
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Cardiovasc. Med. , 17 April 2023
Sec. Cardiac Rhythmology
Volume 10 - 2023 | https://doi.org/10.3389/fcvm.2023.1084051
This article is part of the Research Topic Malignant Arrhythmias and Trigger Mechanisms View all 9 articles
 Dirk Bandorski1*†
Dirk Bandorski1*† Sebastian Heibel2,†
Sebastian Heibel2,† Reinhard Höltgen3
Reinhard Höltgen3 Harilaos Bogossian4Hossein Ardeschir Ghofrani5Markus Zarse6Henning Gall5
Harilaos Bogossian4Hossein Ardeschir Ghofrani5Markus Zarse6Henning Gall5
Background: In patients with pulmonary hypertension (PH), increased pulmonary vascular resistance (PVR) may lead to increased right ventricular afterload and cardiac remodelling, potentially providing the substrate for ventricular arrhythmias. Studies dealing with long term monitoring of patients with PH are rare. The present study evaluated the incidence and the types of arrhythmias retrospectively recorded by Holter ECG in patients with newly detected PH during a long-term Holter ECG follow-up. Moreover, their impact on patient survival was evaluated.
Patients and methods: Medical records were screened for demographic data, aetiology of PH, incidence of coronary heart disease, level of brain natriuretic peptide (BNP), results from Holter ECG monitoring, 6-minute walk test distance, echocardiographic data and hemodynamic data derived from right heart catheterization. Two subgroups were analyzed: 1. patients (n = 65) with PH (group 1 + 4) and derivation of at least 1 Holter ECG within 12 months from initial detection of PH and 2. patients (all PH etiologies, n = 59) with 3 follow-up Holter ECGs. The frequency and complexity of premature ventricular contractions (PVC) was classified into “lower” and “higher” (=non sustained ventricular tachycardia, nsVT) burden.
Results: Holter ECG revealed sinus rhythm (SR) in most of the patients (n = 60). Incidence of atrial fibrillation (AFib) was low (n = 4). Patients with premature atrial contractions (PAC) tend to have a shorter period of survival (p = 0.098), PVC were not correlated with significant survival differences. During follow-up PAC and PVC were common in all PH groups. Holter ECG revealed non sustained ventricular tachycardia in 19/59 patients [(32.2%); n = 6 during first Holter-ECG, n = 13 during second/third Holter-ECG]. In all patients suffering from nsVT during follow-up previous Holter ECG revealed multiform/repetitive PVC. PVC burden was not linked to differences in systolic pulmonary arterial pressure, right atrial pressure, brain natriuretic peptide and results of six-minute walk test.
Conclusion: Patients with PAC tend to have a shortened survival. None of the evaluated parameters (BNP, TAPSE, sPAP) was correlated with the development of arrhythmias. Patients with multiform/repetitive PVC seem to be at risk for ventricular arrhythmias.
Pulmonary hypertension (PH) is defined as an elevation of the mean pulmonary arterial pressure (mPAP) > 20 mmHg at rest (1)—an earlier definition included mPAP < 25 mmHg (2, 3)—concomitant with either pulmonary vascular resistance (PVR) ≥ 3 Wood units (WU) and pulmonary capillary wedge pressure (PcWP) ≤ 15 mmHg in precapillary forms or PVR < 3 WU and PcWP > 15 mmHg in postcapillary forms (4). Increased PVR leads to increased afterload of the right ventricle and cardiac remodelling (5), which could provide the substrate for cardiac arrhythmias (6, 7). In most studies regarding cardiac rhythm in PH patients have undergone repeated standard electrocardiograms (ECG) to evaluate supraventricular arrhythmias (8–12). In three studies, the authors evaluated the incidence of ventricular arrhythmias in patients who underwent 24-h Holter ECG for close monitoring of their heart rhythm (13–15). There are few data about the onset of arrhythmias after the first diagnosis of PH and in none of the recent studies patients underwent repeated Holter ECG monitoring.
We performed the present study to evaluate the incidence and type of arrhythmias identified by Holter ECG in patients who have been newly diagnosed with PH and who underwent long-term Holter ECG follow-up. In addition, we examined the influence of the arrhythmias found on patient survival.
Data of the patients of the PH department of University Hospital of Giessen, Germany from a period of 10 consecutive years were retrospectively analysed. They included patients with PH (any subgroup) and a recording of at least one Holter ECG within 12 months from the initial detection of PH. Medical records were screened for the following data: demographic data, aetiology of PH, incidence of coronary artery disease (CAD), level of brain natriuretic peptide (BNP), results from Holter ECG monitoring, 6-minute walk test (6MWT) distance, echocardiographic data, and hemodynamic data derived from right heart catheterisation (RHC). The findings were obtained from patient files; thus, the number in the subgroups can deviate from the total number of patients if information is missing.
These data are part of the doctoral thesis of Sebastian Heibel. To match the data with other studies (8, 10–12), a subgroup of patients with group 1 PH [pulmonary arterial hypertension (PAH)] and group 4 [chronic thromboembolic pulmonary hypertension (CTEPH)] was formed. To evaluate heart rhythm over the disease process, another subgroup was created, including all patients with three follow-up Holter ECGs (Figure 1) of all PH aetiologies. Patients were seen in a structured follow up (according to the clinic's internal procedure) every 3 to 6 months in the pulmonary hypertension outpatient department with clinical examination, echocardiography and Holter monitoring based on medical necessity. Data of last contact and corresponding survival status were noted.
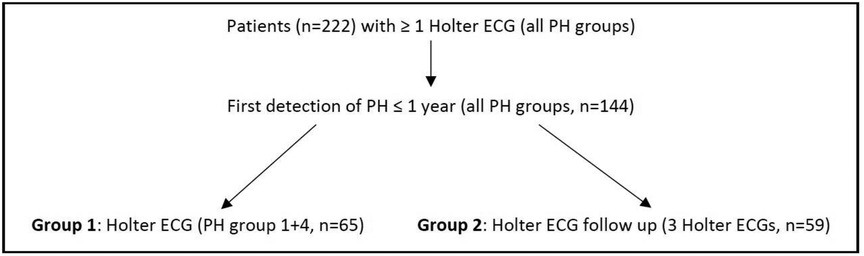
Figure 1. Description of the study population. ECG = electrocardiogram; PH = pulmonary hypertension.
The study and the study design were approved by the institutional review board (Ethics Commission of the Faculty of Medicine, Justus Liebig Universität Giessen, reference number: 107/13). The study was registered in ClinicalTrials.gov (ID: NCT05496504, Protocol ID: PH09_08_2022).
Patients underwent Holter ECG monitoring (GETEMED, Teltow, Germany) for 24 h to detect arrhythmias and heart rate variability (HRV). Detected arrhythmias were classified following the terminology of the European Society of Cardiology (ESC) (16, 17). In accordance with a previous study from our group (14), the following arrhythmias were considered potentially prognostic relevant: infrahisian atrioventricular (AV) block (second-degree type 2 and third-degree AV block are associated with a poor outcome if undetected and/or untreated) (18), atrial flutter (due to its danger of 1:1 AV conduction) and ventricular tachycardias [increased rate of sudden cardiac death (SCD) in patients with a reduced ejection fraction] (17, 19).
Non-life-threatening arrhythmias were defined as follows: premature atrial contractions (PAC), non-sustained or sustained supraventricular tachycardias (e.g., atrial tachycardia or atrial fibrillation, which are not reported to be related to SCD) and isolated premature ventricular contractions (PVC). PVC were graded by the physicians analysing the Holter ECGs using the Lown classification as a surrogate parameter (20). The predictive value of Lown's grading system has only been proved for CAD or for arrhythmias after myocardial infarction (MI) and the risk of a prognostic deterioration does not generally increase with the class (21). Nevertheless, the occurrence of a high burden of PVCs as well as nsVT are seen as risk factors for SCD (22) and this classification has become established in clinical practice for long-term ECG diagnosis, including in patients with other underlying diseases—for example, PH (23). Lown grade 4b was classified as non-sustained ventricular tachycardia (nsVT, ≥3 beats in duration, terminating spontaneously in less than 30 s) (24). Since the use of the classification is no longer recommended, we differentiated the arrhythmic burden by PVCs between patients with lower burden (Lown 0–4a) and higher burden (Lown 4b).
The results of Holter ECG recordings were correlated with echocardiography, RHC data, laboratory values and the 6MWT distance.
In accordance with the guidelines of the American Thoracic Society (ATS), patients walked along a 100-foot floor at their own pace to cover as much distance as possible in 6 min (25). The total distance walked was determined.
Transthoracic echocardiographs were evaluated by experienced investigators (GE, Boston, Massachusetts, United States). The following diameters and valves were measured: the left atrial diameter (edge-to-edge method, parasternal long axis view), the right atrial diameter (four-chamber view, measured at end systole), the left ventricular ejection fraction (LVEF, biplane Simpson method, two- and four-chamber view), tricuspid annular plane systolic excursion (TAPSE), and systolic pulmonary artery pressure (sPAP). All measurements were carried out in accordance with the guidelines of the American Society of Echocardiography (26–29).
RHC was performed via the right jugular vein. Hemodynamic measurements included mean right atrial pressure (mRAP), mPAP, PcWP, PVR, the cardiac index (CI, thermodilution method), and mixed venous oxygen saturation (SvO2).
After pseudonymisation, all statistical analysis was performed using SPSS® Statistics, Versions 21 and 28 (IBM Corp., Armonk, NY, United States). The patient data are presented as the mean [standard deviation (SD)] or median [interquartile range (IQR)]. Statistical evaluation included possible correlations between baseline and follow-up Holter ECG monitoring and echocardiography as well as clinical and laboratory parameters. Pearson's chi-squared test or Fisher's exact test was used for descriptive statistical comparisons. To control the type I error of multiple testing, one-way analysis of variance (ANOVA) followed by Tukey's honestly significant difference (HSD) post hoc test was used for multiple comparisons. Levene's test for homogeneity of variances was performed in every analysis. Mortality analysis was carried out using the Kaplan–Meier (KM) method to analyse “time-to-event” data. The event status consisted of two mutually exclusive events: censored (loss to follow-up) or event (death). The Mantel–Cox log rank test was used to test the equality of the overall survival distributions between the groups. For all analyses, p < 0.05 was considered a statistically significant result. p-values between 0.05–0.1 were considered as trend towards statistical significance.
Sixty-five patients (female, n = 43; male, n = 22) were enrolled. The mean age was 64 ± 15 years. 21 patients (32%) had PAH (group 1), 3 patients (5%) had group 1′ PH and 41 patients (63%) had CTEPH (group 4). 15 patients (23%) had an anamnesis of CAD (group 1, n = 5; group 4, n = 10) without the need for treatment or myocardial infarction. The data of echocardiography, right heart catheterization, BNP and 6MWT are shown in Table 1.
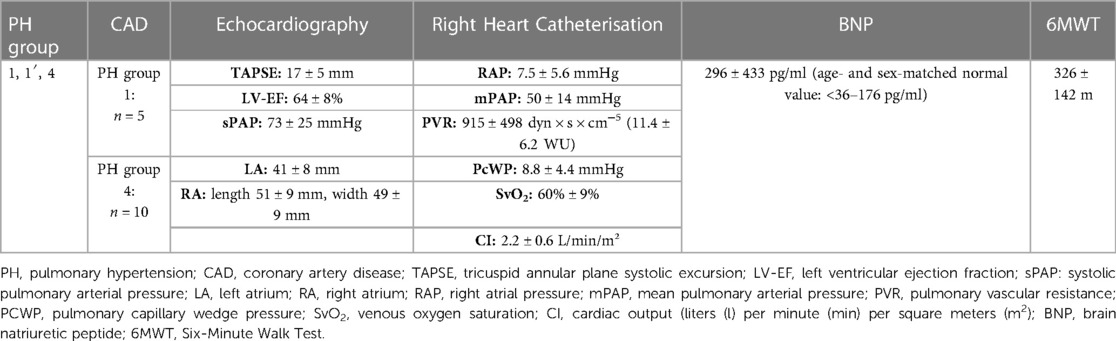
Table 1. Group 1 baseline values.
Holter ECG revealed sinus rhythm (SR) in 60 patients (92%; CAD, n = 15) and atrial fibrillation in 4 patients (7%; CAD: n = 1). Mean heart rate was 76 ± 11 beats per minute (bpm), minimal heart rate 60 ± 11 bpm, and maximal heart rate 118 ± 26 bpm. The standard deviation of NN intervals as an indicator of HRV (SDNN) was decreased, with a mean of 77 ± 11 ms (normal value:141 ± 39 ms). PAC occurred in 19 patients (PH group 1: n = 6, CAD: n = 3, PH group 4: n = 13, CAD: n = 3). PVC were found in 51 patients (PH group 1: n = 17, CAD: n = 5; PH group 4: n = 34, CAD = 10). The most complicated PVC were salves of ≥3 PVC (nsVT, n = 7).
Due to low number of patients, no subgroup analysis was performed for the above-mentioned parameters.
No significant survival difference between groups with SR and with AFib was found taking into account the small sample size of the AFib group (n = 4).
The 1-, 3-, and 5-year survival rates were 92.5%, 79.5%, and 76.5%, respectively, for patients without PAC vs. 90.7%, 61.3%, and 51.1%, respectively, for patients with PAC (Figure 2; log rank test p = 0.098).
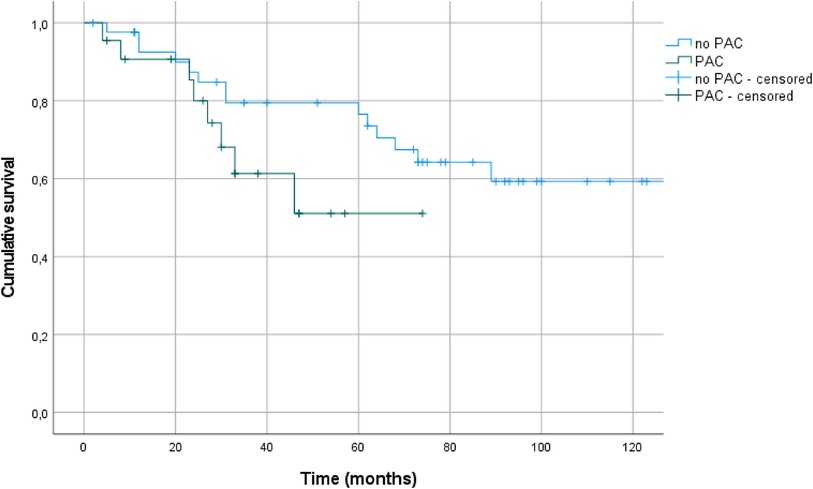
Figure 2. Kaplan–Meier plots (+ = censored data) for survival of patients with (n = 19) or without (n = 46) premature atrial contractions (PAC).
Survival data showed no differences between patients with lower and higher PVC burden (log rank test p = 0.849, Figure 3).
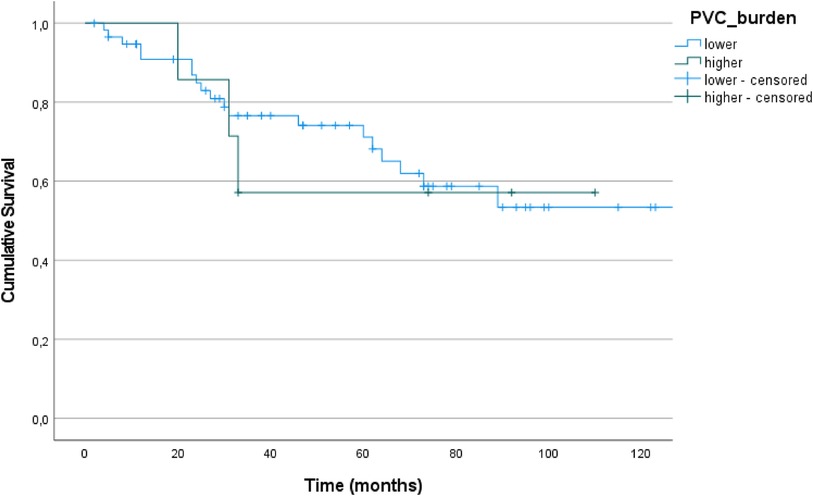
Figure 3. Kaplan–Meier plots (+ = censored data) for survival of patients with lower (n = 51) and higher (n = 7) PVC burden.
Fifty nine patients (female, n = 29; male, n = 30) underwent three Holter ECGs. The median time between the first and the second examination was 3 months [IQR 1–10]. The distribution of time interval from Holter examination 1 to Holter examination 3 was left skewed. The median was 14 months [IQR 6–34]. The mean age at the first Holter monitoring was 65 ± 13 years. There were patients in all PH groups: group 1, n = 14; group 1′, n = 3; group 2, n = 9; group 3, n = 12; group 4, n = 19; and group 5, n = 2. Sixteen patients had an anamnesis of CAD (group 1, n = 5; group 2, n = 4; group 3, n = 3; group 4, n = 4; and group 5, n = 0) without MI.
Holter ECG revealed SR in most patients. AFib and other heart rhythms occurred less frequently (Table 2).
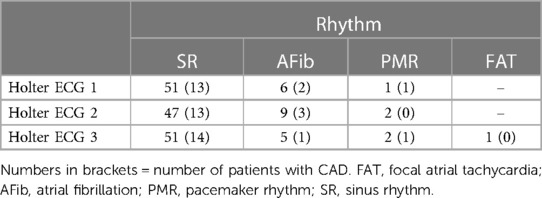
Table 2. Number of patients with each heart rhythm in the three consecutive Holter electrocardiograms.
Holter ECG revealed a mean heart rate of 76 ± 14 bpm at Holter ECG 1, 77 ± 14 bpm at Holter ECG 2, and 79 ± 14 bpm at Holter ECG 3. The minimal heart rate was 58 ± 13, 59 ± 11, and 61 ± 12 bpm (Holter ECG 1/2/3) and the maximal heart rate 115 ± 23, 114 ± 18, and 119 ± 22 bpm (Holter ECG 1/2/3). The SDNN interval was 76 ± 13 ms, 71 ± 15 ms and 76 ± 14 ms for Holter ECG 1, 2 and 3, respectively.
PVC occurred frequently in all patients over the entire period. There was no apparent trend for PAC (Table 3). No significant differences between PH groups were found (Holter ECG 1, 2, and 3: PVC, p = 0.413/0.342/0.307, respectively; PAC, p = 0.40/0.696/0.904, respectively).
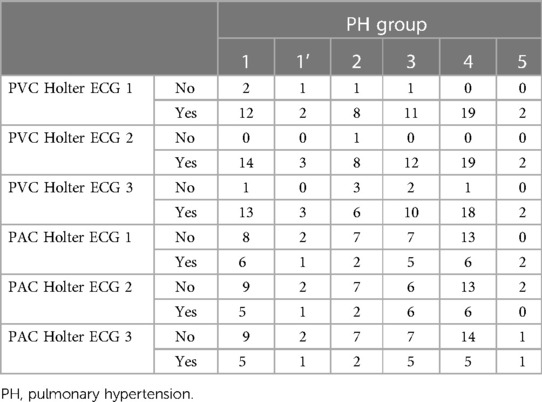
Table 3. Premature ventricular contractions (PVC) and premature atrial contractions (PAC) for each Holter electrocardiogram (ECG).
Because of a small number of cases, no analysis of the subgroups (heart rhythm) was carried out for the parameters mentioned.
All patients had a normal LVEF at the first echocardiography (lower/higher PVC burden: 60 vs. 59%; p = 0.340). There were no significant differences in echocardiography, BNP, and 6MWT between patients with lower or higher burden of PVC (Table 4).
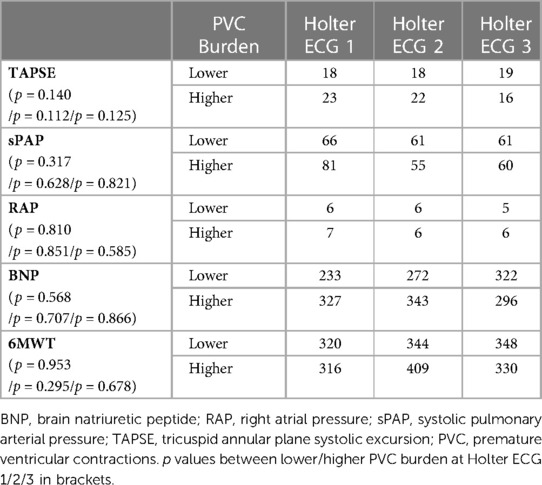
Table 4. PVC burden and six-minute walk test (6MWT), echocardiographic data, and brain natriuretic peptide during Holter electrocardiogram (ECG) follow-up.
During follow-up, there were no statistically significant differences between the occurrence of complex VPC between PH subgroups (detailed data not shown).
Eleven patients had an altered heart rhythm during Holter ECG follow-up. Patients with a change from SR to AFib were in PH groups 1, 2, 4, and 5. Three patients had an anamnesis of CAD (Table 5).
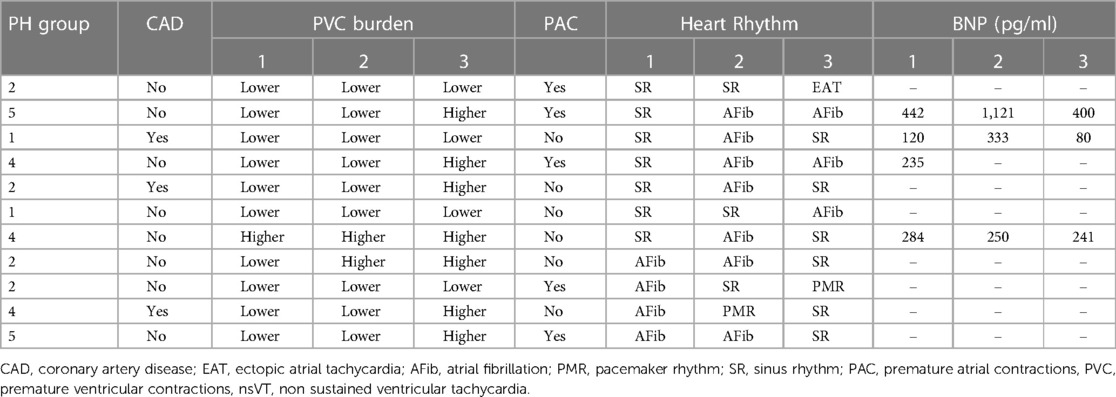
Table 5. Patients with changing heart rhythm during Holter electrocardiogram follow-up.
Six patients had nsVTs during the first Holter ECG. Non sustained VT episodes occurred in 13 patients during the Holter ECG follow-up. In most patients, nsVT was found during follow-up. Patients with nsVT were from all PH groups (Table 6). In all patients, the first Holter ECG already revealed multiform/repetitive PVC. BNP values, sPAP and TAPSE showed no clear association to PVC burden or occurrence of nsVT (further information available in Supplement S1).
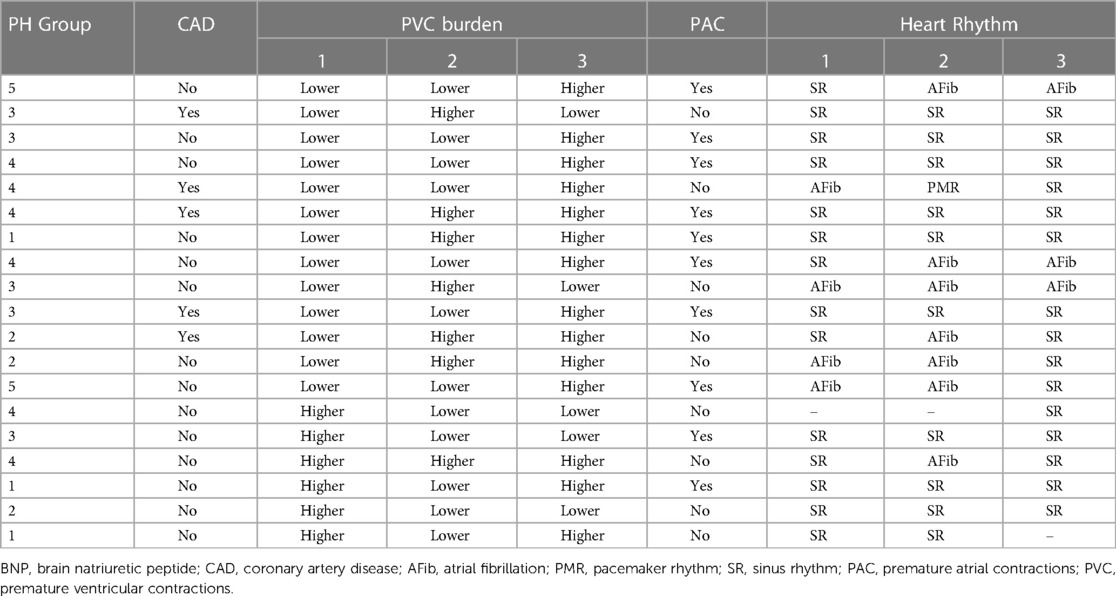
Table 6. Patients with non-sustained ventricular tachycardia (nsVT) during Holter electrocardiogram follow-up.
Between patients (n = 11) with conversion to AFib during the three Holter ECGs no statistically significant difference of survival was found (1-, 3-, and 5-year survival: SR 100%, 79% and 73.2%, respectively, AFib 100%, 60% and 30%, respectively; log rank test p = 0.131; Figure 4).
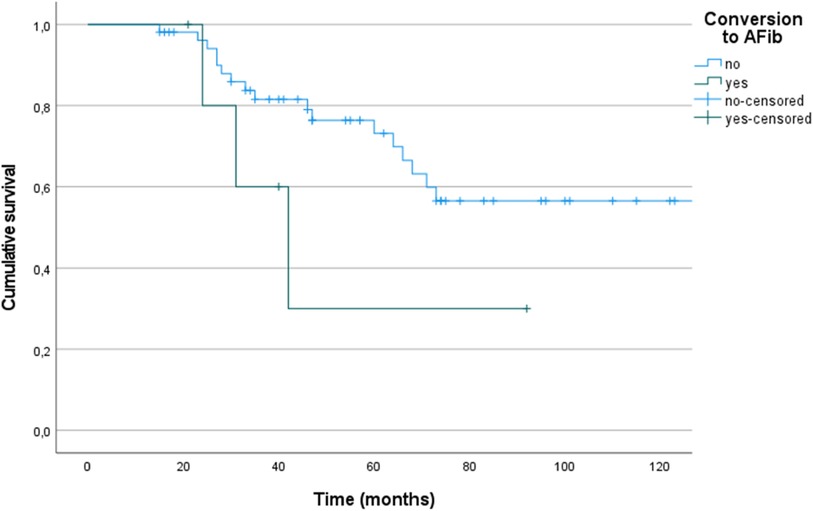
Figure 4. Kaplan–Meier plots (+ = censored data) for survival of patients with sinus rhythm (n = 48) and atrial fibrillation (AFib, n = 11).
Analysis of survival revealed no statistically significant differences between patients with nsVT during Holter ECG monitoring and patients with permanent SR during follow-up (1-, 3-, and 5-year survival: SR 100%, 83.7% and 73.3%, respectively, nsVT 100%, 70.6% and 62.7%, respectively; log rank test p = 0.377; Figure 5).

Figure 5. Kaplan–Meier plots (+ = censored data) for survival of patients with sinus rhythm (n = 40) and non-sustained ventricular tachycardia (nsVT, n = 19).
To our knowledge, our study is the first work to monitor patients with PH with repetitive Holter ECGs over a longer time [14 months (IQR 6–34)] and a long-term follow-up (120 months). The study contains two parts: First, to match our data with other studies (8, 10–12), we enrolled patients with group 1 and 4 PH (part 1). The first diagnosis of PH was made within the previous 12 months to minimise the potential influence of longstanding PH related effects on the heart leading to arrhythmias (30). Second, to follow up heart rhythm we analysed another subgroup including patients of all PH aetiologies with three follow-up Holter ECGs (part 2). We discuss the two parts of the study separately.
In contrast to other studies, only few patients (n = 4/65, 6.15%) had supraventricular tachycardia (AFib). In other studies, the incidence of supraventricular tachycardia has varied between 11.7% and 46.4% over a follow-up interval of 6–13 years (31). These results are in accordance with findings in two recent studies (12/43 and 162/641 patients) (32, 33). Interestingly, the number of patients with nsVT was high in our cohort [19/59 (32.2%); n = 6 during first Holter ECG, n = 13 during second/third Holter-ECG]. These findings are in contrast to most other studies with an incidence of nsVT between 5.9% and 13% (13, 32). Likewise, in other studies patients with nsVT mainly had group 2 PH (group 1 vs. 2, 15% vs. 48%) (34). A slightly higher prevalence than the aforementioned studies (but still clearly lower than in our study) was found recently with 16.7% of patients having nsVT in a cohort of patients with PH of all groups (group 1, 2.5%; group 3, 3.1%; group 4, 1.8%; group 5, 0%) (35).
Most of the studies evaluating survival revealed a statistically significant shorter survival of patients with supraventricular tachycardia (8, 12, 36–39). In contrast to these results, in two studies survival of patients with supraventricular tachycardia was not significantly shorter (15) or had no influence on survival (37). In our study, the small number of patients with supraventricular tachycardia (AFib, n = 4) did not allow any conclusion regarding survival time.
The incidence and prognostic value of PAC and PVC in patients with PH has not been investigated in studies before. The current AHA/ACC/HRS guidelines do not mention patients with PH (17).
Due to the individuality of quantification of PAC the results regarding the survival data of patients with PAC are difficult to assess. Our patients with PAC showed a trend towards shortened survival. In another study evaluating the prognostic relevance of PAC in patients with different indications for Holter ECG the burden of PAC was independently associated with mortality (40). In their meta-analysis, Himmelreich et al. (2019) found that frequent PAC during Holter ECG were associated with AFib (41). In contrast, our data showed PAC during Holter ECG in 4/11 patients with AFib for one or more of the three Holter ECGs.
Regarding survival of patients with nsVT, the data in the present study are consistent with our previous study (42).
SR was the most common rhythm in our patients. LVEF (during Holter ECG 1) was normal in nearly all patients. CAD was present in 16/59 patients (PH group 1: 5/14; group 2: 4/9; group 3: 3/12; group 4: 4/19; group 5: 0/2), especially in 3/11 patients with AFib and in 5/19 patients with nsVT. These findings indicate that in patients with PH, mechanisms other than ischaemia/CAD seem to be responsible for arrhythmias (see below).
Holter ECG monitoring revealed PAC frequently, but all in all, the distribution was without statistically significant differences between PH groups. PVC occurred often with high frequency in all PH groups, too. Witte et al. (2016) evaluated patients with PH who underwent 24-hour Holter ECG (43): Patients with PH group 1 had a higher burden of PVC and a decrease in HRV (SDNN). In patients with PH group 4, the number of PVC differed from controls (“higher total count of PVC”), whereas in patients with PH and COPD, both PAC and PVC were more frequent than in controls and SDNN was similar to patients with PH group 1. Another study also revealed frequent PVC and reduced HRV (SDNN) in PH patients compared with controls (44). Increased PAC, PVC, and arrhythmias are known to occur in patients with COPD (45, 46).
At the time of Holter ECG 1, patients (with three Holter ECGs) with nsVTs had higher values of sPAP and BNP. This association was less clear at the time of Holter ECGs 2 and 3. Therefore, sPAP and BNP values are not sufficient to identify patients with more frequent arrhythmias (or at risk for arrhythmias).
Another interesting observation is that patients with an initial occurrence of multiform/repetitive PVC at Holter ECG 1 continued to show complex PVC during follow-up. All patients who showed conversion to AFib had multiform/repetitive PVC. These findings may indicate greater impairment of right heart function.
In patients converting to AFib and patients with prevalent nsVT no statistical significant differences in survival was found. It must be noted that in our study the number of patients developing supraventricular arrhythmia (AFib) was small (n = 11). Most of the studies evaluating survival have revealed significantly shortened survival of patients with supraventricular tachycardia (8, 12, 36–39). However, some studies have revealed no significant difference (15, 39).
Based on the literature, different causes seem to be responsible for arrhythmias in patients with PH. Umar et al. (2012) found that in rats with PH induced by subcutaneous injection of monocrotaline, early afterdepolarisations (EADs) from the right ventricular epicardial surface triggered ventricular tachycardia. The study revealed two underlying mechanisms that maintain ventricular arrhythmias: focal and incomplete re-entrant wave fronts during ventricular fibrillation (6).
Rosas-Peralta et al. (2006) revealed an autonomic cardiac disturbance in patients with group 1 and 2 PH (Eisenmenger syndrome). Increased sympathetic tone led to loss of the circadian rhythm of HRV. After administering treprostinil, there was a recovery of sympathovagal balance. The authors concluded the changes may be markers of autonomic dysbalance that favour the development of arrhythmias and SCD. The sympathovagal balance in PH could be considered an important risk marker (47).
Another important cause for arrhythmias in patients is cardiac fibrosis. In rats with PH, increased myocardial fibrosis generates the substrate for the initiation and maintenance of ventricular arrhythmias (6, 48, 49). Cardiomyocytes from a failing right ventricle exhibited prolonged action potential duration, EADs, triggered activity, and spontaneous re-entrant ventricular arrhythmias caused by right-sided AP alternans at physiological rates (50).
Noteworthy, in a basic science study with rats receiving monocrotaline leading to advanced PAH, the treated rats showed prolongation of action potential duration (APD), increased APD heterogeneity and other changes, which led to rapid pacing and susceptibility to sustained VT.
A selective intra-tracheal gene delivery (of aerosolized AAV1 carrying S2a resulting in selective upregulation of the human isoform of SERCA2a) in the lung but not the heart improved monocrotaline-induced prolongation of cardial action potential duration and thus suppressed the incidence of pacing-induced VT (51).
Histology studies in humans have revealed right ventricular fibrosis in patients with PAH (52, 53). These results are consistent with electrophysiological findings in patients with PH, which have revealed cardiac fibrosis. However, the experience with electrophysiology studies in patients with PH is very limited. Medi et al. reported that patients with right atrial dilatation/remodelling showed a reduction in conduction velocity and an increase in areas of low voltage or electrical silence due to interstitial fibrosis (54).
In a patient with PH caused by atrial septal defect and partial anomalous pulmonary venous drainage, electrophysiology studies revealed a non-sustained focal activation and its origin very close to a small low-voltage area at the lateral wall of the right ventricle near the tricuspid annulus, suggesting structural remodelling of the RV (55).
Another invasive tool used to estimate cardiac fibrosis is electroanatomic mapping (high-density peak-to-peak voltage mapping). A taxable and locatable electrophysiological catheter is introduced into the right ventricle using electro-anatomical and additive fluoroscopic guidance to receive three-dimensional geometry and a peak-to-peak voltage and scar map. In patients with arrhythmogenic right ventricular dysplasia, researchers noted concordance between electroanatomic findings and magnetic resonance imaging (MRI) or echocardiographic findings (56).
A new non-invasive tool for the diagnosis of cardiac fibrosis is MRI. Myocardial tissue characterisation in PAH is feasible using late gadolinium enhancement and T1 values (57). In the future, it will be interesting to use MRI to quantify the fibrosis degree in patients with ventricular arrhythmia to determine whether the fibrosis degree correlates with the grade of ventricular arrhythmic burden and risk of arrhythmias or SCD in general.
Our study is not free of limitations: It was conducted as a single center study. Because PH is a rare disease, only a relatively small number of patients could be included. The retrospective design of the study (missing data) and the number of different examiners meant that no standardised findings of the Holter ECGs were available. The frequency of PAC during Holter ECG was stated subjectively by the physician (qualitative/quantitative). A more extensive rhythm monitoring was carried out by Holter ECG monitoring, but it must be noted that this is not a full rhythm monitoring over a longer period of time.
Finally, based on the study design the follow up scheme was set due to clinical need and not specific study requirements, which has impact on survival analyses and the follow-up Holter monitorings. However, especially the interval between the different Holter monitoring dates is considered acceptable.
Our present study was conducted to detect the arrhythmic burden in PH and its potential prognostic significance. In our PH cohort patients with PAC tend to a shortened survival, in contrast the occurrence of nsVT was not linked to an impaired survival prognosis. None of the evaluated parameters (BNP, TAPSE, sPAP) was correlated with the development of arrhythmias. Patients showing multiform/repetitive PVC seem to stay at risk for complex ventricular arrhythmias over a longer time in the disease process. Further research to verify our results with the inclusion of a higher number of subjects, preferably within the frame of multicentric studies, is desirable.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by Ethics Commission of the Faculty of Medicine, Justus-Liebig-Universität Giessen. Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
Substantial contributions to the conception or design of the work (DB, SH, AG, HAG); or the acquisition (DB, SH), analysis (DB, SH, HG), or interpretation of data for the work (all authors). Drafting the work or revising it critically for important intellectual content (all authors). Provide approval for publication of the content (all authors). Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved (all authors). All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fcvm.2023.1084051/full#supplementary-material.
1. Humbert M, Kovacs G, Hoeper MM, Badagliacca R, Berger RMF, Brida M, et al. 2022 ESC/ERS guidelines for the diagnosis and treatment of pulmonary hypertension. Eur Heart J. (2022) 43(38):3618–731. doi: 10.1093/eurheartj/ehac237
2. Galiè N, Humbert M, Vachiery JL, Gibbs S, Lang I, Torbicki A, et al. ESC_ERS guidelines for the diagnosis and treatment of pulmonary hypertension. Eur Respir J. (2015) 46:903–75. doi: 10.1093/eurheartj/ehv317
3. Hoeper MM, Bogaard HJ, Condliffe R, Frantz R, Khanna D, Kurzyna M, et al. Definitions and diagnosis of pulmonary hypertension. J Am Coll Cardiol. (2013) 62(25 Suppl):D42–50. doi: 10.1016/j.jacc.2013.10.032
4. Simonneau G, Montani D, Celermajer DS, Denton CP, Gatzoulis MA, Krowka M, et al. Haemodynamic definitions and updated clinical classification of pulmonary hypertension. Eur Respir J. (2019) 53(1):1801913. doi: 10.1183/13993003.01913-2018
5. Runo JR, Loyd JE. Primary pulmonary hypertension. Lancet. (2003) 361(9368):1533–44. doi: 10.1016/S0140-6736(03)13167-4
6. Umar S, Lee JH, de Lange E, Iorga A, Partow-Navid R, Bapat A, et al. Spontaneous ventricular fibrillation in right ventricular failure secondary to chronic pulmonary hypertension. Circ Arrhythm Electrophysiol. (2012) 5(1):181–90. doi: 10.1161/CIRCEP.111.967265
7. Lee JK, Kodama I, Honjo H, Anno T, Kamiya K, Toyama J. Stage-dependent changes in membrane currents in rats with monocrotaline-induced right ventricular hypertrophy. Am J Physiol. (1997) 272(6 Pt 2):H2833–42. doi: 10.1152/ajpheart.1997.272.6.H2833
8. Olsson KM, Nickel NP, Tongers J, Hoeper MM. Atrial flutter and fibrillation in patients with pulmonary hypertension. Int J Cardiol. (2013) 167(5):2300–5. doi: 10.1016/j.ijcard.2012.06.024
9. Rottlaender D, Motloch LJ, Schmidt D, Reda S, Larbig R, Wolny M, et al. Clinical impact of atrial fibrillation in patients with pulmonary hypertension. PLoS ONE. (2012) 7(3):e33902. doi: 10.1371/journal.pone.0033902
10. Ruiz-Cano MJ, Gonzalez-Mansilla A, Escribano P, Delgado J, Arribas F, Torres J, et al. Clinical implications of supraventricular arrhythmias in patients with severe pulmonary arterial hypertension. Int J Cardiol. (2011) 146(1):105–6. doi: 10.1016/j.ijcard.2010.09.065
11. Tongers J, Schwerdtfeger B, Klein G, Kempf T, Schaefer A, Knapp JM, et al. Incidence and clinical relevance of supraventricular tachyarrhythmias in pulmonary hypertension. Am Heart J. (2007) 153(1):127–32. doi: 10.1016/j.ahj.2006.09.008
12. Wen L, Sun ML, An P, Jiang X, Sun K, Zheng L, et al. Frequency of supraventricular arrhythmias in patients with idiopathic pulmonary arterial hypertension. Am J Cardiol. (2014) 114(9):1420–5. doi: 10.1016/j.amjcard.2014.07.079
13. Bandorski D, Schmitt J, Kurzlechner C, Erkapic D, Hamm CW, Seeger W, et al. Electrophysiological studies in patients with pulmonary hypertension: a retrospective investigation. Biomed Res Int. (2014) 2014:617565. doi: 10.1155/2014/617565
14. Bandorski D, Erkapic D, Stempfl J, Holtgen R, Grunig E, Schmitt J, et al. Ventricular tachycardias in patients with pulmonary hypertension: an underestimated prevalence? A prospective clinical study. Herzschrittmacherther Elektrophysiol. (2015) 26(2):155–62. doi: 10.1007/s00399-015-0364-8
15. Bandorski D, Bogossian H, Ecke A, Wiedenroth C, Gruenig E, Benjamin N, et al. Evaluation of the prognostic value of electrocardiography parameters and heart rhythm in patients with pulmonary hypertension. Cardiol J. (2016) 23(4):465–72. doi: 10.5603/CJ.a2016.0044
16. Brugada J, Katritsis DG, Arbelo E, Arribas F, Bax JJ, Blomstrom-Lundqvist C, et al. 2019 ESC guidelines for the management of patients with supraventricular tachycardiaThe task force for the management of patients with supraventricular tachycardia of the European society of cardiology (ESC). Eur Heart J. (2020) 41(5):655–720. doi: 10.1093/eurheartj/ehz467
17. Zeppenfeld K, Tfelt-Hansen J, de Riva M, Winkel BG, Behr ER, Blom NA, et al. 2022 ESC guidelines for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death. Eur Heart J. (2022) 43(40):3997–4126. doi: 10.1093/eurheartj/ehac262
18. Glikson M, Nielsen JC, Kronborg MB, Michowitz Y, Auricchio A, Barbash IM, et al. 2021 ESC guidelines on cardiac pacing and cardiac resynchronization therapy. Eur Heart J. (2021) 42(35):3427–520. doi: 10.1093/eurheartj/ehab364
19. Baumgartner H, Bonhoeffer P, De Groot NM, de Haan F, Deanfield JE, Galie N, et al. ESC Guidelines for the management of grown-up congenital heart disease (new version 2010). Eur Heart J. (2010) 31(23):2915–57. doi: 10.1093/eurheartj/ehq249
20. Lown B, Wolf M. Approaches to sudden death from coronary heart disease. Circulation. (1971) 44(1):130–42. doi: 10.1161/01.CIR.44.1.130
21. Bigger JT Jr., Weld FM. Analysis of prognostic significance of ventricular arrhythmias after myocardial infarction. Shortcomings of lown grading system. Br Heart J. (1981) 45(6):717–24. doi: 10.1136/hrt.45.6.717
22. Bastiaenen R, Batchvarov V, Gallagher MM. Ventricular automaticity as a predictor of sudden death in ischaemic heart disease. Europace. (2012) 14(6):795–803. doi: 10.1093/europace/eur342
23. Machraoui A, Schött D, Martin W, Lawo T, Barmeyer J, Ulmer WT. Ventricular arrhythmias in cor pulmonale. The effect of oxygen treatment. Dtsch Med Wochenschr. (1986) 111(14):535–8. doi: 10.1055/s-2008-1068485
24. Zipes DP, Camm AJ, Borggrefe M, Buxton AE, Chaitman B, Fromer M, et al. ACC/AHA/ESC 2006 guidelines for management of patients with ventricular arrhythmias and the prevention of sudden cardiac death–executive summary: a report of the American college of cardiology/American heart association task force and the European society of cardiology committee for practice guidelines (writing committee to develop guidelines for management of patients with ventricular arrhythmias and the prevention of sudden cardiac death) developed in collaboration with the European heart rhythm association and the heart rhythm society. Eur Heart J. (2006) 27(17):2099–140. doi: 10.1093/eurheartj/ehl199
25. Laboratories, A.T.S.C.o.P.S.f.C.P.F. ATS Statement: guidelines for the six-minute walk test. Am J Respir Crit Care Med. (2002) 166(1):111–7. doi: 10.1164/ajrccm.166.1.at1102
26. Baumgartner H, Hung J, Bermejo J, Chambers JB, Evangelista A, Griffin BP, et al. Echocardiographic assessment of valve stenosis: eAE/ASE recommendations for clinical practice. J Am Soc Echocardiogr. (2009) 22(1):1–23; quiz 101–2. doi: 10.1016/j.echo.2008.11.029
27. Lang RM, Badano LP, Mor-Avi V, Afilalo J, Armstrong A, Ernande L, et al. Recommendations for cardiac chamber quantification by echocardiography in adults: an update from the American society of echocardiography and the European association of cardiovascular imaging. J Am Soc Echocardiogr. (2015) 28(1):1–39.e14. doi: 10.1016/j.echo.2014.10.003
28. Rudski LG, Lai WW, Afilalo J, Hua L, Handschumacher MD, Chandrasekaran K, et al. Guidelines for the echocardiographic assessment of the right heart in adults: a report from the American society of echocardiography endorsed by the European association of echocardiography, a registered branch of the European society of cardiology, and the Canadian society of echocardiography. J Am Soc Echocardiogr. (2010) 23(7):685–713; quiz 786-8. doi: 10.1016/j.echo.2010.05.010
29. Zoghbi WA, Enriquez-Sarano M, Foster E, Grayburn PA, Kraft CD, Levine RA, et al. Recommendations for evaluation of the severity of native valvular regurgitation with two-dimensional and Doppler echocardiography. J Am Soc Echocardiogr. (2003) 16(7):777–802. doi: 10.1016/S0894-7317(03)00335-3
30. Wanamaker B, Cascino T, McLaughlin V, Oral H, Latchamsetty R, Siontis KC. Atrial arrhythmias in pulmonary hypertension: pathogenesis, prognosis and management. Arrhythm Electrophysiol Rev. (2018) 7(1):43–8. doi: 10.15420/aer.2018.3.2
31. Bandorski D, Bogossian H, Ghofrani A, Schmitt J, Holtgen R. Tachycardia and pulmonary arterial hypertension. Herzschrittmacherther Elektrophysiol. (2020) 31(1):33–8. doi: 10.1007/s00399-020-00668-w
32. Andersen MO, Diederichsen SZ, Svendsen JH, Carlsen J. Assessment of cardiac arrhythmias using long-term continuous monitoring in patients with pulmonary hypertension. Int J Cardiol. (2021) 334:110–5. doi: 10.1016/j.ijcard.2021.03.047
33. Fingrova Z, Ambroz D, Jansa P, Kuchar J, Lindner J, Kunstyr J, et al. The prevalence and clinical outcome of supraventricular tachycardia in different etiologies of pulmonary hypertension. PLoS ONE. (2021) 16(1):e0245752. doi: 10.1371/journal.pone.0245752
34. Uznanska-Loch B, Wiklo K, Trzos E, Wierzbowska-Drabik K, Chrzanowski L, Kasprzak JD, et al. Advanced and traditional electrocardiographic risk factors in pulmonary arterial hypertension: the significance of ventricular late potentials. Kardiol Pol. (2018) 76(3):586–93. doi: 10.5603/KP.a2017.0257
35. Xue L, Yang YC, Zhao Q, Zhao ZH, Zeng QX, Yang T, et al. The spectrum and prevalence of arrhythmia in different clinical pulmonary hypertension groups in Chinese population. Clin Cardiol. (2022) 45(5):495–502. doi: 10.1002/clc.23803
36. Cannillo M, Grosso Marra W, Gili S, D'Ascenzo F, Morello M, Mercante L, et al. Supraventricular arrhythmias in patients with pulmonary arterial hypertension. Am J Cardiol. (2015) 116(12):1883–9. doi: 10.1016/j.amjcard.2015.09.039
37. Kanmanthareddy A, Reddy YM, Boolani H, Duthuluru S, Pillarisetti J, Vallakati A, et al. Incidence, predictors, and clinical course of atrial tachyarrhythmias in patients with pulmonary hypertension. J Interv Card Electrophysiol. (2014) 41(1):9–14. doi: 10.1007/s10840-014-9928-5
38. Malaczynska-Rajpold K, Komosa A, Blaszyk K, Araszkiewicz A, Janus M, Olasinska-Wisniewska A, et al. The management of supraventricular tachyarrhythmias in patients with pulmonary arterial hypertension. Heart Lung Circ. (2016) 25(5):442–50. doi: 10.1016/j.hlc.2015.10.008
39. Smith B, Genuardi MV, Koczo A, Zou RH, Thoma FW, Handen A, et al. Atrial arrhythmias are associated with increased mortality in pulmonary arterial hypertension. Pulm Circ. (2018) 8(3):2045894018790316. doi: 10.1177/2045894018790316
40. Lin CY, Lin YJ, Chen YY, Chang SL, Lo LW, Chao TF, et al. Prognostic significance of premature atrial complexes burden in prediction of long-term outcome. J Am Heart Assoc. (2015) 4(9):e002192. doi: 10.1161/JAHA.115.002192
41. Himmelreich JCL, Lucassen WAM, Heugen M, Bossuyt PMM, Tan HL, Harskamp RE, et al. Frequent premature atrial contractions are associated with atrial fibrillation, brain ischaemia, and mortality: a systematic review and meta-analysis. Europace. (2019) 21(5):698–707. doi: 10.1093/europace/euy276
42. Bandorski D, Bogossian H, Stempfl J, Seeger W, Hecker M, Ghofrani A, et al. Prognostic relevance of nonsustained ventricular tachycardia in patients with pulmonary hypertension. Biomed Res Int. (2016) 2016:1327265. doi: 10.1155/2016/1327265
43. Witte C, Meyer Zur Heide Genannt Meyer-Arend JU, Andrie R, Schrickel JW, Hammerstingl C, Schwab JO, et al. Heart rate variability and arrhythmic burden in pulmonary hypertension. Adv Exp Med Biol. (2016) 934:9–22. doi: 10.1007/5584_2016_18
44. Yi HT, Hsieh YC, Wu TJ, Huang JL, Lin WW, Liang KW, et al. Heart rate variability parameters and ventricular arrhythmia correlate with pulmonary arterial pressure in adult patients with idiopathic pulmonary arterial hypertension. Heart Lung. (2014) 43(6):534–40. doi: 10.1016/j.hrtlng.2014.05.010
45. Goudis CA. Chronic obstructive pulmonary disease and atrial fibrillation: an unknown relationship. J Cardiol. (2017) 69(5):699–705. doi: 10.1016/j.jjcc.2016.12.013
46. Kusunoki Y, Nakamura T, Hattori K, Motegi T, Ishii T, Gemma A, et al. Atrial and ventricular arrhythmia-associated factors in stable patients with chronic obstructive pulmonary disease. Respiration. (2016) 91(1):34–42. doi: 10.1159/000442447
47. Rosas-Peralta M, Sandoval-Zarate J, Attie F, Pulido T, Santos E, Granados NZ, et al. Clinical implications and prognostic significance of the study on the circadian variation of heart rate variability in patients with severe pulmonary hypertension. Gac Med Mex. (2006) 142(1):19–28.16548288
48. Benoist D, Stones R, Drinkhill M, Bernus O, White E. Arrhythmogenic substrate in hearts of rats with monocrotaline-induced pulmonary hypertension and right ventricular hypertrophy. Am J Physiol Heart Circ Physiol. (2011) 300(6):H2230–7. doi: 10.1152/ajpheart.01226.2010
49. Tanaka Y, Takase B, Yao T, Ishihara M. Right ventricular electrical remodeling and arrhythmogenic substrate in rat pulmonary hypertension. Am J Respir Cell Mol Biol. (2013) 49(3):426–36. doi: 10.1165/rcmb.2012-0089OC
50. Strauss B, Bisserier M, Obus E, Katz MG, Fargnoli A, Cacheux M, et al. Right predominant electrical remodeling in a pure model of pulmonary hypertension promotes reentrant arrhythmias. Heart Rhythm. (2022) 19(1):113–24. doi: 10.1016/j.hrthm.2021.09.021
51. Strauss B, Sassi Y, Bueno-Beti C, Ilkan Z, Raad N, Cacheux M, et al. Intra-tracheal gene delivery of aerosolized SERCA2a to the lung suppresses ventricular arrhythmias in a model of pulmonary arterial hypertension. J Mol Cell Cardiol. (2019) 127:20–30. doi: 10.1016/j.yjmcc.2018.11.017
52. Rain S, Handoko ML, Trip P, Gan CT, Westerhof N, Stienen GJ, et al. Right ventricular diastolic impairment in patients with pulmonary arterial hypertension. Circulation. (2013) 128(18):2016–25; 1–10. doi: 10.1161/CIRCULATIONAHA.113.001873
53. van der Bruggen CE, Happe CM, Dorfmuller P, Trip P, Spruijt OA, Rol N, et al. Bone morphogenetic protein receptor type 2 mutation in pulmonary arterial hypertension: a view on the right ventricle. Circulation. (2016) 133(18):1747–60. doi: 10.1161/CIRCULATIONAHA.115.020696
54. Medi C, Kalman JM, Ling LH, Teh AW, Lee G, Lee G, et al. Atrial electrical and structural remodeling associated with longstanding pulmonary hypertension and right ventricular hypertrophy in humans. J Cardiovasc Electrophysiol. (2012) 23(6):614–20. doi: 10.1111/j.1540-8167.2011.02255.x
55. Chung HH, Kim JB, Hong SH, Lee HJ, Joung B, Lee MH. Radiofrequency catheter ablation of hemodynamically unstable ventricular tachycardia associated with systemic sclerosis. J Korean Med Sci. (2012) 27(2):215–7. doi: 10.3346/jkms.2012.27.2.215
56. Boulos M, Lashevsky I, Reisner S, Gepstein L. Electroanatomic mapping of arrhythmogenic right ventricular dysplasia. J Am Coll Cardiol. (2001) 38(7):2020–7. doi: 10.1016/S0735-1097(01)01625-4
Keywords: pulmonary hypertension, PH, Holter ECG, arrhythmias, prognosis
Citation: Bandorski D, Heibel S, Höltgen R, Bogossian H, Ghofrani HA, Zarse M and Gall H (2023) Incidence and prognostic significance of malignant arrhythmias during (repetitive) Holter electrocardiograms in patients with pulmonary hypertension. Front. Cardiovasc. Med. 10:1084051. doi: 10.3389/fcvm.2023.1084051
Received: 29 October 2022; Accepted: 20 March 2023;
Published: 17 April 2023.
Edited by:
Grigorios Korosoglou, GRN Klinik Weinheim, GermanyReviewed by:
Lukas Jaroslaw Motloch, University Hospital Salzburg, Paracelsus Medical University, Austria© 2023 Bandorski, Heibel, Höltgen, Bogossian, Ghofrani, Zarse and Gall. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Dirk Bandorski ZGlyay5iYW5kb3Jza2lAdC1vbmxpbmUuZGU=
†These authors have contributed equally to this work and share first authorship
Specialty Section: This article was submitted to Cardiac Rhythmology, a section of the journal Frontiers in Cardiovascular Medicine
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.