 Chiranjivi Adhikari1,2*
Chiranjivi Adhikari1,2* Rojana Dhakal3,4
Rojana Dhakal3,4 Lal Mani Adhikari5
Lal Mani Adhikari5 Bijaya Parajuli6
Bijaya Parajuli6 Khem Raj Subedi7
Khem Raj Subedi7 Yeshoda Aryal8
Yeshoda Aryal8 Arjun Kumar Thapa9
Arjun Kumar Thapa9 Komal Shah2
Komal Shah2- 1Department of Public Health, SHAS, Pokhara University, Pokhara, Nepal
- 2Indian Institute of Public Health Gandhinagar, Gandhinagar, India
- 3Department of Nursing, School of Health and Allied Sciences, Pokhara University, Pokhara, Nepal
- 4Department of Life and Health Sciences, University of Nicosia, Nicosia, Cyprus
- 5Health Research and Social Development Forum International, Kathmandu, Nepal
- 6Ministry of Health and Population, Gandaki Province, Myagdi Health Office, Myagdi, Nepal
- 7Department of Economics, Far Western University, Tikapur Multiple Campus, Kailali, Nepal
- 8Ministry of Health and Population, Kathmandu, Nepal
- 9Department of Economics, School of Humanities and Social Sciences, Pokhara University, Pokhara, Nepal
Objective: Health Technology Assessment (HTA) is a comprehensive and important tool for assessment and decision-making in public health and healthcare practice. It is recommended by the WHO and has been applied in practice in many countries, mostly the developed ones. HTA might be an important tool to achieve universal health coverage (UHC), especially beneficial to low-and-middle-income countries (LMIC). Even though the Package for Essential Non-communicable Diseases (PEN) has already been initiated, there is a clear policy gap in the HTA of any health device, service, or procedure, including the assessment of cardiovascular risk factors (CVRFs) in Nepal. Hence, we carried out the review to document the HTA supported evidence of hypertension and diabetes screening, as CVRFs in Nepal.
Materials and methods: We searched in PubMed, Cochrane, and Google Scholar, along with some gray literature published in the last 6 years (2016–2021) in a systematic way with a controlled vocabulary using a well-designed and pilot tested search strategy, screened them, and a total of 53 articles and reports that matched the screening criteria were included for the review. We then, extracted the data in a pre-designed MS-Excel format, first in one, and then, from it, in two, with more specific data.
Results: Of 53 included studies, we reported the prevalence and/or proportion of hypertension and diabetes with various denominators. Furthermore, HTA-related findings such as cost, validity, alternative tool or technology, awareness, and intervention effectiveness have been documented and discussed further, however, not summarized due to their sparingness.
Conclusion: Overall, the prevalence of DM (4.4–18.8%) and HTN (17.2–70.0%) was reported in most studies, with a few, covering other aspects of HTA of DM/HTN. A national policy for establishing an HTA agency and some immediately implementable actions are highly recommended.
Introduction
Health technology assessment (HTA) is a multidisciplinary approach incepted during the 1970s for assessing technologies such as drugs, devices, procedures, settings of care, services or programs, including the screening in health care with the collection of data from epidemiological, clinical efficacy, quality of life, service utilization, and cost (both health systems' and patients' out of pocket payments) studies.
HTA assists in evidence informed health policy making on the introduction and use of health technologies. Since any state or country has competing priorities, policy-makers often decide what is the best buy for the available evidence-base and the budget, which can further help as suggested by the WHO, in developing the health benefit package (HBP) for any state or country (1). At least two dimensions (if not three) of universal health coverage?the proportion of the cost and the services covered are directly linked to and implicated by HTA. Countries like the USA, Australia and Canada have been benefiting from HTA for decades, whereas Asian countries like South Korea, Japan, China, and India (recently) are gaining momentum (2). As per a survey carried out by WHO in 2015, Nepal has neither rendered a national HTA body nor is there clarity on how HTA is used in decision-making (3).
According to the global burden of disease study (GBOD) conducted in Nepal in 2017, non-communicable diseases were responsible for two-thirds of all deaths (66%), while high blood pressure and high fasting blood glucose levels were responsible for 14 and 10% of all deaths, respectively (4). Screening can avert disability adjusted life years (DALYs) of 2.33–3.1 in the case of hyperglycaemia (5) and is cost-effective in both hyperglycaemia and hypertension (5, 6).
Diabetes is a metabolic disorder identified by screening using technologies like laboratory tests that include fasting plasma glucose, 2-h (2-h) post-load plasma glucose after a 75-g oral glucose tolerance test (OGTT); hemoglobin A1c (HbA1c); and random blood glucose in the presence of signs and symptoms. Diabetes is defined as fasting plasma glucose of 7.0 mmol/L (126 mg/dl), 2-h post-load plasma glucose of 11.1 mmol/L (200 mg/dl) (5), HbA1c ≥ 6.5% (48 mmol/ml); or a random blood glucose of ≥11.1 mmol/L (200 mg/ dl) in the presence of signs and symptoms. If elevated values are detected in asymptomatic people, repeat testing, preferably with the same test, is recommended as soon as practicable on a subsequent day to confirm the diagnosis (7).
Raised blood pressure can be identified at either a clinic, home-based, or ambulatory screening, and the diagnosis can be made with repeated measurements at 1–4 week intervals. In addition to this, blood tests, echocardiography, urine dipstick, albumin, and liver functions tests are other additional tests that are carried out in hypertensive suspects or diagnosed cases (8). As a part of assessing cardiovascular risk, mean systolic blood pressure should be measured over two separate occasions. For those who are already on anti-hypertensive medicine, the most recent recorded pretreatment value should be adopted as given by the National Institute for Health and Care Excellence/British Hypertension Society (NICE/BHS) guideline (9).
The population-based screening for diabetes and hypertension at a frequency ranging from every year to every 20 years was not cost-effective at the present level healthcare systems in India. However, it was estimated that screening at 3-to-5-year intervals could be cost-effective if the proportion of newly diagnosed and treated patients increased by more than 20%. Providing population-based screening of those two disease conditions through primary health centers (PHC) could be cost-effective; therefore they need to be strengthened at PHC level (10). A comparative study of BP measured in Shardaben General Hospital, India by digital and aneroid sphygmomanometers showed mean SBP as 108.92 ± 15.14 and 109.66 ± 16.81, and mean DBP as 76.20 ± 12.25 and 78.02 ± 14.35 mm of Hg, respectively, justifying that the bias for mean SBP and DBP was clinically non-significant and both instruments can be used interchangeably (11).
Diagnosing hypertension by sphygmomanometer is considered the gold standard as it has a high level of accuracy. A study from West Bengal showed that the aneroid device had better accuracy than the digital device as compared to the mercury sphygmomanometer (12). The mercury sphygmomanometer, which was widely used in the past to measure blood pressure in an office or clinic, has now been largely phased out in US hospitals, leading to the use of non-mercury, aneroid, or hybrid manometers in clinic and hospital settings (13, 14). Ambulatory monitoring was the most cost-effective strategy for all ages of men and women after an initial raised reading at the clinic or at home for blood pressure diagnosis, and so, it should be taken as a reference standard (15, 16).
Similarly, other instruments like 12-lead portable ECG devices for the screening of cardiovascular diseases in Ahemdabad found that screening at PHC by ECG saves 2.9 lives per year at an incremental cost of 89.97 USD, yielding a cost-effectiveness ratio of 31.07 USD, so the facility to screen cardiac abnormality at PHC level is highly recommended for risk adults and symptomatic cases (17). It coincides with the US preventive services task force for screening for prediabetes and type 2 diabetes at ages 35–70 years in a primary setting, which has a moderate net benefit. It was suggested that screening every 3 years may be a reasonable approach for adults with normal blood glucose as the initial normal glucose test result is limited. The diagnosis of type 2 diabetes should be confirmed with repeated tests. Now, the US Preventive Services Task Force (USPTSF) changed their practice of 2015 recommendation and lowered the initial age of screening from age 40 to 35 among adults who were obese or overweight (18).
In Bhutan, an economic evaluation of the World Health Organization (WHO)'s Package of Essential Non-communicable diseases (PEN) found that the ambulatory but high-risk screening (where people who are overweight, obese, or >40 years for DM and/or HTN, visiting primary care facilities) represents good value for money compared to “no screening” (19). However, if performed on a regular basis and taking into account the specific population group and the existing non-disease to disease conversion rate, opportunistic high-risk approach screening may also yield high results (but may not confirm cases) (20).
The Indian diabetes risk score (IDRS) was used in a study from Tamil Nadu, India to determine the prevalence of type 2 diabetes high-risk cases. Use of the IDRS could reduce the cost of diabetes screening in India and so, being suggested to use in mass screening (21). Insulin pumps or glucose sensors appear cost-effective, particularly in populations with higher HbA1c levels and rates of hypoglycaemia. However, the cost-effectiveness for combined insulin pumps and glucose sensors was less clear (22).
A study from Kuwait assessing type 2 diabetes and hypertension using machine-learning among 89,858 diabetics, 58,745 hypertensives, and 30,522 co-morbids shows that >85 and >90% accuracies were achieved for diabetes and hypertension, respectively using simple non-laboratory-based parameters. Talking more about the prediction, ethnicity is seen as a significant factor to the predictive models such as Asian-specific models and assessments perform even better (23). Population based screening for high- risk strategies can prevent cardiovascular disease. Also, it was suggested that where resources are limited, further advice be taken to take a total risk approach to identify several risk factors targeting to high-risk group to identify hypertension. Targeting high-risk groups for screening can help reduce costs because resources are not spent on the entire population. Early detection results in timely treatment and management of risk factors, which ultimately assists in reducing morbidity and mortality and reducing health-related costs (24).
A 540-person study in rural West Virginia was designed to identify diabetic risk using an HbA1c test and a diabetes risk assessment tool. Results showed that 61.8% of participants were at high risk for diabetes. It shows that community-based screenings are an effective way to assess diabetes risk (25).
Because cardiovascular risk factors were prevalent among Nepal's rural population, comprehensive intervention targeting all risk factors should be planned and implemented to reduce the burden of CVD in Nepal (26). Nepal has yet to work to implement health policies to tackle CVD or other NCDs. Recently, CVD management has been focused on treatment as there has been a rise in the availability of interventional cardiology and cardiothoracic surgery services (27). An assessment of health facilities for the implementation of a non-communicable disease package in Nepal among 92 health facilities in Kailali and Ilam districts revealed the gaps in the capacity of health institutions and the system in terms of training, supply, equipment, and diagnostics (28).
According to WHO, HTA should include the complete range of interventions or technology, and not be limited to just one. Technologies and methods considered in HTA include safety, clinical effectiveness, equity issues, ethical issues, feasibility, and acceptability of the health care system by providers and patients (29). Based on serum HbA1c levels, diabetes screening was offered at the Durham Veterans Affairs Medical Center for people aged 45–64 years old. Participants with an HbA1c ≥ 6.0% were invited for a follow-up measurement of blood pressure fasting plasma glucose, and health-related quality of life (HRQoL) were measured. Those with HbA1c ≥ 7.0% or fasting plasma glucose ≥7 mmol/dl are diagnosed as having unrecognized diabetes. There was no difference in the HRQoL of patients diagnosed with diabetes and those not diagnosed with diabetes. Screening for diabetes has minimal, if any, “labeling” effect with respect to quality of life (30).
Hypertensive disorders are the risk factors for cardiovascular diseases in Nepal, and there is a wide gap and socio-economic disparity in hypertension management. In Nepal, the overall prevalence of high blood pressure was 19.6 percent. Furthermore, less than one-third of the population was treated, and <20% had their blood pressure under control. Wealth and education-based inequalities in awareness, treatment, and control measures of raised BP were significantly high in urban and rural areas (31). In this scenario, Nepal has developed PEN protocols and initiated the program in 2016 (32). These signify (but are not limited to) the systematic assessment of equity, cost, clinical efficacy, safety, ethically sound, feasible, and acceptability of health devices, procedures, and services before their population-wide applications.
Materials and methods
Review framework
We used the following methodological framework to conduct this scoping review; (1) Identifying review questions, (2) Creating review objectives, (3) Establishing eligibility criteria, (4) Creating a search strategy and identifying search sources, (5) Screening records and data extraction, and (6) Evidence synthesis.
Search strategy
A comprehensive search was conducted using PubMed, Google Scholar, and the Cochrane databases, with publication date limits of the last 6 years (2016–2021). We also searched for reports, theses, and abstracts in gray literature and in citation searches.
A search strategy was finalized after developing a search strategy in consultation with the experts in the field. We searched with keywords such as screening, hypertension, diabetes, hyperglycaemia, Nepal, non-communicable, review, raised blood pressure, surveillance in the title, abstract, and keywords (ti; ab; kw); and with the medical subject heading (MeSH) descriptors such as heart disease risk factor, diagnostic techniques, blood pressure, diabetes mellitus. We searched on the basis of outcome indicators as illustrated in Table 1.
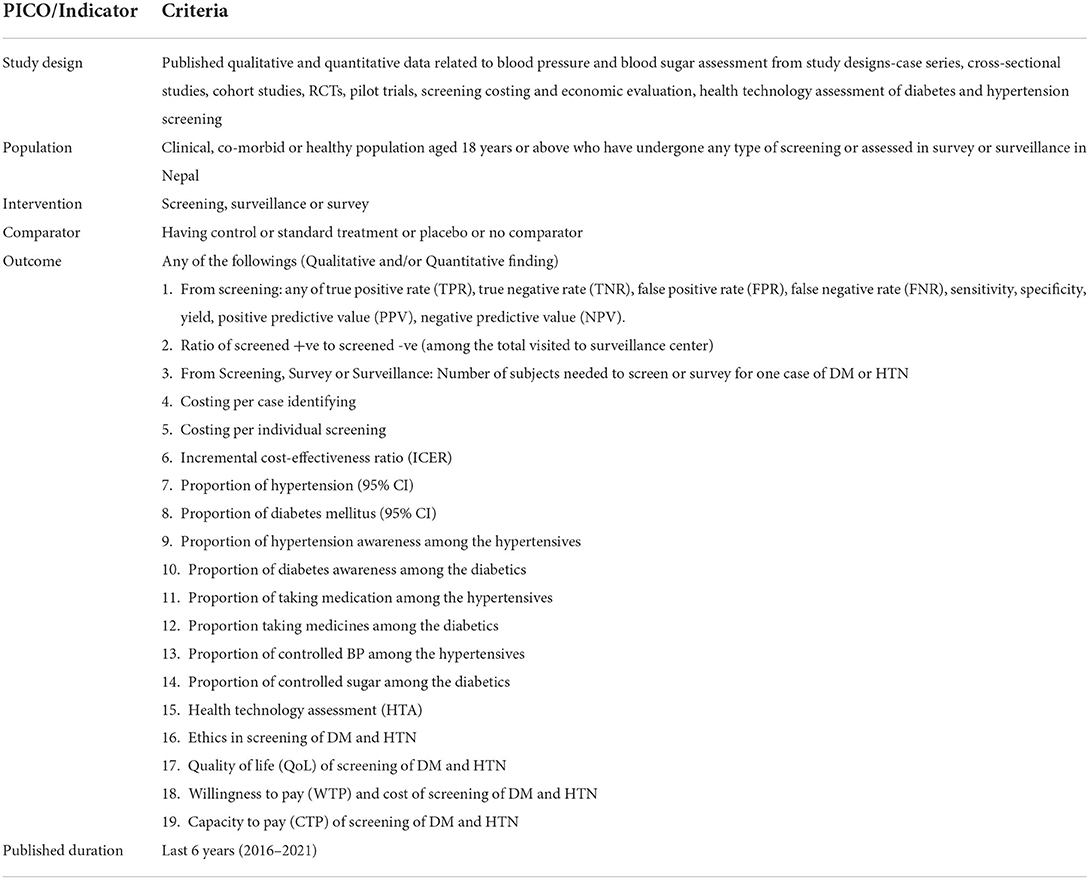
Table 1. PICO indicators and criteria for scoping review.
Study selection
After the strategy was finalized among all, a researcher, having trained and previous experience in systematic search and evidence synthesis, independently screened studies for eligibility and relevance. Studies were considered to be eligible if they had any of the outcome indicators as illustrated in Figure 1, including abstracts and reports. However, we excluded the protocols.
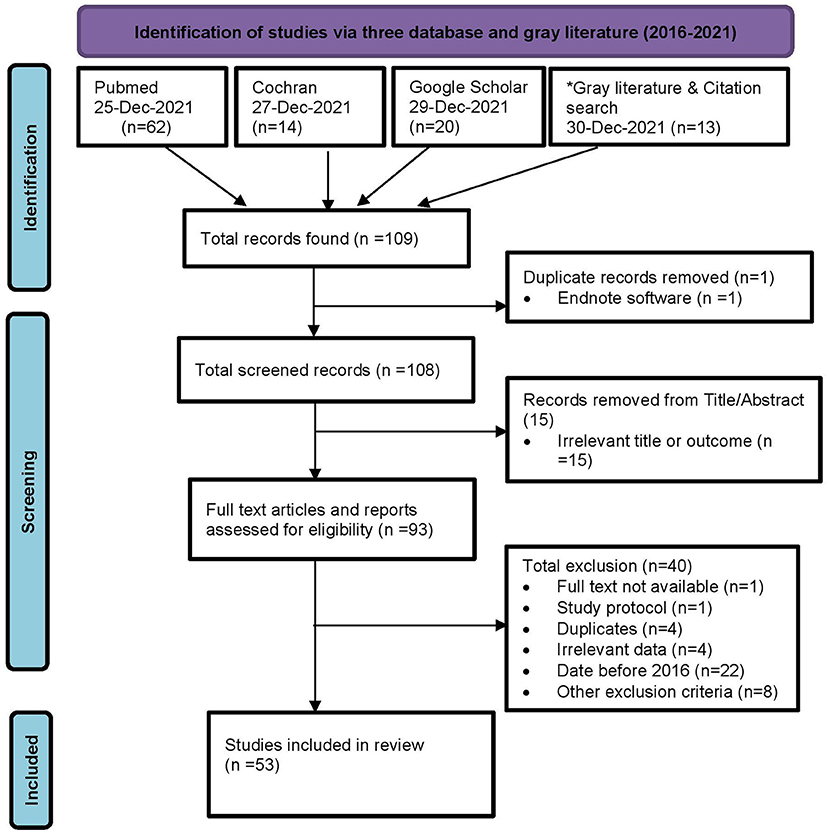
Figure 1. PRISMA chart of screening and included studies. *Gray literature search includes Shahid Gangalal National Heart Center (2), Mrigendra Samjhana Medical Trust (MSMT) (1), National Health Research Council (2), Ministry of Health and Population, Dept. of Health Services (3), Others (3), and Citation search (2).
Data extraction and data synthesis
Three different data extraction grids were developed by two review authors (CA and KS) and then sent to two authors (LMA and BP) for data extraction, from whom CA again obtained and compiled the data. Information regarding authors, country, study year, study type, sample size, geography, sex, age, ethnicity, and outcomes measures (Table 2), including key findings, and strengths and limitations (Table 3), was extracted from 53 individual studies (Figure 1), which were included in the review.
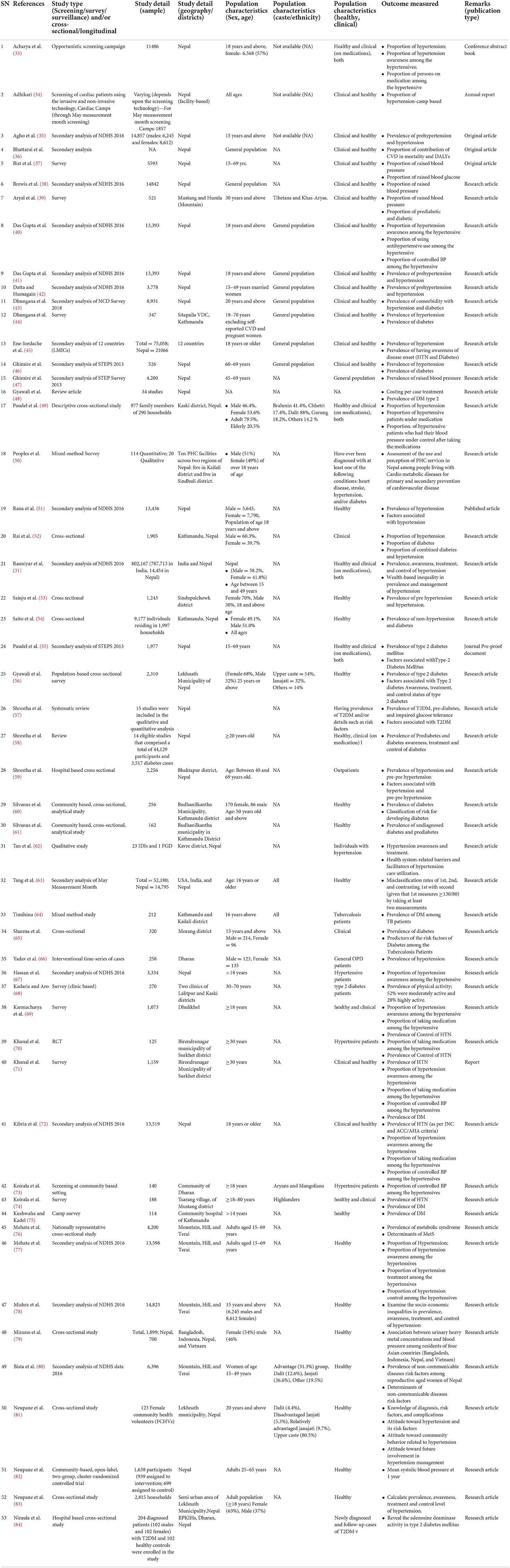
Table 2. Characteristics of the included studies.

Table 3. Key findings, strengths, and limitations of included studies.
Results
After excluding duplicates, irrelevant studies, and further eligibility assessment, 53 articles were included in the scoping review.
Of the 53 included studies, 11 reported both DM and HTN prevalence. Participants aged 50 years and older from Bagmati Province and Terai had a higher prevalence of DM. Similarly, people aged 60–69 years from Karnali Province and urban hills had a higher prevalence of HTN. A higher DM prevalence was reported among the clinical participants. For HTN, it was higher among both healthy and clinical participants. Similarly, studies/screenings carried out in ambulatory settings had a higher prevalence for DM, but for HTN, it was reported to be higher in the camps. Males had a higher prevalence among participants with DM and HTN, and co-morbidity for both diseases ranged from 5.7 to 20.2%. Interestingly, pre-HTN and pre-DM were reported among about one-third of the participants, and importantly, for both DM and HTN, a minimum of one-fourth were unaware, and among those on medication, a maximum of only about half had their diseases under control (Table 4; Figure 2).
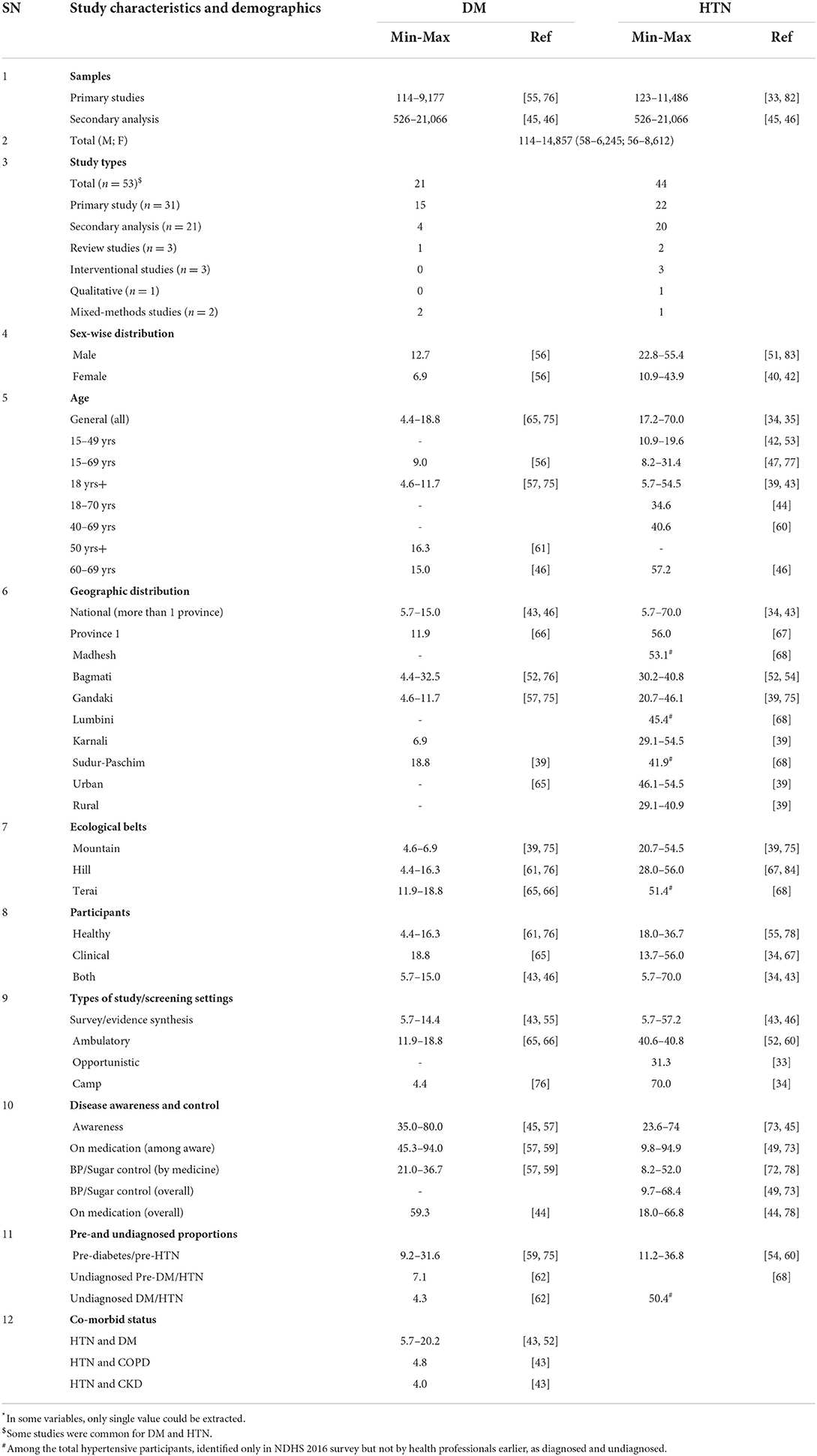
Table 4. Disease-wise summary prevalence/proportion (range*) of included studies.
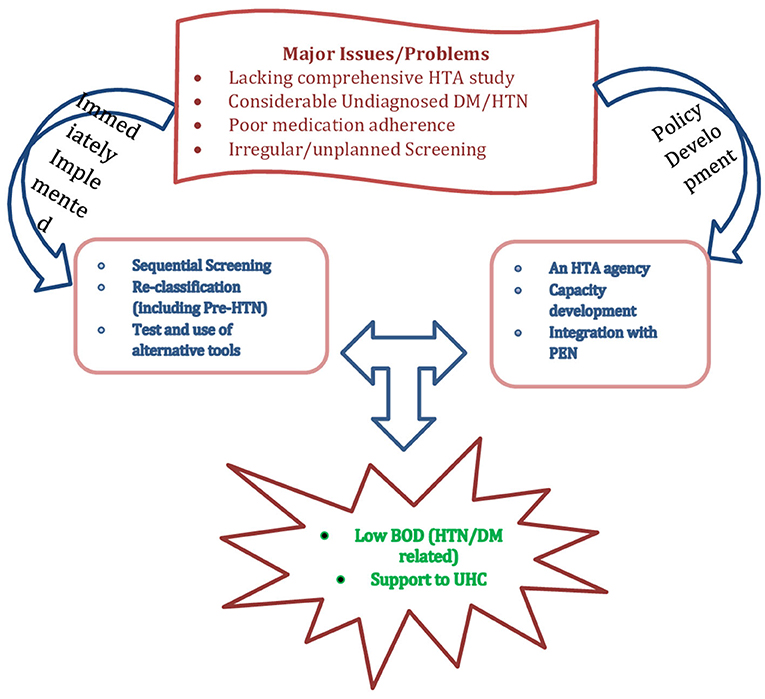
Figure 2. Summary of findings.
Validation and alternative use of the technology
The Indian Diabetes Risk Score (IDRS) is a simple tool that includes four statements to screen for diabetes and, with a cut-off score of 60, among the Nepalese population, revealed a sensitivity and a specificity of 84.2 and 55.2%, respectively, and hence could be a suitable alternative for diabetes and prediabetes screening (60). A hospital-based study revealed that measurement of serum Adenosine Deaminase (ADA), a biomarker, can be an alternative tool for glycaemic control and monitoring. It showed a significant correlation with HbA1c, fasting blood sugar (FBS) and post-prandial glucose (84). Similarly, a simple technological change in classification in the national guideline, changing the category of (130–140)/(80–90) mm of Hg as pre-HTN as defined by the Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC 7) to HTN as newly defined by the American Heart Association/American College of Cardiology (AHA/ACC), can reduce cardiovascular and related health problems by early detection and thereby save more lives and money (40). Another application of sequential screening, BP ≥130/80 mm of Hg, if assessed a second time (without assessing all for a second time), would give almost the same result but reduce the cost (time, human resources) by 40–60% during the camp and other opportunistic screenings (63). Moreover, the relationship of heavy metals with BP indicates that we need to address the problems of NCD prevention and control from a different perspective. On the other hand, HTN and DM are both webbed with multiple risk factors. For example, the triad of HDL-C, abdominal obesity and HTN was found among nearly 1 in 10 (8.2%) persons (76), and 6% women of reproductive age had co-occurrence of two NCD risk factors. This implies that these problems the rather be addressed with multiple and complex interventions, along with some feasible policy interventions (Figure 2).
Cost, DALYs, and equity
The prevalence of HTN was found to be more than seven (7.1) times higher among the wealthy than among the poor (31) but undiagnosed HTN was found to be disproportionate (1.6 times higher) among those with lower socioeconomic status (C = −0.18, p 0.001) (67). According to a qualitative finding, 52% of rural and 63% of urban people considered the medicine used to treat HTN and DM to be expensive (50). A review of costing studies showed that in DM, USD 445.9 (±27,535), 16.2 and 5.1 are needed per annum per patient, per prescription, and per visit per patient, respectively (48), thus, implicating medication non-adherence (Figure 2).
Awareness, medication adherence, and intervention efficacy
Nine out of every 10 people have moderate to high chances of developing DM (60), which indicates the importance of early interventions. HTN medication was missed due to forgetfulness, negligence, and unaffordability (62), which could be attributed to a lack of or poor HTN knowledge among community members (50) and the female community health volunteers (FCHVs) (81). However, when these cadres were trained and prepared as change agents, the intervention could reduce a mean blood pressure by 2.3–4.9 mm Hg and increase the proportion of BP control and knowledge of the community members (70, 82).
Discussion
Overall, the prevalence of high blood pressure was found to be as low as 5.7% (43) and as high as 70% (46) nationally, and up to 55% (39) in Karnali province and in urban areas. Similarly, DM was found to be between 5.7 (43) and 15% (46) nationwide, though it was as low as 6.9% (39) and as high as 32.5% (52) in Karnali and Bagmati provinces, respectively. Similarly, there is also a wide variation in DM (45–94%) and HTN (9–95%) awareness (49, 56, 58, 72), disease/disorder controlled by medicine (56, 58, 71, 77) in the population. This variation should be considered when planning and implementing the relevant programs for coverage and efficacy (Figure 2). A combined study of systematic review and expert consultation carried out in eight European countries found that the incorporation of additional social value judgments beyond clinical benefit assessment and economic evaluation could help further explain heterogeneity in coverage recommendations and decision-making (85). Similarly, it would be wise to compare the cost in lieu of the yield and the diagnoses that the screening strategies give. In an ambulatory high-risk approach carried out in the Bhutan PEN evaluation study (19), a 10% of eligibility and around 23% of diagnosis for HTN and a 10% of eligibility and 26% of diagnosis for DM may be contrasted with a 13% of eligibility and 17% of diagnosis for HTN and a 19% of eligibility and 22% of diagnosis in an opportunistic high-risk screening approach carried out in Karnataka, India (20). In these two studies, number of diagnoses was higher in ambulatory high-risk approach but yield was higher in opportunistic high-risk approach.
Producing HTA capacity in a country like Nepal may run up against different problems at various stages, such as policy sensitization, development and implementation, expertise development, and overall management. A similar program carried out by the Health Intervention and Technology Assessment Program (HITAP) of Thailand in India, Colombia, Myanmar, the Philippines, and Vietnam revealed experiences suggesting that it is not only technical capacity, such as analytical techniques for conducting economic evaluation, but also management, coordination, and communication capacity should be strengthened (86). Inequality in HTN was observed to have up to 1.6 times higher prevalence among the poorest and underprivileged (31, 67). A combined study of documentary review and interviews carried out by Ciani et al. in Italy during the early stage of HTA development, argued that not only the central agency should be in place, but also a fully coordinated and harmonized multi-level structure of HTA was imperative (87). Then, the Italian National Healthcare System was one of the most decentralized systems since the devolution reform approved in 2001, and Nepal is more or less, at present, in a similar situation with devolution of power to the local levels with a 3-tier governing system.
Regarding the universal health coverage (UHC) and social health security program (SHSP) that are underway, we are adopting and scaling-up different benefit packages by assessing only a few to many, but not all components. The early results of Thai universal coverage in 2009–10 showed that HTA is helpful for informing coverage decisions for health benefit packages because it enhances the legitimacy of policy decisions by increasing the transparency, inclusiveness, and accountability of the process (88). The National Institute for Health Research HTA programme also suggests that synthesized evidence, rather than depending upon clinical trials, should be taken into account, for decision analysis and that the findings of a trial be linked to systematic reviews and meta-analyses (89).
Limitations
The included studies' principal limitations were costing comparisons of technologies in light of comparative validity and precision. Furthermore, there was a lack of ethical, ICER, quality of life, and willingness and capacity to pay for various technologies.
Conclusion
Overall, 53 studies, including some secondary analysis and the reviews, mainly reported the prevalence of DM of 4.4–18.8% and HTN of 17.2–70%. In addition to establishing an HTA national agency, some immediate actions and a systematic HTA of both diseases, covering a representative sample, is highly recommended before warranting.
Author contributions
CA, KSh, RD, and LA conceptualized the review, developed the search strategy, the data extraction grids, and edited. CA, LA, and BP curated data. CA, KSh, and KSu carried out the formal analysis. CA, BP, LA, and AT extracted the data. CA and KSh administered, supervised, and validated the project. CA, RD, LA, BP, KSu, AT, YA, and KSh wrote the draft. All authors reviewed the final manuscript and agreed for submission.
Conflict of interest
Author LA was employed by HERD International.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
2. Liu G, Wu EQ, Ahn J, Kamae I, Xie J, Yang H. The development of health technology assessment in asia: current status and future trends. Value Health Reg Issues. (2020) 21:39–44. doi: 10.1016/j.vhri.2019.08.472
3. WHO. Global Survey on Health Technology Assessment by National Authorities. Geneva: WHO (2015). p. 40.
4. NHRC MoHp MEOR. Nepal Burden of Disease 2017: A Country Report based on the Global Burden of Disease 2017 Study. Kathmandu: Nepal Health Research Council (2019) p. 68.
5. Lohse N, Marseille E, Kahn JG. Development of a model to assess the cost-effectiveness of gestational diabetes mellitus screening and lifestyle change for the prevention of type 2 diabetes mellitus. Int J Gynaecol Obstet Off Organ Int Fed Gynaecol Obstet. (2011) 115(Suppl. 1):S20–25. doi: 10.1016/S0020-7292(11)60007-6
6. Kostova D, Spencer G, Moran AE, Cobb LK, Husain MJ, Datta BK, et al. The cost-effectiveness of hypertension management in low-income and middle-income countries: a review. BMJ Glob Health. (2020) 5:e002213. doi: 10.1136/bmjgh-2019-002213
7. Regional Committee for the Western Pacific 064. Noncommunicable Disease. Manila: WHO Regional Office for the Western Pacific (2013).
8. Unger T, Borghi C, Charchar F, Khan NA, Poulter NR, Prabhakaran D, et al. 2020 international society of hypertension global hypertension practice guidelines. Hypertension. (2020) 75:1334–57. doi: 10.1161/HYPERTENSIONAHA.120.15026
9. McCormack T, Krause T, O'Flynn N. Management of hypertension in adults in primary care: NICE guideline. Br J Gen Pract. (2012) 62:163–4. doi: 10.3399/bjgp12X630232
10. Kaur G, Chauhan AS, Prinja S, Teerawattananon Y, Muniyandi M, Rastogi A, et al. Cost-effectiveness of population-based screening for diabetes and hypertension in India: an economic modelling study. Lancet Public Health. (2022) 7:e65–73. doi: 10.1016/S2468-2667(21)00199-7
11. Kakkad K, Damor P, Parmar B, Patel S. Comparative study of blood pressure measurement by aneroid and digital manual sphygmomanometer. Natl J Community Med. (2016) 7:700–2. Available online at: https://www.njcmindia.com/index.php/file/article/view/1034
12. Shahbabu B. Which is more accurate in measuring the blood pressure? A digital or an aneroid sphygmomanometer. J Clin Diagn Res. (2016) 10:LC11–4. doi: 10.7860/JCDR/2016/14351.7458
13. Ogedegbe G, Pickering T. Principles and techniques of blood pressure measurement. Cardiol Clin. (2010) 28:571–86. doi: 10.1016/j.ccl.2010.07.006
14. Kurtz TW, Griffin KA, Bidani AK, Davisson RL, Hall JE. Recommendations for blood pressure measurement in humans and experimental animals. Hypertension. (2005) 45:299–310. doi: 10.1161/01.HYP.0000150857.39919.cb
15. Lovibond K, Jowett S, Barton P, Caulfield M, Heneghan C, Hobbs FR, et al. Cost-effectiveness of options for the diagnosis of high blood pressure in primary care: a modelling study. Lancet. (2011) 378:1219–30. doi: 10.1016/S0140-6736(11)61184-7
16. Muntner P, Shimbo D, Carey RM, Charleston JB, Gaillard T, Misra S, et al. Measurement of blood pressure in humans: a scientific statement from the American Heart Association. Hypertension. (2019) 73:e35–66. doi: 10.1161/HYP.0000000000000087
17. Shah K, Pandya A, Kotwani P, Saha S, Desai C, Tyagi K, et al. Cost-effectiveness of portable electrocardiogram for screening cardiovascular diseases at a primary health center in Ahmedabad District, India. Front Public Health. (2021) 9:1798. doi: 10.3389/fpubh.2021.753443
18. US Preventive Services Task Force. Screening for prediabetes and type 2 diabetes: US preventive services task force recommendation statement. JAMA. (2021) 326:736–43. doi: 10.1001/jama.2021.12531
19. Wangchuk D, Virdi NK, Garg R, Mendis S, Nair N, Wangchuk D, et al. Package of essential noncommunicable disease (PEN) interventions in primary health-care settings of Bhutan: a performance assessment study. WHO South-East Asia J Public Health. (2014) 3:154–60. doi: 10.4103/2224-3151.206731
20. Raghuveer P, Anand T, Tripathy JP, Nirgude AS, Reddy MM, Nandy S, et al. Opportunistic screening for diabetes mellitus and hypertension in primary care settings in Karnataka, India: a few steps forward but still some way to go. F1000Research. (2020) 9:335. doi: 10.12688/f1000research.22825.1
21. Sathiya Narayanan S, Shankar S, Padmini SK. Prevalence of type 2 diabetes using Indian diabetes risk score and its risk factors in a rural area of Tamil Nadu, India. Int J Community Med Public Health. (2017) 4:2778–82. doi: 10.18203/2394-6040.ijcmph20173322
22. Pease A, Zomer E, Liew D, Lo C, Earnest A, Zoungas S. Cost-effectiveness of health technologies in adults with type 1 diabetes: a systematic review and narrative synthesis. Syst Rev. (2020) 9:171. doi: 10.1186/s13643-020-01373-y
23. Farran B, Channanath AM, Behbehani K, Thanaraj TA. Predictive models to assess risk of type 2 diabetes, hypertension and comorbidity: machine-learning algorithms and validation using national health data from Kuwait—a cohort study. BMJ Open. (2013) 3:e002457. doi: 10.1136/bmjopen-2012-002457
24. Schmidt B-M, Durao S, Toews I, Bavuma CM, Hohlfeld A, Nury E, et al. Screening strategies for hypertension. Cochrane Database Syst Rev. (2020) 2020:CD013212. doi: 10.1002/14651858.CD013212.pub2
25. Misra R, Fitch C, Roberts D, Wright D. Community-based diabetes screening and risk assessment in rural West Virginia. J Diabetes Res. (2016) 2016:2456518. doi: 10.1155/2016/2456518
26. Khanal MK, Mansur Ahmed MSA, Moniruzzaman M, Banik PC, Dhungana RR, Bhandari P, et al. Prevalence and clustering of cardiovascular disease risk factors in rural Nepalese population aged 40–80 years. BMC Public Health. (2018) 18:677. doi: 10.1186/s12889-018-5600-9
27. Vaidya A. Tackling cardiovascular health and disease in Nepal: epidemiology, strategies and implementation. Heart Asia. (2011) 3:87–91. doi: 10.1136/heartasia-2011-010000
28. Aryal BK, Daud M, Thapa A, Mahotra A, Magar SA, Malla CK. Assesssment of health facilities for implementation of package of essential non-communicable disease in Nepal: baseline study in Kailali and Ilam District. J Nepal Health Res Counc. (2018) 16:149–55. doi: 10.3126/jnhrc.v16i2.20301
29. World Health Organization, Bertram M, Dhaene G, Tan-Torres Edejer T. Institutionalizing Health Technology Assessment Mechanisms: A How to Guide. World Health Organization (2021). p. 56.
30. Edelman D, Olsen MK, Dudley TK, Harris AC, Oddone EZ. Impact of diabetes screening on quality of life. Diabetes Care. (2002) 25:1022–6. doi: 10.2337/diacare.25.6.1022
31. Rauniyar SK, Rahman MdM, Rahman MdS, Abe SK, Nomura S, Shibuya K. Inequalities and risk factors analysis in prevalence and management of hypertension in India and Nepal: a national and subnational study. BMC Public Health. (2020) 20:1341. doi: 10.1186/s12889-020-09450-6
32. PHC Revitalization Division DoHS. PEN Control. Govt. of Nepal, Ministry of Health and Population.
33. Acharya P, Koirala S, Soti PB, Sharma S, Sapkota A, Kafle S, et al. Abstract P125: Hypertension, awareness, treatment, and control in nepal: results from may measurement month 2020. Blood Pressure Screen Hypert. (2021) 78(Suppl. 1):AP125. doi: 10.1161/hyp.78.suppl_1.P125
34. Adhikari CM. Sahid Gangalal Cardiac Hospital (SGCH) Annual Report, 2018. Kathmandu: SGCH (2018).
35. Agho KE, Osuagwu UL, Ezeh OK, Ghimire PR, Chitekwe S, Ogbo FA. Gender differences in factors associated with prehypertension and hypertension in Nepal: a nationwide survey. PLoS ONE. (2018) 13:e0203278. doi: 10.1371/journal.pone.0203278
36. Bhattarai S, Aryal A, Pyakurel M, Bajracharya S, Baral P, Citrin D, et al. Cardiovascular disease trends in Nepal – An analysis of global burden of disease data 2017. Int J Cardiol Heart Vasc. (2020) 30:100602. doi: 10.1016/j.ijcha.2020.100602
37. Bista B, Dhimal M, Bhattarai S, Neupane T, Xu YY, Pandey AR, et al. Prevalence of non-communicable diseases risk factors and their determinants: Results from STEPS survey 2019 Nepal. PloS ONE. (2021) 16:e0253605. doi: 10.1371/journal.pone.0253605
38. Brewis A, Choudhary N, Wutich A. Low water access as a gendered physiological stressor: Blood pressure evidence from Nepal. Am J Hum Biol Off J Hum Biol Counc. (2019) 31:e23234. doi: 10.1002/ajhb.23234
39. Aryal N, Weatherall M, Bhatta YKD, Mann S. Lipid profiles, glycated hemoglobin, and diabetes in people living at high altitude in Nepal. Int J Environ Res Public Health. (2017) 14:41. doi: 10.3390/ijerph14091041
40. Das Gupta R, Bin Zaman S, Wagle K, Crispen R, Hashan MR, Al Kibria GM. Factors associated with hypertension among adults in Nepal as per the Joint National Committee 7 and 2017 American College of Cardiology/American Heart Association hypertension guidelines: a cross-sectional analysis of the demographic and health survey 2016. BMJ Open. (2019) 9:e030206. doi: 10.1136/bmjopen-2019-030206
41. Das Gupta R, Shabab Haider S, Sutradhar I, Hasan M, Joshi H, Rifat Haider M, et al. Gender differences in hypertension awareness, antihypertensive use and blood pressure control in Nepalese adults: findings from a nationwide cross-sectional survey. J Biosoc Sci. (2020) 52:412–38. doi: 10.1017/S0021932019000531
42. Datta BK, Husain MJ. Spousal alcohol consumption and female hypertension status: evidence from Nepal. Public Health. (2020) 185:312–7. doi: 10.1016/j.puhe.2020.05.049
43. Dhungana RR, Karki KB, Bista B, Pandey AR, Dhimal M, Maskey MK. Prevalence, pattern and determinants of chronic disease multimorbidity in Nepal: secondary analysis of a national survey. BMJ Open. (2021) 11:e047665. doi: 10.1136/bmjopen-2020-047665
44. Dhungana RR, Thapa P, Devkota S, Banik PC, Gurung Y, Mumu SJ, et al. Prevalence of cardiovascular disease risk factors: a community-based cross-sectional study in a peri-urban community of Kathmandu, Nepal. Indian Heart J. (2018) 70(Suppl. 3):S20–7. doi: 10.1016/j.ihj.2018.03.003
45. Ene-Iordache B, Perico N, Bikbov B, Carminati S, Remuzzi A, Perna A, et al. Chronic kidney disease and cardiovascular risk in six regions of the world (ISN-KDDC): a cross-sectional study. Lancet Glob Health. (2016) 4:e307–319. doi: 10.1016/S2214-109X(16)00071-1
46. Ghimire S, Mishra SR, Baral BK, Dhimal M, Callahan KE, Bista B, et al. Noncommunicable disease risk factors among older adults aged 60-69 years in Nepal: findings from the STEPS survey (2013). J Hum Hypertens. (2019) 33:602–12. doi: 10.1038/s41371-019-0161-7
47. Ghimire U, Shrestha N, Gyawali B, Pradhan PMS, Mishra SR. Prevalence of American Heart Association defined ideal cardiovascular health metrics in Nepal: findings from a nationally representative cross-sectional study. Int Health. (2020) 12:325–31. doi: 10.1093/inthealth/ihz088
48. Gyawali B, Ferrario A, van Teijlingen E, Kallestrup P. Challenges in diabetes mellitus type 2 management in Nepal: a literature review. Glob Health Action. (2016) 9:31704. doi: 10.3402/gha.v9.31704
49. Paudel P, Chalise S, Neupane DR, Adhikari N, Paudel S, Dangi NB. Prevalence of hypertension in a community. J Nepal Med Assoc. (2020) 58:1011–7. doi: 10.31729/jnma.5316
50. Peoples N, Gong E, Gautam K, Khanal SN, Kohrt BA, Koirala S, et al. Perception and use of primary healthcare services among people with cardiometabolic diseases in two resource-limited areas in Nepal: a mixed methods study. Front Public Health. (2021) 9:698030. doi: 10.3389/fpubh.2021.698030
51. Rana J, Ahmmad Z, Sen KK, Bista S, Islam RM. Socioeconomic differentials in hypertension based on JNC7 and ACC/AHA 2017 guidelines mediated by body mass index: Evidence from Nepal demographic and health survey. PLoS ONE. (2020) 15:e0218767. doi: 10.1371/journal.pone.0218767
52. Rai BB, Shresthra MK, Thapa R, Essex RW, Paudyal G, Maddess T. Pattern and presentation of vitreo-retinal diseases: an analysis of retrospective data at a tertiary eye care center in Nepal. Asia-Pac J Ophthalmol Phila Pa. (2019) 8:481–8. doi: 10.1097/01.APO.0000604400.50700.2d
53. Sainju NK, Shah RK, Joshi SK. Screening for hypertension and obesity in rural population of Nepal. Kathmandu Univ Med J KUMJ. (2018) 16:4–7. Available online at: http://www.kumj.com.np/issue/61/4-7.pdf
54. Saito E, Gilmour S, Yoneoka D, Gautam GS, Rahman MM, Shrestha PK, et al. Inequality and inequity in healthcare utilization in urban Nepal: a cross-sectional observational study. Health Policy Plan. (2016) 31:817–24. doi: 10.1093/heapol/czv137
55. Paudel S, Tran T, Owen AJ, Smith BJ. The contribution of physical inactivity and socioeconomic factors to type 2 diabetes in Nepal: a structural equation modelling analysis. Nutr Metab Cardiovasc Dis. (2020) 30:1758–67. doi: 10.1016/j.numecd.2020.06.003
56. Gyawali B, Hansen MRH, Povlsen MB, Neupane D, Andersen PK, McLachlan CS, et al. Awareness, prevalence, treatment, and control of type 2 diabetes in a semi-urban area of Nepal: Findings from a cross-sectional study conducted as a part of COBIN-D trial. PLoS ONE. (2018) 13:e0206491. doi: 10.1371/journal.pone.0206491
57. Shrestha DB, Budhathoki P, Sedhai YR, Marahatta A, Lamichhane S, Nepal S, et al. Type 2 diabetes mellitus in Nepal from 2000 to 2020: a systematic review and meta-analysis. F1000Research. (2021) 10:543. doi: 10.12688/f1000research.53970.1
58. Shrestha N, Mishra SR, Ghimire S, Gyawali B, Mehata S. Burden of diabetes and prediabetes in nepal: a systematic review and meta-analysis. Diabetes Ther Res Treat Educ Diabetes Relat Disord. (2020) 11:1935–46. doi: 10.1007/s13300-020-00884-0
59. Shrestha R, Upadhyay SK, Khatri B, Bhattarai JR, Kayastha M, Upadhyay MP. BMI, waist to height ratio and waist circumference as a screening tool for hypertension in hospital outpatients: a cross-sectional, non-inferiority study. BMJ Open. (2021) 11:e050096. doi: 10.1136/bmjopen-2021-050096
60. Silvanus V, Dhakal N, Pokhrel A, Baral BK, Panta PP. Community based screening for diabetes and prediabetes using the indian diabetes risk score among adults in a semi-urban area in Kathmandu, Nepal. Nepal Med Coll J. (2019) 21:12–20. doi: 10.3126/nmcj.v21i1.24839
61. Silvanus V, Kafle PP, Pokhrel A, Baral BK, Pokhrel BR. Evaluation of fasting capillary glucose and fasting plasma glucose as screening tests for diabetes and prediabetes among adults in a semi-urban area in the Kathmandu District, Nepal. Nepal Med Coll J. (2019) 21:265–75. doi: 10.3126/nmcj.v21i4.27615
62. Tan J, Xu H, Fan Q, Neely O, Doma R, Gundi R, et al. Hypertension care coordination and feasibility of involving female community health volunteers in hypertension management in Kavre District, Nepal: a qualitative study. Glob Heart. (2020) 15:73. doi: 10.5334/gh.872
63. Tang O, Kou M, Lu Y, Miller ER III, Brady T, Dennison-Himmelfarb C, et al. Simplified hypertension screening approaches with low misclassification and high efficiency in the United States, Nepal, and India. J Clin Hypertens Greenwich Conn. (2021) 23:1865–71. doi: 10.1111/jch.14299
64. Timilsina S. The Acceptability of Screening of Diabetes Mellitus Among Tuberculosis Patients at Directly Observed Treatment Shortcourse (dots) Center in Selected Districts of Nepal (Doctoral Dissertation). Gadjah Mada University, Yogyakarta, Indonesia. p. 14.
65. Sharma B, Khanal VK, Jha N, Pyakurel P, Gurung GN. Study of the magnitude of diabetes and its associated risk factors among the tuberculosis patients of Morang, Eastern Nepal. BMC Public Health. (2019) 19:1545. doi: 10.1186/s12889-019-7891-x
66. Yadav AK, Lewis OD, Sharma SK, Mahato IP, Bhandari R, Gupta SK, et al. Screening and management of hypertension in a General Practice Outpatient Department of a tertiary level teaching hospital in eastern region of Nepal. Health Renaiss. (2017) 13:58–67. doi: 10.3126/hren.v13i1.17949
67. Hasan MM, Tasnim F, Tariqujjaman M, Ahmed S, Cleary A, Mamun A. Examining the prevalence, correlates and inequalities of undiagnosed hypertension in Nepal: a population-based cross-sectional study. BMJ Open. (2020) 10:e037592. doi: 10.1136/bmjopen-2020-037592
68. Kadariya S, Aro AR. Barriers and facilitators to physical activity among urban residents with diabetes in Nepal. PLoS ONE. (2018) 13:e0199329. doi: 10.1371/journal.pone.0199329
69. Karmacharya BM, Koju RP, LoGerfo JP, Chan KCG, Mokdad AH, Shrestha A, et al. Awareness, treatment and control of hypertension in Nepal: findings from the Dhulikhel Heart Study. Heart Asia. (2017) 9:1–8. doi: 10.1136/heartasia-2016-010766
70. Khanal MK, Bhandari P, Dhungana RR, Bhandari P, Rawal LB, Gurung Y, et al. Effectiveness of community-based health education and home support program to reduce blood pressure among patients with uncontrolled hypertension in Nepal: a cluster-randomized trial. PLoS ONE. (2021) 16:e0258406. doi: 10.1371/journal.pone.0258406
71. Khanal MK, Dhungana RR, Bhandari P, Gurung Y, Paudel KN. Prevalence, associated factors, awareness, treatment, and control of hypertension: Findings from a cross sectional study conducted as a part of a community based intervention trial in Surkhet, Mid-western region of Nepal. PLoS ONE. (2017) 12:e0185806. doi: 10.1371/journal.pone.0185806
72. Kibria GMA, Swasey K, Kc A, Mirbolouk M, Sakib MN, Sharmeen A, et al. Estimated change in prevalence of hypertension in Nepal following application of the 2017. ACC/AHA Guideline. JAMA Netw Open. (2018) 1:e180606. doi: 10.1001/jamanetworkopen.2018.0606
73. Koirala B, Rauniar GP, Ghimire A, Sharma SK. Counseling on life style modification and knowledge and belief of hypertension and its management among hypertensive patients visiting community based screening and management program in Eastern Nepal. J Chitwan Med Coll. (2018) 8:19–23. doi: 10.3126/jcmc.v8i1.23713
74. Koirala S, Nakano M, Arima H, Takeuchi S, Ichikawa T, Nishimura T, et al. Current health status and its risk factors of the Tsarang villagers living at high altitude in the Mustang district of Nepal. J Physiol Anthropol. (2018) 37:20. doi: 10.1186/s40101-018-0181-y
75. Kushwaha A, Kadel AR. Prevalence of type 2 diabetes mellitus among people attending medical camp in a community hospital. JNMA J Nepal Med Assoc. (2020) 58:314–7. doi: 10.31729/jnma.4953
76. Mehata S, Shrestha N, Mehta RK, Bista B, Pandey AR, Mishra SR. Prevalence of the Metabolic Syndrome and its determinants among Nepalese adults: Findings from a nationally representative cross-sectional study. Sci Rep. (2018) 8:14995. doi: 10.1038/s41598-018-33177-5
77. Mehata S, Shrestha N, Mehta R, Vaidya A, Rawal LB, Bhattarai N, et al. Prevalence, awareness, treatment and control of hypertension in Nepal: data from nationally representative population-based cross-sectional study. J Hypertens. (2018) 36:1680–8. doi: 10.1097/HJH.0000000000001745
78. Mishra SR, Ghimire S, Shrestha N, Shrestha A, Virani SS. Socio-economic inequalities in hypertension burden and cascade of services: nationwide cross-sectional study in Nepal. J Hum Hypertens. (2019) 33:613–25. doi: 10.1038/s41371-019-0165-3
79. Mizuno Y, Shimizu-Furusawa H, Konishi S, Inaoka T, Ahmad SA, Sekiyama M, et al. Associations between urinary heavy metal concentrations and blood pressure in residents of Asian countries. Environ Health Prev Med. (2021) 26:101. doi: 10.1186/s12199-021-01027-y
80. Bista B, Dhungana RR, Chalise B, Pandey AR. Prevalence and determinants of noncommunicable diseases risk factors among reproductive aged women of Nepal: Results from Nepal Demographic Health Survey 2016. PLoS ONE. (2020) 15:e0218840. doi: 10.1371/journal.pone.0218840
81. Neupane D, McLachlan CS, Mishra SR, Kallestrup P. Understanding and motivations of female community health volunteers about blood pressure control: a prerequisite for developing community-based hypertension interventions in Nepal. Glob Heart. (2017) 12:227–32. doi: 10.1016/j.gheart.2016.09.003
82. Neupane D, McLachlan CS, Mishra SR, Olsen MH, Perry HB, Karki A, et al. Effectiveness of a lifestyle intervention led by female community health volunteers versus usual care in blood pressure reduction (COBIN): an open-label, cluster-randomised trial. Lancet Glob Health. (2018) 6:e66–73. doi: 10.1016/S2214-109X(17)30411-4
83. Neupane D, Shrestha A, Mishra SR, Bloch J, Christensen B, McLachlan CS, et al. Awareness, prevalence, treatment, and control of hypertension in western Nepal. Am J Hypertens. (2017) 30:907–13. doi: 10.1093/ajh/hpx074
84. Niraula A, Thapa S, Kunwar S, Lamsal M, Baral N, Maskey R. Adenosine deaminase activity in type 2 diabetes mellitus: does it have any role? BMC Endocr Disord. (2018) 18:58. doi: 10.1186/s12902-018-0284-9
85. Angelis A, Lange A, Kanavos P. Using health technology assessment to assess the value of new medicines: results of a systematic review and expert consultation across eight European countries. Eur J Health Econ. (2018) 19:123–52. doi: 10.1007/s10198-017-0871-0
86. Tantivess S, Chalkidou K, Tritasavit N, Teerawattananon Y. Health technology assessment capacity development in low-and middle-income countries: experiences from the international units of HITAP and NICE. F1000Research. (2017) 6:2119. doi: 10.12688/f1000research.13180.1
87. Ciani O, Tarricone R, Torbica A. Diffusion and use of health technology assessment in policy making: what lessons for decentralised healthcare systems? Health Policy. (2012) 108:194–202. doi: 10.1016/j.healthpol.2012.09.017
88. Mohara A, Youngkong S, Velasco RP, Werayingyong P, Pachanee K, Prakongsai P, et al. Using health technology assessment for informing coverage decisions in Thailand. J Comp Eff Res. (2012) 1:137–46. doi: 10.2217/cer.12.10
Keywords: health technology assessment (HTA), cardiovascular, risk factor, hypertension, diabetes, screening, review, Nepal
Citation: Adhikari C, Dhakal R, Adhikari LM, Parajuli B, Subedi KR, Aryal Y, Thapa AK and Shah K (2022) Need for HTA supported risk factor screening for hypertension and diabetes in Nepal: A systematic scoping review. Front. Cardiovasc. Med. 9:898225. doi: 10.3389/fcvm.2022.898225
Received: 17 March 2022; Accepted: 12 July 2022;
Published: 01 August 2022.
Edited by:
Richard Yang Cao, Shanghai Xuhui Central Hospital, ChinaReviewed by:
Chun-Bae Kim, Yonsei University, South KoreaYi Hong, The First Rehabilitation Hospital of Shanghai, China
Copyright © 2022 Adhikari, Dhakal, Adhikari, Parajuli, Subedi, Aryal, Thapa and Shah. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Chiranjivi Adhikari, Y2hpcmFuYWRoaWthcmlAZ21haWwuY29t