 Lulu Dai
Lulu Dai Jiawei Xu
Jiawei Xu Yuerong Jiang
Yuerong Jiang Keji Chen
Keji Chen
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Cardiovasc. Med. , 09 June 2022
Sec. Cardiovascular Therapeutics
Volume 9 - 2022 | https://doi.org/10.3389/fcvm.2022.905607
Background: This meta-analysis mainly aimed to compare the impact of prasugrel and ticagrelor on platelet reactivity (PR) in patients with acute coronary syndrome (ACS).
Methods: We searched four electronic databases to identify randomized controlled trials and cohort studies comparing the impact of prasugrel and ticagrelor on PR in patients with ACS. We performed group analyses according to three detection methods, drug dose [loading dose (LD) and maintenance dose (MTD)] and LD effect time, and assessed the robustness of the results through sensitivity analysis.
Results: Twenty-five studies with 5,098 patients were eligible. After LD, the incidence of high on-treatment platelet reactivity (HTPR) of ticagrelor was significantly lower than that of prasugrel within 6–18 h based on vasodilator-stimulated phosphoprotein (VASP) test [RR = 0.25 (0.07, 0.85), P = 0.03], there was no significant difference between ticagrelor and prasugrel in the following results: platelets inhibitory effect within 24–48 h based on VerifyNow P2Y12 (VN) assay (P = 0.11) and VASP test (P = 0.20), and the incidence of HTPR within 2–6 h based on VN assay (P = 0.57) and within 24–48 h based on VN assay (P = 0.46) and VASP test (P = 0.72), the incidence of low on-treatment platelet reactivity (LTPR) within 6–18 h based on VASP test (P = 0.46) and 48 h based on VN assay (P = 0.97) and VASP test (P = 0.73). After MTD, the platelet inhibitory effect of ticagrelor was stronger than that of prasugrel based on VN assay [WMD = −41.64 (−47.16, −36.11), P < 0.00001]and VASP test [WMD = −9.10 (−13.88, −4.32), P = 0.0002], the incidence of HTPR of ticagrelor was significantly lower than that of prasugrel based on VN assay [RR = 0.05 (0.02, 0.16), P < 0.00001], the incidence of LTPR of ticagrelor was significantly higher than prasugrel based on VN assay [RR = 6.54 (4.21, 10.14), P < 0.00001] and VASP test [RR = 2.65 (1.78, 3.96), P < 0.00001], the results of Multiple Electrode Aggregometry (MEA) test was inconsistent with the other two detection methods in platelet inhibitory effect and the incidence of HTPR and LTPR. There was no significant difference between ticagrelor and prasugrel in the following clinical outcomes: all-cause death (P = 0.86), cardiovascular death (P = 0.49), myocardial infarction (P = 0.67), stroke (P = 0.51), target vessel revascularization (P = 0.51), stent thrombosis (P = 0.90), TIMI major bleeding (P = 0.86) and bleeding BARC type ≥ 2 (P = 0.77). The risk of bleeding BARC type 1 of ticagrelor was significantly higher than prasugrel [RR = 1.44 (1.03, 2.02), P = 0.03].
Conclusions: Compared with prasugrel, ticagrelor might have a stronger platelet inhibition effect, with a lower incidence of HTPR and a higher incidence of LTPR and bleeding BARC type 1, while there might be no significant difference in the risk of thrombosis/ischemic, bleeding BARC Type ≥ 2 and TIMI major bleeding. A higher incidence of LTPR might indicate a higher risk of bleeding BARC type 1. The results of VN assay were consistent with that of VASP test, and not with the MEA test.
Systematic Review Registration: https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42022304205, identifier: CRD42022304205.
Platelets are a key part of the occurrence and development of adverse atherosclerotic thrombotic events. Inhibition of platelet function reduces the incidence of cardiovascular adverse events (1). Dual antiplatelet therapy (DAPT), which consists of aspirin and a P2Y12 inhibitor, is currently standard of care for secondary prevention oral antithrombotic therapy in patients with acute coronary syndrome (ACS) and post-percutaneous coronary intervention (2–4). Clopidogrel, a second-generation thienopyridine, is currently most widely used P2Y12 inhibitor in clinical practice (5). However, the pharmacological limitations of clopidogrel mainly include weak platelet inhibition, slow-onset and long duration of action, and significant pharmacodynamic and pharmacokinetic variability among individuals (6). Studies have shown that individuals treated with clopidogrel exhibit a wide range of response variability due to both genetic and non-genetic factors, such as genetic polymorphism, low bioavailability and drug interactions (7, 8). High on-clopidogrel platelet reactivity during DAPT is an important sign of vascular risk, especially stent thrombosis, in patients with ACS (9).
Therefore, new P2Y12 inhibitors, such as ticagrelor and prasugrel, were developed to overcome major pharmacokinetic limitations of clopidogrel. Compared with clopidogrel, ticagrelor and prasugrel are more potent P2Y12 inhibitors, which can produce a more reliable and stronger platelet inhibitory effect and have also shown superiority in the reduction of ischemic vascular events, however, increase the incidence of bleeding events (10–13). Ticagrelor, a cyclopenthyl-triazolopyrimidine, is a reversible antagonist of platelet P2Y12 receptor and does not need to be converted to active metabolites, while prasugrel, a third-generation thiophene pyridine, converts into its active metabolite in vivo and then irreversibly inhibits the p2y12 receptor (6). The antiplatelet mechanism of action of ticagrelor and prasugrel is different, and the responsiveness to platelets is also different, which possibly result in differences in biological and clinical outcomes. Platelet reactivity (PR), highly variable and associated with thrombosis and bleeding events, is a critical pharmacodynamic ingredient in patients receiving antiplatelet therapy (14). Evidence supports the association of high on-treatment platelet reactivity (HTPR) and low on-treatment platelet reactivity (LTPR) with ischemic events and bleeding events, respectively (9, 15).
There have been many meta-analyses comparing adverse clinical outcomes between prasugrel and ticagrelor, such as cardiovascular death, stroke, myocardial infarction and bleeding events, while relatively fewer meta-analyses directly comparing the impact of the two drugs on PR. In the latest meta-analysis comparing the impact of two drugs on PR, only two of the included studies reported HTPR based on VerifyNow P2Y12 (VN) assay, and none reported LTPR based on VN assay (16). In addition, the latest meta-analysis didn't assess robustness of results with high heterogeneity by sensitivity analyses. Currently, few meta-analyses compare the incidence of LTPR in the treatment of prasugrel and ticagrelor. Therefore, we conducted a meta-analysis with a more comprehensive search of literatures, and included randomized controlled trials (RCTs) and cohort studies that comparing the impact of ticagrelor and prasugrel of loading dose (LD) and maintenance dose (MTD) on PR according to VN assay, vasodilator-stimulated phosphoprotein (VASP) test and Multiple Electrode Aggregometry (MEA), further summarized the risk ratios of HTPR and LTPR of the two drugs, to compare the pharmacodynamic differences of that, while clinical outcomes in studies that met the eligibility criteria were also compared.
Our meta-analysis was performed based on the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) and the Meta-analysis of Observational Studies in Epidemiology (MOOSE) reporting guidelines (17, 18). Protocol of this meta-analysis was registered in the International Prospective Register of Systematic Reviews (PROSPERO), registration number: CRD42022304205.
A comprehensive search of PubMed, Embase, Web of Science and Cochrane library was conducted without language restrictions through a combination of Boolean logical operators with keywords, which including “Prasugrel Hydrochloride”, “Hydrochloride, Prasugrel”, “Prasugrel HCl”, “HCl, Prasugrel”, “CS 747”, “747, CS”, “CS-747”, “CS747”, “Prasugrel”, “Efient”, “Effient”, “LY 640315”, “640315, LY”, “LY640315”, “LY-640315”, “Ticagrelor ”, “Brilique”, “AZD 6140”, “AZD6140”, “AZD-6140”, “Brilinta”, “platelet reactivity”, “vasodilator-stimulated phosphoprotein”, “vasodilator stimulated phosphoprotein”, “VerifyNow”, “Verify Now”, “multiple electrode aggregometry ”, “Acute Coronary Syndrome”, “Acute Coronary Syndromes”, “Coronary Syndrome, Acute”, “Coronary Syndromes, Acute”, “Syndrome, Acute Coronary”, “Syndromes, Acute Coronary”, “st segment elevation acute myocardial infarction”, “non-st segment elevation acute myocardial infarction” and “unstable angina” (inception to Apr 26, 2022). We also examined the references of relevant meta-analyses and reviews to track potentially relevant literatures. Table 1 shows the search strategy of PubMed. The search strategies of Embase, Web of science, and Cochrane are detailed in Supplementary Tables 1–3 respectively.
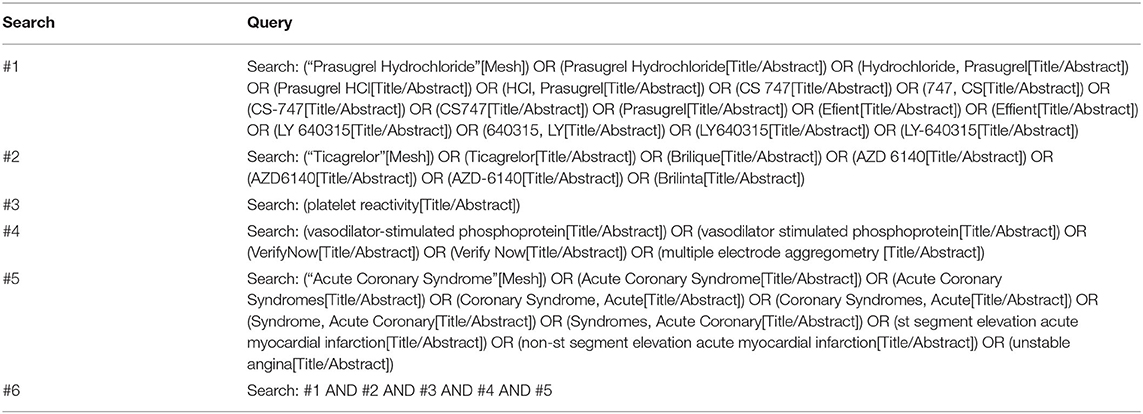
Table 1. PubMed search strategy.
Inclusion criteria: (1) RCTs or cohort studies; (2) comparison of prasugrel and ticagrelor on PR; (3) patients with ACS took aspirin combined with standard doses of prasugrel [180 mg (LD), 90 mg bid (MTD)] or ticagrelor [60 mg (LD), 10 mg bid (MTD)] orally; (4) studies reported one or more of the five outcome measures: P2Y12 response unit (PRU), platelet response index (PRI), the area under the curve of aggregation tracing (AUC), HTPR and LTPR.
Exclusion criteria: (1) duplicate publications; (2) conference abstracts or no full text; (3) no outcome measures of interest; (4) non-standard dosage of ticagrelor or prasugrel; (5) required data was not available.
NoteExpress (version 3.2) was applied to manage retrieved records. Two researchers reviewed titles and abstracts independently of each other based on inclusion and exclusion criteria. Potential literatures that met the criteria required further full-text review. If there were any disagreements on the list of eligible literatures, the list would be reviewed by a third researcher as an arbitrator.
After pilot extraction, two researchers independently extracted the required data and cross-checked it. If data was inconsistent, the researchers needed to carefully review the original literature. Missing data should be supplemented by contacting the original author by email, letter, etc. If relevant data was still not available, the literature would be excluded. The following data was required: first author, publication year, study type, general patient characteristics (sample, mean age and proportion of male), type of patients, Whether PCI was performed, treatment dose, platelet function test time and method, definition of HTPR or LTPR, follow-up time, primary outcome (PRU, PRI, AUC, HTPR, LTPR) and secondary outcome (all-cause death, cardiovascular death, myocardial infarction, stroke, target vessel revascularization, stent thrombosis, TIMI minor or minimal bleeding, TIMI major bleeding, bleeding BARC type 1 and bleeding BARC type ≥ 2).
The literature quality of RCTs was evaluated using the Cochrane handbook (version 6.2) (19), including seven evaluation items: random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective reporting, and other biases, each of which was judged to be at low, uncertain or high risk of bias. The literature quality of cohort studies was evaluated using the Newcastle-Ottawa Scale (NOS) (20), including selection of study groups, comparability of groups, and ascertainment of outcomes (cohort studies) or ascertainment of exposure (case-control studies). According to NOS, we could award a cohort study a maximum of four stars in selection, two stars in comparability, and three stars in outcome. The assessment was carried out independently by two researchers, they would cross-check results and resolve a division of opinion through discussion. If it was difficult to reach an agreement, the arbitration would be held in a third researcher.
We calculated the Cochran's Q-statistic and I2 index to estimate heterogeneity between studies. Fixed effects model was adopted if statistical heterogeneity was absent or low (P values ≥ 0.1 and I2 < 50%). Random effects model was adopted if statistical heterogeneity was significant (P values < 0.1 and/or I2 ≥ 50%). For continuous data and dichotomous data, the weighted mean difference (WMD) with 95% confidence intervals (CI) and risk ratio (RR) with 95% CI was used, respectively. We conducted the sensitivity analysis by changing the effects model and eliminating literature one by one to establish the robustness of the combined results when statistical heterogeneity was significant. If outcomes were documented in at least ten or more literatures, detection of publication bias was carried out. We adopted the funnel plot, Egger' test, and Begg' test in detection of publication bias (21, 22). Data and figures were analyzed and generated using Review Manager software (version 5.4), STATA (version 15.1), and R software (version 4.0.1). All analyses were two-tailed, with an α of 0.05.
According to search strategy, we retrieved 313 studies. After removing duplicate studies, 191 studies remained. We screened titles and abstracts and then excluded 144 studies. We conducted a further full-text review of the remaining 47 studies that might meet the eligibility criteria. Finally, 25 (23–47) studies were identified. Detailed screening process is presented in Figure 1.
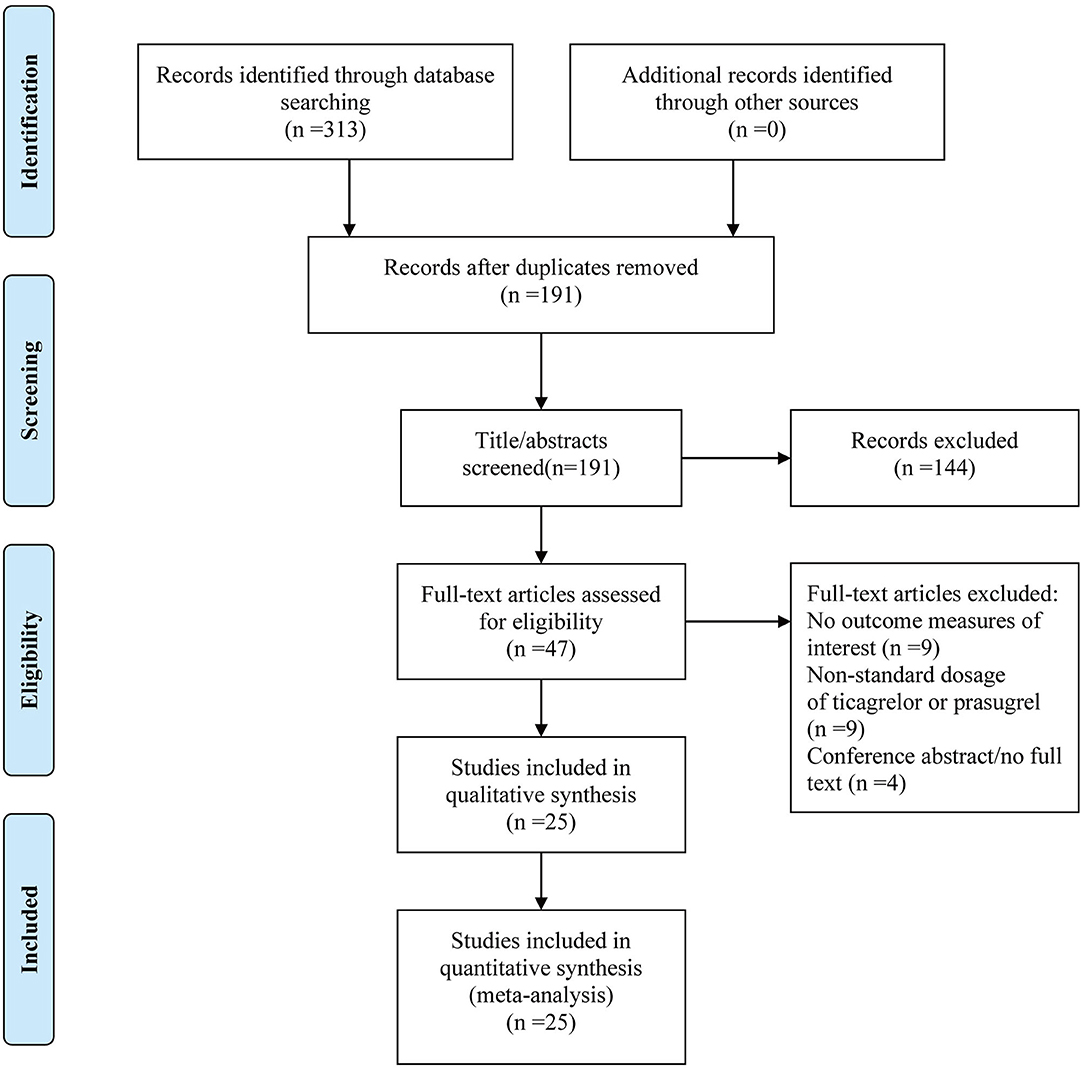
Figure 1. Flow diagram of literature selection and identification.
Among included studies, 11 (25, 26, 29, 30, 33–37, 39, 47) studies were RCTs, 13 (23, 24, 27, 31, 32, 38, 40–46) studies were prospective cohort studies, and one (28) study was retrospective cohort study. The publication dates of 25 studies ranged from 2012 to 2022. The total sample size was 5098 patients, 2600 in ticagrelor group and 2498 in prasugrel group. The patients were all middle-aged and elderly. In terms of Platelet function test method, ten (23, 25, 26, 28–30, 32, 37–39) studies only used VN, six (24, 27, 34–36, 40) studies only used VASP, five studies only used MEA, two (33, 47) studies used VN and VASP, and two (31, 46) studies used VN and MEA. Seven (24, 25, 27, 30, 34, 35, 47) studies only tested platelet function after the treatment of LD. Seventeen (23, 28, 29, 31–33, 36–46) studies only tested platelet function after the treatment of MTD. One (26) study tested platelet function after the treatment of LD and MTD. The characteristic of each selected study is detailed in Table 2.
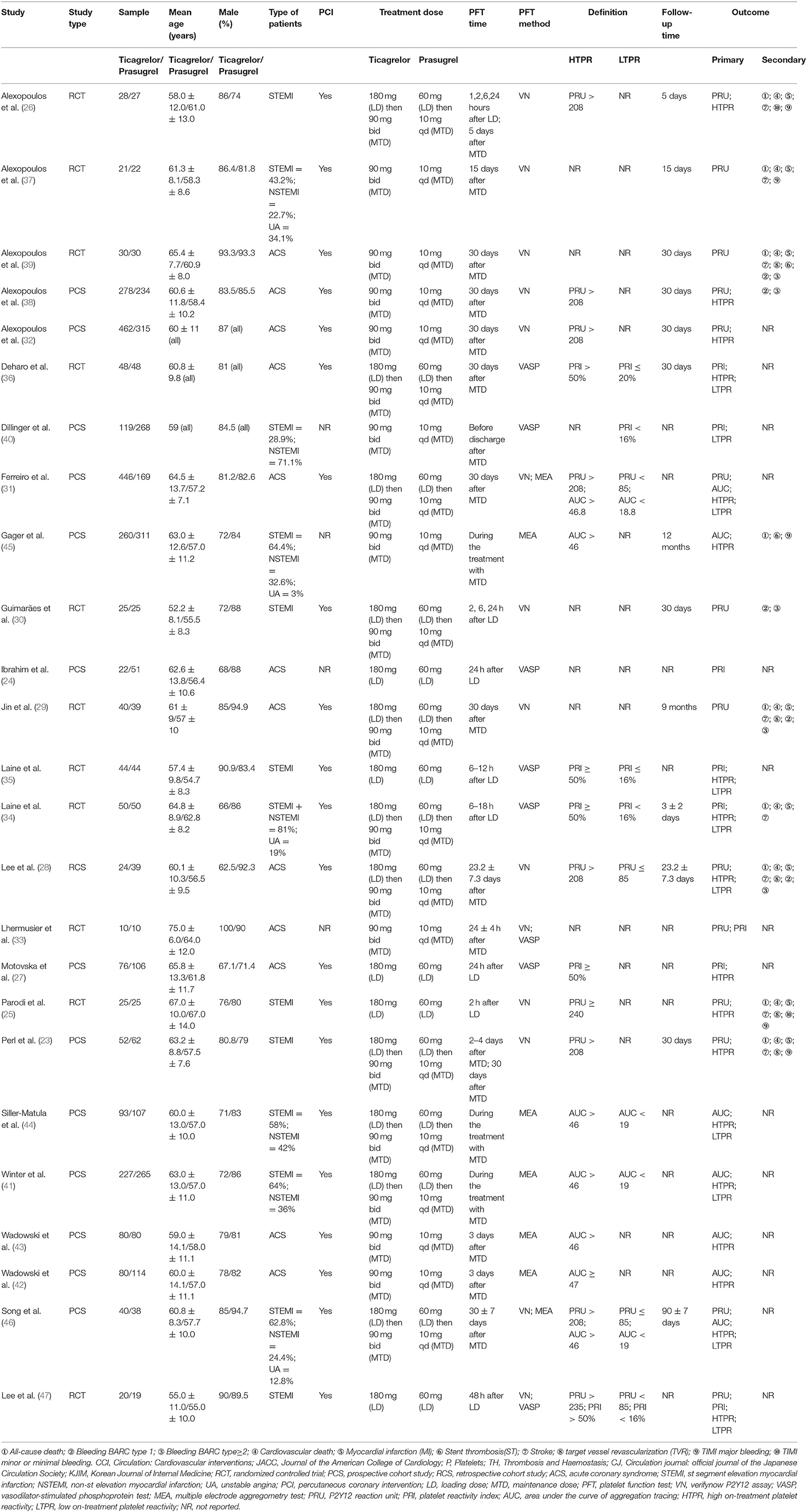
Table 2. Characteristic of selected studies.
The overall methodological quality of 11 RCTs was generally high (Figures 2, 3). Three (26, 37, 39) RCTs showed low risk in seven items. Each RCT showed low risk in random sequence generation and incomplete outcome data. Seven (25, 29, 33–36, 47) RCTs showed unclear risk in allocation concealment. Five (25, 30, 33, 35, 36) RCTs showed unclear risk in blinding. Four (33–36) RCTs showed unclear risk in selective reporting. Two (33, 36) RCTs showed unclear risk in other bias.
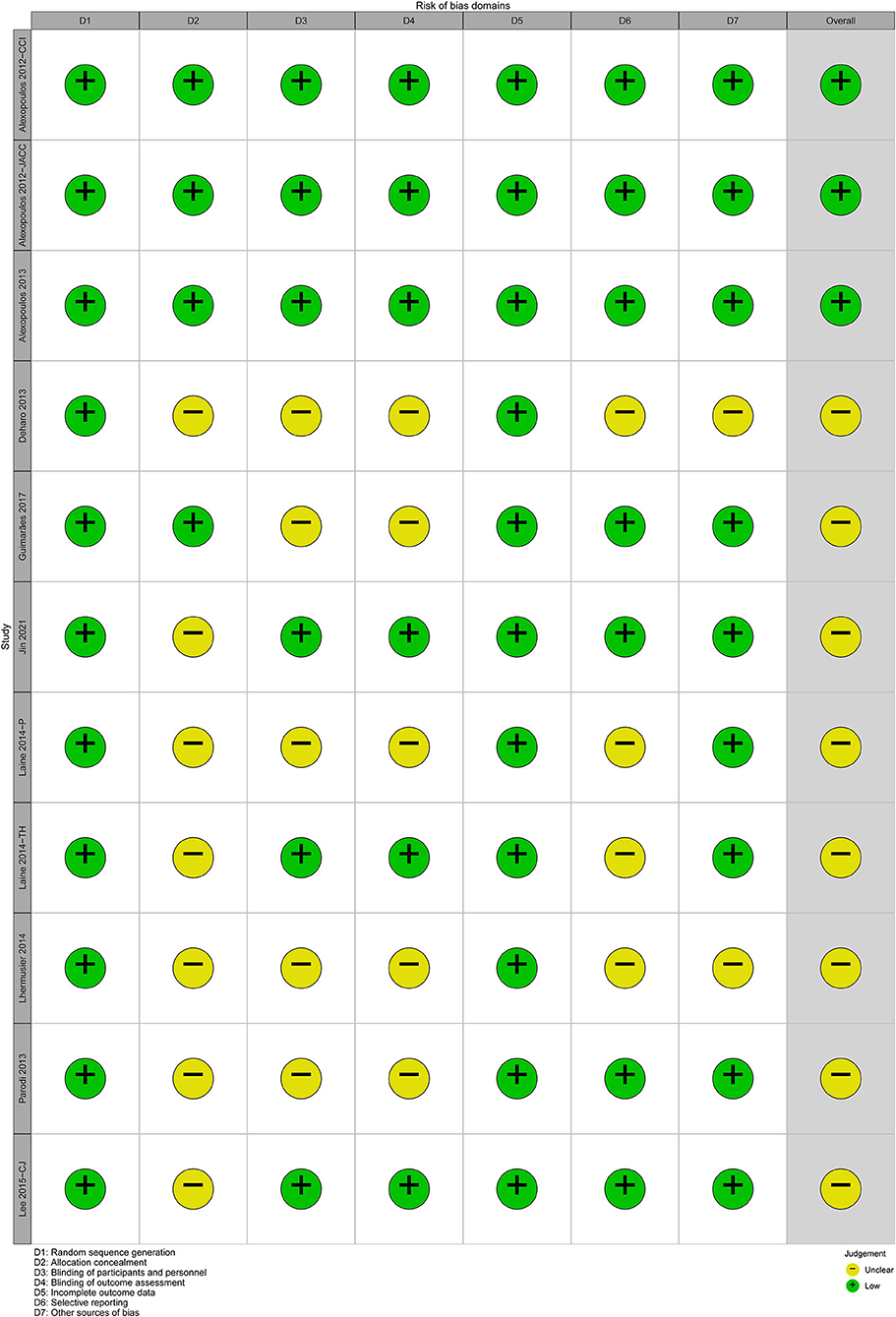
Figure 2. Traffic light plot of risk of bias.
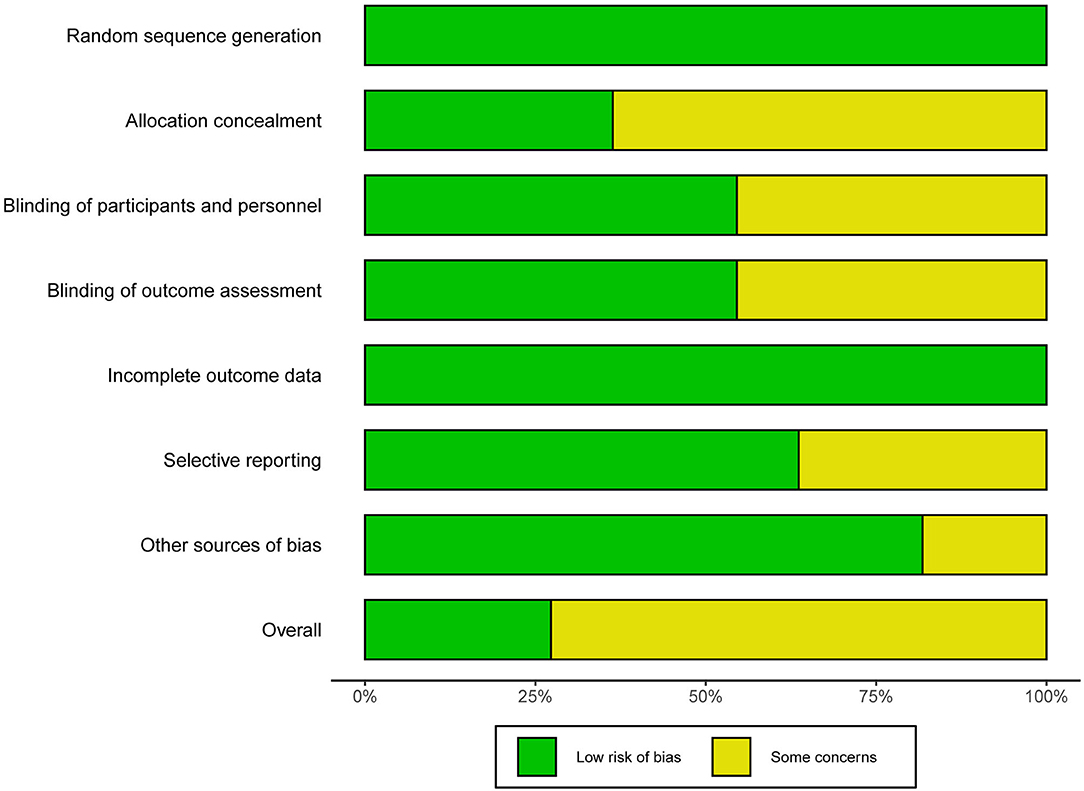
Figure 3. Summary plot of risk of bias.
The overall methodological quality of 14 cohort studies was generally high with the NOS scores ranged from 6 to 9 (Table 3). Six (27, 31, 40, 42–44) studies were rated six stars, three (24, 28, 41) were rated seven stars, four (23, 38, 45, 46) were rated eight stars, and one (32) was rated nine stars.
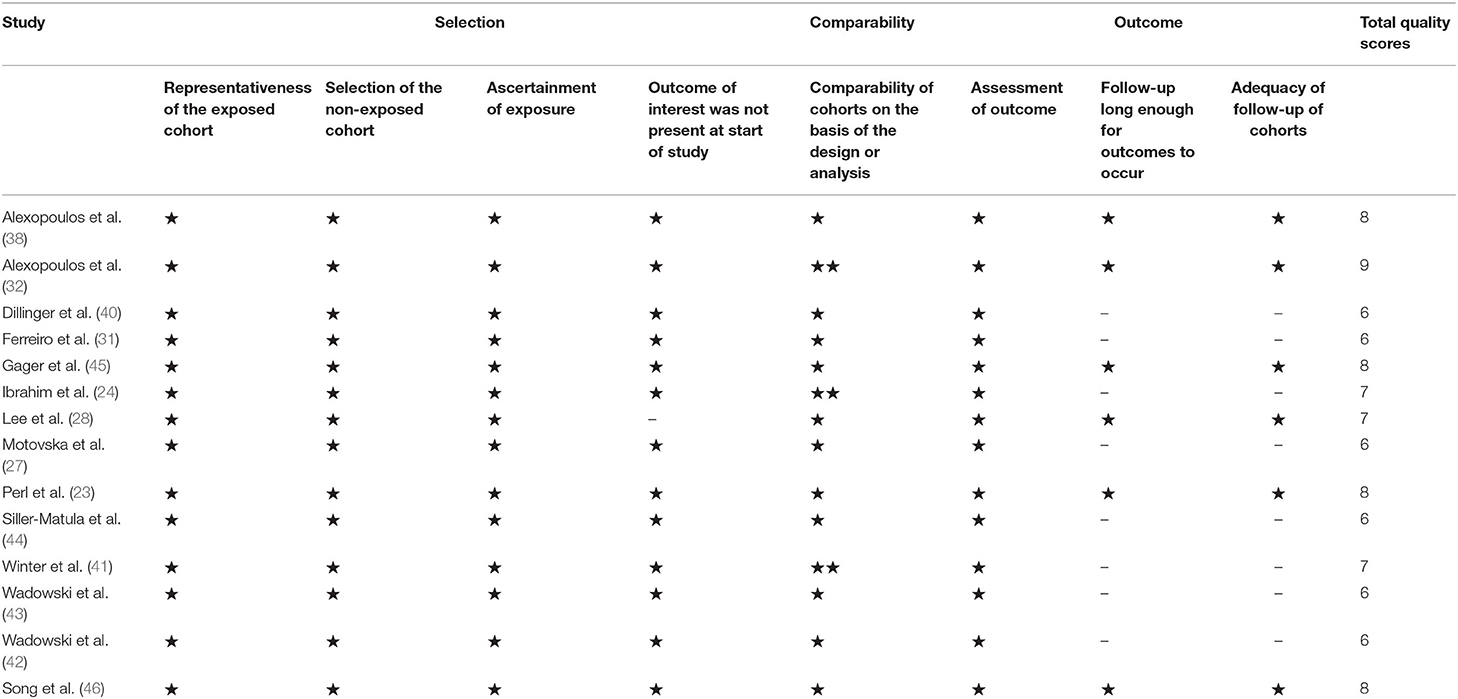
Table 3. Quality assessment of the included cohort studies.
Considering that the LD effect can be separated as early effect and late effect, and the studies containing data of PR after LD used two detection methods (VN and VASP), therefore, we grouped the data of PR after LD according to the detection time (within 2–6 h, within 6–18 h and within 24–48 h) and method. The meta-analysis results of PR after LD were showed in Figure 4.
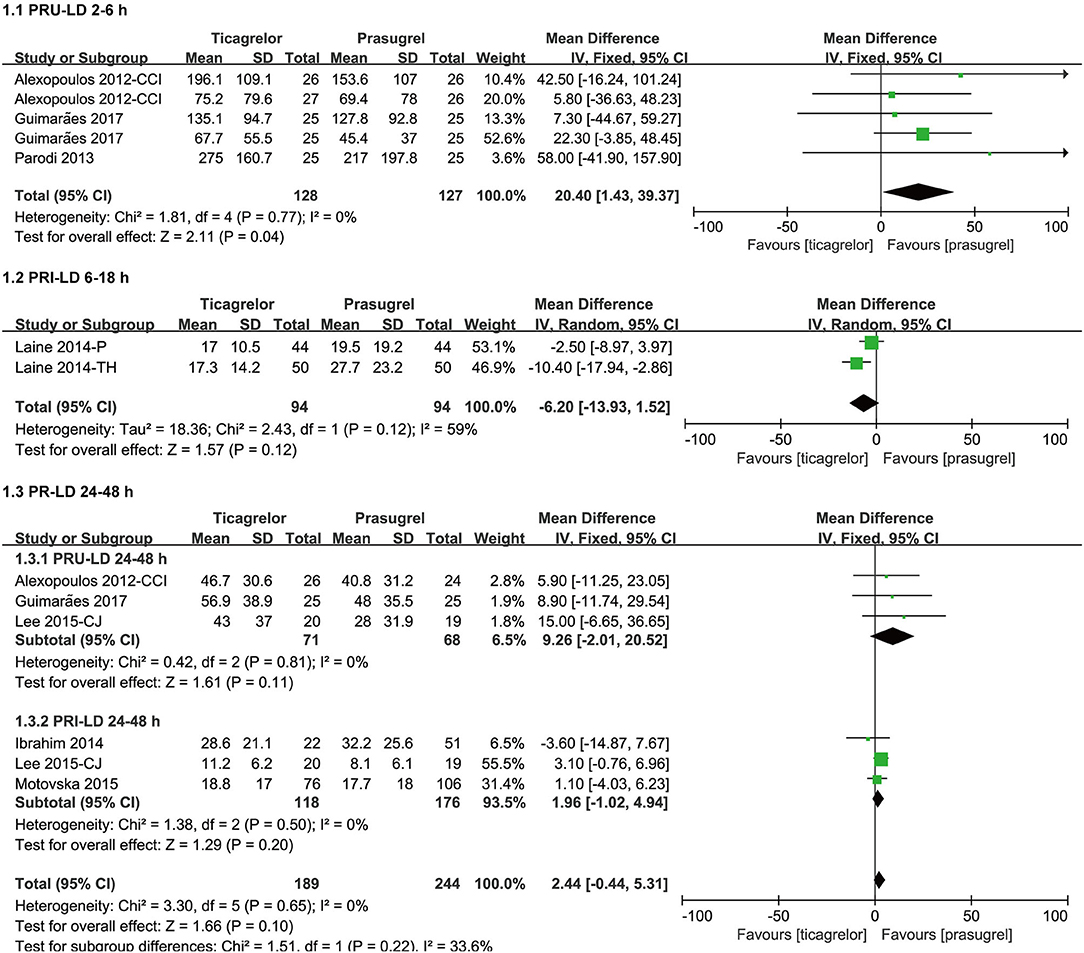
Figure 4. Forest plots of meta-analysis results of PR after LD.
Three (25, 26, 30) studies which included five sets of data compared PRU after LD within 2–6 h in ticagrelor group and prasugrel group. Ticagrelor group had a significantly higher PRU than prasugrel group [WMD = 20.40 (1.43, 39.37), P = 0.04] after LD within 2–6 h. It was worth noting that the P value of the overall effect test was 0.04, so though there was no heterogeneity among the five sets of data in the three studies (P = 0.77, I2 = 0%), sensitivity analysis was still carried out by eliminating studies one by one, and then we found that when eliminating the 6 h data of the study (30), the result substantially changed, the PRU after LD within 2–6 h of the two groups was not significantly different [WMD = 18.28 (−9.29, 45.85), P = 0.19] (Supplementary Figure 2).
Two (34, 35) studies compared PRI after LD within 6–18 h in ticagrelor group and prasugrel group. The impact of ticagrelor and prasugrel on PRI after LD within 6–18 h was not significantly different [WMD = −6.20 (−13.93, 1.52), P = 0.12, random effects model]. There was moderate heterogeneity among the two studies (P = 0.12, I2 = 59%). A sensitivity analysis was conducted by changing the effects model, and then found that ticagrelor group had a significantly lower PRI than prasugrel group [WMD = −5.85 (−10.76, −0.94), P = 0.02, fixed effects model] after LD within 6–18 h (Supplementary Figure 2), the results of different effect models were inconsistent.
Three (26, 30, 47) studies compared PRU after LD within 24–48 h in ticagrelor group and prasugrel group. The impact of ticagrelor and prasugrel on PRU after LD within 24–48 h was not significantly different [WMD = 9.26 (−2.01, 20.52), P = 0.11]. There was no heterogeneity among the three studies (P = 0.81, I2 = 0%).
Three (24, 27, 47) studies compared PRI after LD within 24–48 h in ticagrelor group and prasugrel group. The impact of ticagrelor and prasugrel on PRI after LD within 24–48 h was not significantly different [WMD = 1.96 (−1.02, 4.94), P = 0.20]. There was no heterogeneity among the three studies (P = 0.50, I2 = 0%).
Studies containing data of PR after MTD used three detection methods (VN, VASP and MEA), therefore, we grouped the data of PR after MTD according to the detection method. The meta-analysis results of PR after MTD were showed in Figure 5.
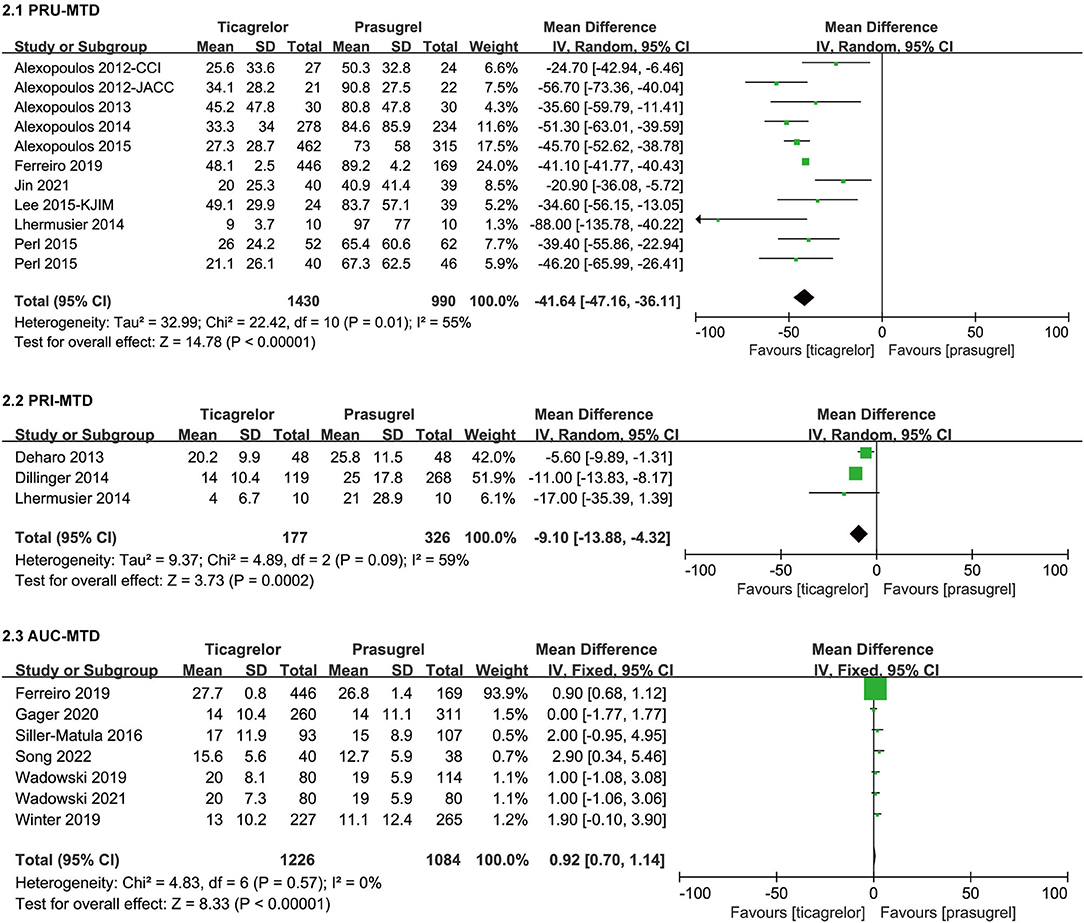
Figure 5. Forest plots of meta-analysis results of PR after MTD.
Song 2022 (46) was the sub-study of Jin et al. (29), therefore, we only included the data of PRU after MTD of Jin et al. for analysis. Eleven (23, 26, 28, 29, 31–33, 37–39, 46) studies which actually included 11 sets of data compared PRU after MTD in ticagrelor group and prasugrel group. After MTD, ticagrelor group had a significantly lower PRU than prasugrel group [WMD = −41.64 (-47.16,−36.11), P < 0.00001, random effects model], with moderate heterogeneity among the 11 sets of data (P = 0.01, I2 = 55%). A sensitivity analysis was conducted by eliminating study one by one and changing the effects model [WMD = −41.14 (−41.81, −40.47), P < 0.00001, fixed effects model] (Supplementary Figure 2), the result didn't substantially change.
Three (33, 36, 40) studies compared PRI after MTD in ticagrelor group and prasugrel group. After MTD, ticagrelor group had a significantly lower PRI than prasugrel group [WMD = −9.10 (−13.88, −4.32), P = 0.0002, random effects model], with moderate heterogeneity among studies (P = 0.09, I2 = 59%). A sensitivity analysis was conducted by eliminating study one by one and changing the effects model [WMD = −9.49 (−11.83, −7.14), P < 0.00001, fixed effects model] (Supplementary Figure 2), the result didn't substantially change.
Seven (31, 41–46) studies compared AUC after MTD in ticagrelor group and prasugrel group. Ticagrelor group had a slightly higher AUC than prasugrel group [WMD = 0.92 (0.70, 1.14), P < 0.00001]. There was no heterogeneity among the seven studies (P = 0.57, I2 = 0%).
Considering that the LD effect can be separated as early effect and late effect, and the studies containing data of HTPR after LD used two detection methods (VN and VASP), therefore, we grouped the data of HTPR after LD according to the detection time (within 2–6 h, within 6–18 h and within 24–48 h) and method. The meta-analysis results of HTPR after LD were showed in Figure 6.
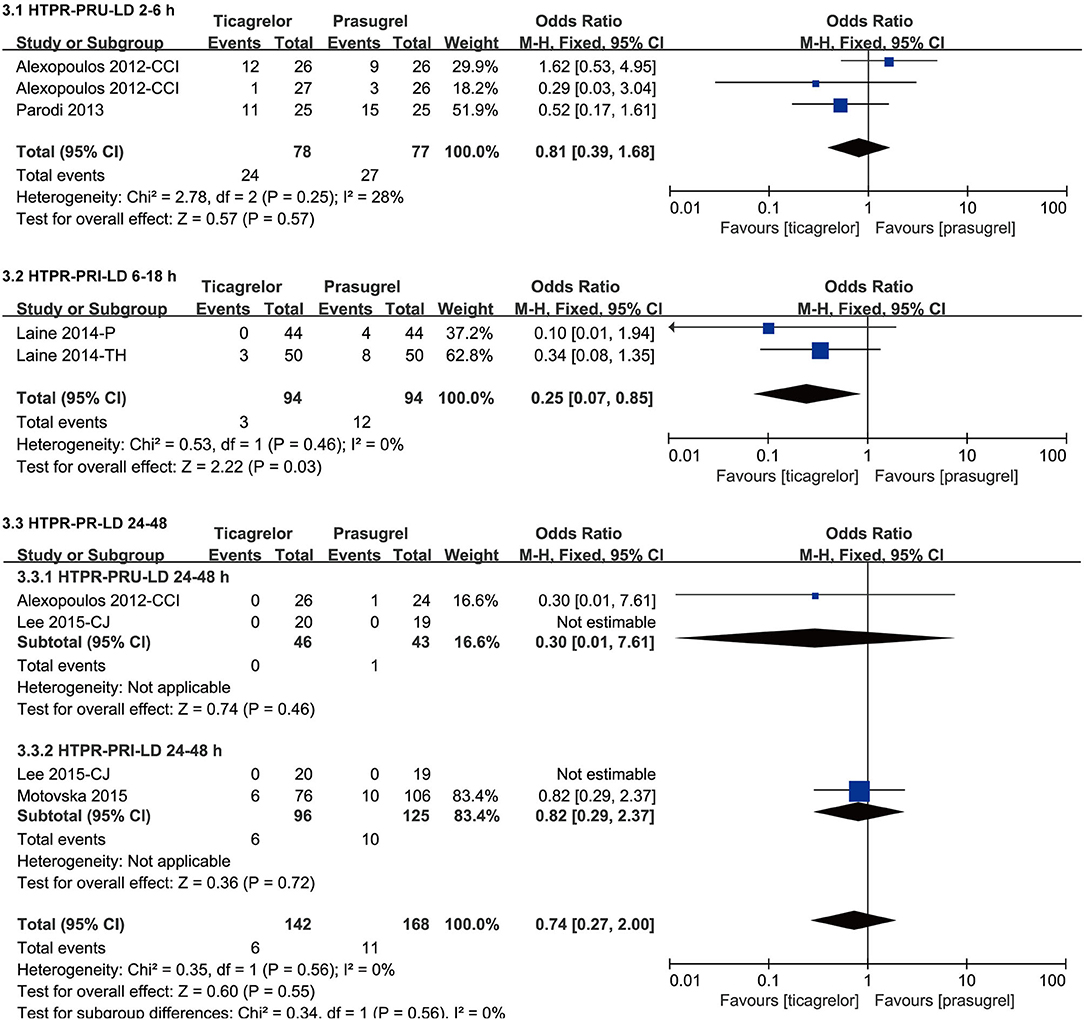
Figure 6. Forest plots of meta-analysis results of HTPR after LD.
Two (25, 26) studies which included three sets of data compared the incidence of HTPR based on PRU after LD within 2–6 h in ticagrelor group and prasugrel group. According to the VN assay, the incidence of HTPR after LD within 2–6 h of the two groups was not significantly different [RR = 0.81 (0.39, 1.68), P = 0.57], with relatively lower heterogeneity among the three sets of data in the two studies (P = 0.25, I2 = 28%).
Two (34, 35) studies compared the incidence of HTPR based on PRI after LD within 6–18 h in ticagrelor group and prasugrel group. According to the VASP test, ticagrelor group had a significantly lower incidence of HTPR after LD within 6–18 h than prasugrel group [RR = 0.25 (0.07, 0.85), P = 0.03, fixed effects model]. It was worth noting that the results of PRI after LD within 6–18 were inconsistent according to different effect models, so though there was no heterogeneity among the two studies (P = 0.46, I2 = 0%), sensitivity analysis was still carried out by changing the effects model [RR = 0.27 (0.08, 0.95), P = 0.04, random effects model] (Supplementary Figure 2), the result didn't substantially change.
Two (26, 47) studies compared the incidence of HTPR based on PRU after LD within 24–48 h in ticagrelor group and prasugrel group. According to the VN assay, the incidence of HTPR after LD within 24–48 h of the two groups was not significantly different [RR = 0.30 (0.01, 7.61), P = 0.46].
Two (27, 47) studies compared the incidence of HTPR based on PRI after LD within 24-48 hours in ticagrelor group and prasugrel group. According to the VASP test, the incidence of HTPR after LD within 24–48 h of the two groups was not significantly different [RR = 0.82 (0.29, 2.37), P = 0.72].
Studies containing data of HTPR after MTD used three detection methods (VN, VASP and MEA), therefore, we grouped the data of HTPR after MTD according to the detection method. The meta-analysis results of HTPR after MTD were showed in Figure 7.
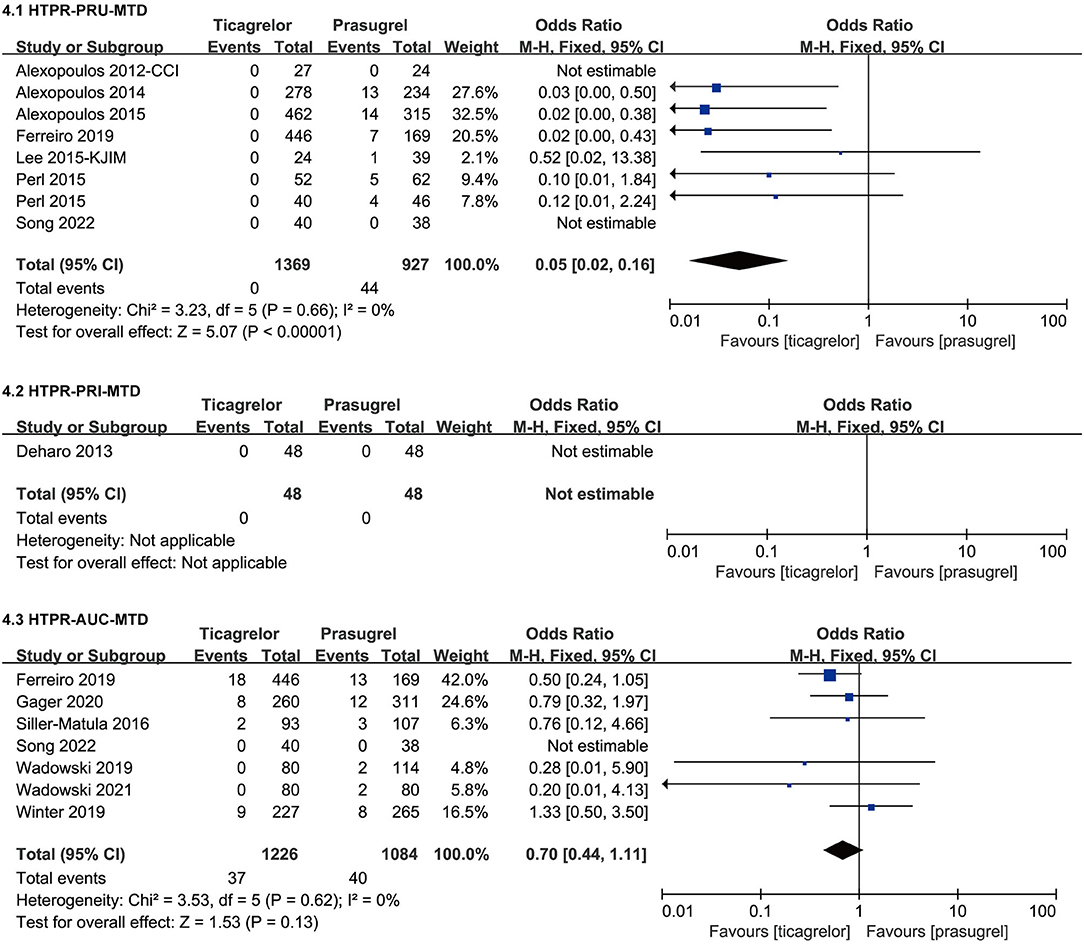
Figure 7. Forest plots of meta-analysis results of HTPR after MTD.
Seven (23, 26, 28, 31, 32, 38, 46) studies which included eight sets of data compared the incidence of HTPR based on PRU after MTD in ticagrelor group and prasugrel group. According to the VN assay, ticagrelor group had a significantly lower incidence of HTPR after MTD than prasugrel group [RR = 0.05 (0.02, 0.16), P < 0.00001]. There was no heterogeneity among the eight sets of data in the seven studies (P = 0.66, I2 = 0%).
Only one (36) study compared the incidence of HTPR based on PRI after MTD in ticagrelor group and prasugrel group. According to VASP test, no HTPR occurred in the two groups after 30 days of MTD treatment.
Seven (31, 41–46) studies compared the incidence of HTPR based on AUC after MTD in ticagrelor group and prasugrel group. According to the MEA test, the incidence of HTPR after MTD of the two groups was not significantly different [RR = 0.70 (0.44, 1.11), P = 0.13]. There was no heterogeneity among the seven studies (P = 0.62, I2 = 0%).
Considering that the LD effect can be separated as early effect and late effect, and the studies containing data of LTPR after LD used two detection methods (VN and VASP), therefore, we grouped the data of LTPR after LD according to the detection time (within 6–18 h and 48 h) and method. The meta-analysis results of LTPR after LD were showed in Figure 8.
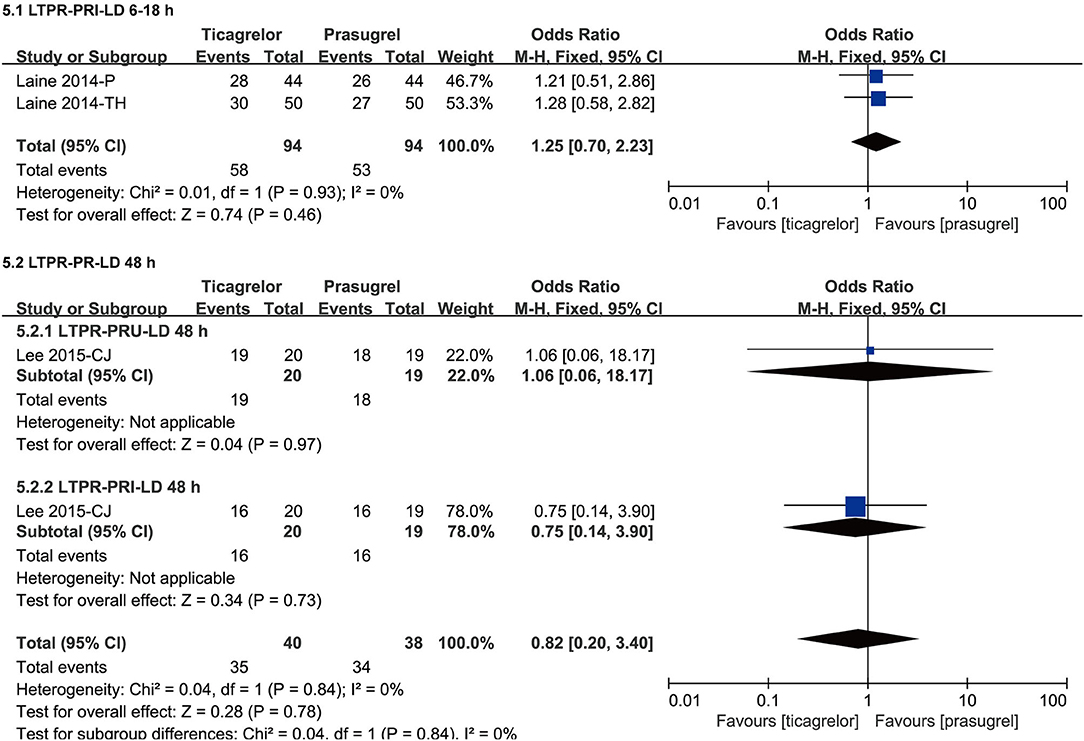
Figure 8. Forest plots of meta-analysis results of LTPR after LD.
Two (34, 35) studies compared the incidence of LTPR based on PRI after LD within 6–18 h in ticagrelor group and prasugrel group. According to the VASP test, the incidence of LTPR after LD within 6–18 h of the two groups was not significantly different [RR = 1.25 (0.70, 2.23), P = 0.46]. There was no heterogeneity among the two studies (P = 0.93, I2 = 0%).
One (47) study compared the incidence of LTPR based on both PRU and PRI at 48 h after LD in ticagrelor group and prasugrel group. According to the VN assay and VASP test, the incidence of LTPR at 48 h after LD of the two groups was both not significantly different [PRU, RR = 1.06 (0.06, 18.17), P = 0.97; PRI, RR = 0.75 (0.14, 3.90), P = 0.73]. There was no heterogeneity among the results based on the two test methods (P = 0.84, I2 = 0%).
Studies containing data of LTPR after MTD used three detection methods (VN, VASP and MEA), therefore, we grouped the data of LTPR after MTD according to the detection method. The meta-analysis results of LTPR after MTD were showed in Figure 9.
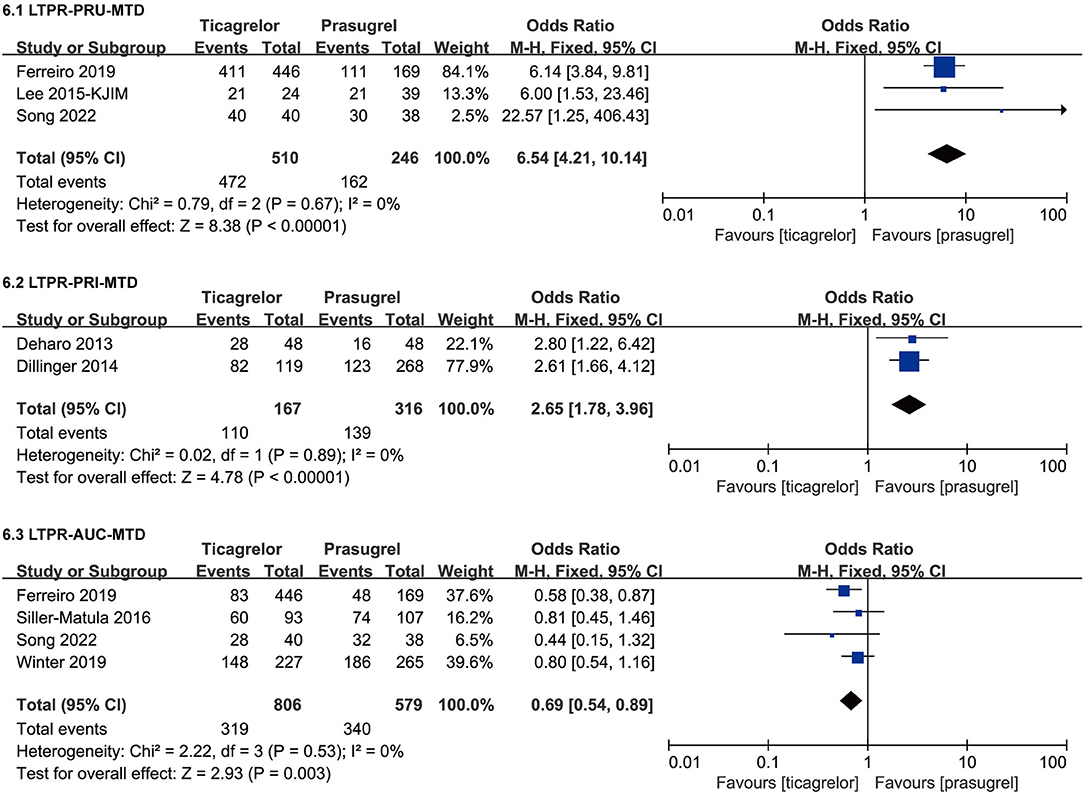
Figure 9. Forest plots of meta-analysis results of LTPR after MTD.
Three (28, 31, 46) studies compared the incidence of LTPR based on PRU after MTD in ticagrelor group and prasugrel group. According to the VN assay, ticagrelor group had a significantly higher incidence of LTPR after MTD than prasugrel group [RR = 6.54 (4.21, 10.14), P < 0.00001]. There was no heterogeneity among the three studies (P = 0.67, I2 = 0%).
Two (36, 40) studies compared the incidence of LTPR based on PRI after MTD in ticagrelor group and prasugrel group. According to the VASP test, ticagrelor group had a significantly higher incidence of LTPR after MTD than prasugrel group [RR = 2.65 (1.78, 3.96), P < 0.00001]. There was no heterogeneity among the two studies (P = 0.89, I2 = 0%).
Four (31, 41, 44, 46) studies compared the incidence of LTPR based on AUC after MTD in ticagrelor group and prasugrel group. According to the MEA test, ticagrelor group had a slightly lower incidence of LTPR after MTD than prasugrel group [RR = 0.69 (0.54, 0.89), P = 0.003]. It was worth noting that the result based on AUC was opposite to those based on PRU and PRI, so though there was no heterogeneity among the four studies (P = 0.53, I2 = 0%), sensitivity analysis was still carried out by eliminating studies one by one, and then we found that when eliminating the study (31), the result substantially changed, the incidence of LTPR based on AUC after MTD of the two groups was not significantly different [RR = 0.76 (0.56, 1.03), P = 0.08] (Supplementary Figure 2).
The meta-analysis results of ten clinical outcomes were shown in Supplementary Figure 1 and Table 4.
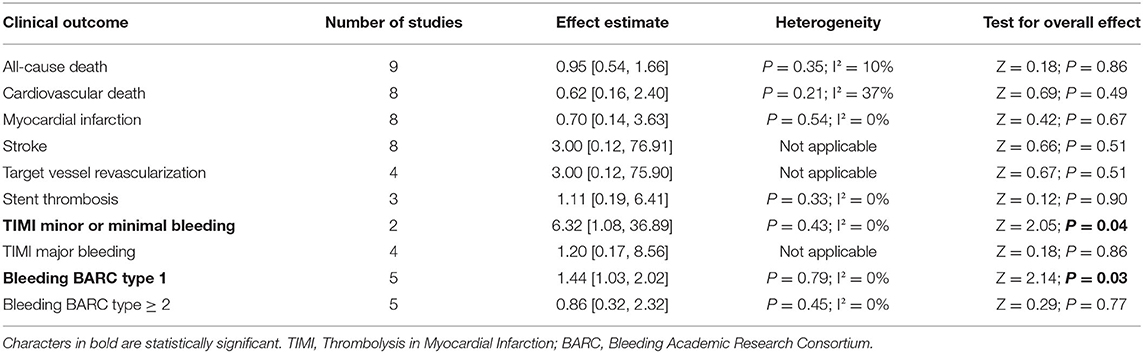
Table 4. Meta-analysis results of clinical outcomes.
The incidence of the following eight clinical outcomes was not statistically different between ticagrelor and prasugrel [all-cause death, P = 0.86; cardiovascular death, P = 0.49; myocardial infarction, P = 0.67; stroke, P = 0.51; target vessel revascularization, P = 0.51; stent thrombosis, P = 0.90; TIMI major bleeding, P = 0.86; bleeding BARC type ≥ 2, P = 0.77].
Ticagrelor had a significantly higher incidence of the following two clinical outcomes than prasugrel [TIMI minor or minimal bleeding, RR = 6.32 (1.08, 36.89), P = 0.04; bleeding BARC type 1, RR = 1.44 (1.03, 2.02), P = 0.03]. The sensitivity analysis was performed by changing the effects model, the result of bleeding BARC type 1 didn't substantially change, however, the result of TIMI minor or minimal bleeding was not robust, the incidence of TIMI minor or minimal bleeding between the two drugs was not significantly different after changing to random effects model [RR = 5.5 (0.88, 34.24), P = 0.07] (Supplementary Figure 2).
Eleven (23, 26, 28, 29, 31–33, 37–39, 46) studies which included 11 sets of data compared PRU after MTD in ticagrelor group and prasugrel group, so we performed a publication bias to detect the presence of small sample effects, neither funnel plot nor statistical tests found evidence of publication bias (Supplementary Figure 3, Egger's test, P = 0.758; Begger's test, P = 0.533). There were insufficient studies related to other outcomes, so we could not conduct publication bias test for other outcomes.
PR is an important indicator to evaluate the pharmacodynamic effect of antiplatelet drugs. Results of PR after LD suggested that after LD, the impact of prasugrel and ticagrelor on PRU and PRI within 24–48 h was no significantly different, however the results of the impact on PRU within 2–6 h and on PRI within 6–18 h (only two studies were included) substantially changed after the sensitivity analysis by eliminating literature one by one and changing effects model, which means that the results of 2–6 h and 6–18 h after LD are not robust, more studies are needed. Based on the current data alone, after LD within 24–48 h, there was no difference in the impact of prasugrel and ticagrelor on PR, while within 2–6 h and 6–18 h, we cannot jump to conclusions. Results of PR after MTD suggested that after MTD, the PRU and PRI of ticagrelor group were both significantly lower than those of prasugrel group, however, the AUC of ticagrelor group were slightly higher than that of prasugrel group, the results of VN assay were consistent with that of VASP test, and not with the MEA test. According to VN assay and VASP tests, after MTD, ticagrelor had stronger platelet inhibition than prasugrel, which may be related to different pharmacokinetic and pharmacodynamic properties of the two drugs: prasugrel is a prodrug that irreversibly antagonizes the P2Y12 receptor by conversion to an active metabolite, while ticagrelor does not require metabolic activation to exert activity, binding to P2Y12 receptors in a reversible manner (1), in addition, ticagrelor increases the concentration of plasma adenosine in patients with ACS by inhibiting red blood cell uptake of adenosine, thereby activating A2 adenosine receptors on platelets, increasing intracellular cAMP levels, and inducing VASP phosphorylation by cAMP-dependent protein kinase (48), and the extra adenosine effect of ticagrelor compared to prasugrel may have overestimated the level of PR inhibition assessed by VASP test (40). Research had shown that the results of different platelet function assays differ substantially (49), our study confirmed this once again, there are differences in the assessment of PR between the MEA test and the other two detention methods, which may be related to the sensitivity of the MEA test itself, which suggest that we need to conduct more specialized studies on the consistency of multiple platelet function assays and the correlation between these methods, which may be helpful for personalized antiplatelet therapy guided by PR. On the basis of current results, we can reach the following conclusion, according to VN assay and VASP tests, after LD within 24–48 h, there was no significant difference in platelet inhibition between ticagrelor and prasugrel; after MTD, ticagrelor had stronger platelet inhibition than prasugrel; there are differences in the assessment of PR between the MEA test and the other two detention methods.
Results of HTPR after LD suggested that after LD, the incidence of HTPR in prasugrel group and ticagrelor group within 2–6 h according to VN assay as well as within 24–48 h according to VN assay and VASP test was no significantly different, however within 6–18 h according to VASP test, the incidence of HTPR in prasugrel group was significantly higher than that in ticagrelor group. Results of HTPR after MTD suggested that after MTD, the incidence of HTPR in prasugrel group was significantly higher than that in ticagrelor group according to VN assay, only one study compared the incidence of HTPR after MTD measured by VASP test in the two groups and no HTPR occurred in either group, and according to MEA test, the incidence of HTPR after MTD in prasugrel group and ticagrelor group was no significantly different, which was inconsistent with the results of the VN assay. Some studies have indicated that rate of HTPR may be influenced by different definition and assessment methods (50, 51), this may account for the inconsistency. HTPR had shown to be have a link with increased risk of thrombotic/ischemic events (9). Therefore, based on the above results, we speculated that compared to ticagrelor, prasugrel might have a higher thrombotic/ischemic risk, however, actual clinical results were not the same as we speculated. Recently, Schüpke et al. randomly assigned patients with ACS in a multicenter, randomized, open-label trial and for whom invasive evaluation was planned to receive either ticagrelor or prasugrel (52). In the ISAR-REACT 5 experiment, the incidence of stroke, myocardial infarction, or death in prasugrel group were significantly lower than that in ticagrelor group (52), while according to our meta-analysis results of clinical outcomes, the incidence of thrombotic/ischemic events such as myocardial infarction, stroke, target vessel revascularization, stent thrombosis in two groups was no significant difference. Our included studies predominantly compared PR, studies that met our eligible criteria and reported clinical outcomes were mostly followed up for one month, only two (29, 45) studies followed up for 9 month and 1 year. However, the ISAR-REACT 5 experiment was followed up for 1 year, which may be the reason for the inconsistency with us. Of course, neither our meta-analysis nor the ISAR-REACT 5 experiment found that prasugrel had a higher risk of thrombotic/ischemic than ticagrelor. In summary, although the incidence of HTPR in prasugrel group might be higher than that in the ticagrelor group, comparing the incidence of HTPR between the two drugs alone does not lead to a conclusion of which drug causes a higher risk of thrombosis/ischemia.
Results of LTPR after LD suggested that after LD, the incidence of LTPR in prasugrel group and ticagrelor group was no significantly different within 6–18 h according to VASP test as well as 48 h according to VN assay and VASP test. Results of LTPR after MTD suggested that after MTD, the incidence of LTPR in ticagrelor group was significantly higher than prasugrel group according to VN assay and VASP test, while the result according to MEA assay was not robust, more studies are needed. LTPR had shown to be associated with a higher bleeding risk (53–55). From our findings, it can be speculated that compared to prasugrel, ticagrelor might have a higher bleeding risk. In the ISAR-REACT 5 experiment, major bleeding (BARC type 3 through 5) was observed in 5.4% of patients in the ticagrelor group and 4.8% of patients in the prasugrel group, while there was no significant difference in the incidence of major bleeding between the two groups (52). Our meta-analysis results of clinical outcomes reached a similar conclusion, there was no significant difference of the incidence of TIMI major bleeding, bleeding BARC type ≥ 2 in the two drugs. Besides, we also found that the incidence of bleeding BARC type 1 in ticagrelor group was significantly higher than prasugrel group. In summary, there was no significant difference between ticagrelor and prasugrel in the risk of bleeding BARC Type ≥ 2 and TIMI major bleeding, the incidence of bleeding BARC type 1 in ticagrelor group was significantly higher than prasugrel group and a higher incidence of LTPR in ticagrelor than prasugrel might indicate a higher risk of bleeding BARC type 1.
There are several strengths in our meta-analysis. First, in the previous meta-analysis of the impact of ticagrelor and prasugrel on PR, in addition to the PR-related outcomes, no clinical outcomes were included for analysis. However, in our meta-analysis, in addition to comparing the impact of the two drugs on PR and further analyzing the risks of HTPR and LTPR, the clinical outcomes were also included in the analysis, and discussed the association between HTPR and LTPR and thrombosis/ ischemic and bleeding event. Second, in the previous meta-analysis, the impact of the two drugs on PR were analyzed in groups based only on the drug doses (LD and MTD) and two detection methods (VA assay and VASP test). However, we are beyond that also included data of MEA test, and grouped the LD effect by time (within 2–6 h, within 6–18 h, within 24–48 h) to conduct a more detailed analysis. Third, compared with previous meta-analysis of the impact of ticagrelor and prasugrel on PR, we conducted a more comprehensive search and included more literatures, as far as we know, this is the first meta-analysis to assess the incidence of LTPR in the two P2Y12 inhibitors based on VN assay and MEA test. Finally, the studies included in our meta-analysis, both RCTs and cohort studies, had a high overall methodological quality.
There are several limitations of our meta-analysis to be noted. First, our meta-analysis only included studies comparing standard doses of prasugrel and ticagrelor, and the studies comparing the half-dose prasugrel and half-dose ticagrelor were not included. Second, the results of PRU within 2–6 h after LD, PRI within 6–18 h after LD, AUC-based LTPR after MTD were not robust, and only one study compared the incidence of HTPR after MTD measured by VASP test, thus, more large-scale randomized controlled studies are needed for further validation in the future.
Compared with prasugrel, ticagrelor might have a stronger platelet inhibition effect, with a lower incidence of HTPR and a higher incidence of LTPR and bleeding BARC type 1, while there might be no significant difference in the risk of thrombosis/ischemic, bleeding BARC Type ≥ 2 and TIMI major bleeding. A higher incidence of LTPR might indicate a higher risk of bleeding BARC type 1. The results of VN assay were consistent with that of VASP test, and not with the MEA test.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author/s.
LD and YJ devised the paper. LD and JX identified studies, conducted data collection and extraction, and analyzed the data. LD completed the first draft of the paper. KC provided guidelines for this meta-analysis. All authors approved the final version of the manuscript.
This research was financially supported by CACMS Innovation Fund (CI2021A00908) and National Natural Science Foundation of China (81373822).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fcvm.2022.905607/full#supplementary-material
Supplementary Figure 1. Forest plots of meta-analysis results of clinical outcomes.
Supplementary Figure 2. Sensitivity analysis for PRU-LD 2-6 h, PRI-LD 6-18 h, PRU-MTD, PRI-MTD, HTPR-PRI-LD 6-18 h, LTPR-AUC-MTD, TIMI Minor or Minimal Bleeding, and Bleeding BARC type 1.
Supplementary Figure 3. Funnel plot of comparison of PRU after MTD between ticagrelor group and prasugrel group.
Supplementary Table 1. Embase search strategy.
Supplementary Table 2. Web of science search strategy.
Supplementary Table 3. Cochrane search strategy.
1. Angiolillo DJ, Capranzano P. Pharmacology of emerging novel platelet inhibitors. Am Heart J. (2008) 156:S10–15. doi: 10.1016/j.ahj.2008.06.004
2. Neumann FJ, Sousa-Uva M, Ahlsson A, Alfonso F, Banning AP, Benedetto U, et al. 2018 ESC/EACTS Guidelines on myocardial revascularization. Eur Heart J. (2019) 40:87–165. doi: 10.1093/eurheartj/ehy855
3. Valgimigli M, Bueno H, Byrne RA, Collet JP, Costa F, Jeppsson A, et al. 2017 ESC focused update on dual antiplatelet therapy in coronary artery disease developed in collaboration with EACTS. Eur J Cardiothorac Surg. (2018) 53:34–78. doi: 10.1016/j.rec.2017.11.020
4. Roffi M, Patrono C, Collet JP, Mueller C, Valgimigli M, Andreotti F, et al. 2015 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation: Task Force for the Management of Acute Coronary Syndromes in Patients Presenting without Persistent ST-Segment Elevation of the European Society of Cardiology (ESC). Eur Heart J. (2016) 37:267–315. doi: 10.1093/eurheartj/ehv320
5. Patti G, Micieli G, Cimminiello C, Bolognese L. The role of clopidogrel in 2020: a reappraisal. Cardiovasc Ther. (2020) 2020:8703627. doi: 10.1155/2020/8703627
6. Schilling U, Dingemanse J, Ufer M. Pharmacokinetics and pharmacodynamics of approved and investigational P2Y12 receptor antagonists. Clin Pharmacokinet. (2020) 59:545–66. doi: 10.1007/s40262-020-00864-4
7. Akkaif MA, Daud NAA, Sha'Aban A, Ng ML, Abdul Kader MAS, Noor DAM, et al. The role of genetic polymorphism and other factors on clopidogrel resistance (CR) in an asian population with coronary heart disease (CHD). Molecules. (2021) 26:1987. doi: 10.3390/molecules26071987
8. Serebruany VL, Steinhubl SR, Berger PB, Malinin AI, Bhatt DL, Topol EJ. Variability in platelet responsiveness to clopidogrel among 544 individuals. J Am Coll Cardiol. (2005) 45:246–51. doi: 10.1016/j.jacc.2004.09.067
9. Marcucci R, Grifoni E, Giusti B. On-treatment platelet reactivity: state of the art and perspectives. Vascul Pharmacol. (2016) 77:8–18. doi: 10.1016/j.vph.2015.10.005
10. Wallentin L, Becker RC, Budaj A, Cannon CP, Emanuelsson H, Held C, et al. Ticagrelor versus clopidogrel in patients with acute coronary syndromes. N Engl J Med. (2009) 361:1045–57. doi: 10.1056/NEJMoa0904327
11. Wiviott SD, Braunwald E, McCabe CH, Montalescot G, Ruzyllo W, Gottlieb S, et al. Prasugrel versus clopidogrel in patients with acute coronary syndromes. N Engl J Med. (2007) 357:2001–15. doi: 10.1056/NEJMoa0706482
12. Fan ZG, Zhang WL, Xu B, Ji J, Tian NL, He SH. Comparisons between ticagrelor and clopidogrel following percutaneous coronary intervention in patients with acute coronary syndrome: a comprehensive meta-analysis. Drug Des Devel Ther. (2019) 13:719–30. doi: 10.2147/DDDT.S196535
13. Zhang L, Lu J, Dong W, Tian H, Feng W, You H, et al. Meta-analysis of comparison of the newer P2Y12 inhibitors (Oral Preparation or Intravenous) to clopidogrel in patients with acute coronary syndrome. J Cardiovasc Pharmacol. (2017) 69:147–55. doi: 10.1097/FJC.0000000000000451
14. Garcia A, Dunoyer-Geindre S, Nolli S, Reny JL, Fontana P. An ex vivo and in silico study providing insights into the interplay of circulating mirnas level, platelet reactivity and thrombin generation: looking beyond traditional pharmacogenetics. J Pers Med. (2021) 11:323. doi: 10.3390/jpm11050323
15. Stone GW, Witzenbichler B, Weisz G, Rinaldi MJ, Neumann FJ, Metzger DC, et al. Platelet reactivity and clinical outcomes after coronary artery implantation of drug-eluting stents (ADAPT-DES): a prospective multicentre registry study. Lancet. (2013) 382:614–23. doi: 10.1016/S0140-6736(13)61170-8
16. Wen M, Li Y, Qu X, Zhu Y, Tian L, Shen Z, et al. Comparison of platelet reactivity between prasugrel and ticagrelor in patients with acute coronary syndrome: a meta-analysis. BMC Cardiovasc Disord. (2020) 20:430. doi: 10.1186/s12872-020-01603-0
17. Stroup DF, Berlin JA, Morton SC, Olkin I, Williamson GD, Rennie D, et al. Meta-analysis of observational studies in epidemiology: a proposal for reporting. Meta-analysis Of Observational Studies in Epidemiology (MOOSE) group. JAMA. (2000) 283:2008–12. doi: 10.1001/jama.283.15.2008
18. Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Ann Intern Med. (2009) 151:264–9. doi: 10.7326/0003-4819-151-4-200908180-00135
19. Higgins JPT, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, et al. Cochrane Handbook for Systematic Reviews of Interventions version 6.2 (updated February 2021). Cochrane, (2021). Available online at: http://www.training.cochrane.org/handbook [accessed December 27, 2021].
20. Wells GA, Shea B, O'Connell D, Peterson J, Welch V, Losos M, et al. The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses. Ottawa Hospital Research Institute, (2021). Available online at: http://www.ohri.ca/Programs/clinical_epidemiology/oxford.asp [accessed December 27, 2021].
21. Begg CB, Mazumdar M. Operating characteristics of a rank correlation test for publication bias. Biometrics. (1994) 50:1088–101. doi: 10.2307/2533446
22. Egger M, Davey SG, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ. (1997) 315:629–34. doi: 10.1136/bmj.315.7109.629
23. Perl L, Zemer-Wassercug N, Rechavia E, Vaduganathan M, Orvin K, Weissler-Snir A, et al. Comparison of platelet inhibition by prasugrel versus ticagrelor over time in patients with acute myocardial infarction. J Thromb Thrombolysis. (2015) 39:1–7. doi: 10.1007/s11239-014-1119-9
24. Ibrahim K, Christoph M, Schmeinck S, Schmieder K, Steiding K, Schoener L, et al. High rates of prasugrel and ticagrelor non-responder in patients treated with therapeutic hypothermia after cardiac arrest. Resuscitation. (2014) 85:649–56. doi: 10.1016/j.resuscitation.2014.02.004
25. Parodi G, Valenti R, Bellandi B, Migliorini A, Marcucci R, Comito V, et al. Comparison of prasugrel and ticagrelor loading doses in ST-segment elevation myocardial infarction patients: RAPID (Rapid Activity of Platelet Inhibitor Drugs) primary PCI study. J Am Coll Cardiol. (2013) 61:1601–6. doi: 10.1016/j.jacc.2013.01.024
26. Alexopoulos D, Xanthopoulou I, Gkizas V, Kassimis G, Theodoropoulos KC, Makris G, et al. Randomized assessment of ticagrelor versus prasugrel antiplatelet effects in patients with ST-segment-elevation myocardial infarction. Circ Cardiovasc Interv. (2012) 5:797–804. doi: 10.1161/CIRCINTERVENTIONS.112.972323
27. Motovska Z, Ondrakova M, Bednar F, Knot J, Ulman J, Maly M. Selection of P2Y12 antagonist, treatment initiation, and predictors of high on-treatment platelet reactivity in a “real World” registry. Thromb Res. (2015) 135:1093–9. doi: 10.1016/j.thromres.2015.04.014
28. Lee JH, Ahn SG, Park B, Park SW, Kang YS, Lee JW, et al. A pharmacodynamic study of the optimal P2Y12 inhibitor regimen for East Asian patients with acute coronary syndrome. Korean J Intern Med. (2015) 30:620–8. doi: 10.3904/kjim.2015.30.5.620
29. Jin CD, Kim MH, Song K, Jin X, Lee KM, Park JS, et al. Pharmacodynamics and outcomes of a de-escalation strategy with half-dose prasugrel or ticagrelor in east asians patients with acute coronary syndrome: results from HOPE-TAILOR trial. J Clin Med. (2021) 10:2699. doi: 10.3390/jcm10122699
30. Guimarães LF, Généreux P, Silveira D, Pesaro AE, Falcão F, Barbosa BR, et al. P2Y12 receptor inhibition with prasugrel and ticagrelor in STEMI patients after fibrinolytic therapy: analysis from the SAMPA randomized trial. Int J Cardiol. (2017) 230:204–8. doi: 10.1016/j.ijcard.2016.12.173
31. Ferreiro JL, Vivas D, De La Hera JM, Marcano AL, Lugo LM, Gómez-Polo JC, et al. High and low on-treatment platelet reactivity to P2Y12 inhibitors in a contemporary cohort of acute coronary syndrome patients undergoing percutaneous coronary intervention. Thromb Res. (2019) 175:95–101. doi: 10.1016/j.thromres.2019.01.021
32. Alexopoulos D, Vogiatzi C, Stavrou K, Vlassopoulou N, Perperis A, Pentara I, et al. Diabetes mellitus and platelet reactivity in patients under prasugrel or ticagrelor treatment: an observational study. Cardiovasc Diabetol. (2015) 14:68. doi: 10.1186/s12933-015-0232-1
33. Lhermusier T, Voisin S, Murat G, Mejean S, Garcia C, Bataille V, et al. Switching patients from clopidogrel to novel P2Y12 receptor inhibitors in acute coronary syndrome: comparative effects of prasugrel and ticagrelor. Eur Heart J. (2014) 35:349. doi: 10.1016/j.ijcard.2014.04.208
34. Laine M, Frere C, Toesca R, Berbis J, Barnay P, Pansieri M, et al. Ticagrelor versus prasugrel in diabetic patients with an acute coronary syndrome a pharmacodynamic randomised study. Thromb Haemost. (2014) 111:273–8. doi: 10.1160/TH13-05-0384
35. Laine M, Gaubert M, Frère C, Peyrol M, Thuny F, Yvorra S, et al. COMparison of Platelet reactivity following prAsugrel and ticagrelor loading dose in ST-Segment elevation myocardial infarctION patients: The COMPASSION study. Platelets. (2015) 26:570–2. doi: 10.3109/09537104.2014.959914
36. Deharo P, Bassez C, Bonnet G, Pankert M, Quilci J, Alessi MC, et al. Prasugrel versus ticagrelor in acute coronary syndrome: a randomized comparison. Int J Cardiol. (2013) 170:e21–22. doi: 10.1016/j.ijcard.2013.10.043
37. Alexopoulos D, Galati A, Xanthopoulou I, Mavronasiou E, Kassimis G, Theodoropoulos KC, et al. Ticagrelor versus prasugrel in acute coronary syndrome patients with high on-clopidogrel platelet reactivity following percutaneous coronary intervention: a pharmacodynamic study. J Am Coll Cardiol. (2012) 60:193–9. doi: 10.1016/j.jacc.2012.03.050
38. Alexopoulos D, Stavrou K, Koniari I, Gkizas V, Perperis A, Kontoprias K, et al. Ticagrelor vs prasugrel one-month maintenance therapy: impact on platelet reactivity and bleeding events. Thromb Haemost. (2014) 112:551–7. doi: 10.1160/TH14-02-0119
39. Alexopoulos D, Xanthopoulou I, Mavronasiou E, Stavrou K, Siapika A, Tsoni E, et al. Randomized assessment of ticagrelor versus prasugrel antiplatelet effects in patients with diabetes. Diabetes Care. (2013) 36:2211–6. doi: 10.2337/dc12-2510
40. Dillinger JG, Silberman SM, Dit Sollier CB, Amsallem M, Sideris G, Voicu S, et al. Ticagrelor effectiveness overestimated by VASP index Platelet inhibition by ticagrelor versus prasugrel in acute coronary syndrome patients according to platelet function tests. Int J Cardiol. (2014) 176:557–9. doi: 10.1016/j.ijcard.2014.07.019
41. Winter MP, Schneeweiss T, Cremer R, Biesinger B, Hengstenberg C, Prueller F, et al. Platelet reactivity patterns in patients treated with dual antiplatelet therapy. Eur J Clin Invest. (2019) 49:e13102. doi: 10.1111/eci.13102
42. Wadowski PP, Pultar J, Weikert C, Eichelberger B, Panzer B, Huber K, et al. Protease-activated receptor-mediated platelet aggregation in acute coronary syndrome patients on potent P2Y12 inhibitors. Res Pract Thromb Haemostasis. (2019) 3:383–90. doi: 10.1002/rth2.12213
43. Wadowski PP, Pultar J, Weikert C, Eichelberger B, Lang IM, Koppensteiner R, et al. Comparison of Light Transmission Aggregometry With Impedance Aggregometry in Patients on Potent P2Y12 Inhibitors. J Cardiovasc Pharmacol Ther. (2021) 26:260–8. doi: 10.1177/1074248420968706
44. Siller-Matula JM, Akca B, Neunteufl T, Maurer G, Lang IM, Kreiner G, et al. Inter-patient variability of platelet reactivity in patients treated with prasugrel and ticagrelor. Platelets. (2016) 27:373–7. doi: 10.3109/09537104.2015.1095874
45. Gager GM, Jilma B, Winter MP, Hengstenberg C, Lang IM, Toma A, et al. Ticagrelor and prasugrel are independent predictors of improved long-term survival in ACS patients. Eur J Clin Investig. (2020) 50:e13304. doi: 10.1111/eci.13304
46. Song K, Jin X, Kim MH, Li JX, Jin CD, Yuan SL, et al. Differences in optimal platelet reactivity after potent P2Y12 inhibitor treatment in acute coronary syndrome patients undergoing percutaneous coronary intervention. J Clin Med. (2022) 11:2480–92. doi: 10.3390/jcm11092480
47. Lee YS, De Jin C, Kim MH, Guo LZ, Cho YR, Park K, et al. Comparison of prasugrel and ticagrelor antiplatelet effects in korean patients presenting with st-segment elevation myocardial infarction. Circul J. (2015) 79:1248–54. doi: 10.1253/circj.CJ-15-0270
48. Gessi S, Varani K, Merighi S, Ongini E, Borea PA. A(2A) adenosine receptors in human peripheral blood cells. Br J Pharmacol. (2000) 129:2–11. doi: 10.1038/sj.bjp.0703045
49. Helten C, Naguib D, Dannenberg L, Pöhl M, Ayhan A, Hohlfeld T, et al. Platelet function testing: dead or alive. J Thromb Haemost. (2018) 16:984–6. doi: 10.1111/jth.13997
50. Lemesle G, Landel JB, Bauters A, Delhaye C, Bonello L, Sudre A, et al. Poor agreement between light transmission aggregometry, Verify Now P2Y12 and vasodilatator-stimulated phosphoprotein for clopidogrel low-response assessment: a potential explanation of negative results of recent randomized trials. Platelets. (2014) 25:499–505. doi: 10.3109/09537104.2013.840363
51. Bonello L, Tantry US, Marcucci R, Blindt R, Angiolillo DJ, Becker R, et al. Consensus and future directions on the definition of high on-treatment platelet reactivity to adenosine diphosphate. J Am Coll Cardiol. (2010) 56:919–33. doi: 10.1016/j.jacc.2010.04.047
52. Schüpke S, Neumann FJ, Menichelli M, Mayer K, Bernlochner I, Wöhrle J, et al. Ticagrelor or Prasugrel in Patients with Acute Coronary Syndromes. N Engl J Med. (2019) 381:1524–34. doi: 10.1056/NEJMoa1908973
53. Cuisset T, Grosdidier C, Loundou AD, Quilici J, Loosveld M, Camoin L, et al. Clinical implications of very low on-treatment platelet reactivity in patients treated with thienopyridine: the POBA study (predictor of bleedings with antiplatelet drugs). JACC Cardiovasc Interv. (2013) 6:854–63. doi: 10.1016/j.jcin.2013.04.009
54. Patti G, Pasceri V, Vizzi V, Ricottini E, Di Sciascio G. Usefulness of platelet response to clopidogrel by point-of-care testing to predict bleeding outcomes in patients undergoing percutaneous coronary intervention (from the Antiplatelet Therapy for Reduction of Myocardial Damage During Angioplasty-Bleeding Study). Am J Cardiol. (2011) 107:995–1000. doi: 10.1016/j.amjcard.2010.11.025
Keywords: prasugrel, ticagrelor, platelet reactivity, acute coronary syndrome, meta-analysis
Citation: Dai L, Xu J, Jiang Y and Chen K (2022) Impact of Prasugrel and Ticagrelor on Platelet Reactivity in Patients With Acute Coronary Syndrome: A Meta-Analysis. Front. Cardiovasc. Med. 9:905607. doi: 10.3389/fcvm.2022.905607
Received: 27 March 2022; Accepted: 20 May 2022;
Published: 09 June 2022.
Edited by:
Xiaofeng Yang, Temple University, United StatesReviewed by:
Moo Kim, Dong-A University Hospital, South KoreaCopyright © 2022 Dai, Xu, Jiang and Chen. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Keji Chen, a2pjaGVudmlwQDE2My5jb20=; Yuerong Jiang, amlhbmdfeXVlcm9uZ0AxNjMuY29t
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.