
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Cardiovasc. Med., 04 May 2022
Sec. Cardiovascular Therapeutics
Volume 9 - 2022 | https://doi.org/10.3389/fcvm.2022.899235
 Xia Xu1†
Xia Xu1† Yumeng Li1†Shuqing Shi1†Jiayu Lv1Yajiao Wang2Haoran Zheng3Xinxin Mao2Huaqin Wu4*Bingxuan Zhang1*
Yumeng Li1†Shuqing Shi1†Jiayu Lv1Yajiao Wang2Haoran Zheng3Xinxin Mao2Huaqin Wu4*Bingxuan Zhang1* Qingqiao Song1*
Qingqiao Song1*
Cardiovascular disease (CVD) has become a huge challenge for the global public health system due to its high morbidity, mortality and severe economic burden. In recent years, angiotensin receptor neprilysin inhibitor (ARNI), a new class of drugs, has shown good therapeutic effects on CVD patients in several clinical studies, reducing the morbidity and mortality of CVD patients. In this study, we retrieved publications on ARNI research in the cardiovascular field from the Web of Science core collection and analyzed the annual output, spatial and temporal distribution, institutions and authors, core journals, keywords and co-cited literature based on CiteSpace. As a result, 604 publications were retrieved, and the number of annual publications generally increased year by year, with the largest number of articles. The analysis of the co-occurrence of output countries and authors showed that a few developed countries such as the United States, Canada, and United Kingdom are the most active in this field, forming academic groups represented by John Joseph Valentine McMurray and Scott D. Solomon, and New England Journal of Medicine, Cirulation, and Journal of the American College of Cardiology are the most popular journals in the field, with research hotspots focused on ARNI in the treatment of total ejection fraction heart failure, hypertension and its target organ damage, with the potential for future benefit throughout the cardiovascular event chain as research progresses. This study reveals the prospective application of ARNI in the cardiovascular field and the research hotspots, providing broader and deeper guidance for its use in the clinic, which is beneficial to improve the treatment and prognosis of CVD patients.
Cardiovascular disease (CVD) refers to a group of diseases involving the heart or blood vessels, including heart failure, hypertensive heart disease, rheumatic heart disease, stroke, and many other vascular and cardiac problems (1). In 2017, it was reported that there were approximately 485.6 million people with CVD worldwide, of which 17.8 million died from CVD, an increase of 21.1 and 28.5% (2), respectively, compared to a decade earlier. CVD has become the most common cause of death worldwide and one of the most serious health problems worldwide, accounting for 31% of all deaths worldwide (3). In addition to deaths, CVDs represent a significant economic burden, accounting for a large portion of global healthcare expenditures and lost productivity. In a recent report, the American Heart Association estimated that the healthcare costs and lost productivity of CVD are expected to grow from $555 billion in 2015 to $1.1 trillion in 2035, and with the cost of home, informal or unpaid care provided to CVD patients, the total cost of CVD will reach $1.2 trillion (4). Therefore, prevention and treatment of CVD onset, progression, and recurrence is currently a huge challenge for global public health systems.
At present, the commonly used therapeutic drugs for CVD mainly include angiotensin-converting enzyme inhibitors, angiotensin receptor antagonists, β-receptor antagonists, vasodilators, diuretics, a-receptor antagonists, positive inotropic drugs, lipid-modulating drugs, antiarrhythmics, calcium channel blockers, etc. Although they have improved the quality of life and survival rate of CVD patients to a certain extent, the action of the above drugs is relatively single, and the combination of several drugs is often required to achieve good results in the treatment of some refractory CVD. Angiotensin receptor neprilysin inhibitor (ARNI) is a dual neuroendocrine regulator with simultaneous inhibition of angiotensin receptor and enkephalinase, which is effective in treating myocardial remodeling by dilating blood vessels, promoting sodium and urine excretion, and inhibiting myocardial remodeling (5). It has shown great potential in the treatment of hypertension (6, 7), arrhythmia (8, 9), myocardial infarction (10, 11), diabetes mellitus (12, 13), and diabetic nephropathy (14, 15). Previous studies on ARNI have mostly explored one aspect of its role or mechanism, and most of the overviews of its role have been in the form of textual discussions. This review will provide the first visual analysis of ARNI research in the cardiovascular system based on CiteSpace software to analyze the current status of research in this field, research hotspots and emerging research directions over the past 20 years in a more visual way, highlighting milestone research results to help understand the development trend of this new drug and promote its widespread use in CVD patients.
The main databases for bibliometric analysis are Web of Science, PubMed, Cochrane Library, etc. This study chose Web of Science because the change database is a large comprehensive, multidisciplinary, high-impact academic journal, and the study confirmed that applying Web of Science database for CiteSpace visual analysis can provide better knowledge mapping effect (16, 17). The proposed search formula is: TS = (Angiotensin receptor neprilysin inhibitor OR ARNI OR Sacubitril Valsartan Sodium Tablets), refining the category: Cardiovascular System. Time span: 2000–2022; Language: English; 3 book chapters, 2 corrections, and 1 news item were excluded, and 604 relevant documents were obtained from the search. All the above operations were completed within 1 day (February 7, 2022). All records including titles, authors, abstracts, keywords, cited references, etc., were exported in plain text format and named in the format of “download_***.txt” as analysis data of CiteSpace.
CiteSpace is a Java-based application developed by Prof. Chaomei Chen at Drexel University to help visualize and analyze knowledge domains and emerging trends, showing the structure and distribution of scientific knowledge (18, 19). Some studies have shown that CiteSpace focuses on finding key points in the development of a field or domain, especially key turning points. Due to its rich functionality it has become an effective method for analyzing big data today (20, 21). After importing the data into CiteSpace, data cleaning was first performed, and then a series of network structure and temporal analyses were performed based on the data, mainly including country, institution, author, journal, keywords, and co-cited literature. The results are displayed in the form of visual graphs, where nodes represent research items, and the larger the node, the more frequently the item appears or is cited; links between nodes describe the co-occurrence or co-citation between these nodes, and the thickness of the line represents the strength of the link, and the shade or hue of the node and link color indicates the temporal order of the item’s appearance (22). Centrality is an indicator used to measure the importance of an element. If the centrality is greater than 0.1, the element is considered relatively important and is represented by a purple ring (23). Cluster analysis is also an important analysis in CiteSpace, where modularity Q and mean contour are two important evaluation metrics in cluster analysis, with Q > 0.3 indicating a sufficiently significant cluster structure and mean contour >0.5 indicating convincing clustering results (24). The basic parameters of CiteSpace software are set: Time Slicing: 2000–2022, Years Per Slice: 1 year; Top N per slice = 50; Pruning: Pathfinder, Pruning sliced networks, Pruning the merged networks.
By web of science citation analysis, the research of ARNI in the cardiovascular system showed a steady upward trend in the number of published articles per year between 2000 and 2021 (Figure 1A), which has been in a low heat period from 2000 to 2014, with fewer related studies reported and less than 30 total publications. The number of published papers increased steadily from 2015 to 2018. 40 papers were published in 2015 alone, more than the total of the previous 15 years, with an average annual growth of 12 papers and an average annual growth rate of 37.5%, indicating that the research heat and importance of this field has been noticed. The number of articles published in this field has shown an obvious upward trend in the past 3 years, with a total of more than 100 papers published per year, and has been at a high level of heat, with an average annual growth of 24 articles and an average annual growth rate of 29.6%, indicating that the research in this field has entered a period of rapid development and is being paid more and more attention. To date, these articles have been cited 15,887 times, with an average of 24.82 citations per article. Early in the study, the average annual citation frequency of articles was low due to less research on the application of ARNI in the cardiovascular system, and since 2015 the average annual citation frequency of published articles has rapidly increased and stabilized at around 300 per year, further demonstrating that research on ARNI in the cardiovascular system has entered a more mature stage (Figure 1B). The reason for this may be due to the increase in the number of patients with cardiovascular disease worldwide on the one hand and suggests a better understanding of the drug on the other. Among all published articles, ARTICLES had the highest number of 53.0%, followed by REVIEWS with 22.0% (Figure 1C). Clinical trials are one of the most important methods of medical research (25), such as randomized controlled trials and cross-sectional studies, which can assess the efficacy and safety of ARNI in order to provide useful information and guidance for the long term.
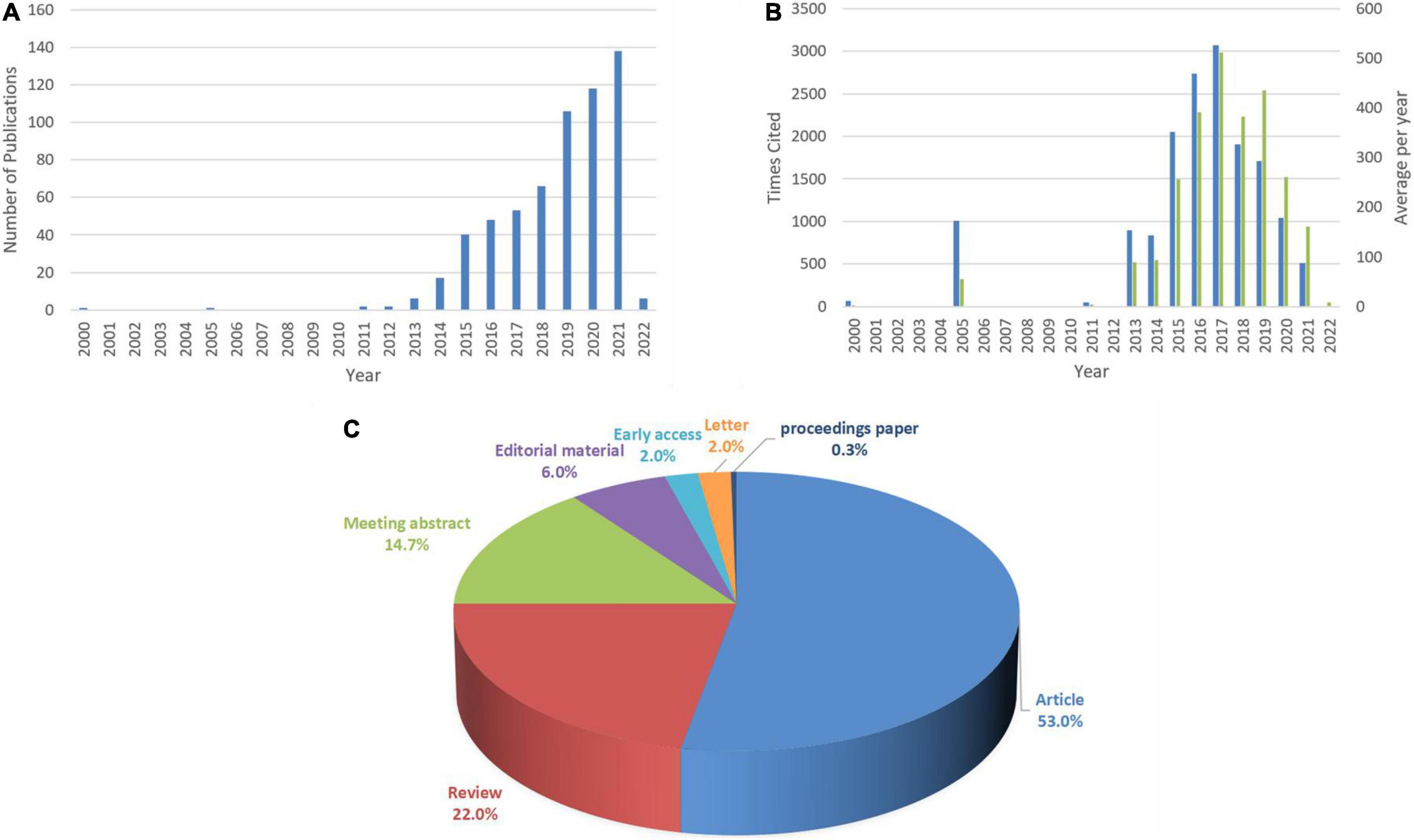
Figure 1. Annual number, Times Cited frequency, average per year citation frequency and document type of ARNI publications in cardiovascular system research. (A) Annual distribution of the number. (B) Blue represents Times Cited and green for average per year frequency of citations. (C) Type of documents.
A total of 74 countries published articles related to ARNI research in the cardiovascular system from 2000 to 2021 (Figure 2A), and it can be seen from Figure 2 and Table 1 that the top 11 countries in terms of publications are United States (269), United Kingdom (102), Italy (91), Canada (77), and Germany (62) (Figures 2B,C), with the time of publication concentrated after 2012. The most cited country for published articles was the United States (10,913 citations), followed by United Kingdom (4,953 citations) and Canada (4,265 citations) (Figure 2D). In addition, France publications had the highest average number of citations (72.33 citations on average), followed by Canada (55.39 citations on average) and Sweden (54.87 citations on average) (Figure 2E). h-index is a new method for evaluating academic achievement, and a higher h-index indicates a more influential paper, with United States (54), United Kingdom (43) and Canada (35) were the three countries with the highest h-index (Figure 2F). The national co-occurrence network visualized in Figure 2G contains 100 nodes and 262 links, which are often considered as important turning points that may lead to transformative discoveries and act as bridges in terms of their high intermediary centrality (≥0.10) (22, 26), as seen in the figure, Denmark (0.32) ranks first, followed by Argentina (0.31) and Czechia (0.20), implying that they play an important role in expanding knowledge to other countries. Combining these three paper evaluation indicators shows that United States, United Kingdom, and Canada are the three most influential countries in this research area. However, it is worth noting that there is less cooperation between these countries and other countries, and the cooperation between countries should be strengthened in the future to drive the development of this field.
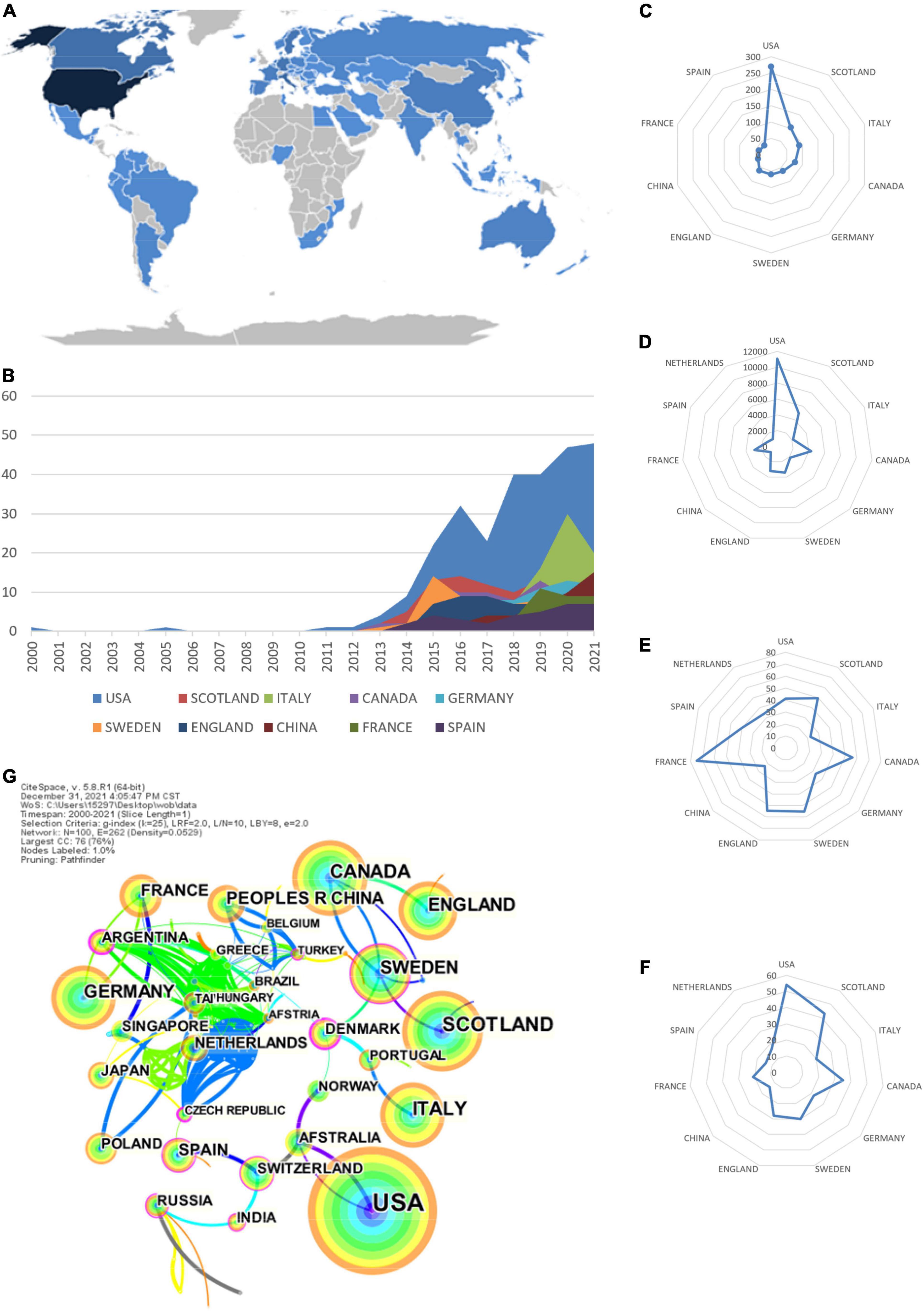
Figure 2. Leading countries for ARNI application research in the cardiovascular system. (A) Geographical distribution of global output; (B) Annual output trend of the top 10 productive countries; (C) Radar map of the top 11 productive countries; (D) Radar map of TGCS of the top 11 productive countries; (E) Radar map of average cited of the top 11 productive countries; (F) Radar map of h-index for the top 11 producing countries; (G) CiteSpace visualization of the countries participating in the ARNI in Cardiovascular Systems Study. Notes: The size of node reflects the co-occurrence frequencies, and the links indicate the co-occurrence relationships. The color of node and line represents different years, and node with purple round means high betweenness centrality (>0.1).
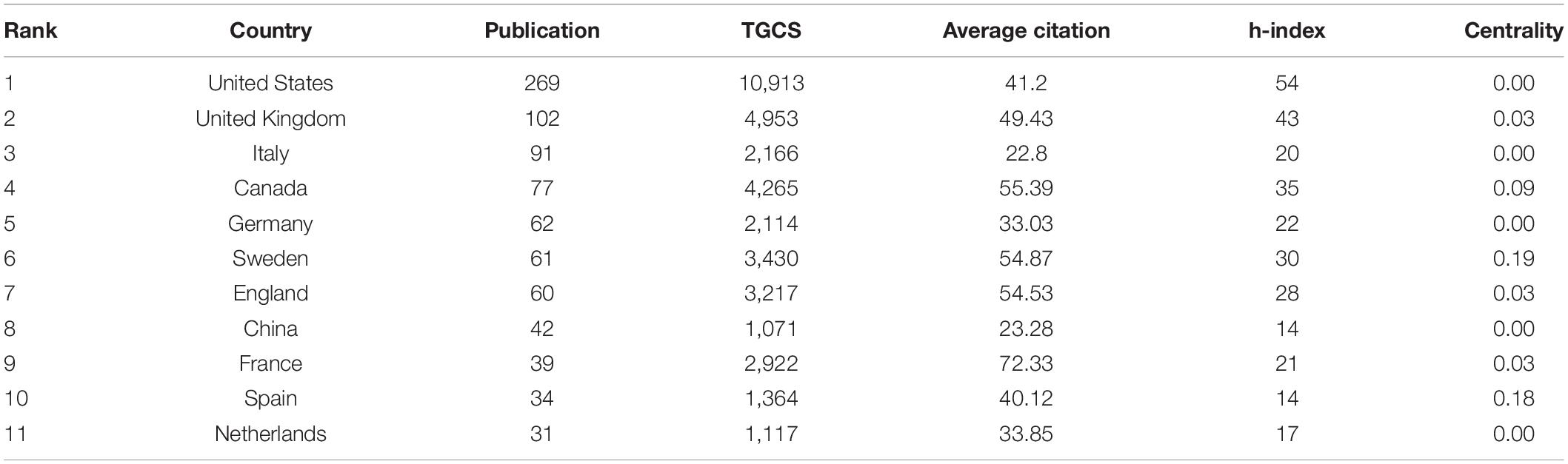
Table 1. Top 11 producing countries studied by ARNI in the cardiovascular system.
A total of 332 institutions published articles on the use of ARNI in the cardiovascular system (Figure 3). The top 10 institutions in terms of research output are shown in Figure 3 and Table 2, with University of Glasgow (n = 97) leading in terms of output, followed by Novartis Pharmaceuticals (n = 90), Brigham and Women’s Hospital (n = 87), University of Montreal (n = 58), and University of Gothenburg (n = 48). The top three institutions in terms of centrality were Cleveland Clinic (0.23), Associazione Nazionale Medici Cardiologi Ospedalieri (0.18), and Charles University Prague (0.17). As shown in the figure, there is closer cooperation between institutions.
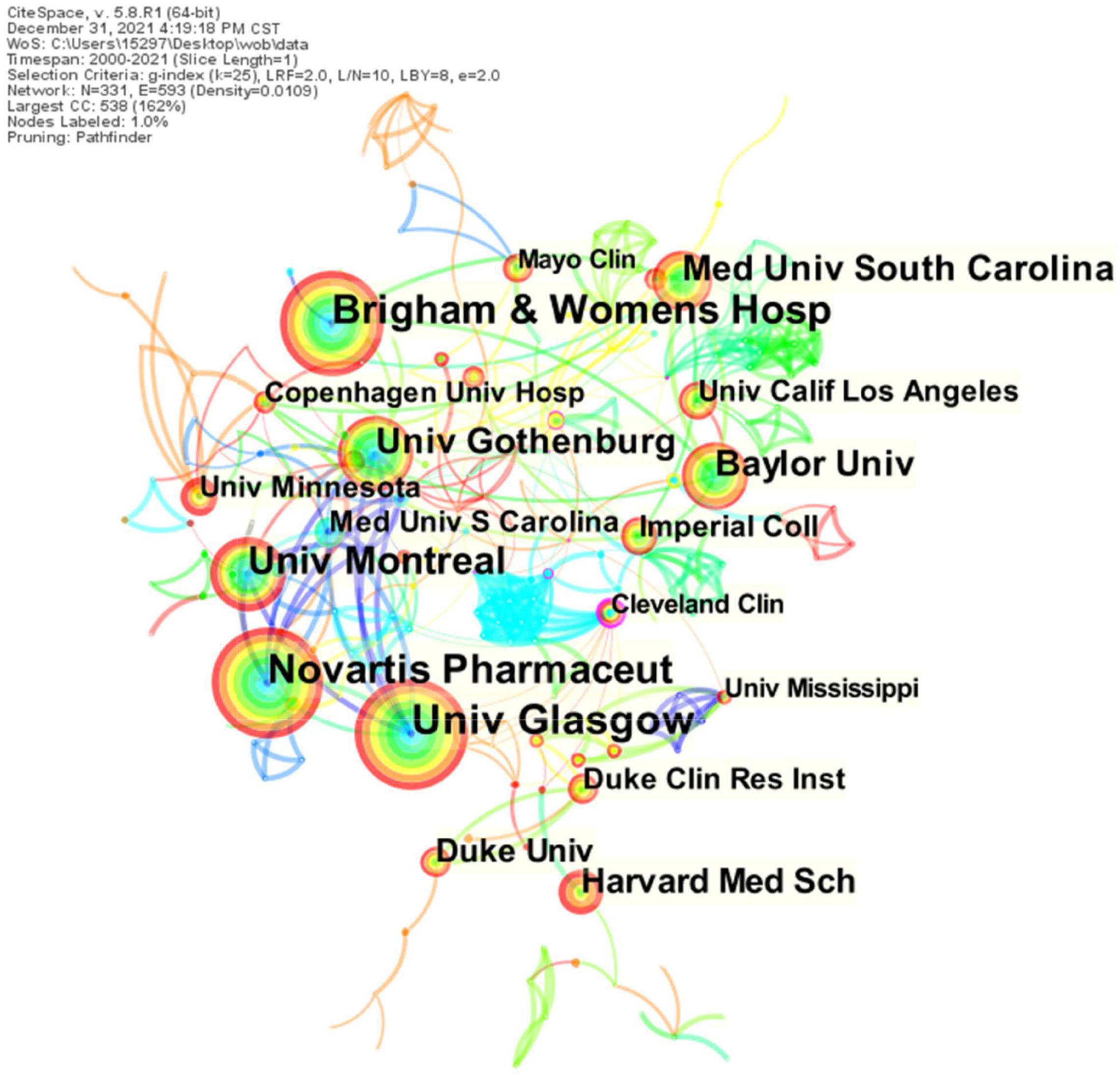
Figure 3. CiteSpace visualization of institutions participating in ARNI’s research in the cardiovascular system. The circular nodes represent institutions; the links between nodes represent interactions between institutions.
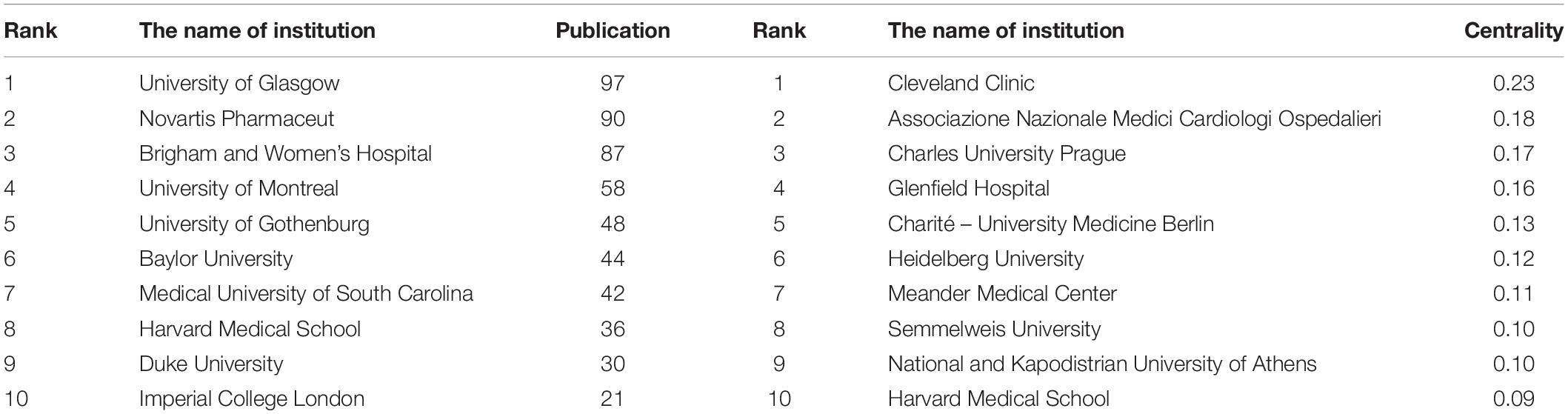
Table 2. Top 10 institutions involved in ARNI cardiovascular system research in terms of volume and centrality of publications.
A total of 402 authors published articles on ARNI in cardiovascular system research, with the three most prolific authors being Scott D. Solomon (75 articles), Milton Packer (65 articles) and John Joseph Valentine McMurray (61 articles) (Figure 4A and Table 3). Of note is the relatively low centrality of authors (<0.03), indicating that the impact of authors on ARNI research in the cardiovascular system needs to be improved, with each node representing one author and the larger the node the more articles published. The thicker lines represent closer collaboration between authors, and it is clear from Figure 4A that there is communication and collaboration between authors in the field. Co-cited authors are those authors who are co-cited in publications, and co-citation is a key indicator of author contribution (27). The top 10 co-cited authors are shown in Figure 4B and Table 4, only nine authors have more than 100 citations, with John Joseph Valentine McMurray (403) ranked first, followed by Milton Packer (225), Clyde W. Yancy (202) and Scott D. Solomon (198). The highest centrality was Konstam M. A. (0.38), Massie B. M. (0.32), and Cohn J. N. (0.31). John Joseph Valentine McMurray, an early investigator of ARNI studies in the cardiovascular system, conducted the PARADIGM-HF study (28) in 2013, showing that LCZ696, compared with the high-dose ACEI analog enalapril, was associated with a reduction in cardiovascular mortality and the primary endpoint (the composite endpoint of cardiovascular death and heart failure hospitalization). Based on this study, in 2014 the Canadian Cardiovascular Society (CCS) (29) updated its guidelines for the management of patients with heart failure, recommending for the first time a dual angiotensin receptor and enkephalinase inhibitor (ARNI). In the United States, Prof. Scott D. Solomon has been a driving force in this field for more than 10 years, conducting studies on the therapeutic role of sacubitril valsartan in heart failure and accelerating the use and dissemination of this drug in clinical care. However, their low centrality indicates that they have less interaction with other authors and do not play an important role in expanding their knowledge to other authors.
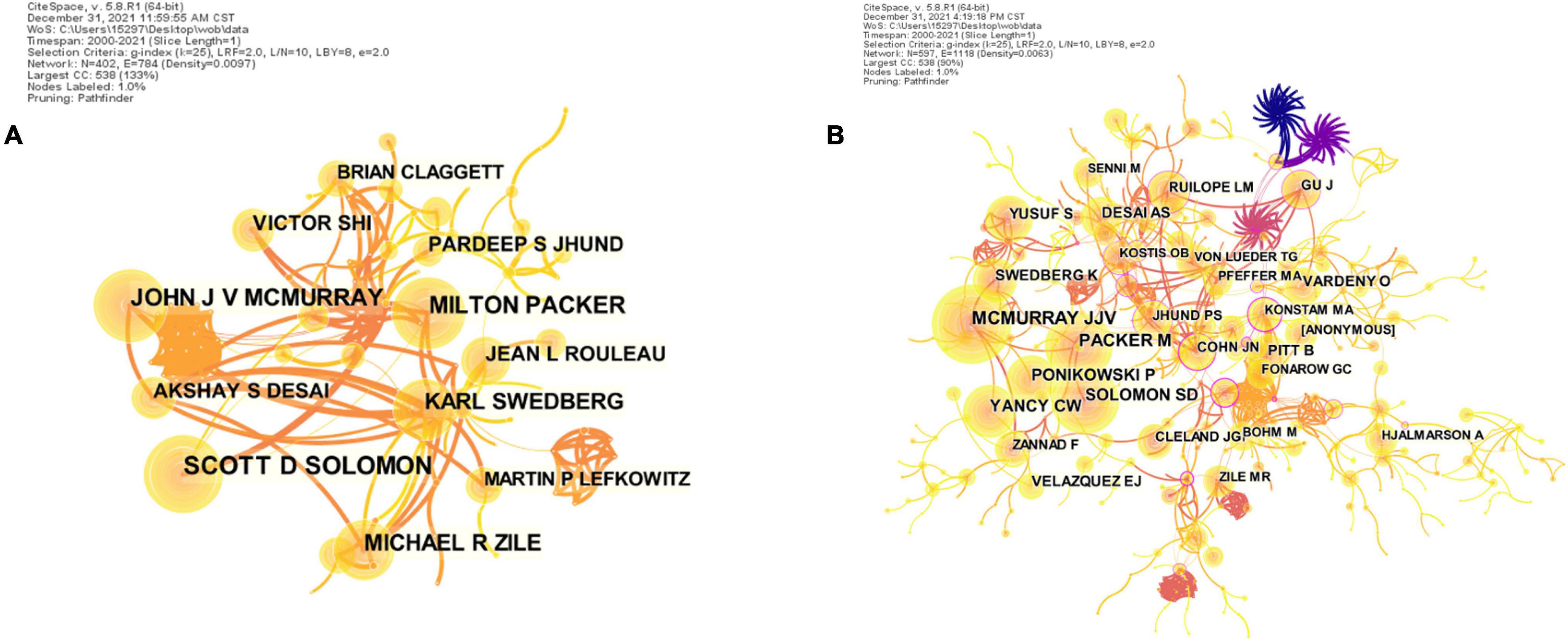
Figure 4. CiteSpace visualization of the authors (A) and co-cited authors (B) involved in ARNI research in the cardiovascular system. Circle node represent author of papers; link between nodes represent partnerships.
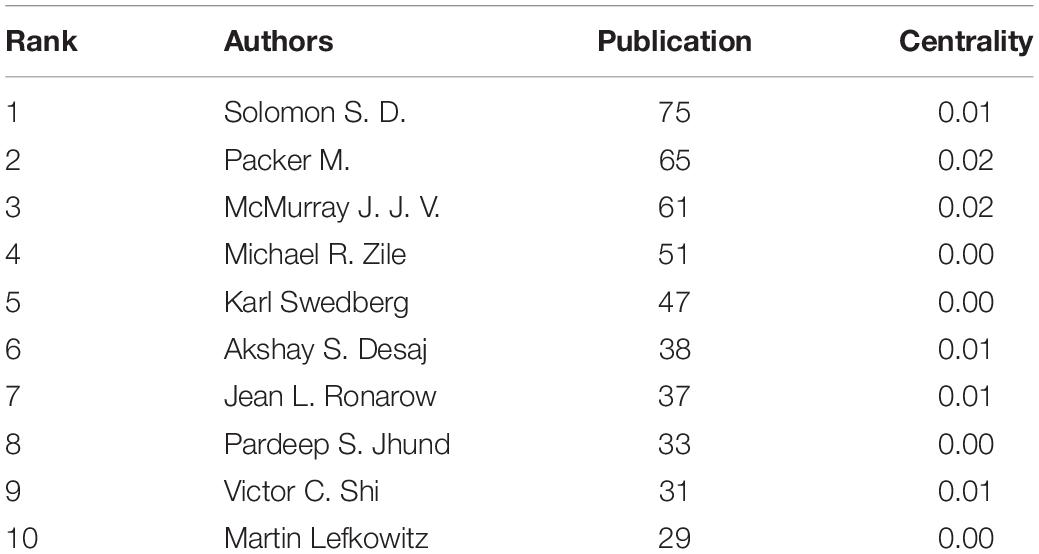
Table 3. Top 10 authors in terms of number and centrality of articles related to ARNI in cardiovascular system research.
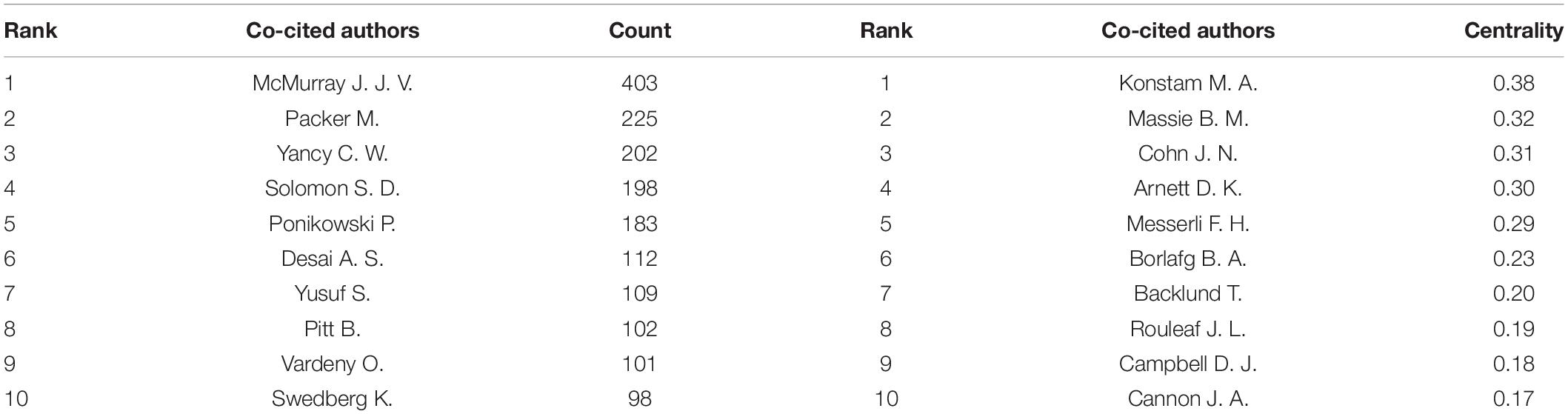
Table 4. Top 10 co-cited authors in terms of number and centrality of articles related to ARNI in cardiovascular system research.
All articles on ARNI research in the cardiovascular field were published in a total of 102 journals. The top 5 most cited journals and the top 5 journals with the highest centrality were found through journal co-citation co-presentation shown in Table 3, New England Journal of Medicine (452 total citations) was the most prolific journal followed by Cirulation (413 total citations) and Journal of the American College of Cardiology (377 total citations). The journal with the highest centrality was American Journal of Hypertension (0.37), followed by American Heart Journal (0.12), and Journal of Cardiovascular Medicine (0.10) (Figure 5 and Table 5), all three with good centrality (≥0.01), indicating that they are the more influential journals. The double map overlay shows the two main citation paths. The published articles were concentrated in journals in the fields of medicine, medical, and clinical, while the cited articles were mostly published in journals in the fields of molecular, biology, genetics, health, nursing, and medicine (Figure 6).
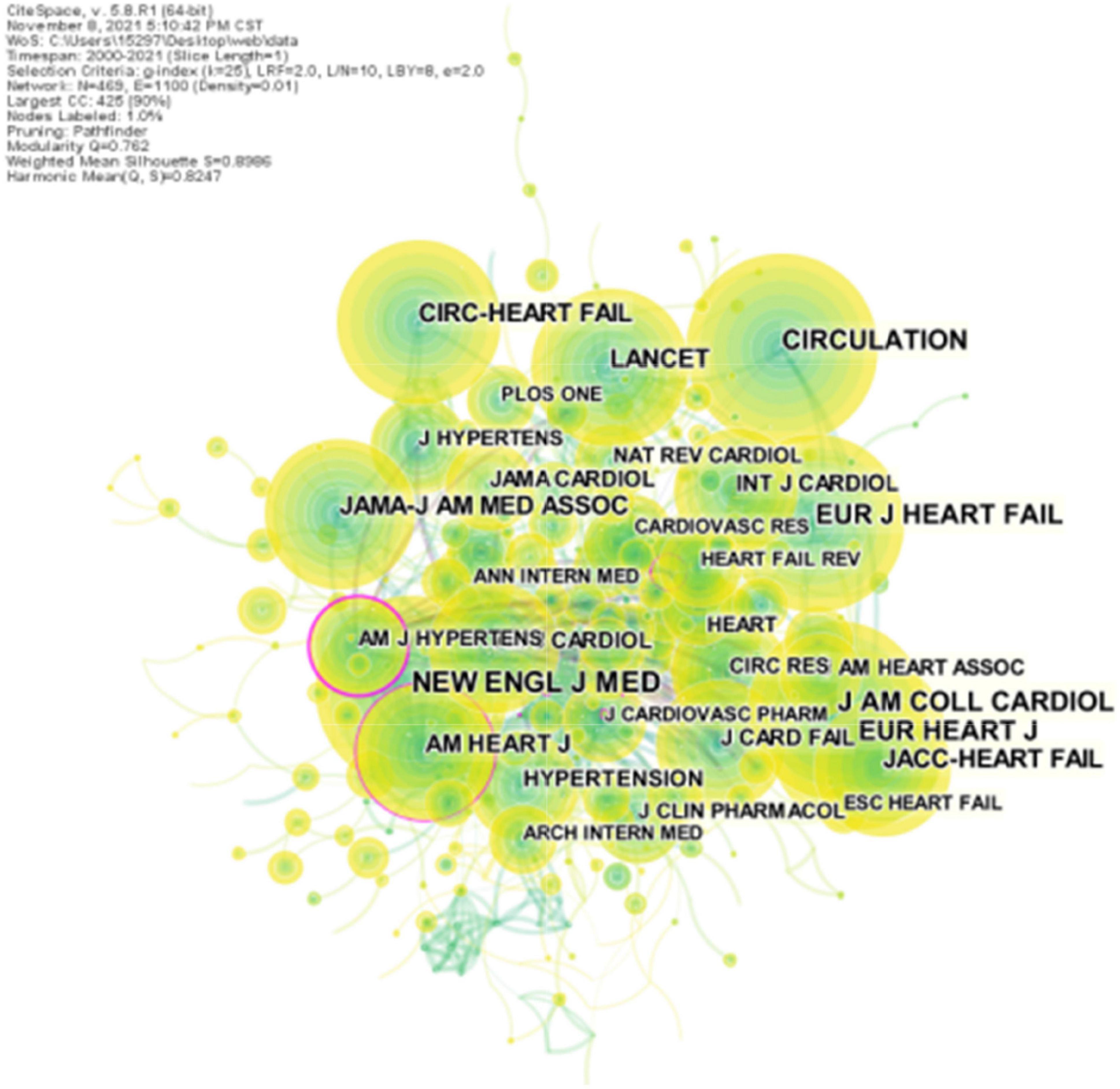
Figure 5. CiteSpace visualization of co-cited journals involved in ARNI research in the cardiovascular system. The circle nodes represent co-cited journals; the links between nodes represent interdisciplinary interactions in the literature.

Table 5. The top 5 core and the top five centrality journals on ARNI study in the cardiovascular system.
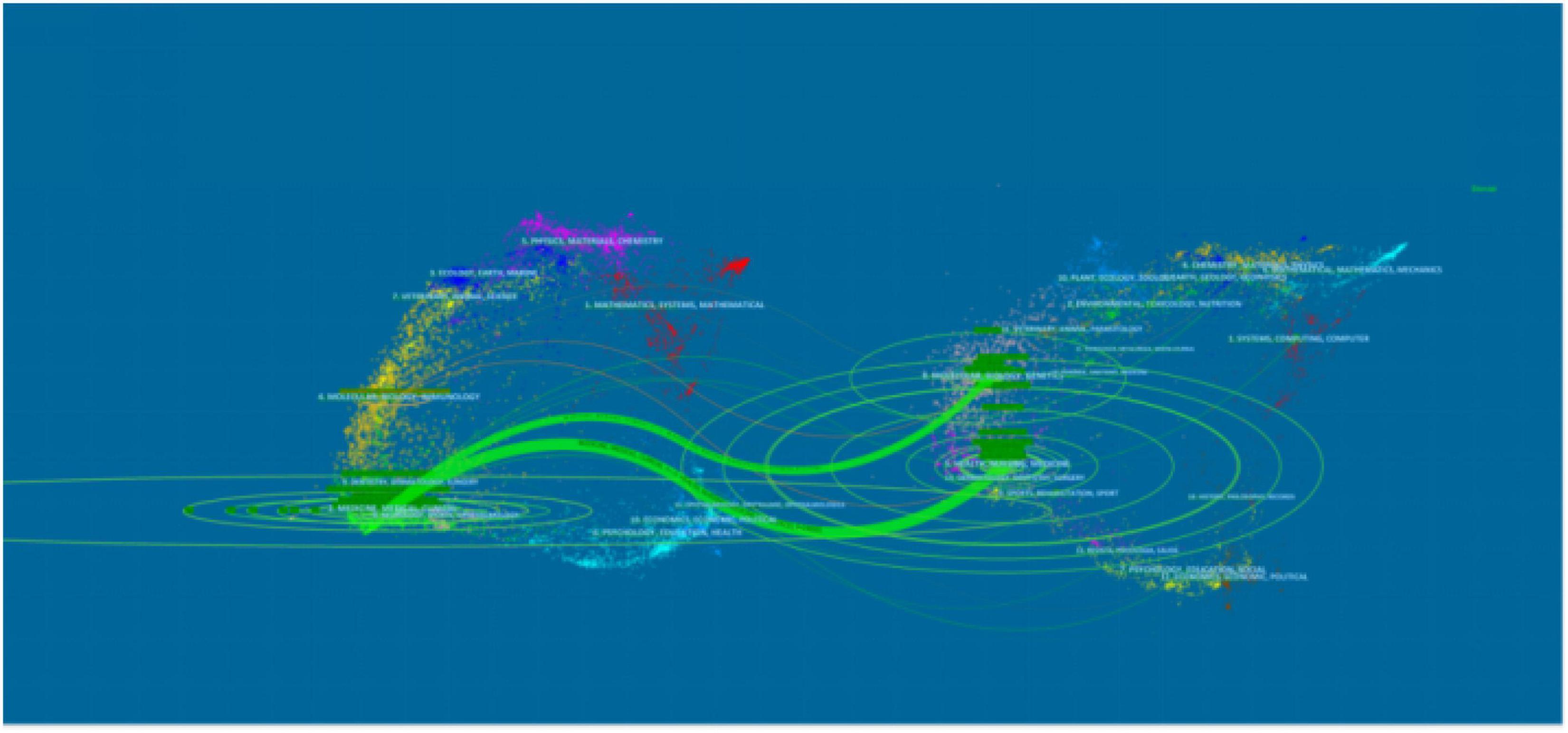
Figure 6. The dual-map overlay of citations of articles on the application of ARNI in the cardiovascular field (The left side were the citing journal, the right side were the cited journal, and the line path represents the citation relationship).
Keywords are condensed and extracted from the content of an article to reflect the topic and content of the representative article, and high-frequency keywords are often used to reflect hot issues in the research field (30). Keyword co-occurrence network is a text content-based analysis method, and we extracted 383 keywords at the time of data collection (Figure 7A), and the top 25 most cited keywords were found by keyword burst (Figure 7B); the blue line represents the time interval, and the red segment represents the burst cycle time of the keywords; from the figure, we can see that the burst keywords are mainly focused on ARNI and the treatment of related disease studies, angiotensin II, angiotensin receptor neprilysin inhibitor, randomized trial, heart failure trial, neutral endopeptidase inhibition, global mortality began to break out in the early stages. Thereafter fibrosis, systolic hypertension, and PARADIGM-HF trials began to explode; in recent years, sacubitril-valsartan, and left ventricular ejection fraction have become new keywords for the outbreak.
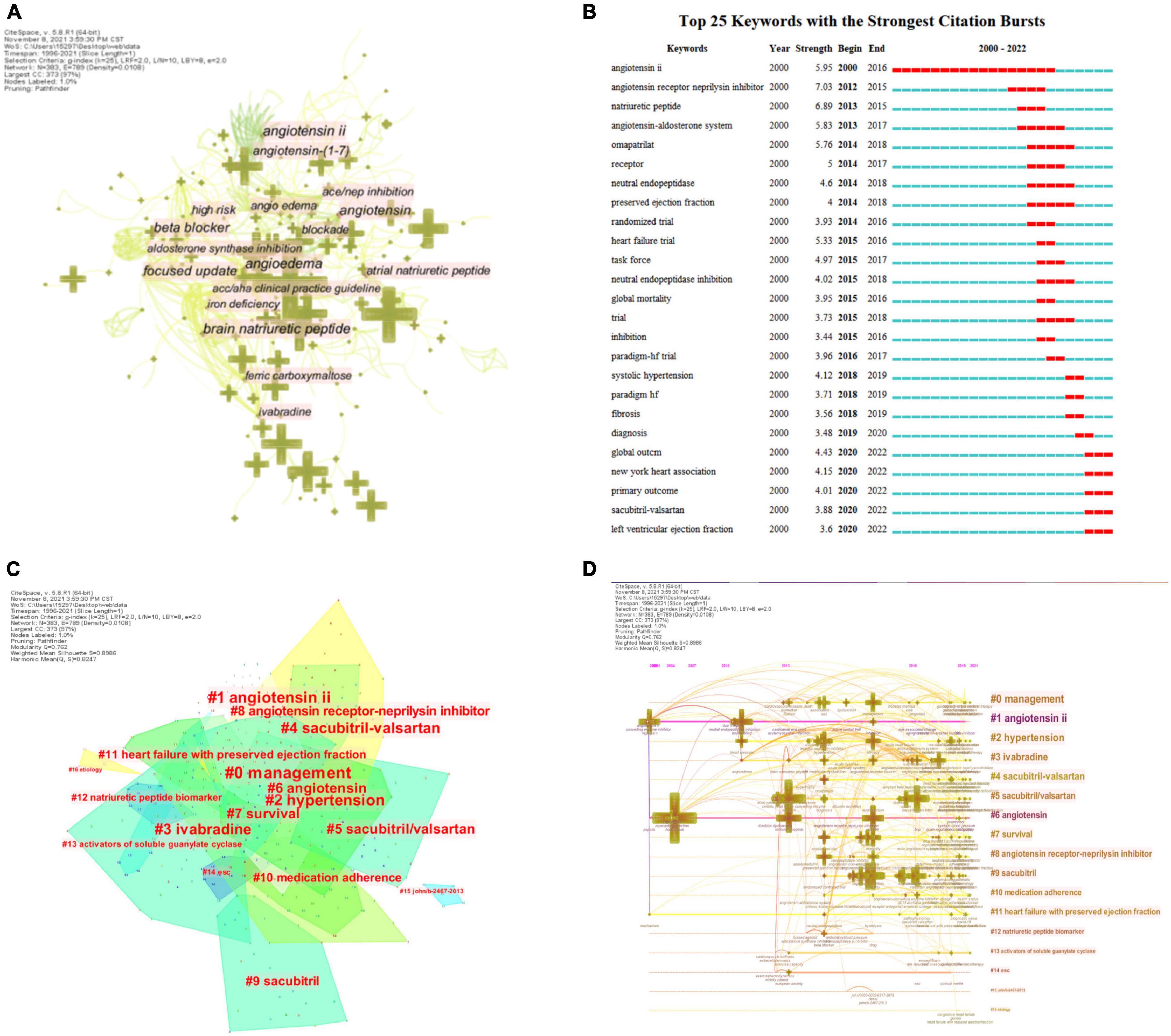
Figure 7. CiteSpace visualization of keywords involved in ARNI research in the cardiovascular system. (A) Network of the main keywords in publications on ARNI in cardiovascular system research and related research. (B) Time trend graph of burst keywords. (C) Cluster analysis of keywords. (D) The timeline view of Keyword clusters.
Clustering analysis based on log likelihood ratio (LLR) revealed a total of 17 clusters with a modularity Q of 0.762 and a mean profile value of 0.8986, showing good homogeneity (31). They contain a large number of concerns of ARNI research in the cardiovascular field, including drugs [#1 angiotensin II (32), #3 ivabradine (33), #4 sacubitril-valsartan (34), #5 sacubitril/valsartan (35), #6 angiotensin (36), #8 angiotensin receptor-neprilysin inhibitor (37), #9 sacubitril (38)], indications [#2 hypertension (39), #11 heart failure with preserved ejection fraction (40)], management [#0 management (41)], guidelines [#14 ESC (42)], etiology [#16 etiology (43)], and observables [#7 survival (44), #10 medication adherence (45), #12 natriuretic peptide biomarkers (46)] (Figures 7C,D). In recent years, due to the emergence of some important new evidence-based medicine for heart failure drugs, the 2021 ESC guidelines (47) have been updated in this regard, and the status of ARNI has been importantly elevated to become the first-line drug for heart failure treatment, which brings hope for the treatment of heart failure patients. Not only that, several clinical studies in recent years have found that ARNI, represented by sacubitril valsartan, has good therapeutic effects in lowering blood pressure as a new generation drug, and its mechanism of action mainly includes diuretic, natriuretic, vasodilator and anti-sympathetic activity (48–53). Based on this, the 2020 International Society of Hypertension (ISH) Global Hypertension Practice Guidelines first recommended it as the preferred antihypertensive treatment for heart failure patients, bringing new hope for the treatment of hypertensive patients.
Co-citation analysis was proposed by Small and later introduced to the co-citation analysis of references, the phenomenon that two or more references are cited in the same literature (54), and the analysis of literature with higher co-citation frequency and centrality can obtain the disciplinary research base, which was obtained after CiteSpace analysis for the last 21 years of ARNI and The visualization of the co-cited literature in the field of cardiovascular disease-related research for the last 21 years (N = 631, E = 1264). N denotes nodes/number and E denotes the concatenation of objects between nodes. As can be seen, N = 631 and E = 1264 in the co-cited literature mapping, indicating that there are 631 co-cited References included in the mapping, each node represents a co-cited literature, and the line between the nodes represents the cross-citation between references, indicating that there are 1,264 citations between references. As shown in Figure 8, in which the circular nodes represent references, and the larger the node, the higher the citation frequency of the reference literature. Of the top 10 co-cited articles, 8 were clinical studies and 2 were guidelines for the management of heart failure (Table 6). The clinical studies focused on the safety and efficacy of ARNI in the treatment of patients with various types of heart failure, and their pharmacokinetics and pharmacodynamics were investigated. It can be seen that the study of the therapeutic effects of ARNI in heart failure remains a major aspect of current research.
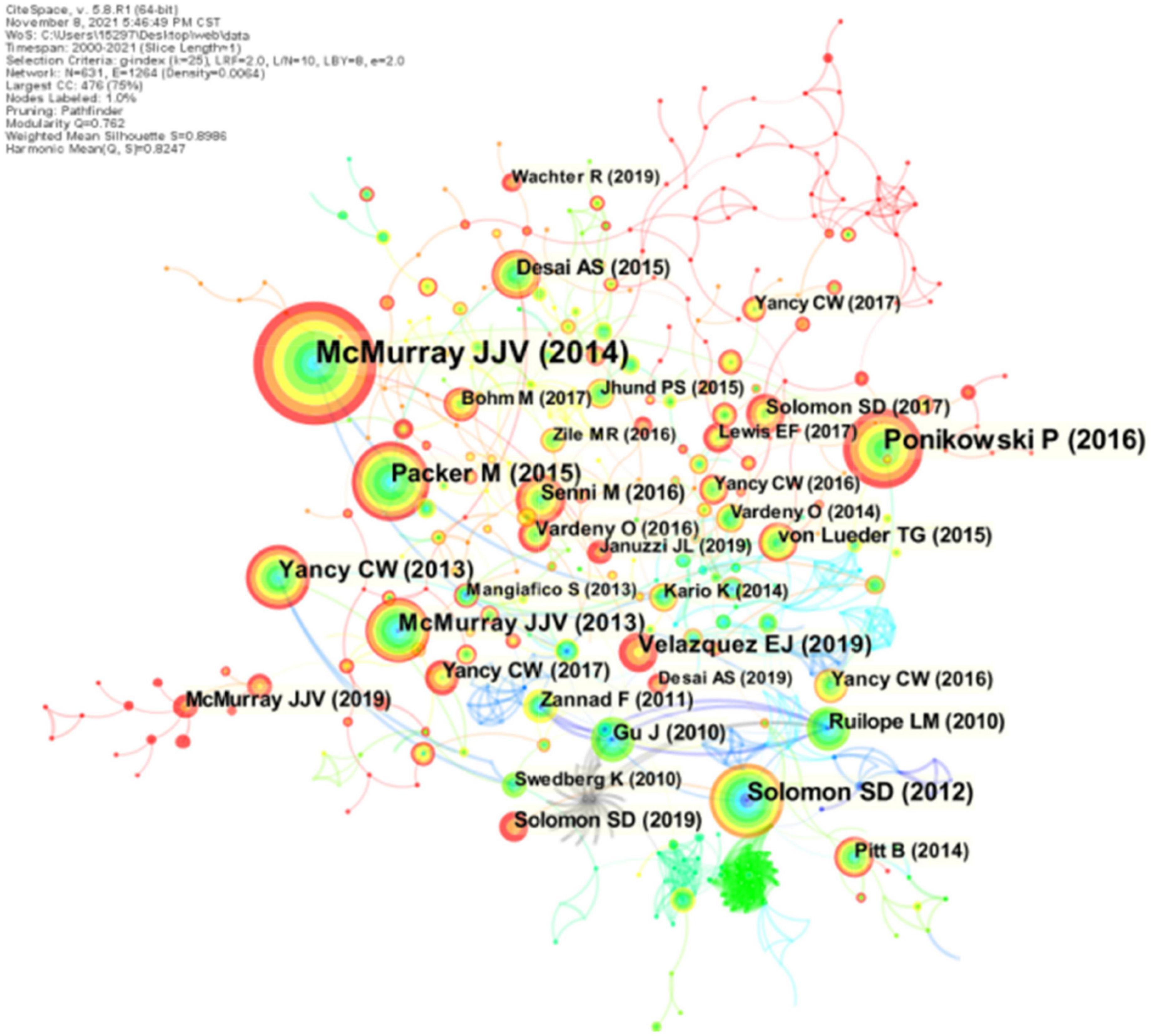
Figure 8. CiteSpace visualization of the co-cited reference involved in ARNI studies in the cardiovascular system. Circle node represents reference; the line between the nodes indicates the frequency of the two references being cited at the same time. The betweenness centrality of the nodes with red circle is >0.1.
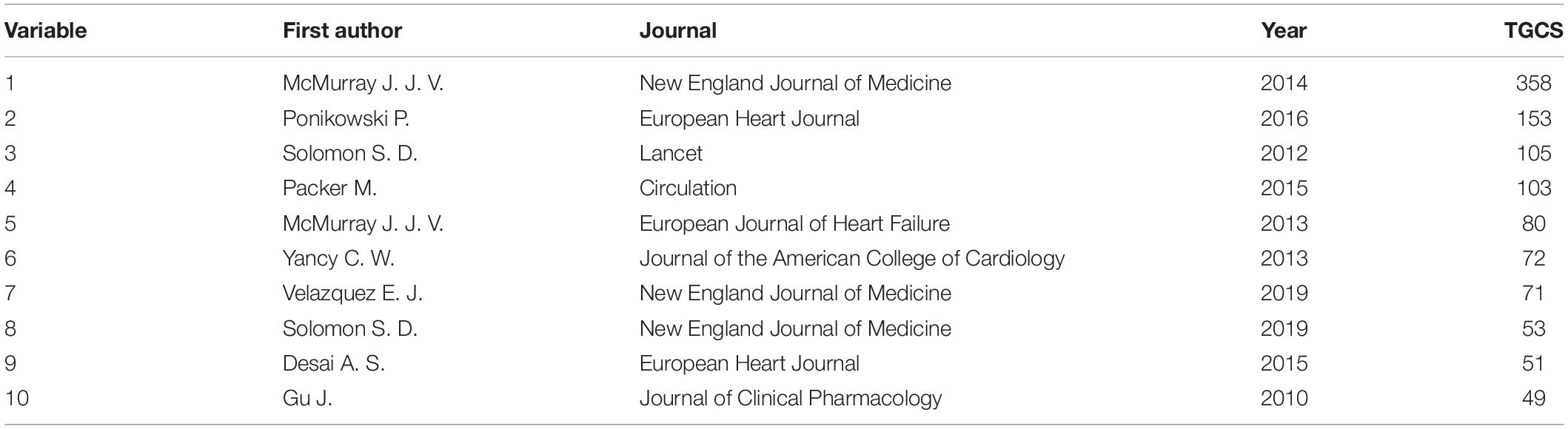
Table 6. Top 10 most cited papers.
A subsequent cluster analysis of the cited references identified 16 clusters with a modularity Q of 0.8492 and an average profile value of 0.9537 (Figure 9A and Table 7). Based on this, a visual timeline was executed for the clusters, combining clustering and time slicing techniques to not only reflect the distribution of topics in the field, but also to depict the trends and interconnections of the research topics over time (Figure 9B). The blue and green colors in the figure indicate literature from earlier times, while the yellow and red nodes represent more recent literature. As seen in the figure, early studies focused on the therapeutic mechanisms, indications and possible adverse effects of ARNI in cardiovascular disease (Cluster #4, Cluster #6–10). With the accumulation of strong evidence, this question has been largely answered and the focus of research has therefore shifted to the designation of therapeutic specifications for ARNI in cardiovascular disease (cluster #0) and new combination therapeutics (cluster #16), among others. Notably, in recent years SGLT2i, a novel agent, has been shown to increase urinary glucose excretion, urinary sodium excretion and osmotic diuresis, improve myocardial energy metabolism, inhibit sympathetic activity, modulate the cardiac inflammatory response, improve ventricular remodeling, and improve cardiac function, with benefits for the cardiac-renal-metabolic system (55). 2021 ESC guidelines (29) even emphasize that all HFrEF patients should receive a combination of four drugs: ACEI/ARNI, β-blocker (BB), aldosterone receptor antagonist (MRA), and SGLT2. In conclusion, the co-citation analysis of ARNI references in the cardiovascular field is a way to learn more about the evolution and hotspots of this research field and helps to identify the core topics and concerns in the field.
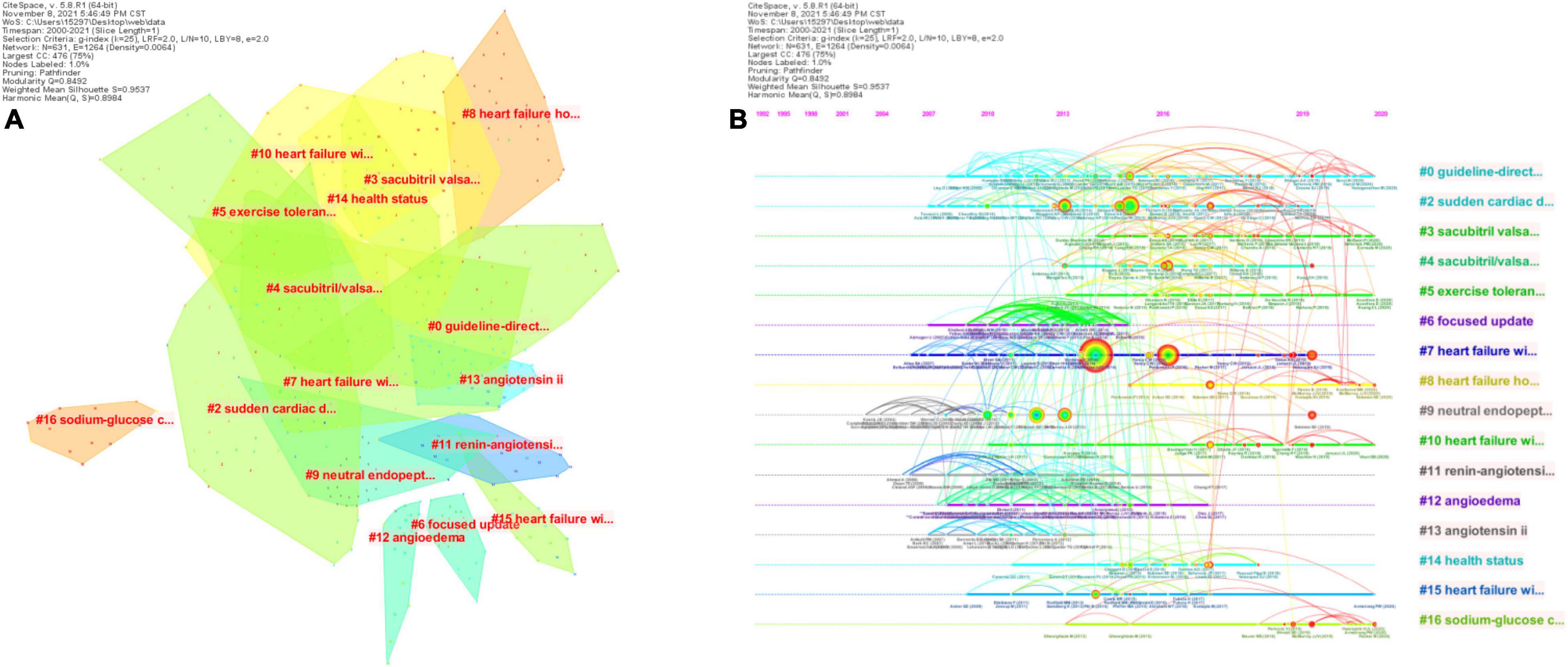
Figure 9. CiteSpace visualization of the cluster analysis of the co-cited literature involved in ARNI studies in the cardiovascular system. (A) Cluster analysis of co-cited references; (B) Timeline distribution of clusters.
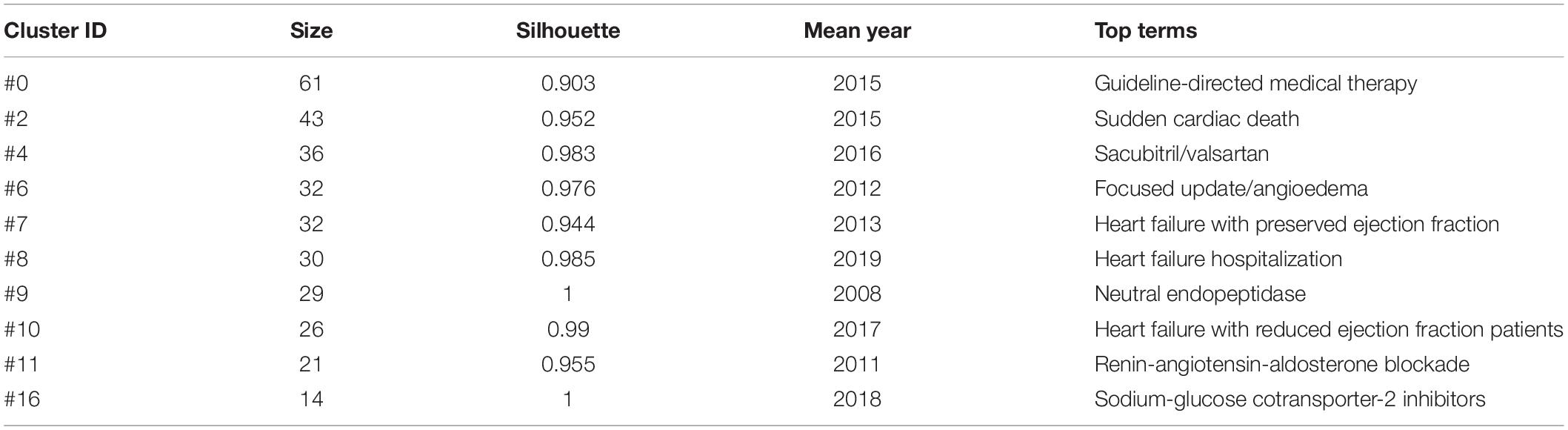
Table 7. The 10 co-cited reference clusters of ARNI studies in the cardiovascular system.
This study analyzed the knowledge hotspots and new development trends of ARNI research in the cardiovascular field using bibliometric methods, and found that the number of publications in this field showed a yearly increase and entered a more mature stage of development, but there is still an imbalance in its development between regions and countries, with only one developing country, China, among the top 10 countries in terms of the number of publications, which indicates that the research in this field in the past 20 This indicates that Chinese research in this field has made great progress over the past 20 years. However, the vast majority of research is concentrated in developed countries such as the United States, the United Kingdom, and Canada, and accordingly these countries have formed several of the most active academic groups, with Prof. Scott D. Solomon’s group at Brigham and Women’s Hospital in the United States, Prof. Milton Packer’s group at Baylor University Medical Center in Dallas, and Prof. John G. G. Gutierrez’s group at University of Glasgow in the United Kingdom, but the low centrality of these authors suggests that they do not play a significant role in expanding their knowledge to other authors, and therefore communication and collaboration between authors should be enhanced to promote the field.
The top three journals in terms of IF are New England Journal of Medicine (IF 2021 = 91.24), Lancet (IF 2021 = 79.321) and JAMA- Journal of the American Medical Association (IF 2021 = 56.272). It is suggested that ARNI research articles in the cardiovascular field are mainly published in journals with higher impact factors and they are cited more frequently. IF is a quantitative indicator representing the impact size of journals, reflecting the citation rate, academic level and paper quality, indicating that research papers in this field are of high quality and provide strong evidence for the clinical application of the drug.
According to the analysis, we got that ARNI research in the field of heart failure is the main research direction, and there are three important points in its development history, the first one is the 2014 Canadian Cardiovascular Society (CCS) updated the guidelines for the management of heart failure patients based on the results of the PARADIGM-HF study, which for the first time The second is the update of the 2016 ACC/AHA/HFSA (56) heart failure guidelines, based on the results of the PARADIGM trial, which recommended ARNI as a class I drug, the first time recommending ARNI as an alternative to ACEI therapy for patients with poor outcomes. Drug for reducing mortality in some patients with chronic heart failure (HFrEF). This guideline update not only upgraded the recommendation level of ARNI class of drugs in the cardiovascular field, but also clearly indicated the scope of application of the drug, providing clearer guidance for clinical use; the third is a major update of the 2021 ESC heart failure guideline based on the PIONEER-HF study (57) and the PARAGON-HF study (40), which strengthened the first-line recommendation of ARNI status, with sacubitril valsartan available as a starting drug in HFrEF patients who have not previously used an ACEI and, for the first time, including sacubitril valsartan as a therapeutic agent for HFmrEF, and with the PARAGON-HF study confirming that ARNI reduces the composite endpoint of heart failure hospitalization and cardiovascular death in HFpEF patients by 13%. With the approval of the HFpEF indication by the FDA, this makes ARNI the only class of drugs that can treat total ejection fraction heart failure, broadening the therapeutic scope of the drug and thus better guiding clinical practice.
As research on this class of drugs continues, the effectiveness of ARNI in the treatment of other cardiovascular diseases is becoming a topic of interest for researchers, with an important keyword cluster being hypertension. Notably, the first antihypertensive study of ARNI was published in Lancet in 2010, and its results showed that ARNI could dose-dependently lower patients’ blood pressure and was superior to valsartan (58). Several subsequent studies have found that ARNI is not only effective in controlling blood pressure, but also improves it in patients with hypertension combined with left ventricular hypertrophy, coronary artery disease, and chronic kidney disease. For example, the EVALUATE-HF study and the PROVE-HF study found that sacubitril valsartan treatment of HFrEF patients resulted in rapid improvement of cardiac remodeling indexes such as left ventricular end-systolic volume index (LVESVi), left ventricular end-diastolic volume index (LVEDVi), left atrial volume index (LAVI), and left ventricular mass index (LVMI), with 1 year of treatment consistently reversing cardiac remodeling (59, 60). Subgroup analysis of the PARADIGM-HF study showed that sacubitril valsartan significantly reduced the risk of the composite coronary endpoint (cardiovascular death, non-fatal myocardial infarction, unstable angina, other angina hospitalization, or coronary revascularization) by up to 17% compared with ACEI (46). In a study of an Asian population with hypertension combined with CKD, sacubitril valsartan reduced systolic blood pressure by 20.5 mm Hg and urinary albumin/creatinine ratio (UACR) by a significant 15.1% in patients with hypertension combined with CKD (61). In the future, it is believed that sacubitril valsartan will fill more gaps in the full management of the cardiovascular event chain, giving full benefits to cardiovascular patients.
This study is based on the high morbidity and mortality of cardiovascular disease and the serious economic burden it brings to study the value of the application of ARNI. Through this study, it is found that ARNI can effectively improve the long-term prognosis of patients with cardiovascular disease, and at the same time, the drug can act on the whole course of cardiovascular events, helping to delay the progression of the disease and reduce the occurrence of adverse cardiovascular events. The use of this drug can also improve the quality of life of such patients, reducing the costs required for hospitalization and care, and reducing the economic burden on families and society. This shows that the study of this drug in the cardiovascular system brings real economic benefits and social impact.
There are also certain shortcomings in this study. First, this study mainly uses Web of Science core database for literature search, although it enriches the search strategy as much as possible, there is still a possibility that relevant literature is not included; in addition, this study mainly uses CiteSpace for literature analysis, and the difference in the quality of the retrieved literature data will lead to a reduction in the quality and credibility of the plotted images, and combining the two methods of CiteSpace and VOSviewer can provide a more accurate analysis of the literature.
The bibliometric analysis revealed a promising research landscape for ARNI in the cardiovascular field with a significant increase in related publications. The main contributors to this research area were clearly identified, and it was found that the relevant literature mainly focuses on the application of ARNI in heart failure, hypertension and other diseases, which may benefit in the future throughout the cardiovascular event chain. However, regional and national differences still exist, and there is a need to strengthen cooperation between countries. It is hoped that this study will lead to a greater understanding of the prospects of ARNI in the cardiovascular field and promote its clinical application for better treatment and prognosis of CVD patients.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author/s.
Written informed consent was not obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
QS, XX, and SS devised the research plan and established the methodology. XX, SS, YL, JL, and YW wrote the original draft. HZ and XM were in charge of software, literature retrieval, and visualization. HW, BZ, and XX modified and polished the manuscript. All authors contributed to the article and approved the submitted version.
This work was supported by the National Natural Science Foundation of China (81904191 and 82004348), Guang’anmen Hospital of China Academy of Chinese Medical Sciences (2018S420), and Capital Health Development Research Special Project (2020-2-4153).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
We wish to thank Prof. Chaomei Chen for developing CiteSpace and making it freely available to the public.
1. Amini M, Zayeri F, Salehi M. Trend analysis of cardiovascular disease mortality, incidence, and mortality-to-incidence ratio: results from global burden of disease study 2017. BMC Public Health. (2021) 21:401. doi: 10.1186/s12889-021-10429-0
2. GBD 2017 Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990-2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. (2018) 392:1789–858. doi: 10.1016/S0140-6736(18)32279-7
4. Dunbar SB, Khavjou OA, Bakas T, Hunt G, Kirch RA, Leib AR, et al. Projected costs of informal caregiving for cardiovascular disease: 2015 to 2035: a policy statement from the American Heart Association. Circulation. (2018) 137:e558–77. doi: 10.1161/CIR.0000000000000570
5. Hubers SA, Brown NJ. Combined angiotensin receptor antagonism and neprilysin inhibition. Circulation. (2016) 133:1115–24. doi: 10.1161/CIRCULATIONAHA.115.018622
6. Yamamoto K, Rakugi H. Angiotensin receptor-neprilysin inhibitors: comprehensive review and implications in hypertension treatment. Hypertens Res. (2021) 44:1239–50. doi: 10.1038/s41440-021-00706-1
7. Anderson SL, Marrs JC. Sacubitril/valsartan: evaluation of safety and efficacy as an antihypertensive treatment. Drugs Context. (2018) 7:212542. doi: 10.7573/dic.212542
8. Sutanto H, Dobrev D, Heijman J. Angiotensin receptor-neprilysin inhibitor (ARNI) and cardiac arrhythmias. Int J Mol Sci. (2021) 22:8994. doi: 10.3390/ijms22168994
9. Tsai YN, Cheng WH, Chang YT, Hsiao YW, Chang TY, Hsieh YC, et al. Mechanism of angiotensin receptor-neprilysin inhibitor in suppression of ventricular arrhythmia. J Cardiol. (2021) 78:275–84. doi: 10.1016/j.jjcc.2021.04.011
10. Liu J, Zheng X, Zhang C, Zhang C, Bu P. Lcz696 Alleviates Myocardial Fibrosis After Myocardial Infarction Through the sFRP-1/Wnt/β-Catenin Signaling Pathway. Front Pharmacol. (2021) 12:724147. doi: 10.3389/fphar.2021.724147
11. She J, Lou B, Liu H, Zhou B, Jiang GT, Luo Y, et al. ARNI versus ACEI/ARB in reducing cardiovascular outcomes after myocardial infarction. ESC Heart Fail. (2021) 8:4607–16. doi: 10.1002/ehf2.13644
12. Seferovic JP, Solomon SD, Seely EW. Potential mechanisms of beneficial effect of sacubitril/valsartan on glycemic control. Ther Adv Endocrinol Metab. (2020) 11:2042018820970444. doi: 10.1177/2042018820970444
13. Esser N, Zraika S. Neprilysin inhibition: a new therapeutic option for type 2 diabetes? Diabetologia. (2019) 62:1113–22. doi: 10.1007/s00125-019-4889-y
14. Esser N, Paquot N. Intérêt de la combinaison sacubitril/valsartan dans le diabète de type 2 [Potential role of sacubitril/valsartan combination in type 2 diabetes]. Rev Med Suisse. (2021) 17:1418–22. doi: 10.53738/revmed.2021.17.747.1418
15. Roksnoer LC, van Veghel R, Clahsen-van Groningen MC, de Vries R, Garrelds IM, Bhaggoe UM, et al. Blood pressure-independent renoprotection in diabetic rats treated with AT1 receptor-neprilysin inhibition compared with AT1 receptor blockade alone. Clin Sci. (2016) 130:1209–20. doi: 10.1042/CS20160197
16. Falagas ME, Pitsouni EI, Malietzis GA, Pappas G. Comparison of PubMed, Scopus, Web of Science, and Google Scholar: strengths and weaknesses. FASEB J. (2008) 22:338–42. doi: 10.1096/fj.07-9492LSF
17. Martín-Martín A, Orduna-Malea E, Thelwall M, Delgado López-Cózar E. Google scholar, web of science, and scopus: a systematic comparison of citations in 252 subject categories. J Informetr. (2018) 12:1160–77. doi: 10.1016/j.joi.2018.09.002
18. Chen CM. Searching for intellectual turning points: progressive knowledge domain visualization. Proc Natl Acad Sci USA. (2004) 101:5303–10. doi: 10.1073/pnas.0307513100
19. Synnestvedt MB, Chen C, Holmes JH. CiteSpace II: visualization and knowledge discovery in bibliographic databases. AMIA Annu Symp Proc. (2005) 2005:724–8.
20. van Eck NJ, Waltman L. Software survey: VOSviewer, a computer program for bibliometric mapping. Scientometrics. (2010) 84:523–38. doi: 10.1007/s11192-009-0146-3
21. Donnelly JP. A. systematic review of concept mapping dissertations. Eval Program Plann. (2017) 60:186–93. doi: 10.1016/j.evalprogplan.2016.08.010
22. Chen CM, Hu Z, Liu S, Tseng H. Emerging trends in regenerative medicine: a scientometric analysis in CiteSpace. Expert Opin Biol Ther. (2012) 12:593–608. doi: 10.1517/14712598.2012.674507
23. Chen C. The centrality of pivotal points in the evolution of scientific networks. In: Proceedings of the International Conference on Intelligent User Interfaces (IUI 2005). New York, NY: ACM Press (2005). p. 98–105. doi: 10.1145/1040830.1040859
24. Liu T, Yang L, Mao H, Ma F, Wang Y, Zhan Y. Knowledge domain and emerging trends in podocyte injury research from 1994 to 2021: a bibliometric and visualized analysis. Front Pharmacol. (2021) 12:772386. doi: 10.3389/fphar.2021.772386
25. Yuan G, Shi J, Jia Q, Shi S, Zhu X, Zhou Y, et al. Cardiac rehabilitation: a bibliometric review from 2001 to 2020. Front Cardiovasc Med. (2021) 8:672913. doi: 10.3389/fcvm.2021.672913
26. Chen C. Science mapping: a systematic review of the literature. J Data Inf Sci. (2017) 2:1–40. doi: 10.1515/jdis-2017-0006
27. Chen D, Zhang G, Wang J, Chen S, Wang J, Nie H, et al. Mapping trends in moyamoya angiopathy research: a 10-year bibliometric and visualization-based analyses of the Web of Science Core Collection (WoSCC). Front Neurol. (2021) 12:637310. doi: 10.3389/fneur.2021.637310
28. McMurray JJ, Packer M, Desai AS, Gong J, Lefkowitz MP, Rizkala AR, et al. Dual angiotensin receptor and neprilysin inhibition as an alternative to angiotensin-converting enzyme inhibition in patients with chronic systolic heart failure: rationale for and design of the Prospective comparison of ARNI with ACEI to Determine Impact on Global Mortality and morbidity in Heart Failure trial (PARADIGM-HF). Eur J Heart Fail. (2013) 15:1062–73. doi: 10.1093/eurjhf/hft052
29. Canadian Cardiovascular Society [CCS]. CCS Heart Failure Guidelines: 2014 update on new therapies, biomarkers, and anemia management. Can Cardiovasc Congress. (2014).
30. Shi JJ, Bo RQ, Hu YH, Qiu ZL, Chu YG, Song QQ, et al. Visual analysis of the relationship between atherosclerosis and immune response study based on CiteSpace V. J Integr Med Cardiovasc Dis. (2019) 17:33–9.
31. Chen C. CiteSpace II: detecting and visualizing emerging trends and transient patterns in scientific literature. J Am Soc Inf Sci Tech. (2006) 57:359–77. doi: 10.1002/asi.20317
32. Clements RT, Vang A, Fernandez-Nicolas A, Kue NR, Mancini TJ, Morrison AR, et al. Treatment of Pulmonary Hypertension With Angiotensin II Receptor Blocker and Neprilysin Inhibitor Sacubitril/Valsartan. Circ Heart Fail. (2019) 12:e005819. doi: 10.1161/CIRCHEARTFAILURE.119.005819
33. Gordin JS, Fonarow GC. New medications for heart failure. Trends Cardiovasc Med. (2016) 26:485–92. doi: 10.1016/j.tcm.2016.02.008
34. Nordberg Backelin C, Fu M, Ljungman C. Early experience of Sacubitril-Valsartan in heart failure with reduced ejection fraction in real-world clinical setting. ESC Heart Fail. (2020) 7:1049–55. doi: 10.1002/ehf2.12644
35. Sciatti E, Senni M, Lombardi CM, Gori M, Metra M. Sacubitril/valsartan: from a large clinical trial to clinical practice. J Cardiovasc Med. (2018) 19:473–9. doi: 10.2459/JCM.0000000000000687
36. Huo JY, Jiang WY, Chen C, Chen R, Ge TT, Chang Q, et al. Effects of angiotensin receptor neprilysin inhibitors on inducibility of ventricular arrhythmias in rats with ischemic cardiomyopathy. Int Heart J. (2019) 60:1168–75. doi: 10.1536/ihj.19-065
37. Revuelta-López E, Núñez J, Gastelurrutia P, Cediel G, Januzzi JL, Ibrahim NE, et al. Neprilysin inhibition, endorphin dynamics, and early symptomatic improvement in heart failure: a pilot study. ESC Heart Fail. (2020) 7:559–66. doi: 10.1002/ehf2.12607
38. Eiringhaus J, Wünsche CM, Tirilomis P, Herting J, Bork N, Nikolaev VO, et al. Sacubitrilat reduces pro-arrhythmogenic sarcoplasmic reticulum Ca2+ leak in human ventricular cardiomyocytes of patients with end-stage heart failure. ESC Heart Fail. (2020) 7:2992–3002. doi: 10.1002/ehf2.12918
39. Kuchulakanti PK. ARNI in cardiovascular disease: current evidence and future perspectives. Future Cardiol. (2020) 16:505–15. doi: 10.2217/fca-2019-0089
40. Solomon SD, McMurray JJV, Anand IS, Ge J, Lam CSP, Maggioni AP, et al. Angiotensin-Neprilysin Inhibition in Heart Failure with Preserved Ejection Fraction. N Engl J Med. (2019) 381:1609–20. doi: 10.1056/NEJMoa1908655
41. Januzzi JL, Butler J, Fombu E, Maisel A, McCague K, Piña IL, et al. Rationale and methods of the Prospective Study of Biomarkers, Symptom Improvement, and Ventricular Remodeling During Sacubitril/Valsartan Therapy for Heart Failure (PROVE-HF). Am Heart J. (2018) 199:130–6. doi: 10.1016/j.ahj.2017.12.021
42. Ponikowski P, Voors AA, Anker SD, Bueno H, Cleland JGF, Coats AJS, et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: the task force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC)Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur Heart J. (2016) 37:2129–200. doi: 10.1093/eurheartj/ehw128
43. Balmforth C, Simpson J, Shen L, Jhund PS, Lefkowitz M, Rizkala AR, et al. Outcomes and effect of treatment according to etiology in HFrEF: an analysis of PARADIGM-HF. JACC Heart Fail. (2019) 7:457–65. doi: 10.1016/j.jchf.2019.02.015
44. Simpson J, Jhund PS, Silva Cardoso J, Martinez F, Mosterd A, Ramires F, et al. Comparing LCZ696 with enalapril according to baseline risk using the MAGGIC and EMPHASIS-HF risk scores: an analysis of mortality and morbidity in PARADIGM-HF. J Am Coll Cardiol. (2015) 66:2059–71. doi: 10.1016/j.jacc.2015.08.878
45. Rasmussen AA, Wiggers H, Jensen M, Berg SK, Rasmussen TB, Borregaard B, et al. Patient-reported outcomes and medication adherence in patients with heart failure. Eur Heart J Cardiovasc Pharmacother. (2021) 7:287–95. doi: 10.1093/ehjcvp/pvaa097
46. Mogensen UM, Køber L, Kristensen SL, Jhund PS, Gong J, Lefkowitz MP, et al. The effects of sacubitril/valsartan on coronary outcomes in PARADIGM-HF. Am Heart J. (2017) 188:35–41. doi: 10.1016/j.ahj.2017.02.034
47. Bauersachs J, Soltani S. Herzinsuffizienzleitlinien 2021 der ESC [Guidelines of the ESC 2021 on heart failure]. Herz. (2022) 47:12–8. doi: 10.1007/s00059-021-05084-5
48. Lin DS, Wang TD, Buranakitjaroen P, Chen CH, Cheng HM, Chia YC, et al. Angiotensin receptor neprilysin inhibitor as a novel antihypertensive drug: evidence from Asia and around the globe. J Clin Hypertens. (2021) 23:556–67. doi: 10.1111/jch.14120
49. Wang TD, Tan RS, Lee HY, Ihm SH, Rhee MY, Tomlinson B, et al. Effects of sacubitril/valsartan (LCZ696) on natriuresis, diuresis, blood pressures, and NT-proBNP in salt-sensitive hypertension. Hypertension. (2017) 69:32–41. doi: 10.1161/HYPERTENSIONAHA
50. Kario K, Sun N, Chiang FT, Supasyndh O, Baek SH, Inubushi-Molessa A, et al. Efficacy and safety of LCZ696, a first-in-class angiotensin receptor neprilysin inhibitor, in Asian patients with hypertension: a randomized, double-blind, placebo-controlled study. Hypertension. (2014) 63:698–705. doi: 10.1161/HYPERTENSIONAHA.113.02002
51. Supasyndh O, Sun N, Kario K, Hafeez K, Zhang J. Long-term (52-week) safety and efficacy of Sacubitril/valsartan in Asian patients with hypertension. Hypertens Res. (2017) 40:472–6. doi: 10.1038/hr.2016.151
52. Huo Y, Li W, Webb R, Zhao L, Wang Q, Guo W. Efficacy and safety of sacubitril/valsartan compared with olmesartan in Asian patients with essential hypertension: a randomized, double-blind, 8-week study. J Clin Hypertens. (2019) 21:67–76. doi: 10.1111/jch.13437
53. Williams B, Cockcroft JR, Kario K, Zappe DH, Brunel PC, Wang Q, et al. Effects of sacubitril/valsartan versus olmesartan on central hemodynamics in the elderly with systolic hypertension: the PARAMETER Study. Hypertension. (2017) 69:411–20.
54. Small H. Co-citation in the scientific literature: a new measure of the relationship between two documents. J Am Soc Info Sci. (1973) 24:265–9. doi: 10.1002/asi.4630240406
55. Vallon V, Verma S. Effects of SGLT2 Inhibitors on Kidney and Cardiovascular Function. Annu Rev Physiol. (2021) 83:503–28. doi: 10.1146/annurev-physiol-031620-095920
56. Writing Committee Members, Yancy CW, Jessup M, Bozkurt B, Butler J, Casey DE Jr., et al. 2016 ACC/AHA/HFSA focused update on new pharmacological therapy for heart failure: an update of the 2013 ACCF/AHA guideline for the management of heart failure: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Failure Society of America. Circulation. (2016) 134:e282–93. doi: 10.1161/CIR.0000000000000435
57. Velazquez EJ, Morrow DA, DeVore AD, Duffy CI, Ambrosy AP, McCague K, et al. PIONEER-HF Investigators. Angiotensin-Neprilysin Inhibition in Acute Decompensated Heart Failure. N Engl J Med. (2019) 380:539–48. doi: 10.1056/NEJMoa1812851
58. Ruilope LM, Dukat A, Böhm M, Lacourcière Y, Gong J, Lefkowitz MP. Blood-pressure reduction with LCZ696, a novel dual-acting inhibitor of the angiotensin II receptor and neprilysin: a randomised, double-blind, placebo-controlled, active comparator study. Lancet. (2010) 375:1255–66. doi: 10.1016/S0140-6736(09)61966-8
59. Desai AS, Solomon SD, Shah AM, Claggett BL, Fang JC, Izzo J, et al. Effect of sacubitril-valsartan vs enalapril on aortic stiffness in patients with heart failure and reduced ejection fraction: a randomized clinical trial. JAMA. (2019) 322:1077–84. doi: 10.1001/jama.2019.12843
60. Januzzi JL Jr., Prescott MF, Butler J, Felker GM, Maisel AS, McCague K, et al. Association of change in N-terminal Pro-B-Type natriuretic peptide following initiation of sacubitril-valsartan treatment with cardiac structure and function in patients with heart failure with reduced ejection fraction. JAMA. (2019) 322:1085–95. doi: 10.1001/jama.2019.12821
Keywords: angiotensin receptor neprilysin inhibitor, cardiovascular disorders, CiteSpace, research hotspots, mapping knowledge domains
Citation: Xu X, Li Y, Shi S, Lv J, Wang Y, Zheng H, Mao X, Wu H, Zhang B and Song Q (2022) The Application of Angiotensin Receptor Neprilysin Inhibitor in Cardiovascular Diseases: A Bibliometric Review From 2000 to 2022. Front. Cardiovasc. Med. 9:899235. doi: 10.3389/fcvm.2022.899235
Received: 18 March 2022; Accepted: 19 April 2022;
Published: 04 May 2022.
Edited by:
Xiaofeng Yang, Temple University, United StatesReviewed by:
Claudiu Cicea, Bucharest University of Economic Studies, RomaniaCopyright © 2022 Xu, Li, Shi, Lv, Wang, Zheng, Mao, Wu, Zhang and Song. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Huaqin Wu, eXVhbnNoYW55dW4yNjUwQDE2My5jb20=; MTUyOTcxODcwMkBxcS5jb20=; Bingxuan Zhang, emJ4MTExOEAxMjYuY29t; emJ4YmoyMDIxQDEyNi5jb20=; Qingqiao Song, U29uZ3FxOTg1QDEyNi5jb20=; c3FxYmoyMDIyQDEyNi5jb20=
†These authors share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.