 Agastya D. Belur
Agastya D. Belur Naresh Solankhi2
Naresh Solankhi2
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Cardiovasc. Med. , 20 June 2023
Sec. Structural Interventional Cardiology
Volume 10 - 2023 | https://doi.org/10.3389/fcvm.2023.1139360
This article is part of the Research Topic Frontiers in Cardiovascular Medicine: Rising Stars 2022 View all 75 articles
Aortic stenosis (AS) is a common valve disorder among the elderly, and these patients frequently have concomitant coronary artery disease (CAD). Risk factors for calcific AS are similar to those for CAD. Historically, the treatment of these conditions involved simultaneous surgical replacement of the aortic valve (AV) with coronary artery bypass grafting. Since the advancement of transcatheter AV therapies, there have been tremendous advancements in the safety, efficacy, and feasibility of this procedure with expanding indications. This has led to a paradigm shift in our approach to the patient with AS and concomitant CAD. Data regarding the management of CAD in patients with AS are largely limited to single-center studies or retrospective analyses. This article aims to review available literature around the management of CAD in patients with AS and assist in the current understanding in approaches toward management.
The prevalence of aortic stenosis (AS) exponentially increases with age, from 0.2% in the 50–59-year group, 1.3% in the 60–69-year group, and 3.9% in the 70–79-year group to 9.8% in those aged 80–89 years (1–3). Modifiable and non-modifiable risk factors for coronary artery disease (CAD) such as older age, smoking, obesity, diabetes, dyslipidemia, chronic renal insufficiency, and end-stage renal disease requiring dialysis have also been implicated in the pathophysiology of AS (4). Given the common risk factors, clinicians often encounter AS and CAD concurrently in approximately half of all patients undergoing transcatheter aortic valve replacement (TAVR) (5, 6). The prevalence of concomitant CAD and AS is estimated to be higher in some studies, occurring in 60% of patients undergoing surgical aortic valve replacement (SAVR) (7) and 65% among patients undergoing TAVR (8). Historically, the treatment of these conditions involved simultaneous surgical replacement of the aortic valve (AV) with coronary artery bypass grafting (CABG). The development of TAVR has brought about a paradigm shift in our approach to patients with AS. Given the lack of robust data and clinical trials on managing the patient with concomitant AS and CAD, the ideal strategy in these patients including target lesion revascularization, timing of percutaneous coronary intervention (PCI), and choice of antiplatelet/antithrombotic therapy post-TAVR is based on institutional/operator preferences vaguely guided by the data based on a retrospective analysis or relatively small single/multicenter experiences.
Given the significant overlap between the risk factors, demographic profiles, and symptoms of AS and CAD described above, it is often difficult to decipher etiology of the patient's presenting complaints. In patients with severe AS, it is imperative to evaluate the coronary anatomy to rule out obstructive CAD. This enables providers to risk-stratify patients prior to valve replacement and allows for developing a strategy of revascularization if needed.
Contrast-enhanced coronary CT angiography (CCTA) has been shown to have excellent negative predictive value in diagnosing CAD, including detection of in-stent restenosis and bypass graft stenosis of the proximal coronary artery (9–12). In light of this data, current guidelines give a class I recommendation of performing CCTA in patients who have low pretest probability of CAD undergoing workup for TAVR and class IIa recommendation of considering pre-procedural CCTA in patients with low to intermediate pretest probability of CAD who are being worked up for valve surgery (13). Further, if the renal function is normal, CCTA can be combined with CT assessment of the peripheral circulation and cardiac structure as an initial imaging test, reserving invasive coronary angiography for cases wherein CCTA is non-diagnostic or significant CAD is found on non-invasive imaging.
Current guidelines give a class I recommendation for invasive coronary angiography to define coronary anatomy and diagnose potentially severe CAD in patients with high pretest probability of CAD (14). This class I recommendation for coronary angiography prior to valve intervention is expanded to include all patients with angina, objective evidence of ischemia, left ventricular (LV) systolic dysfunction, history of CAD, and coronary risk factors (including males who are >40 years of age and postmenopausal females) if valve surgery is being considered (13).
Coronary flow reserve (CFR) is the maximal increase in myocardial blood flow above its resting level for a given perfusion pressure when coronary vasculature is maximally dilated and is used to assess coronary microcirculation. The most common causes of decreased CFR are dysfunction of myocardial microcirculation and narrowing of the epicardial arteries. AS has been shown to reduce CFR through mechanisms that are not fully understood (15). Long-term pressure overload leading to abnormally high LV workload due to AS results in a reduction of coronary blood flow at rest as well as during hyperemia and high extravascular compression of microcirculation and is thought to be the mechanism of decreased CFR in these patients (16). This limits the capacity to increase coronary circulation to match myocardial oxygen demand even in the absence of angiographic CAD and is understandably one of the key elements responsible for myocardial ischemia in patients with AS. In fact, this decrease in CFR has been implicated as a potential mechanism of anginal chest pain among patients with AS who do not have CAD. Reduced CFR has been shown to correlate better with hemodynamic indices of AS severity such as transvalvular pressure gradient and effective valve area rather than LV mass (17).
The index of microvascular resistance (IMR) is a quantitative and reproducible measurement of coronary microcirculation that can be calculated during cardiac catheterization using a pressure wire as a product of mean distal pressure and mean hyperemic transit time. Although the IMR is independent of epicardial coronary disease, it is recorded after administration of a hyperemic agent such as adenosine and may thus be susceptible to the downstream hemodynamic effects of a stenotic AV (18). This is discussed in detail below. A high IMR indicates increased coronary microvascular resistance, and this was shown to be associated with higher incidence of adverse outcomes such as death or rehospitalization with heart failure symptoms in a cohort of patients who had IMR measured during cardiac catheterization for ST-segment elevation myocardial infarction (19). In a study by Gutiérrez-Barrios et al., authors found an elevated IMR on invasive assessment and a low baseline microvascular coronary resistance in patients with AS (20). This increase in IMR under hyperemic conditions despite low baseline values may contribute to coronary microvascular dysfunction in this patient population. Severe AS may possibly contribute to the development of symptoms, LV dysfunction, and adverse outcomes seen in this patient population (21, 22), and it is up to the discretion of the providers to determine whether a patient's symptoms are from CAD, severe AS, or, as is frequently the case, a combination of both.
Coronary hemodynamics are affected by severe AS with reduced resting and peak hyperemic flow as described above. This may affect the fractional flow reserve (FFR), which is a calculated ratio between coronary pressure distal to a coronary artery stenosis and aortic pressure under conditions of maximum myocardial hyperemia by using a pressure wire to obtain these measurements. However, in a small study of 133 coronary lesions that were assessed by FFR in 54 patients with severe AS, post-TAVR variations in FFR were found to be minor (23). Authors concluded that coronary lesions deemed to be borderline by FFR might become functionally significant after valve replacement, although FFR-guided interventions were infrequent even in patients with angiographically significant lesions.
Instantaneous wave-free ratio (iFR) is measured using pressure wires, by passing them to a point distal to a stenotic lesion. iFR calculates the ratio of the distal coronary artery pressure to the pressure within the aortic outflow tract during a resting period of diastole known as the “wave-free period.” A study by Götberg et al. explored a composite of death from any cause, unplanned revascularization, and non-fatal myocardial infarction within 12 months in a cohort of 2,037 patients with stable angina or acute coronary syndrome (ACS) who were randomly assigned to undergo revascularization guided by either iFR or FFR. In these patients without AS, iFR-guided PCI was shown to be non-inferior to FFR-guided PCI (24).
A small study of 28 patients with CAD and severe AS assessed subjects using both whole-cycle hyperemic and diastolic wave-free flows. Systolic and hyperemic coronary flows were found to significantly increase post-TAVR; consequently, authors concluded that hyperemic indices such as FFR could potentially underestimate the severity of coronary stenosis in patients with severe AS. TAVR was reported to have no effect on flow during the wave-free period of diastole, suggesting that indices such as iFR that are calculated during this period are potentially free of the confounding effect of AS (16). A slightly larger study by Yamanaka et al. studied a cohort of 95 patients with severe AS, assessing 116 coronary arteries with intermediate stenosis. Authors compared iFR values with FFR values and adenosine-stress myocardial perfusion imaging as indicators of myocardial ischemia and found that both the iFR and FFR values exhibited good correlation with myocardial ischemia diagnosed on perfusion scintigraphy. The study concluded that in patients with severe AS, a good correlation exists between iFR and FFR (25).
Randomized controlled trials of functional studies of coronary artery stenosis in patients with AS are ongoing. The only available data on this topic are conflicting, derived from small, non-randomized observational studies. There are no recommendations for picking one modality over the other in current guidelines, and both modalities are deemed to be safe and feasible. A slight preference for iFR in patients with AS may be observed because it does not require the administration of a vasodilator to induce hyperemia and is theoretically less influenced by the hemodynamic effects of the stenotic AV (13).
Given that SAVR for treatment of AS has been in effect for longer than TAVR, it is understood that more robust data on the long-term effects and outcomes of CAD on patients undergoing valve surgery are found. The presence of untreated CAD has been shown to increase perioperative mortality in patients undergoing SAVR (26, 27). Further, incomplete revascularization may lead to LV systolic dysfunction and a worse postoperative survival rate when compared to patients who receive complete revascularization (13). The historical rationale for simultaneous CABG and SAVR first came from relatively small and limited early surgical data that showed patients undergoing SAVR with unrevascularized CAD had poorer long-term outcomes compared with those that had CABG (28, 29). A larger and more recent study reinforced this rationale by showing that concomitant CABG reduced the risk of late death by more than 33% without increasing operative mortality in patients undergoing SAVR with coexistent CAD (30). However, this survival benefit was seen mostly in patients who received a left internal mammary graft to the left anterior descending artery, and a similar benefit was not seen in those that had bypass grafting of the circumflex or right coronary arteries.
The impact of CAD on outcomes of TAVR is not as robust, and current data are incongruent. A meta-analysis by Sankaramangalam et al. analyzed 8,013 patients who underwent TAVR using a random-effects model. The study showed no significant difference for all-cause mortality at 30 days after TAVR between patients with and without CAD, with a cumulative odds ratio of 1.07 (95% confidence interval, 0.82–1.40; p = 0.62). However, patients in the CAD group had a significantly higher incidence of all-cause mortality at 1 year when compared with patients without CAD, with a cumulative odds ratio of 1.21 (95% confidence interval, 1.07–1.36; p = 0.002) (31). Another study by Millan-Iturbe et al. prospectively followed 944 patients with AS undergoing TAVR, of whom 224 were found to have obstructive CAD. Two-thirds of all participants underwent coronary revascularization before TAVR; half of those patients with one-vessel disease and only one-third of those with multivessel disease were completely revascularized. Long-term survival rates by Kaplan–Meier analysis of the total TAVR population at 5 and 9 years were 64.7% and 54.1%, respectively. The study concluded that in patients with or without obstructive CAD who underwent pre-TAVR revascularization, there was no difference in survival or need for revascularization post-TAVR (32). A multicenter observational study from Israel by Witberg et al. analyzed 1,270 patients with severe AS undergoing TAVR. Subjects were stratified into having no CAD, non-severe CAD defined as a SYNTAX (Synergy Between Percutaneous Coronary Intervention with Taxus and Cardiac Surgery) score of <22 and severe CAD defined as a SYNTAX score of >22. Subjects were further stratified by revascularization completeness into having “reasonable” incomplete revascularization defined as a residual SYNTAX score of <8 or incomplete revascularization defined as a residual SYNTAX score of >8. Of the 1,270 patients, 817 (64%) had no CAD, 331 (26%) had non-severe CAD, and 122 (10%) had severe CAD. When compared to patients with no CAD over a median follow-up period of 1.9 years, patients with severe CAD or incomplete revascularization had higher mortality, but no similar difference was seen in the non-severe CAD or “reasonable” incomplete revascularization groups. After multivariate adjustment, both incomplete revascularization (hazard ratio: 1.720; p = 0.031) and severe CAD (hazard ratio: 2.091; p = 0.017) were associated with increased mortality (33).
In summary, data on study findings concerning CAD treatment and TAVR are highly heterogeneous, and different definitions of CAD are used in various studies, making a comparison of results extremely difficult. A reasonable approach would be to risk-stratify patients based on the location and severity of their CAD based on a SYNTAX score and consider other factors such as concomitant comorbidities, frailty, and patient preference before having a multidisciplinary discussion to individualize a strategy for SAVR with CABG vs. TAVR with PCI vs. a hybrid approach based on all these factors, with special consideration for timing of revascularization as discussed below.
Performing PCI prior to TAVR has a potential benefit of reducing myocardial ischemia and associated adverse outcomes during and after TAVR. Patients with unrevascularized CAD are at higher risk of ischemia and hemodynamic instability during the TAVR procedure, particularly during the rapid ventricular pacing phase at the time of balloon valve dilatation and prosthesis deployment. Further, staging a PCI prior to TAVR reduces the risk of developing contrast-induced nephropathy by spacing out contrast use and avoiding a single, cumulatively higher dose of contrast that may be needed for concomitant TAVR and PCI. On the other hand, PCI requires patients to be started on dual antiplatelet therapy which may increase the risk of bleeding during TAVR, who may already be at increased risk of bleeding and adverse outcomes related to the same from AS via acquired von Willebrand syndrome, frailty, and other comorbidities. The current guidelines recommend continuing dual antiplatelet therapy prior to TAVR with no interruption for the procedure. Severe AS may increase the risk of adverse outcomes during PCI (34). Although rare, if femoral artery access is used for PCI, vascular complications at the access site may make femoral access for TAVR difficult (35).
A systematic review and meta-analysis by Bajaj et al. aimed to determine safety and feasibility of PCI in patients undergoing TAVR and identify optimal timing of revascularization (staged PCI before TAVR vs. concomitant PCI and TAVR) in this patient population. Authors found that staged PCI prior to TAVR or concomitant PCI and TAVR to treat significant CAD (defined as any >50% coronary artery stenosis) were both safe and feasible revascularization options, with no significant difference in 30-day cardiovascular events and mortality at 6 months to 1 year. Unlike the increased risk of adding SAVR to CABG, addition of PCI to TAVR conferred no additional procedural risk. In their subgroup analysis, authors found no significant difference in 30-day mortality, increased risk of life-threatening bleeding, incidence of stroke, and major access site complications between both groups. The only significant difference was a higher incidence of renal insufficiency from combined TAVR and PCI when compared to staged PCI prior to TAVR (36). An analysis of 22,344 patients using the Nationwide Inpatient Sample showed that when compared to patients who underwent only TAVR during their hospitalization, patients who underwent PCI and TAVR during the same hospitalization had higher incidence of in-hospital mortality and an increase in vascular complications (37). The ACTIVATION (PercutAneous Coronary inTervention prIor to transcatheter aortic VAlve implantaTION) trial showed similar observed rates of death and rehospitalizations at 1 year between patients who underwent PCI and no PCI prior to TAVR; however, the non-inferiority margin was not met, and PCI was associated with a higher incidence of bleeding (38). A study by van Rosendael et al. showed no significant difference in overall mortality after a median follow-up of 2 years between patients undergoing PCI within 30 days and >30 days before TAVR. However, authors reported a significant increase in minor vascular injury and bleeding complications after TAVR among patients who had PCI performed within 30 days before TAVR (39). The ongoing Danish NOTION-3 trial (40) seeks to compare outcomes between FFR-guided PCI prior to TAVR and no revascularization prior to TAVR, and its results are eagerly awaited.
The only available data on timing of PCI in patients undergoing TAVR are conflicting, with significant heterogeneity in the definition and methods of detection of CAD in the aforementioned papers. Studies have overall favored PCI prior to TAVR, showing that this method is safe and feasible (34, 36, 41), even in patients with left main CAD which needs special consideration given proximity of the left main ostium to native valve leaflets and the TAVR prosthesis (42). In patients who are unstable and have very elevated AV gradient who are consequently at high risk to undergo PCI alone or in those who have simple, uncomplicated coronary lesions or in those who have ostial lesions with high risk of coronary occlusion, combined PCI and TAVR may be an acceptable strategy (34). Current guidelines recommend an individualized, patient-centric approach to deciding the timing of PCI, including consideration of multiple clinical (presence and severity of angina, bleeding risk, ability to take dual antiplatelet therapy prior to TAVR, etc.) and anatomic (lesion location, severity and complexity, technical feasibility, etc.) factors. Staged PCI before TAVR is a common strategy, although the timing of pre-TAVR PCI remains controversial. There is a class IIa recommendation to consider revascularization with PCI before TAVR in patients with significant left main or proximal CAD with or without angina (13).
In patients undergoing PCI/TAVR, there is a preference for revascularization before valve replacement, an approach driven by the thought that critical CAD rather than symptomatic AS could be contributing to the patient's symptoms and that significant CAD could potentially lead to hemodynamic compromise during the TAVR procedure (6).
Surgical management of CAD and concomitant SAVR is not without risks. Addition of CABG to SAVR doubles the in-hospital mortality (approximately 4.4%–9%), increases cross-clamp time, and increases time spent on cardiopulmonary bypass (43, 44). Further, this may not be a feasible treatment option in patients presenting with ACS, those who are poor surgical candidates for a myriad of reasons (advanced age, renal insufficiency, severe lung disease, end-stage liver disease, cachexia, morbid obesity, peripheral artery disease, severe cerebrovascular disease, pulmonary hypertension, immunosuppression or active infection, active malignancy, and chest wall deformities, among others), those requiring valve reoperation, and those with poor or limited conduit vessels. In light of available data, the current American College of Cardiology and American Heart Association valve guidelines give a class IIa recommendation for consideration of CABG in selective patients who are undergoing any valve repair or replacement who have significant proximal CAD (≥70% reduction in luminal diameter of major coronary arteries or ≥50% reduction in luminal diameter in the left main coronary artery and/or physiological significance defined as FFR <0.8 or iFR <0.89) (13). In these patients with severe AS and significant CAD, the presence of complex bifurcation left main and/or multivessel CAD with a SYNTAX score of >33 has a class IIa recommendation for considering SAVR and CABG over TAVR and PCI (13).
Given the risks of adding CABG to SAVR, it is proposed that some patients may benefit from a hybrid treatment modality that combines PCI with SAVR. Put simply, the rationale behind this is to convert a single high-risk procedure into potentially lower-risk isolated procedures to achieve the same outcome (45). Similar to PCI before TAVR, the addition of dual antiplatelet therapy after PCI substantially increases the risk of bleeding complications during SAVR, and timing of PCI in the hybrid approach is a matter of debate. The first study to explore this treatment option was a retrospective analysis of 26 patients between 1997 and 2003 by Byrne et al. that showed that this hybrid strategy is an alternative to the CABG/SAVR approach among high-risk patients, especially those who have myocardial infarction complicated by shock. Although there was lower mortality among patients who underwent the hybrid approach, it came at the cost of increased bleeding complications and rates of blood transfusions (46). Similar results were obtained by Brinster et al., especially among older patients and those at higher risk of complications (47). In a larger study, Santana et al. retrospectively assessed 65 patients who underwent hybrid PCI with minimally invasive SAVR and matched them to 52 control patients who underwent conventional CABG/SAVR between 2005 and 2011. The median number of days between PCI and surgery was 24 (interquartile range, 2.5–37). Patients who received the hybrid approach had a significantly lower incidence of overall death, stroke, renal insufficiency, length of stay in the intensive care unit, and total length of stay in the hospital. There was no statistically significant difference in in-hospital mortality, number of units of blood transfused, incidence of post-procedure bleeding, and reoperation rates between both groups (48). Although the hybrid approach enables a multidisciplinary team of interventional cardiologists and cardiothoracic surgeons to perform PCI followed by minimally invasive valve replacement safely and without substantial risk for stent thrombosis or early restenosis despite holding antiplatelet therapy for the latter (49), there is a decreased likelihood of choosing hybrid PCI/SAVR in the current era of TAVRs and highly refined revascularization approaches.
Given the shared pathophysiology between AS and CAD discussed above, most of the coronary events occurring after TAVR are thought to be related to an atherothrombotic mechanism either via progression of CAD or failure of a PCI performed before the TAVR (50). Other potential mechanisms are thought to involve impaired coronary flow dynamics and coronary hypoperfusion related to the TAVR bioprosthesis (51) or coronary embolism related to subclinical leaflet thrombosis in bioprosthetic AV thrombosis (52).
In a cohort of 779 TAVR recipients, Vilalta et al. reported a 10% incidence of ACS after a median follow-up of about 2 years after TAVR. Of these events, 36% were due to type 2 non–ST-segment elevation myocardial infarction (NSTEMI), followed by unstable angina (35%), type 1 NSTEMI (28%), and STEMI (1%). Authors found that only 39% of these patients benefited from PCI. The all-cause mortality was reported at 37% at a median follow-up of 21 months post-ACS, with an overall poor prognosis of ACS occurring after TAVR (53). In a larger cohort of 142,845 patients who had received TAVR, Mentias et al. reported that 4.7% of the patients with ACS were admitted after a median time of 297 days (interquartile range: 85–662 days). Of these, 48% occurred within the first 6 months after TAVR. NSTEMI was found to be the most common presentation post-TAVR, one-third of whom were treated using an invasive approach. The invasive approach for the management of NSTEMI was associated with a higher risk of repeat revascularization (adjusted hazard ratio: 1.29; 95% confidence interval: 1.16–1.43; p < 0.001) but overall lower adjusted long-term mortality (adjusted hazard ratio: 0.69; 95% confidence interval: 0.66–0.73; p < 0.01). Furthermore, when compared to patients who presented with NSTEMI, patients who presented with STEMI had a higher 30-day and 1-year mortality (31.4% vs. 15.5% and 51.2% vs. 41.3%, respectively; p < 0.01). Limitations of this study included inclusion of only inpatients, so any patients who underwent elective coronary interventions as outpatients would have been excluded. Information on serum biomarker levels such as troponin and electrocardiogram tracings were not available for authors. Patients with type 2 NSTEMI were excluded from this study. Authors lacked information on drugs such as antiplatelets, anticoagulants, and statins that would affect the incidence and outcomes of ACS, and they also had no information on surgical scores, culprit lesions, coronary anatomy, success of PCI, and repeat revascularization site. The study was large and well-powered, but residual confounding could not be entirely excluded despite propensity score matching analysis to adjust for measured confounders (54). A summary of the studies performed on treatment of AS in patients with concomitant CAD (Table 1).
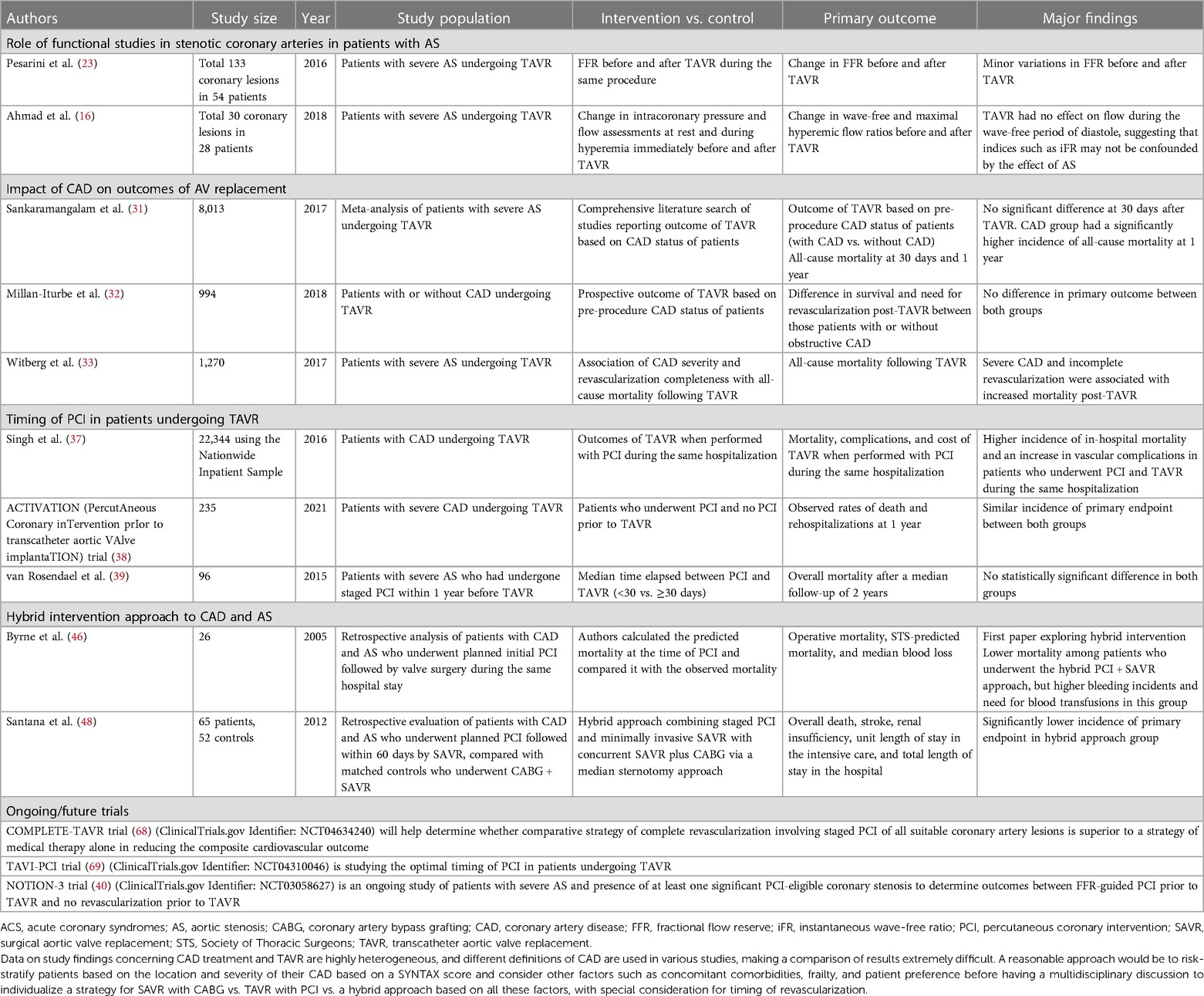
Table 1. A summary of the studies performed on treatment of AS in patients with concomitant CAD.
Although feasible and safe (55, 56), revascularization with PCI after performing TAVR comes with a unique set of procedural problems including potential prosthesis interference in cannulation of coronary ostia, especially when a supra-annular valve prosthesis is used (57). Certain prostheses may also require specialized techniques to achieve commissural alignment to be able to engage coronary ostia (58). Further, there is a concern that manipulation of catheters may potentially dislodge the TAVR prosthesis. A study from Berlin by Pasic et al. analyzed 46 patients undergoing PCI immediately after transapical TAVR. Authors treated AS as “the most proximal coronary artery stenosis” given its hemodynamic effects described above; the authors’ rationale was to fix AS with TAVR to minimize procedural complications of PCI by reducing myocardial oxygen demand. However, this study only included patients with non-complex CAD that could be fixed by single-stage, straightforward PCI. In the transapical TAVR and PCI group, survival at 12, 24, and 36 months was 87.1%, 69.7%, and 69.7%, respectively. Authors raised concerns about early stent thrombosis with acute myocardial infarction in as many as 1%–3% of patients after PCI but concluded that overall this was a safe and feasible approach to treating concomitant CAD and AS (59).
Available data are related to isolated cases and small series worldwide (42, 50, 60–65). A study by Yudi et al. recommended the systematic use of 6-French catheters, as well as selecting a femoral or left radial approach for patients with a Medtronic CoreValve system, and a femoral or radial (left or right) approach for patients with an Edwards Sapien valve. Further, authors developed a proposed catheter selection algorithm depending on the type of TAVR bioprosthesis, the type of procedure (diagnostic coronary angiogram or PCI), and the position of the transcatheter valve commissure with respect to the coronary ostium (66).
TAVR indications are expanding with younger and healthier patients being referred and successfully undergoing this procedure. In light of this, future prospective studies should evaluate revascularization strategies in TAVR patients, including comparison between FFR and iFR for lesion assessment and randomized controlled trials of SAVR with vs. without CABG (67). The COMPLETE-TAVR (68) (ClinicalTrials.gov Identifier: NCT04634240) is an ongoing randomized, multicenter trial that will help determine whether a comparative strategy of complete revascularization involving staged PCI of all suitable coronary artery lesions is superior to a strategy of medical therapy alone in reducing the composite cardiovascular outcome. The optimal timing of PCI in patients undergoing TAVR is being studied in the TAVI-PCI trial (69) (ClinicalTrials.gov Identifier: NCT04310046). Additionally, studies will need to validate the most optimal catheters for coronary angiograms and PCI in patients who need invasive management of CAD after TAVR and also determine the feasibility and failure rates for each bioprosthetic valve type.
CAD and AS are frequently encountered together, and it is of utmost importance to determine the need and methods for revascularization by a multidisciplinary team, after appropriately using a combination of invasive and non-invasive testing to risk-stratify patients. The nature and severity of the patient's symptoms and their coronary and valve anatomy often determine the best approach to treat concomitant CAD and AS. TAVR offers a safer and less invasive option for the treatment of AS compared to SAVR, and this has brought about a paradigm shift in our approach to these patients with many providers opting for a strategy that involves PCI/TAVR or PCI with minimally invasive SAVR over combined CABG/SAVR. Unfortunately, the lack of strong data has led to considerable heterogeneity in the management of these patients. As we await more definitive evidence, the collaborative efforts of a multidisciplinary team are essential to manage and optimize favorable outcomes in patients with concomitant CAD and AS.
ADB, NS, and RS: study design, literature review, and statistical analysis; data management, data analysis, and drafting the manuscript; access to the data; and final approval. NS and RS: manuscript revision, intellectual revisions, and mentorship. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
ACS, acute coronary syndrome; AS, aortic stenosis; AV, aortic valve; CABG, coronary artery bypass grafting; CAD, coronary artery disease; CCTA, contrast-enhanced coronary CT angiography; CFR, coronary flow reserve; FFR, fractional flow reserve; iFR, instantaneous wave-free ratio; LV, left ventricular; PCI, percutaneous coronary intervention; SAVR, surgical aortic valve replacement; SYNTAX, Synergy Between Percutaneous Coronary Intervention with Taxus and Cardiac Surgery; TAVR, transcatheter aortic valve replacement.
1. d'Arcy JL, Coffey S, Loudon MA, Kennedy A, Pearson-Stuttard J, Birks J, et al. Large-scale community echocardiographic screening reveals a major burden of undiagnosed valvular heart disease in older people: the OxVALVE population cohort study. Eur Heart J. (2016) 37(47):3515–22. doi: 10.1093/eurheartj/ehw229
2. Osnabrugge RL, Mylotte D, Head SJ, Van Mieghem NM, Nkomo VT, LeReun CM, et al. Aortic stenosis in the elderly: disease prevalence and number of candidates for transcatheter aortic valve replacement: a meta-analysis and modeling study. J Am Coll Cardiol. (2013) 62(11):1002–12. doi: 10.1016/j.jacc.2013.05.015
3. Coffey S, Cox B, Williams MJ. The prevalence, incidence, progression, and risks of aortic valve sclerosis: a systematic review and meta-analysis. J Am Coll Cardiol. (2014) 63(25 Pt A):2852–61. doi: 10.1016/j.jacc.2014.04.018
4. Faggiano P, Antonini-Canterin F, Baldessin F, Lorusso R, D'Aloia A, Cas LD. Epidemiology and cardiovascular risk factors of aortic stenosis. Cardiovasc Ultrasound. (2006) 4:27. doi: 10.1186/1476-7120-4-27
5. Rapp AH, Hillis LD, Lange RA, Cigarroa JE. Prevalence of coronary artery disease in patients with aortic stenosis with and without angina pectoris. Am J Cardiol. (2001) 87(10):1216–7, A7. doi: 10.1016/s0002-9149(01)01501-6
6. Walther T, Hamm CW, Schuler G, Berkowitsch A, Kötting J, Mangner N, et al. Perioperative results and complications in 15,964 transcatheter aortic valve replacements: prospective data from the GARY registry. J Am Coll Cardiol. (2015) 65(20):2173–80. doi: 10.1016/j.jacc.2015.03.034
7. Kvidal P, Bergstrom R, Horte LG, Stahle E. Observed and relative survival after aortic valve replacement. J Am Coll Cardiol. (2000) 35(3):747–56. doi: 10.1016/s0735-1097(99)00584-7
8. D'Ascenzo F, Conrotto F, Giordana F, Moretti C, D'Amico M, Salizzoni S, et al. Mid-term prognostic value of coronary artery disease in patients undergoing transcatheter aortic valve implantation: a meta-analysis of adjusted observational results. Int J Cardiol. (2013) 168(3):2528–32. doi: 10.1016/j.ijcard.2013.03.062
9. Mark DB, Berman DS, Budoff MJ, Carr JJ, Gerber TC, Hecht HS, et al. ACCF/ACR/AHA/NASCI/SAIP/SCAI/SCCT 2010 expert consensus document on coronary computed tomographic angiography: a report of the American College of Cardiology Foundation Task Force on Expert Consensus Documents. J Am Coll Cardiol. (2010) 55(23):2663–99. doi: 10.1016/j.jacc.2009.11.013
10. Opolski MP, Kim WK, Liebetrau C, Walther C, Blumenstein J, Gaede L, et al. Diagnostic accuracy of computed tomography angiography for the detection of coronary artery disease in patients referred for transcatheter aortic valve implantation. Clin Res Cardiol. (2015) 104(6):471–80. doi: 10.1007/s00392-014-0806-z
11. Andreini D, Pontone G, Mushtaq S, Bartorelli AL, Ballerini G, Bertella E, et al. Diagnostic accuracy of multidetector computed tomography coronary angiography in 325 consecutive patients referred for transcatheter aortic valve replacement. Am Heart J. (2014) 168(3):332–9. doi: 10.1016/j.ahj.2014.04.022
12. Chieffo A, Giustino G, Spagnolo P, Panoulas VF, Montorfano M, Latib A, et al. Routine screening of coronary artery disease with computed tomographic coronary angiography in place of invasive coronary angiography in patients undergoing transcatheter aortic valve replacement. Circ Cardiovasc Interv. (2015) 8(7):e002025. doi: 10.1161/CIRCINTERVENTIONS.114.002025
13. Otto CM, Nishimura RA, Bonow RO, Carabello BA, Erwin JP, Gentile F, et al. 2020 ACC/AHA guideline for the management of patients with valvular heart disease: executive summary: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. (2021) 143(5):e35–71. doi: 10.1161/CIR.0000000000000932
14. Thalji NM, Suri RM, Daly RC, Dearani JA, Burkhart HM, Park SJ, et al. Assessment of coronary artery disease risk in 5463 patients undergoing cardiac surgery: when is preoperative coronary angiography necessary? J Thorac Cardiovasc Surg. (2013) 146(5):1055–63, 1064.e1; discussion 1063–4. doi: 10.1016/j.jtcvs.2013.06.046
15. Garcia D, Camici PG, Durand LG, Rajappan K, Gaillard E, Rimoldi OE, et al. Impairment of coronary flow reserve in aortic stenosis. J Appl Physiol (1985). (2009) 106(1):113–21. doi: 10.1152/japplphysiol.00049.2008
16. Ahmad Y, Götberg M, Cook C, Howard JP, Malik I, Mikhail G, et al. Coronary hemodynamics in patients with severe aortic stenosis and coronary artery disease undergoing transcatheter aortic valve replacement: implications for clinical indices of coronary stenosis severity. JACC Cardiovasc Interv. (2018) 11(20):2019–31. doi: 10.1016/j.jcin.2018.07.019
17. Rajappan K, Rimoldi OE, Dutka DP, Ariff B, Pennell DJ, Sheridan DJ, et al. Mechanisms of coronary microcirculatory dysfunction in patients with aortic stenosis and angiographically normal coronary arteries. Circulation. (2002) 105(4):470–6. doi: 10.1161/hc0402.102931
18. Eftekhari A, Westra J, Stegehuis V, Holm NR, van de Hoef TP, Kirkeeide RL, et al. Prognostic value of microvascular resistance and its association to fractional flow reserve: a DEFINE-FLOW substudy. Open Heart. (2022) 9(1):e001981. doi: 10.1136/openhrt-2022-001981
19. Fearon WF, Low AF, Yong AS, McGeoch R, Berry C, Shah MG, et al. Prognostic value of the index of microcirculatory resistance measured after primary percutaneous coronary intervention. Circulation. (2013) 127(24):2436–41. doi: 10.1161/CIRCULATIONAHA.112.000298
20. Gutiérrez-Barrios A, Gamaza-Chulián S, Agarrado-Luna A, Ruiz-Fernández D, Calle-Pérez G, Marante-Fuertes E, et al. Invasive assessment of coronary flow reserve impairment in severe aortic stenosis and ecochadiographic correlations. Int J Cardiol. (2017) 236:370–4. doi: 10.1016/j.ijcard.2017.01.150
21. Bartel T, Yang Y, Müller S, Wenzel RR, Baumgart D, Philipp T, et al. Noninvasive assessment of microvascular function in arterial hypertension by transthoracic Doppler harmonic echocardiography. J Am Coll Cardiol. (2002) 39(12):2012–8. doi: 10.1016/s0735-1097(02)01906-x
22. McConkey HZR, Marber M, Chiribiri A, Pibarot P, Redwood SR, Prendergast BD. Coronary microcirculation in aortic stenosis. Circ Cardiovasc Interv. (2019) 12(8):e007547. doi: 10.1161/CIRCINTERVENTIONS.118.007547
23. Pesarini G, Scarsini R, Zivelonghi C, Piccoli A, Gambaro A, Gottin L, et al. Functional assessment of coronary artery disease in patients undergoing transcatheter aortic valve implantation: influence of pressure overload on the evaluation of lesions severity. Circ Cardiovasc Interv. (2016) 9(11):e004088. doi: 10.1161/CIRCINTERVENTIONS.116.004088
24. Götberg M, Christiansen EH, Gudmundsdottir IJ, Sandhall L, Danielewicz M, Jakobsen L, et al. Instantaneous wave-free ratio versus fractional flow reserve to guide PCI. N Engl J Med. (2017) 376(19):1813–23. doi: 10.1056/NEJMoa1616540
25. Yamanaka F, Shishido K, Ochiai T, Moriyama N, Yamazaki K, Sugitani A, et al. Instantaneous wave-free ratio for the assessment of intermediate coronary artery stenosis in patients with severe aortic valve stenosis: comparison with myocardial perfusion scintigraphy. JACC Cardiovasc Interv. (2018) 11(20):2032–40. doi: 10.1016/j.jcin.2018.07.027
26. Lund O, Nielsen TT, Pilegaard HK, Magnussen K, Knudsen MA. The influence of coronary artery disease and bypass grafting on early and late survival after valve replacement for aortic stenosis. J Thorac Cardiovasc Surg. (1990) 100(3):327–37. doi: 10.1016/S0022-5223(19)35524-2
27. Beach JM, Mihaljevic T, Svensson LG, Rajeswaran J, Marwick T, Griffin B, et al. Coronary artery disease and outcomes of aortic valve replacement for severe aortic stenosis. J Am Coll Cardiol. (2013) 61(8):837–48. doi: 10.1016/j.jacc.2012.10.049
28. Mullany CJ, Elveback LR, Frye RL, Pluth JR, Edwards WD, Orszulak TA, et al. Coronary artery disease and its management: influence on survival in patients undergoing aortic valve replacement. J Am Coll Cardiol. (1987) 10(1):66–72. doi: 10.1016/s0735-1097(87)80161-4
29. Czer LS, Gray RJ, Stewart ME, De Robertis M, Chaux A, Matloff JM. Reduction in sudden late death by concomitant revascularization with aortic valve replacement. J Thorac Cardiovasc Surg. (1988) 95(3):390–401. doi: 10.1016/S0022-5223(19)35758-7
30. Thalji NM, Suri RM, Daly RC, Greason KL, Dearani JA, Stulak JM, et al. The prognostic impact of concomitant coronary artery bypass grafting during aortic valve surgery: implications for revascularization in the transcatheter era. J Thorac Cardiovasc Surg. (2015) 149(2):451–60. doi: 10.1016/j.jtcvs.2014.08.073
31. Sankaramangalam K, Banerjee K, Kandregula K, Mohananey D, Parashar A, Jones BM, et al. Impact of coronary artery disease on 30-day and 1-year mortality in patients undergoing transcatheter aortic valve replacement: a meta-analysis. J Am Heart Assoc. (2017) 6(10):e006092. doi: 10.1161/JAHA.117.006092
32. Millan-Iturbe O, Sawaya FJ, Lønborg J, Chow DHF, Bieliauskas G, Engstrøm T, et al. Coronary artery disease, revascularization, and clinical outcomes in transcatheter aortic valve replacement: real-world results from the east Denmark heart registry. Catheter Cardiovasc Interv. (2018) 92(4):818–26. doi: 10.1002/ccd.27440
33. Witberg G, Regev E, Chen S, Assali A, Barbash IM, Planer D, et al. The prognostic effects of coronary disease severity and completeness of revascularization on mortality in patients undergoing transcatheter aortic valve replacement. JACC Cardiovasc Interv. (2017) 10(14):1428–35. doi: 10.1016/j.jcin.2017.04.035
34. Perez S, Thielhelm TP, Cohen MG. To revascularize or not before transcatheter aortic valve implantation? J Thorac Dis. (2018) 10(Suppl 30):S3578–87. doi: 10.21037/jtd.2018.09.85
35. Kotronias RA, Kwok CS, George S, Capodanno D, Ludman PF, Townend JN, et al. Transcatheter aortic valve implantation with or without percutaneous coronary artery revascularization strategy: a systematic review and meta-analysis. J Am Heart Assoc. (2017) 6(6):e005960. doi: 10.1161/JAHA.117.005960
36. Bajaj A, Pancholy S, Sethi A, Rathor P. Safety and feasibility of PCI in patients undergoing TAVR: a systematic review and meta-analysis. Heart Lung. (2017) 46(2):92–9. doi: 10.1016/j.hrtlng.2016.12.003
37. Singh V, Rodriguez AP, Thakkar B, Patel NJ, Ghatak A, Badheka AO, et al. Comparison of outcomes of transcatheter aortic valve replacement plus percutaneous coronary intervention versus transcatheter aortic valve replacement alone in the United States. Am J Cardiol. (2016) 118(11):1698–704. doi: 10.1016/j.amjcard.2016.08.048
38. Patterson T, Clayton T, Dodd M, Khawaja Z, Morice MC, Wilson K, et al. ACTIVATION (Percutaneous coronary inTervention prIor to transcatheter aortic VAlve implantaTION): a randomized clinical trial. JACC Cardiovasc Interv. (2021) 14(18):1965–74. doi: 10.1016/j.jcin.2021.06.041
39. van Rosendael PJ, van der Kley F, Kamperidis V, Katsanos S, Al Amri I, Regeer M, et al. Timing of staged percutaneous coronary intervention before transcatheter aortic valve implantation. Am J Cardiol. (2015) 115(12):1726–32. doi: 10.1016/j.amjcard.2015.03.019
40. Engstrom T. Revascularization in patients undergoing transcatheter aortic valve implantation (NOTION-3). Available at: https://clinicaltrials.gov/ct2/show/NCT03058627. (Accessed February 5, 2023).
41. Goel SS, Agarwal S, Tuzcu EM, Ellis SG, Svensson LG, Zaman T, et al. Percutaneous coronary intervention in patients with severe aortic stenosis: implications for transcatheter aortic valve replacement. Circulation. (2012) 125(8):1005–13. doi: 10.1161/CIRCULATIONAHA.111.039180
42. Chakravarty T, Sharma R, Abramowitz Y, Kapadia S, Latib A, Jilaihawi H, et al. Outcomes in patients with transcatheter aortic valve replacement and left main stenting: the TAVR-LM registry. J Am Coll Cardiol. (2016) 67(8):951–60. doi: 10.1016/j.jacc.2015.10.103
43. Hannan EL, Wu C, Bennett EV, Carlson RE, Culliford AT, Gold JP, et al. Risk index for predicting in-hospital mortality for cardiac valve surgery. Ann Thorac Surg. (2007) 83(3):921–9. doi: 10.1016/j.athoracsur.2006.09.051
44. Pibarot P, Dumesnil JG. Improving assessment of aortic stenosis. J Am Coll Cardiol. (2012) 60(3):169–80. doi: 10.1016/j.jacc.2011.11.078
45. Byrne JG, Leacche M, Vaughan DE, Zhao DX. Hybrid cardiovascular procedures. JACC Cardiovasc Interv. (2008) 1(5):459–68. doi: 10.1016/j.jcin.2008.07.002
46. Byrne JG, Leacche M, Unic D, Rawn JD, Simon DI, Rogers CD, et al. Staged initial percutaneous coronary intervention followed by valve surgery (“hybrid approach”) for patients with complex coronary and valve disease. J Am Coll Cardiol. (2005) 45(1):14–8. doi: 10.1016/j.jacc.2004.09.050
47. Brinster DR, Byrne M, Rogers CD, Baim DS, Simon DI, Couper GS, et al. Effectiveness of same day percutaneous coronary intervention followed by minimally invasive aortic valve replacement for aortic stenosis and moderate coronary disease (“hybrid approach”). Am J Cardiol. (2006) 98(11):1501–3. doi: 10.1016/j.amjcard.2006.08.010
48. Santana O, Funk M, Zamora C, Escolar E, Lamas GA, Lamelas J. Staged percutaneous coronary intervention and minimally invasive valve surgery: results of a hybrid approach to concomitant coronary and valvular disease. J Thorac Cardiovasc Surg. (2012) 144(3):634–9. doi: 10.1016/j.jtcvs.2011.11.008
49. Rosol Z, Vasudevan A, Sawhney R, Hebeler RF, Tecson KM, Stoler RC. Hybrid intervention approach to coronary artery and valvular heart disease. Proc (Bayl Univ Med Cent). (2020) 33(4):520–3. doi: 10.1080/08998280.2020.1784638
50. Faroux L, Guimaraes L, Wintzer-Wehekind J, Junquera L, Ferreira-Neto AN, Del Val D, et al. Coronary artery disease and transcatheter aortic valve replacement: JACC state-of-the-art review. J Am Coll Cardiol. (2019) 74(3):362–72. doi: 10.1016/j.jacc.2019.06.012
51. Ducci A, Tzamtzis S, Mullen MJ, Burriesci G. Hemodynamics in the valsalva sinuses after transcatheter aortic valve implantation (TAVI). J Heart Valve Dis. (2013) 22(5):688–96.24383382
52. Makkar RR, Fontana G, Jilaihawi H, Chakravarty T, Kofoed KF, De Backer O, et al. Possible subclinical leaflet thrombosis in bioprosthetic aortic valves. N Engl J Med. (2015) 373(21):2015–24. doi: 10.1056/NEJMoa1509233
53. Vilalta V, Asmarats L, Ferreira-Neto AN, Maes F, de Freitas Campos Guimarães L, Couture T, et al. Incidence, clinical characteristics, and impact of acute coronary syndrome following transcatheter aortic valve replacement. JACC Cardiovasc Interv. (2018) 11(24):2523–33. doi: 10.1016/j.jcin.2018.09.001
54. Mentias A, Desai MY, Saad M, Horwitz PA, Rossen JD, Panaich S, et al. Incidence and outcomes of acute coronary syndrome after transcatheter aortic valve replacement. JACC Cardiovasc Interv. (2020) 13(8):938–50. doi: 10.1016/j.jcin.2019.11.027
55. Geist V, Sherif MA, Khattab AA. Successful percutaneous coronary intervention after implantation of a CoreValve percutaneous aortic valve. Catheter Cardiovasc Interv. (2009) 73(1):61–7. doi: 10.1002/ccd.21744
56. Zajarias A, Eltchaninoff H, Cribier A. Successful coronary intervention after percutaneous aortic valve replacement. Catheter Cardiovasc Interv. (2007) 69(4):522–4. doi: 10.1002/ccd.21028
57. Barbanti M, Costa G, Picci A, Criscione E, Reddavid C, Valvo R, et al. Coronary cannulation after transcatheter aortic valve replacement: the RE-ACCESS study. JACC Cardiovasc Interv. (2020) 13(21):2542–55. doi: 10.1016/j.jcin.2020.07.006
58. Tarantini G, Nai Fovino L, Scotti A, Massussi M, Cardaioli F, Rodinò G, et al. Coronary access after transcatheter aortic valve replacement with commissural alignment: the ALIGN-ACCESS study. Circ Cardiovasc Interv. (2022) 15(2):e011045. doi: 10.1161/CIRCINTERVENTIONS.121.011045
59. Pasic M, Dreysse S, Unbehaun A, Buz S, Drews T, Klein C, et al. Combined elective percutaneous coronary intervention and transapical transcatheter aortic valve implantation. Interact Cardiovasc Thorac Surg. (2012) 14(4):463–8. doi: 10.1093/icvts/ivr144
60. Blumenstein J, Kim WK, Liebetrau C, Gaede L, Kempfert J, Walther T, et al. Challenges of coronary angiography and intervention in patients previously treated by TAVI. Clin Res Cardiol. (2015) 104(8):632–9. doi: 10.1007/s00392-015-0824-5
61. Allali A, El-Mawardy M, Schwarz B, Sato T, Geist V, Toelg R, et al. Incidence, feasibility and outcome of percutaneous coronary intervention after transcatheter aortic valve implantation with a self-expanding prosthesis. Results from a single center experience. Cardiovasc Revasc Med. (2016) 17(6):391–8. doi: 10.1016/j.carrev.2016.05.010
62. Zivelonghi C, Pesarini G, Scarsini R, Lunardi M, Piccoli A, Ferrero V, et al. Coronary catheterization and percutaneous interventions after transcatheter aortic valve implantation. Am J Cardiol. (2017) 120(4):625–31. doi: 10.1016/j.amjcard.2016.10.046
63. Boukantar M, Gallet R, Mouillet G, Belarbi A, Rubimbura V, Ternacle J, et al. Coronary procedures after TAVI with the self-expanding aortic bioprosthesis Medtronic CoreValve™, not an easy matter. J Interv Cardiol. (2017) 30(1):56–62. doi: 10.1111/joic.12363
64. Htun WW, Grines C, Schreiber T. Feasibility of coronary angiography and percutaneous coronary intervention after transcatheter aortic valve replacement using a Medtronic™ self-expandable bioprosthetic valve. Catheter Cardiovasc Interv. (2018) 91(7):1339–44. doi: 10.1002/ccd.27346
65. Tanaka A, Jabbour RJ, Testa L, Agnifili M, Ettori F, Fiorina C, et al. Incidence, technical safety, and feasibility of coronary angiography and intervention following self-expanding transcatheter aortic valve replacement. Cardiovasc Revasc Med. (2019) 20(5):371–5. doi: 10.1016/j.carrev.2019.01.026
66. Yudi MB, Sharma SK, Tang GHL, Kini A. Coronary angiography and percutaneous coronary intervention after transcatheter aortic valve replacement. J Am Coll Cardiol. (2018) 71(12):1360–78. doi: 10.1016/j.jacc.2018.01.057
67. Davidson LJ, Davidson CJ. CAD strategy in the TAVR era. Catheter Cardiovasc Interv. (2019) 93(3):553–4. doi: 10.1002/ccd.28135
68. Staged complete revascularization for coronary artery disease vs medical management alone in patients with AS undergoing transcatheter aortic valve replacement (COMPLETE TAVR). (2023). Available at: https://clinicaltrials.gov/ct2/show/NCT04634240. (Accessed February 5, 2023).
69. NCT04310046 CgI. Optimal timing of transcatheter aortic valve implantation and percutaneous coronary intervention—The TAVI PCI Trial (TAVI-PCI). (2023). Available at: https://clinicaltrials.gov/ct2/show/NCT04310046. (Accessed February 5, 2023).
Keywords: coronary artery disease, percutaneous coronary intervention, transcatheter aortic valve replacement, surgical aortic valve replacement, aortic stenosis
Citation: Belur AD, Solankhi N and Sharma R (2023) Management of coronary artery disease in patients with aortic stenosis in the era of transcatheter aortic valve replacement. Front. Cardiovasc. Med. 10:1139360. doi: 10.3389/fcvm.2023.1139360
Received: 6 January 2023; Accepted: 30 May 2023;
Published: 20 June 2023.
Edited by:
Anna Malashicheva, Institute of Cytology, RussiaReviewed by:
Damiano Regazzoli, Humanitas Research Hospital, Italy© 2023 Belur, Solankhi and Sharma. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ravi Sharma ZHJzaGFybWEucmF2aUBnbWFpbC5jb20=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.