
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Cardiovasc. Med., 07 February 2023
Sec. Cardiovascular Biologics and Regenerative Medicine
Volume 10 - 2023 | https://doi.org/10.3389/fcvm.2023.1040188
This article is part of the Research TopicInsights in Cardiovascular Biologics and Regenerative Medicine: 2022View all 6 articles
 Luís Henrique Wolff Gowdak1Isolmar Tadeu Schettert1Carlos Eduardo Rochitte1
Luís Henrique Wolff Gowdak1Isolmar Tadeu Schettert1Carlos Eduardo Rochitte1 Leonardo P. de Carvalho1Marcelo Luiz Campos Vieira1Luís Alberto Oliveira Dallan1Sérgio Almeida de Oliveira1Luiz Antonio Machado César1José Oscar Reis Brito2Luiz César Guarita-Souza3
Leonardo P. de Carvalho1Marcelo Luiz Campos Vieira1Luís Alberto Oliveira Dallan1Sérgio Almeida de Oliveira1Luiz Antonio Machado César1José Oscar Reis Brito2Luiz César Guarita-Souza3 Antonio Carlos Campos de Carvalho4,5Jose Eduardo Krieger1* on behalf of the MiHeart/IHD Investigators
Antonio Carlos Campos de Carvalho4,5Jose Eduardo Krieger1* on behalf of the MiHeart/IHD InvestigatorsBackground: Post-procedure residual ischemia is associated with worse prognosis in patients with coronary artery diasease (CAD).
Objective: We evaluated whether autologous bone marrow-derived cells (BMC) contribute to additional reduction in regional stress-induced myocardial ischemia (SIMI) in patients undergoing incomplete coronary artery bypass graft surgery (CABG).
Methods: In a double-blind, randomized, placebo-controlled trial, we enrolled 143 patients (82% men, 58 ± 11 years) with stable CAD and not candidates for complete CABG. They received 100 million BMC (n = 77) or placebo (n = 66) injected into ischemic non-revascularized segments during CABG. The primary outcome was improvement on SIMI quantified as the area at risk in injected segments assessed by cardiovascular magnetic resonance (CMR) 1, 6, and 12 months after CABG.
Results: The reduction in global SIMI after CABG was comparable (p = 0.491) in both groups indicating sustained beneficial effects of the surgical procedure over 12 month period. In contrast, we observed additional improvement in regional SIMI in BMC treated group (p = 0.047). Baseline regional SIMI values were comparable [18.5 (16.2–21.0) vs. 18.5 (16.5–20.7)] and reached the lowest values at 1 month [9.74 (8.25; 11.49) vs. 12.69 (10.84; 14.85)] for BMC and placebo groups, respectively. The ischemia’s improvement from baseline represented a 50% difference in regional SIMI in favor of the BMC transplanted group at 30 days. We found no differences in clinical and LVEF% between groups during the 12 month follow-up period. The 1 month rate of major adverse cerebral and cardiovascular events (MACCE) (p = 0.34) and all-cause mortality (p = 0.08) did not differ between groups 1 month post intervention.
Conclusion: We provided evidence that BMC leads to additional reduction in regional SIMI in chronic ischemic patients when injected in segments not subjected to direct surgical revascularization. This adjuvant therapy deserves further assessment in patients with advanced CAD especially in those with microcirculation dysfunction.
Clinical trial registration: https://clinicaltrials.gov/, identifier NCT01727063
Coronary artery bypass graft surgery (CABG) remains the most performed procedure in cardiovascular surgery (1). The importance of achieving complete revascularization and its impact on the long-term prognosis of patients with multivessel coronary artery disease (CAD) has been addressed in many observational studies and subgroup analyses of randomized clinical trials. In a meta analysis comprising 35 studies and almost 90,000 patients, complete revascularization was associated with lower long-term mortality risk, myocardial infarction and repeat coronary revascularization (2). Based on myocardial perfusion serial testing after PCI for stable angina in the ACME trial (3), normalization of perfusion abnormalities was associated with improved survival compared to patients with persistent ischemia. In the COURAGE trial (4), the extent of residual ischemic myocardium increased the risk of death or myocardial infarction (MI) at 5 years. Nevertheless, the rates of incomplete revascularization varied from 16% in the ARTS I trial (5) to 36% in the MASS II trial (6) or 43% in the SYNTAX CABG trial (7), indicating an yet unmet clinical need.
In myocardial ischemia animal models, stem cell-induced neoangiovasculogenesis and decreased inflammation are associated with increased myocardial perfusion. This response is due to a not fully characterized paracrine effect influencing the development of new vessels and endothelial dysfunction improvements (8–11). Nevertheless, the rate of cell homing is poor and influenced by several factors including the route of delivery and number of cells injected, which has not been thoroughly investigated (12–14), thereby affecting cell-based strategies. Moreover, new vessels presumably induced by cell therapy should remain functionally active, and not provide a transient response associated with an incomplete vessel formation, to favorably impact chronic ischemic cardiomyopathies (15).
Most of the initial studies using autologous bone marrow mononuclear cells (BMC) during CABG focused on cell therapy effects on left ventricular function recovery, which provided modest benefit (16–18). Conversely, few studies addressed the increase in myocardial perfusion and endothelial dysfunction improvements after injection of BMC in patients with severe CAD undergoing CABG. We and others have demonstrated that autologous BMC injection into ischemic, viable myocardium in a small series of patients undergoing incomplete CABG is safe (19) and leads to an increase in myocardial perfusion regardless of number of successfully implanted grafts (20). Thus, in the present MiHeart/IHD trial we hypothesized that intramyocardial injection of autologous BMC, adjuvant to CABG, provides additional regional reduction in SIMI.
MiHeart/IHD study was a multicenter, randomized, double-blind, placebo-controlled trial performed at eight different Brazilian sites (21). Patients were randomly assigned 1:1 via computer-generated block randomization using R software, version 1.9.0 (R Foundation for Statistical Computing),1 with variable block size (blocks of 2, 4, or 6 patients), to receive either autologous BMC or placebo (saline solution) during surgery. Randomization took place after bone marrow aspiration with the patient already in the operating room. All investigators related to patient‘s care or myocardial perfusion study analysis were blind to the allocated groups of randomization. The only unblinded investigator was the Hematologist, whose sole task in the trial was to support the preparation of the injected material.
The study protocol followed the recommendations of the Helsinki Declaration and Good Clinical Practice norms on medical research in humans. The protocol was approved by National Committee of Ethics in Research and local Institutional Review Board from all participating centers. All patients provided a signed, written, informed consent. The trial was sponsored by the Brazilian Ministry of Health (Process #0-1-04-0967-0-0) and registered at clinicaltrials.gov (NCT01727063).
Patients were eligible if the following criteria were met: (1) age between 18 and 80 years; (2) symptoms of angina or angina equivalent due to obstructive CAD documented by invasive angiography; (3) demonstrable myocardial ischemia by two different imaging methods; (4) unsuitability for complete myocardial revascularization according to the Heart Team; patients could be eligible if anticipated that myocardial perfusion might not be adequately restored due to poor distal beds.
Patients were excluded if any of the following were present: (1) LVEF < 25% assessed by echocardiogram; (2) life expectancy below 1 year; (3) cancer in the past 5 years or any blood disorders; (4) severe heart disease of other etiologies; (5) ACS in the past 3 months before surgery, or (6) chronic kidney disease stage five requiring dialysis.
All patients, regardless of the assigned group, underwent bone marrow aspiration. Immediately before surgery, 100 mL of bone marrow aspirate was obtained from the right posterior iliac crest and heparinized. The cell suspension was isolated by density gradient centrifugation on Ficoll-Paque Plus™ (GE Healthcare, Pittsburgh, PA, USA) and washed with heparinized saline. After cell counting using the Türk’s solution, a minimum of 100 million cells were resuspended in 4 mL normal saline, placed in four 1-mL syringes ready for injection. Cell viability assessed by trypan blue exclusion assay needed to be greater than 90% to be deemed adequate for injection. The different BMC sub-populations were assessed in all samples using a standard panel of monoclonal antibodies including VEGFR2 (KDR/Flk-1), CD34, CD117, CD3 antibody, CD4, CD8, CD15, CD19, CD45, CD56, and Stro-1. The percentage of cells expressing CD34 + marker of human hematopoietic stem cells was 1.6 ± 0.8 in BMC-treated patients.
Coronary artery bypass graft surgery was performed during cardiopulmonary bypass and warm blood cardioplegic arrest. Once all bypasses had been completed, 20 aliquots (0.2 mL) of BMC suspension or placebo were injected into non-revascularizable ischemic myocardium supplied by a main coronary artery. The 1 ml syringes used for injection were carefully prepared to prevent the surgical team from identifying the injected solution in both groups. The Cardiovascular Surgeon prospectively decided which segments ought to be injected after careful coronary angiography analysis before randomization. The injections were performed in the cardioplegic heart and special care was taken to prevent backflow after cell delivery by gentlly pressuring the injection site for few seconds.
The primary outcome was improvement in regional stress-induced myocardial ischemia (SIMI) quantified as% of the area at risk in injected segments assessed by cardiovascular magnetic resonance (CMR) 1, 6, and 12 months after CABG. Among the non-invasive stress methods, SIMI by CMR is recognized as an accurate technique to detect inducible myocardial ischemia and infarction with high sensitivity and specificity (22). Moreover, several large studies have shown its prognostic value for predicting CV events (23).
We hypothesized that BMC-treated segments have a higher regional Δ reduction% (Myo ischemia at any given time point – Myo ischemia at baseline) compared to the placebo. Secondary endpoints included global Δ reduction%, improvement in LV function, and a decrease in angina functional class. The primary safety endpoint was major cerebral and cardiovascular adverse events (MACCE) during the first month after surgery.
The CMR exam was performed in 114 patients (BMC group = 59 pts and placebo group = 55 pts) following a standard protocol that included LV short and long-axis cine images acquisition (steady-state free precession – SSFP sequence) and late gadolinium enhancement. First-pass myocardial perfusion was acquired in the LV short-axis plane and obtained 2–3 min after pharmacological stress using dipyridamole at 0.56 mg.kg–1 injected over 4 min. A single dose of 0.05 mM.kg–1 of non-ionic, low-osmolar Gd-based contrast agent was injected into the antecubital vein by power injector at a rate of 5 mL.s–1 followed by 20 mL saline flush. Aminophylline was intravenously injected immediately after the stress perfusion image sequence. The heart was divided into 17 segments for myocardium perfusion assessment (20), which was determined not only in injected ischemic segment but also in non-injected myocardial segments; each segment was scored as presenting normal perfusion (0) mild (1), moderate (2) or severe (3) perfusion defect. The % of global ischemic burden (Myo ischemia%) was calculated as follows:
Where 51 represents the maximal global ischemic score (17 segments × 3 = 51). The % of regional ischemic burden (Myo ischemia%) in injected segments was calculated as follows:
Where n = number of injected segments. All myocardial perfusion studies by CMR were analyzed blindly by a core lab after collecting scans. Investigators examining the images were not aware of which intervention group or time point the images belonged. Moreover, they were also unaware of which myocardial segments had been injected or revascularized.
Data analyses were performed using a commercially available statistical package (IBM Corp., Released 2011. IBM SPSS Statistics for Windows, Version 20.0. Armonk, NY: IBM Corp). The results for continuous variables are presented as mean ± SD, and for categorical variables as percentages. All datasets were tested for normality using the Shapiro–Wilk test. Global and regional SIMI comparisons were analyzed using generalized linear mixed models. Interaction between group and time was included in the analysis and significance was considered for a P ≤ 0.01 (24). Categorical data were compared using Fisher’s exact test. In patients undergoing complete myocardial revascularization, because myocardial segments previously selected as targets were injected with either BMC or placebo, an intention-to-treat analysis was performed.
We assessed for eligibility 161 patients, and 143 were randomized, 77 assigned to BMC and 66 to placebo (Figure 1). The two groups were well matched at baseline (Table 1). Patients were predominantly middle-aged men on optimal medical therapy for symptom control and cardioprotection. A significant proportion of patients had a previous myocardial revascularization procedure, and LV function was preserved or slightly compromised and did not change after CABG (Supplementary Table 1). Incomplete myocardial revascularization was performed in 90 patients (63%), 49 in BMC group (64%) and 41 (62%) in placebo group (P = 0.86). The remaining 53 (37%) patients underwent complete revascularization despite poor distal arterial beds and followed the intention to treat study design, meaning that target myocardial segments were injected as planned with BMC or placebo, regardless the vascular graft placement.
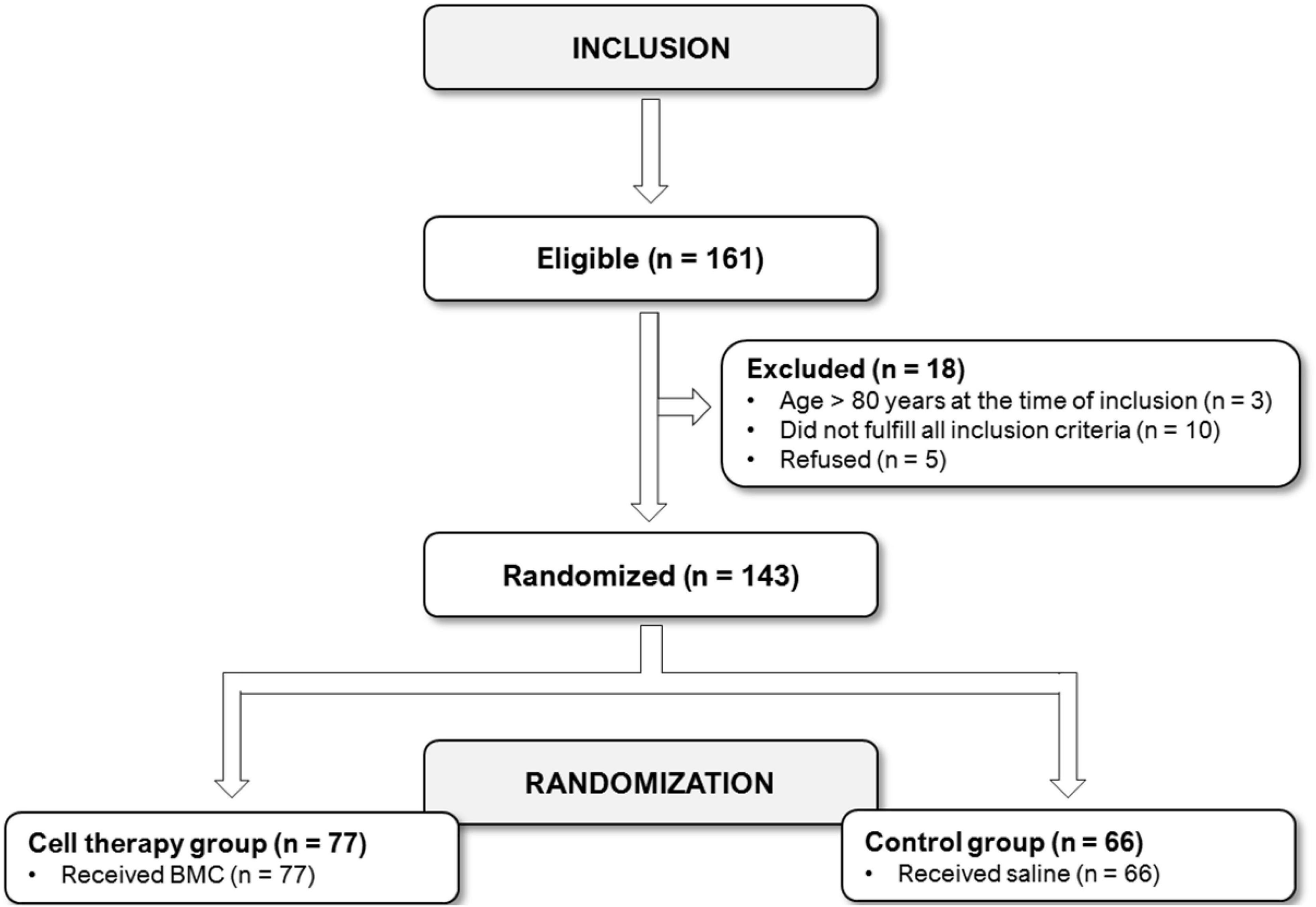
Figure 1. Patient’s flowchart.
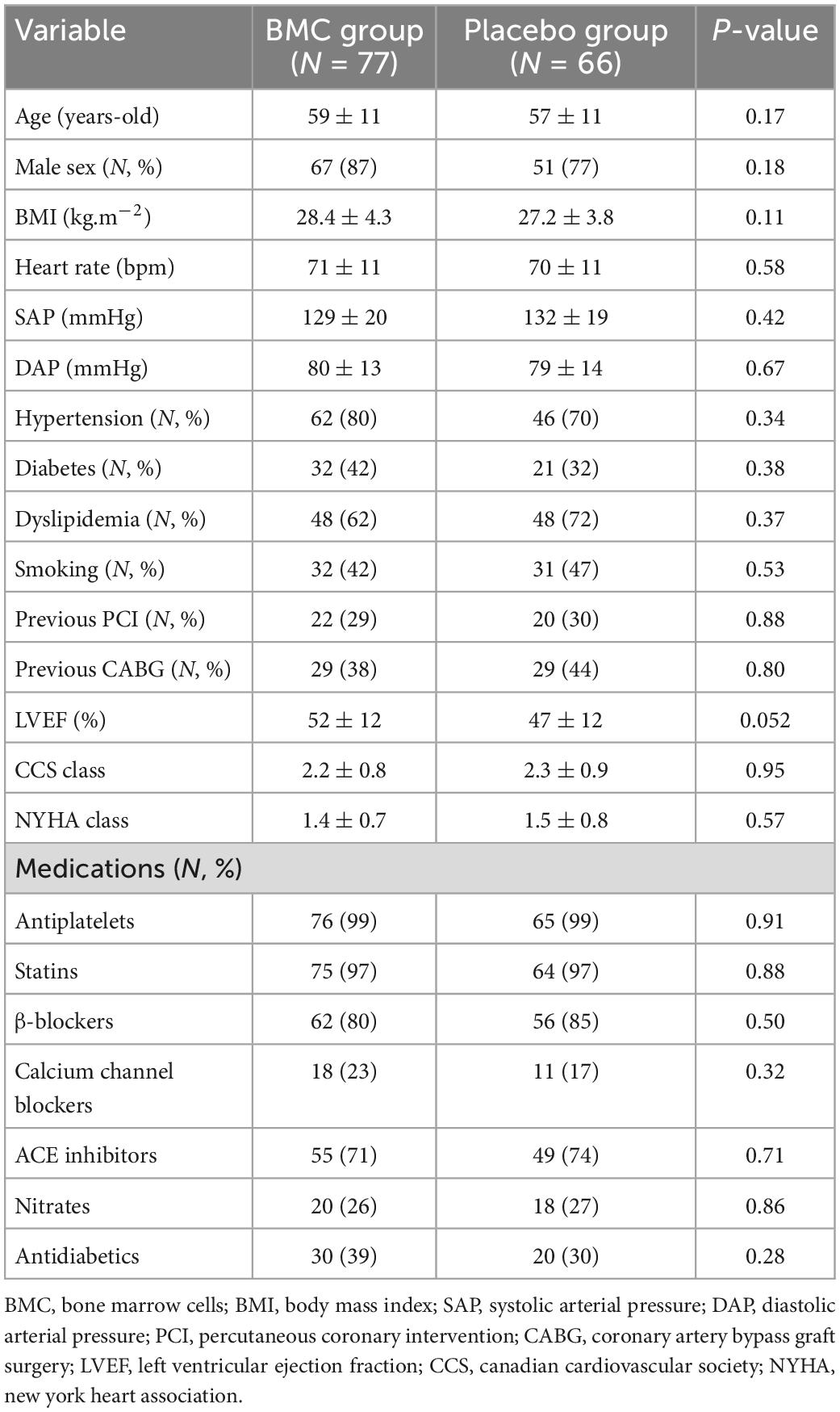
Table 1. Baseline clinical features.
We found no differences in BMCs sub-populations among the placebo or treated group using a standard panel of monoclonal antibodies against VEGFR2 (KDR/Flk-1), CD34, CD117, CD3 antibody, CD4, CD8, CD15, CD19, CD45, CD56, and Stro-1. The percentage of cells expressing CD34 + marker of human hematopoietic stem cells, believed to contribute to neoangiovasculogenesis, averaged 1.6 ± 0.8% in the samples from BMC-treated patients.
The significant reduction in global SIMI after CABG was comparable (p = 0.491) in both groups indicating sustained beneficial effects of the surgical procedure over the 12 month period (Figure 2 and Table 2). In contrast, we observed additional improvement in regional SIMI only in BMC treated group (p = 0.047) (Figure 2 and Table 2). Baseline regional SIMI values were comparable [18.5 (16.2–21.0) vs. 18.5 (16.5–20.7)] and reached the lowest values at 1 month [9.74 (8.25; 11.49) vs. 12.69 (10.84; 14.85)] for BMC and placebo groups, respectively (Table 2). These results show a 50% improvement in reducing ischemia as indicated by the difference in regional SIMI in favor of the BMC transplanted group at 30 days.
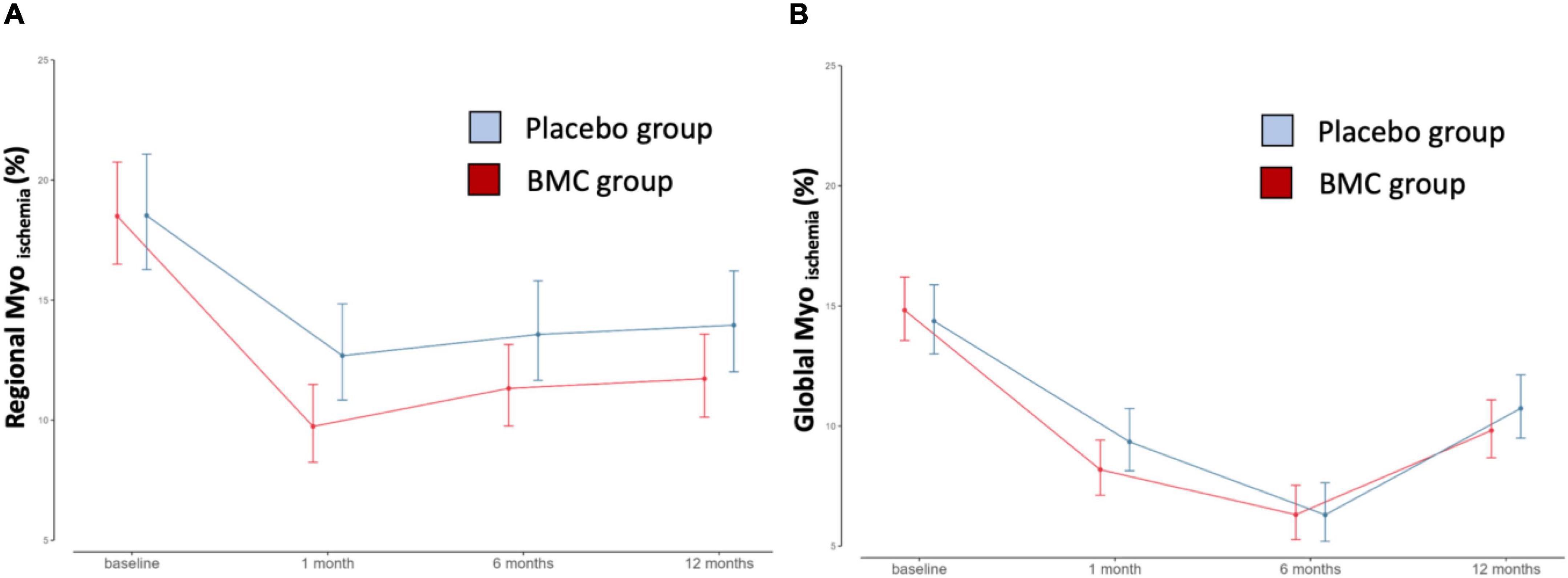
Figure 2. Regional and global stress-induced myocardial ischemia (SIMI). (A) Regional stress-induced ischemia (P-value = 0.047); (B) global stress-induced ischemia in different time points after CABG in patients receiving BMC vs. placebo group (P-value = 0.491).
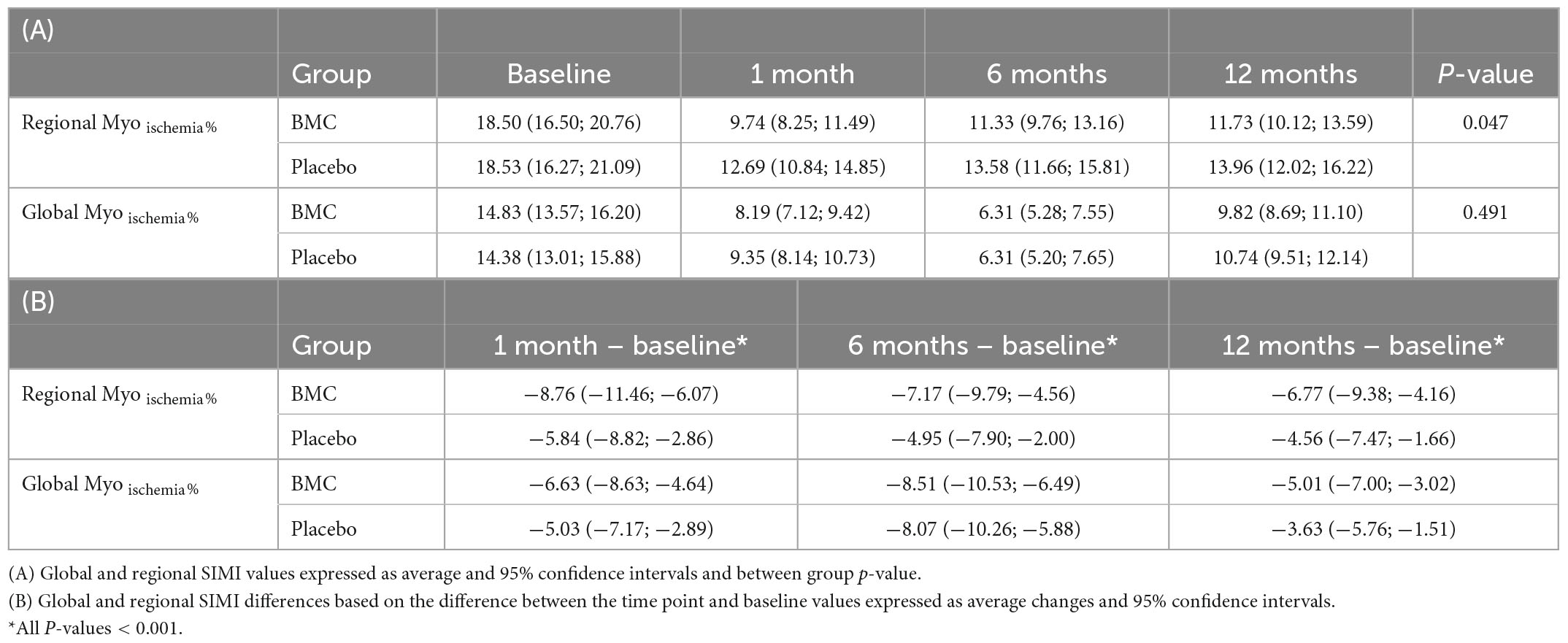
Table 2. Effect of BMC on regional and global stress induced myocardial ischemia (SIMI).
We observed no significant differences between the groups during the 12 month follow-up period nor in clinical or echocardiographic features including angina, chronic coronary symptoms, NYHA classification, or LVEF% (Supplementary Table 1).
The rate of adverse events at 12 months after CABG did not differ between the treated versus the placebo group, especially MACCE (p = 0.34) and all-cause mortality (p = 0.08) that also remained the same at 1 month post-cell transplantation in both groups (Supplementary Table 2).
Bone marrow-derived cells have been administered in humans by different routes for decades and highterto have not raised concerns about safety issues. In contrast, efficacy, measured as improvement of cardiac left ventricle ejection fraction, has shown only modest and non-sustained improvements (16–18). In the present study, we provided evidence that BMCs treatment improves stress-induced myocardial ischemia using CMR, which is considered one of the most reliable non-invasive methods to evaluate microvascular ischemia. These results are consistent with the notion that BMSc stimulate local neoangiovasculogenesis and/or improve coronary microvascular dysfunction. These findings are further supported by data obtained in a subgroup analyses of the present study where we observed that BMCs transplantation improves coronary flow reserve in ischemic non-revascularized myocardium (25).
A major challenge in the area is that neither dosage or injection routes have been standardized as usual for drug development. Pre-clinical evidence indicates that retention associated to BMCs direct injection in the myocardium is low (less than 10%), and very low or negligible when delivered by other routes (13, 14). Other aspect to consider is related to the choice of surrogate endpoints, such as left ventricle ejection fraction improvement, that has been selected early on when it was believed that adult multipotent stem cells could give rise to cardiomyocytes and regeneration. This concept was not confirmed in later studies, but still the majority of the meta analyses focuses on the improvement of cardiac function as measured by left ventricle ejection fraction (16–18). In this context, most of the clinical trials were not designed to assess the more likely effects of cell transplantation on neoangiovasculogenesis or improvements in microcirculation dysfunction consistent with recent evidence pointing to a mechanism of action related to paracrine effects associated with adult multipotent stem cells transplantation (9, 26).
The REPAIR-AMI long-term follow-up at 2 and 5 years, one of the most long-lasting follow-up analysis after BMC injection, demonstrates favorable clinical outcomes, including cardiovascular death and rehospitalization for heart failure (27). The Doppler substudy of the REPAIR-AMI trial suggested cell injection-induced improvement in coronary flow reserve, which was blunted after AMI, whereas in the placebo group there was significant less improvement (28). At 4-month follow-up, CFR in infarct artery slightly improved in placebo group, but was markedly increased by 90% in BMC-treated patients. Likewise in the present study, there was improvement in the minimal microvascular resistance during maximal hyperemia associated with BMC therapy. It is tempting to speculate that that functional improvement in microvascular dysfunction at early stage after BMC transplantation may lead to long-term benefits. We also observed a reduction in SIMI accompanied by improvement in CFR associated with BMC transplantation (25), indicating that the recovery and/or improvement in the microcirculation is a relevant end-point to be targeted.
Microvascular dysfunction accompanies the majority of pathologies of failing organs and tissues. Coronary microvascular dysfunction encompasses several pathogenetic mechanisms involving coronary microcirculation and plays a major role in determining myocardial ischemia and heart failure development (29, 30). BMCs may modulate the microvascular endothelial and metabolic functions, which may contribute to ameliorate myocardial tissue perfusion, resulting in the recovery of the coronary microvascular function, as evidenced by an improvement in coronary flow reserve (31). In this study, we focused on assessing the effects of BMCs on tissue perfusion and its impact on the ischemic burden of the ischemic non-revascularized cardiac segments, especially considering that the study group comprised mild-low risk patients with preserved LVEF. The data demonstrated that BMC injection provided a significant improvement in decreasing regional SIMI compared to placebo over the 12 month period. Moreover, the greatest improvement in the regional ischemia was observed 30 days post-transplatation, representing a 50% improvement compared to the placebo group that benefited only from the CBGE suggesting that more efforts may be directed at increasing cell retention and/or strategies to augment the frequency of the cell delivery.
Interestingly, the results of the COURAGE and BARI-2D trials randomized patients with stable ischemic heart disease after optimal medical therapy (OMT) to a routine revascularization failed to demonstrate MACCE reduction. One may speculate that despite improvement in ischemic burden, large vessels revascularization has no added impact on hard outcomes, which implies the existence of additional factors affecting the outcomes. It may be counterintuitive that routine revascularization for stable ischemic heart disease has no impact on death or MI rates, even though the intervention “fixes” or bypasses the stenosis and relieves ischemia. Nevertheless, it is important to emphasize that a relatively high proportion of participants in the COURAGE and BARI-2D trials remained with moderate to severe residual ischemia after revascularization. These findings indicate a potential benefit of adding strategies targeting neoangiovasculogenesis and/or microvascular dysfunction to complement epicardial vessel revascularization therapy. While the present study did not disclose the underlying patho-physiological mechanisms related to BMCs-induced SIMI reduction, there is a well-established inverse association between coronary flow reserve and atherosclerotic disease progression (32).
Mounting evidence suggests that adult multipotent stem cells may exert paracrine effects by secreting cardio-protective factors (9, 26). These secreted factors may stimulate vascular growth and remodeling, attenuate fibrosis, modulate inflammation, regulate cell differentiation and survival, and recruit resident stem or progenitor cells. Recently, studies have shown that these factors may be clustered into extracellular membrane vesicles, including exosomes and microsomes, which can then transfer proteins, lipids, RNA, and microRNAs to mediate cardioprotection (33, 34). One may speculate that these mechanisms contributed to our findings, but it will be critical to assess the SIMI reduction impact on MACCE in long-term follow-up, which remains to be done.
Altogether, we provided evidence for a BMC-induced improvement in SIMI in ischemic non-revascularized cardiac segments, implying neoangiovasculogenesis and/or restoration of microvasculature function to explain the ischemia reduction. Considering that these results were obtained with a single intramyocardial BMC injection, it will be critical to focus on approaches to increase cell retention and extend the actions of the beneficial effects as an adjunct therapy for ischemic cardiac areas to complement epicardial flow restoration.
The regional analysis was performed by matching the myocardial segmentation map used for perfusion studies with surgeon’s description of which segments had been injected. We acknowledge that some imprecisions may have occurred in pairing the surgeons’ reports with that map. Despite our efforts, there was a decrease in the number of patients that completed the MRI series during the study. This is somewhat expected since claustrophobia and anxiety related symptoms are frequent and known causes of failure in completing postoperative MRI (35). Nevertheless, we provided compelling and robust results despite the losses of procedures in some patients. The adverse events during the 12 month observational period and MACCE at the first month post-cell transplantation remained the same in the experimental and placebo groups. Despite this finding, a major challenge for the groups, scientific societies and regulatory boards is the development of guidelines to standardize these cell procedures as to minimize the possibility of side effects and to enable the comparison of the reported results. Finally, a longer follow-up with an appropriate number of patients would be necessary to determine the combined strategy’s impact on clinically relevant endpoints such as mortality, non-fatal myocardial infarction or rehospitalizations.
We provided evidence that intramyocardial injection of BMC reduces SIMI in ischemic non-revascularized cardiac segments suggesting that this strategy may target the affected microcirculation by activating cardiac neoangiovasculogenesis and/or improving endothelial dysfunction. These findings suggest that adult multipotent stem cells transplantation has a potential as an adjuvant therapy to complement flow restoration of ischemic myocardium.
The original contributions presented in this study are included in this article/Supplementary material, further inquiries can be directed to the corresponding author.
The studies involving human participants were reviewed and approved by the Brazilian National Committee of Ethics in Research and local Institutional Review Boards from all participant centers. The patients/participants provided their written informed consent to participate in this study.
LG, SO, and JK designed and conceptualized the study. LG, MV, LD, SO, LC, JB, and LG-S selected and assisted the patients. LG, IS, and CR collected and analyzed the data. LG, CR, and JK prepared the first draft. LPC and JK prepared the final version. AC, SO, and JK obtained the funds and coordinated the study. All authors contributed to the article and approved the submitted version.
This work was supported by a grant from the Ministry of Health of Brazil (FINEP Process #0-1-04-0967-0-0). The authors had reported that they have no relationships relevant to the contents of this manuscript to disclose.
We are indebted to Bernardo Tura and Eduardo Hill to coordinate randomization and data-management processes and Tiago M dos Santos for expert advice with data analysis, Maria de Lourdes Junqueira for the technical expertise in cell handling and Drs. Jose C. Meneghetti, Jose Soares Junior, and Maria Clementina P. Giorgi for discussions of the SPECT data.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fcvm.2023.1040188/full#supplementary-material
BMC, bone marrow cell; CABG, coronary artery bypass graft surgery; CAD, coronary artery disease; CMR, cardiovascular magnetic resonance; LVEF, left ventricle ejection fraction; OMT, optimal medical therapy; SIMI, stress-induced myocardial ischemia.
1. D’Agostino R, Jacobs J, Badhwar V, Fernandez F, Paone G, Wormuth D, et al. The society of thoracic surgeons adult cardiac surgery database: 2018 update on outcomes and quality. Ann Thor Surg. (2018) 105:15–23. doi: 10.1016/j.athoracsur.2017.10.035
2. Garcia S, Sandoval Y, Roukoz H, Adabag S, Canoniero M, Yannopoulos D, et al. Outcomes after complete versus incomplete revascularization of patients with multivessel coronary artery disease: a meta-analysis of 89,883 patients enrolled in randomized clinical trials and observational studies. J Am Coll Cardiol. (2013) 62:1421–31. doi: 10.1016/j.jacc.2013.05.033
3. Parisi A, Hartigan P, Folland E. Evaluation of exercise thallium scintigraphy versus exercise electrocardiography in predicting survival outcomes and morbid cardiac events in patients with single- and double-vessel disease: findings from the angioplasty compared to medicine (ACME) study. J Am Coll Cardiol. (1997) 30:1256–63. doi: 10.1016/S0735-109700293-3
4. Shaw L, Berman D, Maron D, Mancini G, Hayes S, Hartigan P, et al. Optimal medical therapy with or without percutaneous coronary intervention to reduce ischemic burden: results from the clinical outcomes utilizing revascularization and aggressive drug evaluation (COURAGE) trial nuclear substudy. Circulation. (2008) 117:1283–91. doi: 10.1161/CIRCULATIONAHA.107.743963
5. Van den Brand M, Rensing B, Morel M, Foley D, De Valk V, Breeman A, et al. The effect of completeness of revascularization on event-free survival at one year in the ARTS trial. J Am Coll Cardiol. (2002) 39:559–64. doi: 10.1016/S0735-109701785-5
6. Vieira R, Hueb W, Gersh B, Lima E, Pereira A, Rezende P, et al. Effect of complete revascularization on 10-year survival of patients with stable multivessel coronary artery disease: MASS II trial. Circulation. (2012) 126:158–63. doi: 10.1161/CIRCULATIONAHA.111.084236
7. Head S, Davierwala P, Serruys P, Redwood S, Colombo A, Mack M, et al. Coronary artery bypass grafting vs. percutaneous coronary intervention for patients with three-vessel disease: final five-year follow-up of the SYNTAX trial. Eur Heart J. (2014) 35:2821–30. doi: 10.1093/eurheartj/ehu213
8. Waksman R, Baffour R. Bone marrow and bone marrow derived mononuclear stem cells therapy for the chronically ischemic myocardium. Cardiovasc Radiat Med. (2003) 4:164–8. doi: 10.1016/S1522-186500163-X
9. Shafei A, Ali M, Ghanem H, Shehata A, Abdelgawad A, Handal H, et al. Mechanistic effects of mesenchymal and hematopoietic stem cells: new therapeutic targets in myocardial infarction. J Cell Biochem. (2018) 119:5274–86. doi: 10.1002/jcb.26637
10. Bao L, Meng Q, Li Y, Deng S, Yu Z, Liu Z, et al. C-kit positive cardiac stem cells and bone marrow–derived mesenchymal stem cells synergistically enhance angiogenesis and improve cardiac function after myocardial infarction in a paracrine manner. J Card Fail. (2017) 23:403–15. doi: 10.1016/j.cardfail.2017.03.002
11. Dariolli R, Naghetini MV, Marques E, Takimura C, Jensen L, Kiers B, et al. Allogeneic pASC transplantation in humanized pigs attenuates cardiac remodeling post-myocardial infarction. PLoS One. (2017) 12:e0176412. doi: 10.1371/journal.pone.0176412
12. Nakamuta J, Danoviz M, Marques F, dos Santos L, Becker C, Gonçalves G, et al. Cell therapy attenuates cardiac dysfunction post myocardial infarction: effect of timing, routes of injection and a fibrin scaffold. PLoS One. (2009) 4:e6005. doi: 10.1371/journal.pone.0006005
13. Danoviz M, Nakamuta J, Marques F, dos Santos L, Alvarenga E, dos Santos A, et al. Rat adipose tissue-derived stem cells transplantation attenuates cardiac dysfunction post infarction and biopolymers enhance cell retention. PLoS One. (2010) 5:e12077. doi: 10.1371/journal.pone.0012077
14. Li S, Lai T, Sun Z, Han M, Moriyama E, Wilson B, et al. Tracking cardiac engraftment and distribution of implanted bone marrow cells: comparing intra-aortic, intravenous, and intramyocardial delivery. J Thor Cardiovasc Surg. (2009) 137:1225–1233.e1. doi: 10.1016/j.jtcvs.2008.11.001
15. Pettersson A, Nagy J, Brown L, Sundberg C, Morgan E, Jungles S, et al. Heterogeneity of the angiogenic response induced in different normal adult tissues by vascular permeability factor/vascular endothelial growth factor. Laborat Invest. (2000) 80:99–115. doi: 10.1038/labinvest.3780013
16. Qin S, He C, Xu J, Lai X, Liu S, He W. Meta-analysis of coronary artery bypass graft surgery combined with stem cell transplantation in the treatment of ischemic heart diseases. Coron Artery Dis. (2015) 26:170–5. doi: 10.1097/MCA.0000000000000193
17. Gyöngyösi M, Wojakowski W, Lemarchand P, Lunde K, Tendera M, Bartunek J, et al. Meta-analysis of cell-based CaRdiac stUdiEs (ACCRUE) in patients with acute myocardial infarction based on individual patient data. Circ Res. (2015) 116:1346–60. doi: 10.1161/CIRCRESAHA.116.304346
18. Gyöngyösi M, Haller P, Blake D, Rendon E. Meta-analysis of cell therapy studies in heart failure and acute myocardial infarction. Circ Res. (2018) 123:301–8. doi: 10.1161/CIRCRESAHA.117.311302
19. Gowdak L, Schettert I, Baptista E, Lopes N, Rochitte C, Vieira M, et al. Intramyocardial injection of autologous bone marrow cells as an adjunctive therapy to incomplete myocardial revascularization - safety issues. Clinics. (2008) 63:207–14. doi: 10.1590/S1807-59322008000200009
20. Gowdak L, Schettert I, Rochitte C, Lisboa L, Dallan L, César L, et al. Early increase in myocardial perfusion after stem cell therapy in patients undergoing incomplete coronary artery bypass surgery. J Cardiovasc Trans Res. (2011) 4:106–13. doi: 10.1007/s12265-010-9234-2
21. Tura B, Martino H, Gowdak L, dos Santos R, Dohmann H, Krieger J, et al. Multicenter randomized trial of cell therapy in cardiopathies - MiHeart study. Trials. (2007) 8:1–4. doi: 10.1186/1745-6215-8-2
22. Patel A, Salerno M, Kwong R, Singh A, Heydari B, Kramer C. Stress cardiac magnetic resonance myocardial perfusion imaging: JACC review topic of the week. J Am Coll Cardiol. (2021) 78:1655–68. doi: 10.1016/j.jacc.2021.08.022
23. Pezel T, Hovasse T, Kinnel M, Unterseeh T, Champagne S, Toupin S, et al. Prognostic value of stress cardiovascular magnetic resonance in asymptomatic patients with known coronary artery disease. J Cardiovasc Magnet Res. (2021) 23:1–11. doi: 10.1186/s12968-021-00721-8
25. Assuncao-Jr A, Rochitte C, Kwong R, Wolff Gowdak L, Krieger J, Jerosch-Herold M. Bone marrow cells improve coronary flow reserve in ischemic nonrevascularized myocardium: a MiHeart/IHD quantitative perfusion CMR substudy. JACC Cardiovasc Imaging. (2022) 15:812–24. doi: 10.1016/j.jcmg.2021.12.011
26. Mabotuwana N, Rech L, Lim J, Hardy S, Murtha L, Rainer P, et al. Paracrine factors released by stem cells of mesenchymal origin and their effects in cardiovascular disease?: a systematic review of pre clinical studies. Stem Cell Rev Rep. (2022) 18:2606–28. doi: 10.1007/s12015-022-10429-6
27. Assmus B, Rolf A, Erbs S, Elsässer A, Haberbosch W, Hambrecht R, et al. Clinical outcome 2 years after intracoronary administration of bone marrow–derived progenitor cells in acute myocardial infarction. Circ Heart Fail. (2010) 3:89–96. doi: 10.1161/CIRCHEARTFAILURE.108.843243
28. Erbs S, Linke A, Schächinger V, Assmus B, Thiele H, Diederich K, et al. Restoration of microvascular function in the infarct-related artery by intracoronary transplantation of bone marrow progenitor cells in patients with acute myocardial infarction: the doppler substudy of the reinfusion of enriched progenitor cells and infa. Circulation. (2007) 116:366–74. doi: 10.1161/CIRCULATIONAHA.106.671545
29. Sinha A, Rahman H, Webb A, Shah A, Perera D. Untangling the pathophysiologic link between coronary microvascular dysfunction and heart failure with preserved ejection fraction. Eur Heart J. (2021) 42:4431–41. doi: 10.1093/eurheartj/ehab653
30. De Sousa I, Alaniz M, Teixeira S, Rodrigues MV, Krieger J. Uncovering emergent phenotypes in endothelial cells by clustering of surrogates of cardiovascular risk factors. Sci Rep. (2022) 22:1–16. doi: 10.1038/s41598-022-05404-7
31. Wang X, Bai L, Liu X, Shen W, Tian H, Liu W, et al. Cardiac microvascular functions improved by MSC-derived exosomes attenuate cardiac fibrosis after ischemia–reperfusion via PDGFR-β modulation. Int J Cardiol. (2021) 344:13–24. doi: 10.1016/j.ijcard.2021.09.017
32. Sdringola S, Johnson N, Narula J, Gould K. Serial quantitative assessment of absolute coronary flow and flow reserve with CAD progression to events. JACC Cardiovasc Imaging. (2013) 6:735–8. doi: 10.1016/j.jcmg.2012.07.019
33. de Oliveira N, Neri E, Silva C, Valadão I, Fonseca-Alaniz M, Zogbi C, et al. Multicellular regulation of miR-196a-5p and miR-425-5 from adipose stem cell-derived exosomes and cardiac repair. Clin Sci. (2022) 136:1281–301. doi: 10.1042/CS20220216
34. O’Brien K, Breyne K, Ughetto S, Laurent L, Breakefield X. RNA delivery by extracellular vesicles in mammalian cells and its applications. Nat Rev Mol Cell Biol. (2020) 21:585–606. doi: 10.1038/s41580-020-0251-y
Keywords: myocardial ischemia, coronary artery disease, bone marrow cells, coronary artery bypass graft surgery (CABG), cardiovascular magnetic resonance, stress induced myocardial ischemia
Citation: Gowdak LHW, Schettert IT, Rochitte CE, de Carvalho LP, Vieira MLC, Dallan LAO, de Oliveira SA, César LAM, Brito JOR, Guarita-Souza LC, de Carvalho ACC and Krieger JE (2023) Additional improvement in regional myocardial ischemia after intracardiac injection of bone marrow cells during CABG surgery. Front. Cardiovasc. Med. 10:1040188. doi: 10.3389/fcvm.2023.1040188
Received: 09 September 2022; Accepted: 23 January 2023;
Published: 07 February 2023.
Edited by:
Vincenzo Lionetti, Sant’Anna School of Advanced Studies, ItalyReviewed by:
Howard Leong-Poi, St. Michael’s Hospital, United KingdomCopyright © 2023 Gowdak, Schettert, Rochitte, de Carvalho, Vieira, Dallan, de Oliveira, César, Brito, Guarita-Souza, de Carvalho and Krieger. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jose Eduardo Krieger,  ai5rcmllZ2VyQGhjLmZtLnVzcC5icg==
ai5rcmllZ2VyQGhjLmZtLnVzcC5icg==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.