 Mengdi Ren
Mengdi Ren Yuyan Ma1†
Yuyan Ma1† Yuye Ning
Yuye Ning Hui Liu
Hui Liu Yu Yao
Yu Yao Fengwei Guo
Fengwei Guo
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Cardiovasc. Med. , 01 July 2022
Sec. Heart Failure and Transplantation
Volume 9 - 2022 | https://doi.org/10.3389/fcvm.2022.932044
This article is part of the Research Topic Novel Phenotyping and Risk Stratification Strategies for Heart Failure View all 16 articles
Background: Reports of the clinical outcomes associated with the co-occurrence of atrial cardiomyopathy (ACM) and lung cancer (LC) are limited.
Objectives: This study aims to investigate the influence of ACM on the prognosis of LC patients and related clinical determinants.
Methods: Newly diagnosed LC patients from January 1st, 2015, to December 31st, 2020, were retrospectively enrolled at the First Affiliated Hospital of Xi’an Jiaotong University. The demographics and overall survival (OS) of the patients with or without ACM were compared. The survival rate was analyzed using the Kaplan–Meier method and multivariate Cox regression analysis. Binary logistic regression analysis was used to determine the risk factors for ACM.
Results: A total of 306 patients (65.04 ± 10.30 years of age, 72.88% male) were analyzed. The prevalence of ACM in the non-small cell lung cancer (241, 78.76%) and small cell lung cancer (65, 21.24%) population was not statistically different. Overall, 53 (17.32%) LC patients had coexisting ACM. ACM patients were older (69 vs. 64, p = 0.0013) and had higher D-dimer levels (1.0 vs. 0.6, p = 0.001), lower serum calcium levels (2.23 vs. 2.31, p = 0.001), lower left ventricular ejection fraction (LVEF) values (67% vs. 69%, p = 0.036) and had more frequent coronary comorbidity disease (16.98% vs. 8.82%, p = 0.031). The median OS for patients with or without ACM was 15 months and 25 months, respectively (p = 0.018). Coexisting ACM compared to non-ACM was associated with worse OS in patients with LC (HR = 1.543, 95% CI: 1.042–2.283, p = 0.030).
Conclusion: Coexisting ACM is associated with undesirable survival outcomes in patients with LC. These findings could help us to better understand the cardiac burden in these patients and provide additional risk stratification for them.
Lung cancer (LC) and cardiovascular disease (CVD) are two leading reasons of morbidity and mortality worldwide (1, 2). With the survival of LC patients greatly improved due to multiple revolutionary oncological treatments, such as immunotherapy and targeted-based therapy, several concomitant conditions that significantly impact survival, including CVD, and ischemic stroke (IS) (3, 4), have increased markedly (5, 6). LC and CVD share many risk factors that affect cancer-related survival (7, 8). A study showed that cancer patients are 2–6 times more likely to die of CVD or stroke than the general population (9).
Atrial cardiomyopathy (ACM), initially proposed more than a decade ago, is a pathophysiological concept describing covert atrial structural lesions and functions that involve architectural or physiological changes in the atria (10, 11). Previous research has considered ACM as one of the important etiologies of embolic stroke of undetermined source (ESUS), a subset of cryptogenic ischemic IS (12). The mechanisms of cryptogenic IS include occult structural cardiac lesion, hyper viscosity syndrome or undiagnosed cancer (13). Although it is widely acknowledged that there is a close association between IS and cancer (especially LC) (14), the mechanisms underlying the heightened risks of IS in cancer patients are still uncertain. Moreover, many ACM-related risk factors, such as advanced age, hypertension, diabetes, coronary heart disease, and chronic obstructive pulmonary disease (COPD) (15), are very common in LC patients (16, 17). In addition, cancer and anticancer therapy may cause pathological changes and directly affect atrial substrates (18). Therefore, it can be reasonably inferred that LC patients are also at high risk of ACM, which may confer a higher IS risk.
The influence of ACM on the prognosis of LC patients has never been studied. In this context, we hypothesized that coexisting ACM would be associated with an increased risk of IS and poor prognosis among general LC patients. We investigated the association of ACM with LC outcomes and further examined the related clinical parameters of ACM.
A total of 306 patients with newly diagnosed LC at the First Affiliated Hospital of Xi’an Jiaotong University between January 2015 and December 2020 were retrospectively enrolled in this study. The design of study is described in Figure 1. The protocol was carried out on the basis of the Declaration of Helsinki and approved by the Ethics Committee of the First Affiliated Hospital of Xi’an Jiaotong University (Approval No. XJTU1AF2021LSK-117). These patients were divided into two groups: LC patients with or without ACM. All clinical covariates were abstracted from electronic medical records.
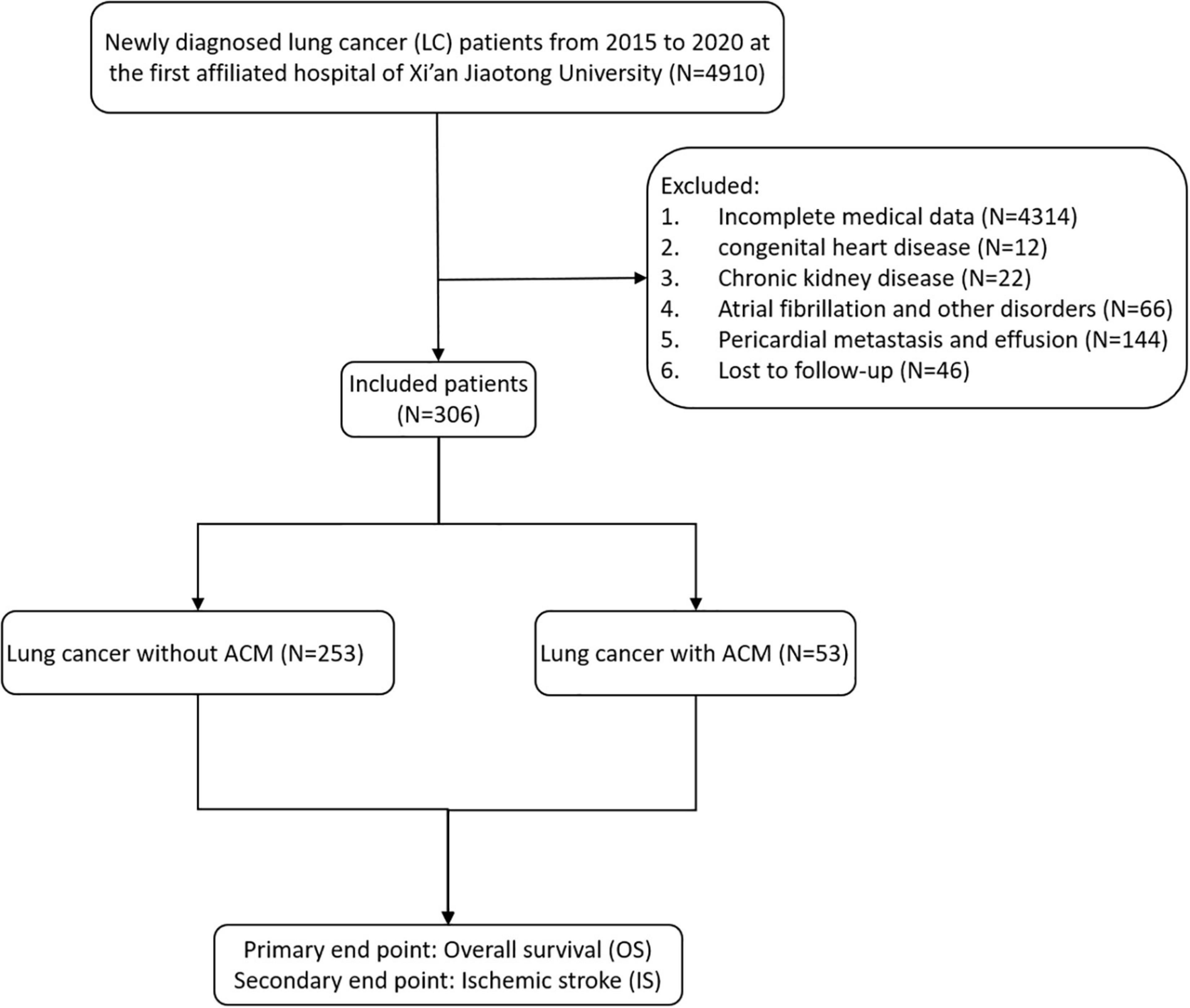
Figure 1. Flowchart detailing patient enrollment.
ACM was defined as having at least one of the following biomarkers according to published literature: (1) p-wave terminal force in V1 (PTFV1) > 5,000 μV* ms; (2) N-terminal pro–B-type natriuretic peptide (NT-proBNP) > 250 pg/mL; and (3) severe left atrial enlargement (LAE: female > 38 mm; male > 40 mm) (19–21).
The inclusion criteria were as follows: (1) newly histologically or cytologically confirmed LC patients and (2) complete medical data for defining ACM and assessing cancer, namely, electrocardiogram (ECG), echocardiography, and NT-proBNP data.
Patients with any of the following conditions were excluded from this cohort: (1) cardiac and valvular history (congenital heart disease, other cardiomyopathies), myocardial infarction within 4 weeks, severe heart failure (left ventricular ejection fraction (LVEF) < 30%), intra-atrial thrombus, or infective endocarditis; (2) pericardial disease (pericardial metastasis, pericardial effusion); (3) heart arrhythmia disorder (atrial flutter, atrial fibrillation); and 4. renal insufficiency (serum creatinine ≥ 186 μmol/L or eGFR < 60 mL/min or chronic kidney disease (CKD) grade 3 and above).
Descriptive statistics are held up as the mean ± standard deviation (SD) for continuous normally distributed variables and as the median (25th percentile, 75th percentile) [M (QL, QU)] for non-normally distributed data. Categorical variables are presented as frequencies and percentages.
For continuous variables, the independent sample t-test is used to compare normally distributed data, and the Wilcoxon rank sum test was used to compare non-normal variables. Count data were statistically analyzed using the chi-square or Fisher exact test. Binary logistic regression was used to determine the risk factors for ACM. Overall survival (OS) was estimated by the Kaplan–Meier method, and significance was evaluated using the log-rank (Mantel–Cox) test. Mortality hazard ratios (HRs) were generated by multivariate Cox regression analysis using univariate Cox predictors. Statistical significance was defined as a p < 0.05.
Our study included 306 patients; their median age was 65 years (range 29–94), and 72.88% were male. In all, 53 (17.32%) patients met the ACM diagnostic criteria. In Table 1, we present the baseline clinical characteristics of the LC patients with or without ACM. The distributions of sex, smoking history, pathological subtype, clinical stage, extrapulmonary/brain metastasis, hypertension, prior stroke, diabetes, and COPD were similar between the groups (p> 0.05), while those of age and coronary disease were different across the groups (p< 0.05). The ACM group had a slightly higher age (69.42 vs. 63.87) and more frequent coronary comorbidity disease (16.98% vs. 8.82%). We then analyzed the gene mutations and PD-L1 characteristics of the non-small-cell lung cancer (NSCLC) subgroup. The distributions of EGFR mutations/ALK fusions and PD-L1 expression levels were not related to ACM in the NSCLC patients (Table 2).
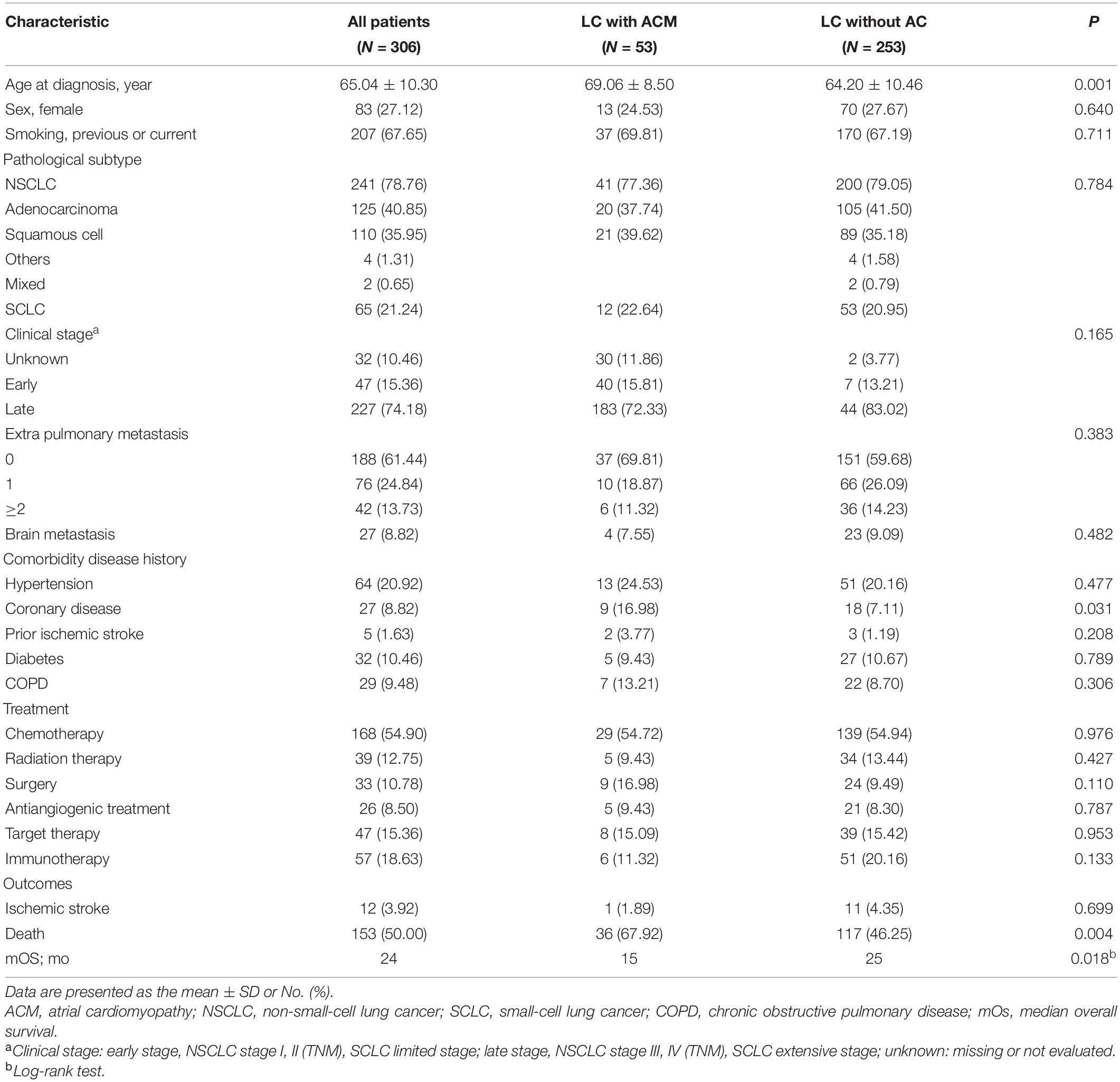
Table 1. Demographic characteristics of patients with LC.
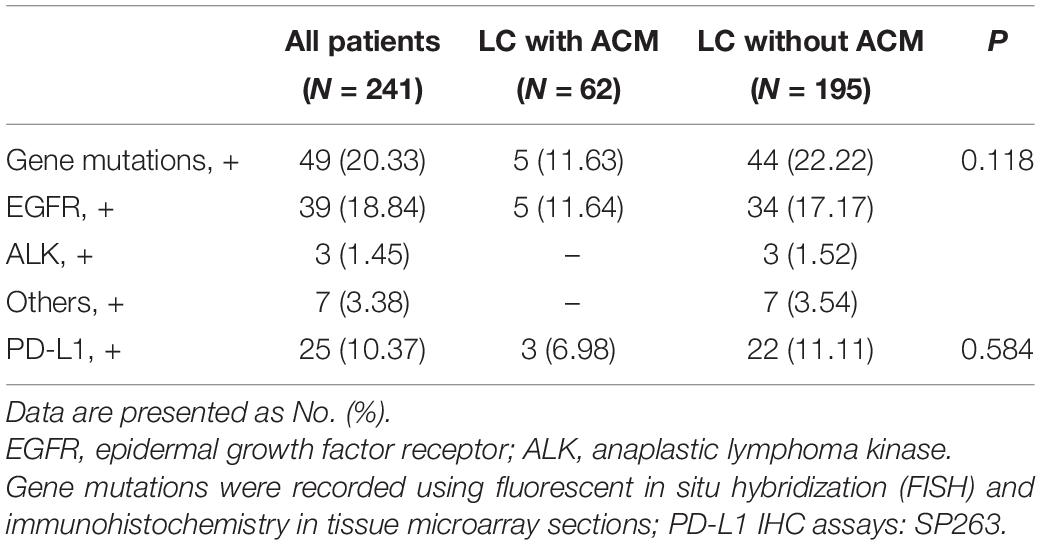
Table 2. Gene mutations and PD-L1 characteristics in the NSCLC subgroup.
Overall, the prevalence of ACM in the LC patients was 17.32% (Table 3). The prevalence of ACM in the NSCLC (241, 78.76%) and small-cell lung cancer (SCLC) (65, 21.24%) populations was not significantly different. The prevalence of ACM in the NSCLC and SCLC populations was not significantly different. In all the LC patients, the frequency of ACM was mostly due to the presence of NT-proBNP (94.34%) and a PTFV1 value > 5,000 μV⋅ms (9.43%). The prevalence of severe LAE was 7.55% in the ACM patients (Table 3).

Table 3. Prevalence of ACM in NSCLC vs. SCLC patients.
Half of the LC patients (153 of 306) died. To avoid deviation caused by different distributions of treatment methods, all the treatments that patients received after diagnosis were recorded (Table 1). The therapeutic mode was similar for patients with ACM compared to those without ACM, which implies that ACM is a risk factor for survival regardless of the subsequent treatment.
To verify this, univariate analysis showed that sex, pathological subtype, clinical stage, smoking history, and ACM positivity had a significant association with survival (Table 4). Notably, Kaplan–Meier curves and log-rank tests showed that ACM was significantly associated with worse survival in LC patients (Figure 2). The median overall survival (mOS) for this LC patients was 23 months. The mOS for patients with or without ACM was 15 months and 25 months, respectively (p = 0.018) (Table 1).
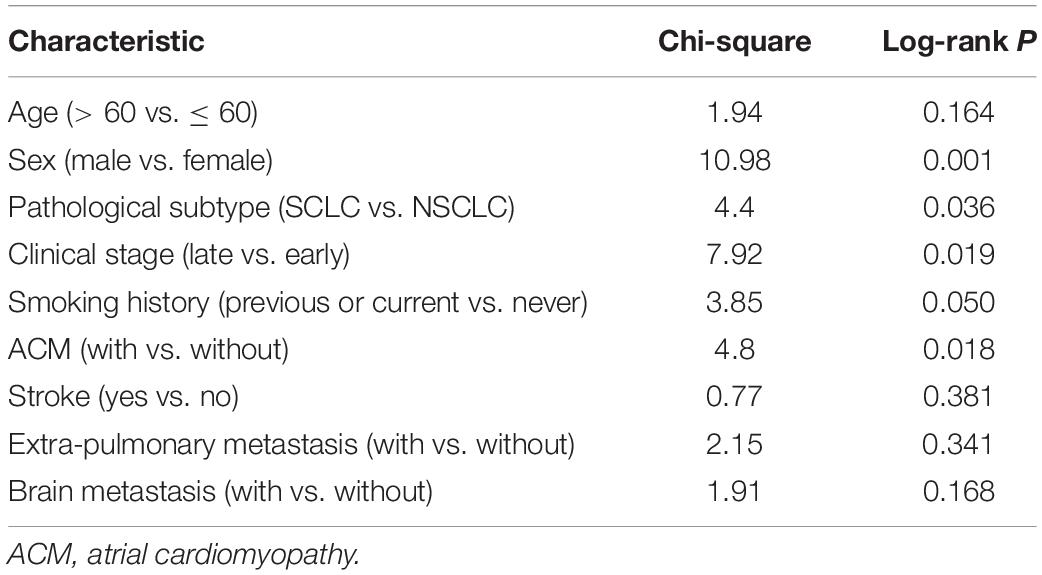
Table 4. Univariate analyses of overall survival.
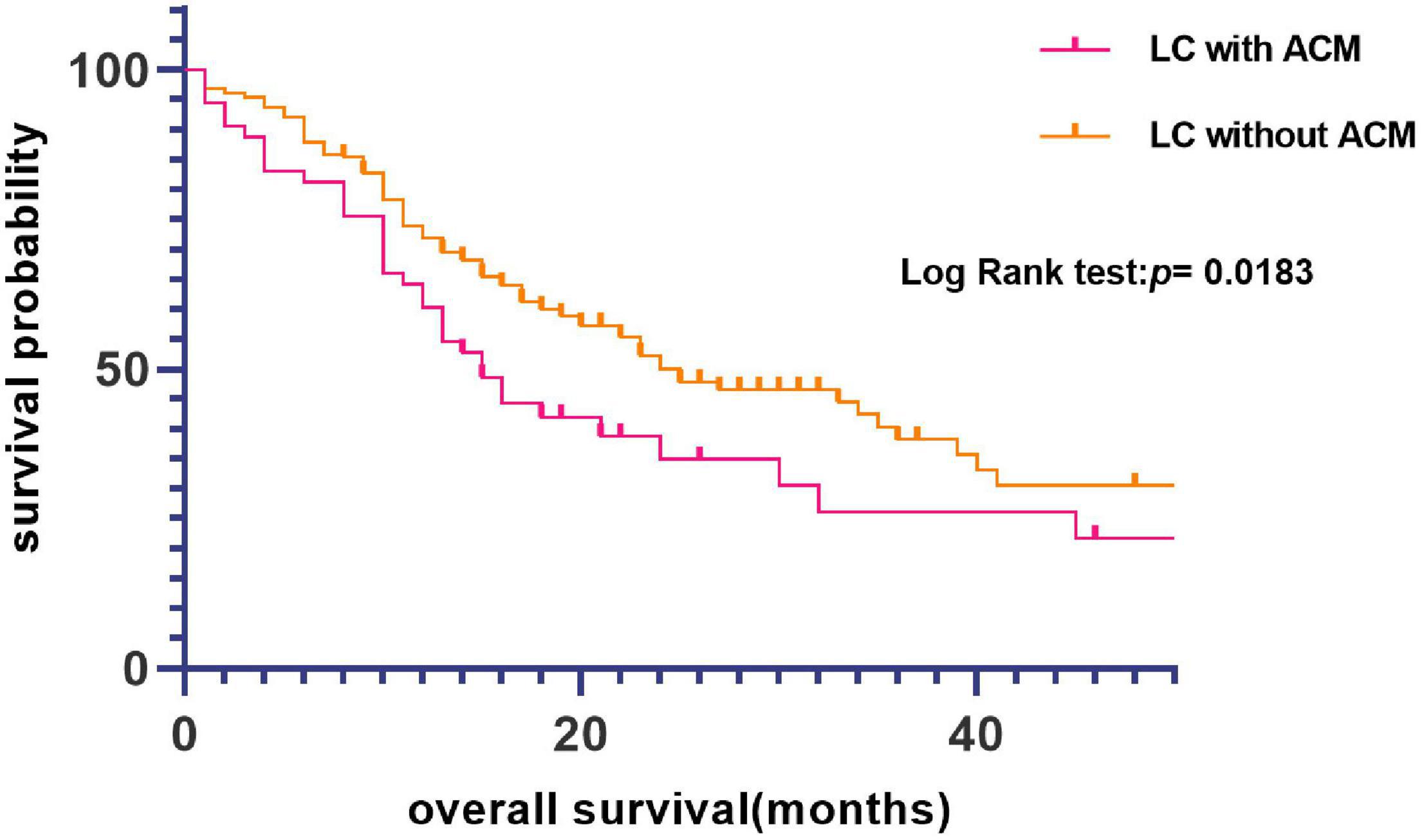
Figure 2. Kaplan–Meier curve of overall survival (OS) based on atrial cardiomyopathy (ACM).
In the multi-variable analysis of the Cox regression models, ACM was significantly associated with worse OS [hazard ratio (HR) = 1.556; 95% CI, 1.069–2.264; p = 0.021]. In the multivariate Cox proportional hazard model adjusting for clinicopathologic variables, the HR of the patients with ACM was 1.543 (95% CI, 1.042–2.283; p = 0.030) compared with that for the patients without ACM (Table 5), suggesting that ACM was an independent risk factor for LC patient prognosis.
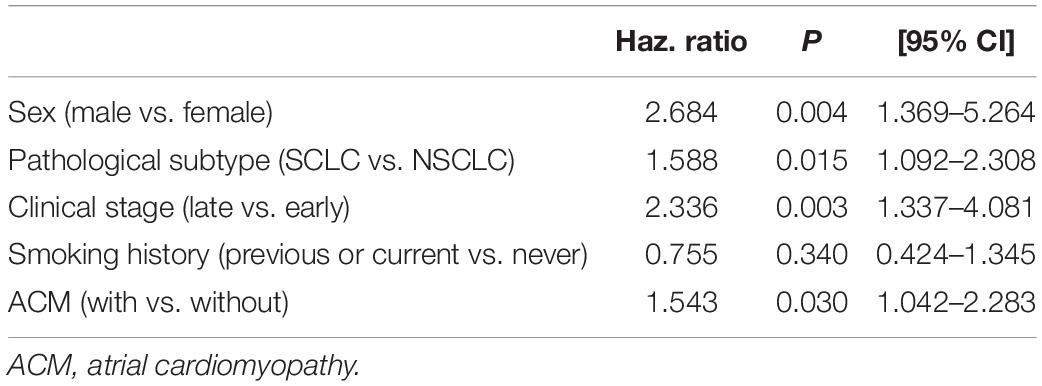
Table 5. Multivariate Cox proportional hazard analyses of overall survival.
Given that 18.5% of the LC patients had ACM and exhibited worse survival, we examined the risk factors in this group. The ECG, echocardiography, complete blood count (CBC) and blood biochemical examination tests performed closest to the date of diagnosis were used for the analysis. Our results showed that ACM patients had higher PTFV1 values (2,350 vs. 1,530, p < 0.000), higher NT-proBNP levels (460.1 vs. 68.54, p < 0.000), lower oxygen saturation values (95 vs. 96, p = 0.0299), higher pH (1.43 vs. 1.42, p = 0.0111), higher D-dimer levels (1.0 vs. 0.6, p = 0.0006) and prothrombin time (PT) (12.9 vs. 12.2, p = 0.0065), lower lymphocyte (1.17 vs. 1.28, p = 0.0469) and hemoglobin levels (123 vs. 133, p = 0.0049), higher CRP levels (mean CRP: 28.35 vs. 18.86, p = 0.00373), lower serum calcium levels (2.23 vs. 2.31, p = 0.001), and lower phosphate levels (0.96 vs. 1.03, p = 0.0046) (Table 6 and Supplementary Table 1).
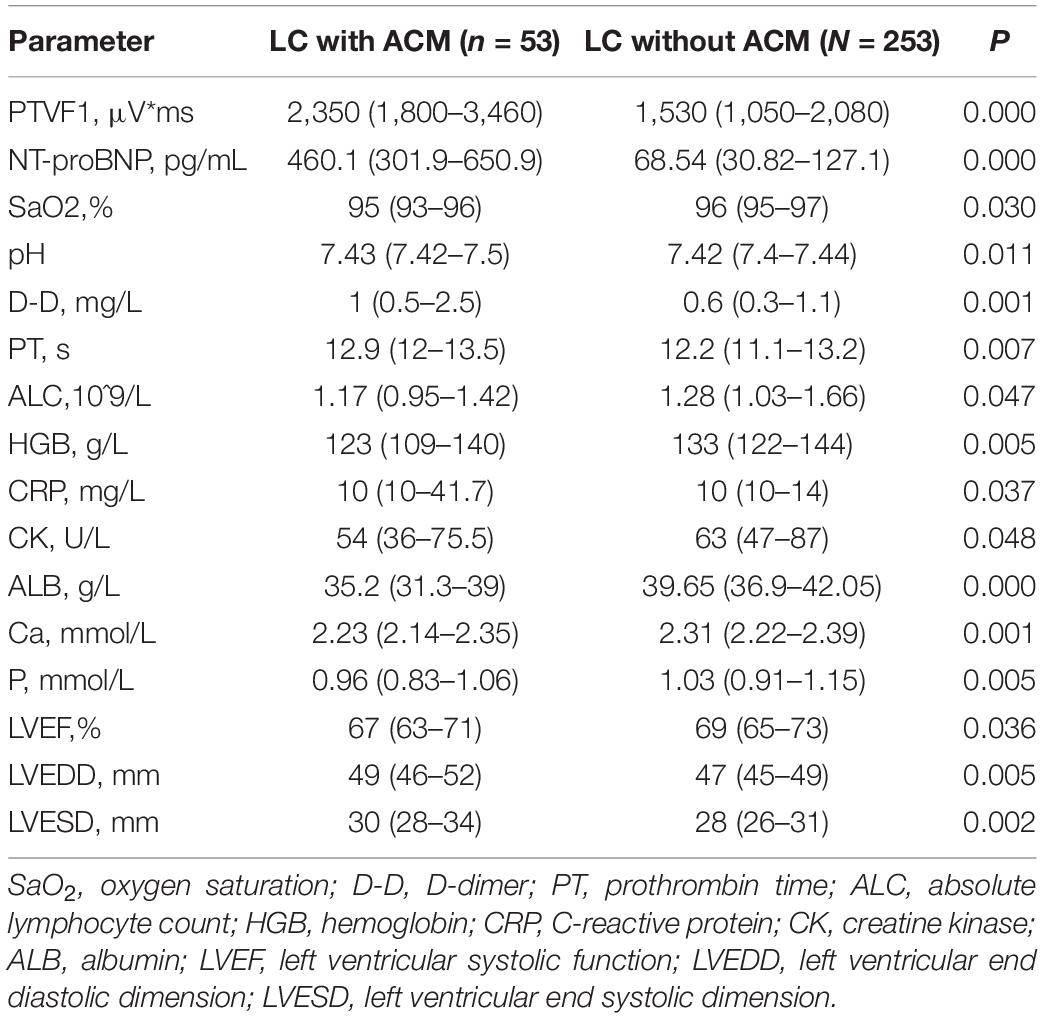
Table 6. Comparison of baseline LC patients with/without ACM.
In addition, admission transthoracic echocardiograms were reviewed for all the patients. Those with ACM had lower LVEF values (67% vs. 69%, p = 0.0357). Univariate logistic analysis showed that patients with lower LVEF values were likely to be complicated with ACM (OR = 0.938, p = 0.007, 95% CI, 0.895–0.938). Hematological examinations and echocardiography indexes were included in the multivariate logistic regression analysis. As shown in Table 7, we found that higher D-dimer levels (p = 0.016, OR = 1.246) and lower serum calcium levels (p = 0.019, OR = 0.001) were significant risk factors for ACM. In the multivariate analysis, transthoracic echocardiogram indexes failed to show any meaningful value (Supplementary Table 2).
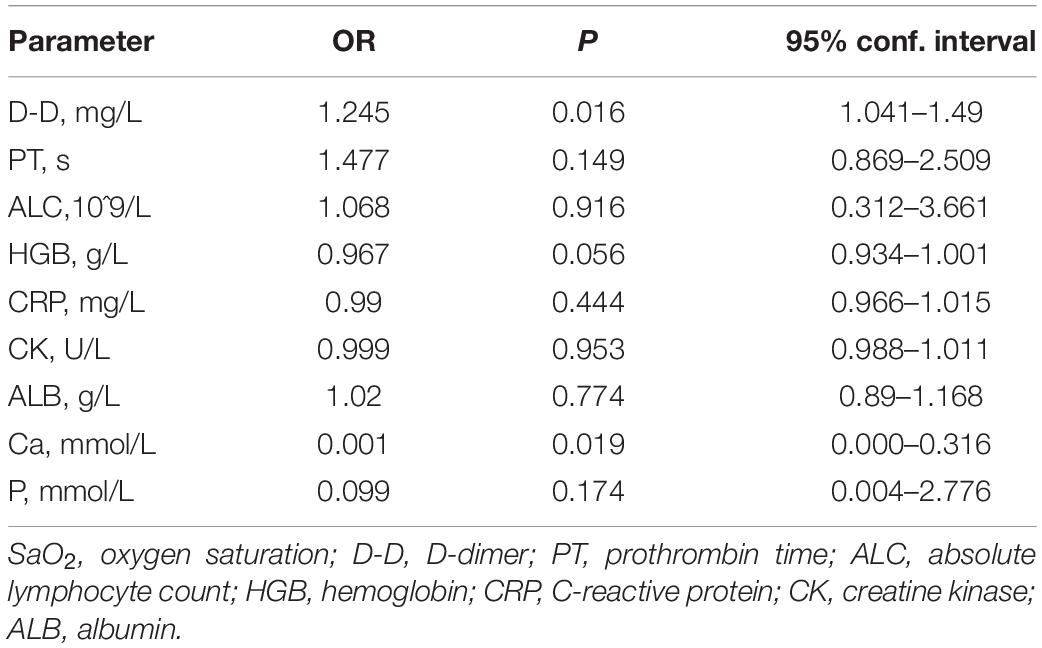
Table 7. Multivariate logistic regression analysis of clinical parameters.
In this observational, retrospective cohort study, 585 patients with LC were followed for a median of 20 months. In our study, the prevalence of LC patients with ACM was 17.32%, and these patients had a higher age (69 vs. 65) and more frequent coronary comorbidity disease (16.98% vs. 8.82%). However, the prevalence of ACM in LC patients was not significantly different in different pathological subtypes. In addition, we found that coexisting ACM was associated with worse OS (15 vs. 25) in patients with LC, who had higher D-dimer levels, lower serum calcium levels and lower LVEF values than the non-ACM patients. Together, these findings support that the comorbidity of ACM is associated with poorer survival in LC patients. However, we did not find that cancer-related IS was associated with ACM. These data highlight the need for further studies to better investigate the underlying mechanisms of stroke and cancer.
Any abnormalities of the atria of structural, architectural, contractile, or electrophysiological changes have been used to define a new entity known as ACM (22). In EHRAS (European Heart Rhythm Association; EHRA/Heart Rhythm Society; HRS/Asian Pacific Heart Rhythm Association; APHRS/Latin American Society of Electrophysiology and Cardiac Stimulation; SOLAECE) classification, ACM were defined into four types: principal cardiomyocyte changes; fibrotic changes; combined cardiomyocyte-pathology/fibrosis and non-collagen infiltration (23). However, most patients would not receive myocardial biopsy, making histological and pathopysiological classification hard to evaluate. At present, there is no absolute diagnostic criteria for ACM, but most of the studies are defined by the relevant markers of ACM. For example, it is reported that PTFV 1 abnormality is related to the increase of left atrial volume and the decrease of left atrial emptying fraction and reservoir function (24). Any pathological state that causes atrial dysfunction can lead to the increase of PTFV1, implying this ECG biomarkers may be the signs of ACM. Numerous randomized studies have adopted the combined biomarkers to define ACM (25). Other biomarkers includes LAE, paroxysmal supraventricular tachycardia, bayes syndrome, and serum biomarkers associated with atrial dysfunction, etc. In recent years, more emerging imaging techniques (such as cardiac computed tomography or magnetic resonance imaging and so on) have been used for accurate assessment of atrial structure and function, which may provide more supports of detecting ACM (26, 27). A study use late gadolinium enhancement MRI (LGE-MRI) to evaluate atrial fibrosis and it is associated with appendage thrombus (28).
A previous study reported that the prevalence of ACM (26.6%) is increased in patients with ESUS compared to patients with other established etiologies for IS (21). In this study, we found that 17.32% of the LC patients had ACM. The key clinical determinants of ACM are unclear, but it is reported to be related to many disease or conditions, such as aging, smoking, hypertension, diabetes, coronary heart disease, and heart failure (15, 29). These high-risk factors overlap in most LC patients (30). This is also shown in this study. In addition, ACM-related biomarkers play an important role in the development of malignancies (18), suggesting that some physiological changes are shared by LC and ACM. For example, various studies have confirmed that NT-proBNP, a biomarker of ACM, and other biomarkers of CVD have prognostic significance in cancer (31, 32). A study showed that coexisting CVD precancerous polyps lead to tumor progression and secretion of cardiac excreted factors, mechanically supporting the above hypothesis (33).
On the other hand, recognition of the interaction between cancer and atrial fibrillation (AF) has shed new light on the relationship with ACM. The basic pathology characteristic of AF and ACM is myocardial fibrosis. Fibrosis can be caused by inflammation and its mediators (34), such as systemic infection and autoimmune diseases, and may also occur in chronic inflammation (such as cancer) (35). Atrial fibrosis can precede AF or even exist without AF, which implies that ACM is the substrate for AF (18). This means that cancer or other coexisting subclinical inflammatory diseases (such as hypertension and coronary artery disease) and conditions (like aging and endocrine abnormalities) can produce inflammatory mediators, which change atrial electrophysiology and structural substrates (36). Many studies have reported that patients with malignancy have increased susceptibility to AF (37, 38), which also supports this theory.
We explored the relationship between ACM and LC and its influence on the survival of LC patients. The coexisting ACM was significantly associated with worse survival in patients with LC.
The biological mechanisms by which ACM may influence prognosis are unclear, but several lines of evidence suggest that this result is biologically reasonable. First, cancer is a systemic inflammatory condition originated from a combination of genetic, habitual and environmental factors (39). ACM has been associated with several clinical comorbidities and inflammatory conditions, such as systemic infections (15, 34). This means that the various comorbidities or conditions that may adversely affect the occurrence and outcomes of LC could also lead to ACM. Second, the factors that cause abnormalities in atrial tissue substrates can also be systemic manifestations of tumor progression. Cancer can promote the development of atrial fibrosis, leading to metabolic and electrolyte abnormalities, fluid imbalance, and infections. These inflammatory states then contribute to atrial remodeling (40), making ACM a prognostic marker. In other words, there is a bidirectional and progressive relationship between ACM and LC. The abnormality of many ACM-related markers has been shown to be associated with the prognosis of cancer patients. For example, NT-proBNP levels are related to the severity of malignancy without cardiac disease or cardiotoxicity in anticancer therapy (41, 42). In addition, atrial lesions have substantial related adverse outcomes including arrhythmogenic changes, atrial fibroblast proliferation, hyperinnervation, and thrombogenic changes (23, 43), all of which can lead to worse prognosis in lung cancer patients. For instance, arterial thrombosis is a marker of occult cancer (especially lung cancer) and an unfavorable prognostic factor (44, 45). Taken together, with the effect of cancer and other risk factors, pathological changes of atrial cells (like myocardial hypertrophy, fibrosis, and fatty infiltration and so on) results in mechanical dysfunction or abnormal electrical conduction, which eventually converts to atrial dilatation and the congestive heart failure. These factors all contributes to the worse survival of LC. Our study showed that patients with lower LVEF values were likely to be complicated with ACM, which buttressed that view.
A new perspective of the relationship between AF and stroke has emerged in the past decade.
Although AF has been proved to be related to IS, the causal relationship between them is still indirect. A study found that there was no consistent time correlation between AF and IS (46).
A study reported that variants of chromosome associated with increased risk of cardioembolic IS, even in those not detected to have AF (47). A study reported nearly 65% of patients with cryptogenic stroke have ACM (20). These evidences verify that ACM may be the basis of IS.
Taken together, ACM is an important marker of increased risk of thromboembolism, particularly IS. Atrial abnormality forms the substrate for thrombus formation and AF may be a sign of potential risk of ACM. ACM itself, even without AF, is a risk factor for stroke (48). The mechanism of elevated risk of thrombus formation is likely related to the interaction between a generalized and local pro-thrombotic and inflammatory state (22). Moreover, atrial fibrosis, enlargement, and dysfunction may further lead to atrial congestion, pre-thrombotic state and subsequent IS (49).
Clinical trials have shown that treatment with ACM may reduce the risk of IS (50). Cryptogenic stroke (40–51%) is more common in cancer patients than in the general population (51). Compared with cancer-free controls, survivors of LC show a higher risk of stroke (52). Previous studies have reported that 45–65% of cryptogenic stroke patients have comorbidities of ACM (19, 20). Therefore, there are good reasons to hypothesize that ACM has a strong association with cancer-related stroke.
Unfortunately, we have not demonstrated this relevance in this set of data. The univariate analysis showed that there was no significant correlation between stroke and survival (Table 4). There are several possible reasons. The main reason is that the number of stroke events was too small in this cohort to verify the conclusion. Some patients received treatments at other centers, leading to some lost-to-follow-up and thus unknown ending events. Moreover, in order to evaluate the comorbidity of ACM, many patients with incomplete information occurring ending events were excluded from analysis. However, given that ACM is associated with a second era in understanding the relationship of disorders of the atria to stroke risk and anticoagulant therapy is still open to debate, we look forward to more research in this field in the future to reveal the etiology of stroke in cancer patients.
Our study has limitations due to its single-center design, small sample size, and incomplete matching or exclusion of many patients from the analysis. Second, data were extract retrospectively, and much clinical information related to tumor assessment was not complete and lacked elaboration. Third, this study failed to analyze the impact of completing treatment for some patients who received treatments at other centers. More studies are needed in the future, such as prospective studies to determine reliable biomarkers to predict cancer-related stroke and clinical trials to determine the treatment and prevention of ACM.
Our study provides the first evidence that the comorbidity of ACM predicts worse prognosis in patients with LC. In addition, we found that higher D-dimer levels, lower serum calcium levels, and lower LVEF values were significant risk factors for ACM. NT-proBNP and PTFV1 are not routine clinical assessments for cancer patients. Our results imply that patients with those abnormal indexes may have coexisting ACM and a worse prognosis. Given that patients with ACM have a higher risk of poor survival, more frequent follow-up and detection in these patients should be considered.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by the Ethics Committee of the First Affiliated Hospital of Xi’an Jiaotong University. The patients/participants provided their written informed consent to participate in this study.
MR and YM contributed to clinical data collection and analysis. HL and XS provided support and assistance in data extraction. All authors contributed to the article and approved the submitted version.
This study was supported by the Shaanxi Provincial Key R&D Program General Project (2022SF-058).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
We thank the Biobank of First Affiliated Hospital of Xi’an Jiaotong University for providing clinical data.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fcvm.2022.932044/full#supplementary-material
1. Duarte CW, Lindner V, Francis SA, Schoormans D. Visualization of cancer and cardiovascular disease co-occurrence with network methods. JCO Clin Cancer Inform. (2017) 1:1–12. doi: 10.1200/CCI.16.00071
2. Zhou M, Wang H, Zeng X, Yin P, Zhu J, Chen W, et al. Mortality, morbidity, and risk factors in China and its provinces, 1990-2017: a systematic analysis for the global burden of disease study 2017. Lancet. (2019) 394:1145–58. doi: 10.1016/S0140-6736(19)30427-1
3. Navi BB, Iadecola C. Ischemic stroke in cancer patients: a review of an underappreciated pathology. Ann Neurol. (2018) 83:873–83. doi: 10.1002/ana.25227
4. Armenian SH, Xu L, Ky B, Sun C, Farol LT, Pal SK, et al. Cardiovascular disease among survivors of adult-onset cancer: a community-based retrospective cohort study. J Clin Oncol. (2016) 34:1122–30. doi: 10.1200/JCO.2015.64.0409
5. Stoltzfus KC, Zhang Y, Sturgeon K, Sinoway LI, Trifiletti DM, Chinchilli VM, et al. Fatal heart disease among cancer patients. Nat Commun. (2020) 11:2011.
6. Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global cancer statistics 2020: globocan estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. (2021) 71:209–49. doi: 10.3322/caac.21660
7. Lyon AR, Dent S, Stanway S, Earl H, Brezden-Masley C, Cohen-Solal A, et al. Baseline cardiovascular risk assessment in cancer patients scheduled to receive cardiotoxic cancer therapies: a position statement and new risk assessment tools from the cardio-oncology study group of the heart failure association of the European society of cardiology in collaboration with the international cardio-oncology society. Eur J Heart Fail. (2020) 22:1945–60. doi: 10.1002/ejhf.1920
8. Alvarez-Cardona JA, Ray J, Carver J, Zaha V, Cheng R, Yang E, et al. Cardio-oncology education and training: JACC council perspectives. J Am Coll Cardiol. (2020) 76:2267–81. doi: 10.1016/j.jacc.2020.08.079
9. Sturgeon KM, Deng L, Bluethmann SM, Zhou S, Trifiletti DM, Jiang C, et al. A population-based study of cardiovascular disease mortality risk in US cancer patients. Eur Heart J. (2019) 40:3889–97. doi: 10.1093/eurheartj/ehz766
10. Hammwöhner M, Bukowska A, Mahardika W, Goette A. Clinical importance of atrial cardiomyopathy. Int J Cardiol. (2019) 287:174–80.
11. Dong M, Liu T, Li G. Atrial cardiomyopathy–a not yet classified cardiomyopathy? Int J Cardiol. (2011) 151:394–6. doi: 10.1016/j.ijcard.2011.07.003
12. Leifer D, Rundek T. Atrial cardiopathy: a new cause for stroke? Neurology. (2019) 92:155–6. doi: 10.1212/WNL.0000000000006749
13. Mac Grory B, Flood SP, Apostolidou E, Yaghi S. Cryptogenic stroke: diagnostic workup and management. Curr Treat Options Cardiovasc Med. (2019) 21:77. doi: 10.1007/s11936-019-0786-4
14. Navi BB, Reiner AS, Kamel H, Iadecola C, Okin PM, Elkind MSV, et al. Risk of arterial thromboembolism in patients with cancer. J Am Coll Cardiol. (2017) 70:926–38.
15. Guichard JB, Nattel S. Atrial cardiomyopathy: a useful notion in cardiac disease management or a passing fad? J Am Coll Cardiol. (2017) 70:756–65. doi: 10.1016/j.jacc.2017.06.033
16. Zhai R, Yu X, Shafer A, Wain JC, Christiani DC. The impact of coexisting COPD on survival of patients with early-stage non-small cell lung cancer undergoing surgical resection. Chest. (2014) 145:346–53. doi: 10.1378/chest.13-1176
17. Mao Y, Yang D, He J, Krasna MJ. Epidemiology of lung cancer. Surg Oncol Clin N Am. (2016) 25:439–45. doi: 10.1016/j.jtho.2015.09.015
18. Ren M, Yao Y, Yue X, Ning Y, Yang Y. Atrial cardiomyopathy and atrial fibrillation in cancer. Cardiol Res Pract. (2021) 2021:6685953. doi: 10.1155/2021/6685953
19. Ntaios G, Perlepe K, Lambrou D, Sirimarco G, Strambo D, Eskandari A, et al. Prevalence and overlap of potential embolic sources in patients with embolic stroke of undetermined source. J Am Heart Assoc. (2019) 8:e012858. doi: 10.1161/JAHA.119.012858
20. Yaghi S, Boehme AK, Hazan R, Hod EA, Canaan A, Andrews HF, et al. Atrial cardiopathy and cryptogenic stroke: a cross-sectional pilot study. J Stroke Cerebrovasc Dis. (2016) 25:110–4. doi: 10.1016/j.jstrokecerebrovasdis.2015.09.001
21. Jalini S, Rajalingam R, Nisenbaum R, Javier AD, Woo A, Pikula A. Atrial cardiopathy in patients with embolic strokes of unknown source and other stroke etiologies. Neurology. (2019) 92:e288–94.
22. Yaghi S, Kamel H, Elkind MSV. Atrial cardiopathy: a mechanism of cryptogenic stroke. Expert Rev Cardiovasc Ther. (2017) 15:591–9. doi: 10.1080/14779072.2017.1355238
23. Goette A, Kalman JM, Aguinaga L, Akar J, Cabrera JA, Chen SA, et al. EHRA/HRS/APHRS/SOLAECE expert consensus on atrial cardiomyopathies: definition, characterization, and clinical implication. Europace. (2016) 18:1455–90.
24. Tiffany Win T, Ambale Venkatesh B, Volpe GJ, Mewton N, Rizzi P, Sharma RK, et al. Associations of electrocardiographic P-wave characteristics with left atrial function, and diffuse left ventricular fibrosis defined by cardiac magnetic resonance: the PRIMERI Study. Heart Rhythm. (2015) 12:155–62. doi: 10.1016/j.hrthm.2014.09.044
25. Kamel H, Longstreth WT Jr., Tirschwell DL, Kronmal RA, Broderick JP, Palesch YY, et al. The AtRial cardiopathy and antithrombotic drugs in prevention after cryptogenic stroke randomized trial: rationale and methods. Int J Stroke. (2019) 14:207–14. doi: 10.1177/1747493018799981
26. Oakes RS, Badger TJ, Kholmovski EG, Akoum N, Burgon NS, Fish EN, et al. Detection and quantification of left atrial structural remodeling with delayed-enhancement magnetic resonance imaging in patients with atrial fibrillation. Circulation. (2009) 119:1758–67. doi: 10.1161/CIRCULATIONAHA.108.811877
27. Kurotobi T, Iwakura K, Inoue K, Kimura R, Toyoshima Y, Ito N, et al. The significance of the shape of the left atrial roof as a novel index for determining the electrophysiological and structural characteristics in patients with atrial fibrillation. Europace. (2011) 13:803–8. doi: 10.1093/europace/eur039
28. Akoum N, Fernandez G, Wilson B, McGann C, Kholmovski E, Marrouche N. Association of atrial fibrosis quantified using LGE-MRI with atrial appendage thrombus and spontaneous contrast on transesophageal echocardiography in patients with atrial fibrillation. J Cardiovasc Electrophysiol. (2013) 24:1104–9. doi: 10.1111/jce.12199
29. Patnaik JL, Byers T, DiGuiseppi C, Dabelea D, Denberg TD. Cardiovascular disease competes with breast cancer as the leading cause of death for older females diagnosed with breast cancer: a retrospective cohort study. Breast Cancer Res. (2011) 13:R64. doi: 10.1186/bcr2901
30. Esposito K, Chiodini P, Colao A, Lenzi A, Giugliano D. Metabolic syndrome and risk of cancer: a systematic review and meta-analysis. Diabetes Care. (2012) 35:2402–11.
31. Tuñón J, Higueras J, Tarín N, Cristóbal C, Lorenzo Ó, Blanco-Colio L, et al. N-Terminal pro-brain natriuretic peptide is associated with a future diagnosis of cancer in patients with coronary artery disease. PLoS One. (2015) 10:e0126741. doi: 10.1371/journal.pone.0126741
32. Narayan V, Thompson EW, Demissei B, Ho JE, Januzzi JL Jr., Ky B. Mechanistic biomarkers informative of both cancer and cardiovascular disease: JACC state-of-the-art review. J Am Coll Cardiol. (2020) 75:2726–37. doi: 10.1016/j.jacc.2020.03.067
33. Meijers WC, Maglione M, Bakker SJL, Oberhuber R, Kieneker LM, de Jong S, et al. Heart failure stimulates tumor growth by circulating factors. Circulation. (2018) 138:678–91.
34. Hu YF, Chen YJ, Lin YJ, Chen SA. Inflammation and the pathogenesis of atrial fibrillation. Nat Rev Cardiol. (2015) 12:230–43.
35. Zhao H, Wu L, Yan G, Chen Y, Zhou M, Wu Y, et al. Inflammation and tumor progression: signaling pathways and targeted intervention. Signal Transduction Targeted Ther. (2021) 6:263. doi: 10.1038/s41392-021-00658-5
36. Leiva O, AbdelHameid D, Connors JM, Cannon CP, Bhatt DL. Common pathophysiology in cancer, atrial fibrillation, atherosclerosis, and thrombosis: JACC: cardiooncology state-of-the-art review. JACC CardioOncol. (2021) 3:619–34. doi: 10.1016/j.jaccao.2021.08.011
37. Jakobsen CB, Lamberts M, Carlson N, Lock-Hansen M, Torp-Pedersen C, Gislason GH, et al. Incidence of atrial fibrillation in different major cancer subtypes: a nationwide population-based 12 year follow up study. BMC Cancer. (2019) 19:1105. doi: 10.1186/s12885-019-6314-9
38. D’Souza M, Smedegaard L, Madelaire C, Nielsen D, Torp-Pedersen C, Gislason G, et al. Incidence of atrial fibrillation in conjunction with breast cancer. Heart Rhythm. (2019) 16:343–8. doi: 10.1016/j.hrthm.2018.10.017
39. Cao X, Wang X, Wang H, Xu G, Yu H. Systemic inflammation status relates to anti-inflammatory drug benefit and survival in rectal cancer. J Surg Res. (2022) 269:249–59. doi: 10.1016/j.jss.2021.08.028
40. Chu G, Versteeg HH, Verschoor AJ, Trines SA, Hemels MEW, Ay C, et al. Atrial fibrillation and cancer – an unexplored field in cardiovascular oncology. Blood Rev. (2019) 35:59–67. doi: 10.1016/j.blre.2019.03.005
41. Pavo N, Cho A, Wurm R, Strunk G, Krauth M, Agis H, et al. N-terminal B-type natriuretic peptide (NT-proBNP) is associated with disease severity in multiple myeloma. Eur J Clin Invest. (2018) 48:e12905. doi: 10.1111/eci.12905
42. Patel SR, Herrmann J, Vierkant RA, Olson JE, Couch FJ, Hazim A, et al. N-Terminal pro brain natriuretic peptide, sST2, and galectin-3 levels in breast cancer survivors. J Clin Med. (2021) 10:3313. doi: 10.3390/jcm10153313
43. Hoit BD. Left atrial size and function: role in prognosis. J Am Coll Cardiol. (2014) 63:493–505. doi: 10.1016/j.jacc.2013.10.055
44. Sundbøll J, Veres K, Horváth-Puhó E, Adelborg K, Sørensen HT. Risk and prognosis of cancer after lower limb arterial thrombosis. Circulation. (2018) 138:669–77. doi: 10.1161/CIRCULATIONAHA.117.032617
45. Mulder FI, Horváth-Puhó E, van Es N, Pedersen L, Büller HR, Bøtker HE, et al. Arterial thromboembolism in cancer patients: a Danish population-based cohort study. JACC CardioOncol. (2021) 3:205–18. doi: 10.1016/j.jaccao.2021.02.007
46. Brambatti M, Connolly SJ, Gold MR, Morillo CA, Capucci A, Muto C, et al. Temporal relationship between subclinical atrial fibrillation and embolic events. Circulation. (2014) 129:2094–9.
47. Gretarsdottir S, Thorleifsson G, Manolescu A, Styrkarsdottir U, Helgadottir A, Gschwendtner A, et al. Risk variants for atrial fibrillation on chromosome 4q25 associate with ischemic stroke. Ann Neurol. (2008) 64:402–9. doi: 10.1002/ana.21480
48. Kamel H, Okin PM, Elkind MS, Iadecola C. Atrial fibrillation and mechanisms of stroke: time for a new model. Stroke. (2016) 47:895–900. doi: 10.1161/STROKEAHA.115.012004
49. Goldberger JJ, Arora R, Green D, Greenland P, Lee DC, Lloyd-Jones DM, et al. Evaluating the atrial myopathy underlying atrial fibrillation: identifying the arrhythmogenic and thrombogenic substrate. Circulation. (2015) 132:278–91.
50. Healey JS, Gladstone DJ, Swaminathan B, Eckstein J, Mundl H, Epstein AE, et al. Recurrent stroke with rivaroxaban compared with aspirin according to predictors of atrial fibrillation: secondary analysis of the NAVIGATE ESUS randomized clinical trial. JAMA Neurol. (2019) 76:764–73. doi: 10.1001/jamaneurol.2019.0617
51. Salazar-Camelo RA, Moreno-Vargas EA, Cardona AF, Bayona-Ortiz HF. Ischemic stroke: a paradoxical manifestation of cancer. Crit Rev Oncol Hematol. (2021) 157:103181. doi: 10.1016/j.critrevonc.2020.103181
Keywords: lung cancer, atrial cardiomyopathy, atrial fibrillation, oncocardiology, ischemic stroke
Citation: Ren M, Ma Y, Wei M, Ning Y, Liu H, Shi X, Yao Y and Guo F (2022) Atrial Cardiomyopathy Predicts Worse Outcome in Patients With Lung Cancer. Front. Cardiovasc. Med. 9:932044. doi: 10.3389/fcvm.2022.932044
Received: 29 April 2022; Accepted: 30 May 2022;
Published: 01 July 2022.
Edited by:
Tong Liu, Tianjin Medical University, ChinaReviewed by:
Feng Hu, Shanghai Jiao Tong University, ChinaCopyright © 2022 Ren, Ma, Wei, Ning, Liu, Shi, Yao and Guo. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yu Yao, MTM1NzIxMDE2MTFAMTYzLmNvbQ==; Fengwei Guo, Z3VvZmVuZ3dlaUB4anR1LmVkdS5jbg==
†These authors have contributed equally to this work and share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.