
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Cardiovasc. Med. , 12 October 2022
Sec. General Cardiovascular Medicine
Volume 9 - 2022 | https://doi.org/10.3389/fcvm.2022.973043
 Beata Uziȩbło-Życzkowska1*
Beata Uziȩbło-Życzkowska1* Agnieszka Kapłon-Cieślicka2,3
Agnieszka Kapłon-Cieślicka2,3 Monika Gawałko2,3,4,5Monika Budnik2,3
Monika Gawałko2,3,4,5Monika Budnik2,3 Katarzyna Starzyk6Beata Wożakowska-Kapłon6Ludmiła Daniłowicz-Szymanowicz7Damian Kaufmann7Maciej Wójcik2,8
Katarzyna Starzyk6Beata Wożakowska-Kapłon6Ludmiła Daniłowicz-Szymanowicz7Damian Kaufmann7Maciej Wójcik2,8 Robert Błaszczyk8Jarosław Hiczkiewicz9,10Katarzyna Łojewska10
Robert Błaszczyk8Jarosław Hiczkiewicz9,10Katarzyna Łojewska10 Katarzyna Mizia-Stec2,11,12
Katarzyna Mizia-Stec2,11,12 Maciej Wybraniec2,11,12Katarzyna Kosmalska13Marcin Fijałkowski14Anna Szymańska15Aleksandra Gos15Maciej Haberka2,16Michał Kucio16Błazej Michalski2,17Karolina Kupczyńska2,17Anna Tomaszuk-Kazberuk18Katarzyna Wilk-Śledziewska18Renata Wachnicka-Truty19
Maciej Wybraniec2,11,12Katarzyna Kosmalska13Marcin Fijałkowski14Anna Szymańska15Aleksandra Gos15Maciej Haberka2,16Michał Kucio16Błazej Michalski2,17Karolina Kupczyńska2,17Anna Tomaszuk-Kazberuk18Katarzyna Wilk-Śledziewska18Renata Wachnicka-Truty19 Marek Koziński2,19Paweł Burchardt2,20
Marek Koziński2,19Paweł Burchardt2,20 Paweł Krzesiński1,2
Paweł Krzesiński1,2Background: Our aim was to assess the characteristics and to identify predictors of left atrial thrombus (LAT) in patients under age 65 with atrial fibrillation (AF) or atrial flutter (AFl).
Methods: We conducted a subanalysis of a multicenter, prospective, observational study [the LATTEE registry]. Consecutive AF/AFl patients referred for cardioversion or ablation were enrolled.
Results: Of the 3,109 patients included in the study, 1,276 were under age 65 (41%). Compared to non-LAT patients, those with LAT (n = 76) had higher CHA2DS2-VASc score (p < 0.001), more frequently had non-paroxysmal AF/AFl (p < 0.001), heart failure (p < 0.001), history of diabetes mellitus (p = 0.001), transient ischemic attack (p = 0.04), coronary artery disease (p = 0.02), and chronic kidney disease (p < 0.001). The LAT patients were also more often smokers (p = 0.004) and were more frequently treated with vitamin K antagonists (VKAs) (p < 0.001). Transthoracic echocardiography revealed a higher left atrial area (p < 0.001), lower left ventricular ejection fraction (LVEF) (p < 0.001), and lower value of LA appendage emptying volume in LAT than in non-LAT patients (p < 0.001). LVEF (OR 2.95; 95% CI: 1.32–6.59, p = 0.008), non-paroxysmal AF/AFl (OR 7.1; 95% CI: 2.05–24.63, p = 0.002) and treatment with VKAs (OR 4.92; 95% CI: 2.48–9.75, p < 0.001) were identified as independent predictors of LAT in younger patients.
Conclusions: Our study, which focused on younger patients with AF/AFl, indicated substantial clinical and echocardiographic differences between participants with and without LAT. In the AF/AFl patients younger than age 65, the independent predictors of LAT included non-paroxysmal AF/AFl, lower LVEF, and treatment with VKAs.
Atrial fibrillation (AF) is a supraventricular arrhythmia primarily seen in the elderly (1, 2). The risk of thromboembolic complications in AF is closely related to age, as reflected in the strong prognostic power of this factor in the CHA2DS2-VASc scale and by clinical data showing an extremely high risk of stroke in patients over 80 years old (3, 4). A previous study showed that older patients with AF have a high risk of thromboembolic events, regardless of the other components of the CHA2DS2-VASc score (5). However, AF-related thromboembolic events also occur in young and middle-aged patients, even those with low CHA2DS2-VASc scores and without organic heart diseases (6, 7).
Only single reports have been made to describe predictors of left atrial thrombus (LAT) in younger AF patients. No consensus has yet been reached regarding whether thromboembolic risk in these subjects should be estimated based only on approved models for the general AF population (8). The aim of this study was to identify LAT predictors achievable before transesophageal echocardiography (TEE) in AF/AF flutter (AFl) patients under age 65.
The analysis was carried out on a subgroup of patients from the left atrial thrombus on transesophageal echocardiography (LATTEE) registry (ClinicalTrials.gov Identifier: NCT03591627), which was a prospective, cross-sectional, observational, and multicenter study. Data were collected from consecutive AF or AFl patients who were enrolled at 13 cardiology centers. The reasons for admission were catheter ablation or cardioversion and TEE performed directly before the procedure. The methods of the study were previously described in detail (9, 10). Briefly, consecutive hospitalized patients diagnosed with AF/AFl who underwent TEE before direct current cardioversion or catheter ablation were included in the registry. The LATTEE registry was conducted in 13 Polish cardiology centers from November 2018 in the coordinating center and lasted 12 months or longer from the beginning of the study at each participating center (i.e., until the inclusion of at least 200 patients at each participating center; the last patient was enrolled in May 2020). Referral for TEE and the performance of other diagnostic tests depended on the routine practice of a particular center. All patients admitted for AF/AFl ablation were included in the study. Regarding non-emergency electrical cardioversion due to AF/AFL, four cardiology centers performed TEE on all patients, whereas nine centers performed TEE only on those patients suspected of not having received anticoagulant treatment in the previous 3 weeks.
Numerous data, including baseline demographic characteristics, AF type, medical history, concomitant diseases, laboratory and echocardiography test results, and current pharmacotherapy, were collected prospectively from all enrolled patients. Echocardiography examinations (transthoracic echocardiography [TTE] and TEE) were performed by certified echocardiographers. Echocardiographic data included left atrial area (LAa), left ventricular end-diastolic diameter (LVDd), left ventricular ejection fraction (LVEF), and left atrial appendage emptying velocity (LAAV). All echocardiographic measurements were conducted according to the current guidelines (11). The diagnostic criteria for heart failure (HF) with reduced EF (HFrEF), HF with mildly reduced EF (HFmrEF), and HF with preserved EF (HFpEF) were adopted for AF and AFl patients, as recommended in the European Society of Cardiology guidelines (3, 12). In this study, the presence of thrombus in the left atrial appendage (LAA) and spontaneous echocardiographic contrast (SEC) in both LA and LAA was evaluated. An LA thrombus was identified as a circular or irregular echodense mass in LA or LAA that was not part of the endocardium or pectinate muscles (13). The estimated glomerular filtration rate (eGFR) was calculated using the Cockcroft-Gault formula. Chronic kidney disease was defined as diagnosed kidney damage or a glomerular filtration rate (GFR) <60 mL/min/1.73 m2 for 3 months or more, irrespective of cause. The CHA2DS2-VASc score was calculated according to the current guidelines (3).
The study was conducted according to good clinical practice guidelines and the Declaration of Helsinki and was approved by the ethics committee (AKBE/113/2018). Data were entered anonymously into the registry database. The ethics committee waived the requirement to obtain informed consent from the patients.
Statistical analyses were performed with IBM SPSS Statistics 25 (SPSS Inc., Chicago, IL, USA). Data were shown as a median and interquartile range or as the number of patients and percentages, where appropriate. The chi-square test was used to test the relationship between nominal variables and to confirm that the compared groups of people were equal. The Mann-Whitney U test was used to evaluate any statistically significant differences between the two independent groups. The Kruskal-Wallis test was used to assess whether statistically significant differences existed between more than two groups. If those differences were detected, an appropriate post-hoc test was used. The effect size and the effect of the quantitative factor on thrombus occurrence were measured using the Eta-squared values, which indicated which of the quantitative, statistically significant parameters were better at differentiating the compared groups of patients. The logistic regression analysis included the variables with the highest statistically significant differences (the p-value was considered significant when <0.05).
In total, 3,109 AF or AFl patients were included in the study. Detailed data about the entire LATTEE registry group were included in previous manuscripts (9, 10).
As expected, the individual age groups of the AF and AFl patients differed in terms of many parameters. Younger patients were more often male, had the paroxysmal type of arrhythmia, and had significantly fewer comorbidities. These patients were also characterized by better heart function (LVEF and LAAV), higher body mass index (BMI), and better kidney function (measured by eGFR). Detailed data on the differences in individual age groups are shown in Table 1. LAT was detected in 76 (6.0%) patients aged 65 years or younger compared to 172 (9.4%) patients older than age 65 (p < 0.001).
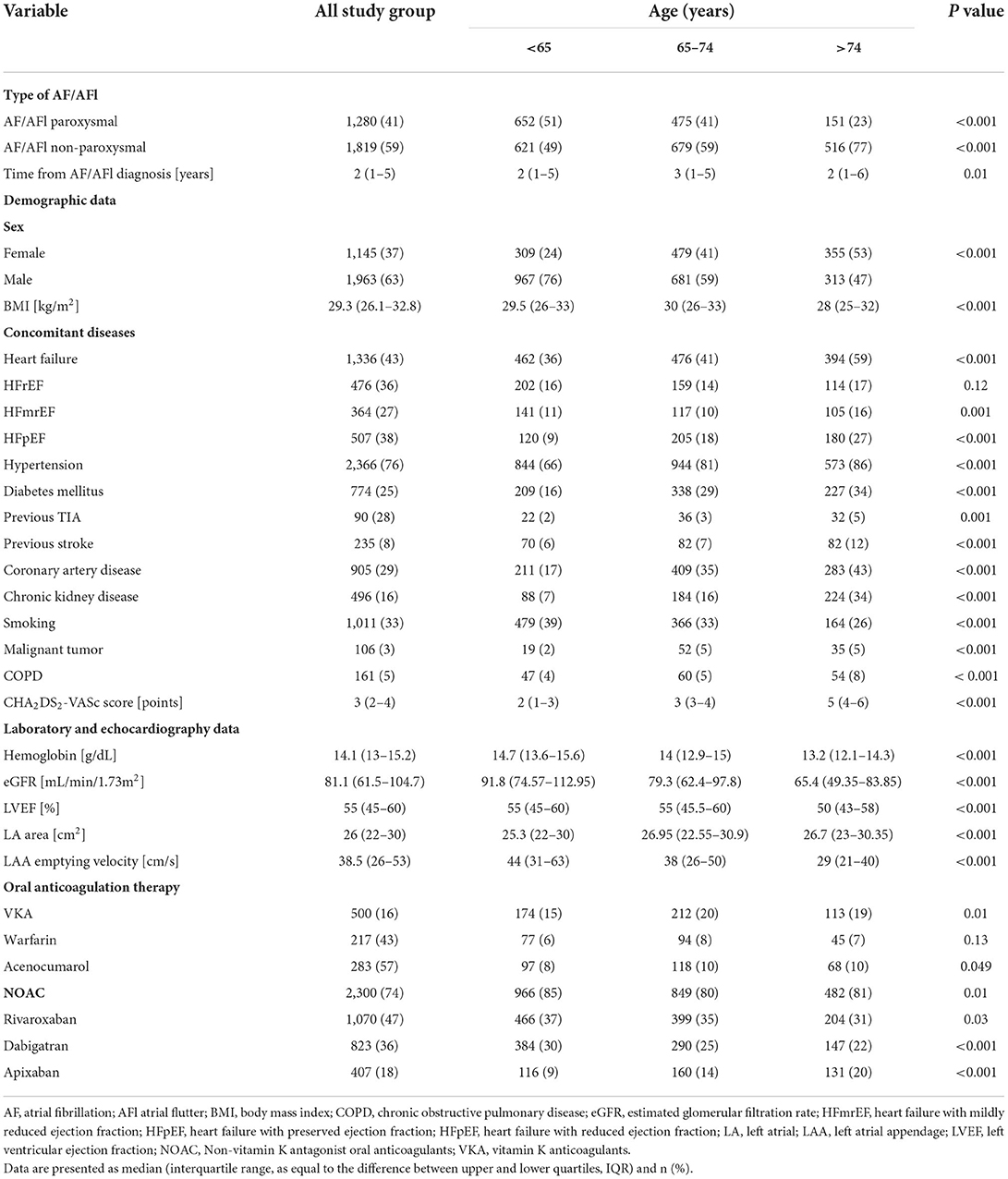
Table 1. Characteristics of the study group according to age category.
A subgroup of 1,276 patients younger than age 65 was subjected to further detailed analysis. The patients aged <65 years with LAT and non-LAT were comparable in terms of general parameters, such as sex (p = 0.68) or BMI (p = 0.51). Non-paroxysmal AF/AFl and comorbidities were significantly more frequent in the LAT subjects. Significant differences were also found in the echocardiographic parameters between the subgroups, as LAT patients had a larger left atrium size (LAa, p < 0.001), lower LVEF (p < 0.001), and lower LAAV (p < 0.001) (Table 2). Supplementary Table S1 shows that effect size measures for quantitative variables differentiated the LAT group from the non-LAT group.
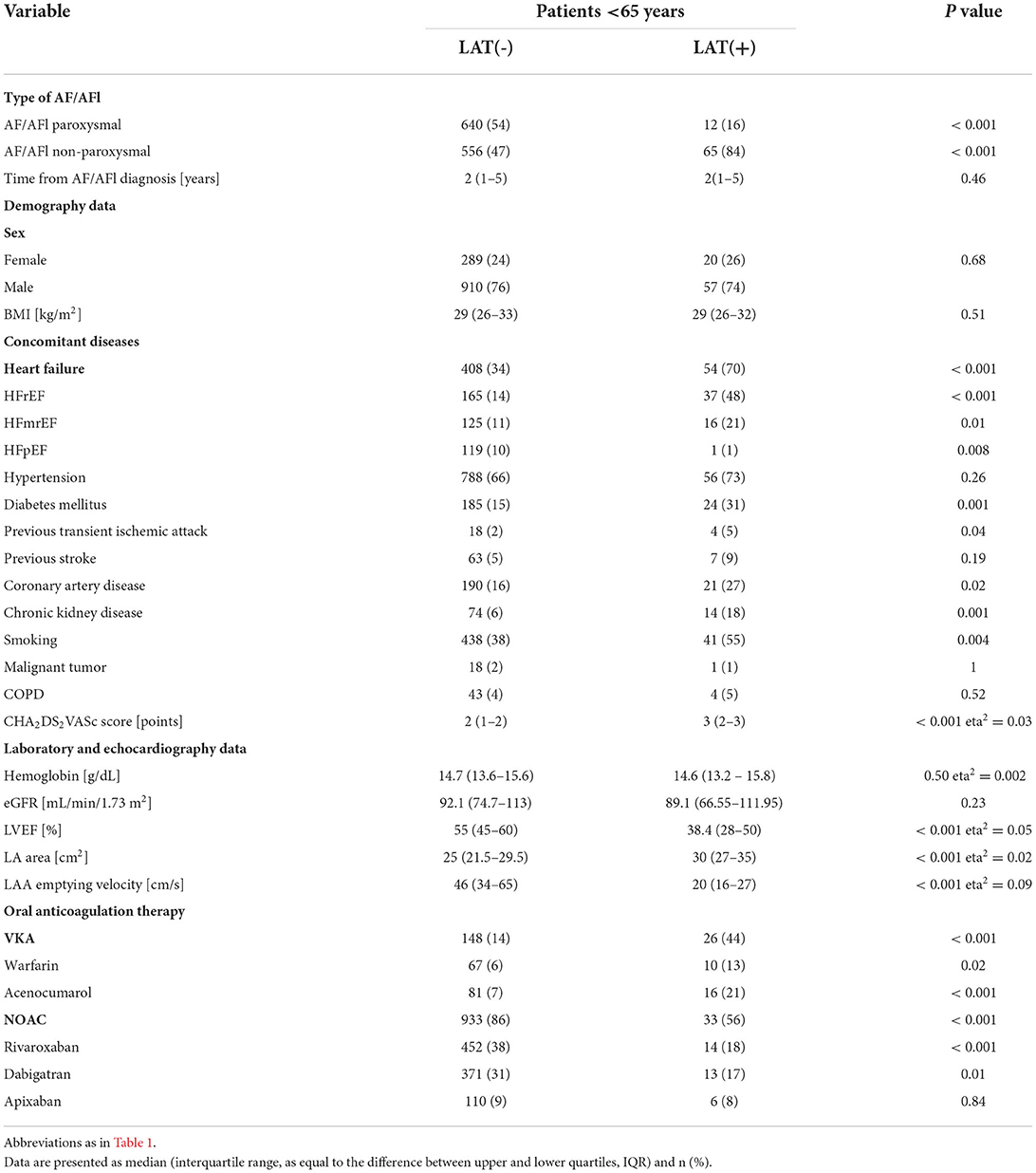
Table 2. Detailed characteristic of patients aged < 65 years according to the presence of a left atrial thrombus.
We next identified the LAT predictors that were achievable without performing the TEE. Our multivariate regression analysis included the following variables (which were statistically significant in univariable logistic regression): AF/AFl-non-paroxysmal, HF, diabetes mellitus (DM), coronary artery disease, smoking, treatment with vitamin K antagonists (VKAs), CHA2DS2-VASc score, LVEF, LAa, and chronic kidney disease (CKD). The independent LAT predictors (odds ratio; 95% confidence interval [CI]) were treatment with VKAs (4.92; 2.48–9.75; p < 0.001), LVEF value (2.95; 1.32–6.59; p = 0.008), and non-paroxysmal AF/AFl (7.1; 2.05–24.63; p = 0.002) (Table 3).
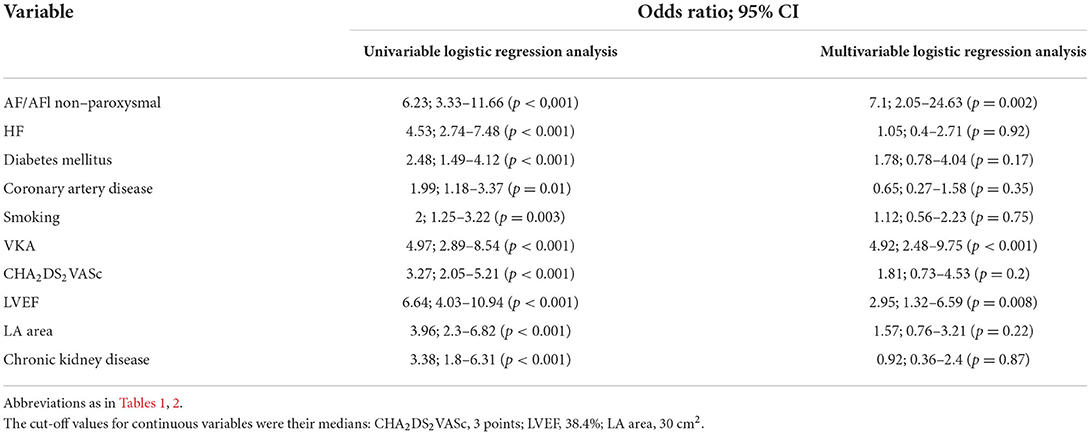
Table 3. Results of univariable and multivariable logistic regression analysis – predictors of left atrial thrombus.
In the group of patients with AF or AFl and younger than age 65, we successfully identified clinical (non-paroxysmal AF/AFl), echocardiographic (LVEF), and therapeutic (treatment with VKAs) LAT predictors. The multivariable logistic regression revealed that other well-established stroke risk factors, such as diabetes mellitus, coronary artery disease, and even the CHA2DS2VASc score, were not independent of these variables.
As expected, the LAT prevalence was less frequent in younger patients with AF and AFl than in older patients with AF/AFl, in agreement with previous studies (8, 14). Subjects under age 65 who were burdened with cardiovascular comorbidities, such as HF, DM, previous transient ischemic attack (TIA), coronary artery disease, and CKD, were more likely to have LAT. Some comorbidities (HF, DM, and TIA) are components of the CHA2DS2-VASc scale; therefore, their role in increasing thromboembolic risk has been proven. Likewise, CKD has recently been reported as a significant risk factor for thromboembolism in AF patients (15–17). Kapłon-Cieślicka et al. (15) demonstrated that a new CHA2DS2VASc-RAF score (where R stands for renal dysfunction and AF for non-paroxysmal AF) was better than the CHADS and CHA2DS2VASc scales used to predict LAT in patients with AF.
In our study, younger patients with AF/AFl smoked more often than older ones from the whole LATTEE group. The univariate analysis identified smoking as a risk factor for thrombus in the left atrium or left atrial appendage, but this result was not confirmed by multivariate analysis. Nevertheless, the association between smoking and the risk of AF occurrence or thromboembolism is inconclusive. Chamberlain et al. (18) showed a more than twofold increased risk of AF attributed to smoking, whereas current smoking was not a significant AF predictor in the Framingham risk score (19). Inao et al. (20) revealed that current smokers had reduced LAAV and more often had dense left atrial spontaneous echo contrast, indicating an impact of smoking on thromboembolic risk in patients with AF. Other authors also found that smoking was associated with a higher thromboembolic risk in AF patients, even after adjustment for well-recognized risk factors used in stroke risk stratification schemes (21). In the present study, among the many factors differentiating subgroups of young patients with AF/AFl with and without LAT, we found only three parameters that were independent risk factors for LAT: non-paroxysmal AFl, LVEF, and treatment with VKAs.
An increased risk of thromboembolism has been previously shown due to non-paroxysmal AF/AFl (15, 22, 23). An extensive systematic review and meta-analysis, including 12 studies containing 99,996 patients with AF, showed an unadjusted risk ratio of 1.355 (p < 0.001) for thromboembolism in non-paroxysmal AF vs. paroxysmal AF. Moreover, non-paroxysmal AF patients had a higher risk of all-cause mortality (1. 217; p < 0.001) (24). Lin et al. (25) retrospectively analyzed a group similar to ours (mean age 52.10 ± 9.64 years) in terms of the clinical, laboratory, and echocardiographic data of 705 patients with non-valvular AF and low risk of stroke (CHA2DS2-VASc score of 0 or 1) and found an independent association between non-paroxysmal AF and LAT or spontaneous echocardiographic contrast in those patients (OR = 3.766, 95% CI: 1.282–11.061, p = 0.016). In that study, approximately 80% of patients with LAT/SEC had non-paroxysmal AF, which is comparable to our result of 84% in the present study.
Many recent studies have confirmed the advantage of non-vitamin K antagonist oral anticoagulants (NOACs) over VKAs in reducing thromboembolic risk (26, 27). These results are reflected in the current guidelines, in which NOACs are explicitly recommended as a choice over VKAs to treat patients with AF. In our previous study, the LAT prevalence in the group of AF patients with IIa class anticoagulation recommendations was higher in the AF patients treated with VKAs than with NOACs (8.4 vs. 3.4%, p = 0.010). Our multivariate logistic regression revealed a threefold higher LAT risk after treatment with VKAs than with NOACs (28). However, our study was observational and we were unable to estimate a time in therapeutic range (TTR) for our participants. We have only the INR result performed at admission for 482 of the 500 patients treated with VKAs, and the mean value was 2.5 ± 1.1. The lower relative efficacy of VKAs in our observational registry may be explained by the lower time in the therapeutic range in real-world patients compared to the time in the therapeutic range achieved in patients included in clinical trials. This could suggest an even greater benefit of NOACs compared to VKAs in the real-world AF population.
Our finding of a negative prognostic value for left ventricular systolic dysfunction is in agreement with other reports confirming decreased LVEF as a powerful and independent predictor of LAT formation in AF patients (24). Melduni et al. (29) reported an LVEF value of ≤ 40% as significantly increasing the probability of LAT. Likewise, in our previous study, which consisted of 768 AF patients (mean age, 63 years), LVEF was also one of the independent LAT predictors (30). Recently, a large Chinese study (36,007 NVAF inpatients from 602 hospitals) identified a lower LVEF as an important predictor of LAT (31). The authors demonstrated that a higher LVEF (per 5%, OR 0.95, 95% CI 0.92–0.97, P = 0.017) indicated a reduced prevalence of LAT.
Our results suggest that the pathogenesis of LAT formation in AF patients is complex and that other components of the CHA2DS2-VASc scale should also be considered. In our study, the independent predictors of LAT in patients younger than 65 with AF/AFl were: non-paroxysmal AF or AFl, LVEF, and treatment with vitamin K antagonists.
The registry-based character of this multicenter study imposes some limitations on our findings. First, the echocardiographic examinations were performed by numerous physicians (at least 1 at each study site). This fact might have had some impact on the obtained results, especially regarding possible measurement bias in assessing the presence of LAT. However, at each center, all examinations were performed by experienced echocardiographers, and if a thrombus was suspected, all images were reviewed by a second experienced echocardiographer trained in TEE. A second limitation is that we evaluated the presence of LAT, assuming it to be a surrogate of a high risk of thromboembolism. Finally, no follow-up was conducted for clinical events; therefore, we could not verify the value of our model in predicting long-term patient prognosis.
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
The studies involving human participants were reviewed and approved by Ethics Committee of Medical University of Warsaw. Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
BU-Ż, AK-C, MG, and PK: conceptualization and methodology. BU-Ż: formal analysis and writing–original draft preparation. BU-Ż and PK: resources. PK, AK-C, and MKo: writing–review and editing. BU-Ż, PK, and AK-C: visualization. PK, AK-C, and BW-K: supervision. All authors contributed to investigation, data collection and manuscript revision, read, and approved the submitted version.
The LATTEE Registry was initiated on the Scientific Platform of the ‘Club 30’ of the Polish Cardiac Society. The authors thank also Elzbieta Wabich (Gdańsk), Jan Budzianowski (Zielona Góra), Konrad Pieszko (Zielona Góra), Sebastian Liedtke (Gdańsk), Marek Szołkiewicz (Gdańsk), Małgorzata Maciorowska and Agnieszka Jurek (Warsaw), for their assistance in data collection.
Author AK-C honoraria for lectures from Bayer, Boehringer Ingelheim, Pfizer, outside the submitted work.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fcvm.2022.973043/full#supplementary-material
AF, atrial fibrillation; AFl, atrial flutter; BMI, body mass index; CKD, chronic kidney disease; DM, diabetes mellitus; eGFR, estimated glomerular filtration rate; ESC, European Society of Cardiology; HF, heart failure; HFmrEF, heart failure with mildly reduced ejection fraction; HFpEF, heart failure with preserved ejection fraction; HFrEF, heart failure with reduced ejection fraction; LAA, left atrial appendage; LAa, left atrial area; LAAV, left atrial appendage emptying velocity; LAT, left atrial thrombus; LVEF, left ventricular ejection fraction; LVDd, left ventricular end-diastolic diameter; NOACs, non-vitamin K antagonist oral anticoagulants; SEC, spontaneous echocardiographic contrast; TEE, transesophageal echocardiography; TIA, transient ischemic attack; TTE, transthoracic echocardiography; VKAs, vitamin-K antagonists.
1. Levy S. Atrial fibrillation, the arrhythmia of the elderly, causes and associated conditions. Anadolu Kardiyol Derg. (2002) 2:55–60.
2. Krijthe BP, Kunst A, Benjamin EJ, Lip GJH, Franco OH, Hofman A, et al. Projections on the number of individuals with atrial fibrillation in the European Union, from 2000 to 2060. Eur Heart J. (2013) 34:2746–51. doi: 10.1093/eurheartj/eht280
3. Hindricks G, Potpara T, Dagres N, Arbelo E, Bax JJ, Blomström-Lundqvist C, et al. ESC Scientific Document Group. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association of Cardio-Thoracic Surgery (EACTS). Eur Heart J. (2021) 42:373–498. doi: 10.1093/eurheartj/ehaa612
4. Mitrousi K, Lip GYH, Apostolakis S. Age as a risk factor for stroke in atrial fibrillation patients: implications in thromboprophylaxis in the era of novel oral anticoagulants. J Atr Fibrillation. (2013) 6:783. doi: 10.4022/jafib.783
5. Kim YG, Choi JI, Boo KY, Kim DY, Hong Y, Kim MS, et al. Impact of age on thromboembolic events in patients with non-valvular atrial fibrillation. Clin Cardiol. (2020) 43:78–85. doi: 10.1002/clc.23293
6. Gourraud JB, Khairy P, Abadir S, Tadros R, Cadrin-Tourigny J, Macle L, et al. Atrial fibrillation in young patients. Expert Rev Cardiovasc Ther. (2018) 16:489–500. doi: 10.1080/14779072.2018.1490644
7. De With RR, Marcos EG, Van Gelder IC, Rienstra M. Atrial fibrillation progression and outcome in patients with young-onset atrial fibrillation. Europace. (2018) 20:1750–7. doi: 10.1093/europace/euy028
8. Gawałko M, Budnik M, Uziebło-Zyczkowska B, Gorczyca I, Krzesiński P, Scisło P, et al. Risk of left atrial appendage thrombus in older patients with atrial fibrillation. Arch Med Sci. (2020) 5. doi: 10.5114/aoms/126028
9. Kapłon-Cieślicka A, Gawałko M, Budnik M, Uziebło-Zyczkowska B, Krzesiński P, Starzyk K, et al. Left atrial thrombus in atrial fibrillation/flutter patients in relation to anticoagulation strategy: registry. J Clin Med. (2022) 11:2705. doi: 10.3390/jcm11102705
10. Kapłon-Cieślicka A, Budnik M., Gawałko M, Wójcik M, Błaszczyk R, Uziebło-Zyczkowska B, et al. The rationale and design of the LATTEE registry - the first multicenter project on the Scientific Platform of the “Club 30” of the Polish Cardiac Society. Kardiol Pol. (2019) 77:1078–80. doi: 10.33963/KP.15011
11. Lang RM, Badano LP, Mor-Avi V, Afilalo J, Armstrong A, Ernande L, et al. Recommendations for cardiac chamber quantification by echocardiography in adults: an update from the american society of echocardiography and the european association of cardiovascular imaging. J Am Soc Echocardiogr. (2015) 28:1–39. doi: 10.1016/j.echo.2014.10.003
12. Ponikowski P, Voors AA, Anker SD, Bueno H, Cleland JGF, Coats AJS, et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur Heart J. (2016) 37:2129–200. doi: 10.1093/eurheartj/ehw128
13. Manning WJ, Weintraub RM, Waksmonski CA, Hearing JM, Rooney PS, Maslow AD, et al. Accuracy of transesophageal echocardiography for identifying left atrial thrombi. A prospective, intraoperative study. Ann Intern Med. (1995) 123:817–22. doi: 10.7326/0003-4819-123-11-199512010-00001
14. Di Minno MND, Ambrosino P, Russo AD, Casella M, Tremoli E, Tondo C. Prevalence of left atrial thrombus in patients with non-valvular atrial fibrillation. A systematic review and meta-analysis of the literature. Thromb Haemost. (2016) 115:663–77. doi: 10.1160/th15-07-0532
15. Kapłon-Cieślicka A, Budnik M, Gawałko M, Peller M, Gorczyca I, Michalska A, et al. Atrial fibrillation type and renal dysfunction as important predictors of left atrial thrombus. Heart. (2019) 105:1310–5. doi: 10.1136/heartjnl-2018-314492
16. Beyer-Westendorf J, Kreutz R, Posch F, Ay C. The CHA2DS2-VASc score strongly correlates with glomerular filtration rate and predicts renal function decline over time in elderly patients with atrial fibrillation and chronic kidney disease. Int J Cardiol. (2018) 253:71–7. doi: 10.1016/j.ijcard.2017.10.110
17. Piccini JP, Stevens SR, Chang Y, Singer DE, Lokhnygina Y, Go AS, et al. Renal dysfunction as a predictor of stroke and systemic embolism in patients with nonvalvular atrial fibrillation: validation of the R(2)CHADS(2) index in the ROCKET AF (Rivaroxaban Once-daily, oral, direct factor Xa inhibition Compared with vitamin K antagonism for prevention of stroke and Embolism Trial in Atrial Fibrillation) and ATRIA (AnTicoagulation and Risk factors In Atrial fibrillation) study cohorts. Circulation. (2013) 127:224–32. doi: 10.1161/CIRCULATIONAHA.112.107128
18. Chamberlain AM, Agarwal SK, Folsom AR, Duval S, Soliman EZ, Ambrose M, et al. Smoking and incidence of atrial fibrillation: results from the Atherosclerosis Risk in Communities (ARIC) study. Heart Rhythm. (2011) 8:1160–6. doi: 10.1016/j.hrthm.2011.03.038
19. Schnabel RB, Sullivan LM, Levy D, Pencina MJ, Massaro JM, D'Agostino RB, et al. Development of a risk score for atrial fibrillation (Framingham Heart Study): a community-based cohort study. Lancet. (2009) 373:739–45. doi: 10.1016/S0140-6736(09)60443-8
20. Inao K, Hirai T, Nakagawa K, Numa S, Ohara K, Fukuda N, et al. Transesophageal echocardiographic thromboembolic risk is associated with smoking status in patients with atrial fibrillation. J Arrhythm. (2017) 33:613–8. doi: 10.1016/j.joa.2017.07.012
21. Albertsen IE, Rasmussen LH, Lane DA, Overvad TF, Skjoth F, Overvad K, et al. The impact of smoking on thromboembolism and mortality in patients with incident atrial fibrillation: insights from the danish diet, cancer, and health study. Chest. (2014) 145:559–66. doi: 10.1378/chest.13-1740
22. Boriani G, Botto GL, Padeletti L, Santini M, Capucci A, Gulizia M, et al. Italian AT−500 Registry Investigators. Improving stroke risk stratification using the CHADS2 and CHA2DS2-VASc risk scores in patients with paroxysmal atrial fibrillation by continuous arrhythmia burden monitoring. Stroke. (2011) 42:1768–70. doi: 10.1161/STROKEAHA.110.609297
23. Ganesan AN, Chew DP, Hartshorne T, Selvanayagam JB, Aylward PE, Sanders P, et al. The impact of atrial fibrillation type on the risk of thromboembolism, mortality, and bleeding: a systematic review and metaanalysis. Eur Heart J. (2016) 37:1591–602. doi: 10.1093/eurheartj/ehw007
24. Echocardiographic predictors of stroke in patients with atrial Fibrillation: a prospective study of 1066 patients from 3 clinical trials. Arch Intern Med. (1998) 158:1316–20. doi: 10.1001/archinte.158.12.1316
25. Lin WD, Xue YM, Liu FZ, Fang XH, Zhan XZ, Liao HT, et al. Left atrial enlargement and non-paroxysmal atrial fibrillation as risk factors for left atrial thrombus/spontaneous Echo contrast in patients with atrial fibrillation and low CHA2DS2-VASc score. J Geriatr Cardiol. (2020) 17:155–9. doi: 10.11909/j.issn.1671-5411.2020.03.001
26. Alqarawi W, Birnie DH, Spence S, Ramirez DF, Redpath CJ, Lemery R, et al. Prevalence of left atrial appendage thrombus detected by transoesophageal echocardiography before catheter ablation of atrial fibrillation in patients anticoagulated with non-vitamin K antagonist oral anticoagulants. Europace. (2019) 21:48–53. doi: 10.1093/europace/euy129
27. Ruff CT, Giugliano RP, Braunwald E, Hoffman EB, Deenadayalu N, Ezekowitz MD, et al. Comparison of the efficacy and safety of new oral anticoagulants with warfarin in patients with atrial fibrillation: a meta-analysis of randomised trials. Lancet. (2014) 383:955–62. doi: 10.1016/S0140-6736(13)62343-0
28. Uziebło-Zyczkowska B, Krzesiński P, Jurek A, Budnik M, Gorczyca I, Kapłon-Cieślicka A, et al. Prevalence and risk factors of left atrial thrombus in patients with atrial fibrillation and lower class (IIa) recommendation to anticoagulants. Cardiovasc Diagn Ther. (2020) 10:717–24. doi: 10.21037/cdt-20-151
29. Melduni RM, Gersh BJ, Wysokinski WE, Ammash NM, Friedman PA, Hodge DO, et al. Real-time pathophysiologic correlates of left atrial appendage thrombus in patients who underwent transesophageal-guided electrical cardioversion for atrial fibrillation. Am J Cardiol. (2018) 121:1540–7. doi: 10.1016/j.amjcard.2018.02.044
30. Uziebło-Zyczkowska B, Krzesiński P, Jurek A, Kapłon-Cieślicka A, Gorczyca I, Budnik M, et al. Left ventricular ejection fraction is associated with the risk of thrombus in the left atrial appendage in patients with atrial fibrillation. Cardiovasc Ther. (2020) 10:717–24. doi: 10.1155/2020/3501749
Keywords: atrial fibrillation, thromboembolic risk factors, young age group, left atrial thrombus, transesophageal echocardiography
Citation: Uziȩbło-Życzkowska B, Kapłon-Cieślicka A, Gawałko M, Budnik M, Starzyk K, Wożakowska-Kapłon B, Daniłowicz-Szymanowicz L, Kaufmann D, Wójcik M, Błaszczyk R, Hiczkiewicz J, Łojewska K, Mizia-Stec K, Wybraniec M, Kosmalska K, Fijałkowski M, Szymańska A, Gos A, Haberka M, Kucio M, Michalski B, Kupczyńska K, Tomaszuk-Kazberuk A, Wilk-Śledziewska K, Wachnicka-Truty R, Koziński M, Burchardt P and Krzesiński P (2022) Risk factors for left atrial thrombus in younger patients (aged < 65 years) with atrial fibrillation or atrial flutter: Data from the multicenter left atrial thrombus on transesophageal echocardiography (LATTEE) registry. Front. Cardiovasc. Med. 9:973043. doi: 10.3389/fcvm.2022.973043
Received: 19 June 2022; Accepted: 08 September 2022;
Published: 12 October 2022.
Edited by:
Gian Marco Rosa, San Martino Hospital (IRCCS), ItalyReviewed by:
Edoardo Bertero, University Hospital Würzburg, GermanyCopyright © 2022 Uziȩbło-Życzkowska, Kapłon-Cieślicka, Gawałko, Budnik, Starzyk, Wożakowska-Kapłon, Daniłowicz-Szymanowicz, Kaufmann, Wójcik, Błaszczyk, Hiczkiewicz, Łojewska, Mizia-Stec, Wybraniec, Kosmalska, Fijałkowski, Szymańska, Gos, Haberka, Kucio, Michalski, Kupczyńska, Tomaszuk-Kazberuk, Wilk-Śledziewska, Wachnicka-Truty, Koziński, Burchardt and Krzesiński. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Beata Uziȩbło-Życzkowska, YnV6aWVibG8tenljemtvd3NrYUB3aW0ubWlsLnBs
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.