieliński, National Institute of Cardiology, PolandReviewed by:
Peter Lee, Brown University, United States© 2023 Schmitto, Kuuva, Kronström, Hanke and Kankuri. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Esko Kankuri ZXNrby5rYW5rdXJpQGhlbHNpbmtpLmZp
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.