
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Cardiovasc. Med. , 14 July 2022
Sec. Cardiovascular Surgery
Volume 9 - 2022 | https://doi.org/10.3389/fcvm.2022.892516
This article is part of the Research Topic Current Trends and Strategies for the Management of Type A Aortic Dissection View all 11 articles
 Arash Mehdiani1
Arash Mehdiani1 Yukiharu Sugimura1
Yukiharu Sugimura1 Louise Wollgarten1
Louise Wollgarten1 Moritz Benjamin Immohr1
Moritz Benjamin Immohr1 Sebastian Bauer1Hubert Schelzig2
Sebastian Bauer1Hubert Schelzig2 Markus Udo Wagenhäuser2Gerald Antoch3Artur Lichtenberg1*
Markus Udo Wagenhäuser2Gerald Antoch3Artur Lichtenberg1* Payam Akhyari1
Payam Akhyari1Introduction: Acute aortic dissection type A (AADA) is associated with high perioperative morbidity and mortality. A novel non-covered hybrid prosthesis (Ascyrus Medical Dissection Stent (AMDS) Hybrid Prosthesis, Cryolife/Jotec, Hechingen, Germany) can be easily implanted to stabilize the true lumen (TL), improve remodeling, and preserve organ perfusion. Although developed for implantation in aortic zone 0, occasionally, partial replacement of the aortic arch and further distal implantation of AMDS may appear favorable. Implantation of AMDS with anastomosis line beyond zone 0 has not been described yet.
Materials and Methods: Between 08/2019 and 12/2020, a total of n = 97 patients were treated due to AADA at a single University hospital. Of those, n = 28 received an AMDS hybrid prosthesis, of whom in eight patients, due to intraoperative finding the distal anastomosis line was placed distal to the brachiocephalic trunk. Three patients had AMDS implantation in zone I and four were treated by implantation of the prostheses in zone II, and one patient had the implantation performed in zone III. Clinical outcome and the development of a proportional area of TL and false lumen (FL) at defined levels of the thoracic aorta were analyzed.
Results: None of the surviving patients (87.5%) showed signs of clinical malperfusion (i.e., stroke, spinal cord injury, and need for dialysis). A postoperative CT scan showed an open TL in all patients. The proportion of TL with respect to total aortic diameter (TL+FL) was postoperatively significantly higher in zone III (p = 0.016) and at the level of T11 (p = 0.009). The mean area of TL+FL was comparable between pre- and postoperative CT-scan (p = n.s.). One patient with preoperative resuscitation died of multiple organ failure on extracorporeal life support on postoperative day 3.
Conclusion: Implantation of AMDS can be safely performed in patients who need partial replacement of the aortic arch beyond zone 0. The advantages of the AMDS can be combined with those of the total arch repair (remodeling of the arch and prevention of TL collapse) without the possible disadvantages (risk of spinal cord injury).
Acute aortic dissection type A (AADA) remains a life-threatening condition despite the continuous improvement of operative technique and perioperative care for decades (1). Emergency surgery represents the first-line therapy and aims at replacement of the ascending aorta and removal of the primary entry tear (2). An extension of surgery to the aortic arch is preferred when an intimal tear is localized in this region (3–5). In the extreme, total aortic arch replacement (TAR) with concomitant implantation of a stent-graft prosthesis in the descending thoracic aorta (referred to as frozen elephant trunk) may be performed, which is currently regarded as the ultimate solution at the technical level to promote favorable aortic remodeling (6, 7). However, real-world data demonstrate a significant increase in 30-day mortality with TAR when compared with the technically more simple replacement for the ascending aorta with an open distal anastomosis, the so-called hemiarch replacement (HAR) (8), while HAR has been associated with an increased risk for aortic re-intervention in the follow-up (9). To simplify the therapy of AADA and make the operation performable for most surgeons irrespective of their specific experience profile, HAR has become a commonly applied technique. Furthermore, according to previous reports, TAR can be performed by nearly all surgeons due to the simplification of the implantation technique, however, an increased risk of stroke remains (10, 11). The Ascyrus Medical Dissection Stent (AMDS Hybrid Prosthesis, Cryolife/Jotec, Hechingen, Germany) has been designed to simplify surgical treatment of the downstream thoracic aorta by implantation line located proximal to the brachiocephalic trunk (zone 0), in addition to the standard replacement of the ascending aorta. Initial short-term results from a multicenter study suggest that the use of AMDS may have a positive impact by (1) sealing the distal anastomotic line to avoid distal anastomotic line new entry (DANE), (2) further supporting positive aortic remodeling by avoiding true lumen (TL) collapse, and (3) also reducing malperfusion associated with AADA (12). However, DANE is only one of several factors contributing to adverse remodeling of the aortic arch and the downstream thoracic aorta. The presence of intimal tear in the aortic arch and a retrograde perfusion of the supra-aortic vessels due to a re-entry further distally in the supra-aortic vessels have been reported as relevant factors requiring an extension of aortic replacement beyond zone 0 (13). Until now, there are reports on the outcome and prognostic value of AMDS implantation distal to the brachiocephalic trunk, i.e., beyond zone 0. It may be hypothesized that such an approach preserves the beneficial impact of AMDS on remodeling of the distal thoracic aorta while reducing the impact of retrograde supra-aortic perfusion of false lumen (FL) and also reducing the proportion of dissected aortic wall in the arch region. This report summarizes our experience with a consecutive series of patients undergoing emergency aortic surgery for AADA involving AMDS implantation in the aortic arch zone I–III.
In this study, 97 consecutive patients undergoing cardiac surgery due to AADA at a single university hospital between 08/2019 and 12/2020 were reviewed. Of these, 28 patients (28.9%) received an AMDS hybrid prosthesis at the decision of the attending surgeon. This report analyses the in-hospital course and outcome of those patients in whom AMDS was implanted with the anastomosis line beyond zone 0: three in zone I (between the brachiocephalic trunk and the left common carotid artery, LCCA), four in zone II [between LCCA and left subclavian artery (LSA)], and one in zone III (distal to the LSA) (Table 1).
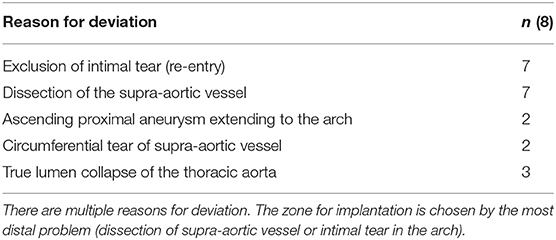
Table 1. Reasons for deviation from zone 0.
Demographic data, comorbidities, intraoperative procedures, and postoperative variables of outcome were collected systematically and entered prospectively into a standardized institutional database. Expected mortality was determined using prognostic models from the literature [EuroScore II, Penn, and German Registry for Acute Aortic Dissection Type A (GERAADA) models (14)]. These data were analyzed retrospectively in this study.
The AMDS consists of an uncovered stent part and a proximal felt neck. Both elements intend to readapt the intima against the media and the adventitia and thereby reduce the force of separation between these layers, especially in the area of the anastomosis. This reduces the incidence of DANE and leads to remodeling of the aorta. Due to the fact that the stent is not covered, an occlusion of vertebral vessels is impossible.
Operative diagnosis was confirmed in all patients based on preoperative contrast-enhanced CT scans covering at least the thoracic cavity. Measurement of the aortic diameter was performed as described before (15) and suggested by STORAGE guidelines (16). Regardless of the localization of intimal tear (entry), the total diameter of the aorta including the aortic wall (such as TL and FL) at the level of zone I and at the level of pulmonary bifurcation was documented. All patients received at least one postoperative CT scan. In all in-hospital survivors, pre-discharge CT scans were performed.
Arch growth was determined in centerline measurement on the planes perpendicular to the aorta using multiplanar CT reformation at the level of zone III. The diameter and the area of TL and FL were measured at the level zone III and at the level of the 11th thoracic vertebrae (T11). For comparison, CT scan images obtained prior to the operation and prior to discharge were analyzed. For a standardized comparison, the ratio of TL area to FL area was calculated and analyzed.
All patients underwent emergency surgery with cardiopulmonary bypass (CPB) initiated with arterial cannulation via the right axillary artery and venous cannulation of the right atrium or the right femoral vein. By clamping the innominate artery, lower body circulatory arrest was initiated at a body core temperature of 26–28°C measured in the bladder, while unilateral antegrade cerebral perfusion was achieved with continued perfusion of the right axillary artery. After transecting the ascending aorta, a balloon-inflatable perfusion catheter was endoluminally introduced, and perfusion of the LCCA was achieved for bilateral antegrade cerebral perfusion as the standard technique. Intraoperative near-infrared spectroscopy (NIRS) was used to monitor cerebral oxygenation, particularly during CPB time and hypothermic lower body circulatory arrest (HCA). Further aortic transection was performed up to the intended anastomosis line. AMDS was then implanted using a Teflon stripe on the adventitial aortic side to re-enforce the anastomosis line. Either a branched prosthesis (n = 3) or a tube graft (n = 5) was used for partial arch replacement. During reperfusion time, supra-aortic vessels were anastomosed to side branches where a branched prosthesis was used, or a small-diameter single tube graft (10 or 12 mm) was employed as an interposition graft for anastomosis of the supra-aortic vessels (Figure 1).
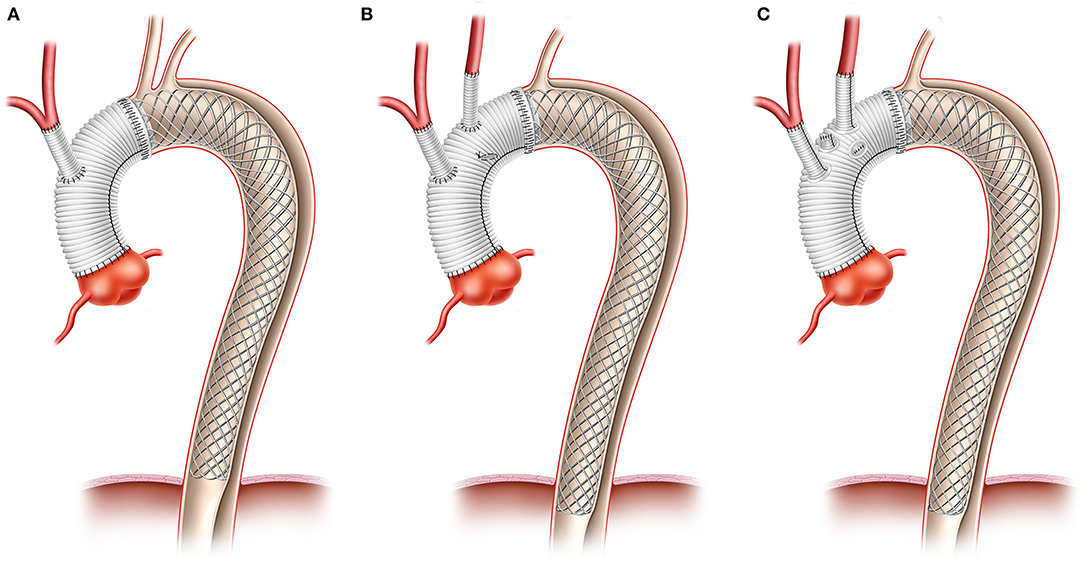
Figure 1. Morphology of different surgical procedure. Anastomosis was ether performed in zone I using a single tube graft for INA (A), or more distally using single tubes for the anastomosis of supra aortic vessels (B) or a branched prosthesis (C).
This study was approved by the Ethics Committee of the Medical Faculty of the Heinrich Heine University Düsseldorf (Ref. 2016116135).
Statistical analyses were performed with the Statistical Package for Social Sciences® (SPSS) 25.0 (IBM, Chicago, USA). Using this program, descriptive statistics and statistical comparisons between CT measurements were performed using the Wilcoxon matched-pairs signed rank test. A p-value of < 0.05 was considered statistically significant. Data are presented as mean ± standard error of mean (SEM).
Baseline characteristics are presented in Table 2. While the mean age was 63 ± 15 years, three patients were women (37.5%). No patient had previous cardiac surgery. Furthermore, two patients (25%) presented with prior intubation, of whom one patient was intubated in the setting of cardio-pulmonary resuscitation, while another patient was intubated due to neurological deterioration. Another patient presented with isolated left leg paresis. In addition, two patients were admitted to the hospital due to angina symptoms and ST elevation. The mean predicted 30-day mortality by the GERAADA score was 35.16 ± 18.33%. In the preoperative CT scan, two patients showed pericardial effusion. Angiographic signs of malperfusion were found in all patients.
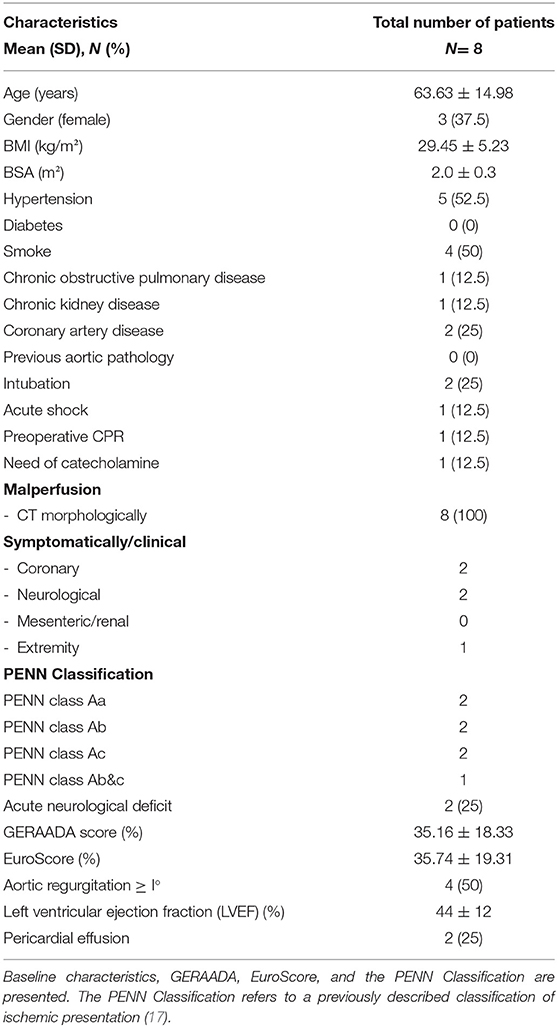
Table 2. Baseline characteristics.
Surgical and perioperative data are presented in Table 3. The mean CPB time was 285.25 ± 61.67 min. The lowest body core temperature was 26.2 ± 1.2°C. While lower body HCA time was 65.0 ± 12.6 min and cerebral perfusion time was 158.8 ± 63.2 min. Myocardial protection was achieved with the crystalloid cardioplegic solution in one patient, whereas a cold blood cardioplegic solution was used in the remaining seven patients.
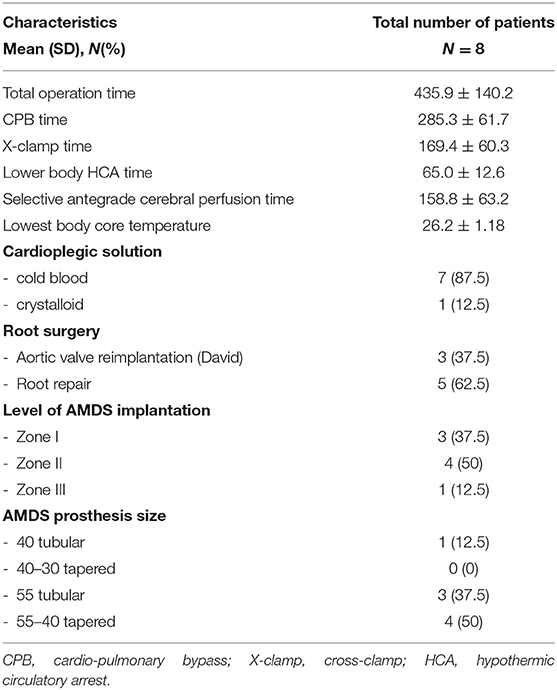
Table 3. Surgical and perioperative data.
Implantation of the AMDS was performed at the level of aortic arch zone III (n = 1), zone II (n = 4), or zone I (n = 3).
Measures of the postoperative outcome are summarized in Table 4. One patient with preoperative shock and cardiopulmonary resuscitation (CPR) needed postoperative extracorporeal life support (ECLS) with a consecutive bleeding disorder and the need for re-thoracotomy. This patient experienced therapy-refractory multiple organ failure and died on postoperative day 3. In-hospital and 30-day mortality were 12.5%. The mean duration of ICU stay was 4.72 ± 2.55 days, patients were discharged from the hospital after an average of 14.86 days. One patient underwent re-intubation due to CO2-retention and showed prolonged weaning from ventilator, underwent tracheotomy, and was transferred to respiratory weaning center on postoperative day 13. The mean ventilation time was 2.24 ± 0.88 days. Among surviving patients (7/8), no patient showed relevant postoperative neurological deficit (e.g., stroke and spinal cord injury). All survivors had a Glasgow Coma Scale (GCS) of 15 and a Richmond Agitation Sedation Scale (RASS) of 0 at the time point of discharge.
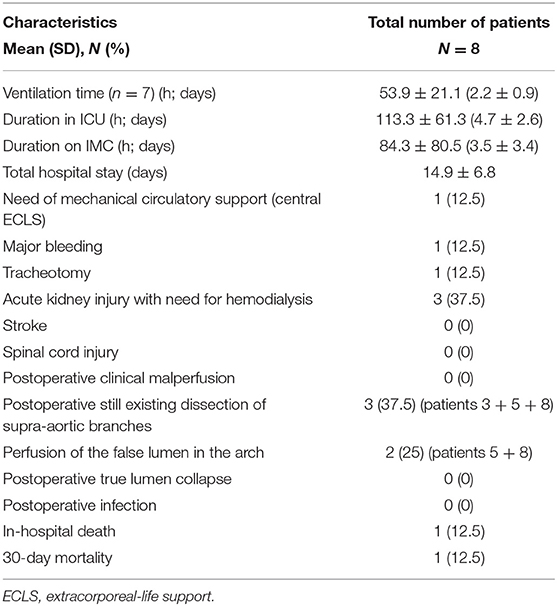
Table 4. Postoperative outcome.
Postoperative CT scans demonstrated that no patient suffered from TL collapse. At the level of the aortic arch, perfusion of the FL was detected in only two patients (arch remodeling). No patients experienced postoperative clinical malperfusion whereby in three patients, a dissection of supra-aortic vessels was detected even after the operation.
Table 5 shows the CT measurements. Area analyses demonstrated a significant enlargement of the TL in zone III and further distally (T11) when assessing postoperative images as compared with the preoperative status. A decrease in mean cross-sectional area of FL in the latter aortic segments was observed. The ratio between cross-sectional areas of TL and FL, respectively, was significantly higher postoperatively with more than doubled values at the level of zone III. The total diameter increased slightly at both analyzed levels of the thoracic aorta (Figure 2).
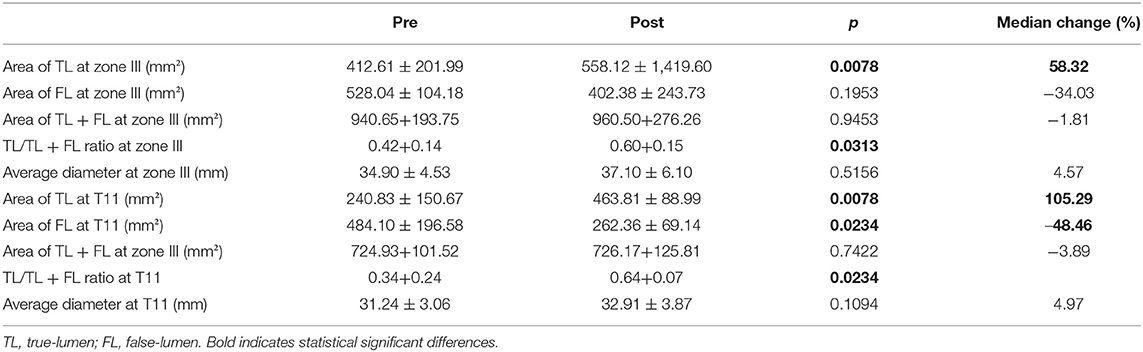
Table 5. CT measurements.
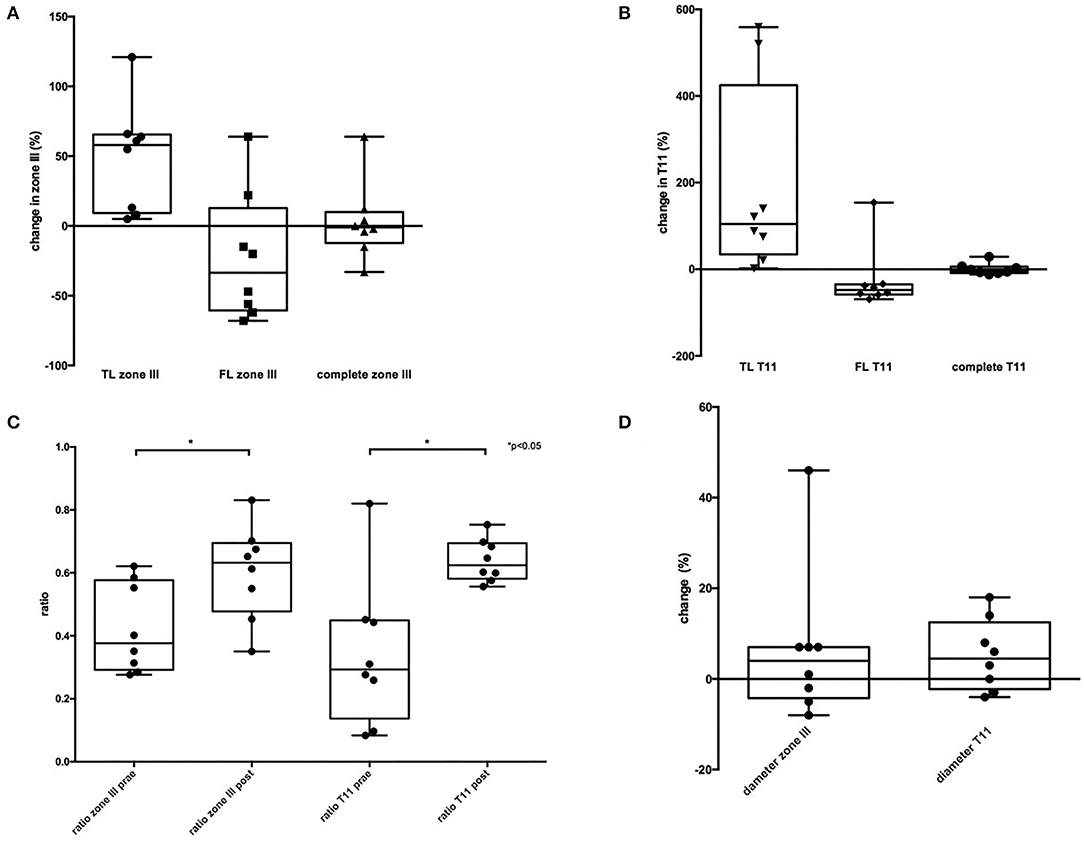
Figure 2. Comparison of CT-measurement. (A) Showing an enlargement of the true lumen (TL) and a decrease of the false lumen (FL) in zone III. Area of TL + FL did not changed. (B) TL showed a significantly bigger increase in T11 and a significant decrease of the FL. Area of TL + FL did not changed. (C) ratio of TL/TL + FL was postoperatively significant higher in both zones compared to preoperative CT. (D) total diameter showed no significant difference.
In this study, we demonstrate that implantation of an AMDS hybrid prosthesis beyond aortic arch zone 0 is feasible, reproducible, and safe. No patient suffered from postoperative spinal cord injury or malperfusion syndrome. A significant increase in perfused TL could be observed at different segments of the aorta, while a significant reduction of FL cross-sectional area was observed.
Obviously, a shorter operation time can be life-rescuing in the particular emergency settings of surgery for AADA (18). The primary aim of surgery in those patients with significantly impaired outcomes is early survival. Furthermore, the freedom of re-intervention should be aimed for as surgery and interventional procedures are associated with further risk of mortality and morbidity.
Hemiarch repair is associated with a shorter CPB time and operation time. However, the need for a second operation can be possible (9, 19–21). While total arch replacement with the frozen elephant trunk allows for the distal extension of the stent and allows sealing of potential distal intima tears. At the same time, covered stents can lead to spinal artery occlusion and spinal cord injury (22). In addition, neurological complications, e.g., stroke and TIA, can be higher in patients treated with TAR (7, 23). However, few AADA centers describe the feasibility of TAR due to a simplified operation technique with a proximalized distal anastomose line, in the acute setting of aortic dissection. Still, many centers prefer HAR over more complex surgery involving extended aortic arch replacement with or without stent graft implantation (TAR).
The AMDS hybrid prosthesis consists of an uncovered stent part and a proximal felt neck located at the level of the anastomotic line. Therefore, this device represents a hybrid solution intended for implantation at aortic zone 0 with technical complexity compared to that of the hemiarch replacement. However, the first clinical results suggest that an additional benefit of aortic remodeling with reduced malperfusion and a lower rate of DANE speak in favor of the implementation of AMDS (12, 24).
A few scenarios can make the use of the AMDS in the first moment impossible (Table 1). However, by shifting the distal anastomosis line more distally, AMDS could also be implanted in cases with focal re-entry in the aortic arch region. By careful preoperative assessment of the CT scan, preoperative determination of surgical strategy and location of the anastomotic line may be possible in the majority of patients presenting with AADA. The results presented herein show that this technique is a safe and reproducible alternative to TAR, combining the benefits from simple hemiarch with some benefits otherwise observed with the more complex total arch replacement. Intimal tears in the arch region could be resected, dissected supra-aortic vessels could be repaired in most patients, TL collapse could be prevented in all patients, and the risk of spinal cord injury was virtually omitted. We could also confirm the results of Bozso et al. (24), that by using the ADMS, DANE could be prevented and no antegrade perfusion was performed, which also led to the remodeling of the aorta.
The CT analysis showed a significant increase in the TL at the level of zone III and T11 in our cohort. No TL collapse was observed in any part of the aorta. The area of FL was reduced in six patients in zone III and seven patients in T11, leading to a relatively stable total area in both zones, indicating remodeling of the arch and the descending aorta. The ratios of TL/TL+FL were significantly higher in both zones, which may be regarded as evidence of favorable remodeling. While the ratio in preoperative CT scans is below 0.5 (meaning the proportion of TL compared with the entire aortic cross-sectional area is <50%), the TL proportion was increased in postoperative CT scans (ratio > 0.5).
In two patients, an increased aortic diameter on postoperative CT with growth of FL area at the level of aortic zone III and T11 was observed. In these patients, a persistent dissection of supra-aortic vessels (in particular of the LSA) was noted. We speculate that a suspected entry/re-entry in that vessel may cause a retrograde flow into the FL and thus may prevent a positive remodeling of the downstream thoracic aorta.
Preoperative CT scans are often not sensitive enough for identifying additional intima tears in the supra-aortic vessels. Recognized dissected supra-aortic vessels should be anastomosed separately to further enforce favorable arch remodeling. However, the associated increase in technical complexity may have a negative impact on the overall outcome, which will have to be addressed in future studies.
The purpose of this study was not to compare TAR with AMDS due to different patient selection criteria. The aim of the study was rather to show that in patients where a standard implantation of AMDS at the level of aortic zone 0 is not favored, a movement of the implantation site distally may be a solution to preserve the advantages associated with the implantation of the hybrid stent. For the first time, we could show that intimal tears in the arch region or circular re-entry sites at supra-aortic vessels can be treated using this strategy. However, a meticulous study of the preoperative CT scan is of paramount value for accurate strategy planning as well as to identify possible reentries in supra-aortic vessels, which may cause postoperative growth of FL and may lead to further need for intervention.
This study has several limitations. First, this is a retrospective observational study with a small number of patients. In addition, only immediate results are demonstrated; follow-up and long-term results are needed to evaluate the role of the presented approach for sustainable positive arch remodeling, especially in those two patients with the growth of the FL in the early period. As a standard, follow-up visits at 3, 6, and 12 months were presumed but could not be realized in all patients due to incompliance. Furthermore, longitudinal observation of a larger cohort is necessary.
The implantation of the novel hybrid prosthesis can be performed safely and reproducibly at the aortic arch levels beyond zone 0 in patients with AADA. Applying this approach, an early remodeling of the aortic arch and the prevention of TL collapse with no risk of spinal cord injury can be achieved.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by Ethics Committee of the Medical Faculty of the Heinrich Heine University Düsseldorf (Ref. 2016116135). Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
AM and PA conceived the concept of the present study and drafted the paper. LW, SB, and YS contributed with data collection. MI and GA supported CT-data acquisition and data processing. MW, AL, and HS contributed to study design. All authors took part in both data interpretation and critical revision of the manuscript.
This study was supported by institutional grants from the Department of Cardiac Surgery, University Hospital and the Medical Faculty of Heinrich Heine University Dusseldorf.
PA and MW have received speaker fees from Cryolife.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Khan H, Hussain A, Chaubey S, Sameh M, Salter I, Deshpande R, et al. Acute aortic dissection type A: impact of aortic specialists on short and long term outcomes. J Card Surg. (2021) 36:952–8. doi: 10.1111/jocs.15292
2. Cohen RG, Hackmann AE, Fleischman F, Baker CJ, Cunningham MJ, Starnes VA, et al. Type A aortic dissection repair: how I teach it. Ann Thorac Surg. (2017) 103:14–7. doi: 10.1016/j.athoracsur.2016.10.048
3. Sievers HH, Rylski B, Czerny M, Baier ALM, Kreibich M, Siepe M, et al. Aortic dissection reconsidered: type, entry site, malperfusion classification adding clarity and enabling outcome prediction. Interact Cardiovasc Thorac Surg. (2020) 30:451–7. doi: 10.1093/icvts/ivz281
4. Rylski B, Beyersdorf F, Kari FA, Schlosser J, Blanke P, Siepe M. Acute type A aortic dissection extending beyond ascending aorta: Limited or extensive distal repair. J Thorac Cardiovasc Surg. (2014) 148:949–54; discussion 54. doi: 10.1016/j.jtcvs.2014.05.051
5. Czerny M, Rylski B. Acute type A aortic dissection reconsidered: it's all about the location of the primary entry tear and the presence or absence of malperfusion. Eur Heart J. (2021) 43:53–55. doi: 10.1093/eurheartj/ehab664
6. Malaisrie SC, Szeto WY, Halas M, Girardi LN, Coselli JS, et al. 2021 The American Association for Thoracic Surgery expert consensus document: Surgical treatment of acute type A aortic dissection. J Thorac Cardiovasc Surg. (2021) 162:735–58 e2. doi: 10.1016/j.jtcvs.2021.04.053
7. Shrestha M, Haverich A, Martens A. Total aortic arch replacement with the frozen elephant trunk procedure in acute DeBakey type I aortic dissections. Eur J Cardiothorac Surg. (2017) 51:i29–34. doi: 10.1093/ejcts/ezw341
8. Ok YJ, Kang SR, Kim HJ, Kim JB, Choo SJ. Comparative outcomes of total arch versus hemiarch repair in acute DeBakey type I aortic dissection: the impact of 21 years of experience. Eur J Cardiothorac Surg. (2021) 60:967–75. doi: 10.1093/ejcts/ezab189
9. Rylski B, Milewski RK, Bavaria JE, Vallabhajosyula P, Moser W, Szeto WY, et al. Long-term results of aggressive hemiarch replacement in 534 patients with type A aortic dissection. J Thorac Cardiovasc Surg. (2014) 148:2981–5. doi: 10.1016/j.jtcvs.2014.05.093
10. Berger T, Kreibich M, Mueller F, Rylski B, Kondov S, Schrofel H, et al. The frozen elephant trunk technique for aortic dissection is safe after previous aortic repair. Eur J Cardiothorac Surg. (2021) 59:130–6. doi: 10.1093/ejcts/ezaa288
11. Nakanishi S, Wakabayashi N, Ise H, Kitahara H, Hirofuji A, Ishikawa N, et al. Proximalized total arch replacement can be safely performed by trainee. Thorac Cardiovasc Surg. (2021) 69:336–44. doi: 10.1055/s-0040-1713354
12. Bozso SJ, Nagendran J, MacArthur RGG, Chu MWA, Kiaii B, El-Hamamsy I, et al. Dissected aorta repair through stent implantation trial: Canadian results. J Thorac Cardiovasc Surg. (2019) 157:1763–71. doi: 10.1016/j.jtcvs.2018.09.120
13. Heo W, Song SW, Lee KH, Kim TH, Baek MY, Yoo KJ, et al. Residual arch tears and major adverse events after acute DeBakey Type I aortic dissection repair. Ann Thorac Surg. (2018) 106:1079–86. doi: 10.1016/j.athoracsur.2018.05.067
14. Czerny M, Siepe M, Beyersdorf F, Feisst M, Gabel M, Pilz M, et al. Prediction of mortality rate in acute type A dissection: the German Registry for Acute Type A Aortic Dissection score. Eur J Cardiothorac Surg. (2020) 58:700–6. doi: 10.1093/ejcts/ezaa156
15. Montagner M, Kofler M, Heck R, Buz S, Starck C, Kurz S, et al. Initial experience with the new type A arch dissection stent: restoration of supra-aortic vessel perfusion. Interact Cardiovasc Thorac Surg. (2021) 33:276–83. doi: 10.1093/icvts/ivab085
16. Rylski B, Pacini D, Beyersdorf F, Quintana E, Schachner T, Tsagakis K, et al. Standards of reporting in open and endovascular aortic surgery (STORAGE guidelines). Eur J Cardiothorac Surg. (2019) 56:10–20. doi: 10.1093/ejcts/ezz145
17. Augoustides JG, Geirsson A, Szeto WY, Walsh EK, Cornelius B, Pochettino A, et al. Observational study of mortality risk stratification by ischemic presentation in patients with acute type A aortic dissection: the Penn classification. Nat Clin Pract Cardiovasc Med. (2009) 6:140–6. doi: 10.1038/ncpcardio1417
18. Yuan H, Sun Z, Zhang Y, Wu W, Liu M, Yang Y, et al. Clinical analysis of risk factors for mortality in Type A Acute Aortic Dissection: a single study From China. Front Cardiovasc Med. (2021) 8:728568. doi: 10.3389/fcvm.2021.728568
19. Norton EL, Wu X, Kim KM, Fukuhara S, Patel HJ, Deeb GM, et al. Is hemiarch replacement adequate in acute type A aortic dissection repair in patients with arch branch vessel dissection without cerebral malperfusion? J Thorac Cardiovasc Surg. (2021) 161:873–84 e2. doi: 10.1016/j.jtcvs.2020.10.160
20. Merkle J, Sabashnikov A, Deppe AC, Zeriouh M, Maier J, Weber C, et al. Impact of ascending aortic, hemiarch and arch repair on early and long-term outcomes in patients with Stanford A acute aortic dissection. Ther Adv Cardiovasc Dis. (2018) 12:327–40. doi: 10.1177/1753944718801568
21. Omura A, Miyahara S, Yamanaka K, Sakamoto T, Matsumori M, Okada K, et al. Early and late outcomes of repaired acute DeBakey type I aortic dissection after graft replacement. J Thorac Cardiovasc Surg. (2016) 151:341–8. doi: 10.1016/j.jtcvs.2015.03.068
22. Preventza O, Liao JL, Olive JK, Simpson K, Critsinelis AC, Price MD, et al. Neurologic complications after the frozen elephant trunk procedure: a meta-analysis of more than 3000 patients. J Thorac Cardiovasc Surg. (2020) 160:20–33 e4. doi: 10.1016/j.jtcvs.2019.10.031
23. Choudhury RY, Basharat K, Zahra SA, Tran T, Rimmer L, Harky A, et al. “Proximalization is advancement”-zone 3 frozen elephant trunk vs zone 2 frozen elephant trunk: a literature review. Vasc Endovascular Surg. (2021) 55:612–8. doi: 10.1177/15385744211002493
Keywords: acute aortic dissection type A (AADA), hemiarch and aortic arch replacement, aortic remodeling, frozen elephant trunk, AMDS
Citation: Mehdiani A, Sugimura Y, Wollgarten L, Immohr MB, Bauer S, Schelzig H, Wagenhäuser MU, Antoch G, Lichtenberg A and Akhyari P (2022) Early Results of a Novel Hybrid Prosthesis for Treatment of Acute Aortic Dissection Type A With Distal Anastomosis Line Beyond Aortic Arch Zone Zero. Front. Cardiovasc. Med. 9:892516. doi: 10.3389/fcvm.2022.892516
Received: 09 March 2022; Accepted: 14 June 2022;
Published: 14 July 2022.
Edited by:
Robert Jeenchen Chen, Stanford University, United StatesReviewed by:
Kai Zhang, The Affiliated Hospital of Xuzhou Medical University, ChinaCopyright © 2022 Mehdiani, Sugimura, Wollgarten, Immohr, Bauer, Schelzig, Wagenhäuser, Antoch, Lichtenberg and Akhyari. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Artur Lichtenberg, YXJ0dXIubGljaHRlbmJlcmdAbWVkLnVuaS1kdWVzc2VsZG9yZi5kZQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.