
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
STUDY PROTOCOL article
Front. Cardiovasc. Med. , 21 June 2022
Sec. Cardiovascular Imaging
Volume 9 - 2022 | https://doi.org/10.3389/fcvm.2022.909347
This article is part of the Research Topic Evaluation of the Left Atrium: Its role in atrial fibrillation and diastolic function View all 6 articles
 Luis López1,2
Luis López1,2 Xavier Rossello2,3*Dora Romaguera2,4Ángel M. Alonso-Gómez4,5
Xavier Rossello2,3*Dora Romaguera2,4Ángel M. Alonso-Gómez4,5 Estefanía Toledo4,6Elena Fortuny2,3Marta Noris2,3Caterina Mas-Lladó1,2Miquel Fiol2,4Raul Ramallal7Lucas Tojal-Sierra5
Estefanía Toledo4,6Elena Fortuny2,3Marta Noris2,3Caterina Mas-Lladó1,2Miquel Fiol2,4Raul Ramallal7Lucas Tojal-Sierra5 Alvaro Alonso8Carlos Fernandez-Palomeque2,3
Alvaro Alonso8Carlos Fernandez-Palomeque2,3Background: The metabolic syndrome (MetS) is associated with increased cardiovascular morbidity and mortality. Characterization of cardiac structural and functional abnormalities due to the MetS can help recognize individuals who would benefit the most from preventive interventions. Transthoracic echocardiography (TTE) provides an opportunity to identify those abnormalities in a reproducible and cost-efficient manner. In research settings, implementation of protocols for the acquisition and analysis of TTE images are key to ensure validity and reproducibility, thus facilitating answering relevant questions about the association of the MetS with cardiac alterations.
Methods and Results: The Palma Echo Platform (PEP) is a coordinated network that is built up to evaluate the underlying structural and functional cardiac substrate of participants with MetS. Repeated TTE will be used to evaluate 5-year changes in the cardiac structure and function in a group of 565 individuals participating in a randomized trial of a lifestyle intervention for the primary prevention of cardiovascular disease. The echocardiographic studies will be performed at three study sites, and will be centrally evaluated at the PEP core laboratory. Planned analyses will involve evaluating the effect of the lifestyle intervention on cardiac structure and function, and the association of the MetS and its components with changes in cardiac structure and function. Particular emphasis will be placed on evaluating parameters of left atrial structure and function, which have received more limited attention in past investigations. This PEP will be available for future studies addressing comparable questions.
Conclusion: In this article we describe the protocol of a central echocardiography laboratory for the study of functional and structural alterations of the MetS.
Metabolic syndrome (MetS) is becoming a global public health issue (1) due to the increasing levels of obesity and physical inactivity among adults in many countries. MetS is defined by the presence of several cardiovascular risk factors (CVRFs), such as insulin resistance, dyslipidemia, and arterial hypertension, which in association with visceral obesity confer a high risk of developing cardiovascular disease (CVD) (2). From a pathophysiological perspective, it is unclear whether MetS have a similar impact on the heart and the arteries (the two components of the cardiovascular system) (3). MetS is associated with atherosclerosis and pro-thrombotic states on the arteries, whereas less is known about the impact of MetS on the function and structure of the heart (4, 5). An early detection of functional and structural myocardial alterations can be useful to better understand the association between MetS and CVD, and to identify those patients with MetS who might benefit from an early intervention (2).
Transthoracic Echocardiography (TTE) is broadly used in clinical practice to evaluate the structure and function of the heart in a non-invasive and inexpensive way (6). Moreover, TTE is a radiation-free test, available in most hospitals. A platform aimed to systematically and consistently evaluate TTEs would be useful to evaluate the underlying structural and functional cardiac substrate of participants with MetS. Thus, we report the rationale and design of the Palma Echo Platform (PEP), a platform aimed to longitudinally assess TTEs collected over a 5-year period among participants with MetS without prior CVD. This platform would be initially an opportunity to evaluate 5-year changes in the cardiac structure and function in a group of 565 individuals participating in a randomized trial of a lifestyle intervention for the primary prevention of CVD, though their use might be extended to other cardiovascular settings.
Participants have been already recruited for the PREvención con DIeta MEDiterranea-Plus (PREDIMED-Plus). This is an ongoing 6-year multicenter, parallel-group, randomized clinical trial, which is currently being conducted in 23 Spanish recruiting centers (universities, hospitals, and research institutes). Participants included women aged 60–75 years and men aged 55–75 years, without known CVD, with a body mass index (BMI) between 27.0 and 40.0 kg/m2 and meeting at least 3 of the following criteria defined by the International Diabetes Federation, the American Heart Association and the National Heart, Lung, and Blood Institute (4), which are: (i) elevated waist circumference (> 80 cm for women, and > 94 cm for men); (ii) elevated triglycerides (> 150 mg/dl) or drug treatment for elevated triglycerides; (iii) reduced HDL-C (< 50 mg/dL for women, and < 40 mg/dL for men) or drug treatment for reduced HDL-C; (iv) elevated blood pressure (systolic > 130 and/or diastolic > 85 mmHg) or antihypertensive drug treatment; and (v) elevated fasting glucose (> 100 mg/dl), drug treatment of elevated glucose or diabetes mellitus. This trial (ISRCTN89898870) PREDIMED-Plus aims to assess the effect of a 6-year weight loss intervention program based on an energy-restricted traditional Mediterranean diet (erMedDiet), physical activity (PA) promotion, and behavioral support, in comparison with a usual care intervention only with energy-unrestricted Mediterranean diet without any advice to increase PA or losing weight on a composite of CV events. The study protocol includes more detailed information and is available in previous publications (7) and at the website (8). All participants provided written informed consent, and the study protocol and procedures were approved according to the ethical standards of the Declaration of Helsinki by all the participating institutions.
Among the 6,874 participants randomized between 2013 and 2016 in this trial, a sub-sample of participants from 3 recruiting centers prospectively and systematically underwent TTE at baseline and follow-up (Figure 1). This study population comprised 565 participants with available baseline TTE recruited in University of Navarra-Preventiva (Navarra, Spain), Hospital Universitario Araba (Vitoria, Spain), and Hospital Universitari Son Espases (Mallorca, Spain).
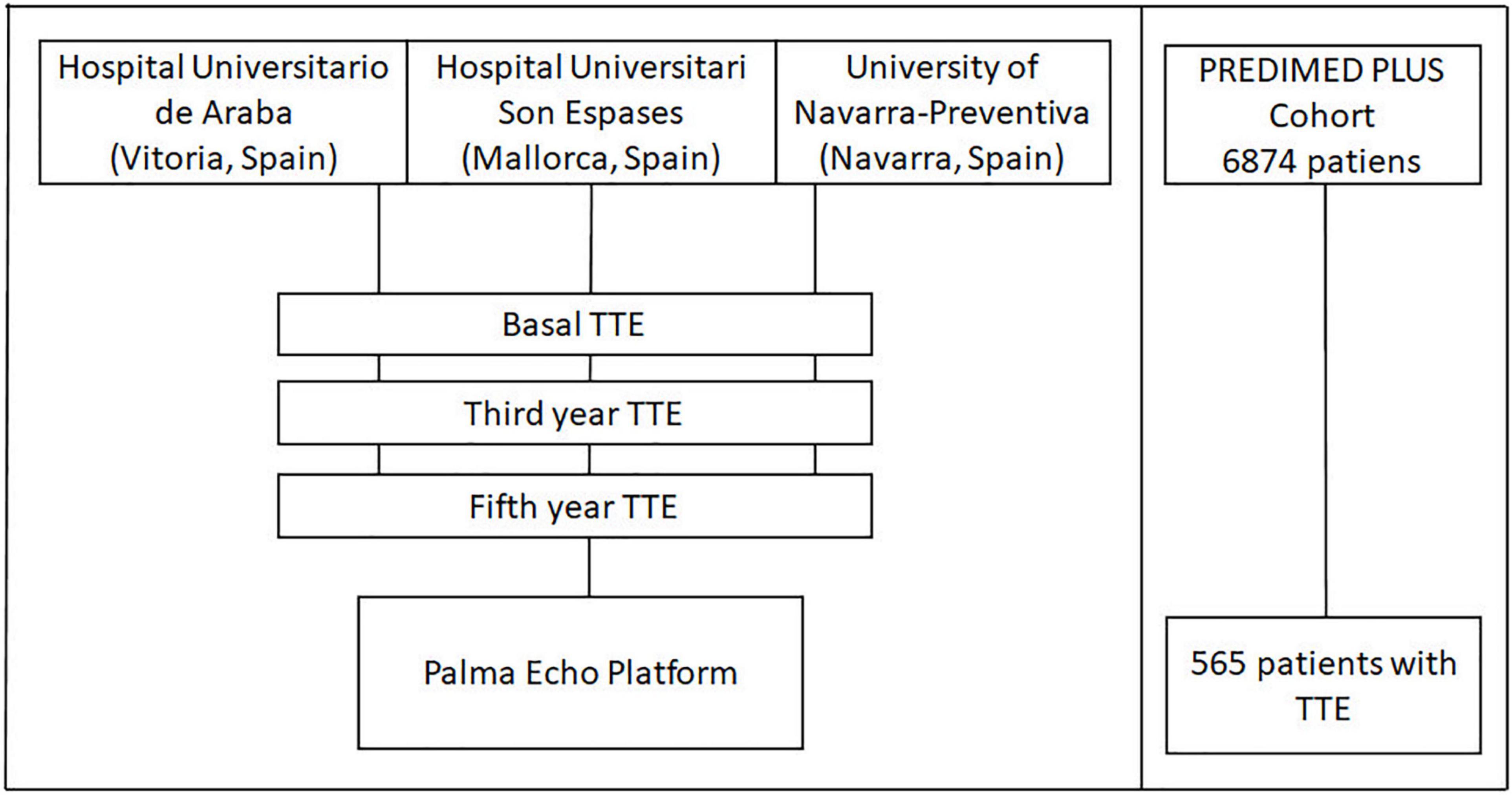
Figure 1. Study outline. TTE, Transthoracic echocardiography.
TTE tests will be used to longitudinally assess structural and functional features of the heart. TTE images were taken for each participant at baseline, and are expected to be taken at two timepoints of the follow-up (year 3 and 5 after the study entry, Figure 1). Data acquisition is performed according to the standards of the European Association of Echocardiography and the American Society of Echocardiography (ASE). Emphasis will be put into following the guidelines for evaluation of left atrial structure and function. Damage in left atrium might be the substrate for the development of atrial fibrillation (AF), among other disarrangements related to MetS. TTEs will be performed at each site following a standardized protocol (Table 1).
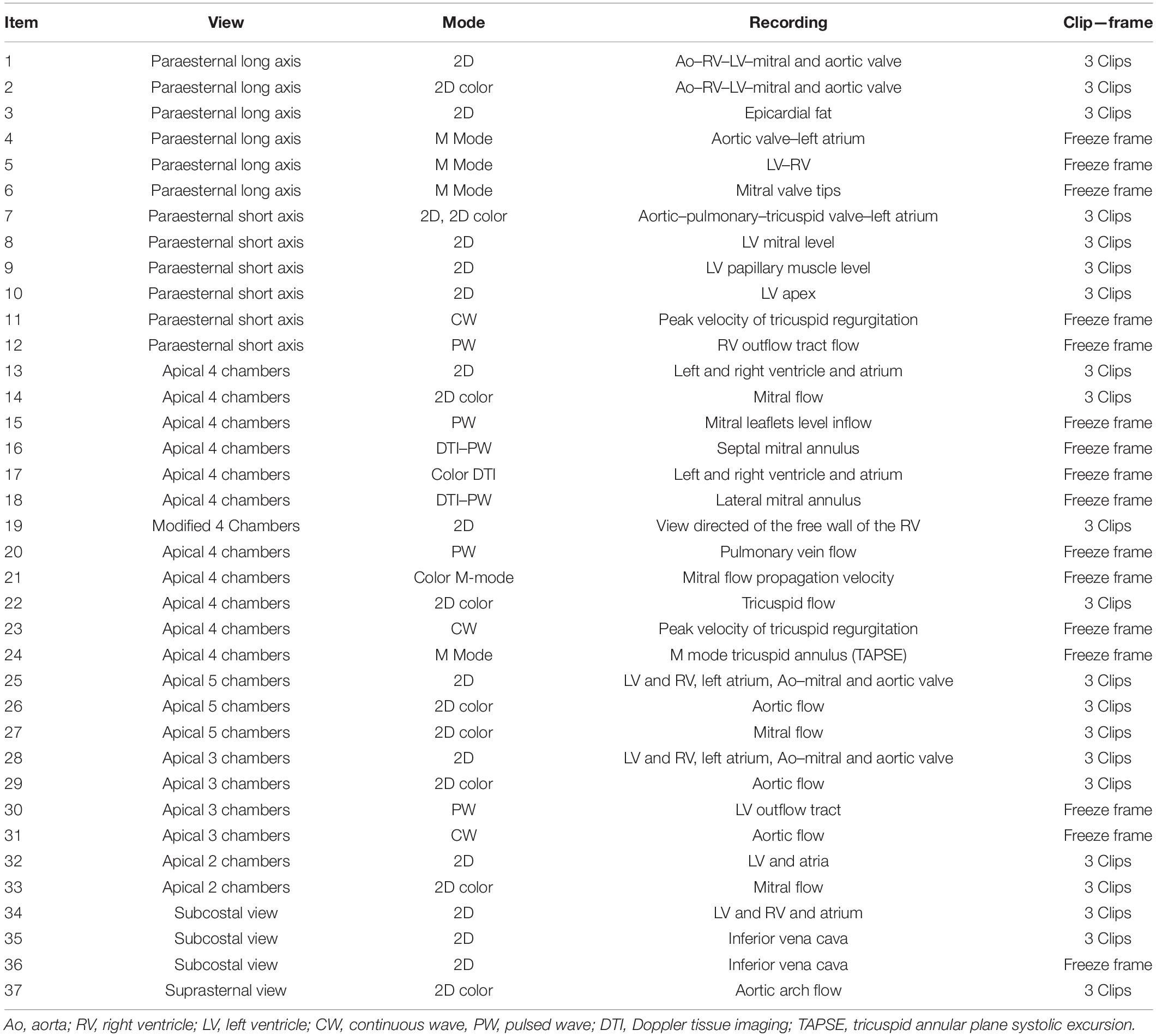
Table 1. Image acquisition protocol.
The PEP will evaluate and measure all TTEs performed by the 3 participating centers using the Echopac version 204 post-processing tool, obtaining video clips of three beats per 2D projection and 15 s in the M-mode studies and Doppler and according to the protocol in Table 1. The CORELAB readers are two independent experts not involved in obtaining the images in any of the study sites, but only evaluating them. Primary and derived measures will be collected systematically, following a standardized protocol (Table 2).
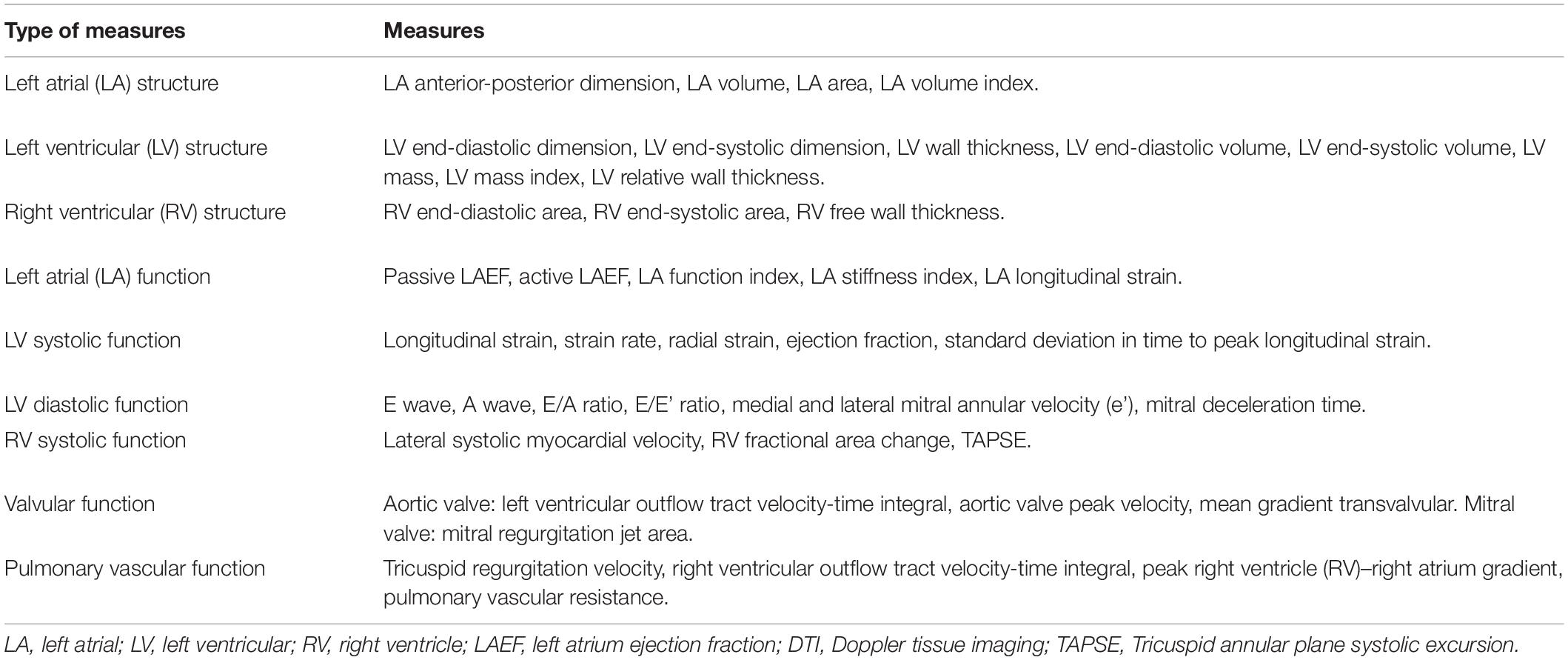
Table 2. Transthoracic echocardiography measures.
Quality of the image-records will be categorized as good, fair or poor. Good quality is when the structure or record under evaluation can be adequately identified and measured in all its aspects, whereas fair quality happens when the structures can be correctly observed, but some measurements are hard to obtain. Poor quality means that the study does not reach the standards to obtain reliable measurements.
Vivid E9 is be used to record TTE tests. Vivid E9 is a diagnostic ultrasound machine for cardiac diagnosis with Doppler physics and instrumentation, transducers are single crystal and matrix array. The following techniques are used to record images:2D and color imaging optimization, tissue Doppler, 2D strain/speckle tracking and Automated Function Imaging (AFI) 3D/4D Volume cardiovascular ultrasound technology. All images are transferred to a common laboratory image repository in the PEP core lab, to be evaluated by the two independent echo evaluators. Post-process analysis is performed with Echopac software, whereas CardioWorflow of General Electric is used to generate an easy-to-export data set for subsequent data management and statistical analyses.
Weight, height and blood pressure are routinely taken at the time of the TTE. Special attention would require the ECG signal (positive QRS). Imaging is recorded in unforced (non-Valsalva) apnea to avoid respiratory movement artifacts. For each view, ≥ 3 full cardiac cycles must be recorded. Raw data will be stored to allow for full post-processing capabilities (Echopac software) for 2D imaging. It is very important to maintain a frame rate of 60–90 frames per second (strain analysis). Color Doppler imaging Doppler Nyquist limit is set at 64 cm/s. For 2D Color TDI imaging is optimized with both imaging depth and sector width to maintain the frame rate as higher as possible. When recording time related display diagnostic techniques (e.g., spectral Doppler, M mode, DTI) the sweep speed used is 25–50 mm/s (not 100) to permit storing as many bytes as possible. If a relevant heart disease is documented during the echocardiographic evaluation (incidental finding), the protocol might be modified to further evaluate the participant. The Image Acquisition Protocol is presented in Table 2, and some illustrations are shown in Figure 2.
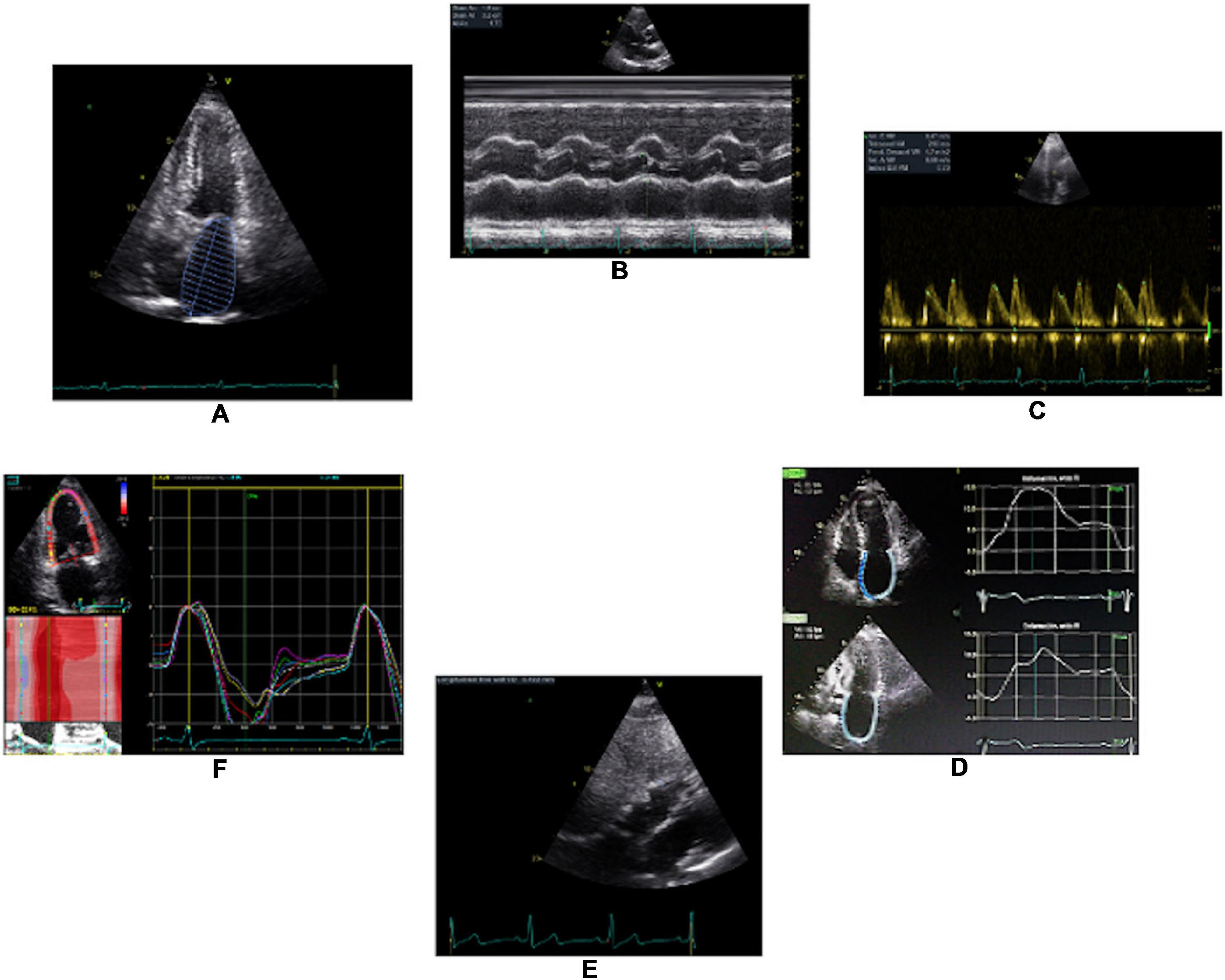
Figure 2. Illustration of some TTE parameters that will be recorded throughout a standardized protocol. (A), left atrial size; (B), left ventricle thickness; (C), E and A waves; (D), left atrium strain; (E), right ventricular thickness; and (F), left ventricular longitudinal strain.
In addition to the imagining data, some clinical data is needed to complete the assessment of participants with MetS. Information on age, sex, educational levels, medical history and family history was collected at baseline. Anthropometric evaluations (weight, height, waist circumference) were measured according to the PREDIMED-Plus protocol. BMI was calculated as weight (kg) divided by the square of height (m2). Further clinical data was collected at baseline, whereas additional data are becoming yearly available, such as food frequency questionnaires, adherence to the Mediterranean diet (surveyed with a 17-item questionnaire), physical activity measurements, blood pressure and electrocardiogram, cognitive neuropsychological tests (six tests every 2 years), the SF-36 (36-item) quality of life questionnaire (baseline and years 1, 3, 5, and 7), and three Psychopathological questionnaires. Further details can be found elsewhere (8). Moreover, some samples, such as plasma, serum, morning spot urine, DNA, and nails, are collected at baseline and years 1, 3, 5, and 7 of follow-up.
The first hypotheses that is going to be tested through this platform will be the potential benefit of lifestyle interventions (erMedDiet, PA promotion and behavioral support) on the AF substrate in the subcohort of 565 participants with MetS from the PREDIMED-Plus trial. We hypothesize that the study intervention will avoid left atrial volume increase and improve left atrial function (assessed with novel measures of left atrial strain). Longitudinal TTE changes will be collected over a period of 5 years in participants from both the control and the intervention arm.
In addition to this initial hypothesis using randomized data, other broader hypotheses will be tested using the TTE data collected in the PEP. The overall aim of these subsequent observational studies will be to assess the association between the individual components of the MetS and some relevant TTE parameters measured either at a cross-sectional-level (baseline), or at longitudinal-level (5 years). Changes or alterations in the cardiac anatomy and function will shed light in the pathophysiology underlying the MetS. This evidence may be useful for the early detection of subjects with very high CV risk who might benefit from an early or intensive intervention.
STATA software version 15.1 (Stata Corp., College Station, TX, United States) and GraphPad Prism version 6.00 (GraphPad Software, La Jolla California, United States) will be used to perform the analyses and produce the graphs, respectively. The results will be adequately reported according to the research reporting guidelines for observational studies, or randomized controlled trials (the STROBE or CONSORT statement, respectively) (9, 10). The interpretation of results will emphasize estimates of effect, precision of those estimates (confidence intervals), and clinical significance rather than p-values and statistical significance (11).
The PEP is a highly coordinated network that has been built up to evaluate the underlying structural and functional cardiac substrate of participants with MetS. Although the information provided by TTEs can be used to answer many research questions, this platform is going to initially test for the potential benefit of lifestyle interventions (erMedDiet, PA promotion, and behavioral support) on the AF substrate in a subcohort of 565 participants with MetS from the PREDIMED-PLUS trial. In addition to this study using randomized data, further subsequent studies will focus on the impact of the individual components of the MetS (e.g., hypertension) on relevant echo markers based, regardless of the interventional allocation. Eventually, clinical outcomes, such as incident AF, ischemic heart disease, and heart failure, will become available to assess the prognostic importance of these echo markers. Given that the individual components of the MetS are risk factors for the development of ischemic heart disease and ventricular systolic and diastolic dysfunction, it is expected that participants with MetS will progressively experience changes in both the coronary arteries and the heart structure, which would precede the development of these clinical outcomes (12). Hence, the longitudinal use of TTE markers to better phenotype and screen patients with MetS represents a good opportunity to both understand the underlying mechanisms of myocardial impairment as well as to identify those patients with MetS who might benefit from an early preventive intervention (13).
The atrium has been traditionally evaluated in its morphological dimension (e.g., atrial volume). In our study, we included novel parameters that may provide relevant information, like left atrial strain and atrial ejection fraction. Traditionally, the function of the left atrium has been studied with parameters surrogated to blood flow during atrial contraction such as the peak A wave velocity or the A wave velocity time integral (14). Furthermore, these parameters are applicable only in sinus rhythm. Left atrial strain represents a direct measure of atrial function and has already been shown to alter earlier than atrial volume in healthy aging (14).
The initial hypotheses that will be tested through this platform will be the potential benefit of lifestyle interventions on the AF substrate in a population with MetS. AF is a common cardiac arrhythmia associated with an increased risk of stroke, heart failure, dementia, and cardiovascular mortality (15, 16). In a large American study, 22% of visits to the emergency department were for AF, and this figure has increased by 30.7% from 2007 to 2014 (17). Current treatments for AF, including antiarrhythmics, oral anticoagulants, and catheter ablation, have limited efficacy and involve significant risks, highlighting the need for prevention strategies (16). Unfortunately, there is little evidence of effective interventions preventing the onset of AF. Previous observational studies have shown that increased body weight is a major risk factor for the development of AF (18). There is an increasing body of evidence suggesting that this association might be mediated through a number of pathways, including alterations of the epicardial adipose tissue biology, activation of inflammatory pathways, development of structural cardiac remodeling, as well as atrial fibrosis. Importantly, weight loss in patients with AF has been associated with a slower progression from paroxysmal to persistent AF, and with a regression from persistent to paroxysmal AF (19). Data from the PREDIMED study has shown that individuals taking a Mediterranean diet enriched in extra-virgin olive oil had lower risk of AF than those receiving a control diet (20). Changes in the atrial substrate are likely to be responsible for the association between obesity, MetS and AF (21, 22), and imaging tests might be helpful to understand the pathophysiological mechanisms underlying the effect of diet and other lifestyle interventions, such as the PREDIMED-Plus intervention (a weight loss intervention program based on an erMedDiet, PA promotion and behavioral support), in AF-related outcomes. The potential effect weight loss on AF has been also studied in patients who already had AF. The ARREST-AF cohort study found that CVRF management, including weight loss, in AF patients undergoing ablation was associated with lower risk of recurrence (23). Using the LEGACY cohort, Ninomiya et al. reported that long-term (> 2 years) weight loss was associated with arrhythmia-free survival and significant changes in echocardiography-assessed left atrial structure (24). Given that these studies were performed on patients with AF, they were unable to address the role that weight loss interventions would have in the primary prevention of AF. The PEP will be suitable to response the scientific question about the potential efficacy of an intensive lifestyle intervention on the AF substrate, measured by TEE.
Although left ventricular ejection fraction and left atrial volume are commonly used to evaluate the mechanics of ventricular contraction, they have some limitations. One of the strongest points of our study is the systematic evaluation of left ventricular longitudinal strain. The heart is a single muscular band that folds over itself in the form of a double spiral, generating three different types of fibers (longitudinal, oblique, and transverse, located in subendocardium, subepicardium, and between both of them, respectively). In ventricular systole, subepicardial, and subendocardial fibers contract at different times and in the opposite direction to achieve an efficient contraction (25). Left ventricular longitudinal strain is a function parameter of subendocardial muscle fibers, which are the first fibers to be affected in systolic ventricular dysfunction (26). Hence, left ventricular longitudinal strain is useful for the detection of subclinical systolic dysfunction, and has been shown to be a sensitive, reproducible parameter with less variability than the left ventricular ejection fraction (27). The information provided by left ventricular longitudinal strain will be useful to phenotype the myocardium in participants with MetS.
PEP will ensure a well-structured platform interpreting echo data in a reliable and reproducible manner. Previous experiences from other randomized studies, such as the ISCHEMIA (International Study of Comparative Health Effectiveness with Medical and Invasive Approaches) and the PARTNER I (Placement of Aortic Transcatheter Valves) trials, have shown the usefulness of setting an echocardiography Core labs to reduce variability and obtain representative and comparable values across participants over time (28–30).
This is a nationwide randomized controlled study, and caution should be taken when extrapolating our potential findings to a real-world population. The quality of the TTE acquisition does not only rely on the evaluator, but on the window of participating subjects, which is particularly challenging in a population with a high body mass index and MetS. Other techniques, such as cardiac magnetic resonance, might be more precise to define tissue characterization and other myocardial parameters (31). Moreover, other echo parameters might be studied in post hoc analyses, such as the maximal epicardial adipose tissue (EAT) thickness at the Rindfleisch fold, measured from parasternal long axis 2D imaging at diastole. Sample size was calculated to estimate the effects of a lifestyle intervention on echo parameters known to be associated with later risk of AF in a sub-sample, taking into account the longitudinal assessment (repeated measures) and multiple testing of echocardiographic parameters. Any association between non-randomized data (such as echo parameters) and CV events (e.g., AF) would be hypothesis-generating.
In this article, we described the protocol of a central echocardiography laboratory (PEP) to assess the myocardial substrate of participants with overweight or obesity and MetS. Repeated TTE performed at three study sites will be used to evaluate 5-year changes in the cardiac structure and function in a group of 565 individuals participating in a randomized trial of a lifestyle intervention for the primary prevention of cardiovascular disease. Planned analyses will involve evaluating the effect of the lifestyle intervention on cardiac structure and function, and the association of the MetS and its components with changes in cardiac structure and function. Particular emphasis will be placed on evaluating parameters of left atrial structure and function, which have received little attention in previous investigations.
DR, MF, AA, and CF-P: conception and design. LL, XR, and DR: drafting of the article. AA, ET, ÁA-G, and DR: obtaining of funding. LL, ÁA-G, ET, EF, MN, CM-L, RR, and LT-S: collection and assembly of data. All authors: critical revision and final approval of the article.
Research reported in this publication was supported by the National Heart, Lung, and Blood Institute of the National Institutes of Health under Award Numbers R01HL137338 and K24HL148521, and administrative supplement to promote diversity 3R01HL137338-03S1. This work was supported by the official Spanish Institutions for funding scientific biomedical research, CIBER Fisiopatología de la Obesidad y Nutrición (CIBEROBN) and Instituto de Salud Carlos III (ISCIII), through the Fondo de Investigación para la Salud (FIS), which was co-funded by the European Regional Development Fund (PI13/00673, PI13/00492, PI13/00272, PI13/01123, PI13/00462, PI13/00233, PI13/02184, PI13/00728, PI13/01090, PI13/01056, PI14/01722, PI14/00636, PI14/00618, PI14/00696, PI14/01206, PI14/01919, PI14/00853, PI14/01374, PI14/00972, PI14/00728, PI14/01471, PI16/00473, PI16/00662, PI16/01873, PI16/01094, PI16/00501, PI16/00533, PI16/00381, PI16/00366, PI16/01522, PI16/01120, PI17/00764, PI17/01183, PI17/00855, PI17/01347, PI17/00525, PI17/01827, PI17/00532, PI17/00215, PI17/01441, PI17/00508, PI17/01732, PI17/00926, PI19/00957, PI19/00386, PI19/00309, PI19/01032, PI19/00576, PI19/00017, PI19/01226, PI19/00781, PI19/01560, PI19/01332, PI20/01802, PI20/00138, PI20/01532, PI20/00456, PI20/00339, PI20/00557, PI20/00886, and PI20/01158); the Especial Action Project entitled: Implementación y evaluación de una intervención intensiva sobre la actividad física Cohorte PREDIMED-Plus; the European Research Council (Advanced Research Grant 2014–2019; agreement #340918); the Recercaixa (number 2013ACUP00194); grants from the Consejería de Salud de la Junta de Andalucía (PI0458/2013, PS0358/2016, PI0137/2018); the PROMETEO/2017/017 grant from the Generalitat Valenciana; the SEMERGEN grant; none of the funding sources took part in the design, collection, analysis, interpretation of the data, or writing the report, or in the decision to submit the manuscript for publication.
The content was solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Lindsay RS, Howard BV. Cardiovascular risk associated with the metabolic syndrome. Curr Diab Rep. (2004) 4:63–8. doi: 10.1007/s11892-004-0013-9
2. Rossello X, Fuster V, Oliva B, Sanz J, Fernández Friera LA, López-Melgar B, et al. Association between body size phenotypes and subclinical atherosclerosis. J Clin Endocrinol Metab. (2020) 105:3734–44. doi: 10.1210/clinem/dgaa620
3. Sattar N, McConnachie A, Shaper AG, Blauw GJ, Buckley BM, de Craen AJ, et al. Can metabolic syndrome usefully predict cardiovascular disease and diabetes? Outcome data from two prospective studies. Lancet. (2008) 371:1927–35. doi: 10.1016/S0140-6736(08)60602-9
4. Alberti KGMM, Eckel RH, Grundy SM, Zimmet PZ, Cleeman JI, Donato KA, et al. Harmonizing the metabolic syndrome: a joint interim statement of the international diabetes federation task force on epidemiology and prevention; national heart, lung, and blood institute; American heart association; world heart federation; international. Circulation. (2009) 120:1640–5. doi: 10.1161/CIRCULATIONAHA.109.192644
5. Koh KK, Han SH, Quon MJ. Inflammatory markers and the metabolic syndrome: insights from therapeutic interventions. J Am Coll Cardiol. (2005) 46:1978–85. doi: 10.1016/j.jacc.2005.06.082
6. Pericas P, Mas-Lladó C, Ramis-Barceló MF, Valadrón I, Noris Mora M, Pasamar Márquez L, et al. Impact of sacubitril-valsartan treatment on diastolic function in patients with heart failure and reduced ejection fraction. High Blood Press Cardiovasc Prev. (2021) 28:167–75. doi: 10.1007/s40292-021-00437-x
7. Martínez-González MA, Buil-Cosiales P, Corella D, Bulló M, Fitó M, Vioque J, et al. Cohort profile: design and methods of the PREDIMED-Plus randomized trial. Int J Epidemiol. (2019) 48:387–8o. doi: 10.1093/ije/dyy225
8. Predimed Plus. Estudio de la Dieta Mediterránea. (2022). Available online at: https://www.predimedplus.com/en/ (accessed March 24, 2022).
9. von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP. The strengthening the reporting of observational studies in epidemiology (STROBE) statement: guidelines for reporting observational studies. Ann Intern Med. (2007) 147:573–7.
10. Schulz KF, Altman DG, Moher D, Consort Group. CONSORT 2010 statement: updated guidelines for reporting parallel group randomised trials. BMJ. (2010) 340:c332. doi: 10.1136/bmj.c332
11. Pocock SJ, Rossello X, Owen R, Collier TJ, Stone GW, Rockhold FW. Primary and secondary outcome reporting in randomized trials: JACC state-of-the-art review. J Am Coll Cardiol. (2021) 78:827–39. doi: 10.1016/J.JACC.2021.06.024
12. Rossello X, González-Del-Hoyo M. Survival analyses in cardiovascular research, part I: the essentials. Rev Española Cardiol. (2022) 75:67–76. doi: 10.1016/j.rec.2021.06.003
13. Sposato LA, Chaturvedi S, Hsieh C-Y, Morillo CA, Kamel H. Atrial fibrillation detected after stroke and transient ischemic attack: a novel clinical concept challenging current views. Stroke. (2022) 53:e94–103. doi: 10.1161/STROKEAHA.121.034777
14. Boyd AC, Richards DAB, Marwick T, Thomas L. Atrial strain rate is a sensitive measure of alterations in atrial phasic function in healthy ageing. Heart. (2011) 97:1513–9. doi: 10.1136/heartjnl-2011-300134
15. Raposeiras-Roubín S, Abu-Assi E, Lizancos Castro A, Barreiro Pardal C, Melendo Viu M, Cespón Fernández M, et al. Nutrition status, obesity and outcomes in patients with atrial fibrillation. Rev Esp Cardiol (Engl Ed). (2022). doi: 10.1016/j.rec.2022.01.006 [Epub ahead of print].
16. Hindricks G, Potpara T, Dagres N, Arbelo E, Bax JJ, Blomström-Lundqvist C, et al. 2020 ESC guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European association for cardio-thoracic surgery (EACTS): the task force for the diagnosis and management of atrial fibrillation of the Europe. Eur Heart J. (2021) 42:373–498. doi: 10.1093/eurheartj/ehaa612
17. Rozen G, Hosseini SM, Kaadan MI, Biton Y, Heist EK, Vangel M, et al. Emergency department visits for atrial fibrillation in the United States: trends in admission rates and economic burden from 2007 to 2014. J Am Heart Assoc. (2018) 7:e009024. doi: 10.1161/JAHA.118.009024
18. Lavie CJ, Pandey A, Lau DH, Alpert MA, Sanders P. Obesity and atrial fibrillation prevalence, pathogenesis, and prognosis: effects of weight loss and exercise. J Am Coll Cardiol. (2017) 70:2022–35. doi: 10.1016/j.jacc.2017.09.002
19. Middeldorp ME, Pathak RK, Meredith M, Mehta AB, Elliott AD, Mahajan R, et al. PREVEntion and regReSsive effect of weight-loss and risk factor modification on atrial fibrillation: the REVERSE-AF study. Europace. (2018) 20:1929–35. doi: 10.1093/europace/euy117
20. Martínez-González MÁ, Toledo E, Arós F, Fiol M, Corella D, Salas-Salvadó J, et al. Extravirgin olive oil consumption reduces risk of atrial fibrillation: the PREDIMED (prevención con dieta mediterránea) trial. Circulation. (2014) 130:18–26. doi: 10.1161/CIRCULATIONAHA.113.006921
21. Reddy YNV, Anantha-Narayanan M, Obokata M, Koepp KE, Erwin P, Carter RE, et al. Hemodynamic effects of weight loss in obesity: a systematic review and meta-analysis. JACC Heart Fail. (2019) 7:678–87. doi: 10.1016/j.jchf.2019.04.019
22. Lim DJ, Ambale-Ventakesh B, Ostovaneh MR, Zghaib T, Ashikaga H, Wu C, et al. Change in left atrial function predicts incident atrial fibrillation: the multi-ethnic study of atherosclerosis. Eur Heart J Cardiovasc Imaging. (2019) 20:979–87. doi: 10.1093/ehjci/jez176
23. Pathak RK, Middeldorp ME, Lau DH, Mehta AB, Mahajan R, Twomey D, et al. Aggressive risk factor reduction study for atrial fibrillation and implications for the outcome of ablation: the ARREST-AF cohort study. J Am Coll Cardiol. (2014) 64:2222–31. doi: 10.1016/j.jacc.2014.09.028
24. Ninomiya T. Japanese legacy cohort studies: the Hisayama study. J Epidemiol. (2018) 28:444–51. doi: 10.2188/jea.JE20180150
25. Torrent Guasp F. [Agonist-antagonist mechanics of the descendent and ascendent segments of the ventricular myocardial band]. Rev Esp Cardiol. (2001) 54:1091–102. doi: 10.1016/s0300-8932(01)76456-1
26. Collier P, Phelan D, Klein A. A test in context: myocardial strain measured by speckle-tracking echocardiography. J Am Coll Cardiol. (2017) 69:1043–56. doi: 10.1016/j.jacc.2016.12.012
27. Park JJ, Park J-B, Park J-H, Cho G-Y. Global longitudinal strain to predict mortality in patients with acute heart failure. J Am Coll Cardiol. (2018) 71:1947–57. doi: 10.1016/j.jacc.2018.02.064
28. Kataoka A, Scherrer-Crosbie M, Senior R, Gosselin G, Phaneuf D, Guzman G, et al. The value of core lab stress echocardiography interpretations: observations from the ISCHEMIA trial. Cardiovasc Ultrasound. (2015) 13:47. doi: 10.1186/s12947-015-0043-2
29. Douglas PS, Waugh RA, Bloomfield G, Dunn G, Davis L, Hahn RT, et al. Implementation of echocardiography core laboratory best practices: a case study of the PARTNER I trial. J Am Soc Echocardiogr. (2013) 26:348–58.e3. doi: 10.1016/j.echo.2013.01.013
30. Barnhart HX, Yow E, Crowley AL, Daubert MA, Rabineau D, Bigelow R, et al. Choice of agreement indices for assessing and improving measurement reproducibility in a core laboratory setting. Stat Methods Med Res. (2016) 25:2939–58. doi: 10.1177/0962280214534651
31. Rossello X, Lopez-Ayala P, Fernández-Jiménez R, Oliver E, Galán-Arriola C, de Molina-Iracheta A, et al. R2 prime (R2’) magnetic resonance imaging for post-myocardial infarction intramyocardial haemorrhage quantification. Eur Heart J Cardiovasc Imaging. (2020) 21:1031–8. doi: 10.1093/ehjci/jez306
Keywords: echocardiagraphy, core laboratory, randomized clinical trial, metabolic syndrome, atrial fibrillation, atrial function
Citation: López L, Rossello X, Romaguera D, Alonso-Gómez ÁM, Toledo E, Fortuny E, Noris M, Mas-Lladó C, Fiol M, Ramallal R, Tojal-Sierra L, Alonso A and Fernandez-Palomeque C (2022) The Palma Echo Platform: Rationale and Design of an Echocardiography Core Lab. Front. Cardiovasc. Med. 9:909347. doi: 10.3389/fcvm.2022.909347
Received: 31 March 2022; Accepted: 30 May 2022;
Published: 21 June 2022.
Edited by:
Liza Thomas, University of New South Wales, AustraliaReviewed by:
Valentina Parisi, University of Naples Federico II, ItalyCopyright © 2022 López, Rossello, Romaguera, Alonso-Gómez, Toledo, Fortuny, Noris, Mas-Lladó, Fiol, Ramallal, Tojal-Sierra, Alonso and Fernandez-Palomeque. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Xavier Rossello, Zmpyb3NzZWxsb0Bzc2liLmVz
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.