 Zhi-Jie Mao
Zhi-Jie Mao Wei-Wei Wen2,†
Wei-Wei Wen2,† Yi-Chen Han
Yi-Chen Han Zhou-Qing Huang
Zhou-Qing Huang Qiang-Li Xie
Qiang-Li Xie- 1The Key Laboratory of Cardiovascular Disease of Wenzhou, Department of Cardiology, The First Affiliated Hospital of Wenzhou Medical University, Wenzhou, China
- 2Department of Cardiovascular Care Unit, The First Affiliated Hospital of Wenzhou Medical University, Wenzhou, China
Objectives: The aim of this study is to assess the influence of cardiopulmonary coupling (CPC) based on RCMSE on the prediction of complications and death in patients with acute type A aortic dissection (ATAAD).
Background: The cardiopulmonary system may be nonlinearly regulated, and its coupling relationship with postoperative risk stratification in ATAAD patients has not been studied.
Methods: This study was a single-center, prospective cohort study (ChiCTR1800018319). We enrolled 39 patients with ATAAD. The outcomes were in-hospital complications and all-cause readmission or death at 2 years.
Results: Of the 39 participants, 16 (41.0%) developed complications in the hospital, and 15 (38.5%) died or were readmitted to the hospital during the two-year follow-up. When CPC-RCMSE was used to predict in-hospital complications in ATAAD patients, the AUC was 0.853 (p < 0.001). When CPC-RCMSE was used to predict all-cause readmission or death at 2 years, the AUC was 0.731 (p < 0.05). After adjusting for age, sex, ventilator support (days), and special care time (days), CPC-RCMSE remained an independent predictor of in-hospital complications in patients with ATAAD [adjusted OR: 0.8 (95% CI, 0.68–0.94)].
Conclusion: CPC-RCMSE was an independent predictor of in-hospital complications and all-cause readmission or death in patients with ATAAD.
1. Introduction
Acute type A aortic dissection (ATAAD) is a cardiovascular emergency disease that can kill 1%–2% of untreated patients every hour following the onset of symptoms (1). Despite timely emergency and essential surgery in the hospital, the in-hospital mortality and complications of patients with acute aortic dissection are still high. Fortunately, thanks to advances in surgical technology and improvements in perioperative care, mortality has decreased over the past decade to 12% (2). Therefore, it is necessary to improve risk prediction for patients with a high risk of complications and death to make timely and appropriate interventions.
The concept of cardiopulmonary coupling (CPC) was advocated in 2005 (3). CPC is now a technique that can reflect the function of cardiopulmonary system action relation and coupling strength by calculating the cross-spectral power and coherence of respiratory tidal volume fluctuations and heart rate variability (HRV) (4). It may provide information on the quantitative presentation of a person's manifestations of cardiovascular autonomic nervous function.
Since the cardiopulmonary system may be regulated in a nonlinear way, a new coupling analysis technique is needed. In recent years, the multiscale entropy (MSE) algorithm has gained massive attention, especially in the cardiovascular and physiological fields (5). Norris et al. found that heart rate (HR) MSE within hours of admission predicted mortality occurring later in 3,154 trauma patients (6). Many studies have shown that MSE is a method that can be used to generate novel clinical prognostic biomarkers.
No known research has focused on exploring the relationship between the definition of CPC based on MSE and the complications and deaths of patients with ATAAD. Therefore, we propose the following hypotheses: the cardiopulmonary coupling index based on refined composite multiscale entropy (CPC-RCMSE) can be used for successful risk stratification in ATAAD patients.
2. Methods
2.1. Study design
This was a prospective cohort study involving all patients after aortic dissection at the First Affiliated Hospital of Wenzhou Medical University from September 2018 through September 2020 (ChiCTR1800018319). The study protocol was approved by the Ethics Committee of the First Affiliated Hospital of Wenzhou Medical University.
The inclusion criteria were as follows: (1) patients aged 18–65 years; (2) patients who met the diagnostic criteria for acute type A aortic dissection and underwent surgery; and (3) patients or family members who voluntarily participated in the trial and signed informed consent. The exclusion criteria were as follows: (1) patients with chest and back deformity (including appearance and organic); (2) pacing patients; (3) patients with an ECG signal quality not up to standard; (4) patients in the terminal stage of chronic wasting disease; (5) patients in persistent coma; and (6) pregnant or nursing women.
2.2. CPC-RCMSE definitions
Electrocardiograph signals and respiratory waveforms were collected for more than 4 h on the first day after returning to the cardiac care unit. The CPC-RCMSE formula was described previously (7).
2.3. Primary outcome
The main end point was the occurrence of death, acute liver failure, acute renal failure, or ventilator-associated pneumonia composite end events in the hospital. The secondary endpoint was all-cause readmission or death at 2 years.
2.3.1. Statistical analysis
Continuous variables are expressed as the mean ± standard deviation (SD). Categorical variables are expressed as the number (percentage). Groups of continuous variables were compared using Student's t test or the Mann‒Whitney U test, and groups of categorical variables were compared using the χ2 test or Fisher's exact test.
Univariate logistic regression analysis was used to investigate the independent risk factors for the compound endpoint of complications in the hospital in patients with ATAAD. All variables significantly associated with in-hospital mortality were candidate variables in the stepwise multivariate analysis. Based on the results of the multivariate logistic regression analysis, we explored whether CPC-RCMSE is an independent predictor of complications in the hospital. A receiver operating characteristic (ROC) curve for CPC-RCMSE was generated. Survival curves were described by the Kaplan‒Meier method and compared by the log-rank test. Statistical analyses were performed by SPSS 25.0 statistical software (SPSS Company, Chicago, IL) and the R language tool. In all analyses, p < 0.05 was statistically significant.
3. Results
3.1. Baseline characteristics
In this study, patients with aortic dissection were selected. The results are presented in Table 1. The average age of the study population was 53.6 ± 10.4 years. A total of 84.6% of the participants were male, 69.2% had hypertension, 16 (41.0%) developed complications in the hospital, and 15 (38.5%) died or were readmitted to the hospital during the two-year follow-up.
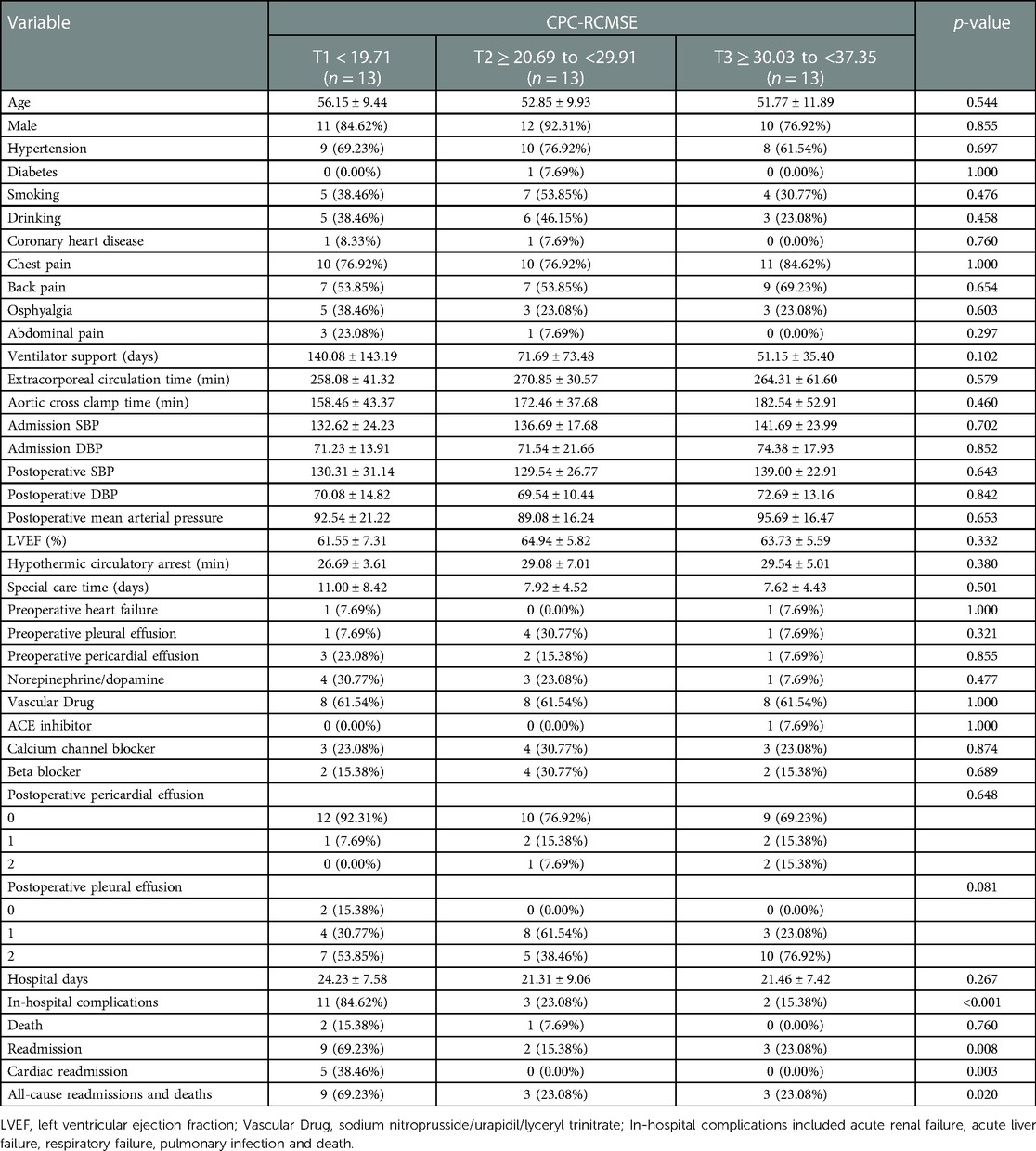
Table 1. Baseline characteristics of aortic dissection patients.
3.1.1. Independent prognostic factors
The univariate logistic analysis results are shown in Table 2. According to multivariate analysis, CPC-RCMSE was independently associated with in-hospital complications. After adjusting for age, sex, ventilator support (days), and special care time (days), CPC-RCMSE remained an independent predictor of in-hospital complications in patients with ATAAD [adjusted OR: 0.8 (95% CI, 0.68–0.94)]. In Model 2, CPC-RCMSE remained an independent risk factor for in-hospital complications after adjusting for age, sex, ventilator duration, special care time, cardioactive drugs, and vasoactive drugs [adjusted OR: 0.77 (95% CI, 0.63–0.95), p < 0.05].
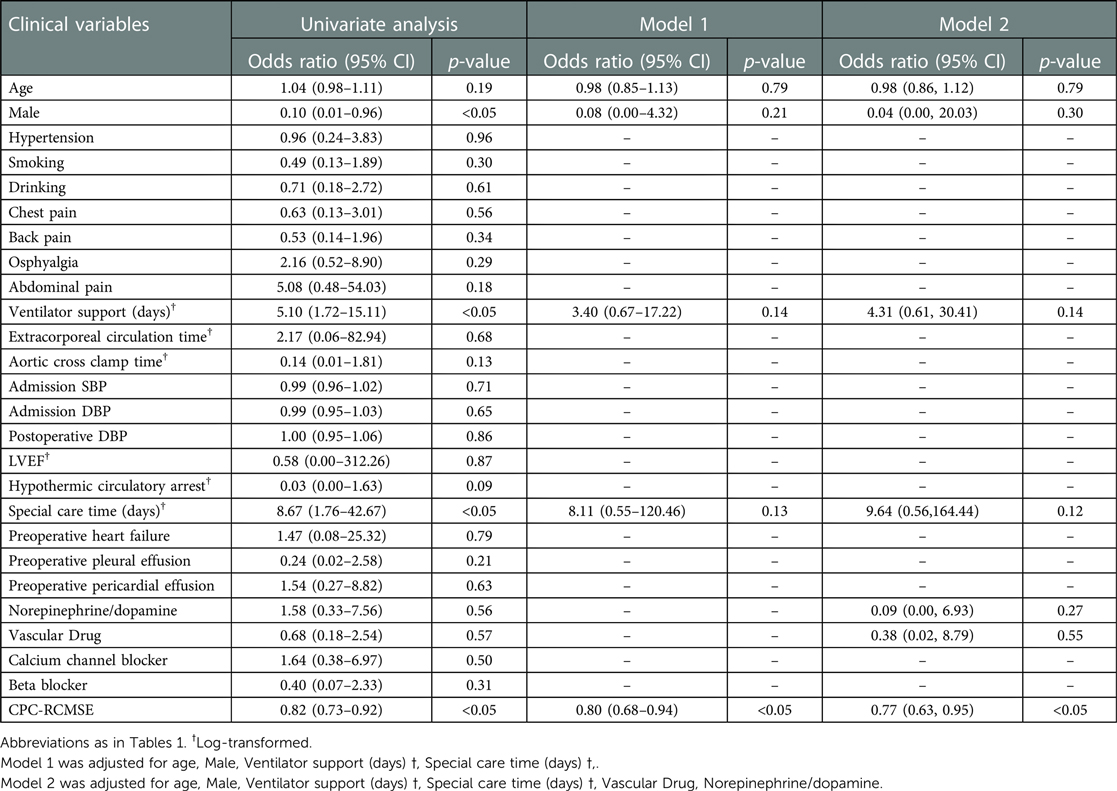
Table 2. Association of CPC-RCMSE with in-hospital complications.
3.2. ROC curve
As shown in Figure 1, when CPC-RCMSE was used to predict in-hospital complications in ATAAD patients, the AUC was 0.853 (p < 0.001). When CPC-RCMSE was used to predict all-cause readmission or death at 2 years, the AUC was 0.731 (p < 0.05).
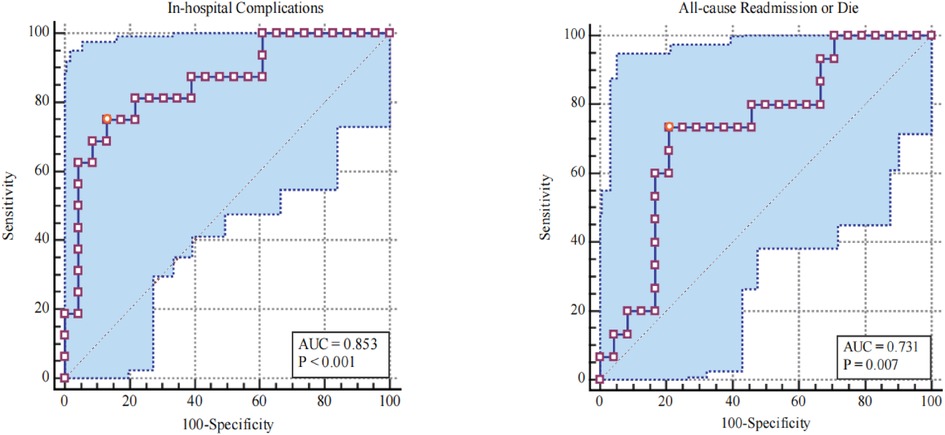
Figure 1. Receiving operating characteristic curves and corresponding AUCs for CPC-RCMSE.
3.3. Kaplan–Meier survival
As shown in Figure 2, the Kaplan‒Meier curves showed significant survival outcomes for all-cause readmission or death at 2 years by CPC-RCMSE score. In patients with a higher CPC-RCMSE score, survival was better (p < 0.0001).
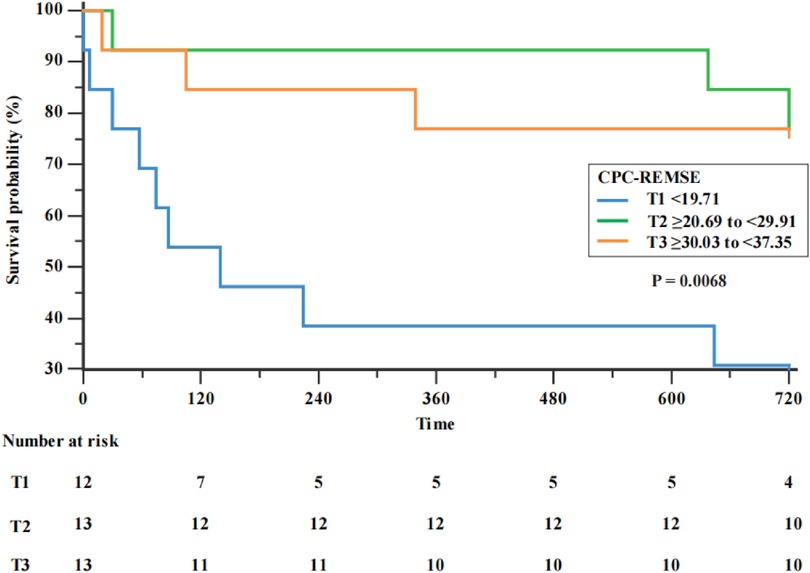
Figure 2. Kaplan–Meier survival by stage of CPC-RCMSE.
4. Discussion
In reviewing the literature, no data were found on the association between CPC-RCMSE and prognosis in ATAAD patients who have undergone surgery. Our findings highlight the prognostic importance for ATAAD. As expected, patients in the highest quintile of CPC-RCMSE had better outcomes. When CPC-RCMSE was used to predict the occurrence of postoperative complications in ATAAD patients, the AUC was 0.853 (p < 0.001), indicating that CPC-RCMSE had a good ability to predict the occurrence of complications in the hospital. When CPC complexity was ≤21.2, the sensitivity was 75%, and the specificity was 86.7%. When CPC complexity was used to predict readmission and death, the AUC was 0.731 (p < 0.05), also indicating good differentiation ability. The results of multivariate analysis indicate the clinical prediction and risk stratification value of CPC-RCMSE.
CPC (3) is based on continuous ECG signals and uses Fourier transform technology to analyze two characteristics of the signal: (1) heart rate variation and (2) the fluctuation of ECG R wave amplitude caused by respiration. From a physiological point of view, CPC can identify the bistable properties of automatic NREM sleep state transitions. One state shows deep sleep features, and the other state exhibits shallow sleep features. Many studies (8, 9) have reported its clinical significance, such as the 24-hour Holter-based CPC analysis (10), which showed that the recurrence rate was lower in atrial fibrillation patients who had unstable sleep before radiofrequency ablation (HR: 0.32; 95% CI, 0.12–0.83).
The cardiopulmonary system likely performs complex regulation in a nonlinear manner. The development of nonlinear dynamics and information theory has made new progress in the study of information transmission among multivariate time series and can complement traditional linear symmetry analysis technology to provide more diagnostic and prognostic information (11, 12). Costa et al. (13) proposed an MSE algorithm to calculate SampEn over a certain scale to represent the complexity of a time series. Pilatia et al. (14) described the application of the MSE algorithm to cardiopulmonary coupling. In our study, we used new algorithms. The RCMSE algorithm reduces the chance of generating indefinite entropy and is more suitable for the application of short time series analysis, such as physiological time series (7). Our study provide evidence for CPC-RCMSE on the prediction of complications and death in patients with ATAAD. Notably, many algorithms have proved to have advantages in the analysis of physiological signals in different study population. In terms of Congestive Heart Failure patients, Liu C et al. (15) determined the differential RR interval time series signal (MSE_dRR) had better statistical stability and better discrimination. Azami H. et al. (16) points out that Refined Composite Dispersion Entropy (RCMDE) increased ability to find differences between physiological signs better than RCMSE. However, the above algorithm has not been tested in ATAAD patients. For this reason, we expect compare the advantages and disadvantages of different algorithms in ATAAD patients with larger samples in future studies.
The results of our study indicated that CPC-RCMSE was an independent risk factor for ATAAD. ATAAD patients were divided into three groups according to their CPC-RCMSE (T1 < 19.71; T2 ≥ 20.69 to <29.91; T3 ≥ 30.03 to <37.35). The Kaplan‒Meier curves showed significant survival outcomes for all-cause readmission or death at 2 years by CPC-RCMSE score. In patients with lower CPC-RCMSE scores, survival was worse (p < 0.0001).
Additionally, we found that CPC-RCMSE was a strong independent predictor associated with in-hospital complications in our study population. When CPC complexity increased by 1 unit, the risk of hospital complications decreased by 20%. Clinical health care workers can be more targeted in meeting patient needs based on CPC-RCMSE scores to improve medical efficiency, shorten hospital stay, reduce care unit costs, and improve patient hospitalization outcomes.
5. Conclusions
CPC-RCMSE is an independent predictor of in-hospital complications in patients with ATAAD. CPC-RCMSE should be used more widely and routinely in the risk stratification of ATAAD patients.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving human participants were reviewed and approved by Human Ethics Committee of the First Affiliated Hospital of Wenzhou Medical University. The patients/participants provided their written informed consent to participate in this study.
Author contributions
Mao Z-J and Wen W-W: wrote the first draft of the manuscript. Han Y-C, Shen L-j and Dong W-h: performed data collection and follow-up. Mao Z-J and Xie Q-L contributed to the study design. Huang Z-Q and Xie Q-L guided the subsequent revisions of this article. All authors contributed to the article and approved the submitted version.
Funding
This work was supported by Zhejiang Province science and technology plan projects: grant no. 2019KY451.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Gawinecka J, Schönrath F, von Eckardstein A. Acute aortic dissection: pathogenesis, risk factors and diagnosis. Swiss Med Wkly. (2017) 147:w14489. doi: 10.4414/smw.2017.14489
2. Conway BD, Stamou SC, Kouchoukos NT, Lobdell KW, Khabbaz KR, Murphy E, et al. Improved clinical outcomes and survival following repair of acute type A aortic dissection in the current era. Interact Cardiovasc Thorac Surg. (2014) 19:971–6. doi: 10.1093/icvts/ivu268
3. Thomas RJ, Mietus JE, Peng CK, Goldberger AL. An electrocardiogram-based technique to assess cardiopulmonary coupling during sleep. Sleep. (2005) 28:1151–61. doi: 10.1093/sleep/28.9.1151
4. Lu M, Penzel T, Thomas RJ. Cardiopulmonary coupling. Adv Exp Med Biol. (2022) 1384:185–204. doi: 10.1007/978-3-031-06413-5_11
5. Thuraisingham RA, Gottwald GA. On multiscale entropy analysis for physiological data. Phys A: Stat Mech Appl. (2006) 366:323–32. doi: 10.1016/j.physa.2005.10.008
6. Riordan WP Jr, Norris PR, Jenkins JM, Morris JA Jr. Early loss of heart rate complexity predicts mortality regardless of mechanism, anatomic location, or severity of injury in 2178 trauma patients. J Surg Res. (2009) 156:283–9. doi: 10.1016/j.jss.2009.03.086
7. Wu S-D, Wu C-W, Lin S-G, Lee K-Y, Peng C-K. Analysis of complex time series using refined composite multiscale entropy. Phys Lett A. (2014) 378:1369–74. doi: 10.1016/j.physleta.2014.03.034
8. Sun QM, Xing L, Wang C, Liang W. Cardiopulmonary coupling analysis predicts early treatment response in depressed patients: a pilot study. Psychiatry Res. (2019) 276:6–11. doi: 10.1016/j.psychres.2019.04.002
9. Choi JH, Thomas RJ, Suh SY, Park IH, Kim TH, Lee SH, et al. Sleep quality change after upper airway surgery in obstructive sleep apnea: electrocardiogram-based cardiopulmonary coupling analysis. Laryngoscope. (2015) 125:1737–42. doi: 10.1002/lary.25101
10. Kim W, Na JO, Thomas RJ, Jang WY, Kang DO, Park Y, et al. Impact of catheter ablation on sleep quality and relationship between sleep stability and recurrence of paroxysmal atrial fibrillation after successful ablation: 24-hour holter-based cardiopulmonary coupling analysis. J Am Heart Assoc. (2020) 9:e017016. doi: 10.1161/JAHA.120.017016
11. Pincus SM. Approximate entropy as a measure of system complexity. Proc Natl Acad Sci U S A. (1991) 88:2297–301. doi: 10.1073/pnas.88.6.2297
12. Metin Akay. “Nonlinear Behavior of Heart Rate Variability as Registered after Heart Transplantation,” in Nonlinear Biomedical Signal Processing, Dynamic Analysis and Modeling, IEEE, 2000, pp. 133–158, doi: 10.1109/9780470545379.ch5
13. Costa M, Goldberger AL, Peng CK. Multiscale entropy analysis of complex physiologic time series. Phys Rev Lett. (2002) 89:068102. doi: 10.1103/PhysRevLett.89.068102
14. Platiša MM, Radovanović NN, Kalauzi A, Milašinović G, Pavlović SU. Multiscale entropy analysis: application to cardio-respiratory coupling. Entropy (Basel, Switzerland) (2020) 22(9):1042. doi: 10.3390/e22091042
15. Liu C, Gao R. Multiscale entropy analysis of the differential RR interval time series signal and its application in detecting congestive heart failure. Entropy. (2017) 19:251. doi: 10.3390/e19060251
Keywords: cardiopulmonary coupling, acute type a aortic dissection, prognostication, composite multiscale entropy, risk stratification
Citation: Mao Z, Wen W, Han Y, Dong W, Shen L, Huang Z and Xie Q (2023) Use of the cardiopulmonary coupling index based on refined composite multiscale entropy for prognostication of acute type A aortic dissection. Front. Cardiovasc. Med. 10:1126889. doi: 10.3389/fcvm.2023.1126889
Received: 18 December 2022; Accepted: 20 February 2023;
Published: 8 March 2023.
Edited by:
Xiangjiu Ding, Shandong University, ChinaReviewed by:
Giampiero Esposito, Monzino Cardiology Center (IRCCS), ItalyCai Cheng, Huazhong University of Science and Technology, China
© 2023 Mao, Wen, Han, Dong, Shen, Huang and Xie. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Qiang-Li Xie eGllcWlhbmdsaUAxNjMuY29t
†These authors have contributed equally to this work
Specialty Section: This article was submitted to Aortic Surgery and Endovascular Repair, a section of the journal Frontiers in Cardiovascular Medicine