
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
STUDY PROTOCOL article
Front. Cardiovasc. Med., 08 September 2022
Sec. Pediatric Cardiology
Volume 9 - 2022 | https://doi.org/10.3389/fcvm.2022.893764
 Joanna Seliga-Siwecka1*
Joanna Seliga-Siwecka1* Ariel Płotko1
Ariel Płotko1 Agata Wójcik-Sep1Renata Bokiniec1Julita Latka-Grot2
Agata Wójcik-Sep1Renata Bokiniec1Julita Latka-Grot2 Małgorzata Żuk3
Małgorzata Żuk3 Konrad Furmańczyk4,5Wojciech Zieliński5,6
Konrad Furmańczyk4,5Wojciech Zieliński5,6 Mariola Chrzanowska5,6
Mariola Chrzanowska5,6Background: Infants with duct dependent heart lesions often require invasive procedures during the neonatal or early infancy period. These patients remain a challenge for pediatric cardiologists, neonatologists, and intensive care unit personnel. A relevant portion of these infant suffer from respiratory, cardiac failure and may develop NEC, which leads to inadequate growth and nutrition, causing delayed or complicated cardiac surgery.
Methods: This randomized control trial will recruit term infants diagnosed with a duct dependant lesion within the first 72 h of life. After obtaining written parental consent patients will be randomized to either the physician led enteral feeding or protocol-based feeding group. The intervention will continue up to 28 days of life or day of cardiosurgical treatment, whichever comes first. The primary outcomes include NEC and death related to NEC. Secondary outcomes include among others, number of interrupted feedings, growth velocity, daily protein and caloric intake, days to reach full enteral feeding and on mechanical ventilation.
Discussion: Our study will be the first randomized control trial to evaluate if standard (as in healthy newborns) initiation and advancement of enteral feeding is safe, improves short term outcomes and does not increase the risk of NEC. If the studied feeding regime proves to be intact, swift implementation and advancement of enteral nutrition may become a recommendation.
Trial registration: The study protocol has been approved by the local ethical board. It is registered at ClinicalTrials.gov NCT05117164.
Congenital heart diseases (CHD) occur with an incidence of six to nine cases per 1,000 births (1). Within this group, infants with duct dependent heart lesions often require invasive procedures during the neonatal or early infancy period. Furthermore, a relevant portion of these infants suffer from respiratory and cardiac failure as well as necrotizing enterocolitis (NEC) which leads to malnutrition and failure to thrive within the first months of life (2, 3). Inadequate growth and nutrition often lead to delayed or complicated cardiac surgery (4). NEC is a very rare condition in full-term neonates, however the risk increases by 10–100 times in patients with CHD (2). The estimated rate of NEC in infants with CHD ranges from 1.6 to 9% and mortality rates go up to 24% (5). The exact pathophysiology of NEC in babies w CHD is unknown but is likely multifactorial. Impaired mesenteric blood flow seen in infants with CHD is caused by the disruption of systemic perfusion during diastole and predisposes the infant to NEC (6, 7). McElhinney et al. have shown that episodes of low cardiac output and shock were significantly associated with NEC with an odd ratio of 6.5 (95% CI 1.8–23.5) (7). Based on a lower pulsation index observed in infants with hypoplastic left heart syndrome (HLHS), Miller et al. hypothesized that infants with HLHS may have an abnormal systemic vasculature that predisposes them to NEC (8, 9).
These patients remain a challenge for pediatric cardiologists, neonatologists, and intensive care unit personnel. As 48% of NEC develops pre-operatively, physicians are often hesitant to start feeding in infants with duct dependent CHD (10, 11). Nevertheless, there is little evidence showing that pre-operative feeds increase the risk of developing NEC, and most of the evidence comes from retrospective trials (11, 12). Current guidelines recommend that in patients with CHD enteral feeding should be initiated within the preoperative period (13). Despite published recommendations, significant differences in practice exist among centers worldwide (14). This approach contributes to poor growth in the perioperative course (15). Furthermore, adequate nutrition prior to surgery improves postoperative outcomes such as better feeding tolerance, wound healing and length of hospital stay (16).
Increasing evidence supports preoperative feeding in this group of patients despite the increased risk of NEC (5, 17–20). However, only retrospective studies are available, and the relationship between the time of enteral feeding initiation, increasing feeding volume, velocity rates and the development of NEC has not yet been documented (21, 22).
In view of the above, we have decided to perform a prospective randomized study, to evaluate whether implementation of a standard enteral nutrition protocol in patients with duct dependent CHD is equally safe in the context of NEC compared to patients fed based on the discretion of the leading physician.
The aim of this study is to assess whether initiation and advancement of enteral feeding is safe, improves short term outcomes and does not increase the risk of NEC in neonates with duct dependant lesions.
Parents of the neonates born after 36 weeks of pregnancy with duct-dependent CHD will be offered participation in the study within the first 3 days of life. After provision of oral and written information about the study, both parents will be asked to sign a written consent for their child to participate in the study (Table 1).
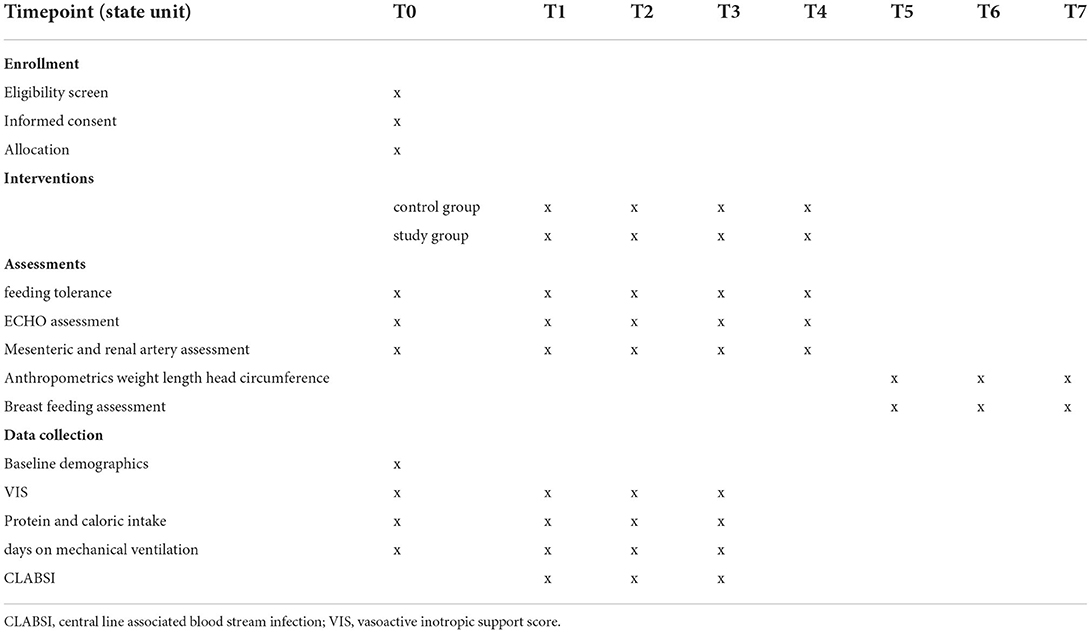
Table 1. Study timetable.
This study is designed as a randomized, parallel-group, superiority multi-center trial, with an 1:1 allocation and stratification by type of lesion.
The study will be carried out in four neonatal centers in Poland, including two neonatal departments at the Medical University of Warsaw (MUW), and one Neonatal Unit at Children's Health Memorial Institute (CHMI), and Polish Mother's Memorial Hospital (PMMH).
Departments of Neonatology at MUW are level III and IV teaching hospitals with approximately 5,000 (150 CHD) deliveries per year. Both units are referral centers for fetuses with CHD. Having access to high-risk mothers will augment recruitment. CHMI and PMMH are regional level IV hospital providing neonatal, cardiac, and surgical care for infants with CHD. A certified breastfeeding consultant is available daily on each unit.
The local feeding regimes for infants with CHD are set at the discretion of the attending doctor. However, the staff, in both units, is willing to implement new procedures to improve neonatal outcome.
All parents of infants diagnosed with a duct dependant lesion and admitted to participating units will be approached by one of the research team members within the first 72 h of life (as full enteral feeding is usually reached at a minimum of 7 days of life). He or she will explain the study and obtain written consent for participating in the trail. Recruitment will take place between June 1st 2022 and June 30st 2024. After obtaining written consent for participating in the trial, the patient's medical record number (MRN) will be immediately registered on REDCap (Research Electronic Data Capture). Patients eligible for the trial must comply with all the following at randomization.
1. Duct dependent CHD: assessment of ductus arteriosus (DA) will be done using the parasternal short axis view or suprasternal view.
• ductal diameter size will be measured using 2D imaging or by color Doppler at the narrowest point usually at the pulmonary end of the duct (mm).
• shunt direction (using pulsed Doppler) will be defined as one of the followings; left to right or right to left shunt, or bidirectional.
2. Term infants.
3. Parental/legal guardian consent.
1. Potential contradictions to early central feeding; neonates with gastrointestinal anatomic and maxillofacial abnormalities.
2. Feeding intolerance defined as vomiting bile or haemorrhagic residuals (23).
3. Hemodynamic instability defined as hypotension requiring at least two inotropes for at least 72 h.
4. > 50% formula based enteral feeding Studies have shown that infants with duct dependent CHD, who were fed with a predominately human milk-based diet have a lower risk of NEC.
5. Birth weight <2500 g In a large multi-center cohort of patients with HLHS, El-Hassan et al. failed to show an increased risk of NEC, but outcomes were worse in the group of babies with low birth weight (24).
Optimal nutrition is crucial to improve short- and long-term outcomes in newborns with CHD. However, large, well designed randomized controlled studies are not available, hence feeding practices differ between units and physicians. Furthermore, a position statement regarding nutritional support for children with critical illnesses (including CHD) is based on studies in preterm populations (13). Given the above, selecting a physician led enteral feeding regime as a comparator is therefore justified.
Patients will be randomized to either the physician led enteral feeding (control group) or protocol-based feeding group (study group).
Patients will receive enteral feeding at the discretion of the leading physician. Feeding practice differs between staff and usually relies on an increase of enteral feeding by 5–20ml/kg/day. Subjective evaluation of feeding tolerance, will be defined as one of the following: bilious or milk residuals, distended abdomen, and vomiting. Withholding or slowing down feeding will be subject to an induvial decision of the attending.
To meet the nutritional goals, infants will receive enteral feeding based on the following protocol (14):
• Minimal enteral nutrition (MEN) will begin within 72 h life at 10 to 20 mL/kg/day, breast milk/donor human milk. MEN will not be included in the caloric goals.
• Advancements in feeding will be set at 20–30 mL/kg/day, but not more than 10 ml per feeding portion to reach a goal of 150 ml/kg/day, but not more than 120ml/kg/day in cases of fluid restriction).
• The goal will be to reach an overall daily caloric intake of minimum 100 kcal/kg/d.
In both groups the interventions will continue up to 28 days of life or day of cardiosurgical treatment, whichever comes first.
In infants who present with one or two of the following symptoms such abdominal distention, visible bowels loops or feeding intolerance (defined as emesis ≥2 consecutive feeds, or gastric residuals of >50% per feed in ≥2 consecutive feeds, bilious residuals, bilious emesis) the intervention will be modified by decreasing enteral nutrition by 50% and substituting the remaining fluid requirements with adequate parenteral nutrition for a maximum of 48 h. If symptoms persist above 48 h, the trial will be discontinued.
The trial will be discontinued if the following occur:
The patient presents with at least three of the following symptoms.
• Abdominal distention.
• Visible bowels loops.
• Feeding intolerance (defined as emesis ≥2 consecutive feeds, or gastric residuals of >50% per feed in ≥2 consecutive feeds, bilious residuals, bilious emesis)..
• Temperature instability (defined as ≥2 consecutive measurements).
• Presence of bowel perforation of NEC confirmed on abdominal x-ray or ultrasound.
Medical notes (MN) of infants included in the study will be visibly marked to promote adherence to the study protocol. A flowchart explaining inclusion, exclusion and discontinuation criteria will be available in the patient's MN. A meeting will be scheduled to introduce the staff to the study protocol including:
• Brief presentation of the study protocol such as justification for undertaking the trial and possible impact of the study outcome on everyday practice.
• Instructions about the way the intervention should be applied.
Reminder sessions will take place on a two-monthly basis at the departments where the study will be conducted. Staff will be asked about any problems they are experiencing with implementing the study.
Participation in clinical trials involving interventions which may bias primary and secondary outcomes results will be prohibited.
The primary outcomes will include Stage II or III of NEC as defined by Kliegman and Walsh (25) and death related to NEC.
Stage II NEC will be defined as distended abdomen and radiological symptoms (intramural and/or portal gas). Stage III NEC will be defined as distended abdomen, radiological symptoms (intramural and/or portal gas) and respiratory and cardiovascular failure requiring mechanical ventilation and inotropic support (25). In surgery verified cases no radiological verification will be required.
Number of interrupted/discontinued feedings per day.
Impact on raw and z-score weight, length, and head circumference will be assessed Measurements will be collected at 3, 6 and 12 months of age and reported as z-scores (26).
Because concomitant use of multiple VA's is common in this group of patients, the vasoactive inotropic support score (VIS) will be calculated to quantify the vasoactive support. The daily VIS will be collected for the complete study period, using the updated definition from Gaies (27). VIS has been previously used to assess enteral feeding safety in a population of critically ill pediatric patients (28). Along the daily scores, the highest VIS and mean VIS will also be calculated.
Daily intakes of energy (Kcal/kg) and protein (g/kg) provided by enteral and parenteral feeding will be calculated.
Defined as sepsis diagnosed >72 h of age, confirmed with a positive blood and/cerebral spinal fluid specimen.
The number of days required to reach 150 ml/kg/day of enteral nutrition, counted from day when milk is started.
The number of days on mechanical ventilation.
Breastfeeding assessment at 3, 6, and 12 months of age. Exclusive breastfeeding will be defined as feeding infants only breast milk, directly from breast or expressed, except drops or syrups consisting of vitamins, mineral supplements, or medicine (29). Partial breastfeeding will be defined as the infant receiving human and formula milk (30).
Anatomic lesions that disrupt systemic blood flow such as duct dependent lesion, may lead to impaired blood flow which increases the risk of NEC. Carlo et al. demonstrated that, this “diastolic steal phenomenon” appeared in 47% of infants with duct dependent CHD, who developed NEC (31).
However, there are no studies evaluating the mesenteric, aortic, and renal artery blood flow changes after the introduction of feeds.
Doppler assessment will be performed on 1, 3, 7, 14, 28 day of life.
The following measurements will be recorded.
• Peak systolic velocity (PSV) in (cm/s).
• End-diastolic velocity (EDV) in (cm/s).
• Resistivity index (RI).
• Pulsation index (PI).
• Superior mesenteric artery (SMA) blood flow assessment will be performed using the sagittal plane of the abdominal cavity, in the longitudinal projection of the vessel, 1 cm below the celiac trunk.
• Right renal artery (RRA) blood flow assessment will be performed using the frontal plane of the abdominal cavity when the hilum of the kidney is visualized (32).
• direction of diastolic flow in the post-ductal aorta (using pulsed Doppler) will be defined as antegrade, absent or retrograde flow (32).
The age (in days) at transfer to a cardiac referral center will recorded, including the length of hospital stay in the referring center, and the reason for transfer.
T0- day 1 of life
T1- day 3 of life
T2- day 7 of life
T3-day 14 of life
T4-day 28 of life
T5- 3 months of age
T6 - 6 months of age
T7- 12 months of age.
Studies have reported an incidence of NEC between 7–20% in babies with duct dependent congenital heart diseases, hence we chose the incidence of 18% in the control arm and 7.6% the intervention group (7, 14, 33–35). Therefore, 192 neonates should be included in each group. In total (assuming 20% lost for follow up), 384 neonates with a duct dependent heart disease should be included in the study. These calculations were performed assuming superiority H0: P1 = P2 vs. H1: P1≥P2 with a power of 80%, a significance level of 5%. References: https://select-statistics.co.uk/calculators/sample-size-calculator-two-proprtions/ (36).
The study will continue until the minimum of 192 valid observations are collected in every arm. As part of the antenatal cardiology consult, women with will be offered a short meeting with a member of the recruitment team. During this appointment, they will be offered participation in the trial. To increase participant enrolment a second patient screen will be carried out by medical staff during admission to the Neonatal Intensive Care Unit. The enrolment period will extend over 36 months. Recruitment rates will be monitored monthly. In return, women will be offered additional breastfeeding support.
A member of the recruitment team will approach caregivers within the infant's first 72 h of life. He or she will explain the study and obtain written consent for participating in the trail. Infants who fulfill inclusion criteria will be randomized.
A study number together with the allocated treatment will be assigned by REDCap. The allocation sequence will be computer-generated. Patient's data along with the result of the allocation will be sent to statistical team. Block randomization with stratification by type of lesion (ductal dependent pulmonary, systematic, or mixing blood flow) will be implemented. Patients will be randomly assigned to standard or physician-led enteral nutrition guidelines in 1:1 ratio. To ensure allocation concealment, the randomization list will remain with the statistical team for the whole duration of the study. The block size will be variable and concealed until primary endpoint analyses.
Thus, randomization will be conducted without any influence of the principal investigators, clinicians, recruitment or follow up staff.
Assessments regarding the clinical course will be conducted by an assessor blind to treatment allocation. Due to the nature of the intervention staff cannot be blinded to allocation but are strongly inculcated not to disclose the allocation status of the participant at the follow up assessments. A member of the research team blinded to treatment allocation will feed data into REDCap.
All baseline data will be collected based on electronic MN.
Patients will be evaluated for NEC based on the presence of at least three of the following clinical symptoms (37–40).
• Abdominal distention.
• Visible bowels loops.
• Feeding intolerance (defined as emesis ≥2 consecutive feeds, or gastric residuals of >50% per feed in ≥2 consecutive feeds, bilious residuals, bilious emesis).
• Temperature instability (defined as ≥2 consecutive measurements).
• Frank bloody stools.
• Cardiovascular instability (hypotension; defined as MAP <30 mmHg, tachycardia >160/' or bradycardia <80/').
• Recurrent apnoea.
• Increase of abdominal girth > 2 cm (allowing inter-observer variability of 1 cm) within 12 h
• Abdominal wall erythema.
And/or at least 2 of the below laboratory findings based on Walsh and Bell criteria (modified by Kliegman) (25, 37).
• Thrombocytopenia < 50 k
• Leukopenia <6 k
• CRP > 10 mg/dl
• PCT > 1 IU/l
• Coagulopathy.
NEC will be diagnosed using the abdominal ultrasonography (AUS) or plain abdominal radiography (AR).
Gray- scale AUS will be used to assess bowel wall echogenicity, measure bowel wall thickness, peristalsis, pneumatosis intestinalis (PI), portal vein gas (PVG), free abdominal air and fluid. The following finding on AUS will be equivalent do NEC (41):
1. A bowel wall thickness of >2, 7 mm accompanied by an increase in echogenicity will be considered as suspicious. Color Doppler (CD) ultrasound will be required to evaluate blood flow in the superior mesenteric artery (SMA), and bowel wall perfusion (BWP). Evaluation of BWP; three categories of flow in the bowel wall will be recognized in color Doppler: normal (1–9 CD signal dots per cm2), increased (“zebra” pattern, “Y” pattern or “ring” pattern), and absent (when no color Doppler signals will be present) which will be reported as transmural necrosis.
2. Bowel wall thickness below 1.0 mm will be considered as abnormal thinning because of ischaemia or necrosis. Measurements will be recorded in relaxed bowel segments.
3. PI will be defined as small intramural hyperechoic focuses in the bowel wall, which will not change position despite peristalsis, respiratory movement, or abdominal compression with the transducer.
4. Abnormal peristaltic contractions of the small bowel will be defined as <10 movements/min.
5. For evaluation of PVG, the portal vein will be adjusted in a transverse or longitudinal section of the liver. PVG will be defined as highly echogenic round particles with a diameter of approximately 1 mm registered within portal circulation.
6. Using a transverse section of the right upper abdomen showing the liver just below the diaphragm, free abdominal gas will be detected as a bright echogenicity between the abdominal wall and the anterior surface of the liver.
7. Free abdominal fluid will be evaluated as an hypoechogenic material between the bowel loops.
To assess the SMA flow the transducer will be held in the longitudinal section just below the xiphoid. Elevated systolic velocities (up to100–120 cm/s), and high diastolic velocity will be suspicious for NEC.
Ultrasonographer experience will vary between centers (5 to 20 years of experience). All examinations will be performed at the bedside and saved on a secure web-based platform. No specific pre-test requirements will be required.
Plain AR using a vertical and horizontal beam will be repeated every 12–24 h as the disease tends to progress rapidly (42). The following plain abdominal radiography findings will be considered typical for NEC:
• PI is most commonly present in the distal small bowel and large bowel, hence it is usually seen in the right lower quadrant, although it may be present in any part of the gastrointestinal tract (43, 44).
• PVG as an extension of intramural gas present in bowel wall veins, passing into the portal vein system (28, 29).
• Free intraperitoneal gas as a result of bowel perforation, which usually is in the distal ileum and proximal colon. It is the only universally accepted radiologic indication for surgical intervention (12).
We will define AUS as positive for NEC when three of the following findings are appreciated on examination (41):
1. Abnormal bowel wall thickness (<1.0 mm or >2,7 mm)
2. PI
3. Free abdominal fluid as a focal fluid collection
4. Abnormal SMA blood flow, or bowel wall perfusion.
And one of the listed findings:
1. Free abdominal air
2. Delayed peristalsis
3. PVG.
AR will be classified as positive for NEC, if one of the following findings will be present (23):
• Intramural gas (pneumatosis intestinalis)
• Portal venous gas
• Free intraperitoneal gas
And
• Bowel dilatation.
Prior to recruitment commencement, a meeting will be scheduled in each center to introduce the study to unit staff. This session will include:
• Brief presentation on study aims and eligibility criteria.
• Introduction to oral and written informed consent process.
• Presentation of data collection platform and its requirements.
• NEC diagnosis guidelines for Radiologists and Ultrasonographers (if requested).
A subsequent meeting will take place two weeks after initiating the study. Staff will be asked about any problems they might be experiencing with implementing the study, such as patient recruitment, data collection and NEC diagnosis.
Multi-center research meetings will be held two times a year for the first 2 years to improve adherence to study protocol, improve recruitment rates and resolve on-going issues.
All data will be collected on a secure electronic database and will be available on request.
All randomized infants who are prematurely discontinued from study drug will be considered off study intervention/on study. They will follow the same participant timetable as those infants who continue study intervention. All these infants will be followed through 12 months as scheduled.
Once an infant is enrolled or randomized, the study site will make every reasonable effort to follow the infant for the entire study period. It is projected that the rate of loss-to-follow-up on an annual basis will be at most 20%. Each study site staff will develop and implement local standard operating procedures to achieve this level of follow-up.
Study data will be collected and managed using REDCap (45, 46), an electronic data capture tools hosted at [Princess Anna Mazowiecka's Hospital MUW]. REDCap is a secure, web-based software platform designed to support data capture for research studies, providing (1) an intuitive interface for validated data capture; (2) audit trails for tracking data manipulation and export procedures; (3) automated export procedures for seamless data downloads to common statistical packages; and (4) procedures for data integration and interoperability with external sources (41, 42).
Data integrity will be enforced through a variety of mechanisms. Referential data rules, valid values, range checks, and consistency checks against data already stored in the database (i.e., longitudinal checks) will be supported. Modifications to data written into the database will be documented through either the data change system or an inquiry system. Data entered in the database will be retrievable for viewing through the data entry applications. The type of activity that an individual user may undertake will be regulated by privileges associated with his/her user identification code and password. A complete back up of the database will be performed twice a month.
Complete patient and study information will be stored on REDCap. Only researchers involved in the study will be provided with a personalized login and password to access the study information. The statistical team will not have access to sensitive data such as date of birth, address, contact details. All records containing the above patient details and relevant medical history will be stored separately in a locked file cabinet.
Not applicable.
As the trial is designed as a superiority study, both primary and secondary outcomes will be analyzed based on the per-protocol (PP) approach.
For primary outcomes and dichotomous secondary outcomes, between-group differences, and the two-sided 95% confidence interval (CI) for the estimated difference approach will be used (47–49).
For continuous outcomes, means/medians and 95% CIs will be calculated. Differences in changes from baseline between treatment groups will be compared using a two-sample t test or Mann-Whitney U-test (50).
Additionally, a predictive model to clarify the risk of NEC complications in both study groups will be implemented. Statistical and machine learning techniques such as decision trees, random forests, and support vector machine (SVM) will be used (51–55).
All statistical calculation will be carried out using R package (The R Foundation Vienna, Austria) and Statsoft (Hamburg, Germany).
Our study is a multicentre study, located in 4 different unit. Three interim analyses (IA) will be performed on the primary end point every 100 recruited patients. IA will be conducted by an independent statistician, blinded for the treatment allocation. This will allow us to track trial data collected on case report forms and generate performance metrics. Additionally, it will make data and study information available in a timely manner and re-estimate the sample size if needed. Results of interim analyses will be reported to the DMC, which will decide whether the trial should be continued or stopped for futility based on the pre-specified criteria. The Peto approach will be used: the trial will be ended using symmetric stopping boundaries at P < 0.001 (56).
Additionally, sensitivity analysis for the primary outcomes will be carried out with an intention-to-treat (ITT) approach. Protocol deviations will be reviewed by a blinded adjudication DMC who will decide by consensus whether a patient should be included in the ITT or per protocol population. We do not plan any subgroup analyses. In case of missing data, standard data imputation algorithms will be used (e.g., multiple imputation) (55).
Access to the full protocol and participation level-data will be given on request from the corresponding author.
Given the methodology (randomized control trial) and vulnerable population (neonates with congenital heart disease) a Data Monitoring Committee (DMC) has been established. It will be combined of experienced, independent researchers and clinicians (biostatisticians, pediatric cardiologists, pediatric gastroenterologists and neonatologists). The DMC will be independent of the study organizers and will not have financial or intellectual conflict of interest.
It will play an advisory role to the sponsor of the trial, not an executive. It will be up to the sponsor whether to decide or not to accept the DMC's recommendations.
The DMC will monitor the study safety, assess the trial continuing validity and scientific merit. Additionally, it will assess patient recruitment, protocol compliance and data quality.
During the period of recruitment to the study, interim analyses will be supplied, in strict confidence, to the DMC, together with any other analyses that the committee may request. This may include analyses of data from other comparable trials. Considering the interim analysis, the DMC will advise the TSC if, in its view the active intervention has been proved, beyond reasonable doubt, to be different from the control (standard management) for all or some types of participants.
The TSC can then decide whether to modify the trial. Unless this happens, the TSC, clinical collaborators will remain ignorant of the interim results.
The frequency of interim analyses will be carried out every 100 recruited patients, however the schedule may be modified based on depend on the judgement of the Chair of the DMC, in consultation with the TSC.
We will define an adverse event (AE) as any untoward medical occurrence in a subject without regard to the possibility of a causal relationship. AE will be collected after the subject has provided consent and enrolled in the study. All AE occurring after entry into the study and until hospital discharge will be recorded. An AE that meets the criteria for a serious adverse event (SAE) between study enrolment and hospital discharge will be reported to the local Ethical Committee. A SAE for this study is any untoward medical occurrence that is believed by the investigators to be causally related to study-intervention and results in any of the following: Life-threatening condition (that is, immediate risk of death); severe or permanent disability, prolonged hospitalization. SAE occurring after a subject is discontinued from the study will NOT be reported unless the investigators feels that the event may have been caused by the study drug or a protocol procedure.
We do not plan to audit the trial, unless requested by the DMC.
Any modifications to the protocol which may impact on the conduct of the study, potential benefit of the patient or may affect patient safety, including changes of study objectives, study design, patient population, sample sizes, study procedures, or significant administrative aspects will require a formal amendment to the protocol. Such will need to be approved by the Research Ethics Board of the Medical University of Warsaw prior to implementation and notified to the health authorities in accordance with local regulations.
We plan to publish the full protocol, so it shall be widely available due to open access. We plan to submit our findings to international peer-reviewed journals (pediatric, gastroenterology, nutrition). Abstract will be submitted to local and international conferences.
Adequate nutrition is essential to improve short-and long-term outcome in newborns born with CHD. However, significant variation among units worldwide exist in introducing and advancing enteral nutrition in this group of babies. Concerns mainly relate to the risk of feeding intolerance and bowel perforation. Our study will be the first randomized control trial to evaluate if standard (as in healthy newborns) initiation and advancement of enteral feeding is safe, improves short term outcomes and does not increase the risk of NEC. If the studied feeding regime proves to be intact, swift implementation and advancement of enteral nutrition may become a recommendation.
The studies involving human participants were reviewed and approved by the Research Ethical Board of the Medical University of Warsaw KB/154/2021. Written, informed consent to participate will be obtained from all participants.
JS-S conceived the study, led the proposal and protocol development. AP, AW-S, MŻ, JL-G, WZ, MC, and RB contributed to study design and to development of the proposal. KF was the lead trial methodologist. All authors contributed to the article and approved the submitted version.
The study will be funded by an internal departmental fund of the Medical University of Warsaw. The funder will not have any role during the study execution, analyses, interpretation of the data or decision to submit results (Grant number: 1W63/1/Z/GW/N/22/22:N).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
NEC, necrotizing enterocolitis; CHD, congenital heart disease; TGA, Transposition of the Great Arteries; TOF, Tetralogy of Fallot; HLHS, Hypoplastic left heart syndrome; MUW, Medical University of Warsaw; CHMI- Children's Health Memorial Institute; MRN, Medical record number; MEN, Minimal enteral nutrition; MN, Medical notes; VIS, Vasoactive inotropes score; VA, vasoactive support; MAP, mean arterial pressure; CRP, C, reactive pressure; PCT, Procalcitonin; AUS, Abdominal ultrasound; CD, Color Doppler; SMA, Superior Mesenteric artery; BWP, Bowel Wall Perfusion; AR, Abdominal radiograph; PVG, Portal vein gas; DMC, Data monitoring committee; CI, Confidence interval; SVM, Support Vector Machine; ITT, intention to treat; TSC, Trial Steering Committee; AE, adverse event; SAE, serious adverse event; CLABSI, central line associated blood stream infection.
1. McCarter RJ, Wilson PD, Boughman JA, Brenner JI. Downing, Congenital cardiovascular malformations in the Baltimore-Washington area. Md Med J. (1985)34:1079–83.
2. Blasquez A, Clouzeau H, Fayon M, Mouton JB, Thambo JB, Enaud R, et al. Evaluation of nutritional status and support in children with congenital heart disease. Eur J Clin Nutr. (2016) 70:528–31. doi: 10.1038/ejcn.2015.209
3. Varan B, Tokel K, Yilmaz G. Malnutrition and growth failure in cyanotic and acyanotic congenital heart disease with and without pulmonary hypertension. Arch Dis Child. (1999) 81:49–52. doi: 10.1136/adc.81.1.49
4. Nydegger A, Bines JE. Energy metabolism in infants with congenital heart disease. Nutrition. (2006) 22:697–704. doi: 10.1016/j.nut.2006.03.010
5. Scahill CJ, Graham EM, Atz AM, Bradley SM, Kavarana MN, Zyblewski SC. Preoperative feeding neonates with cardiac disease. World J Pediatr Congenit Heart Surg. (2017) 8:62–8. doi: 10.1177/2150135116668833
6. Choi G-J, Song J, Kim H, Huh J, Kang IS, Chang YS, et al. Development of necrotizing enterocolitis in full-term infants with duct dependent congenital heart disease. BMC Pediatr. (2022) 22:174. doi: 10.1186/s12887-022-03186-5
7. McElhinney DB, Hedrick HL, Bush DM, Pereira GR, Stafford PW, Gaynor JW, et al. Necrotizing enterocolitis in neonates with congenital heart disease: risk factors and outcomes. Pediatrics. (2000) 106:1080–7. doi: 10.1542/peds.106.5.1080
8. Kelleher ST, McMahon CJ, James A. Necrotizing enterocolitis in children with congenital heart disease: a literature review. Pediatr Cardiol. (2021) 42:1688–99. doi: 10.1007/s00246-021-02691-1
9. Miller TA, Minich LL, Lambert LM. Joss-Moore L, Puchalski MD. Abnormal abdominal aorta hemodynamics are associated with necrotizing enterocolitis in infants with hypoplastic left heart syndrome. Pediatric Cardiology. (2014) 35:616–21. doi: 10.1007/s00246-013-0828-8
10. Siano E, Lauriti G, Ceccanti S, Zani A. Cardiogenic necrotizing enterocolitis: a clinically distinct entity from classical necrotizing enterocolitis. Eur J Pediatr Surg. (2019) 29:14–22. doi: 10.1055/s-0038-1668144
11. Kataria-Hale J, Osborne SW, Hair A, Hagan J, Pammi M. Preoperative feeds in ductal-dependent cardiac disease: a systematic review and meta-analysis hospital. Pediatrics. (2019) 9:998–1006.
12. Scahill CJ, Graham EM, Atz AM, Bradley SM, Kavarana MN, Zyblewski SC. Preoperative feeding neonates with cardiac disease:is the necrotizing enterocolitis fear justified? World J Pediatr Congenit Heart Surg. (2017) 8:62-8.
13. Tume LN, Valla FV, Joosten K, Jotterand Chaparro C, Latten L, Marino LV, et al. Nutritional support for children during critical illness: European Society of Pediatric and Neonatal Intensive Care (ESPNIC) metabolism, endocrine and nutrition section position statement and clinical recommendations. Intensive Care Med. (2020) 46:411–25. doi: 10.1007/s00134-019-05922-5
14. Karpen HE. Nutrition in the cardiac newborns: evidence-based nutrition guidelines for cardiac newborns. Clin Perinatol. (2016) 43:131–45.
15. Toole BJ, Toole LE, Kyle UG, Cabrera AG, Orellana RA, Coss-Bu JA. Perioperative nutritional support and malnutrition in infants and children with congenital heart disease. Congenit Heart Dis. (2014) 9:15–25. doi: 10.1111/chd.12064
16. Slicker J, Sables-Baus S, Lambert LM, Peterson LE, Woodard FK, Ocampo EC, et al. Perioperative feeding approaches in single ventricle infants: a survey of 46 centers. Congenit Heart Dis. (2016) 11:707–15. doi: 10.1111/chd.12390
17. Natarajan G, Reddy Anne S, Aggarwal S. Enteral feeding of neonates with congenital heart disease. Neonatology. (2010) 98:330–6. doi: 10.1159/000285706
18. Maynord PO, Johnson M, Xu M, Slaughter JC, Killen SA. A multi-interventional nutrition program for newborns with congenital heart disease. J Pediatr. (2021) 228:66-73 e2.
19. Slicker J, Hehir DA, Horsley M, Monczka J, Stern KW, Roman B, et al. Nutrition algorithms for infants with hypoplastic left heart syndrome; birth through the first interstage period. Congenit Heart Dis. (2013) 8:89–102. doi: 10.1111/j.1747-0803.2012.00705.x
20. Toms R, Jackson KW, Dabal RJ, Reebals CH, Alten JA. Preoperative trophic feeds in neonates with hypoplastic left heart syndrome. Congenit Heart Dis. (2015) 10:36–42. doi: 10.1111/chd.12177
21. Gephart SM, Moore EF, Fry E. Standardized feeding protocols to reduce risk of necrotizing enterocolitis in fragile infants born premature or with congenital heart disease: implementation science needed. Crit Care Nurs Clin North Am. (2018) 30:457–66. doi: 10.1016/j.cnc.2018.07.003
22. Iannucci GJ, Oster ME, Mahle WT. Necrotising enterocolitis in infants with congenital heart disease: the role of enteral feeds. Cardiol Young. (2013) 23:553–9. doi: 10.1017/S1047951112001370
23. Dutta S, Singh B, Chessell L, Wilson J, Janes M, McDonald K, et al. Guidelines for feeding very low birth weight infants. Nutrients. (2015) 7:423–42. doi: 10.3390/nu7010423
24. Gaafar A, Ismail A, Kadaro AE, Hashim E, Khalil EA, Hassan AE. Necrotizing and suppurative lymphadenitis in Leishmania major infections. Trop Med Int Health. (1996) 1:243–50. doi: 10.1111/j.1365-3156.1996.tb00034.x
25. Kliegman RM, Walsh MC. Neonatal necrotizing enterocolitis: pathogenesis, classification, and spectrum of illness. Curr Probl Pediatr. (1987) 17:213–88.
26. Martinez-Millana A, Hulst JM, Boon M, Witters P, Fernandez-Llatas C, Asseiceira I, et al. Optimisation of children z-score calculation based on new statistical techniques. PLoS One. (2018) 13:e0208362. doi: 10.1371/journal.pone.0208362
27. Gaies MG, Gurney JG, Yen AH, Napoli ML, Gajarski RJ, Ohye RG, et al. Vasoactive-inotropic score as a predictor of morbidity and mortality in infants after cardiopulmonary bypass. Pediatr Crit Care Med. (2010) 11:234–8. doi: 10.1097/PCC.0b013e3181b806fc
28. Panchal AK, Manzi J, Connolly S, Christensen M, Wakeham M, Goday PS, et al. Safety of enteral feedings in critically ill children receiving vasoactive agents. J Parenter Enter Nutr. (2016) 40:236–41. doi: 10.1177/0148607114546533
29. Victora CG, Bahl R, Barros AJ, França GV, Horton S, Krasevec J, et al. Breastfeeding in the 21st century: epidemiology, mechanisms, and lifelong effect. Lancet. (2016) 387:475–90. doi: 10.1016/S0140-6736(15)01024-7
30. Labbok M, Belsey M, Coffin C. A call for consistency in defining breast-feeding. Am J Public Health. (1997) 87:1060–1. doi: 10.2105/AJPH.87.6.1060
31. Carlo WF, Kimball TR, Michelfelder EC, Border WL. Persistent diastolic flow reversal in abdominal aortic doppler-flow profiles is associated with an increased risk of necrotizing enterocolitis in term infants with congenital heart disease. Pediatrics. (2007) 119:330–5. doi: 10.1542/peds.2006-2640
32. Cantinotti M, Giordano R, Corsini I, Dani C, Scalese M, Murzi B, et al. Echocardiographic nomograms for upper abdominal aorta Doppler systolic wave values and systo-diastolic diameters variations in children. J Cardiol. (2018) 71:394–400. doi: 10.1016/j.jjcc.2017.09.016
33. Jeffries HE, Wells WJ, Starnes VA, Wetzel RC, Moromisato DY. Gastrointestinal morbidity after Norwood palliation for hypoplastic left heart syndrome. Ann Thorac Surg. (2006) 81:982–7. doi: 10.1016/j.athoracsur.2005.09.001
34. Lau PE, Cruz SM, Ocampo EC, Nuthakki S, Style CC, Lee TC, et al. Necrotizing enterocolitis in patients with congenital heart disease: a single center experience. J Pediatr Surg. (2018) 53:914–7. doi: 10.1016/j.jpedsurg.2018.02.014
35. Fisher JG, Bairdain S, Sparks EA, Khan FA, Archer JM, Kenny M, et al. Serious congenital heart disease and necrotizing enterocolitis in very low birth weight neonates. J Am Coll Surg. (2015) 220 1018-26 e14. doi: 10.1016/j.jamcollsurg.2014.11.026
36. Wang H, Chow SC. Sample Size Calculation for Comparing Proportions. In: Wiley Encyclopedia of Clinical Trials. New York, NY (2007).
37. Walsh MC, Kliegman RM. Necrotizing enterocolitis: treatment based on staging criteria. Pediatr Clin North Am. (1986) 33:179–201.
38. Neu J, Walker WA. Necrotizing enterocolitis. N Engl J Med. (2011) 364:255–64. doi: 10.1056/NEJMra1005408
39. O'Reilly MLD, Greecher C, L Kimberlin, D Mujsce, et al. Evaluation, development, and implementation of potentially better practices in neonatal intensive care nutrition. Pediatrics. (2003) 111:e461–70.
40. S Krishnamurthy P., Gupta S., Debnath S., Gomber. Slow vs. rapid enteral feeding advancement in preterm newborn infants 1000-1499 g: a randomized controlled trial. Acta Paediatr. (2010) 99:42-6.
41. Bohnhorst B. Usefulness of abdominal ultrasound in diagnosing necrotising enterocolitis. Arch Dis Child Fetal Neonatal Ed. (2013) 98:F445–50. doi: 10.1136/archdischild-2012-302848
42. Epelman M, Daneman A, Navarro OM, Morag I, Moore AM, Kim JH, et al. Necrotizing enterocolitis: review of state-of-the-art imaging findings with pathologic correlation. Radiographics. (2007) 27:285–305. doi: 10.1148/rg.272055098
43. Santulli TV, Schullinger JN, Heird WC, Gongaware RD, Wigger J, Barlow B, et al. Acute necrotizing enterocolitis in infancy: a review of 64 cases. Pediatrics. (1975) 55:376–87.
44. Leonidas JC, Hall RT, Amoury RA. [Critical evaluation of the roentgen signs of neonatal necrotizing enterocolitis]. Ann Radiol. (1976) 19:123–32.
45. Harris PA, Taylor R, Thielke R. Payne, Gonzalez JN, Conde JG. Research electronic data capture (REDCap)–a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. (2009) 42:377–81.
46. Harris PA, Taylor R, Minor BL, Elliott V, Fernandez M, O'Neal L, et al. The REDCap consortium: building an international community of software platform partners. J Biomed Inform. (2019) 95:103208. doi: 10.1016/j.jbi.2019.103208
47. Z. W. A new exact confidence interval for the difference of two binominal proportions. Revstat Stat J. (2020) 18:9.
48. Jaworski S, Zielinski W. New test for comparision of binominal proportions: power comparison. Colloquium Biometricum. (2017) 47:5.
50. Krzych-Falta E, Furmanczyk K, Samolinski B. Specificity and sensitivity assessment of selected nasal provocation testing techniques. Postepy Dermatol Alergol. (2016) 33:464–8. doi: 10.5114/pdia.2016.61339
51. Hastie T, Tibshirani R, Friedman JH, Friedman JH. The Elements of Statistical Learning: Data Mining, Inference, and Prediction. New York: springer. (2009).
52. Zalewska M, Furmańczyk KO, Jaworski S, Niemiro W, Samoliński BO. The prevalence of asthma and declared asthma in Poland on the basis of ECAP survey using correspondence analysis. Comput Math Methods Med. (2013) 2013:597845. doi: 10.1155/2013/597845
53. Chrzanowska M, Alfaro E, Witkowska D. Credit Scoring With Individuals and Ensemble Trees. New York, NY: Wiley Online Library (2018).
54. Chrzanowska M, Alfaro E, Witkowska D. A study on the stability of ensemble trees: example of the Polish credit scoring application. Polish J Environ Stud. (2009) 18:63–8.
55. Austin PC, White IR, Lee DS, van Buuren S. Missing data in clinical research: a tutorial on multiple imputation. Can J Cardiol. (2021) 37:1322–31. doi: 10.1016/j.cjca.2020.11.010
Keywords: congenital heart defect, enteral feeding algorithm, intensive care unit, neonate, duct dependant
Citation: Seliga-Siwecka J, Płotko A, Wójcik-Sep A, Bokiniec R, Latka-Grot J, Żuk M, Furmańczyk K, Zieliński W and Chrzanowska M (2022) Effect of standardized vs. local preoperative enteral feeding practice on the incidence of NEC in infants with duct dependent lesions: Protocol for a randomized control trial. Front. Cardiovasc. Med. 9:893764. doi: 10.3389/fcvm.2022.893764
Received: 10 March 2022; Accepted: 18 July 2022;
Published: 08 September 2022.
Edited by:
Sanjay Patole, King Edward Memorial Hospital, AustraliaReviewed by:
Haribalakrishna Balasubramanian, Surya Hospitals, IndiaCopyright © 2022 Seliga-Siwecka, Płotko, Wójcik-Sep, Bokiniec, Latka-Grot, Żuk, Furmańczyk, Zieliński and Chrzanowska. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Joanna Seliga-Siwecka, am9hbm5hLnNlbGlnYUB3dW0uZWR1LnBs
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.