 Yunxi Li
Yunxi Li Jianglin Liu
Jianglin Liu Minmin Wang1
Minmin Wang1 Haizhao Zhao
Haizhao Zhao Cuifen Zhao
Cuifen Zhao
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Cardiovasc. Med. , 17 March 2023
Sec. Pediatric Cardiology
Volume 10 - 2023 | https://doi.org/10.3389/fcvm.2023.1091778
Background and objective: Syncope is a common emergency with diverse etiologies in children. Among these, cardiac syncope (CS) is associated with high mortality and is usually difficult to diagnose. However, there is still no validated clinical prediction model to distinguish CS from other forms of pediatric syncope. The Evaluation of Guidelines in Syncope Study (EGSYS) score was designed to identify CS in adults and has been validated in several studies. In this study, we aimed to assess the ability of the EGSYS score in predicting CS in children.
Methods: In this retrospective study, we calculated and analyzed the EGSYS scores of 332 children hospitalized for syncope between January 2009 and December 2021. Among them, 281 were diagnosed with neurally mediated syncope (NMS) through the head-up tilt test, and 51 were diagnosed with CS using electrocardiography (ECG), echocardiography (ECHO), coronary computed tomography angiography (CTA), myocardial enzymes and genetic screening. The receiver operating characteristic (ROC) curve and Hosmer-Lemeshow test were used to evaluate the predictive value of the EGSYS score system.
Results: The median scores of 51 children with CS and 281 children with NMS were 4 [interquartile range (IQR): 3-5] and −1 (IQR: -2-1), respectively. The area under the ROC curve (AUC) was 0.922 [95% confidence interval (CI): 0.892-0.952; P < 0.001], indicating that the EGSYS score system has good discrimination. The best cutoff point was ≥3, with a sensitivity and specificity of 84.3% and 87.9%, respectively. The Hosmer-Lemeshow test demonstrated satisfactory calibration (χ²=1.468, P > 0.05) of the score, indicating a good fit of the model.
Conclusion: The EGSYS score appeared to be sensitive for differentiating CS from NMS in children. It might be used as an additional diagnostic tool to aid pediatricians in accurately identifying children with CS in the clinical practice.
Syncope is a transient loss of consciousness (TLOC) and postural tone due to cerebral hypoperfusion followed by rapid and spontaneous complete recovery. Syncope is estimated to occur in approximately 50% of the general population during their lifetime (1). As one of the most common emergencies, syncope accounts for approximately 1% of pediatric emergency department visits (2). There are three major classifications of syncope in children and adolescence: neurally mediated syncope (NMS), cardiac syncope (CS), and unexplained syncope. NMS includes vasovagal syncope (VVS), postural tachycardia syndrome (POTS), orthostatic hypotension (OH), and orthostatic hypertension (OHT). NMS are mostly benign with the main threats leading to syncope-related body injuries or psychological problems (3, 4). However, CS may be associated with a high risk of sudden cardiac death or other adverse events especially in those caused by life-threatening arrhythmia or structural cardiac disease (5–7). Therefore, children with CS require early diagnosis and urgent disease-specific therapy to improve their prognosis.
Nearly 50% of cases can be diagnosed using a detailed patient history, physical examination, and electrocardiography (ECG) (8). However, several studies have shown that the hospital admission rate and medical costs remain high for patients with syncope due to concerns about underlying cardiac disease (9, 10). On the other hand, children with CS especially those caused by a malignant arrhythmia, may have no distinctive abnormal manifestations after syncopal episodes resulting in difficulties in timely diagnosis.
To help triage and manage patients with syncope in the emergency department, Del Rosso et al. (11) developed the Evaluation of Guidelines in Syncope Study (EGSYS) score which is a clinical risk-scoring system to differentiate CS from non-CS. Although this model has been validated in several studies in adults (12–16), whether or not the EGSYS score can be used to identify CS in children is unknown. A recent study by Környei et al. (17) showed that the EGSYS score identified cardiac causes in seven of eight arrhythmic patients with syncope, suggesting the usefulness of the EGSYS score in children with syncope of arrhythmic origin. However, this score has not been tested in other types of pediatric syncope.
In this study, we calculated and analyzed the EGSYS scores of 332 children with syncope of different causes and assessed the predictive value of EGSYS score for the differential diagnosis between CS and NMS in children.
This retrospective observational cohort study was conducted at a large tertiary hospital, Qilu Hospital of Shandong University, between January 2009 and December 2021. We reviewed the clinical data of all children with syncope obtained from our hospital's electronic information system. Subsequently, we included those (a) between the ages of 0 and 18; and (b) diagnosed with NMS and CS, and excluded those (a) with unexplained syncope; (b) incomplete or missing crucial medical records; and (c) TLOC caused by epilepsy, hypoglycemia, hyperventilation, intoxication, hypoxia, transient ischemic attacks, or psychological factors. Finally, 332 children with syncope were included in this study. The diagnostic criteria for NMS and CS were based on the Chinese Pediatric Cardiology Society (CPCS) guidelines for the diagnosis and treatment of syncope (18–20) and European Society of Cardiology (ESC) guidelines for the diagnosis and management of syncope (1, 21).
The data were collected based on the medical records during hospitalizations and included the demographic data (age, sex), medical history, physical examination; the results of 12-lead ECG, 24 hour Holter monitor, and echocardiograph (ECHO). A detailed medical history included the predisposing factors, prodromes, duration of loss of consciousness, family history, and past medical history. Finally, we calculated and analyzed the EGSYS score of each child to explore its predictive value for the differential diagnosis between CS and NMS in children.
Informed consent was obtained from all the children in this study, and the study was approved by the ethics committee of Qilu Hospital, Shandong University (approval No. KYLL-202210-033).
The EGSYS score consists of six predictors (11, 13) (show in Table 1): (1) Abnormal ECG and/or structural heart disease (plus three points), (2) palpitations preceding syncope (plus four points), (3) syncope during effort (plus three points), (4) syncope while supine (plus two points), (5) precipitating and/or predisposing factors (minus one point), and (6) autonomic neurovegetative prodromes (minus one point). All predictors were evaluated for each patient by two trained pediatricians. Then, a total score ranging from −2 to 12 points was calculated as the sum of the points assigned to each predictor. Finally, each patient's score was determined after review by pediatric cardiovascular experts.

Table 1. The evaluation of guidelines in syncope study (EGSYS) scoresa.
All statistical analyses were performed using SPSS version 25.00 (IBM Corporation, New York, United States) and GraphPad Prism version 8.0. Non-normally distributed continuous data were described as median (interquartiles: P25, P75) and differences between groups were compared using the Mann-Whitney U test. Qualitative data were expressed as numbers and percentages (%), and comparisons between the two groups were performed using chi-square tests. The ROC curve was adopted to analyze the discrimination of the EGSYS score. The area under the curve (AUC) represented how well the EGSYS score differentiated cardiac syncope with values of 0.5–0.7, 0.7–0.9, and > 0.9 indicating a low, moderate and high diagnostic value respectively. The best EGSYS score cutoff value was determined based on the maximum Youden index value. The Hosmer-Lemeshow test was used to assess the goodness of fit of the EGSYS score model. A P > 0.05 suggested there was no statistically significant between predictive values and observed values, that is, an acceptable fit of the EGSYS score. Statistical significance was set at P < 0.05.
A total of 332 children were included in the study (Table 2). Of these, 281 children (130 males and 151 females) with a median age of 11.4 (9.7,12.9) years were diagnosed with NMS and 51 children (26 males and 25 females) with a median age of 13.0 (10.7,15.0) years were diagnosed with CS. There were no statistical differences in age or sex between the two groups (P > 0.05).
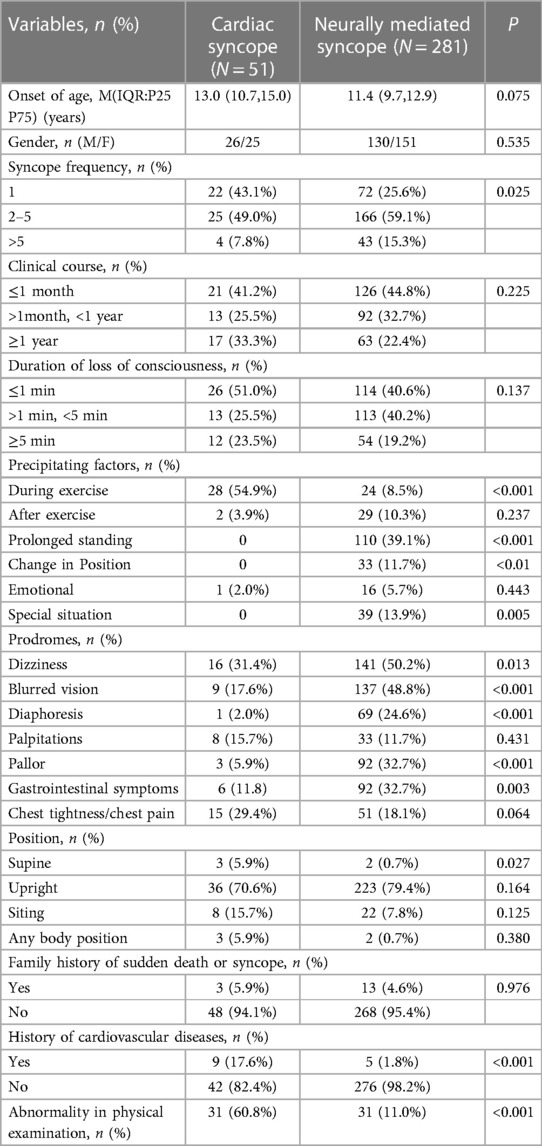
Table 2. Demographic and clinical features of children included.
Table 2 also shows the clinical features of the children with NMS and CS. Significant differences in precipitating factors, prodromes, supine position, history of cardiovascular disease, and physical examination were identified (P < 0.05).
All 281 children with NMS underwent a head-up tilt test. Among them, there were 176 cases of VVS, 26 cases of POTS, 75 cases of VVS with POTS, 3 cases of OH, and 1 case of OHT. In the CS group, there were 27 cases of arrhythmia, 9 cases of structural heart disease, and 15 cases with both causes. The underlying diseases in the children with CS are listed in Table 3.
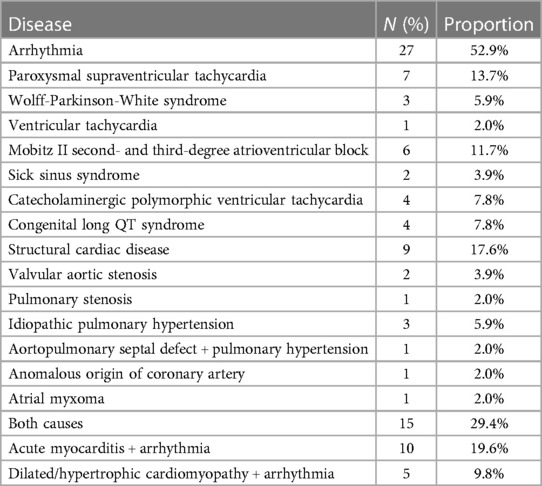
Table 3. The underlying disease of children with cardiac syncope.
A comparison of EGSYS risk factors between the NMS and CS groups is shown in Table 4. Children with CS were more likely to have abnormal ECG findings and/or underlying heart disease (P < 0.05). The rates of syncope attacks during effort and in the supine position were significantly higher in children with CS than in those with NMS (P < 0.05). Autonomic prodromes were more common in the NMS group than in the CS group (P < 0.05). The results of the EGSYS risk factors in the multivariable analysis are shown in Table 5.
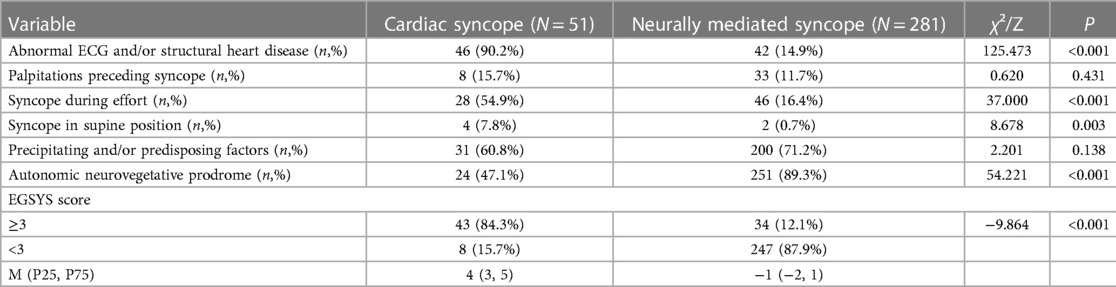
Table 4. Comparison of EGSYS risk factors between two groups.
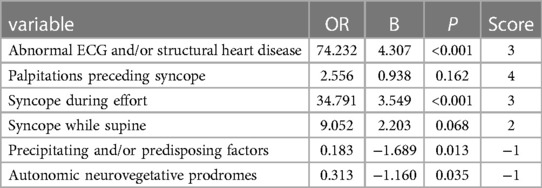
Table 5. The result of EGSYS risk factors on multivariable analysis.
The median EGSYS scores of the CS and NMS groups were 4 (3, 5) and −1 (-2, 1) respectively (P < 0.05; Table 4). The ROC curve for the EGSYS score is shown in Figure 1. The AUC of the EGSYS score was 0.922 [95% confidence interval (CI) 0.892–0.952; P < 0.001]. An EGSYS score ≥ 3 was the best cutoff value for diagnosing CS in children, with a sensitivity and specificity of 84.3% (95% CI 0.709–0.925) and 87.9% (95% CI 0.834–0.914) respectively. The Hosmer-Lemeshow test demonstrated good results for the goodness-of-fit of the model (χ2 = 1.468, P = 0.917).
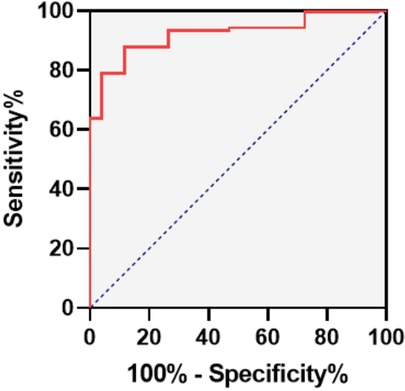
Figure 1. The receiver operating characteristic curve of EGSYS score.
Accurate diagnosis and risk stratification are extremely important for the proper management of patients presenting with syncope. In past researches, several syncope prediction tools based on clinical characteristics were developed and validated in adults (14, 22, 23). The prediction tools used to access the serious event in short-term include the San-Francisco Syncope Rule (SFSR), the Boston Syncope Criteria (BSC), the Risk Stratification of Syncope in the Emergency Department (ROSE) risk score and the Canadian Syncope Risk Score (CSRS) (24). The Osservatorio Epidemiologico sulla Sincope del Lazio (OESIL) risk score is to predict mortality at one year (24). However, these tools have a limited value in children. The SFSR and the ROSE require invasive laboratory tests. The CSRS incorporates a physician's diagnostic impression. The BSC and the OESIL include acquired cardiovascular risk factors, such as age, acute coronary syndrome, and heart failure. In contrast, impaired structural cardiac diseases and cardiac ion channelopathy are more common in younger patients with CS (25). The EGSYS score developed by Del Rosso et al. includes six clinical parameters: abnormal ECG and/or heart disease, palpitations, syncope during exertion, syncope in a supine position, predisposing factors and/or predisposing factors, and autonomic prodromes. Del Rosso et al. reported that the sensitivity and specificity of the EGSYS score for the diagnosis of CS were 92% and 69% respectively. Although several subsequent studies have also indicated that the EGSYS score has acceptable discrimination, it has not been validated in children with syncope.
In this study, we found that NMS and CS had different clinical characteristics in terms of predisposing factors, precursors, supine position, cardiovascular diseases, physical examination, and ECG results. After retrospectively analyzing the clinical data of 332 children with NMS and CS, we found that the calculated EGSYS scores had good sensitivity and specificity for the diagnosis of CS in children. According to the current guidelines for the management of syncope in children and adolescents (1, 26, 27), NMS is mostly triggered by prolonged standing, postural change, dehydration, urination, coughing, emotional surges, and stuffy or crowded environments. Prodromes, such as dizziness, nausea, abdominal discomfort, visual blurring, sweating, hyperventilation, and pallor appear either singularly or in combination before the onset of syncope. CS is more likely to occur during exertion or in the absence of a stimulus. Children with CS often have no prior autonomic prodrome but may sometimes present with chest tightness/pain and palpitations. Children with NMS are usually faint in an upright posture, whereas those with CS may have a syncopal event in any position. Additionally, abnormalities in the physical examination and 12-lead ECG indicated the possibility of cardiac causes. As shown in Table 1, the major risk factors of CS provided by the guidelines have been included in the EGSYS score; thus, the scoring model may help identify patients at higher risk of CS.
Although palpitations preceding syncope had the highest weight in the EGSYS score, our study showed no significant difference between the CS and NMS groups. In adults, palpitations are a common symptom of arrhythmia, such as supraventricular or ventricular tachycardia, atrial fibrillation, and atrial flutter. In such instances, palpitations are accompanied by dizziness, syncope, or near syncope (28). However, palpitations are rarely seen in pediatric clinics and emergency rooms. Children have difficulty understanding the meaning of palpitations and expressing them accurately. Zhang et al. reported a similar phenomenon (29). Therefore, palpitations may be an underrepresented feature in children with CS. However, Hurst et al. (2) analyzed CS patients (age 11.5 ± 4.5 years) in the emergency department and proposed that having palpitations was an indicator predicting CS in the pediatric emergency department, with a sensitivity of 100% and a specificity of 98%. Presently, palpitation-preceding events are still considered “red flags” of CS in many guidelines. Therefore, palpitations immediately followed by syncope should raise suspicions of CS in older children and adolescents.
This is the first study to externally validate a scoring system for predicting CS in children. Normally, an ideal predictive model properly identifies each patient who has an event from those who do not, without misclassification (30). In this study, the AUC of the EGSYS score was 0.922, demonstrating good accuracy in discriminating CS. The optimal cut-off was an EGSYS score of 3, which was consistent with the result reported by Del Rosso et al. (11). An EGSYS score ≥ 3 indicates a high possibility of CS with a sensitivity of 84.3% and a specificity of 87.9%. In such cases, more examinations such as echocardiography, 24 hour Holter monitoring, cardiac electrophysiology, and genetic screening are needed to identify the underlying disease. Furthermore, the P-value of 0.917 for the Hosmer-Lemeshow test represented a satisfactory calibration of the model.
Our study suggested that the EGSYS score appeared to be sensitive for differentiating CS from NMS in children. It might be used as an additional diagnostic tool to aid pediatricians in accurately identifying children with CS in the clinical practice. Further studies in larger populations are required to validate and modify the scoring system for clinical application.
The study had some limitations. It was a single-center retrospective study in hospitalized children, and the number of children with CS was small. We took medical history and made the diagnosis of CS and NMS according to widely accepted CPCS guidelines and ESC guidelines. All patients' diagnoses and medical records were reviewed by pediatric cardiovascular specialist prior to discharge to minimize misclassification. Another concern is the possible recall bias. We acknowledge the undeniable fact that recall bias exists in retrospective studies. In our study, we have excluded those with incomplete and unclear information. Furthermore, the age, sex, and the time since the first syncope episode showed no statistical differences between the two groups. Thus, we think that recall bias was present to a similar extent in both groups, and it was unlikely to have affected our conclusion. In addition, we did not complete the follow-up of all children, so the predictive value of the model for prognosis is unclear. It is necessary to conduct further prospective, multi-center studies with larger sample sizes to validate and modify the EGSYS score in the diagnosis and risk stratification of CS in children. Despite these limitations, the study demonstrated that the EGSYS score might be a simple and useful predictive tool for pediatricians.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding authors.
CZ and QK designed the study. YL, JL, MW, XL and JH collected and reviewed data. YL and JL analyzed data and drafted the manuscript. YL and JL contributed equally to this work. All authors contributed to the article and approved the submitted version.
This study was supported in part by the grants from the Shandong Province Science and Technology Project (#2014GSF118066 and 2019GSF108186).
We would like to thank Editage (www.editage.cn) for English language editing.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Brignole M, Moya A, de Lange FJ, Deharo JC, Elliott PM, Fanciulli A, et al. 2018 ESC guidelines for the diagnosis and management of syncope. Eur Heart J. (2018) 39:1883–948. doi: 10.1093/eurheartj/ehy037.29562304
2. Hurst D, Hirsh DA, Oster ME, Ehrlich A, Campbell R, Mahle WT, et al. Syncope in the pediatric emergency department - can we predict cardiac disease based on history alone? J Emerg Med. (2015) 49:1–7. doi: 10.1016/j.jemermed.2014.12.068.25802162
3. Wang T, Wang F, Li Y, Shi X, Duan H, Zhou K, et al. Clinical characteristics of personality and conduct disorders in child patients with vasovagal syncope: a clinical case-control study. Front Pediatr. (2021) 9:778605. doi: 10.3389/fped.2021.778605.34900878
4. Lee SH, Park SJ, Byeon K, On YK, Yim HR, Kim JS. Prevalence and clinical factors of anxiety and depression in neurally mediated and unexplained syncope. Yonsei Med J. (2013) 54:583–9. doi: 10.3349/ymj.2013.54.3.583.23549800
5. Schunk PC, Ruttan T. Pediatric syncope: high-risk conditions and reasonable approach. Emerg Med Clin North Am. (2018) 36:305–21. doi: 10.1016/j.emc.2017.12.005.29622324
6. Soteriades ES, Evans JC, Larson MG, Chen MH, Chen L, Benjamin EJ, et al. Incidence and prognosis of syncope. N Engl J Med. (2002) 347:878–85. doi: 10.1056/NEJMoa012407.12239256
7. Ruwald MH, Hansen ML, Lamberts M, Hansen CM, Højgaard MV, Køber L, et al. The relation between age, sex, comorbidity, and pharmacotherapy and the risk of syncope: a danish nationwide study. Europace. (2012) 14:1506–14. doi: 10.1093/europace/eus154.22588456
8. Singhi P, Saini AG. Syncope in pediatric practice. Indian J Pediatr. (2018) 85:636–40. doi: 10.1007/s12098-017-2488-9.29119462
9. Deif B, Kang S, Ismail A, Vanniyasingam T, Guzman JC, Morillo CA. Application of syncope guidelines in the emergency department do not reduce admission rates: a retrospective cohort study. Can J Cardiol. (2018) 34:1158–64. doi: 10.1016/j.cjca.2018.07.003.30170671
10. Landwehr K, Meyer S, Flotats-Bastardas M, Poryo M. Syncope in children and adolescents: are the current guidelines being followed? Wien Med Wochenschr. (2021) 171:157–64. doi: 10.1007/s10354-020-00798-3.33439378
11. Del Rosso A, Ungar A, Maggi R, Giada F, Petix NR, De Santo T, et al. Clinical predictors of cardiac syncope at initial evaluation in patients referred urgently to a general hospital: the EGSYS score. Heart. (2008) 94:1620–6. doi: 10.1136/hrt.2008.143123.18519550
12. Plasek J, Doupal V, Fürstova J, Martinek A. The EGSYS and OESIL risk scores for classification of cardiac etiology of syncope: comparison, revaluation, and clinical implications. Biomed Pap Med Fac Univ Palacky Olomouc Czech Repub. (2010) 154:169–73. doi: 10.5507/bp.2010.026.20668500
13. Kariman H, Harati S, Safari S, Baratloo A, Pishgahi M. Validation of EGSYS score in prediction of cardiogenic syncope. Emerg Med Int. (2015) 2015:515370. doi: 10.1155/2015/515370.26649200
14. Kayayurt K, Akoglu H, Limon O, Ergene AO, Yavasi O, Bayata S, et al. Comparison of existing syncope rules and newly proposed anatolian syncope rule to predict short-term serious outcomes after syncope in the turkish population. Int J Emerg Med. (2012) 5:17. doi: 10.1186/1865-1380-5-17.22520447
15. de Sousa Bispo J, Azevedo P, Mota T, Fernandes R, Guedes J, Candeias R, et al. EGSYS Score for the prediction of cardiac etiology in syncope: is it useful in an outpatient setting? Rev Port Cardiol (Engl Ed). (2020) 39:255–61. doi: 10.1016/j.repc.2019.09.009.32534800
16. Albassam OT, Redelmeier RJ, Shadowitz S, Husain AM, Simel D, Etchells EE. Did this patient have cardiac syncope?: the rational clinical examination systematic review. JAMA. (2019) 321:2448–57. doi: 10.1001/jama.2019.8001.31237649
17. Környei L, Szabó A, Róth G, Kardos A, Fogarasi A. Frequency of syncope as a presenting symptom in channelopathies diagnosed in childhood. Can the multivariable EGSYS score unmask these children? Eur J Pediatr. (2021) 180:1553–9. doi: 10.1007/s00431-020-03913-z.
18. Subspecialty Group of Cardiology. The Society of Pediatrics, Chinese Medical Association; Editorial Board, Chinese Journal of Pediatrics. Guidelines for diagnosis of syncope in children. Zhonghua Er Ke Za Zhi. (2009) 47:99–101. Chinese.19573453
19. Subspecialty Group of Cardiology, the Society of Pediatrics. Chinese Medical Association; Editorial Board, Chinese Journal of Pediatrics; Subspecialty Group of Cardiology, the Society of Pediatries, Beijing Medical Association; Professional Board of Syncope in Children, Pediatrician Society, Chinese Medical Doctor Association. Guideline for diagnosis of syncope in children (updated in 2016). Zhonghua Er Ke Za Zhi. (2016) 54:246–50. doi: 10.3760/cma.j.issn.0578-1310.2016.04.003. Chinese.27055420
20. Wang C, Li Y, Liao Y, Tian H, Huang M, Dong XY, et al. 2018 Chinese pediatric cardiology society (CPCS) guideline for diagnosis and treatment of syncope in children and adolescents. Science Bulletin. (2018) 63:1558–64. doi: 10.1016/j.scib.2018.09.019.36751076
21. Moya A, Sutton R, Ammirati F, Blanc JJ, Brignole M, Dahm JB, et al. Guidelines for the diagnosis and management of syncope (version 2009). Eur Heart J. (2009) 30:2631–71. doi: 10.1093/eurheartj/ehp298.19713422
22. Solbiati M, Talerico G, Villa P, Dipaola F, Furlan R, Furlan L, et al. Multicentre external validation of the Canadian syncope risk score to predict adverse events and comparison with clinical judgement. Emerg Med J. (2021) 38:701–6. doi: 10.1136/emermed-2020-210579.34039646
23. Costantino G, Casazza G, Reed M, Bossi I, Sun B, Del Rosso A, et al. Syncope risk stratification tools vs clinical judgment: an individual patient data meta-analysis. Am J Med. (2014) 127:1126.e13–.e25. doi: 10.1016/j.amjmed.2014.05.022.24862309
24. Runser LA, Gauer RL, Houser A. Syncope: evaluation and differential diagnosis. Am Fam Physician. (2017) 95:303–12.28290647
25. Anderson J, O'Callaghan P. Cardiac syncope. Epilepsia. (2012) 7:34–41. doi: 10.1111/j.1528-1167.2012.03713.x.
26. Sanatani S, Chau V, Fournier A, Dixon A, Blondin R, Sheldon RS. Canadian Cardiovascular society and Canadian pediatric cardiology association position statement on the approach to syncope in the pediatric patient. Can J Cardiol. (2017) 33:189–98. doi: 10.1016/j.cjca.2016.09.006.27838109
27. Shen WK, Sheldon RS, Benditt DG, Cohen MI, Forman DE, Goldberger ZD, et al. 2017 ACC/AHA/HRS guideline for the evaluation and management of patients with syncope: a report of the American college of cardiology/American heart association task force on clinical practice guidelines and the heart rhythm society. Heart Rhythm. (2017) 14:e155–217. doi: 10.1016/j.hrthm.2017.03.004.28286247
28. Quan KJ. Palpitation: extended electrocardiogram monitoring: which tests to use and when. Med Clin North Am. (2019) 103:785–91. doi: 10.1016/j.mcna.2019.05.005.31378325
29. Zhang QY, Du JB, Qi JG, Han L, Li WZ. Clinical characteristics of cardiac syncope in children. Zhonghua Er Ke Za Zhi. (2009) 47:44–7. Chinese.19573382
Keywords: syncope, cardiac syncope, neurally mediated syncope, children, EGSYS
Citation: Li Y, Liu J, Wang M, Zhao H, Liu X, Hu J, Zhao C and Kong Q (2023) Predictive value of EGSYS score in the differential diagnosis of cardiac syncope and neurally mediated syncope in children. Front. Cardiovasc. Med. 10:1091778. doi: 10.3389/fcvm.2023.1091778
Received: 7 November 2022; Accepted: 1 March 2023;
Published: 17 March 2023.
Edited by:
Jaspal Dua, Liverpool Heart and Chest Hospital NHS Trust, United KingdomReviewed by:
Runmei Zou, Central South University, China© 2023 Li, Liu, Wang, Zhao, Liu, Hu, Zhao and Kong. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Cuifen Zhao emhhb2N1aWZlbkBzZHUuZWR1LmNu Qingyu Kong bGVvbmFyZDEyMjZAMTI2LmNvbQ==
Specialty Section: This article was submitted to Pediatric Cardiology, a section of the journal Frontiers in Cardiovascular Medicine
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.