 Jing Wang1†
Jing Wang1† Ping Lyu
Ping Lyu
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Cardiovasc. Med. , 05 July 2022
Sec. General Cardiovascular Medicine
Volume 9 - 2022 | https://doi.org/10.3389/fcvm.2022.944424
This article is part of the Research Topic Molecular Mechanism of Vascular Remodelling and Target Organ Damage View all 14 articles
Aim: Systemic inflammation plays an important role in the occurrence and development of acute heart failure. The modified Glasgow Prognostic Score (mGPS) and “lymphocyte C-reactive protein score” (LCS) are used to assess the inflammation levels in cancer patients. The purpose of this study was to assess the prognostic value of these two inflammation-related scoring systems in patients with acute heart failure.
Methods: Two hundred and fifty patients with acute heart failure were enrolled in this study. The mGPS and LCS scores were recorded after admission. All patients were divided into 2 groups: the death group and the survival group according to the 3-month follow-up results. The predictive values of mGPS and LCS were assessed using receiver-operating characteristic (ROC) analyses. Univariate and multivariate logistic analyses were used to evaluate the relationships between variables and endpoint.
Results: The levels of mGPS and LCS in the death group were significantly higher than those in the survival group (P < 0.05). The areas under the ROC curve of the mGPS and LCS for predicting death were 0.695 (95%CI: 0.567~0.823) and 0.736 (95%CI: 0.616~0.856), respectively. Multivariate analysis demonstrated that both LCS, LVEF and serum direct bilirubin were independent predictors of all-cause death, excluding mGPS.
Conclusions: Compared with mGPS, LCS is independently associated with short-term outcomes in patients with acute heart failure. LCS was a clinically promising and feasible prognostic scoring system for patients with acute heart failure.
The incidence of acute heart failure (AHF) has been increasing year by year, and has become the most common reason for unplanned admission of patients over 65 years old (1). Patients with acute heart failure have high hospital costs and long-term mortality. Prognostic assessment has played an increasingly important role in the treatment of these patients. The inseparable association of inflammation and heart failure has long been recognized in many studies (2, 3). Recently, albumin (4, 5), C-reactive protein (6, 7) and lymphocytes (8, 9) have also been reported to predict the prognoses of patients with ADHF, sometimes even better than brain natriuretic peptide in predicting in-hospital death (10).
The modified Glasgow prognostic score (mGPS) and lymphocyte C-reactive protein score (LCS), these two new and readily available markers of inflammation, were initially shown to have independent prognostic value in cancer patients (11–13). Many studies have focused on the correlation between mGPS and prognosis of cardiovascular diseases (14–16), and it has been proved to be an effective and reliable prognostic indicator for patients with acute and chronic heart failure. Recently, Okugawa et al. developed a new inflammatory scoring system based on lymphocyte count and serum CRP level, known as the LCS (12), which has not been demonstrated the effect on prognosis in patients with AHF.
The aim of this study was to evaluate the clinically prognostic efficacy of mGPS and LCS for mortality in patients with AHF and to determine the most clinical practical scoring system for predicting outcomes of patients with AHF.
A total of 250 patients with AHF who were hospitalized in the Department of Cardiology, The Second Affiliated Hospital of Nantong University from October 2019 to October 2020 were eventually included in this study (156 males and 94 females). All patients met the diagnostic criteria for acute heart failure (17).
Patients with rheumatic disease; patients with hematological disease; patients with malignant tumors; patients with chronic or infectious disease; patients with incomplete data and lost to follow-up and pregnant patients were excluded from the study. Patients were also excluded due to chronic or infectious disease or due to taking immunosuppressive drugs for disease control that may influence the status of mGPS and LCS.
Two hundred and fifty-eight patients were initially enrolled in this study, but 250 patients were eventually included according to the exclusion criteria. Of those, 5 patients were excluded because they lacked one of the lymphocyte, CRP and albumin data. For these 5 patients, follow-up was still carried out, and no death occurred in 5 patients. In addition, only 3 patients were lost to follow-up in this study, and these patients were also excluded.
The investigation conformed to the principles outlined in the Declaration of Helsinki. The study was approved by the Ethics Committee of The Affiliated Hospital 2 of Nantong University, Nantong (IRB number: 2019KN104), and informed consent was obtained from all patients.
Demographic data (age, gender, body mass index (BMI), blood pressure, heart rate and treatment) was obtained from medical records. Diagnoses of hypertension and diabetes mellitus, and dyslipidemia were obtained from the patients' medical records or records of patient histories of previous medical therapy. The levels of lymphocyte count, leucocytes, C-reactive protein (CRP) and N-terminal brain natriuretic peptide (NT-proBNP) were measured immediately after admission. All the other measurements such as aspartate transaminase (AST), albumin, total bilirubin, direct bilirubin, total cholesterol, serum creatinine and urea nitrogen were performed on the second day of hospitalization, after fasting. Echocardiographic parameters include left ventricular ejection fraction (LVEF), left atrial diameter (LAD), left ventricular end diastolic diameter (LVEDD), and left ventricular end systolic diameter (LVESD). The glomerular filtration rate was estimated using the chronic kidney disease epidemiology collaboration (CKD-EPI) equation (18). Body mass index (BMI) was calculated as kg/ m2.
All patients were prospectively followed up for 3 months or until death. All-cause mortality was defined as the study end point, and data was obtained from the telephone interview and outpatient visits.
The mGPS, defined based on the combination of serum CRP and albumin, was described as Table 1. Patients with both CRP ≤ 10 mg/L and albumin ≥35 g/L were classified to a score of 0; patients with either CRP >10 mg/L or albumin ≥35 g/L were classified to a score of 1 and patients with both CRP >10 mg/L and albumin <35 g/L were classified to a score of 2 (12).
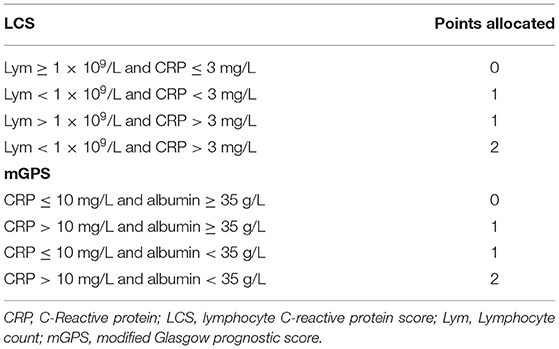
Table 1. Two types of systemic inflammation-based prognostic scores.
The LCS, was established using the circulating lymphocyte count and CRP level as mentioned earlier. Patients with both the lymphocyte count ≥ 1 × 109/L and CRP ≤ 3 mg/L were scored as 0. If only one parameter changes, that is, lymphocyte count <1 × 109/L or CRP >3 mg/L, 1 point was allocated. If both parameters were altered, that is, CRP>3 mg/L and lymphocyte count <1 × 109/L, patients received 2 points (Table 1) (11).
Baseline continuous variables were presented as mean ± standard deviations (SD) or median with the first and fourth quartile (Q1–Q4); depending on the distribution of the data. Categorical data is presented as counts and percentages. For comparisons between the patient groups with different endpoints, the independent samples t-test, the Mann–Whitney U test, and the χ2 test were used. Multivariate analysis using stepwise logistic regression model tested variables that were significant (P < 0.1) in the univariate analysis to determine independent predictors of all-cause mortality. Receiver operating characteristic curve (ROC) was used to evaluate the predictive value of various independent predictors for mortality in patients with acute heart failure. For all tests, a p-value < 0.05 was considered statistically significant. Analyses were performed with the statistical package SPSS 25.0 (SPSS Inc., Chicago, IL).
Two hundred and fifteen patients were included in the study. Demographic, clinical, and laboratory characteristics of patients on admission who reached the endpoint are shown in Table 2. The all-cause mortality rate was 6% in 3 months. The levels of LCS and mGPS in the death group were significantly higher than those in the survival group (P < 0.05). Besides this, the death group had lower LVEF, systolic and diastolic blood pressure, but higher CRP, AST, creatinine, urea nitrogen, NT-proBNP levels, LVESD and incidence of previous myocardial infarction events than the survival group (P < 0.05). No significant differences were observed with respect to gender, age, BMI, white blood cell count, lymphocyte count, hemoglobin, total bilirubin, direct bilirubin, total cholesterol, eGFR and treatment.
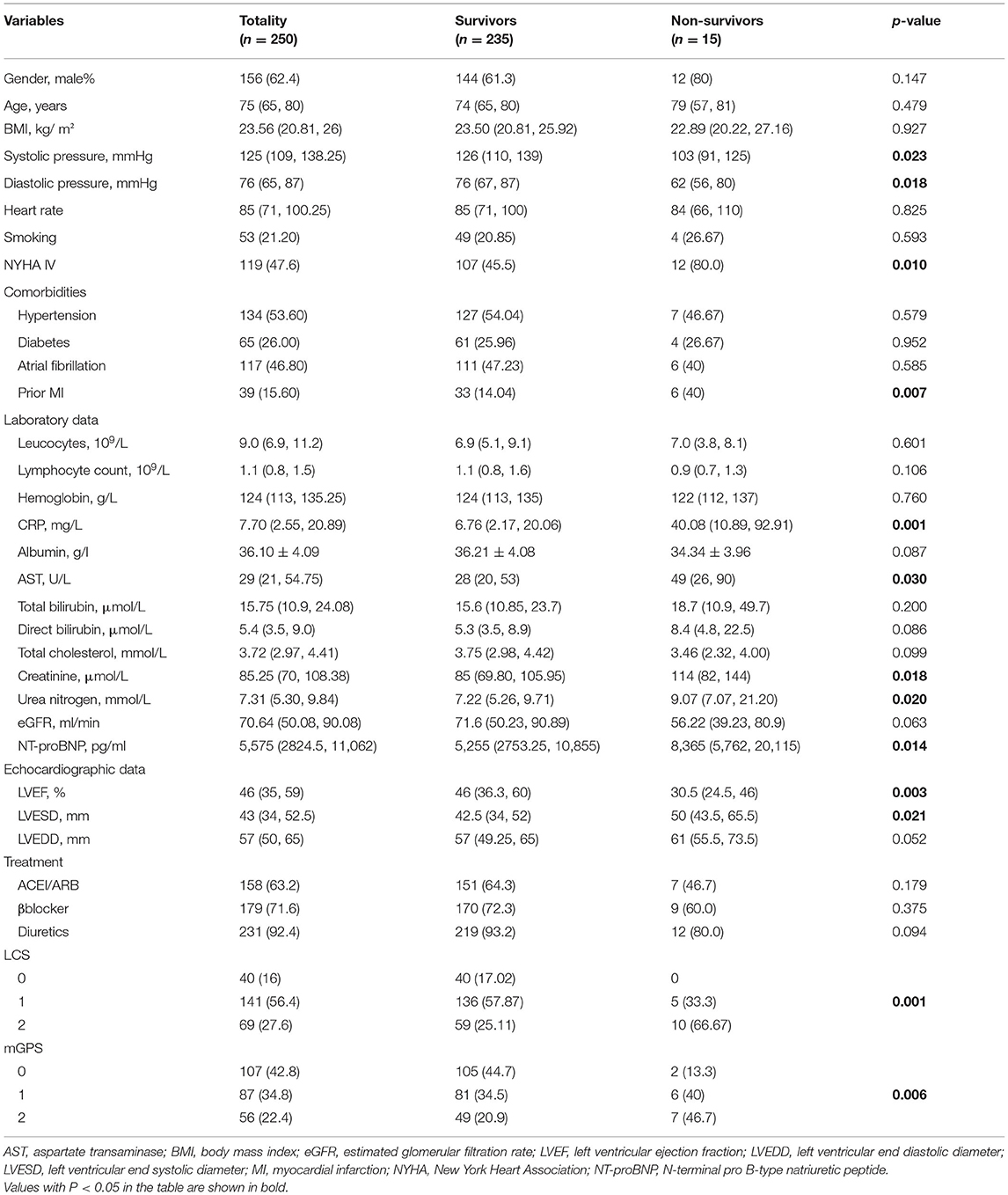
Table 2. Characteristics of patients who reached and did not reach the primary outcome.
On univariate analyses, higher New York Heart Association class, CRP, total bilirubin, direct bilirubin, urea nitrogen, LVESD, LCS and mGPS but lower LVEF, systolic and diastolic blood pressure at admission were significantly associated with outcome (P < 0.05; Table 2). Variables that had a p-value < 0.1 in the univariate analyses were used in a multivariate logistic regression analysis model. After adjusting for other potential confounding factors, multivariate analyses showed that only direct bilirubin (OR: 1.096, 95%CI: 1.019~1.178, p = 0.014), CRP (OR: 1.036, 95%CI: 1.008~1.065, p = 0.011), LVEF (OR: 0.845, 95%CI: 0.750~0.952, p < 0.01) and LCS (OR: 11.694, 95%CI: 1.433~95.409, p = 0.022) at admission were independently associated with the mortality outcomes (Table 3).
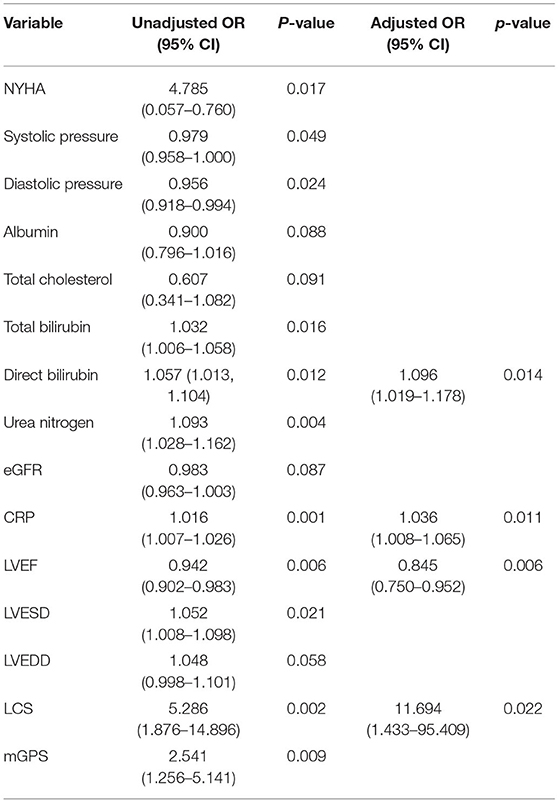
Table 3. Univariate and multivariate analysis of variables associated with prognosis in patients with acute heart failure.
The area under the ROC curve of the mGPS for predicting death was 0.695, with a cut-off level of 0.5 (95%CI: 0.567~0.823), sensitivity of 86.7%, and specificity of 44.7% (p < 0.01; Figure 1). The area under the ROC curve of the LCS for predicting death was 0.736, with a cut-off level of 1.5 (95%CI: 0.616~0.856), sensitivity of 66.7%, and specificity of 74.9% (p < 0.01; Figure 1). Although the AUC of LCS was slightly larger, there was no statistical difference between these two methods (P > 0.05; Figure 1). However, the results of multivariate analyses showed that only LCS was independently associated with the prognosis of patients with acute heart failure.
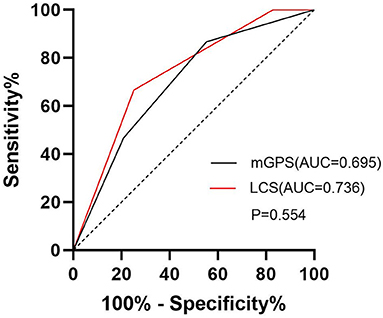
Figure 1. Receiver operating characteristic curves for LCS, and mGPS in the prediction of mortality in patients with acute heart failure. The area under the receiver operating characteristic curve (AUC) for LCS was 0.736, AUC for mGPS was 0.695.
In recent years, more and more studies have elucidated the key role of inflammatory biomarkers in the development of acute heart failure (7, 19–21). Although the role of inflammation in heart failure has been recognized, inflammation scores have not been included in the risk assessment of acute heart failure, and this gap needs to be filled. As mGPS, an inflammatory-based prognostic risk score, has been gradually explored in predicting the prognosis of patients with different types of cancer, cardiovascular physicians are discovering its value in predicting the poor prognosis of patients with acute and chronic heart failure (14–16). In 2019, LCS developed by Okugawa et al. was also proved to be a reliable marker of inflammatory response in patients with gastric cancer (12). To our knowledge, this is the first study to evaluate the predictive value of LCS in patients with acute heart failure and the first study to compare the correlation between mGPS, LCS and prognosis in patients with acute heart failure.
The study showed that the levels of LCS and mGPS in the death group were significantly higher than those in the survival group. Although both mGPS and LCS were associated with 3-month mortality in the univariate analyses (p < 0.05), and there was no significant statistical difference of the AUC between these two scoring systems, only LCS is found to be independently associated with prognosis after adjustment for relevant factors, while mGPS was excluded. In conclusion, LCS has a more promising application in predicting the prognosis of acute heart failure.
The increased level of tumor necrosis factor-α (TNF-α) in the circulation of patients with chronic heart failure since Levine (22) first advocated it in 1990, has been widely explored for decades, and accumulating studies have elucidated the pivotal role of the inflammatory biomarkers in acute and chronic heart failure (7, 19–21). The inflammation-based prognostic score LCS combining CRP and lymphocyte count was originally used to measure systemic inflammatory status and predict prognosis in cancer patients. Similar to heart failure, cancer is also a systemic disease with activated inflammatory response. Previous studies have shown that low lymphocyte counts can help identify patients at higher risk of death in heart transplant patients and in patients with various types of acute or chronic heart failure (9, 23). In addition, high CRP levels on admission and discharge are considered to be closely associated with poor prognosis in patients with acute decompensated heart failure (7, 24). In the LCS scoring system, a lower lymphocyte count and a higher CRP level are assigned a higher score. In fact, several previous studies have hinted in part at the predictive power of LCS in patients with acute heart failure. The elevation of these inflammatory biomarkers in ADHF indicates that ADHF patients are in a significant systemic inflammatory state. In the LCS scoring system, a lower lymphocyte count and a higher CRP level are assigned a higher score, quantifying the inflammatory status and providing a more comprehensive measure of systemic inflammation. This study confirmed the relationship between a more activated inflammatory state and worse prognosis in acute heart failure and reported the successful implementation of the cancer-cohort-derived LCS risk score to a cohort with AHF patients.
In conclusion, this study has shown the clinical utility of the simple and objective inflammation-based score in acute heart failure patients. An activated inflammatory state appears to be characteristic for a more advanced disease. Compared with mGPS, LCS is independently associated with short-term outcomes in patients with acute heart failure. The LCS may help clinicians to identify AHF patients with worse prognosis, for whom more intensive and aggressive treatment may be needed and thus improve their prognosis.
This study was retrospective and all patients enrolled were from the same institution. In the next step, we will include a larger sample size to validate the conclusions of this study and determine whether controlling inflammatory levels in patients with acute heart failure improves patient outcomes. Besides, the follow-up time of this study was only 3 months, so the follow-up time could be extended for further verification.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding authors.
The studies involving human participants were reviewed and approved by the Ethics Committee of The Affiliated Hospital 2 of Nantong University, Nantong (IRB number: 2019KN104). The patients/participants provided their written informed consent to participate in this study.
JW: conceptualization, methodology, investigation, data curation, formal analysis, writing—original draft, and writing—review and editing. LX: conceptualization, methodology, investigation, data curation, and writing—original draft. PL, FZ, and H-LC: investigation and data curation. R-XQ: resources, writing—review and editing, visualization, project administration, and supervision. QZ: resources, formal analysis, writing—original draft, writing—review and editing, visualization, project administration, and supervision. All authors contributed to the article and approved the submitted version.
This work was supported by the Scientific Research Project of Nantong Municipal Health Commission (MA2020004, MB2021010), Project of Nantong Science and Technology Bureau (JCZ21099), and Kangda College of Nanjing Medical University (KD2021KYJJZD012).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
AHF, acute heart failure; mGPS, modified Glasgow prognostic score; LCS, lymphocyte C-reactive protein score; BMI, body mass index; CRP, C-reactive protein; NT-proBNP, N-terminal brain natriuretic peptide; AST, aspartate transaminase; LVEF, left ventricular ejection fraction; LAD, left atrial diameter; LVEDD, left ventricular end diastolic diameter; LVESD, left ventricular end systolic diameter; CKD-EPI, chronic kidney disease epidemiology collaboration; TNF-α, tumor necrosis factor-α.
1. Arrigo M, Jessup M, Mullens W, Reza N, Shah AM, Sliwa K, et al. Acute heart failure. Nat Rev Dis Primers. (2020) 6:16. doi: 10.1038/s41572-020-0151-7
2. Van Linthout S, Tschöpe C. inflammation - cause or consequence of heart failure or both? Curr Heart Fail Rep. (2017) 14:251–65. doi: 10.1007/s11897-017-0337-9
3. Murphy SP, Kakkar R, McCarthy CP, Januzzi JL Jr. Inflammation in heart failure: JACC state-of-the-art review. J Am Coll Cardiol. (2020) 75:1324–40. doi: 10.1016/j.jacc.2020.01.014
4. Mene-Afejuku TO, Moisa EA, Akinlonu A, Dumancas C, Veranyan S, Perez JA, et al. The relevance of serum albumin among elderly patients with acute decompensated heart failure. J Geriatr Cardiol. (2019) 16:522–8. doi: 10.11909/j.issn.1671-5411.2019.07.005
5. Ancion A, Allepaerts S, Robinet S, Oury C, Pierard L, Lancellotti P. Serum albumin level and long-term outcome in acute heart failure. Acta Cardiol. (2019) 74:465–71. doi: 10.1080/00015385.2018.1521557
6. Kalogeropoulos AP, Tang WH, Hsu A, Felker GM, Hernandez AF, Troughton RW, et al. High-sensitivity C-reactive protein in acute heart failure: insights from the ASCEND-HF trial. J Card Fail. (2014) 20:319–26. doi: 10.1016/j.cardfail.2014.02.002
7. Matsumoto H, Kasai T, Sato A, Ishiwata S, Tatsu S, Shitara J, et al. Association between C-reactive protein levels at hospital admission and long-term mortality in patients with acute decompensated heart failure. Heart Vessels. (2019) 34:1961–8. doi: 10.1007/s00380-019-01435-9
8. Milo-Cotter O, Teerlink JR, Metra M, Felker GM, Ponikowski P, Voors AA, et al. Low lymphocyte ratio as a novel prognostic factor in acute heart failure: results from the Pre-RELAX-AHF study. Cardiology. (2010) 117:190–6. doi: 10.1159/000321416
9. Marçula M, de Souza Buto MF, Madaloso BA, Nunes RA, Cuoco MA, de Paula RS, et al. Lymphocyte count and prognosis in patients with heart failure. Int J Cardiol. (2015) 188:60–2. doi: 10.1016/j.ijcard.2015.04.043
10. Arques S, Roux E, Stolidi P, Gelisse R, Ambrosi P. Usefulness of serum albumin and serum total cholesterol in the prediction of hospital death in older patients with severe, acute heart failure. Arch Cardiovasc Dis. (2011) 104:502–8. doi: 10.1016/j.acvd.2011.06.003
11. McMillan D. The systemic inflammation-based Glasgow Prognostic Score: a decade of experience in patients with cancer. Cancer Treat Rev. (2013) 39:534–40. doi: 10.1016/j.ctrv.2012.08.003
12. Okugawa Y, Toiyama Y, Yamamoto A, Shigemori T, Ichikawa T, Yin C, et al. Lymphocyte-to-C-reactive protein ratio and score are clinically feasible nutrition-inflammation markers of outcome in patients with gastric cancer. Clin Nutr. (2020) 39:1209–17. doi: 10.1016/j.clnu.2019.05.009
13. Chen YR, Chen YL, Ouyang SS, Xu HW, Li P, He LJ, et al. Prognostic efficacy of preoperative mGPS, SIS and LCS in patients with gastric cancer. Clin Chim Acta. (2020) 511:81–9. doi: 10.1016/j.cca.2020.09.027
14. Bolat I, Biteker M. Modified Glasgow Prognostic Score is a novel predictor of clinical outcome in heart failure with preserved ejection fraction. Scand Cardiovasc J. (2020) 54:174–8. doi: 10.1080/14017431.2019.1709656
15. Cho A, Arfsten H, Goliasch G, Bartko PE, Wurm R, Strunk G, et al. The inflammation-based modified Glasgow prognostic score is associated with survival in stable heart failure patients. ESC Heart Fail. (2020) 7:654–62. doi: 10.1002/ehf2.12625
16. Namiuchi S, Sugie T, Saji K, Takii T, Suda A, Kato A. The systemic inflammation-based Glasgow Prognostic Score as a prognostic factor in patients with acute heart failure. J Cardiovasc Med. (2015) 16:409–15. doi: 10.2459/JCM.0000000000000184
17. Ponikowski P, Voors AA, Anker SD, Bueno H, Cleland JGF, Coats AJS, et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: the Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur Heart J. (2016) 37:2129–200. doi: 10.1093/eurheartj/ehw128
18. Levey AS, Stevens LA, Schmid CH, Zhang YL, Castro AF III, Feldman HI, et al. A new equation to estimate glomerular filtration rate. Ann Internal Med. (2009) 150:604–12. doi: 10.7326/0003-4819-150-9-200905050-00006
19. Tromp J, Khan MAF, Mentz RJ, O'Connor CM, Metra M, Dittrich HC, et al. Biomarker profiles of acute heart failure patients with a mid-range ejection fraction. JACC Heart Fail. (2017) 5:507–17. doi: 10.1016/j.jchf.2017.04.007
20. Goonewardena S, Stein A, Tsuchida R, Rattan R, Shah D, Hummel S. Monocyte subsets and inflammatory cytokines in acute decompensated heart failure. J Card Fail. (2016) 22:358–65. doi: 10.1016/j.cardfail.2015.12.014
21. Mann D. Incident heart failure in chronic inflammatory diseases: is it time to rethink stage A heart failure? JACC Heart Fail. (2020) 8:499–500. doi: 10.1016/j.jchf.2020.02.006
22. Levine B, Kalman J, Mayer L, Fillit H, Packer M. Elevated circulating levels of tumor necrosis factor in severe chronic heart failure. N Engl J Med. (1990) 323:236–41. doi: 10.1056/NEJM199007263230405
23. Acanfora D, Gheorghiade M, Trojano L, Furgi G, Pasini E, Picone C, et al. Relative lymphocyte count: a prognostic indicator of mortality in elderly patients with congestive heart failure. Am Heart J. (2001) 142:167–73. doi: 10.1067/mhj.2001.115792
Keywords: acute heart failure, inflammation, LCS, mGPS, prognosis
Citation: Wang J, Xie L, Lyu P, Zhou F, Cai H-L, Qi R-X and Zhang Q (2022) Short-Term Prognostic Efficacy of mGPS and LCS in Patients With Acute Heart Failure. Front. Cardiovasc. Med. 9:944424. doi: 10.3389/fcvm.2022.944424
Received: 15 May 2022; Accepted: 15 June 2022;
Published: 05 July 2022.
Edited by:
Jia Qi, Shanghai Jiao Tong University, ChinaReviewed by:
Zhang Jinlong, Yancheng First Peoples' Hospital, ChinaCopyright © 2022 Wang, Xie, Lyu, Zhou, Cai, Qi and Zhang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Qing Zhang, enpoYW5ncWluZzMyQHNpbmEuY24=; Rong-Xing Qi, bnRkb2NxaXJvbmd4aW5nQHNpbmEuY29t
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.