 Thibault Schaeffer
Thibault Schaeffer Luca Koechlin1
Luca Koechlin1 Oliver Reuthebuch
Oliver Reuthebuch
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
CASE REPORT article
Front. Cardiovasc. Med. , 25 May 2023
Sec. Heart Valve Disease
Volume 10 - 2023 | https://doi.org/10.3389/fcvm.2023.1135496
This article is part of the Research Topic Case Reports in Heart Valve Disease: 2022 View all 11 articles
Structural valve deterioration (SVD) of transcatheter implanted aortic valve (TAVR) prostheses leading to prosthesis dysfunction is an uncommon yet increasingly described complication. Literature is scarce on specific mechanisms and clinical presentation of SVD after TAVR, notably on self-expanding valve ACURATE Neo. We report on two cases with severe bioprosthetic failure after ACURATE Neo implantation due to leaflet disruption, and we treated them with surgical aortic valve replacement. Based on the literature, we further discuss the incidence of SVD after TAVR, the durability of ACURATE NEO, and the modes of failure of biological valve prostheses.
Structural valve deterioration (SVD) refers to intrinsic alterations of bioprosthetic heart valves such as leaflet fibrosis and/or calcification, leaflet tear, and pannus that eventually lead to their hemodynamic dysfunction. Bioprosthetic failure (BVF) defines any clinically expressive valve dysfunction related to SVD or other conditions, such as endocarditis and prosthetic valve thrombosis, that eventually requires valve reoperation or reintervention (1). The clinical manifestation of bioprosthetic failure varies according to the severity of valve dysfunction. Literature is scarce on specific mechanisms and clinical presentation of SVD after TAVR, notably on self-expanding valve ACURATE Neo (Boston Scientific, Ecublens, Switzerland). We herein report on two cases with distinct mechanisms of SVD after ACURATE Neo implantation leading to BVF.
A 70-year-old man was implanted with ACURATE Neo (size M) for symptomatic, severe aortic valve stenosis. The procedure was unremarkable, and transthoracic echocardiography (TTE) at discharge showed a mean aortic transvalvular aortic gradient of 7 mmHg and trivial paravalvular regurgitation. Approximately 4 years (54 months) later, he presented to his regional hospital with rapidly progressive dyspnea. TTE revealed severe aortic valve regurgitation (AR). After transfer to our tertiary center, transesophageal echocardiography (TEE) demonstrated a well-seated TAVR prosthesis with severe intraprosthetic, eccentric AR (see Figures 1A,B). Transvalvular aortic gradients were slightly elevated (mean pressure gradient 18 mmHg). Blood cultures were negative. Considering the intermediate surgical risk of the patient, we opted for an emergent TAVR explant and surgical aortic valve replacement (SAVR). Intraoperative inspection of the prosthesis revealed a leaflet disruption with its adjacent strut in the noncoronary position (see Figure 1C). There were no signs of endocarditis. Extraction of the prosthesis was complicated due to extensive pannus arising from the heavily calcified native aortic valve. Due to subsequent lacerations of the aortic annulus, the aortomitral junction was reconstructed with a bovine pericardial patch, and a 23-mm stented bioprosthesis was implanted in the aortic position. The postoperative course was uneventful, and the patient was promptly discharged. After an internal review, the manufacturer was unable to identify the cause of prosthesis dysfunction. According to the manufacturer's archive, the referenced device had passed all tests during manufacturing and met all required specifications before approval for final distribution and sale.
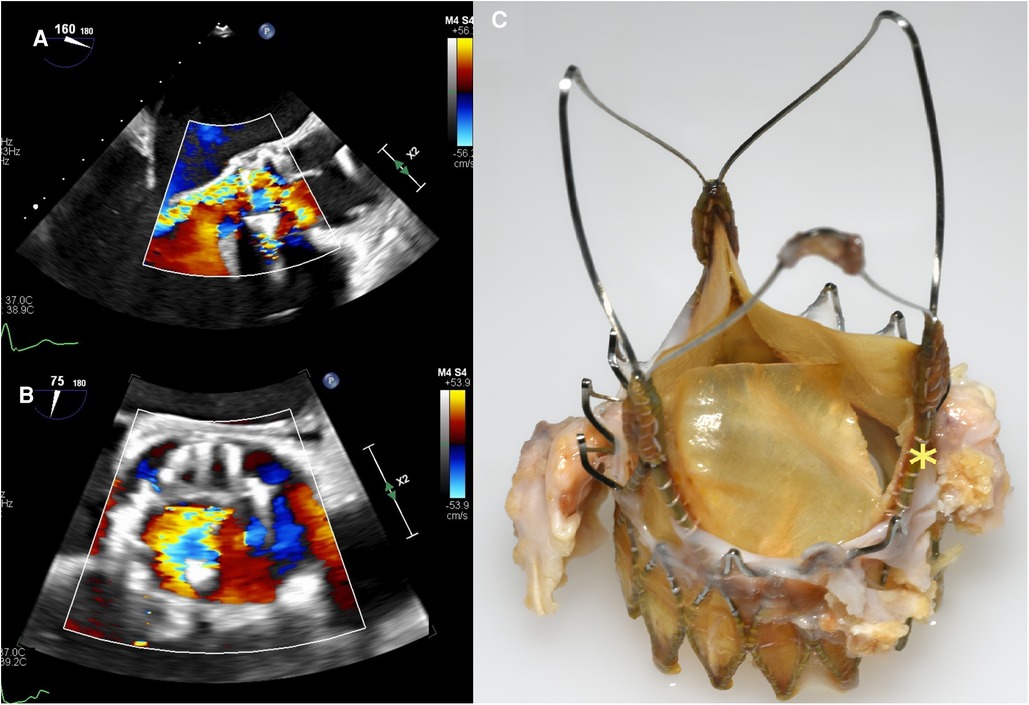
Figure 1. Case 1: transesophageal echocardiography three-chamber view with color-flow Doppler (A) and aortic valve-centered short-axis view with color-flow Doppler (B) showing an eccentric, severe intraprosthetic regurgitation. (C) Explanted ACURATE Neo prosthesis with leaflet disruption with its adjacent strut in the noncoronary position (yellow asterisk).
An 80-year-old woman was implanted with ACURATE Neo (size S) for symptomatic aortic valve stenosis. Moderate residual AR after valve deployment was immediately addressed with single balloon dilatation. TTE at discharge and at the 1-year routine control showed no significant regurgitation and low transaortic gradients. After barely 2 years (23 months), the patient complained of sudden dyspnea and medication-refractory elevated blood pressure. TTE performed by her cardiologist revealed a severe AR. TEE after admission at our center demonstrated a partial cusp prolapse on the right-coronary position associated with severe, eccentric AR (see Figures 2A,B). Blood cultures were negative. Given the intermediate surgical risk and to prevent coronary obstruction with limited coronary ostium height (13 mm on both sides), we opted for a TAVR explant and SAVR. Intraoperative inspection of the prosthesis revealed a central tear in the leaflet in the right-coronary position (see Figure 2C). There were no local signs of endocarditis. The extraction of the prosthesis was complicated due to an extensive pannus and endothelialization of the axial stabilization arches anchored in the aortic wall. After prosthesis removal, we implanted a 21-mm surgical bioprosthesis in the aortic position. The postoperative course was besides transitory acute-on-chronic renal failure uneventful, and the patient was discharged after 10 days. Cases summary as timeline is provided in Table 2.
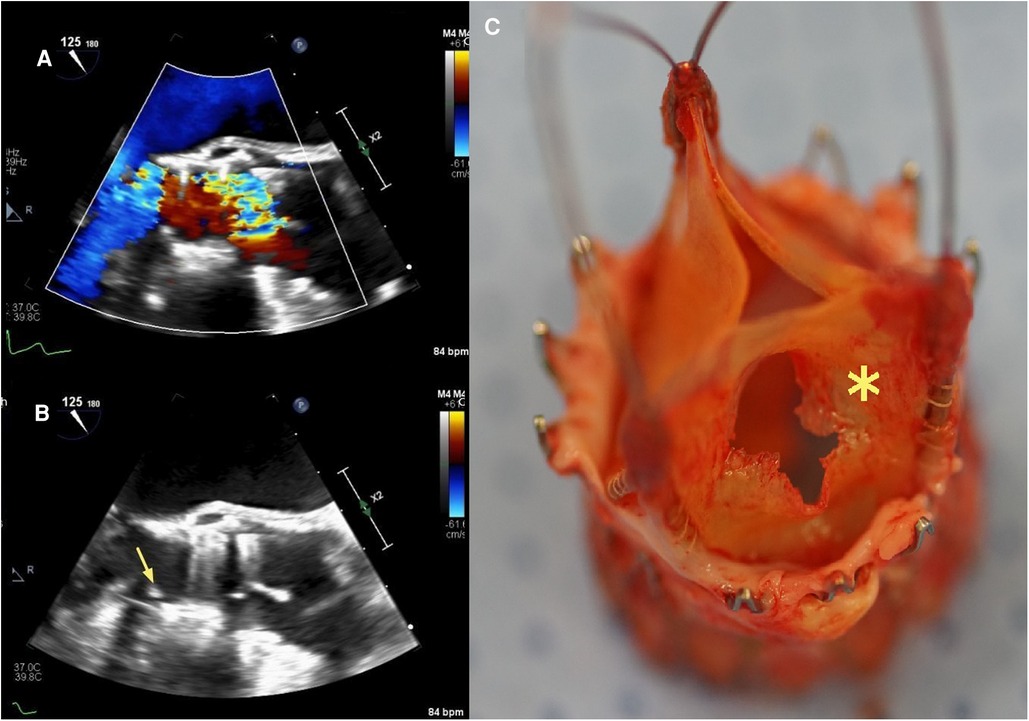
Figure 2. Case 2: transesophageal echocardiography three-chamber view with color-flow Doppler (A) and aortic valve-centered short-axis view with color-flow Doppler (B) showing severe intraprosthetic regurgitation and partial cusp prolapse (yellow arrow) on the right coronary side, respectively. (C) Explanted ACURATE Neo prosthesis with a central tear in the leaflet in the right-coronary position (yellow asterisk).
Data on specific mechanisms of SVD affecting TAVR prostheses, their incidence, and clinical presentation are limited.
The PARTNER-1 (Placement of Aortic Transcatheter Valves) trial (n = 1057) and CoreValve High-Risk Pivotal trial (n = 795) reported extremely low rates of severe SVD with 0% and 0.8% after 5 years for SAPIEN (Edwards Lifesciences, Irvine, CA, USA) and CoreValve (Medtronic, Minneapolis, MN, USA), respectively (2, 3). However, interpretation of these findings is limited due to the small number of survivors at 5 years, as predictable with typically elderly and frail patients included in these historical cohorts. With the introduction of standardized criteria for SVD, longer follow-up, and inclusion of younger, lower-risk patients in prospective TAVR trials in recent years, higher rates of SVD were reported. The NOTION (Nordic Aortic Valve Intervention) trial (n = 139), referring to the European Association of Percutaneous Cardiovascular Interventions (EAPCI), reported SVD risk after CoreValve implantation as high as 4.8% at 6 years (4). Analyzing data from the PARTNER-2A trial (n = 1438) and PARTNER-2/SAPIEN-3 Intermediate-Risk registry (n = 891) and referring to the Valve Academic Research Consortium 3 definitions, Pibarot et al. reported SVD risks of 3.9% and 9.5% at 5 years after implantation of Edwards SAPIEN 3 and Edwards SAPIEN XT, respectively (5). However, the rates of BVF were rather low (1.1% and 3.7% for Edwards SAPIEN 3 and Edwards SAPIEN XT, respectively). Also, large European retrospective cohort studies on multiple TAVR devices reported 5-year rates of SVD ranging from 2.5% to 4.2% and low rates of SVD-related BVF according to the EAPCI guidelines (6, 7). The heterogeneity of the above-mentioned rates of SVD makes their interpretation difficult and can be explained by at least two factors: first, the underestimation of the incidence of SVD given the substantial competitive risk of death in cohorts with a high mortality on short term (e.g., PARTNER-1), and second, the variability of SVD criteria according to the definitions used. An overview of SVD rates reported by the major historical randomized control trials and retrospective cohort studies focusing on TAVR durability is given in Table 1.
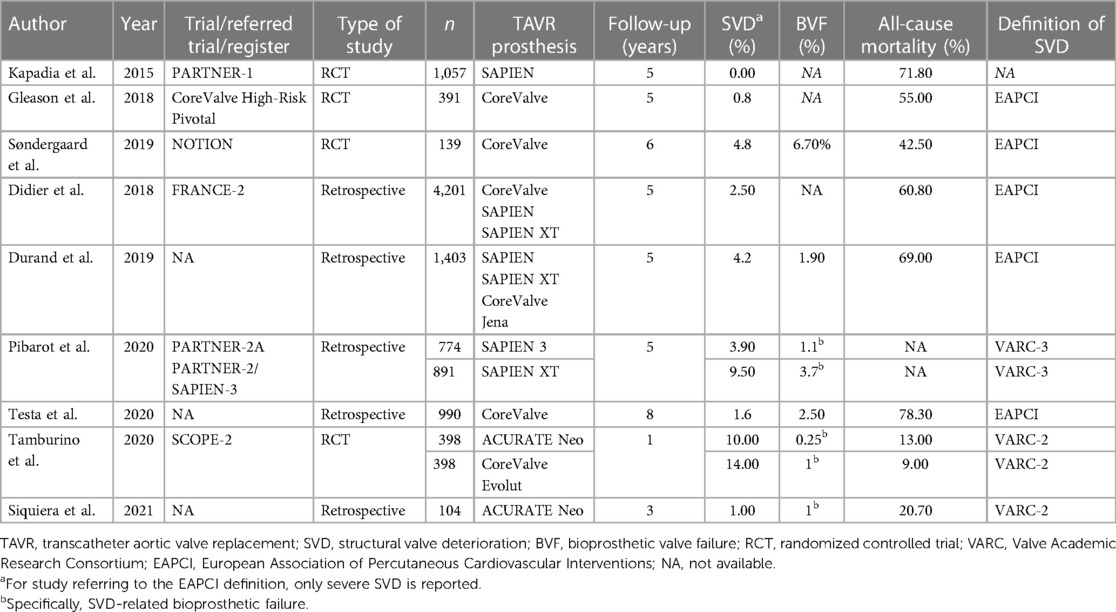
Table 1. Overview of SVD rates reported by the major historical randomized control trials and retrospective cohort studies focusing on TAVR durability.
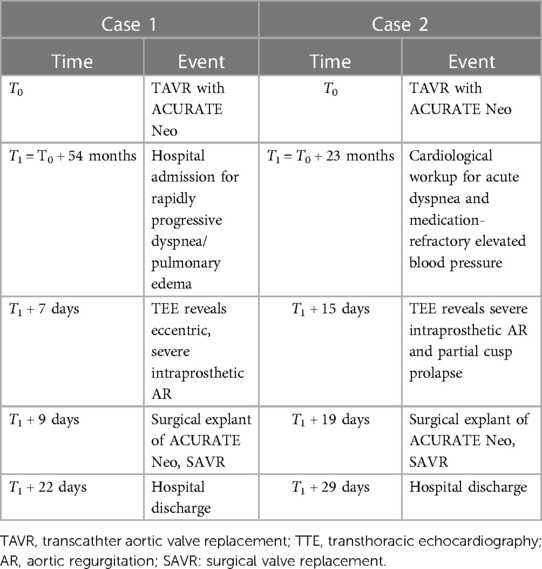
Table 2. Timeline.
When looking at surgical registries of SAVR after TAVR (n = 123 and n = 46), SVD accounted for 10%–15% of indications for TAVR explant in two recent retrospective studies (8, 9).
Since ACURATE Neo is a more recent and less implanted model of the TAVR era, less information is available about long-term outcomes and specific failure mechanisms of this device.
In the SCOPE-2 (Safety and Efficacy Comparison of Two TAVR Systems in a Prospective Randomized Evaluation 2) trial (n = 796), ACURATE Neo was challenged with its self-expandable concurrent Medtronic CoreValve Evolut (10). The authors observed more frequent cardiac deaths at 1 year (8.4% vs. 3.9%; p = 0.01), more frequent severe aortic regurgitation in the short term (10% vs. 3%, p = 0.002), and more frequent structural valve deterioration in the short term (14% vs. 6%, p = 0.004) with ACURATE Neo. However, structural valve deterioration was no more statistically different after 1 year (10% vs. 14%, p = 0.25) and the valve-related dysfunction requiring repeat procedure was similarly low in both devices (1%, p = 0.99). Reporting on mid- and long-term results after ACURATE Neo implantation (n = 104), Siquiera et al. mentioned a single case of SVD-related failure addressed with a valve-in-valve procedure (11). The authors concluded with overall reassuring mid- to long-term outcomes with this device. Findings of the SCOPE-2 trial at 1 year and those of Siquiera et al. are summarized in Table 1. In our institution, we observed a rate of SVD-related BVF of 0.84%, accounting for the two present cases over the past 5 years, which was similar to the previously mentioned studies. Finally, reviewing the international EXPLANT-TAVR registry (n = 269), Bapat et al. noticed six surgical explants of ACURATE Neo (4.5% of all self-/mechanically expandable devices), but neither the causes for explant nor the durability of the failed prostheses was specified (12).
As the number of TAVR in even younger patients increases, the need to manage late complications with TAVR will increase. The number of former implanted and available TAVR models is also increasing. As such, a better understanding of the specific mechanisms of SVD affecting TAVR prostheses is mandatory. Our two cases contribute to increasing knowledge in this area by illustrating two close but specific modes of SVD leading to acute bioprosthetic failure of the ACURATE Neo. A macroscopic examination of the valves revealed no signs of active endocarditis, and the blood cultures were negative. Eubacterial PCR from leaflet samples was not performed to exclude previous endocarditis. Leaflet tear/disruption is a rare yet well-documented mechanism of SVD of surgical bioprostheses, especially those with externally mounted leaflets (13–16). Leaflet disruption in aortic bioprosthesis occurs abruptly, and the affected patient typically presents with acute, clinically poorly tolerated aortic regurgitation, as in the two present cases. In the absence of endocarditis criteria, we assumed that the rupture of the leaflet was due to mechanical fatigue by an analogous mechanism to that affecting surgical bioprostheses. To the best of our knowledge, this issue with ACURATE Neo has never been reported.
As for therapy, we opted for TAVR explant and SAVR. Our strategy was driven in both cases by the limited experience reported with valve-in-valve procedures in failed ACURATE Neo, in the second case by the rather shallow aortic root with subsequent risk of coronary obstruction. Indeed, recent works highlighted the increased risk of coronary obstruction following redo-TAVR with high-profile index bioprosthetic valves such as ACURATE Neo (17). Further studies are warranted to define the best approach to failed TAVR prostheses with respect to the index model, mode of failure, and patient´s anatomy.
The data analyzed in this study is subject to the following licenses/restrictions: Data are available on reasonable request to the corresponding author. Requests to access these datasets should be directed tob2xpdmVyLnJldXRoZWJ1Y2hAdXNiLmNo.
Written informed consent was obtained from both participants for the publication of this case report.
TS drafted the manuscript and created the figures. All authors were involved in the conceptualization, analysis, and interpretation of the diagnostic data and the management strategy described in the manuscript and approved and co-edited the manuscript for submission in its current form. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
SVD, structural valve deterioration; BVF, bioprosthetic valve failure; TAVR, transcathter aortic valve replacement; TTE, transthoracic echocardiography; AR, aortic valve regurgitation; TEE, transesophageal echocardiography; SAVR, surgical aortic valve replacement; EAPCI, European Association of Percutaneous Cardiovascular Interventions.
1. Généreux P, Piazza N, Alu MC, Nazif T, Hahn RT, Pibarot P, et al. Valve Academic Research Consortium 3: updated endpoint definitions for aortic valve clinical research. Eur Heart J. (2021) 42(19):1825–57. doi: 10.1093/eurheartj/ehaa799
2. Kapadia SR, Leon MB, Makkar RR, Tuzcu EM, Svensson LG, Kodali S, et al. PARTNER Trial investigators. 5-year outcomes of transcatheter aortic valve replacement compared with standard treatment for patients with inoperable aortic stenosis (PARTNER 1): a randomised controlled trial. Lancet. (2015) 385(9986):2485–91. doi: 10.1016/S0140-6736(15)60290-2
3. Gleason TG, Reardon MJ, Popma JJ, Deeb M, Yakubov SJ, Lee JS, et al. 5-Year outcomes of self-expanding transcatheter versus surgical aortic valve replacement in high-risk patients. J Am Coll Cardiol. (2018) 72(22):2687–96. doi: 10.1016/j.jacc.2018.08.2146
4. Søndergaard L, Ihlemann N, Capodanno D, Jørgensen TH, Nissen H, Kjeldsen BJ, et al. Durability of transcatheter and surgical bioprosthetic aortic valves in patients at lower surgical risk. J Am Coll Cardiol. (2019) 73(5):546–53. doi: 10.1016/j.jacc.2018.10.083
5. Pibarot P, Ternacle J, Jaber WA, Salaun E, Dahou A, Asch FM, et al. Structural deterioration of transcatheter versus surgical aortic valve bioprostheses in the PARTNER-2 trial. J Am Coll Cardiol. (2020) 76(16):1830–43. doi: 10.1016/j.jacc.2020.08.049
6. Didier R, Eltchaninoff H, Donzeau-Gouge P, Chevreul K, Fajadet J, Leprince P, et al. Five-year clinical outcome and valve durability after transcatheter aortic valve replacement in high-risk patients. Circulation. (2018) 138(23):2597–607. doi: 10.1161/CIRCULATIONAHA.118.036866
7. Durand E, Sokoloff A, Urena-Alcazar M, Chevalier B, Chassaing S, Didier R, et al. Assessment of long-term structural deterioration of transcatheter aortic bioprosthetic valves using the new European definition. Circ Cardiovasc Interv. (2019) 12(4):e007597. doi: 10.1161/CIRCINTERVENTIONS.118.007597
8. Jawitz OK, Gulack BC, Grau-Sepulveda MV, Matsouaka RA, Mack MJ, Holmes DJ, et al. Reoperation after transcatheter aortic valve replacement. JACC Cardiovasc Interv. (2020) 13(13):1515–25. doi: 10.1016/j.jcin.2020.04.029
9. Brescia AA, Deeb GM, Sang SLW, Tanaka D, Grossman PM, Sukulet D, et al. Surgical explantation of transcatheter aortic valve bioprostheses: a statewide experience. Circ Cardiovasc Interv. (2021) 14(4):e009927. doi: 10.1161/CIRCINTERVENTIONS.120.009927
10. Tamburino C, Bleiziffer S, Thiele H, Scholtz S, Hildick-Smith D, Cunningtonet M, et al. Comparison of self-expanding bioprostheses for transcatheter aortic valve replacement in patients with symptomatic severe aortic stenosis: sCOPE 2 randomized clinical trial. Circulation. (2020) 142(25):2431–42. doi: 10.1161/CIRCULATIONAHA.120.051547
11. Siqueira DA, Simonato M, Ramos AA, Bignoto T, Le Bihan D, Barreto RBM, et al. Mid- to long-term clinical and echocardiographic outcomes after transcatheter aortic valve replacement with a new-generation, self-expandable system. Catheter Cardiovasc Interv. (2021) 97(1):167–74. doi: 10.1002/ccd.28999
12. Bapat VN, Zaid S, Fukuhara S, Saha S, Vitanova K, Kiefer P, et al. Surgical explantation after TAVR failure. JACC Cardiovasc Interv. (2021) 14(18):1978–91. doi: 10.1016/j.jcin.2021.07.015
13. Thiene G, Bortolotti U, Valente M, Milano A, Calabrese F, Talenti E, et al. Mode of failure of the hancock pericardial valve xenograft. Am J Cardiol. (1989) 63:129–33. doi: 10.1016/0002-9149(89)91099-0
14. Schoen FJ, Fernandez J, Gonzalez-Lavin L, Cernaianu A. Causes of failure and pathologic findings in surgically removed Ionescu-Shiley standard bovine pericardial heart valve bioprostheses: emphasis on progressive structural deterioration. Circulation. (1987) 76:618–27. doi: 10.1161/01.CIR.76.3.618
15. Luk A, Cusimano RJ, Butany J. Pathologic evaluation of 28 mitroflow pericardial valves: a 12-year experience. Ann Thorac Surg. (2015) 99:48–54. doi: 10.1016/j.athoracsur.2014.07.031
16. Schaeffer T, Berdajs D, Reuthebuch O. Early surgical aortic bioprosthesis failure caused by cusp tear: a word of caution. Clin Case Rep. (2021) 9:286–90. doi: 10.1002/ccr3.3516
Keywords: ACURATE Neo, TAVR explantation, structural valve deterioration (SVD), bioprosthesis failure, surgical aortic replacement
Citation: Schaeffer T, Koechlin L, Jeger R, Leibundgut G and Reuthebuch O (2023) Severe structural valve deterioration after TAVR with ACURATE Neo: report of two cases. Front. Cardiovasc. Med. 10:1135496. doi: 10.3389/fcvm.2023.1135496
Received: 31 December 2022; Accepted: 3 May 2023;
Published: 25 May 2023.
Edited by:
Verena Veulemans, University Hospital of Düsseldorf, GermanyReviewed by:
Francesco Giannini, Maria Cecilia Hospital, Italy© 2023 Schaeffer, Koechlin, Jeger, Leibundgut and Reuthebuch. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Oliver Reuthebuch b2xpdmVyLnJldXRoZWJ1Y2hAdXNiLmNo
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.