
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Cardiovasc. Med. , 02 June 2022
Sec. Heart Failure and Transplantation
Volume 9 - 2022 | https://doi.org/10.3389/fcvm.2022.891468
This article is part of the Research Topic Insights in Heart Failure and Transplantation: 2022 View all 13 articles
 Varius Dannenberg1Matthias Koschutnik1Carolina Donà1Christian Nitsche1Katharina Mascherbauer1Gregor Heitzinger1Kseniya Halavina1Andreas A. Kammerlander1Georg Spinka1Max-Paul Winter1Martin Andreas2Markus Mach2Matthias Schneider3,4Anna Bartunek5Philipp E. Bartko1Christian Hengstenberg1Julia Mascherbauer1,6Georg Goliasch1*
Varius Dannenberg1Matthias Koschutnik1Carolina Donà1Christian Nitsche1Katharina Mascherbauer1Gregor Heitzinger1Kseniya Halavina1Andreas A. Kammerlander1Georg Spinka1Max-Paul Winter1Martin Andreas2Markus Mach2Matthias Schneider3,4Anna Bartunek5Philipp E. Bartko1Christian Hengstenberg1Julia Mascherbauer1,6Georg Goliasch1*Introduction: Severe tricuspid regurgitation (TR) is a common condition promoting right heart failure and is associated with a poor long-term prognosis. Transcatheter tricuspid valve repair (TTVR) emerged as a low-risk alternative to surgical repair techniques. However, patient selection remains controversial, particularly regarding the benefits of TTVR in patients with pulmonary hypertension (PH).
Aim: We aimed to investigate the impact of preprocedural invasive hemodynamic assessment and procedural success on right ventricular (RV) remodeling and outcome.
Methods: All patients undergoing TTVR with a TR reduction of ≥1 grade without precapillary or combined PH [mean pulmonary artery pressure (mPAP) ≥25 mmHg, mean pulmonary artery Wedge pressure ≤ 15 mmHg, pulmonary vascular resistance ≥3 Wood units] were assigned to the responder group. All patients with a TR reduction of ≥1 grade and precapillary or combined PH were classified as non-responders. Patients with a TR reduction ≥2 grade were directly classified as responders, and patients without TR reduction were directly assigned as non-responders.
Results: A total of 107 patients were enrolled, 75 were classified as responders and 32 as non-responders. We observed evidence of significant RV reverse remodeling in responders with a decrease in RV diameters (−2.9 mm, p = 0.001) at a mean follow-up of 229 days (±219 SD) after TTVR. RV function improved in responders [fractional area change (FAC) + 5.7%, p < 0.001, RV free wall strain +3.9%, p = 0.006], but interestingly further deteriorated in non-responders (FAC −4.5%, p = 0.003, RV free wall strain −3.9%, p = 0.007). Non-responders had more persistent symptoms than responders (NYHA ≥3, 72% vs. 11% at follow-up). Subsequently, non-response was associated with a poor long-term prognosis in terms of death, heart failure (HF) hospitalization, and re-intervention after 2 years (freedom of death, HF hospitalization, and reintervention at 2 years: 16% vs. 78%, log-rank: p < 0.001).
Conclusion: Hemodynamic assessment before TTVR and procedural success are significant factors for patient prognosis. The hemodynamic profiling prior to intervention is an essential component in patient selection for TTVR. The window for edge-to-edge TTVR might be limited, but timely intervention is an important factor for a better outcome and successful right ventricular reverse remodeling.

Graphical Abstract. Influence of TR reduction and pulmonary hypertension on RV remodeling and outcome after transcatheter tricuspid edge-to-edge repair. TR, tricuspid regurgitation; PH, pulmonary hypertension; RV, right ventricle; TAPSE, tricuspid annulus plane systolic excursion; FAC, fractional area change; TTVR, transcatheter tricuspid valve repair; HF, heart failure.
Tricuspid regurgitation (TR) is a common condition in the general population. Around 2% are affected by at least moderate TR, compared to 23% in patients with heart failure (HF) (1, 2). Severe TR is associated with increased hospitalization rates due to right heart failure and death (3–6). TR is mostly secondary and can develop in combination with left-sided valvular heart disease and as an isolated valvular lesion (7). Besides medical therapy, surgery has long been the only treatment, but isolated tricuspid valve surgery is associated with increased perioperative mortality (8, 9). Several devices for transcatheter tricuspid valve repair (TTVR) have been recently introduced to clinical practice, but transcatheter edge-to-edge repair is currently the most commonly used method (10). Several prospective observational studies have shown that TTVR can improve symptoms, right ventricular function, and outcome but might be unfavorable in patients with pulmonary hypertension (PH) (11–13). Based on these results, the European Society of Cardiology (ESC) implemented a 2b recommendation for TTVR in the 2021 guidelines for the management of patients with valvular heart disease (14). However, the ACC/AHA guidelines published in 2020 did not include a recommendation for TTVR due to missing evidence (15). Therefore, further studies and randomized controlled trials (RCT) are needed to firmly establish TTVR in the treatment of TR. The study focuses on i) the outcome of TTVR patients separated into different PH groups, ii) the effects of TR reduction and PH on outcome and RV remodeling after TTVR, iii) the (pre)procedural conditions for improved outcome and RV remodeling after TTVR.
We included all patients treated with edge-to-edge TTVR between September 2018 and December 2021 at the Medical University of Vienna. Patients were separately analyzed according to their PH group and were enrolled and classified as either responders or non-responders according to an algorithm illustrated in Figure 1. All patients undergoing TTVR with a TR reduction of ≥1 grade without precapillary or combined PH (mean pulmonary artery pressure (mPAP) ≥25 mmHg, mean pulmonary artery Wedge pressure ≤ 15 mmHg, pulmonary vascular resistance ≥3 Wood units) were assigned to the responder group. All patients with a TR reduction of ≥1 grade and precapillary or combined PH were classified as non-responders. Patients with a TR reduction ≥2 grade were directly classified as responders, and patients without TR reduction were directly assigned as non-responders. Baseline characteristics were recorded before the procedure. The multidisciplinary Heart Team of our center individually discussed and assigned all patients to TTVR based on current guidelines and recommendations. The study protocol was approved by the Ethics Committee of the Medical University of Vienna, and all patients consented to participate.
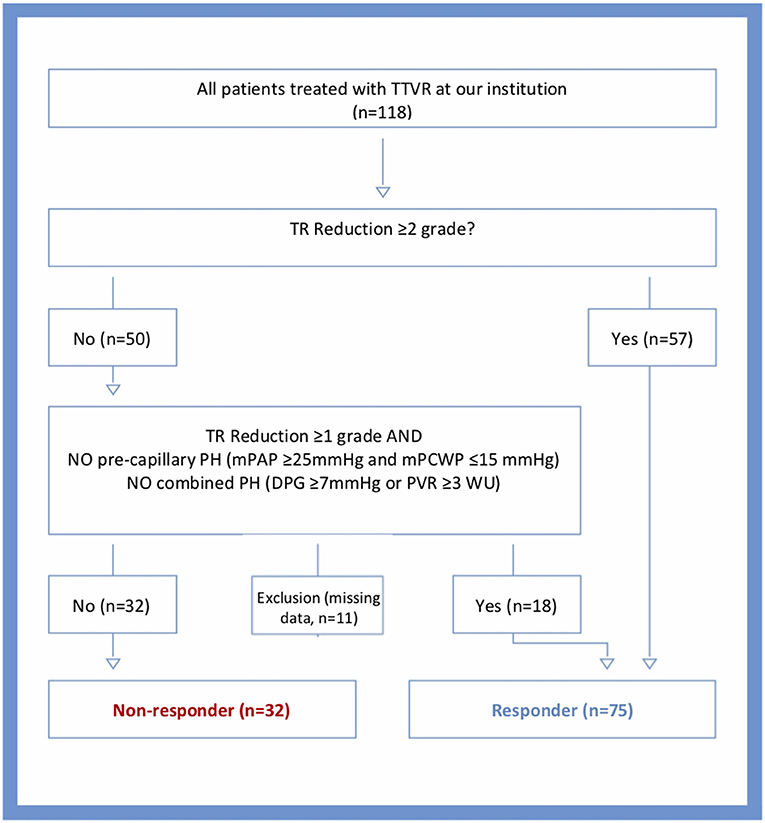
Figure 1. Algorithm for the allocation of patients to responders or non-responders. TTVR, transcatheter tricuspid valve repair; TR, tricuspid regurgitation; PH, pulmonary hypertension; mPCWP, mean pulmonary capillary Wedge pressure; DPG, diastolic pulmonary gradient; PVR, pulmonary vascular resistance; WU, Wood units.
A comprehensive echocardiographic assessment, including transesophageal echocardiography (TEE), was performed according to the American Society of Echocardiography guidelines (16, 17). Physicians and sonographers examined all patients using commercially available equipment (Vivid 7, E9, E95, GE Healthcare; and EPIQ 7, Philips Medical Systems), and board-certified physicians interpreted echocardiograms. Cardiac chamber sizes were evaluated according to the American Society of Echocardiography guideline recommendation (16). A comprehensive assessment of the tricuspid valve and TR was performed with an integrated, multiparametric approach, including the tricuspid valve morphology, vena contracta (VC), effective regurgitation orifice area (EROA), and regurgitant volume (RegVol) using the proximal isovelocity surface area (PISA) method (18). We applied a grading scale ranging from 1 to 5 to define TR severity: grade 1 indicates “mild”, 2 “moderate”, 3 “severe”, 4 “massive”, and 5 “torrential,” as recently proposed (19). Right ventricular systolic function was assessed using tricuspid annular plane systolic excursion (TAPSE), tissue Doppler velocity of the lateral tricuspid annulus (RV s'), fractional area change (FAC), and RV freewall strain and strainrate (20, 21). Systolic pulmonary artery pressure (sPAPecho) was calculated by adding the peak tricuspid regurgitation systolic gradient to the estimated central venous pressure (16). All analyses were performed using GE EchoPac software version 203 (GE Vingmed, Horten, Norway).
Invasive hemodynamic assessment was performed routinely in study participants before TTVR. Hemodynamic measurements were performed using a 7F Swan-Ganz catheter (Edwards Lifesciences GmbH, Austria) via femoral access. Pressures were documented as the average of eight measurements over eight consecutive heart cycles using CathCorLX (Siemens AG, Berlin and Munich, Germany). In addition to pulmonary artery Wedge pressure (PAWP), the systolic (sPAP), diastolic (dPAP), and mean (mPAP) PA pressures were documented. Cardiac output (CO) was measured by Fick's method or thermodilution. If both were available, Fick's method was preferred. Furthermore, the transpulmonary gradient (TPG) and diastolic pulmonary vascular pressure gradient (DPG) were calculated according to current guidelines (22). TPG was computed by subtracting PAWP from mPAP; DPG was calculated as the difference between dPAP and PAWP during a pull-back; pulmonary vascular resistance (PVR) was calculated by dividing TPG by CO. Precapillary PH was defined as mPAP ≥25mmHg and mPCWP ≤ 15 mmHg and combined pre-/postcapillary PH was defined as DPG ≥7mmHg or PVR ≥3 WU (Figure 1) (22). Moreover, coronary angiography was performed in all patients to detect possible coronary artery disease.
TTVR was performed using the Tri-/MitraClip (Abbott Laboratories, North Chicago, Illinois, size XT and XTW) or PASCAL system (Edwards Lifesciences, Irvine, California, size Ace). Both systems were inserted via a steerable guide with a delivery catheter through a right femoral vein access site. Precise valve anatomy and pathophysiology were assessed by transesophageal and transgastric echocardiographic windows using TEE according to recently published literature (23). The devices were positioned in the right atrium in front of the tricuspid valve. Steering of the guide and delivery catheter, rotation of the device arms, loading and grasping of the leaflets, device closure, and release were performed under fluoroscopic and echocardiographic guidance, as recently described (24).
The treating physician determined treatment strategy, device selection, and the number of implants based on the anatomic and clinical conditions of the individual patient.
Patients were followed up prospectively in a specialized outpatient clinic after TTVR at 3 months, 6 months, and annually. We defined the primary endpoint as all-cause mortality during a follow-up period of 2 years. In addition, we defined heart failure (HF) hospitalization as a secondary study endpoint and a composite endpoint, including death, HF hospitalization, and reintervention. Endpoints were collected via the Austrian death registry, telephone calls to patients or relatives, and electronic medical records. All patients gave written informed consent, and the study was approved by the Ethics Committee of the Medical University of Vienna.
Continuous baseline characteristics are presented for all patients and separately for the responder and non-responder groups as mean (SD) and compared with a 2-sided Student's t-test or Wilcoxon rank-sum test. Categorical variables were described as frequencies and compared with chi-square or Fisher's exact test. We compared follow-up data with baseline data for responders and non-responders, applying a paired Student's t-test or Wilcoxon rank-sum test. For different PH groups, we compared RV functional parameters at baseline and follow-up. Using described endpoints, Kaplan-Meier curves were plotted for all PH groups, responders, and non-responders. The log-rank test was applied to estimate the differences between survival curves. A two-sided p-value < 0.05 was considered statistically significant. Furthermore, univariate and multivariate logistic regression were performed using invasive hemodynamic data and patients with one or more and two or more grade TR reduction after TTVR. All analyses were performed using SPSS 27 (IBM SPSS, USA).
A total of 118 patients were treated with TTVR at our institution between September 2018 and December 2021. One hundred and seven patients were included in the study, 75 in the responder group and 32 in the non-responder group. Eleven patients were excluded due to 1 grade TR reduction without invasive hemodynamic measurements. 35 patients had no PH, 2 had precapillary, 32 had postcapillary, and 19 had combined PH. Baseline data are displayed for all patients in Table 1 and for responders and non-responders in Table 2. The mean age of responders was 76 years, and 67% were female. In the non-responder group, the mean age was 77 years, and 59% were female. Concomitant transcatheter mitral valve repair (TMVR) was performed in 35% of the responders and in 47% of the non-responders. A significant difference in baseline characteristics between groups was in the presence of previous percutaneous coronary intervention (PCI, responders: 16% vs. non-responders: 36%, p = 0.022) and TRI-SCORE risk evaluation (responders: 14% vs. non-responders: 27%, p = 0.003) (25).
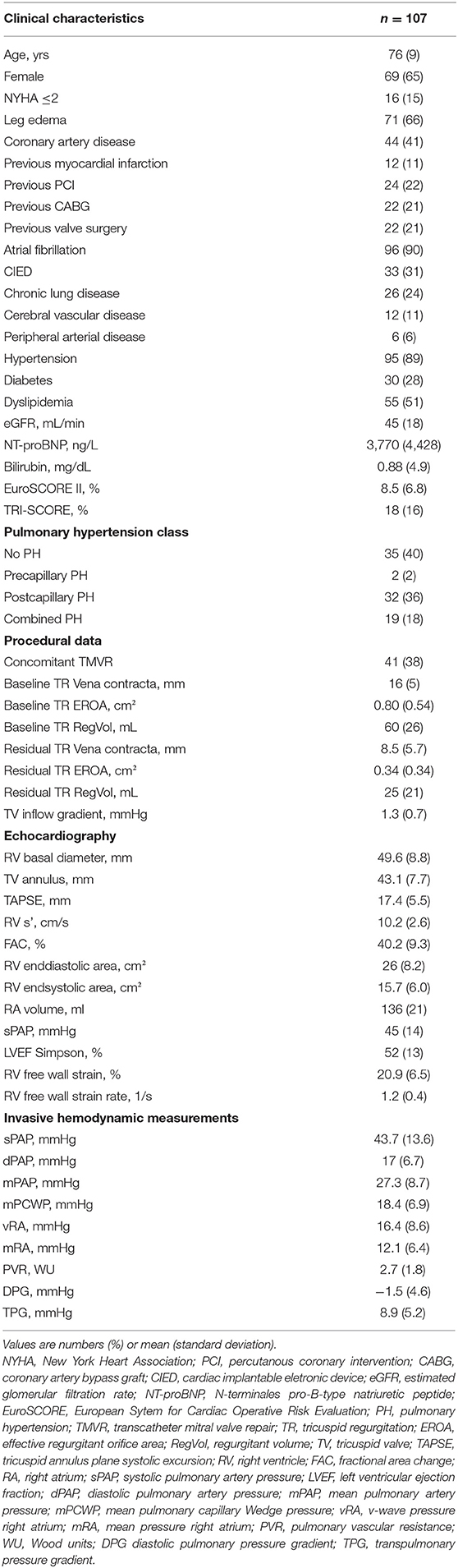
Table 1. Baseline Characteristics for all patients.
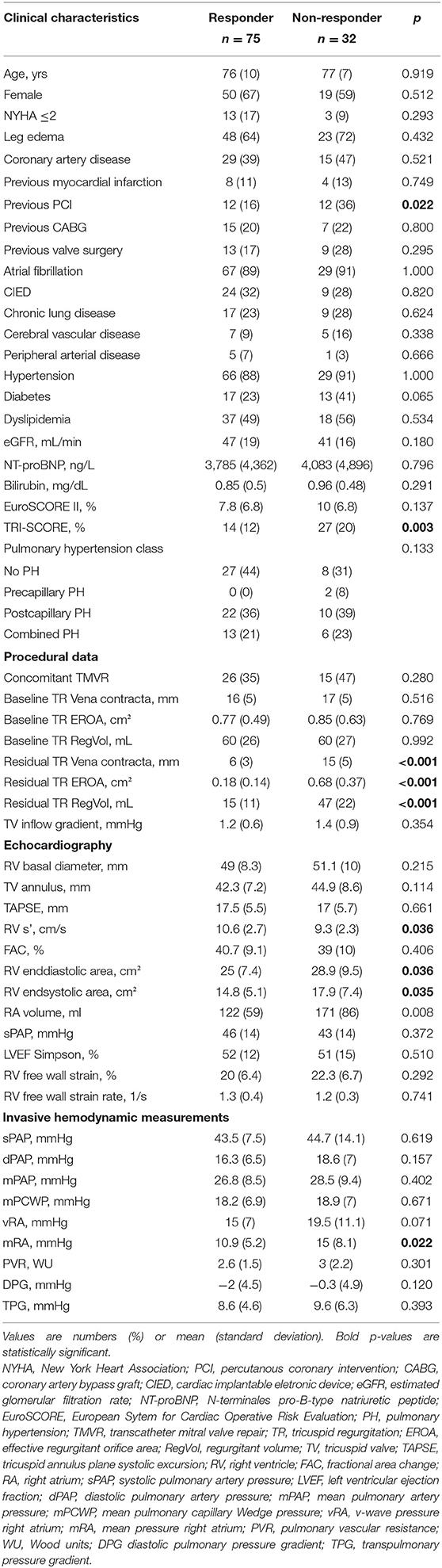
Table 2. Baseline characteristics by groups.
Logistic regression analysis showed a significant relationship between mean RA pressure and ≥1 grade TR reduction in uni- and multivariate analysis (univariate: odds ratio 0.894, conf-interval 0.821–0.974, p = 0.010; multivariate: odds ratio 0.848, conf-interval 0.734–0.979, p = 0.025) and between PVR and ≥1 grade reduction in multivariate analysis (odds ratio 1.008, conf-interval 1.000–1.015, p = 0.047). sPAP, mPAP, and mPCWP and ≥1 grade reduction showed no significant relationship. No value showed a significant association with two or more grade reduction in uni- or multivariate logistic regression.
Follow-up visits were performed at a mean of 229 days post TTVR for responders and 187 days post TTVR for non-responders. For patients undergoing reintervention, outcome data were obtained before reintervention. Leg edema and NYHA classification improved in the responder group significantly (64% to 17% for leg edema, p < 0.001 and 17% to 89% for NYHA ≤ 2, p < 0.001, Figures 2A,C) and did not change significantly in the non-responder group (72% to 78% for leg edema, p = 0.180 and 9% to 18% for NYHA ≤ 2, p = 0.157, Figures 2B,D). The following TR echocardiographic parameter were significantly reduced in the responder group: TR VC [16 (6) to 6 (3) mm, p < 0.001], TR EROA [0.75 (0.48) vs. 0.18 (0.14) cm2, p < 0.001] and TR RegVol [60 (27) vs. 15 (11) mL, p < 0.001] while in the non-responder group only TR RegVol decreased significantly [60 (28) vs. 48 (22) mL, p = 0.016] (Tables 3, 4).
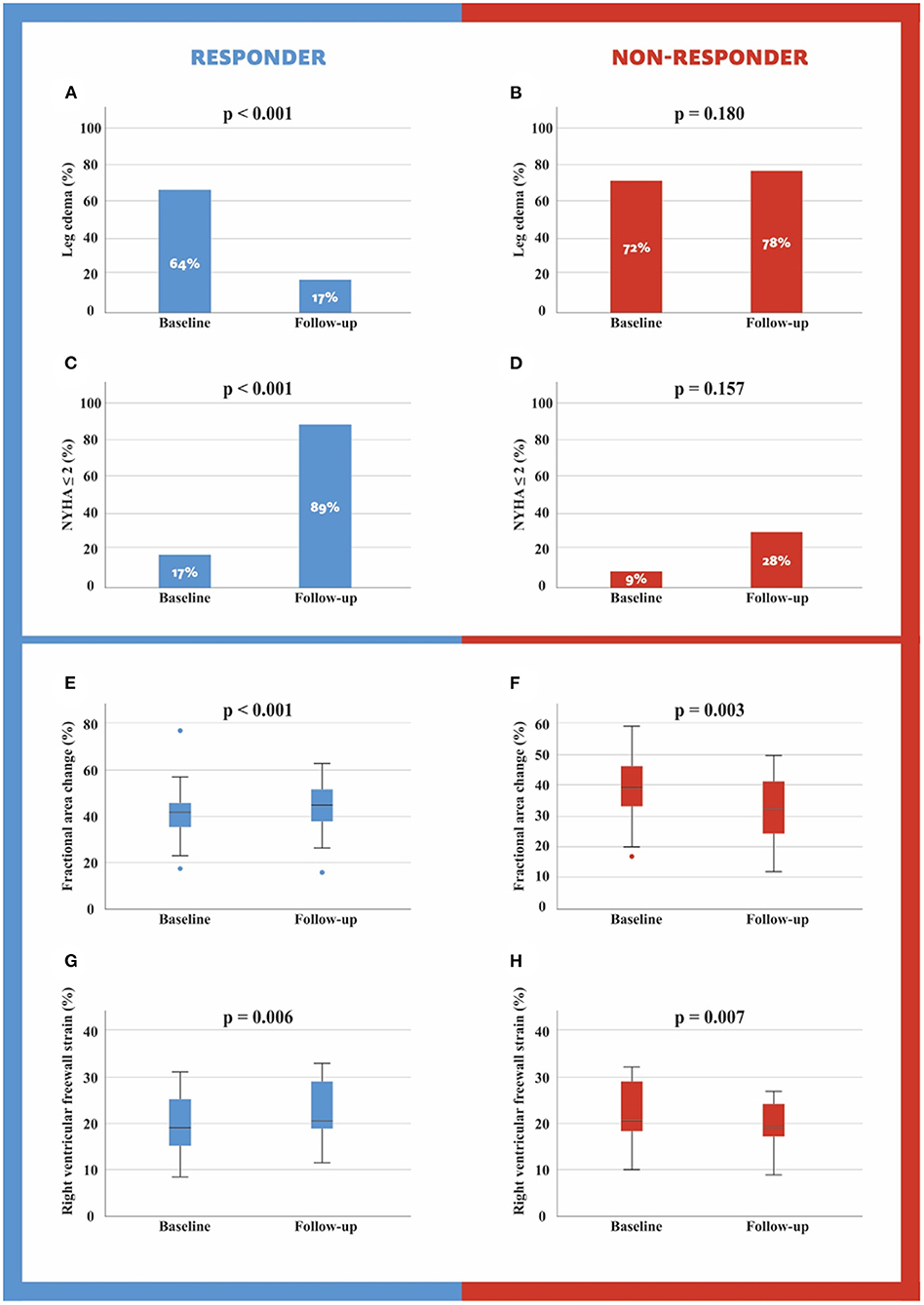
Figure 2. Leg edema and NYHA score at baseline and follow-up for responders and non-responders (A–C). Fractional area change and right ventricular freewall strain at baseline and follow-up for responders and non-responders (D–H).
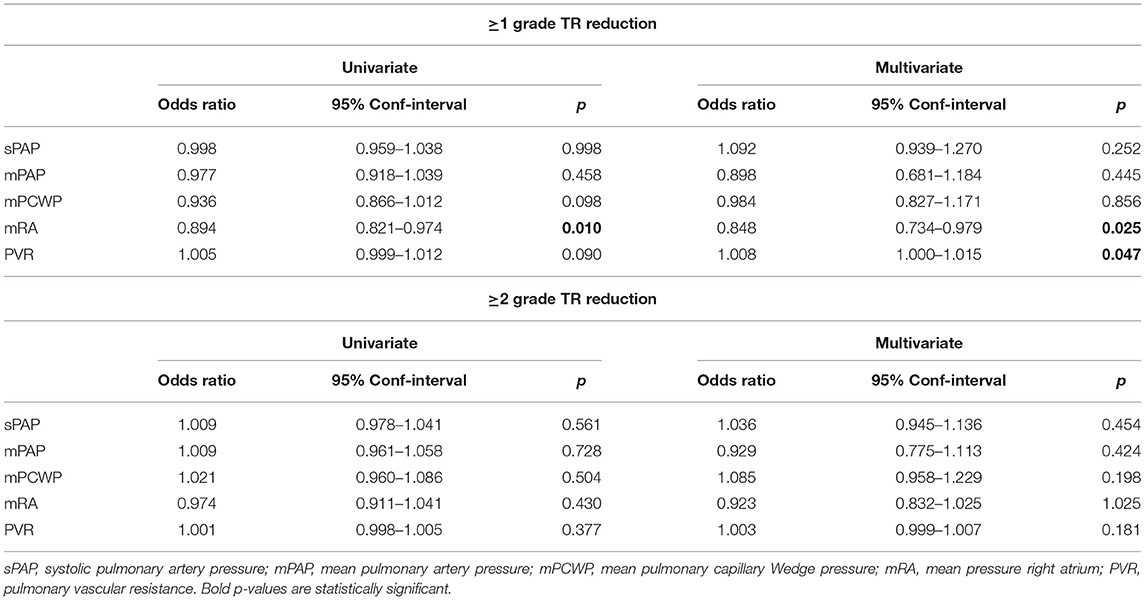
Table 3. Logistic regression analysis for ≥1 and ≥2 grade TR reduction after TTVR and invasive hemodynamic parameters.
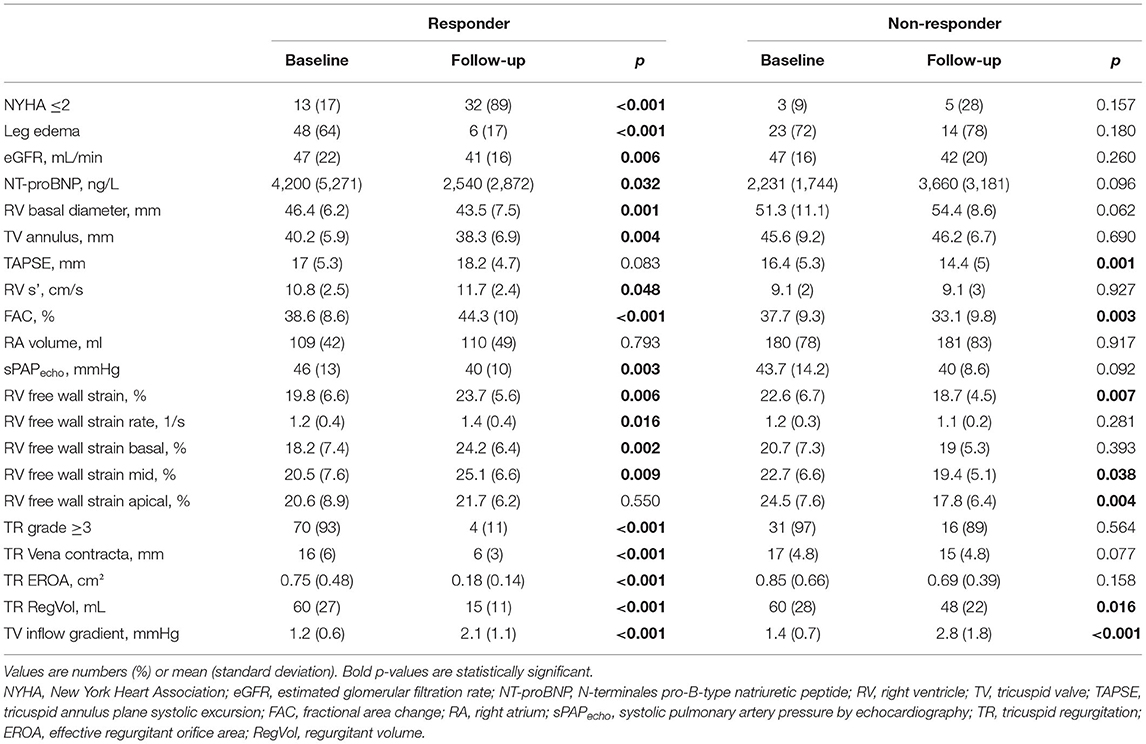
Table 4. Comparison of baseline and follow-up data divided by responder and non-responder.
In the group of responders, RV basal diameter [46.4 (6.2) vs. 43.5 (7.5) mm, p = 0.001] and tricuspid valve (TV) annulus [40.2 (5.9) vs. 38.3 (6.9) mm, p = 0.004] decreased, while RV s' [10.8 (2.5) vs. 11.7 (2.4) m/s, p = 0.048], FAC [38.6 (8.6) vs. 44.3 (10) %, p < 0.001, Figures 2E,F], RV free wall strain [19.8 (6.6) vs. 23.7 (5.6) %, p = 0.006, Figures 2G,H] and RV free wall strain rate [1.2 (0.4) vs. 1.4 (0.4) 1/s, p = 0.016] increased significantly. Furthermore, RV free wall strain basal [18.2 (7.4) vs. 24.2 (6.4) %, p = 0.002] and RV free wall strain mid [20.5 (7.6) vs. 25.1 (6.6) %, p = 0.009] improved (Table 4).
And in the group of non-responders, TAPSE [16.4 (5.3) vs. 14.4 (5) mm, p = 0.001], FAC [37.7 (9.3) vs. 33.1 (9.8) %, p = 0.003] and RV free wall strain [22.6 (6.7) vs. 18.7 (4.5) %, p = 0.007] decreased significantly. Moreover, RV free wall strain mid [22.7 (6.6) vs. 19.4 (5.1) %, p = 0.038] and RV free wall strain apical [24.5 (7.6) vs. 17.8 (6.4) %, p = 0.004] deteriorated (Table 4).
RV functional parameters did not change significantly at follow-up when patients were divided into the different PH groups (Table 5).
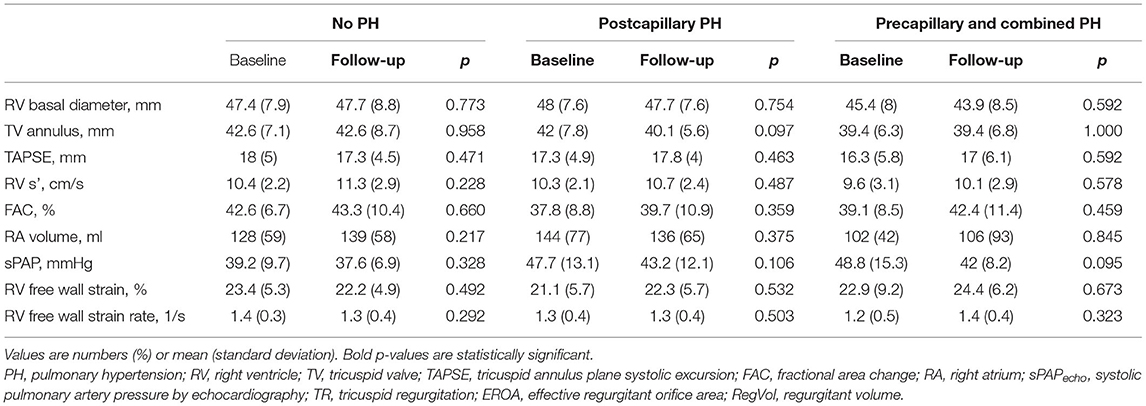
Table 5. Comparison of right ventricular parameters at baseline and follow-up for different PH groups.
A total of 39 events (18 deaths, 14 HF hospitalizations, 7 re-interventions) occurred during the observational period of 24 months [mean observational period 9 (8) months per patient]. In the responder group, 5 deaths, 5 HF hospitalizations, and no reintervention were recorded, whereas in the non-responder group, 13 patients died, 9 were hospitalized for HF, and 7 received reintervention. Rates for the combined endpoint of death, HF hospitalization, and re-intervention at 6 months, 1 year, and 2 years were for responders 11, 13, and 22%; and for non-responders, 51, 75, and 84% (log-rank: p < 0.001, Figure 3D). Similarly, a significant difference between responders and non-responders was found for the combined endpoint of death and HF hospitalization (22% vs. 66%, log-rank: p < 0.001, Figure 3C), for the isolated endpoint of death (12% vs. 47%, log-rank: p < 0.001, Figure 3A), and for the isolated endpoint of HF hospitalization (11% vs. 29%, log-rank: p = 0.021, Figure 3B). In addition, we analyzed outcome according to different PH groups. Rates for the combined endpoint of death and HF hospitalization at 6 months, 1 year, and 2 years for patients without PH were 0, 14, and 14%; for patients with postcapillary PH, 27, 37, and 37%; and for patients with precapillary or combined PH, 51, 51, and 100% (log-rank: p < 0.001, Figure 4A).
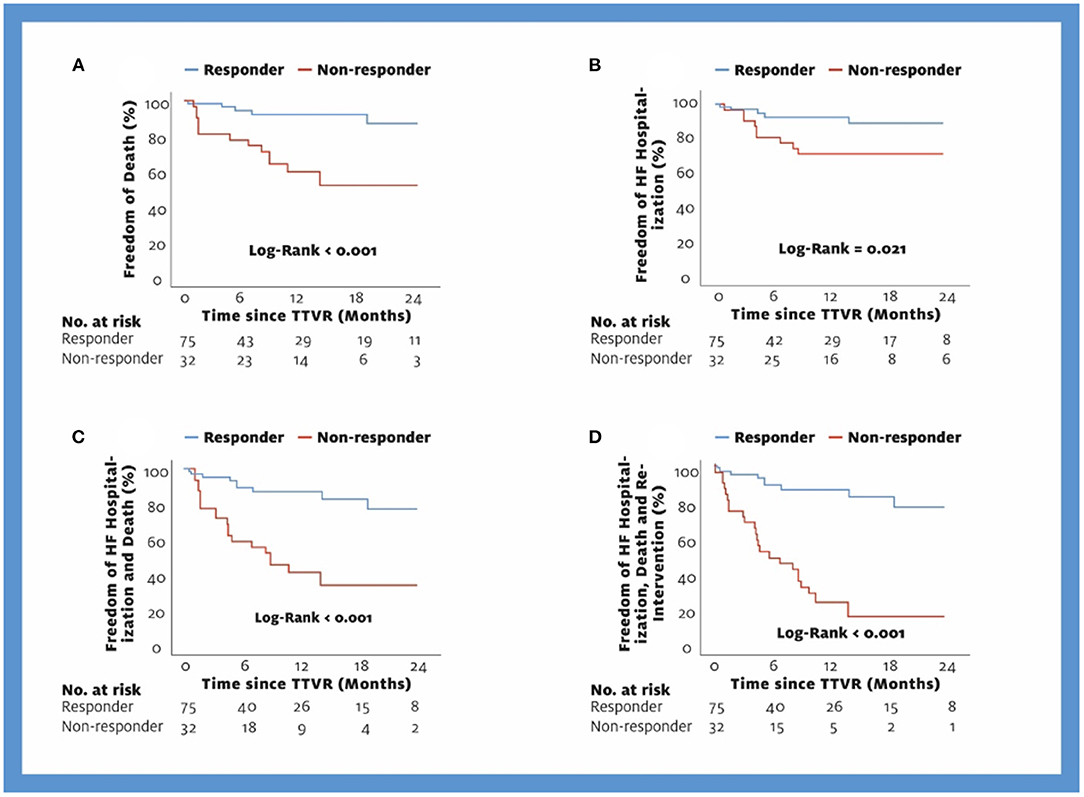
Figure 3. Kaplan-Meier Curves for the endpoints Death (A), HF hospitalization (B), Death and HF hospitalization (C), and Death, HF hospitalization, Re-intervention (D). TTVR, transcatheter tricuspid valve repair; HF, heart failure.
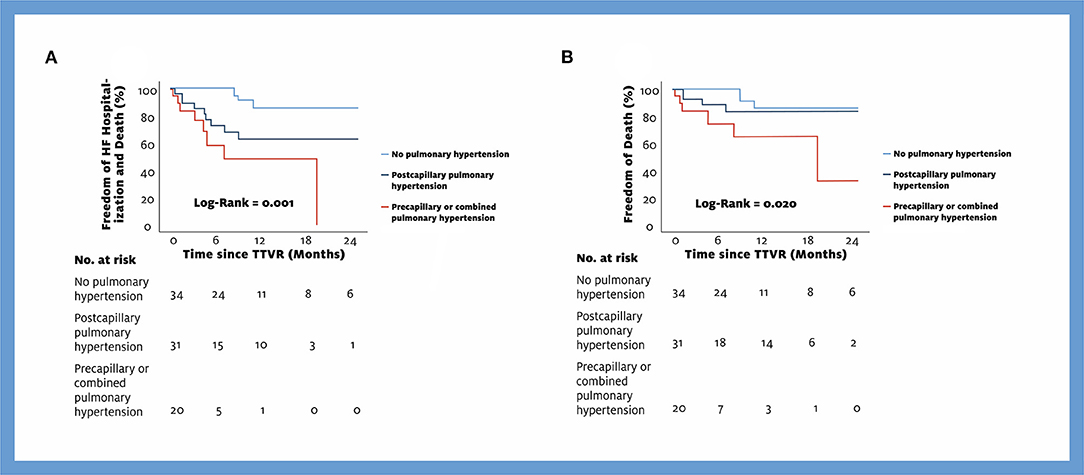
Figure 4. Kaplan-Meier Curves for the endpoints Death and HF hospitalization (A) and Death (B) by different PH groups. TTVR, transcatheter tricuspid valve repair; HF, heart failure.
This prospective observational study divided TTVR patients into responders and non-responders according to pre-interventional hemodynamic assessment and procedural success. We were able to demonstrate three main findings: 1) Significant RV remodeling after TTVR, 2) Subsequent improvement or worsening of RV function depending on preinterventional hemodynamic status and procedural success, 3) Significantly lower mortality in patients with favorable hemodynamics and successful intervention, and 4) differences in outcome between the PH groups but no difference in RV remodeling.
TR is a common disease with multiple causes that had long been treated only with guideline-directed medical therapy. The high prevalence of concomitant TR in various underlying diseases like left heart disease or PH makes patient selection a central issue for TTVR. Procedural success in TTVR is currently an ongoing matter of debate resulting in different definitions. Some authors advocate procedural success as a TR ≤ 2 after the procedure, whereas other authors define success based on the extent of reduction (12, 26). If procedural success is defined as TR ≤ 2 after TTVR, patients with massive or torrential TR have a lower procedural success rate and a higher HF hospitalization rate but a similar mortality rate compared with patients with severe TR (27). Our analysis demonstrated that reduction in TR was an important factor for a favorable outcome, regardless of baseline TR or residual TR after TTVR. We also analyzed invasive hemodynamic parameters and their predictive value for the success of the procedure (Table 3). Only right atrial mean pressure showed univariate and multivariate predictive value for TR reduction after TTVR. Elevated right atrial pressure could be a marker of advanced disease stage and should be considered in patient selection. Other values, such as mPAP or mPCWP, may not have prognostic significance because the number of patients in whom these values were strongly elevated was rather small. Furthermore, in our cohort, a substantial number of patients underwent concomitant TMVR (38%). TMVR is known to reduce pulmonary pressure and tricuspid regurgitation (28). In addition, patients with severe MR and TR who receive TMVR and TTVR might have a better outcome than patients who receive TMVR alone (29). Concomitant TMVR is a potential bias for our results, but responders and non-responders had no significant difference regarding the number of patients undergoing TMVR (responders: 35%, non-responders: 47%, p = 0.280).
Stocker et al. recently demonstrated that patients with precapillary PH who undergo TTVR have a worse outcome than patients without or with postcapillary PH (13). We also demonstrated that outcomes differed between PH groups and were worst in patients with combined or precapillary PH (Figure 4). Postcapillary PH due to left heart disease is a known factor for the occurrence of TR, but an additional precapillary PH component seems to worsen the outcome. Therefore, we included the PH group in our algorithm but also emphasized the success of the procedure. In our cohort, only two patients had precapillary PH and a TR reduction of one grade and were therefore assigned to the non-responder group. This can be explained by our screening for TTVR, which mostly excluded patients with precapillary PH due to early data of TTVR patients (30). The other 9 non-responders with a TR reduction of one TR grade met the criteria for combined PH according to guidelines (22). Still, pulmonary pressure and pulmonary resistance did not differ significantly between responders and non-responders (Table 6). This occurs because only patients with a decrease of one grade were placed in one of the groups according to PH, but still, the outcome in responders is much better. This suggests that, on the one hand, the benefit of a large TR reduction may overcome the poor prognosis of patients with PH. On the other hand, a TR reduction of one grade is not sufficient to compensate for the worse outcome of PH patients.
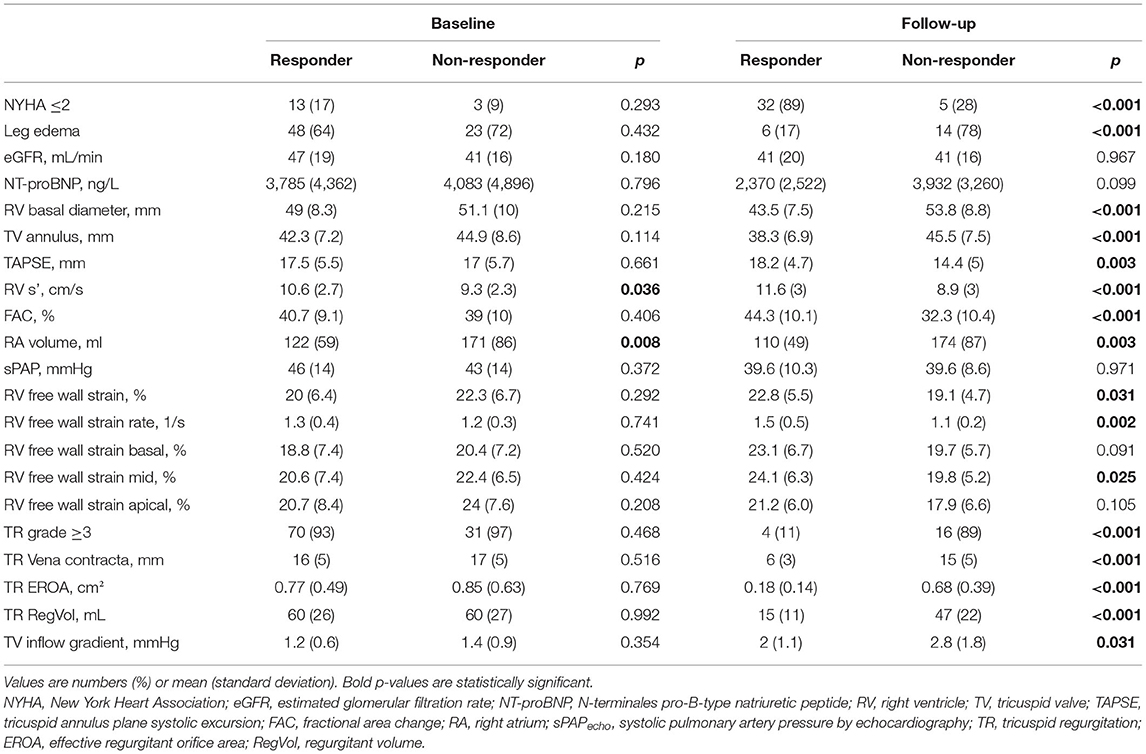
Table 6. Comparison of responder and non-responder data divided by baseline and follow-up examination.
Interestingly, despite the worse outcome of non-responders, both groups differ not much in terms of baseline characteristics. Non-responders had a significantly higher incidence of previous PCI, a larger RV, and RA. The EuroSCORE II was also higher in the non-responder group, but not significantly, whereas the recently introduced TRI-SCORE was able to show a significant difference (25). This is further suggestive that the EuroSCORE II may not be sufficiently prognostic for TR patients and may be inferior to the TRI-SCORE. Nevertheless, the small differences between responders and non-responders in baseline characteristics underline the impact of TR reduction and PH on the outcome.
At echocardiographic follow-up, we observed a significant improvement in RV function and a decrease in RV size in the responder group (Table 4), similar to previous studies (11, 31, 32). However, for the first time, we also analyzed the group of non-responders who showed a decline in RV functional parameters (Table 4). This information supports the value of successful TTVR for TR patients. Interestingly, in the responder group, RV freewall strain increased more in the basal segments than in the apical segments. In contrast, it was reversed in the non-responder group concerning strain decrease (Table 4). The reason for this could be the indirect annuloplasty that occurs during TTVR. In the responder group, this annuloplasty combined with reduced volume overload after substantial TR reduction leads to reverse RV remodeling, especially in the large basal portions. In the group of non-responders, annuloplasty also takes place and probably has a protective effect on the basal parts of the RV, keeping them from deteriorating. However, due to volume overload following an incompletely repaired TR or an increased PVR, apical RV function deteriorates.
In addition to RV remodeling, we also analyzed the outcome with the endpoints of HF hospitalization, death, and re-intervention, also in combined analyses. We demonstrated a clear advantage for the responders (freedom of all endpoints after 2 years: responders 78%, non-responders: 16%, Figure 3D). Taramasso et al. compared TTVR patients with medical-treated patients in a propensity-matched analysis and demonstrated a survival rate of 64% in control patients and 77% in TTVR patients at 1 year (10). In our cohort, 60% of non-responders and 92% of responders survived after 1 year. The comparable outcome of our non-responders and the control patients by Taramasso et al. show that TR reduction of 1 grade in precapillary or combined PH is similar to no intervention in terms of survival. The higher survival of our responders compared with the TTVR group of Taramasso et al. can be explained by the assignment of procedural failures with no TR reduction to the non-responder group. Procedural failures also showed a significantly worse outcome in a separate analysis in the study by Taramasso et al. (10).
We observed a significant clinical improvement in the responder group as measured by NYHA score, which demonstrated an increase in patients with NYHA ≤ II from 17 to 89% (Table 4, p < 0.001). In comparison, in the TRILUMINATE cohort, the number of NYHA ≤ II patients increased from 31 to 83% 1 year after TTVR (p < 0.0001) (11). Our responder patients seem to benefit even more compared to an entire TTVR cohort. However, in our non-responders, NYHA score did not change significantly (p = 0.157), consistent with the worse outcome of this group. We also observed no significant changes in the non-responder group in terms of leg edema (p = 0.180), while leg edema significantly improved in the responder group (p < 0.001). These clinical changes indicate that TTVR can help patients suffering from symptoms of right heart decompensation if PH is not precapillary or combined and at least 1 grade TR reduction is achieved. Finally, we can conclude that our study provides important insights into patient selection and TR reduction required for a good outcome. In addition, we were able to provide more detailed information on RV (reverse) remodeling after TTVR. Upcoming RCTs, such as the TRILUMINATE pivotal trial (unique identifier: NCT03904147), are eagerly awaited to clarify the impact of TTVR on TR patients.
There are several limitations to be considered in this study. We could not include all patients with TTVR from our center because invasive hemodynamic measurements were not available in all patients, mainly if TMVR was performed simultaneously. The changes in RV function and differences in outcome may also be attributable to concomitant TMVR, even though both groups had a similar repair rate (Table 1). Our procedural results are from a highly specialized center, nevertheless, patients from the beginning of TTVR were included. Therefore, the success rate of patients treated today might be higher. No echocardiography core laboratory was involved in image evaluation.
TTVR patients divided into responders and non-responders by preinterventional hemodynamic assessment and procedural success show a marked difference in RV (reverse) remodeling and outcome. While RV function improves in responders, it deteriorates in non-responders. The endpoints of death, HF hospitalization, and reintervention were much more frequently reached by non-responders. Preprocedural hemodynamic assessment may help in patient selection. These encouraging results strengthen the usefulness of TTVR in routine clinical practice.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by Ethik Kommision der Medizinischen Universität Wien. The patients/participants provided their written informed consent to participate in this study.
VD and GG: conception and design and analysis and interpretation of data. VD, GG, JM, and MS: drafting of the manuscript. GG, JM, MK, CD, KM, GH, KH, AB, MM, and GS: critical revision of the manuscript for important intellectual content. M-PW, PB, CH, GG, MA, AK, and CN: final approval of the submitted manuscript. All authors contributed to the article and approved the submitted version.
VD received consulting fees from Abbott, and educational grants from Edwards Lifesciences. JM received proctor fees from Abbott, consulting fees from Edwards Lifesciences, Boston Scientific, Shockwave Medical, and educational grants from Edwards Lifesciences. CH received proctor fees from Edwards Lifesciences and Boston Scientific, Educational grants from Abbott, Edwards Lifesciences, Boston Scientific, and Medtronic. MA received proctor/speaker/consulting fees from Abbott, Edwards, and Medtronic and institutional research funding (Edwards, Abbott, Medtronic, LSI).
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Many thanks to Sophie Lindenthal for her assistance with the graphic design and the IT4Science team of the Medical University of Vienna for data provision.
1. Enriquez-Sarano M, Messika-Zeitoun D, Topilsky Y, Tribouilloy C, Benfari G, Michelena H. Tricuspid regurgitation is a public health crisis. Prog Cardiovasc Dis. (2019) 62:447–51. doi: 10.1016/j.pcad.2019.10.009
2. Benfari G, Antoine C, Miller WL, Thapa P, Topilsky Y, Rossi A, et al. Excess mortality associated with functional tricuspid regurgitation complicating heart failure with reduced ejection fraction. Circulation. (2019) 140:196–206. doi: 10.1161/CIRCULATIONAHA.118.038946
3. Bohbot Y, Chadha G, Delabre J, Landemaine T, Beyls C, Tribouilloy C. Characteristics and prognosis of patients with significant tricuspid regurgitation. Arch Cardiovasc Dis. (2019). doi: 10.1016/j.acvd.2019.06.011
4. Chorin E, Rozenbaum Z, Topilsky Y, Konigstein M, Ziv-Baran T, Richert E, et al. Tricuspid regurgitation and long-term clinical outcomes. Eur Heart J Cardiovasc Imaging. (2019). doi: 10.1093/ehjci/jez216
5. Topilsky Y, Nkomo VT, Vatury O, Michelena HI, Letourneau T, Suri RM, et al. Clinical outcome of isolated tricuspid regurgitation. JACC Cardiovasc Imaging. (2014) 7:1185–94. doi: 10.1016/j.jcmg.2014.07.018
6. Topilsky Y, Maltais S, Medina Inojosa J, Oguz D, Michelena H, Maalouf J, et al. Burden of Tricuspid Regurgitation in Patients Diagnosed in the Community Setting. JACC Cardiovasc Imaging. (2019) 12:433–42. doi: 10.1016/j.jcmg.2018.06.014
7. Mascherbauer J, Kammerlander AA, Zotter-Tufaro C, Aschauer S, Duca F, Dalos D, et al. Presence of isolated tricuspid regurgitation should prompt the suspicion of heart failure with preserved ejection fraction. PLoS One. (2017) 12:e0171542. doi: 10.1371/journal.pone.0171542
8. Zack CJ, Fender EA, Chandrashekar P, Reddy YNV, Bennett CE, Stulak JM, et al. National trends and outcomes in isolated tricuspid valve surgery. J Am Coll Cardiol. (2017) 70:2953–60. doi: 10.1016/j.jacc.2017.10.039
9. Wong WK, Chen SW, Chou AH, Lee HA, Cheng YT, Tsai FC, et al. Late outcomes of valve repair versus replacement in isolated and concomitant tricuspid valve surgery: a nationwide cohort study. J Am Heart Assoc. (2020) 9:e015637. doi: 10.1161/JAHA.119.015637
10. Taramasso M, Benfari G, van der Bijl P, Alessandrini H, Attinger-Toller A, Biasco L, et al. Transcatheter versus medical treatment of patients with symptomatic severe tricuspid regurgitation. J Am Coll Cardiol. (2019) 74:2998–3008. doi: 10.1016/j.jacc.2019.09.028
11. Lurz P, Stephan von Bardeleben R, Weber M, Sitges M, Sorajja P, Hausleiter J, et al. Transcatheter edge-to-edge repair for treatment of tricuspid regurgitation. J Am Coll Cardiol. (2021) 77:229–39. doi: 10.1016/j.jacc.2020.11.038
12. Taramasso M, Alessandrini H, Latib A, Asami M, Attinger-Toller A, Biasco L, et al. Outcomes after current transcatheter tricuspid valve intervention: mid-term results from the international trivalve registry. JACC Cardiovasc Interv. (2019) 12:155–65. doi: 10.1016/j.jcin.2018.10.022
13. Stocker TJ, Hertell H, Orban M, Braun D, Rommel KP, Ruf T, et al. Cardiopulmonary hemodynamic profile predicts mortality after transcatheter tricuspid valve repair in chronic heart failure. JACC Cardiovasc Interv. (2021) 14:29–38. doi: 10.1016/j.jcin.2020.09.033
14. Vahanian A, Beyersdorf F, Praz F, Milojevic M, Baldus S, Bauersachs J, et al. 2021 ESC/EACTS Guidelines for the management of valvular heart disease. Eur Heart J. (2022) 43:561–632. doi: 10.1093/ejcts/ezac209
15. Otto CM, Nishimura RA, Bonow RO, Carabello BA, Erwin JP 3rd, Gentile F, et al. 2020 ACC/AHA Guideline for the management of patients with valvular heart disease: executive summary: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. (2020) 2020:Cir0000000000000932. doi: 10.1161/CIR.0000000000000932
16. Lang RM, Badano LP, Mor-Avi V, Afilalo J, Armstrong A, Ernande L, et al. Recommendations for cardiac chamber quantification by echocardiography in adults: an update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. Eur Heart J Cardiovasc Imaging. (2015) 16:233–70. doi: 10.1093/ehjci/jev014
17. Hahn RT, Abraham T, Adams MS, Bruce CJ, Glas KE, Lang RM, et al. Guidelines for performing a comprehensive transesophageal echocardiographic examination: recommendations from the American Society of Echocardiography and the Society of Cardiovascular Anesthesiologists. J Am Soc Echocardiogr. (2013) 26:921–64. doi: 10.1016/j.echo.2013.07.009
18. Zoghbi WA, Adams D, Bonow RO, Enriquez-Sarano M, Foster E, Grayburn PA, et al. Recommendations for noninvasive evaluation of native valvular regurgitation: a report from the American Society of Echocardiography Developed in Collaboration with the Society for Cardiovascular Magnetic Resonance. J Am Soc Echocardiogr. (2017) 30:303–71. doi: 10.1016/j.echo.2017.01.007
19. Hahn RT, Zamorano JL. The need for a new tricuspid regurgitation grading scheme. Eur Heart J Cardiovasc Imaging. (2017) 18:1342–3. doi: 10.1093/ehjci/jex139
20. Rudski LG, Lai WW, Afilalo J, Hua L, Handschumacher MD, Chandrasekaran K, et al. Guidelines for the echocardiographic assessment of the right heart in adults: a report from the American Society of Echocardiography endorsed by the European Association of Echocardiography, a registered branch of the European Society of Cardiology, and the Canadian Society of Echocardiography. J Am Soc Echocardiogr. (2010) 23:685–713. doi: 10.1016/j.echo.2010.05.010
21. Voigt JU, Pedrizzetti G, Lysyansky P, Marwick TH, Houle H, Baumann R, et al. Definitions for a common standard for 2D speckle tracking echocardiography: consensus document of the EACVI/ASE/Industry Task Force to standardize deformation imaging. J Am Soc Echocardiogr. (2015) 28:183–93. doi: 10.1016/j.echo.2014.11.003
22. Galie N, Humbert M, Vachiery JL, Gibbs S, Lang I, Torbicki A, et al. 2015 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension: the Joint Task Force for the Diagnosis and Treatment of Pulmonary Hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS): Endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC), International Society for Heart and Lung Transplantation (ISHLT). Eur Heart J. (2016) 37:67–119. doi: 10.1093/eurheartj/ehv317
23. Hahn RT, Weckbach LT, Noack T, Hamid N, Kitamura M, Bae R, et al. Proposal for a standard echocardiographic tricuspid valve nomenclature. JACC Cardiovasc Imaging. (2021) 14:1299–305. doi: 10.1016/j.jcmg.2021.01.012
24. Dannenberg V, Schneider M, Bartko P, Koschutnik M, Donà C, Nitsche C, et al. Diagnostic assessment and procedural imaging for transcatheter edge-to-edge tricuspid valve repair: a step-by-step guide. Eur Heart J Cardiovasc Imaging. (2021) 22:8–10. doi: 10.1093/ehjci/jeaa269
25. Dreyfus J, Audureau E, Bohbot Y, Coisne A, Lavie-Badie Y, Bouchery M, et al. TRI-SCORE: a new risk score for in-hospital mortality prediction after isolated tricuspid valve surgery. Eur Heart J. (2021). doi: 10.1093/eurheartj/ehab679
26. Besler C, Orban M, Rommel KP, Braun D, Patel M, Hagl C, et al. Predictors of procedural and clinical outcomes in patients with symptomatic tricuspid regurgitation undergoing transcatheter edge-to-edge repair. JACC Cardiovasc Interv. (2018) 11:1119–28. doi: 10.1016/j.jcin.2018.05.002
27. Miura M, Alessandrini H, Alkhodair A, Attinger-Toller A, Biasco L, Lurz P, et al. Impact of massive or torrential tricuspid regurgitation in patients undergoing transcatheter tricuspid valve intervention. JACC Cardiovasc Interv. (2020) 13:1999–2009. doi: 10.1016/j.jcin.2020.05.011
28. Bannehr M, Kahn U, Okamoto M, Kaneko H, Hähnel V, Neuß M, et al. Post-procedural tricuspid regurgitation predicts long-term survival in patients undergoing percutaneous mitral valve repair. J Cardiol. (2019) 74:524–31. doi: 10.1016/j.jjcc.2019.05.009
29. Mehr M, Karam N, Taramasso M, Ouarrak T, Schneider S, Lurz P, et al. Combined tricuspid and mitral versus isolated mitral valve repair for severe mitral and tricuspid regurgitation: an analysis from the trivalve and TRAMI registries. JACC Cardiovasc Interv. (2020) 13:543–50. doi: 10.1093/eurheartj/ehz748.0052
30. Hausleiter J, Braun D, Orban M, Latib A, Lurz P, Boekstegers P, et al. Patient selection, echocardiographic screening and treatment strategies for interventional tricuspid repair using the edge-to-edge repair technique. EuroIntervention. (2018) 14:645–53. doi: 10.4244/EIJ-D-17-01136
31. Rommel KP, Besler C, Noack T, Blazek S, von Roeder M, Fengler K, et al. Physiological and clinical consequences of right ventricular volume overload reduction after transcatheter treatment for tricuspid regurgitation. JACC Cardiovasc Interv. (2019) 12:1423–34. doi: 10.1016/j.jcin.2019.02.042
32. Orban M, Braun D, Deseive S, Stolz L, Stocker TJ, Stark K, et al. Transcatheter edge-to-edge repair for tricuspid regurgitation is associated with right ventricular reverse remodeling in patients with right-sided heart failure. JACC Cardiovasc Imaging. (2019) 12:559–60. doi: 10.1016/j.jcmg.2018.10.029
Keywords: transcatheter repair, pulmonary hypertension, right ventricular remodeling, patient selection, tricuspid regurgitation
Citation: Dannenberg V, Koschutnik M, Donà C, Nitsche C, Mascherbauer K, Heitzinger G, Halavina K, Kammerlander AA, Spinka G, Winter M-P, Andreas M, Mach M, Schneider M, Bartunek A, Bartko PE, Hengstenberg C, Mascherbauer J and Goliasch G (2022) Invasive Hemodynamic Assessment and Procedural Success of Transcatheter Tricuspid Valve Repair—Important Factors for Right Ventricular Remodeling and Outcome. Front. Cardiovasc. Med. 9:891468. doi: 10.3389/fcvm.2022.891468
Received: 07 March 2022; Accepted: 28 April 2022;
Published: 02 June 2022.
Edited by:
Christoph Edlinger, University Hospital Salzburg, AustriaReviewed by:
Marwin Bannehr, Heart Center Brandenburg, GermanyCopyright © 2022 Dannenberg, Koschutnik, Donà, Nitsche, Mascherbauer, Heitzinger, Halavina, Kammerlander, Spinka, Winter, Andreas, Mach, Schneider, Bartunek, Bartko, Hengstenberg, Mascherbauer and Goliasch. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Georg Goliasch, georg.goliasch@meduniwien.ac.at
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.