
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Cardiovasc. Med. , 23 February 2023
Sec. Heart Valve Disease
Volume 10 - 2023 | https://doi.org/10.3389/fcvm.2023.1076708
This article is part of the Research Topic Comprehensive Insights into Mitral Valve Prolapse: From biology to future perspectives of treatment, passing through diagnostic tools, surgical techniques and transcatheter options View all 12 articles
 Elisabeth Petolat1,2†
Elisabeth Petolat1,2† Alexis Theron2†
Alexis Theron2† Noemie Resseguier3Cyprien Fabre3Giulia Norscini1Rita Badaoui2Gilbert Habib1Frederic Collart2
Noemie Resseguier3Cyprien Fabre3Giulia Norscini1Rita Badaoui2Gilbert Habib1Frederic Collart2 Stéphane Zaffran4
Stéphane Zaffran4 Alizée Porto2Jean-François Avierinos1*
Alizée Porto2Jean-François Avierinos1*Background: Degenerative mitral regurgitation (DMR) due to mitral valve prolapse (MVP) is a common valve disease associated with significant morbidity and mortality. Timing for surgery is debated for asymptomatic patients without Class I indication, prompting the search for novel parameters of early left ventricular (LV) systolic dysfunction.
Aims: To evaluate the prognostic impact of preoperative forward flow indices on the occurrence of post-operative LV systolic dysfunction.
Methods: We retrospectively included all consecutive patients with severe DMR due to MVP who underwent mitral valve repair between 2014 and 2019. LVOTTVI, forward stroke volume index, and forward LVEF were assessed as potential risk factors for LVEF <50% at 6 months post-operatively.
Results: A total of 198 patients were included: 154 patients (78%) were asymptomatic, and 46 patients (23%) had hypertension. The mean preoperative LVEF was 69 ± 9%. 35 patients (18%) had LVEF ≤60%, and 61 patients (31%) had LVESD ≥40 mm. The mean post-operative LVEF was 59 ± 9%, and 21 patients (11%) had post-operative LVEF<50%. Based on multivariable analysis, LVOTTVI was the strongest independent predictor of post-operative LV dysfunction after adjustment for age, sex, symptoms, LVEF, LV end systolic diameter, atrial fibrillation and left atrial volume index (0.75 [0.62–0.91], p < 0.01). The best sensitivity (81%) and specificity (63%) was obtained with LVOTTVI ≤15 cm based on ROC curve analysis.
Conclusion: LVOTTVI represents an independent marker of myocardial performance impairment in the presence of severe DMR. LVOTTVI could be an earlier marker than traditional echo parameters and aids in the optimization of the timing of surgery.
Mitral valve prolapse (MVP) is a common valvular heart disease with a prevalence that approaches that of bicuspid aortic valve and is estimated to occur in between 0.6 and 2.4% of the population (1, 2). MVP has been the leading cause for severe primary mitral regurgitation (MR) requiring surgery in western countries for five decades (3). Mitral valve repair can be achieved in most patients, improving symptoms and restoring life expectancy when surgery is performed before left ventricular (LV) systolic dysfunction, which remains the ultimate complication of organic MR (4), the first cause of post-operative mortality (5) and the hinge point of the highly debated optimal timing for surgical correction. Severe degenerative MR (DMR) management is a controversial topic between defenders of a traditional symptom waiting approach (6) and supporters of earlier surgical strategies (7, 8). The latter note the challenge of early detection of LV impairment in the presence of severe MR-related altered loading conditions (9, 10), the high incidence of unexpected post-operative LV dysfunction despite normal preoperative LV parameters and observational data reporting restoration of outcome after early repair (11–13). In this context, both US and European guidelines rely on clinical and echo triggers to determine the timing for surgery (14, 15), noting that the post-operative outcome of symptomatic patients (16) and of those with preoperative decreased LV ejection fraction (EF) (10) or increased LV end-systolic diameters (LVESD) (9) might not be optimal. Therefore, the aforementioned guidelines open the door for earlier surgical strategies as class IIa indications in patients with no symptoms and normal LV echocardiographic parameters (14, 15) provided that repair is feasible in a high volume Heart Valve Center. However, European guidelines mention left atrial (LA) dilation as an additional condition (15), underlining the current ambiguity surrounding primary MR management. This controversy has prompted cardiologists to search for new indicators of earlier evidence of LV systolic dysfunction in patients with severe DMR to refine surgical timing in asymptomatic patients with normal classic LV echographic markers (17–20). Among those, we tested the hypothesis that in the presence of severe DMR, alterations in forward LV ejection markers, specifically LV outflow tract velocity-time integral (LVOTTVI) and stroke volume index (SVi), could represent simple and reproducible indicators of early LV systolic dysfunction, helping risk stratification and decision-making.
We conducted an observational retrospective single-center study that included all consecutive patients with severe primary degenerative MR (DMR) due to MVP who underwent MV repair between 2014 and 2019, whose forward SVi was available and whose post-operative follow-up (FU) was ≥6 months. Exclusion criteria were outside echocardiographic diagnosis without institutional full evaluation, secondary MR, mitral stenosis, significant aortic valve disease, previous valvular surgery, congenital heart disease and patients with incomplete or unavailable clinical or echo data. Coronary artery disease was not considered an exclusion criterion if it did not generate secondary MR. Patients who denied authorization for anonymous publication of their clinical data for research purposes were also excluded. The study was conducted in accordance with institutional guidelines, national legal requirements and the revised Declaration of Helsinki. All included patients provided written consent for research and publication of their study data (IRB approval number 2019-48).
Data from clinical examination, 12-lead ECG and transthoracic echocardiography (TTE) performed in our institution by experienced cardiologists within 3 months prior to surgery and at 6 months FU were available in all patients. Transthoracic echocardiograms were performed within routine clinical practice using standard methods (21, 22). LV and LA diameters and volumes were recorded in the long axis parasternal and apical views, and the left ventricular ejection fraction (LVEF) was estimated visually using the Simpson biplane method. The diagnosis of MVP was made as recommended (1), and the diagnosis of flail leaflet was based on failure of leaflet coaptation with rapid systolic movement of the flail segment into the LA (23, 24). MR severity was assessed following an integrative approach as recommended (22). Original data were used that were unaltered from the original prospective echocardiographic data collection by means of electronic transfer. The LV outflow tract (LVOT) diameter was measured in the parasternal long axis view, and LVOTTVI was recorded as recommended (22) by pulse wave Doppler in the apical 5-chamber view. Three cardiac cycles at least in sinus rhythm and 10 in atrial fibrillation were averaged. Stroke volume (SV) was calculated as the product of LVOT area by LVOTTVI and was indexed to body surface area (BSA) and referred to as SVi. A threshold of <35 ml/m2 was considered as a priori abnormal by reference to aortic stenosis (25). Forward LVEF was calculated as the ratio of LVOT stroke volume to LV end-diastolic volume (LVEDV), and a value <50% was considered abnormal (26).
The endpoint was the occurrence of post-operative LV systolic dysfunction defined by an LVEF <50% at ≥6 months after MV repair (27). Quantitative variables were described as the means ± standard deviations, and qualitative variables were described as numbers and percentages. Non-normally distributed data were reported as median and interquartile ranges. For univariate analyses, comparisons between groups according to the primary endpoint were made using the Chi2 test if valid (Fisher's exact test otherwise) for the qualitative variables and using Student's t-test if valid (Mann–Whitney test otherwise) for the quantitative variables. For echocardiographic parameters, a univariate logistic regression model was used to estimate crude odds ratios with their 95% CIs quantifying the excess risk of post-operative LV dysfunction. Multivariate analyses were then performed to assess the independent effect of echocardiographic parameters while taking into account potential prognostic factors selected beforehand according to the literature data and to the results of univariate analysis. Adjusted odds ratios were estimated with their 95% CIs. Firth's correction was applied by performing Firth's penalized-likelihood logistic regression to take into account the small number of post-operative LV dysfunction.
Receiver operating characteristic (ROC) curves were established to determine the optimal cutoff value of echocardiographic parameters to predict post-operative LV dysfunction. Echocardiographic parameters were then dichotomized according to the identified cutoff values. Univariate and multivariate Firth's penalized-likelihood logistic regression models were built to estimate crude and adjusted odds ratios with their 95% CIs related to these dichotomized parameters for predicting post-operative LV dysfunction.
All tests were two-sided. All p-values<0.05 were considered significant. We used R version 4.0.5 for all statistical analyses.
One hundred ninety-eight patients were included between 2014 and 2019. The mean age was 64 ± 13 years. The majority of patients were males (74%), and 45 (23%) had a history of atrial fibrillation (AF), which was permanent in 22 (11%). The majority of patients were in NYHA class I-II (78%) at the time of surgery. The mean BNP level was 126 ± 133 pg/ml, and the Euroscore was low (Table 1). All patients had severe DMR as attested by quantitative parameters and the high prevalence of flail leaflets (mean effective regurgitant orifice (ERO) = 50 ± 15 mm2). The middle portion of the posterior leaflet (P2) was the most frequently involved segment either isolated or in combination with other locations. The mean preoperative LVEF was normal, but 35 (18%) patients had a preoperative LVEF ≤60%, and 2 (1%) had an LVEF<50%. The mean LVESD was 35 ± 7 mm, and 61 (31%) patients had LVESD ≥40 mm. The mean LA volume index (LAVI) was 72 ± 24 ml/m2, and 131 (66%) patients had an LAVI ≥60 ml/m2. The mean systolic pulmonary artery pressure (sPAP) was 40 ± 15 mmHg, and 36 (18%) patients had sPAP>50 mmHg. The mean LVOTTVI was 16 ± 3 cm. The forward SVi was 37 ± 8 ml/m2, and 88 (44%) patients had a forward SVi <35 ml/m2. The mean forward LVEF was 38 ± 13%, and 167 (84%) patients had forward LVEF<50% (Table 2).
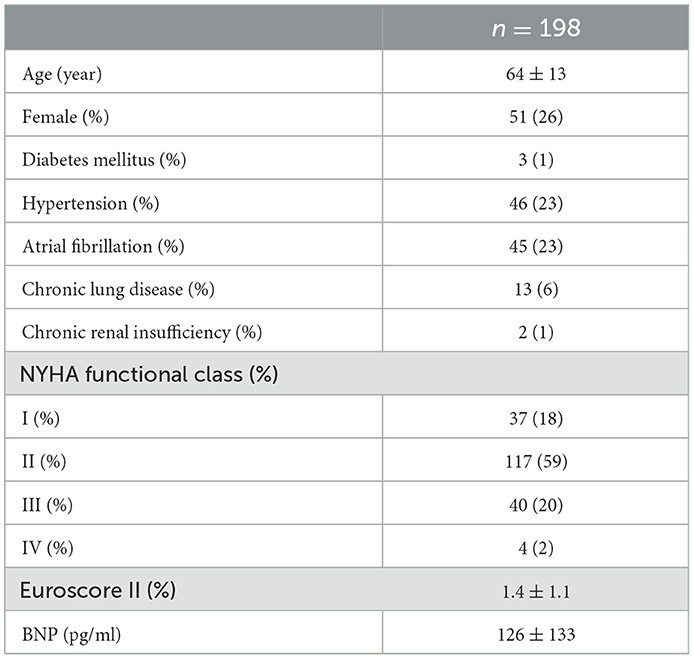
Table 1. Preoperative clinical characteristics of 198 patients subject to mitral valve repair for severe DMR.
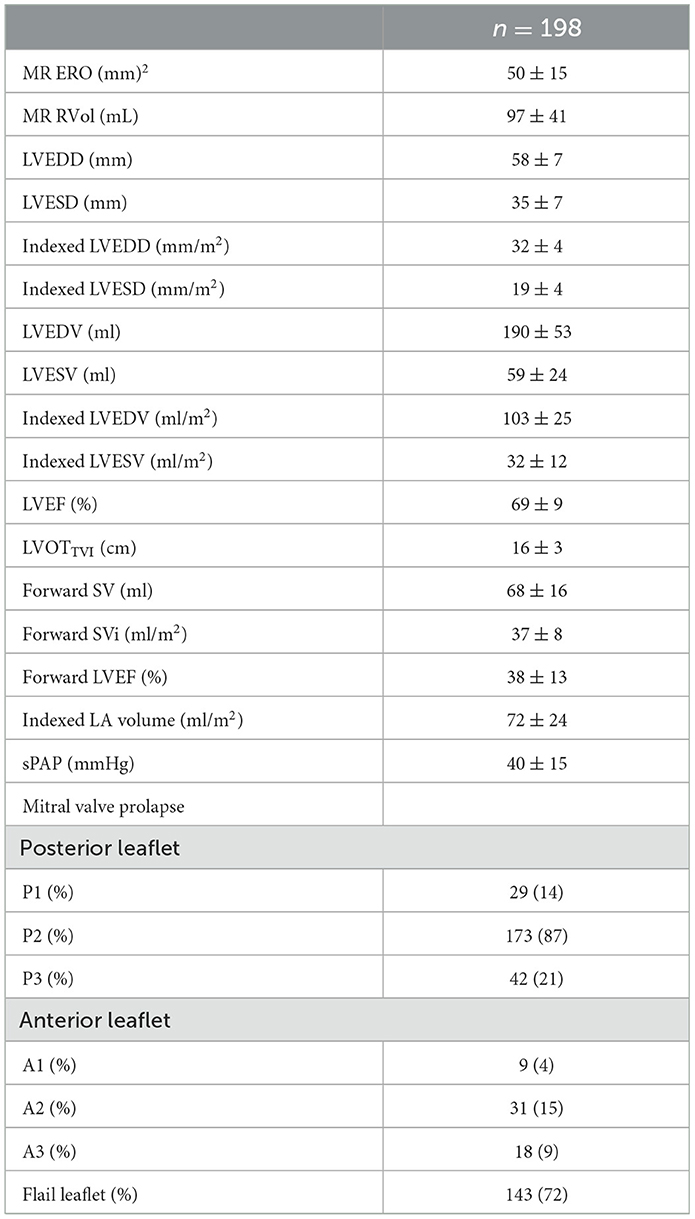
Table 2. Pre-operative echocardiographic characteristics of 198 patients subject to mitral valve repair for severe DMR.
Surgery was indicated by symptoms or LVEF ≤60% or LVESD ≥40 mm (class I indications) in 102 (51.5%) patients and by AF or sPAP ≥50 mmHg while asymptomatic with no overt LV dysfunction (Class IIa indications) in 23 (11.5%). In addition, 73 (37%) patients had “early” class IIa indications (asymptomatic and sinus rhythm and sPAP <50 mmHg and LVEF >60% and LVESD < 40 mm).
All patients underwent MV repair, including 150 patients (76%) with neo-chordae and 48 patients (24%) with leaflet resection. An annuloplasty ring was implanted in all patients. The mean duration of cross-clamping time was 55 ± 18 min. Operative trans-TEE showed no residual MR in 99 (50%) patients, mild MR in 95 (48%) patients and moderate MR in 4 (2%) patients. The LVEF was 55 ± 9% at discharge. No operative deaths or post-operative strokes were noted.
TTE performed at 6 months after FU in all 198 patients showed a mean LVEF of 59 ± 9% with 21 (11%) patients displaying post-operative LV dysfunction. The vast majority of patients had no or trivial MR, 21 (11%) had mild MR, and none had moderate or severe MR.
Univariate risk factors for post-operative LV systolic dysfunction are listed in Table 3 (Figure 1).
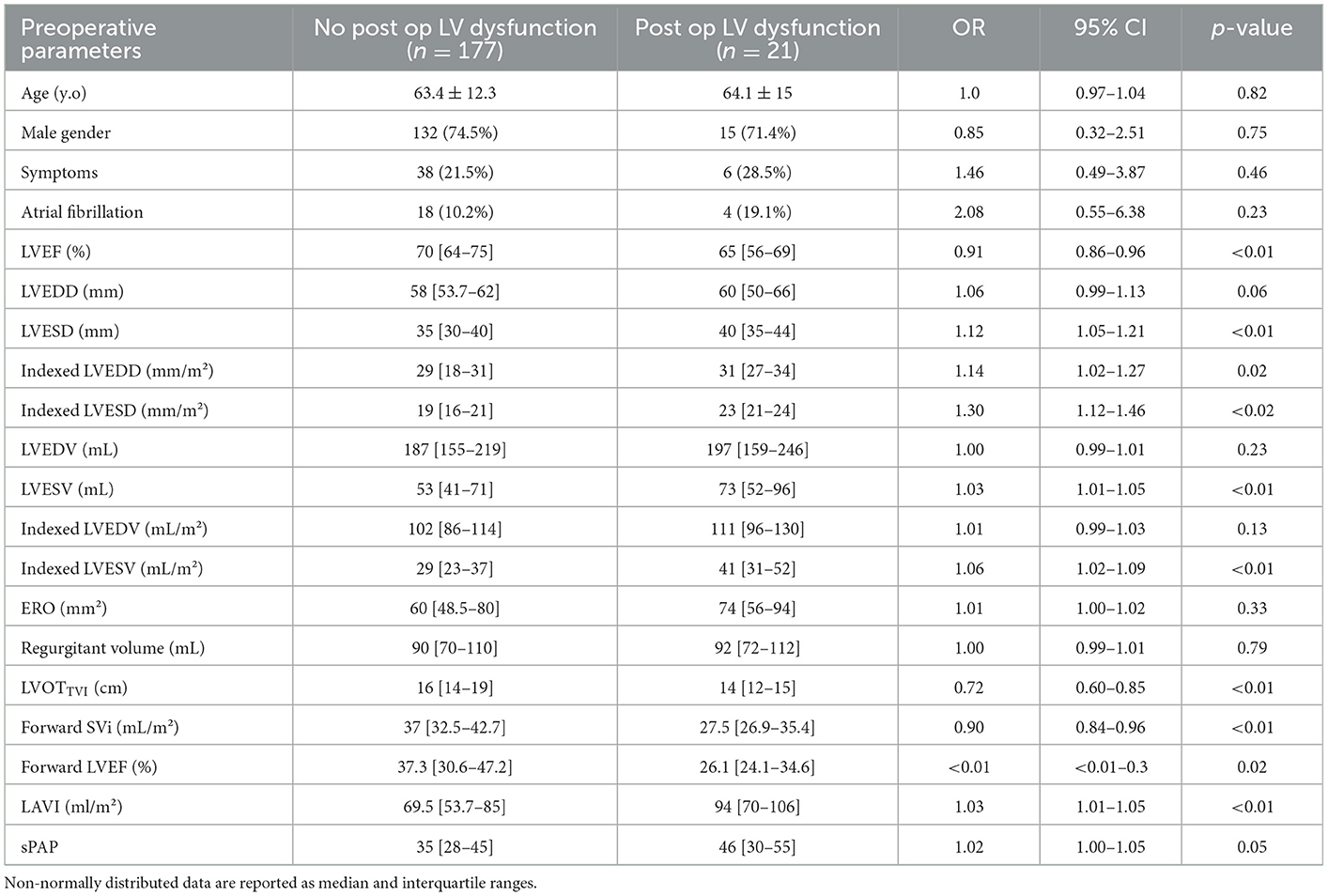
Table 3. Univariate risk factor analysis for predicting post-operative LV systolic dysfunction in 198 patients undergoing mitral valve repair for severe DMR.
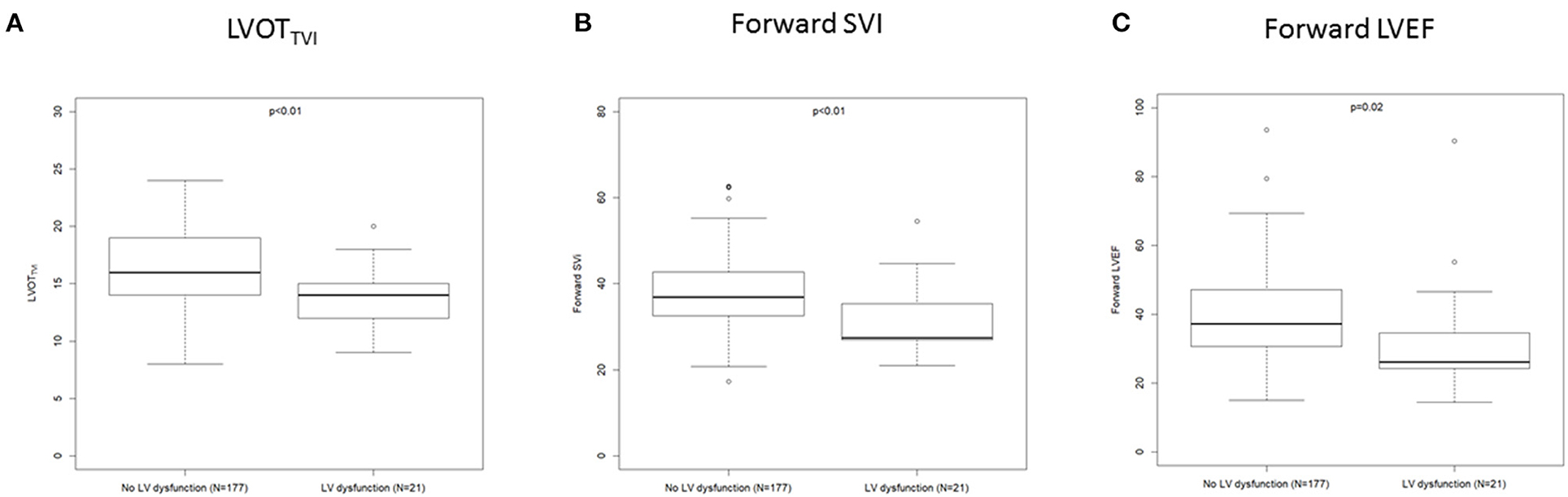
Figure 1. Box plot showing LVOTTVI (A), forward SVi (B), and forward LVEF (C) according to the occurrence of post operative LV dysfunction.
Multivariate analysis (OR [95% CI], p) revealed the following results:
▪ After adjustment for age, sex, NYHA class, LVEF, LVESD and AF, LVOTTVI (0.75 [0.62–0.91], p < 0.01) and mean forward SVi (0.93 [0.87–0.99], p = 0.02) were independently associated with post-operative LV systolic dysfunction, whereas forward LVEF exhibited borderline significance (0.96 [0.92–1.00], p = 0.07). The impact of all classic predictors confirmed in univariate analysis disappeared when simultaneously combined with either LVOTTVI or forward SVi with the exception of LVESD, which remained significant. However, the OR was lower than that of LVOTTVI (Table 4).
▪ After further adjustment for LAVI, LVOTTVI (0.77 [0.64–0.94], p = 0.008) and forward SVi (0.93 [0.87–0.99], p = 0.03) were independently associated with post-operative LV systolic dysfunction, whereas forward LVEF was not (0.96 [0.90–1.01], p = 0.27). The impact of all classic predictors confirmed in univariate analysis disappeared when simultaneously combined with either LVOTTVI or forward SVi with the exception of LVESD and LAVI, which remained significant. However, the OR were lower than that of LVOTTVI (Table 5).
▪ Adjustment to LV end-diastolic volume (LVESV) instead of LVESD did not change the independent impact of LVOTTVI (0.77 [0.64–0.93], p = 0.007) and forward SVi (0.92 [0.86–0.99], p = 0.02), whereas forward LVEF remained nonsignificantly associated with post-operative LV dysfunction (0.96 [0.90–1.01], p = 0.11).
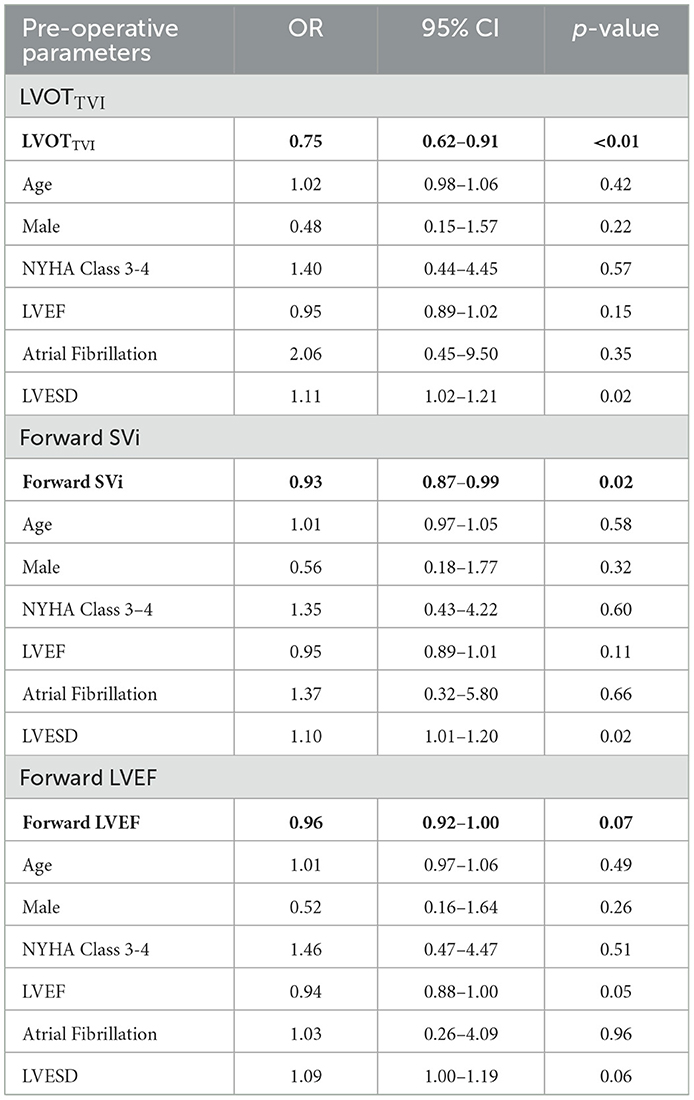
Table 4. Multivariable risk factor analysis for predicting post-operative LV systolic dysfunction in 198 patients undergoing mitral valve repair for severe DMR.
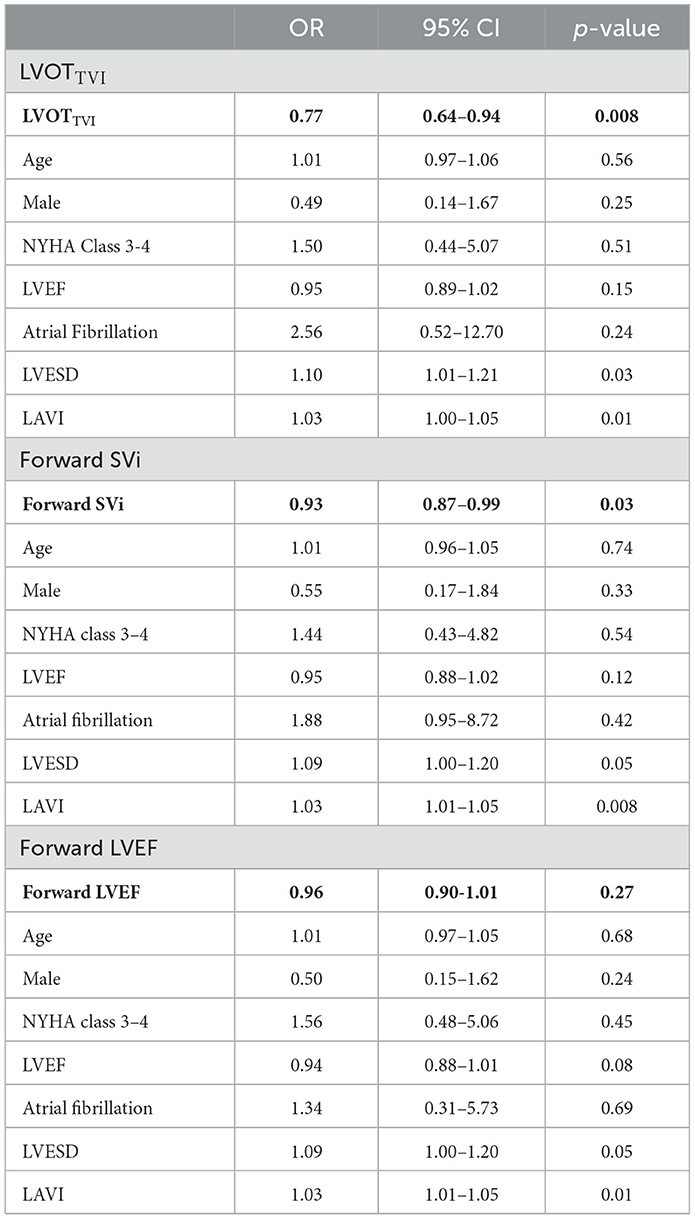
Table 5. Multivariable risk factor analysis for predicting post-operative LV systolic dysfunction in 198 patients subject to mitral valve repair for severe DMR after further adjustment to LAVI.
ROC curves identified thresholds of 15 cm for LVOTTVI (Se = 81% and Sp = 63%), 31 ml/m2 for forward SVI (Se = 67% and Sp = 79%) and 30% for forward LVEF (Se = 62% and Sp = 79%) as the most accurate in predicting post-operative LV dysfunction (Figure 2).
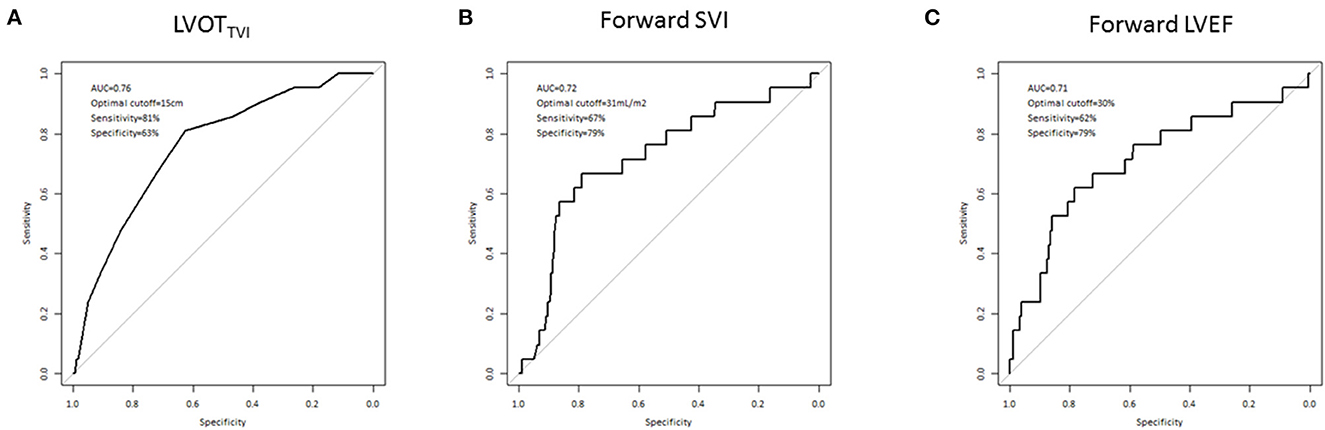
Figure 2. Optimal thresholds for LVOTTVI (A), forward SVi (B), and forward LVEF (C) in predicting post-operative LV systolic dysfunction in 198 patients undergoing mitral valve repair for severe DMR according to ROC curve analysis.
After adjustment for age, sex, NYHA class, LVEF, LVESD, AF, and LAVI, LVOTTVI ≤15 cm (5.97 [1.74–20.50], p < 0.01), forward SVI ≤31 mL/m2 (4.15 [1.43–12.05], p < 0.01) and forward LVEF ≤30% (4.02 [1.31–12.36], p = 0.01) were strongly and independently associated with post-operative LV systolic dysfunction. The impact of LVESD and LAVI was weaker in all models, as attested by the lower OR (Table 6, Supplementary Tables 2S, 3S, 4S).
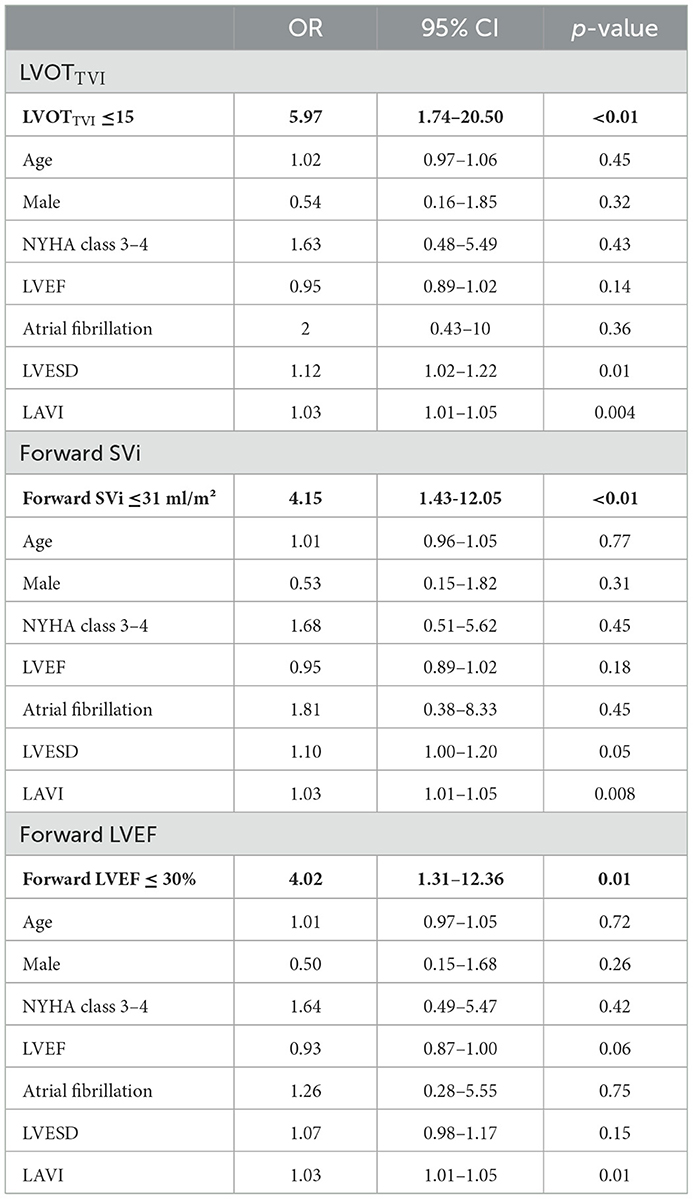
Table 6. Multivariable risk factor analysis for predicting post-operative LV systolic dysfunction in 198 patients subject to mitral valve repair for severe DMR using cutoff values for LVOTTVI, SVi and forward LVEF defined by ROC curve analysis.
Among 95 asymptomatic patients with preoperative LVEF >60% and LVESD <40 mm, 5 patients (5%) developed “unexpected” LV systolic dysfunction. Among these five patients, the mean LVOTTVI was 13.8 ± 2.3 cm, and four patients (80%) had an LVOTTVI ≤15 cm. The forward SVi was 32.8 ± 4.5 ml/m2. The two patients (40%) had a forward SVi ≤31 ml/m2. The mean forward LVEF was 30 ± 3.1% and four patients (80%) had a forward LVEF ≤30%. All of these five patients had at least one of these markers.
Our study including 198 patients with MV repair for severe DMR due to MVP showed that (1) post-operative LV systolic dysfunction occurred in 11% of all patients and in 5% of asymptomatic patients despite normal preoperative classic echocardiographic LV parameters; (2) LVOTTVI and forward SVI were identified as independent risk factors for post-operative LV dysfunction and appeared to be stronger predictors than classic clinical and echocardiographic markers, particularly LVEF; and (3) thresholds of 15 cm for LVOTTVI and 31 ml/m2 for forward SVI could be early indicators of latent LV dysfunction, helping risk stratification and decision-making.
In the absence of randomized trials, DMR due to MVP has nourished a passionate controversy around the optimal timing of surgical indication in asymptomatic patients without signs of overt LV dysfunction for more than two decades. In this debate, supporters of early strategies (13, 23, 28–31) are facing guardians of the historical conservative approach (6, 32). The so-called watchful waiting approach argues that close follow-up until the occurrence of overt symptoms or patent LV dysfunction is not associated with outcome penalty based on two observational studies including small populations with likely moderate MR attested by low LV volumes (6, 32). In contrast, early surgical correction of DMR is supported by profuse observational studies, which reported a strong association between preoperative severe symptoms, decreased LVEF (16), increased LVESD (27), occurrence of AF (33) or pulmonary hypertension, and adverse outcomes both under conservative management and post-operatively (8). In addition, early repair has been associated with LA and LV function preservation (7, 8, 12, 18, 34), better post-operative outcomes than the conservative approach after propensity score matching (13, 29, 30), and restoration of normal life expectancy (35).
LV systolic dysfunction is the ultimate adverse consequence of primary MR and the first cause of post-operative mortality (5, 34). As such, its prevention remains the primary target of DMR treatment. In the compensated stage of chronic MR, LV remodeling is indeed the compensatory response to volume overload, which promotes extracellular matrix disturbances, including dissolution of collagen fibers and rearrangement of myocardial fibers. The transition to the decompensated stage of chronic MR is promoted by a reduction of the sarco-endoplasmic reticulum Ca2+ATPase2, which is also referred to as SERCA 2, and an increase in the secretion of matrix metalloproteinases that initiates matrix proteolytic activity, cell apoptosis and ultimately impaired myocardial contractility (4). Preservation of LV systolic properties by eliminating volume overload “on time” therefore appears to represent the challenge in DMR management. However, assessment of LV systolic function by traditional echocardiographic indices is obscured by the modified loading conditions induced by MR. Classic markers, such as LVEF and LVESD, are pertinent indicators of patent LV dysfunction when altered (9, 10). However, these markers suffer from low sensitivity in the detection of early LV systolic impairment, which might already be present despite normal preoperative values and is subsequently unmasked post-operatively. This phenomenon is referred to as the so-called unexpected post-operative LV dysfunction (27).
Consequently, efforts have been focused on defining new surgical signals with the common objective of preserving LV function, but none have been fully validated to date. Myocardial deformation has been investigated (36), and patients with post-operative LV dysfunction have been shown to have alterations in preoperative global longitudinal strain (GLS). Although GLS seems to be more sensitive than LVEF to detect patients with LV dysfunction in severe MR, it is limited by the need for high-quality images, imperfect sensitivity and variability of GLS thresholds from one echo manufacturer to another. The detection of diffuse myocardial fibrosis by T1 mapping in MRI is currently the subject of active ongoing research and seems promising (37, 38). However, MRI suffers from its lower accessibility than TTE in routine practice. Upstream of LV parameters and mitral valve, LAVI was reported as an independent risk factor for events in patients under conservative treatment (39). However, preoperative LA remodeling is physiologically connected to the occurrence of AF and its dismal consequences both under conservative management and post-operatively (31, 40, 41). In the absence of new effective markers, current guidelines still rely on classic parameters but acknowledge their limitations and open the door for early strategies in asymptomatic patients without Class I signals as reasonable Class IIa indications (14, 15). It is however conceivable that within this subset of asymptomatic patients with normal LVEF and without extreme cavity remodeling, some could benefit from watchful waiting, whereas others should promptly undergo surgery. In this context and in an attempt to refine risk stratifications, we investigated the impact of forward flow indices in predicting the risk of post-operative LV dysfunction in DMR. Indeed, in the presence of MR and despite volume overload, global LV afterload does not increase at variance with aortic regurgitation (AR) due to the double outlet (42), and LV ejection is distributed between forward and backward flow. Forward flow in the setting of MR partly reflects the ability of myocardium to eject forward against arterial afterload instead of regurgitating backward in the low-resistance LA. As such, one can assume that markers of forward flow better reflect LV intrinsic systolic performance than LVEF and LVESD, which implicitly integrate both antegrade and retrograde streams and may overestimate LV systolic function in case of severe MR. In our study population of patients who all benefited from surgical mitral repair, the traditional impact of LVEF and LVESD in predicting post-operative LV dysfunction were actually supplanted by two forward flow indices which, decreased values could be pertinent indicators of systolic dysfunction at an early stage. LVOTTVI and forward SVi were thus strong determinants of post-operative LV systolic dysfunction independent of all known risk factors for outcome. Importantly, all cases of unexpected LV dysfunction could have been detected by alteration of either one of these factors. These data are congruent with a previously published index of LV performance using LVOTTVI in combination with LVESD, which suffered from mixing forward and backward markers (20). Forward LVEF did not reach significance when considered as a continuous variable but did so when the threshold of 30% was considered, which is more restrictive than the previously reported value of 50% (26). Forward LVEF has been identified as predictive of a composite criterion combining MV surgery and post-operative LV systolic dysfunction among patients with severe primary MR and normal ejection fraction (26). This parameter appeared less robust in our data for unclear reasons but might be related to a lack of power or technical issues. LVOTTVI is indeed a surrogate for stroke volume (SV) that is easy to obtain in routine practice with low skill requirements in contrast to forward SVI and forward LVEF. Both of these parameters indeed require the tricky measurement of LV outflow tract diameter, the squared value of which magnifies any inaccuracy in its recording. In addition, forward LVEF requires LV tracing and perfect apical views. Despite reflecting the same physiologic concept, the increased robustness of LVOTTVI observed in our study population could be the consequence of such methodological matters.
Given the retrospective design and relatively small study population employed in this study, these findings require validation in future large-scale prospective studies. Hypertension was present in 23% of patients, and high blood pressure values at the time of echo could have artificially decreased forward flow indices independent of LV function. However, the consistency of their predictive value in all multivariable models and their incremental values over classic signals, particularly in detecting unexpected LV dysfunction, does not favor this hypothesis. In addition, the predictive value of LVOTTVI reported in this study in DMR is consistent with its known impact in the risk stratification of several cardiac diseases, including congestive heart failure (43), stable coronary artery disease and acute myocardial infarction. Decreased LVEF 6 months after mitral surgery is a debatable surrogate for irrevocable post-operative LV dysfunction, which might recover later on but was previously used as an acceptable substitution criterion (27). LVEF follow-up beyond 6 months could help refine the long-term impact of preoperative forward flow index alterations in the quest for ideal surgical signals, i.e., those that indicate surgery without compromising post-operative outcome. Such a signal does not exist in the setting of severe primary MR at present.
In patients with severe DMR, forward flow parameters could represent pertinent indicators of intrinsic LV performance, and alterations in these parameters could serve as earlier markers of latent LV dysfunction compared with conventional echocardiographic indices. Among these parameters, LVOTTVI appears to be the most robust and could be used as an easy recording tool in routine practice for risk stratification, thereby refining surgical indications in patients with no Class I or IIa indications.
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
The studies involving human participants were reviewed and approved by APHM Assistance publique des Hopitaux de Marseille, RGPD: 2019-48 (please see Supplementary files). The patients/participants provided their written informed consent to participate in this study.
All authors listed have made a substantial, direct, and intellectual contribution to the work and approved it for publication.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fcvm.2023.1076708/full#supplementary-material
AF, Atrial fibrillation; AR, Aortic regurgitation; BSA, Body surface area; BNP, Brain natriuretic peptide; DMR, Degenerative mitral regurgitation; EF, Ejection fraction; ERO, Effective regurgitant orifice; FU, Follow up; GLS, Global longitudinal strain; LA, Left atrium; LAVI, Left atrial volume index; LV, Left ventricle; LVEDD, Left ventricular end-diastolic diameter; LVEDV, Left ventricular end-diastolic volume; LVEF, Left ventricular ejection fraction; LVESD, Left ventricular end-systolic diameter; LVESV, Left ventricular end-systolic volume; LVOT, Left ventricular outflow tract; LVOTTVI, Left ventricular outflow tract velocity-time integral; MR, Mitral regurgitation; MRI, Magnetic resonance imaging; MV, Mitral valve; MVP, Mitral valve prolapse; NYHA, New York Heart Association; ROC, Receiver operating characteristic; Rvol, Regurgitant Volume; sPAP, Systolic pulmonary artery pressure; Svi, Stroke volume indexed to BSA; TTE, Transthoracic echocardiography; TVI, Time-velocity integral.
1. Freed LA, Levy D, Levine RA, Larson MG, Evans JC, Fuller DL, et al. Prevalence and clinical outcome of mitral-valve prolapse. N Engl J Med. (1999) 341:1–7. doi: 10.1056/NEJM199907013410101
2. Nkomo VT, Gardin JM, Skelton TN, Gottdiener JS, Scott CG, Enriquez-Sarano M. Burden of valvular heart diseases: a population-based study. The Lancet. (2006) 368:1005–11. doi: 10.1016/S0140-6736(06)69208-8
3. Olson LJ, Subramanian R, Ackermann DM, Orszulak TA, Edwards WD. Surgical pathology of the mitral valve: a study of 712 cases spanning 21 years. Mayo Clin Proc. (1987) 62:22–34. doi: 10.1016/S0025-6196(12)61522-5
4. Pu M, Gao Z, Zhang X, Liao D, Pu DK, Brennan T, et al. Impact of mitral regurgitation on left ventricular anatomic and molecular remodeling and systolic function: implication for outcome. Am J Physiol-Heart Circ Physiol. (2009) 296:H1727–32. doi: 10.1152/ajpheart.00882.2008
5. Enriquez-Sarano M, Tajik AJ, Schaff HV, Orszulak TA, McGoon MD, Bailey KR, et al. Echocardiographic prediction of left ventricular function after correction of mitral regurgitation: Results and clinical implications. J Am Coll Cardiol. (1994) 24:1536–43. doi: 10.1016/0735-1097(94)90151-1
6. Rosenhek R, Rader F, Klaar U, Gabriel H, Krejc M, Kalbeck D, et al. Outcome of watchful waiting in asymptomatic severe mitral regurgitation. Circulation. (2006) 113:2238–44. doi: 10.1161/CIRCULATIONAHA.105.599175
7. Enriquez-Sarano M, Sundt TM. Early surgery is recommended for mitral regurgitation. Circulation. (2010) 121:804–12. doi: 10.1161/CIRCULATIONAHA.109.868083
8. Enriquez-Sarano M, Suri RM, Clavel MA, Mantovani F, Michelena HI, Pislaru S, et al. Is there an outcome penalty linked to guideline-based indications for valvular surgery? Early and long-term analysis of patients with organic mitral regurgitation. J Thorac Cardiovasc Surg. (2015) 150:50–8. doi: 10.1016/j.jtcvs.2015.04.009
9. Tribouilloy C, Grigioni F, Avierinos JF, Barbieri A, Rusinaru D, Szymanski C, et al. Survival implication of left ventricular end-systolic diameter in mitral regurgitation due to flail leaflets: a long-term follow-up multicenter study. J Am Coll Cardiol. (2009) 54:1961–8. doi: 10.1016/j.jacc.2009.06.047
10. Tribouilloy C, Rusinaru D, Maréchaux S. Heart failure with preserved ejection fraction: Looking for new pieces of a complex puzzle. Arch Cardiovasc Dis. (2014) 107:73–6. doi: 10.1016/j.acvd.2014.01.006
11. Mohty D, Orszulak TA, Schaff HV, Avierinos JF, Tajik JA, Enriquez-Sarano M. Very long-term survival and durability of mitral valve repair for mitral valve prolapse. Circulation. (2001) 104(12 Suppl 1):I1–7. doi: 10.1161/circ.104.suppl_1.I-1
12. Badhwar V, Peterson ED, Jacobs JP, He X, Brennan JM, O'Brien SM, et al. Longitudinal outcome of isolated mitral repair in older patients: results from 14,604 procedures performed from 1991 to 2007. Ann Thorac Surg. (2012) 94:1870–9. doi: 10.1016/j.athoracsur.2012.05.105
13. Suri RM, Vanoverschelde JL, Grigioni F, Schaff HV, Tribouilloy C, Avierinos JF, et al. Association between early surgical intervention vs. watchful waiting and outcomes for mitral regurgitation due to flail mitral valve leaflets. JAMA. (2013) 310:609. doi: 10.1001/jama.2013.8643
14. Otto CM, Nishimura RA, Bonow RO, Carabello BA, Erwin JP, Gentile F, et al. ACC/AHA guideline for the management of patients with valvular heart disease. J Am Coll Cardiol. (2021) 77:e25–197. doi: 10.1016/j.jacc.2020.11.035
15. Vahanian A, Beyersdorf F, Praz F, Milojevic M, Baldus S, Bauersachs J, et al. ESC/EACTS guidelines for the management of valvular heart disease. Eur Heart J. (2022) 43:561–632. doi: 10.1093/eurheartj/ehab395
16. Tribouilloy Christophe M, Enriquez-Sarano Maurice, Schaff Hartzell V, Orszulak Thomas A, Bailey Kent R, et al. Impact of preoperative symptoms on survival after surgical correction of organic mitral regurgitation. Circulation. (1999) 99:400–5. doi: 10.1161/01.CIR.99.3.400
17. Clavel MA, Tribouilloy C, Vanoverschelde JL, Pizarro R, Suri RM, Szymanski C, et al. Association of B-type natriuretic peptide with survival in patients with degenerative mitral regurgitation. J Am Coll Cardiol. (2016) 68:1297–307. doi: 10.1016/j.jacc.2016.06.047
18. Le Tourneau T, Messika-Zeitoun D, Russo A, Detaint D, Topilsky Y, Mahoney DW, et al. Impact of left atrial volume on clinical outcome in organic mitral regurgitation. J Am Coll Cardiol. (2010) 56:570–8. doi: 10.1016/j.jacc.2010.02.059
19. Mascle S, Schnell F, Thebault C, Corbineau H, Laurent M, Hamonic S, et al. Predictive value of global longitudinal strain in a surgical population of organic mitral regurgitation. J Am Soc Echocardiogr. (2012) 25:766–72. doi: 10.1016/j.echo.2012.04.009
20. Magne J, Szymanski C, Fournier A, Malaquin D, Avierinos JF, Tribouilloy C. Clinical and prognostic impact of a new left ventricular ejection index in primary mitral regurgitation because of mitral valve prolapse. Circ Cardiovasc Imaging. (2015) 8:3036. doi: 10.1161/CIRCIMAGING.114.003036
21. Tajik AJ, Seward JB, Hagler DJ, Mair DD, Lie JT. Two-dimensional real-time ultrasonic imaging of the heart and great vessels. Technique, image orientation, structure identification, and validation. Mayo Clin Proc. (1978) 53:271–303.
22. Lang RM, Badano LP, Mor-Avi V, Afilalo J, Armstrong A, Ernande L, et al. Recommendations for cardiac chamber quantification by echocardiography in adults: an update from the American society of echocardiography and the european association of cardiovascular imaging. J Am Soc Echocardiogr. (2015) 28:1-39.e14. doi: 10.1016/j.echo.2014.10.003
23. Ling LH, Enriquez-Sarano M, Seward JB, Tajik AJ, Schaff HV, Bailey KR, et al. Clinical outcome of mitral regurgitation due to flail leaflet. N Engl J Med. (1996) 335:1417–23. doi: 10.1056/NEJM199611073351902
24. Grigioni F, Tribouilloy C, Avierinos JF, Barbieri A, Ferlito M, Trojette F, et al. Outcomes in mitral regurgitation due to flail leaflets. JACC Cardiovasc Imaging. (2008) 1:133–41. doi: 10.1016/j.jcmg.2007.12.005
25. Pibarot P, Clavel MA. Management of paradoxical low-flow, low-gradient aortic stenosis. J Am Coll Cardiol. (2015) 65(1):67–71. doi: 10.1016/j.jacc.2014.10.030
26. Dupuis M, Mahjoub H, Clavel M, Côté N, Toubal O, Tastet L, et al. Forward left ventricular ejection fraction: a simple risk marker in patients with primary mitral regurgitation. J Am Heart Assoc. (2017) 3:6309 doi: 10.1161/JAHA.117.006309
27. Tribouilloy C, Rusinaru D, Szymanski C, Mezghani S, Fournier A, Levy F, et al. Predicting left ventricular dysfunction after valve repair for mitral regurgitation due to leaflet prolapse: additive value of left ventricular end-systolic dimension to ejection fraction. Eur J Echocardiogr. (2011) 12:702–10. doi: 10.1093/ejechocard/jer128
28. Ling LH, Enriquez-Sarano M, Seward JB, Orszulak TA, Schaff HV, Bailey KR, et al. Early Surgery in patients with mitral regurgitation due to flail leaflets: a long-term outcome study. Circulation. (1997) 96:1819–25. doi: 10.1161/01.CIR.96.6.1819
29. Montant P, Chenot F, Robert A, Vancraeynest D, Pasquet A, Gerber B, et al. Long-term survival in asymptomatic patients with severe degenerative mitral regurgitation: a propensity score–based comparison between an early surgical strategy and a conservative treatment approach. J Thorac Cardiovasc Surg. (2009) 138:1339–48. doi: 10.1016/j.jtcvs.2009.03.046
30. Kang DH, Park SJ, Sun BJ, Cho EJ, Kim DH, Yun SC, et al. Early surgery vs. conventional treatment for asymptomatic severe mitral regurgitation. J Am Coll Cardiol. (2014) 63:2398–407. doi: 10.1016/j.jacc.2014.02.577
31. Grigioni F, Clavel MA, Vanoverschelde JL, Tribouilloy C, Pizarro R, Huebner M, et al. The MIDA mortality risk score: development and external validation of a prognostic model for early and late death in degenerative mitral regurgitation. Eur Heart J. (2018) 39:1281–91. doi: 10.1093/eurheartj/ehx465
32. Zilberszac R, Heinze G, Binder T, Laufer G, Gabriel H, Rosenhek R. Long-term outcome of active surveillance in severe but asymptomatic primary mitral regurgitation. JACC Cardiovasc Imaging. (2018) 11:1213–21. doi: 10.1016/j.jcmg.2018.05.014
33. Grigioni F, Benfari G, Vanoverschelde JL, Tribouilloy C, Avierinos JF, Bursi F, et al. Long-term implications of atrial fibrillation in patients with degenerative mitral regurgitation. J Am Coll Cardiol. (2019) 73:264–74. doi: 10.1016/j.jacc.2018.10.067
34. Enriquez-Sarano M, Tajik AJ, Schaff HV, Orszulak TA, Bailey KR, Frye RL. Echocardiographic prediction of survival after surgical correction of organic mitral regurgitation. Circulation. (1994) 90:830–7. doi: 10.1161/01.CIR.90.2.830
35. Enriquez-Sarano M, Schaff HV, Orszulak TA, Tajik AJ, Bailey KR, Frye RL. Valve repair improves the outcome of surgery for mitral regurgitation: a multivariate analysis. Circulation. (1995) 91:1022–8. doi: 10.1161/01.CIR.91.4.1022
36. Kim HM, Cho GY, Hwang IC, Choi HM, Park JB, Yoon YE, et al. Myocardial strain in prediction of outcomes after surgery for severe mitral regurgitation. JACC Cardiovasc Imaging. (2018) 11:1235–44. doi: 10.1016/j.jcmg.2018.03.016
37. Edwards NC, Moody WE, Yuan M, Weale P, Neal D, Townend JN, et al. Quantification of left ventricular interstitial fibrosis in asymptomatic chronic primary degenerative mitral regurgitation. Circ Cardiovasc Imaging. (2014) 7:946–53. doi: 10.1161/CIRCIMAGING.114.002397
38. Guglielmo M, Fusini L, Muscogiuri G, Baessato F, Loffreno A, Cavaliere A, et al. T1 mapping and cardiac magnetic resonance feature tracking in mitral valve prolapse. Eur Radiol. (2021) 31:1100–9. doi: 10.1007/s00330-020-07140-w
39. Essayagh B, Antoine C, Benfari G, Messika-Zeitoun D, Michelena H, Le Tourneau T, et al. Prognostic implications of left atrial enlargement in degenerative mitral regurgitation. J Am Coll Cardiol. (2019) 74:858–70. doi: 10.1016/j.jacc.2019.06.032
40. Szymanski C, Magne J, Fournier A, Rusinaru D, Touati G, Tribouilloy C. Usefulness of preoperative atrial fibrillation to predict outcome and left ventricular dysfunction after valve repair for mitral valve prolapse. Am J Cardiol. (2015) 115:1448–53. doi: 10.1016/j.amjcard.2015.02.027
41. Grigioni F, Avierinos JF, Ling LH, Scott CG, Bailey KR, Tajik AJ, et al. Atrial fibrillation complicating the course of degenerative mitral regurgitation: determinants and long-term outcome. J Am Coll Cardiol. (2002) 40:84–92. doi: 10.1016/S0735-1097(02)01922-8
42. Wisenbaugh T, Spann JF, Carabello BA. Differences in myocardial performance and load between patients with similar amounts of chronic aortic versus chronic mitral regurgitation. J Am Coll Cardiol. (1984) 3:916–23. doi: 10.1016/S0735-1097(84)80349-6
Keywords: mitral regurgitation, mitral valve prolapse, left ventricular dysfunction, stroke volume, mitral repair surgery
Citation: Petolat E, Theron A, Resseguier N, Fabre C, Norscini G, Badaoui R, Habib G, Collart F, Zaffran S, Porto A and Avierinos J-F (2023) Prognostic value of forward flow indices in primary mitral regurgitation due to mitral valve prolapse. Front. Cardiovasc. Med. 10:1076708. doi: 10.3389/fcvm.2023.1076708
Received: 21 October 2022; Accepted: 30 January 2023;
Published: 23 February 2023.
Edited by:
Claudia Maria Loardi, Centre Hospitalier Universitaire de Tours, FranceReviewed by:
Michele Di Mauro, Maastricht University Medical Centre, NetherlandsCopyright © 2023 Petolat, Theron, Resseguier, Fabre, Norscini, Badaoui, Habib, Collart, Zaffran, Porto and Avierinos. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jean-François Avierinos,  SmVhbi1mcmFuY29pcy5hdmllcmlub3NAYXAtaG0uZnI=
SmVhbi1mcmFuY29pcy5hdmllcmlub3NAYXAtaG0uZnI=
†These authors have contributed equally to this work and share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.