Erratum: Prognostic impact of physical activity patterns after percutaneous coronary intervention. Protocol for a prospective longitudinal cohort. The PIPAP study
 Nathalia Gonzalez-Jaramillo1,2,3†
Nathalia Gonzalez-Jaramillo1,2,3† Prisca Eser1†
Prisca Eser1† Flurina Casanova1
Flurina Casanova1 Arjola Bano1,2†Oscar H. Franco2†Stephan Windecker1†
Arjola Bano1,2†Oscar H. Franco2†Stephan Windecker1† Lorenz Räber1†
Lorenz Räber1† Matthias Wilhelm1*†
Matthias Wilhelm1*†- 1Department of Cardiology, Inselspital, Bern University Hospital, University of Bern, Bern, Switzerland
- 2Institute of Social and Preventive Medicine, University of Bern, Bern, Switzerland
- 3Graduate School for Health Sciences, University of Bern, Bern, Switzerland
Introduction: Current guidelines recommend wearable activity trackers to detect insufficient physical activity (PA) and help increase PA to prevent or ameliorate cardiovascular disease. However, there is a paucity of data regarding how objectively measured PA trajectories, patterns, and sedentary time, are associated with mortality and recurrent events after percutaneous coronary intervention (PCI) in patients with established coronary artery disease (CAD). Additionally, it remains unclear if early PA and sedentary time after PCI are associated with such outcomes. Therefore, in the present study (ClinicalTrials.gov Identifier: NCT04663373), we aim to establish the associations of objectively measured PA with major adverse cardiac events and mortality at one-year follow-up.
Methods and analysis: In this single-centre observational study, patients with CAD will be prospectively recruited immediately after PCI. All the information from the clinical history, baseline characteristics, and outcomes during follow-up will be obtained from the CARDIOBASE registry. Accelerometer data will be collected for 18 days following hospital discharge and 14 days at one-year follow-up. PA trajectories will be identified by group-based trajectory modeling. Major adverse cardiac events and mortality will be prospectively monitored up to 1 year after PCI. All data will be collected using Research Electronic Data Capture.
Introduction
Coronary artery disease (CAD) is the leading cause of cardiovascular disease (CVD) mortality (1, 2). Lifestyle physical activity (PA) and exercise-based cardiac rehabilitation (CR) successfully reduce the risk of CVD morbidity and mortality and improve the quality of life in patients with CAD (3–5). American and European guidelines (6, 7) thus recommend CR and PA for patients with acute and chronic coronary syndromes, particularly those who undergo percutaneous coronary intervention (PCI) (8).
The use of accelerometers provides objective, feasible, and reliable PA data across its spectrum, including sedentary time, activity counts (divided into time spent in light, moderate and vigorous activity), daily steps, and sleep (9). Some evidence has provided insights into the associations of objectively measured PA and short-term prognosis after hospital admission in patients with CVD. For instance, the number of steps during the three last days of hospital stay after coronary artery bypass grafting is a strong predictor for 30-day cardiac rehospitalization (10). Likewise, in patients hospitalized for decompensated heart failure, physical inactivity within the first week after hospital discharge is associated with 30-day hospital readmission (11).
Current guidelines recommend wearable activity trackers as a tool that may help increase PA (12). However, there is a paucity of data regarding how objectively measured PA patterns and sedentary time are associated with mortality and recurrent events after PCI in patients with CAD. Additionally, it remains unclear if an early increase in PA and a decrease in sedentary time after PCI is associated with such outcomes at 1-year follow-up. Therefore, in the present study (ClinicalTrials.gov Identifier: NCT04663373), we aim first to quantify PA levels, sedentary time, and PA trajectories in participants wearing an accelerometer for 18 days starting on the day of their hospital discharge and for 14 days on 1 year of follow-up. We also aim to evaluate how PA, sedentary time, and PA trajectories early after PCI are associated with major adverse cardiac and cerebrovascular events (MACCE) and 1-year mortality in patients with CAD. Through the extension of the current knowledge and understanding of the role of PA in the prognosis of CAD, these results could enhance cardiovascular health and clinical practice. Our study could emphasize the importance of objectively measured PA and sedentary time as a standard-of-care evaluation in patients with CAD to contribute to clinical decision-making, design tailored interventions and perhaps establish a prognosis.
Objectives
Among patients with CAD who underwent PCI, we aim to establish the association of objectively measured PA and sedentary time with mortality and MACCE at 1-year follow-up.
The aim will be addressed via specific objectives:
(1) Determine the correlation between objectively measured PA, daily step counts, step cadence, inactivity time and sleep time over the 18 days following hospital discharge after PCI and over 14 days at 1-year follow-up.
(2) Compare PA, steps and inactivity between patients subsequently performing CR with patients not performing CR.
(3) Identify PA components and PA trajectories associated with mortality and the first occurrence of MACCE at 12 months.
(4) Identify factors that are associated with different PA trajectories from the immediate period following PCI to 1-year follow-up.
Methods and analysis
Study design and setting
We will conduct an observational, longitudinal monocentric study with a prospective collection of data from the University Hospital of Bern (Inselspital).
Population
Consecutive adult patients with acute or chronic coronary syndrome who underwent PCI.
Selection criteria
Inclusion criteria
(1) Men and women older than 18 years after treatment with PCI for chronic or acute coronary syndrome.
(2) Willingness to participate in the study.
Exclusion criteria
(1) No adequate understanding of how to wear the accelerometer.
(2) Behavioral or cognitive disorders are sufficient to interfere with the patient’s ability to comply with the protocol instructions or follow-up procedures.
(3) Frailty or extensive nursing care needs.
(4) Major surgery, including implantation of cardiac devices, or major neurologic events and cerebrovascular events, within 30 days before screening.
(5) Planned major surgery within the next 20 days after PCI, including staged cardiac surgery.
Sample size calculation
The sample size was calculated based on the available information from the CARDIOBASE registry regarding the proportion of incident cardiovascular events among CAD patients undergoing PCI. The Schoenfeld formula was utilized for survival analysis. Based on the data from the CARDIOBASE registry, we assumed that the proportion of MACCE events within 1 year after the PCI procedure would be 9% (13). We assumed that the physically active patients in the present study would have a 50% reduction in the 1-year risk of incident MACCE, compared to the inactive ones (14). To obtain a power of 80% and a precision of 5%, we estimated a sample size of 726 participants.
Exposures, outcomes, and covariates
Exposures
(a) Each component of the continuum of PA, including sedentary behavior, light, and moderate to vigorous (MVPA) levels of activity, and sleep. Further, the number of daily steps and step cadence.
(b) Trajectories of PA parameters (as stated above) in the short-term (18 days after hospital discharge) and the long-term (hospital discharge to 1-year follow-up).
Outcomes
(a) Main outcomes: (a) MACCE. In line with previous literature on CVD prevention (15), the definition of MACCE will include ischemic endpoints as cardiovascular death, myocardial infarction, stent thrombosis, and stroke; and revascularization endpoints as target lesion revascularization and target vessel revascularization; (b) All-cause mortality.
(b) Secondary outcomes: Individual components of MACCE.
Covariates
(a) Demographic factors: Sex, age, marital status, zip code.
(b) Clinical factors: Personal history of diabetes, dyslipidemia, hypertension, smoking, alcohol intake, body mass index, and CAD presentation at PCI (acute vs. stable), CR attendance.
(c) Procedural-related factors: Number of affected vessels, number of stents, presence of left main disease, and staged angioplasty.
Protocol activities
Consecutive patients who have been hospitalized for percutaneous coronary intervention (PCI) after acute or chronic coronary syndrome (ACS, CCS) will be recruited on the day of discharge or one day before discharge by a team of nurse practitioners who see the patients and inform them about available CR programs. Patients who consider participating will receive a wrist-worn accelerometer, a patient information sheet including an informed consent form and an addressed and prepaid envelope to return the signed consent form and the accelerometer after the study period. They will be asked to wear the accelerometer for 18 days starting from the day of discharge from the hospital. At discharge, the patient will start wearing the accelerometer according to the instructions given by the research team. Patients undergoing staged PCI will receive the accelerometer after the last revascularization. Patients who have their yearly routine checkup at our clinic will receive the accelerometer again after 1 year for another measuring period of 14 days (Figure 1). Patients who perform their yearly check-ups at an external cardiologist will receive the accelerometer for the follow-up measurement by mail. Detailed information concerning the occurrence of clinical outcomes (e.g., date and type of events) will be obtained from the CARDIOBASE database (NCT02241291), a prospective registry collecting all events adjudicated by an independent clinical events committee.
FIGURE 1
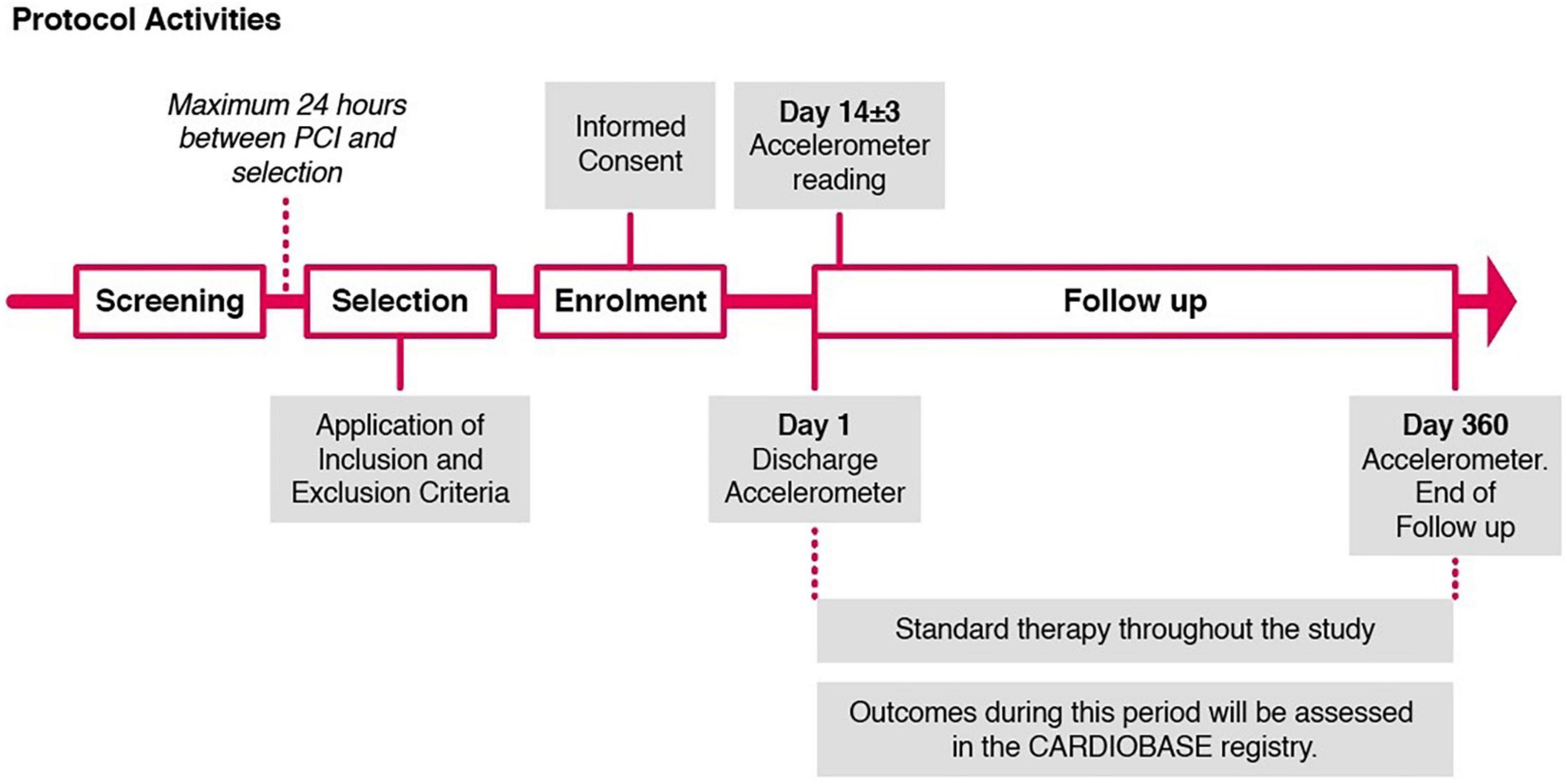
Figure 1. Protocol activities.
At each visit, all the assessments will be recorded on source documentation. A summary of the protocol activities is provided in Figure 1.
Measures
Physical activity monitoring
Tri-axial accelerometers (Axivity AX-3, Axivity Ltd., Newcastle, UK) will be worn continuously on the non-dominant wrist for 18 days. The devices will be programmed with the open-source software AX3 GUI V43 (16) to record tri-axial accelerations of ±8 g at 50 Hz for 18 days starting on the evening of the day of hospital discharge. This period was chosen to achieve at least 14 days of physical activity data also from patients who are transferred to another hospital or home care before returning home. When patients return to the clinic for their follow-up visit after 1 year, they will receive again an accelerometer to be worn for 14 days. Patients completing their yearly follow-up visit with their resident cardiologist will be contacted by mail and if willing to wear the accelerometer again, they will receive it by mail with a prepaid returning envelope.
Data processing
Raw data will be downloaded as cwa files by AX3 GUI V43 and processed by a research-driven open-source R package named GGIR (version 2.4.0) (17, 18). Criteria for data inclusion for analysis is a minimum of 7 days of at least 12 h of daily wear time. The default acceleration metric of the package, which is the Euclidean norm (vector magnitude) minus one (ENMO), will be used for the calculations of the movement component of the raw acceleration data. It describes the conversion of the raw tri-axial acceleration data into an omnidirectional measure of body acceleration (19). The resulting ENMO values are expressed in gravity-based acceleration units (milligravity units [mg]) averaged over 5 s epochs [window sizes = c (5, 900, 3600)].
Physical activity levels
The following activity domains were pre-defined: (20) < 25 mg for inactivity, 25–99 mg for light physical activity [threshold.lig = c (25)] and ≥100 mg for moderate to vigorous physical activity (MVPA) [threshold.mod = c (100)]. Sleep will be identified by the longest daily time window with minimal acceleration and the least positional changes of the wrist (21, 22). Time spent at different PA levels will be accrued in 1 min bouts. During analysis, auto-calibration using local gravity as the reference will be conducted and non-wear time will be determined over a window size of 60 min with a 15-min sliding window [window sizes = c(5, 900, 3600)] (23, 24).
Steps
Whereas activity parameters will be derived directly from GGIR, steps will be determined by a Windowed Peak Detection open-source algorithm (Verisense_step_algorithm, last updated: 14.04.2021) based on the design of Gu et al. (25) and implemented for use in combination with the GGIR R package available on GitHub (26). The input parameters used for the step algorithm were validated in a study with 22 CVD patients during an outdoor exercise session of our CR program (27).
Cadence
Cadences for each minute will be calculated from the meta-data derived by the step algorithm, which includes the number of steps for each 5 s epoch. From this information, we will calculate the mean cadence over the whole 24 h cycle. Moreover, daily minutes with ≥100 steps/min and with 0 steps/min will be extracted (28). We will determine mean cadences for the most active 1, 30, and 60 min, as proposed by Tudor-Locke et al. (29).
Possible sources of bias
Patients cannot see activity or steps on the device, as there is no display on Axivity AX3. However, inherent to the observational design of the study, a selection bias may arise if patients with low PA levels refuse to wear the accelerometer. Information bias would be expected if patients do not wear the accelerometer on days when they move less, as they are told that they will get a personal data summary after the end of their wearing time. On the other hand, patients may make an extra effort to move more due to knowing that their data will be recorded and analyzed (Hawthorne effect).
Data analysis
Statistical analysis plan
All the statistical analyses will be performed in STATA 17IC and R. For all comparisons, a two-sided p-value < 0.05 will be considered statistically significant.
Descriptive statistics will be presented by relative frequencies for qualitative variables or by the mean and standard deviation (SD) or median and interquartile range (IQR), according to the normal distribution of quantitative variables. Unpaired T-tests, Chi-square tests and Mann–Whitney U tests will be used to present statistical differences in baseline characteristics according to the fulfilment of PA recommendations and the identified trajectories. If allowed by the data, we will perform logistic regression models to identify factors associated with short and long-term PA trajectories.
We will use group-based trajectory modeling (30) (GBTM) to identify distinctive clusters of individual PA trajectories and for profiling the characteristics of individuals within the trajectories. GBTM permits the analysis of the effect of time-stable covariates on the probability of group membership and the effect of time-dependent covariates on the trajectory itself (30).
We will test whether mean PA parameters of the whole observation period or trajectories could predict MACCE in addition to traditional risk factors. Furthermore, we will perform receiver operating characteristic (ROC) curves to identify a threshold of the most convenient time to start PA after coronary revascularization. Predictive values of daily steps during the first 2 weeks after hospital discharge will be quantified and tested by the increase in the area under the curve (AUC) of the ROC curve of a model consisting of traditional risk factors (age, sex, cardiovascular risk factors, cardiovascular history, and comorbidities) and time of starting PA after PCI.
We will also use Kaplan–Meier estimates to analyze the association of PA components including sedentary behavior, light, moderate, and high levels of activity, sleep, and the number of steps or step cadence with recurrent cardiovascular events after PCI. After inspection of Schoenfeld residuals to check the proportional hazards assumption, we will perform Cox regression models to compare rates of MACCE among trajectories. Furthermore, the models will be adjusted for age, sex, and clinically relevant variables, including acute vs. chronic CAD, staged PCI, and CR attendance, among others. Time-to-event will be censored at last patient contact for patients without MACCE. Multiple imputations will be performed in case of missing data.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
For all research activities, informed consent will be obtained from participants. Each participant will receive information about the objectives and the procedures of the study. After study completion, all the patients will receive their summary data. Only research team members will have access to data during the study, which will be stored in REDCap, and hosted on secure servers at Inselspital. All data will be anonymized, handled and stored in line with the national data protection laws in Switzerland (31). To protect the identity of participants, they will each be assigned a participant identification number (PIN). The list linking participants’ names to their PIN will be stored separately and securely. Only the principal investigator will have access to that file. The project is approved by the cantonal ethics committee of Bern and is registered in ClinicalTrials (NCT04663373). The CARDIOBASE registry also complies with the Declaration of Helsinki and is approved by the ethics committee.
Author contributions
NG-J, AB, OF, PE, and MW designed the study. FC involved in the patient recruitment. SW, LR, and PE were involved in the data collection. NG-J and PE drafted the manuscript. All authors approved the final version of the manuscript.
Funding
Funding was provided by a grant from the Swiss Heart Foundation (FF19075). Open access funding was provided by the University of Bern.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. GBD 2016 Causes of Death Collaborators. Global, regional, and national age-sex specific mortality for 264 causes of death, 1980-2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet (London, England). (2017) 390:1151–210. doi: 10.1016/s0140-6736(17)32152-9
2. Roth GA, Johnson C, Abajobir A, Abd-Allah F, Abera SF, Abyu G, et al. Global, Regional, and National Burden of cardiovascular diseases for 10 causes, 1990 to 2015. J Am Coll Cardiol. (2017) 70:1–25. doi: 10.1016/j.jacc.2017.04.052
3. Anderson L, Thompson DR, Oldridge N, Zwisler A-D, Rees K, Martin N, et al. Exercise-based cardiac rehabilitation for coronary heart disease. Cochrane Datab Syst Rev. (2016) 2016:CD001800. doi: 10.1002/14651858.CD001800.pub3
4. Moholdt T, Lavie Carl J, Nauman J. Sustained physical activity, not weight loss, associated with improved survival in coronary heart disease. J Am Coll Cardiol. (2018) 71:1094–101. doi: 10.1016/j.jacc.2018.01.011
5. McGregor G, Powell R, Kimani P, Underwood M. Does contemporary exercise-based cardiac rehabilitation improve quality of life for people with coronary artery disease? A systematic review and meta-analysis. BMJ Open. (2020) 10:e036089. doi: 10.1136/bmjopen-2019-036089
6. Collet JP, Thiele H, Barbato E, Barthélémy O, Bauersachs J, Bhatt DL, et al. 2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. Eur Heart J. (2020) 42:1289–367. doi: 10.1093/eurheartj/ehaa575
7. Knuuti J, Wijns W, Saraste A, Capodanno D, Barbato E, Funck-Bretano C, et al. 2019 ESC Guidelines for the diagnosis and management of chronic coronary syndromes. Eur Heart J. (2020) 41:407–77. doi: 10.1093/eurheartj/ehz425
8. Ibanez B, James S, Agewall S, Antunes MJ, Bucciarelli-Ducci C, Bueno H, et al. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: the task force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur Heart J. (2018) 39:119–77. doi: 10.1093/eurheartj/ehx393
9. Smirnova E, Leroux A, Cao Q, Tabacu L, Zipunnikov V, Crainiceanu C, et al. The predictive performance of objective measures of physical activity derived from accelerometry data for 5-year all-cause mortality in older adults: national health and nutritional examination survey 2003-2006. J Gerontol Series A Biol Sci Med Sci. (2020) 75:1779–85. doi: 10.1093/gerona/glz193
10. Takahashi T, Kumamaru M, Jenkins S, Saitoh M, Morisawa T, Matsuda H. In-patient step count predicts re-hospitalization after cardiac surgery. J Cardiol. (2015) 66:286–91. doi: 10.1016/j.jjcc.2015.01.006
11. Waring T, Gross K, Soucier R, ZuWallack R. Measured physical activity and 30-day rehospitalization in heart failure patients. J Cardiopulm Rehabil Prevent. (2017) 37:124–9. doi: 10.1097/hcr.0000000000000204
12. Visseren FLJ, Mach F, Smulders YM, Carballo D, Koskinas KC, Bäck M, et al. 2021 ESC Guidelines on cardiovascular disease prevention in clinical practice: developed by the Task Force for cardiovascular disease prevention in clinical practice with representatives of the European Society of Cardiology and 12 medical societies With the special contribution of the European Association of Preventive Cardiology (EAPC). Eur Heart J. (2021) 42:3227–337. doi: 10.1093/eurheartj/ehab484
13. Gonzalez-Jaramillo N, Marcin T, Matter S, Eser P, Berlin C, Bano A, et al. Clinical outcomes and cardiac rehabilitation in underrepresented groups after percutaneous coronary intervention: an observational study. Eur J Prevent Cardiol. (2022) 29:1093–103. doi: 10.1093/eurjpc/zwab204
14. Gonzalez-Jaramillo N, Wilhelm M, Arango-Rivas AM, Gonzalez-Jaramillo V, Mesa-Vieira C, Minder B, et al. Systematic review of physical activity trajectories and mortality in patients with coronary artery disease. J Am Coll Cardiol. (2022) 79:1690–700. doi: 10.1016/j.jacc.2022.02.036
15. Hwang JK, Lee SH, Song YB, Ahn J, Carriere K, Jang MJ, et al. Glycemic control status after percutaneous coronary intervention and long-term clinical outcomes in patients with type 2 diabetes mellitus. Circ Cardiovasc Intervent. (2017) 10:e004157. doi: 10.1161/circinterventions.116.004157
16. Jackson D. AX3 GUI 2020. (2020). Available online at: https://github.com/digitalinteraction/openmovement/wiki/AX3-GUI (accessed September 7, 2021).
17. Migueles JH, Rowlands AV, Huber F, Sabia S, van Hees VT. GGIR: a research community–driven open source R package for generating physical activity and sleep outcomes from multi-day raw accelerometer data. J Measurement Phys Behav. (2019) 2:188. doi: 10.1123/jmpb.2018-0063
18. van Hees VT. GGIR 2021. (2021). Available online at: https://github.com/cran/GGIR (accessed September 7, 2021).
19. van Hees VT, Gorzelniak L, Dean León EC, Eder M, Pias M, Taherian S, et al. Separating movement and gravity components in an acceleration signal and implications for the assessment of human daily physical activity. PLoS One. (2013) 8:e61691. doi: 10.1371/journal.pone.0061691
20. O’Donnell J, Smith-Byrne K, Velardo C, Conrad N, Salimi-Khorshidi G, Doherty A, et al. Self-reported and objectively measured physical activity in people with and without chronic heart failure: UK Biobank analysis. Open Heart. (2020) 7:e001099. doi: 10.1136/openhrt-2019-001099
21. Nikbakhtian S, Reed AB, Obika BD, Morelli D, Cunningham A, Aral M, et al. Accelerometer-derived sleep onset timing and cardiovascular disease incidence: a UK Biobank cohort study. Eur Heart J Digital Health. (2021) 2:658–66. doi: 10.1093/ehjdh/ztab088
22. van Hees VT, Sabia S, Jones SE, Wood AR, Anderson KN, Kivimäki M, et al. Estimating sleep parameters using an accelerometer without sleep diary. Sci Rep. (2018) 8:12975. doi: 10.1038/s41598-018-31266-z
23. van Hees VT, Fang Z, Langford J, Assah F, Mohammad A, da Silva ICM, et al. Autocalibration of accelerometer data for free-living physical activity assessment using local gravity and temperature: an evaluation on four continents. J Appl Physiol. (2014) 117:738–44. doi: 10.1152/japplphysiol.00421.2014
24. van Hees VT. Accelerometer data processing with GGIR 2021. (2021). Available online at: https://cran.r-project.org/web/packages/GGIR/vignettes/GGIR.html#5_Motivation_and_clarification (accessed August 23, 2021).
25. Gu F, Khoshelham K, Shang J, Yu F, Wei Z. Robust and accurate smartphone-based step counting for indoor localization. IEEE Sensors J. (2017) 17:3453–60. doi: 10.1109/JSEN.2017.2685999
26. Patterson MR. Verisense Step Algorithm. (2021). Available online at: https://github.com/ShimmerEngineering/Verisense-Toolbox/tree/master/Verisense_step_algorithm (accessed April 14, 2021).
27. Femiano R, Werner C, Wilhelm M, Eser P. Validation of open-source step-counting algorithms for wrist-worn tri-axial accelerometers in cardiovascular patients. Gait Posture. (2022) 92:206–11. doi: 10.1016/j.gaitpost.2021.11.035
28. Tudor-Locke C, Schuna JM Jr., Han HO, Aguiar EJ, Green MA, Busa MA, et al. Step-based physical activity metrics and cardiometabolic risk: NHANES 2005-2006. Med Sci Sports Exerc. (2017) 49:283–91. doi: 10.1249/mss.0000000000001100
29. Tudor-Locke C, Han H, Aguiar EJ, Barreira TV, Schuna JM Jr., Kang M, et al. How fast is fast enough? Walking cadence (steps/min) as a practical estimate of intensity in adults: a narrative review. Br J Sports Med. (2018) 52:776. doi: 10.1136/bjsports-2017-097628
30. Nagin DS, Odgers CL. Group-based trajectory modeling in clinical research. Annu Rev Clin Psychol. (2010) 6:109–38. doi: 10.1146/annurev.clinpsy.121208.131413
Keywords: cohort, protocol, prevention, coronary disease - epidemiology, accelerometer
Citation: Gonzalez-Jaramillo N, Eser P, Casanova F, Bano A, Franco OH, Windecker S, Räber L and Wilhelm M (2022) Prognostic impact of physical activity patterns after percutaneous coronary intervention. Protocol for a prospective longitudinal cohort. The PIPAP study. Front. Cardiovasc. Med. 9:976539. doi: 10.3389/fcvm.2022.976539
Received: 23 June 2022; Accepted: 29 August 2022;
Published: 30 September 2022.
Edited by:
Shanthi Mendis, The Geneva Learning Foundation, SwitzerlandReviewed by:
Basuni Radi, National Cardiovascular Center Harapan Kita, IndonesiaAntonino S. Rubino, University of Campania Luigi Vanvitelli, Italy
Copyright © 2022 Gonzalez-Jaramillo, Eser, Casanova, Bano, Franco, Windecker, Räber and Wilhelm. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Matthias Wilhelm, Matthias.Wilhelm@insel.ch
†ORCID: Nathalia Gonzalez-Jaramillo, orcid.org/0000-0003-4975-4439; Prisca Eser, orcid.org/0000-0001-9734-0682; Arjola Bano, orcid.org/0000-0003-0956-7145; Oscar H. Franco, orcid.org/0000-0002-4606-4929; Stephan Windecker, orcid.org/0000-0003-2653-6762; Lorenz Räber, orcid.org/0000-0003-0824-3026; Matthias Wilhelm, orcid.org/0000-0003-4541-3995