
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Cardiovasc. Med. , 09 August 2022
Sec. Cardiovascular Surgery
Volume 9 - 2022 | https://doi.org/10.3389/fcvm.2022.884144
 Lingyu Lin1,2Xuecui Zhang1Shurong Xu1†
Lingyu Lin1,2Xuecui Zhang1Shurong Xu1† Yanchun Peng2†Sailan Li2Xizhen Huang2
Yanchun Peng2†Sailan Li2Xizhen Huang2 Liangwan Chen2*
Liangwan Chen2* Yanjuan Lin2,3*
Yanjuan Lin2,3*Background: Postoperative delirium (POD) is an acute brain dysfunction that is frequently observed in patients undergoing cardiac surgery. Increasing evidence indicates POD is related to higher mortality among cardiac surgical patients, but the results remain controversial. Moreover, a quantitative evaluation of the influence of POD on hospital days, intensive care unit (ICU) time, and mechanical ventilation (MV) time has not been performed.
Objective: This study aimed to evaluate the correlation between POD and outcomes in patients undergoing cardiac surgery by a systematic review and meta-analysis.
Materials and methods: A total of 7 electronic databases (Cochrane Library, PubMed, EMBASE, CINAHL Complete, MEDLINE, Wan-fang database, and China National Knowledge Infrastructure) were searched from January 1980 to July 20, 2021, with language restrictions to English and Chinese, to estimate the impact of the POD on outcome in patients who underwent cardiac surgery. The meta-analysis was registered with PROSPERO (Registration: CRD42021228767).
Results: Forty-two eligible studies with 19785 patients were identified. 3368 (17.0%) patients were in the delirium group and 16417 (83%) were in the non-delirium group. The meta-analysis showed that compared to patients without POD, patients with POD had 2.77-fold higher mortality (OR = 2.77, 95% CI 1.86–4.11, P < 0.001), 5.70-fold higher MV (>24h) rate (OR = 5.70, 95% CI 2.93–11.09, P < 0.001); and longer MV time (SMD = 0.83, 95% CI 0.57–1.09, P < 0.001), ICU time (SMD = 0.91, 95% CI 0.60–1.22, P < 0.001), hospital days (SMD = 0.62, 95% CI 0.48–0.76, P < 0.001).
Conclusion: The synthesized evidence suggests that POD is causally related to the increased risk of mortality, prolonged length of ICU and hospital stay, and a longer duration of MV time. Future research should focus on the interventions for POD, to reduce the incidence.
Systematic review registration: [www.crd.york.ac.uk/PROSPERO], identifier [CRD42021228767].
Cardiovascular disease has become one of the greatest threats to human health in the 21st century (1). The number of patients suffering from cardiovascular disease has increased dramatically over recent years worldwide (1, 2), and the amounts of cardiovascular operations have also increased rapidly. According to the latest report, 1.5 million cardiac surgeries are performed globally every year approximately (3), and the incidence of complications varies from 2 to 60% following cardiac surgery (4). POD is the most common complication among cardiac surgical patients with an incidence of 25–52% (5). It is defined as an acute disturbance of consciousness characterized by acute and fluctuating changes in attention, awareness, and cognition (6), with a poor prognosis. An analysis published in Lancet reported that delirium costs more than $164 billion in health care expenses in the United States each year (7), bringing a heavy economic burden to society. Thereby, the prognosis of POD is receiving greater public attention (8).
In recent years, a large body of evidence indicates that POD in patients undergoing cardiac surgery is significantly associated with poor prognosis. However, the results remain controversial. Compared with patients without POD, cardiac surgical patients who develop POD have higher mortality (9, 10). While others suggest that POD is not significantly related to mortality (11, 12). According to our literature search, only one review evaluated the association between POD and mortality in patients undergoing TAVR which was published in 2020 (13), seven studies are included and the sample size is relatively small. Individual studies have insufficient power to detect the association and to persuade convey conflicting results. Furthermore, a quantitative evaluation of the influence of POD on hospital days, ICU time, and MV time has not been performed.
It should be noted that we do not draw enough attention to delirium since the insufficient recognition and under-reporting (14, 15). Knowledge of the true magnitude of POD and its associated burdens in cardiac surgical patients would allow healthcare professionals to allocate much-needed resources toward reducing morbidity and mortality associated with delirium after cardiac surgery. Therefore, we conducted a systematic review and meta-analysis to explore the relationship between POD and outcomes in these patients, including short-term and after-discharge mortality, hospitalization, ICU stays, and MV time, to provide scientific data for POD management after cardiac surgery.
This systematic review and meta-analysis followed the PRISMA (16) (see Supplementary Table 1). The protocol has been registered in PROSPERO (Registration: CRD42021228767).
We conducted a comprehensive computerized search of the medical literature using 5 major English databases, including Cochrane Library (search date: August 15, 2021), PubMed (search date: August 25, 2021), EMBASE (search date: August 30, 2021), CINAHL Complete (search date: September 5, 2021), and MEDLINE (search date: September 15, 2021). We also searched two major Chinese databases, Wan-fang database (search date: September 20, 2021), and China National Knowledge Infrastructure (search date: September 20, 2021). All these databases were recommended by domain experts in evidence-based medicine. The retrieval scheme was mainly based on a combination of subject words and free words. Search terms included delirium (i.e., delirium, delirious, intensive care delirium, cognitive dysfunction) and cardiac surgery (i.e., cardiac surgery, heart surgery, open heart; see Supplementary Table 2 for the search strategies). A manual search was further performed to search the reference lists of relevant articles. Databases were searched from January 1980 to July 20, 2021, and the language of studies were limited to English and Chinese.
Studies were included if they satisfied the following inclusion criteria: (1) Type of participants: adult patients (aged ≥18 years) undergo cardiac surgery. (2) Type of exposure: POD, and it must be identified using a validated CAM-ICU, CAM, ICDSC; or diagnosed according to DSM-4 or DSM-5. (3) Type of outcome: studies report at least one of the following outcomes, mortality, hospital days, ICU time, and MV time. If mortality was reported at multiple time points, the longest follow-up mortality was used for analysis. (4) Types of studies: prospective or retrospective observational study. When multiple articles included the same population of patients, only the newest, or the most complete publication was selected. The exclusion criteria were as follows: (1) Conference abstracts and articles where the full text was unavailable. (2) Studies of poor quality (the NOS <5). (3) Repeated published literature.
Literature screening was independently conducted by two researchers. First, we used the reference management software Endnote X8 for literature classification, preparation, and removal of duplicates. Then two reviewers independently read titles and abstracts and preliminary screened the literature according to inclusion and exclusion criteria. Finally, the remaining records were evaluated by reading the full-text papers. Reasons for exclusion of studies following full-text reading were recorded. Discrepancies were resolved by discussion or consulting the third reviewer.
Two researchers independently performed the data extraction using a pre-established data extraction table. We recorded the following information (when available): author, publication year, country, study design, sample size, inclusion/exclusion criteria, data collection time, age, gender, types of cardiac surgery, method of POD assessment, clinical outcomes, etc. Authors of studies with missing data were contacted by email to obtain additional data.
Study quality was assessed by two researchers using the NOS (17), which included three aspects: object selection, comparability, and exposure/outcome assessment. NOS scores ranged from 0 to 9, and a score of 0 to 4, 5 to 6, and 7 to 9 indicated low, intermediate, and high quality, respectively, (18). The result of the assessment was cross-checked by two researchers and disagreements were resolved under discussion.
Besides, an assessment of the overall quality of evidence was made according to the Grading of Recommendations, Assessment, Development and Evaluation (GRADE) framework (16). We assessed the risk of bias, consistency of effect, indirectness, imprecision, and publication bias. And we used GRADEpro GDT to generate the evidence profile.
All of data were analyzed by the software RevMan5.3., and P < 0.05 was considered statistically significant. The outcomes were mortality, hospital days, ICU time, and MV time. When MV time was reported as counting data, we extracted the incidence of MV time (>24h). The inverse variance method with a SMD as the measure of an effect estimate was used for continuous variables, whereas the Mantel–Haenszel method with OR and 95% CI was employed for dichotomous variables.
Before the combined data were analyzed by meta-analysis, the heterogeneity of each group was tested. Heterogeneity was qualified by I2 (<25%, low heterogeneity; 25–50%, moderate heterogeneity; and >50%, strong heterogeneity). A fixed-effect model was used when the heterogeneity was low or moderate (P > 0.1, I2 < 50%), and a random-effects model was adopted when heterogeneity was high (P ≤ 0.1, I2 ≥ 50%). To explore the source of heterogeneity, we performed subgroup analyses according to the study designs, sample size, countries, types of cardiac surgery et al. And sensitivity analyses were performed by sequentially removing each study and rerunning the analysis, to verify the robustness of the review conclusions. Furthermore, publication bias was measured using a funnel plot.
A total of 22,032 records were retrieved from the literature search, and 13571 were obtained after the removal of duplicates. By reading titles and abstracts, 13342 studies were excluded, as they did not fulfill the selection criteria. Eventually, 229 articles were included for full-text review, of which 42 (35 and 7 articles in English and Chinese, respectively) were finally included. The literature screening process was listed in Figure 1.
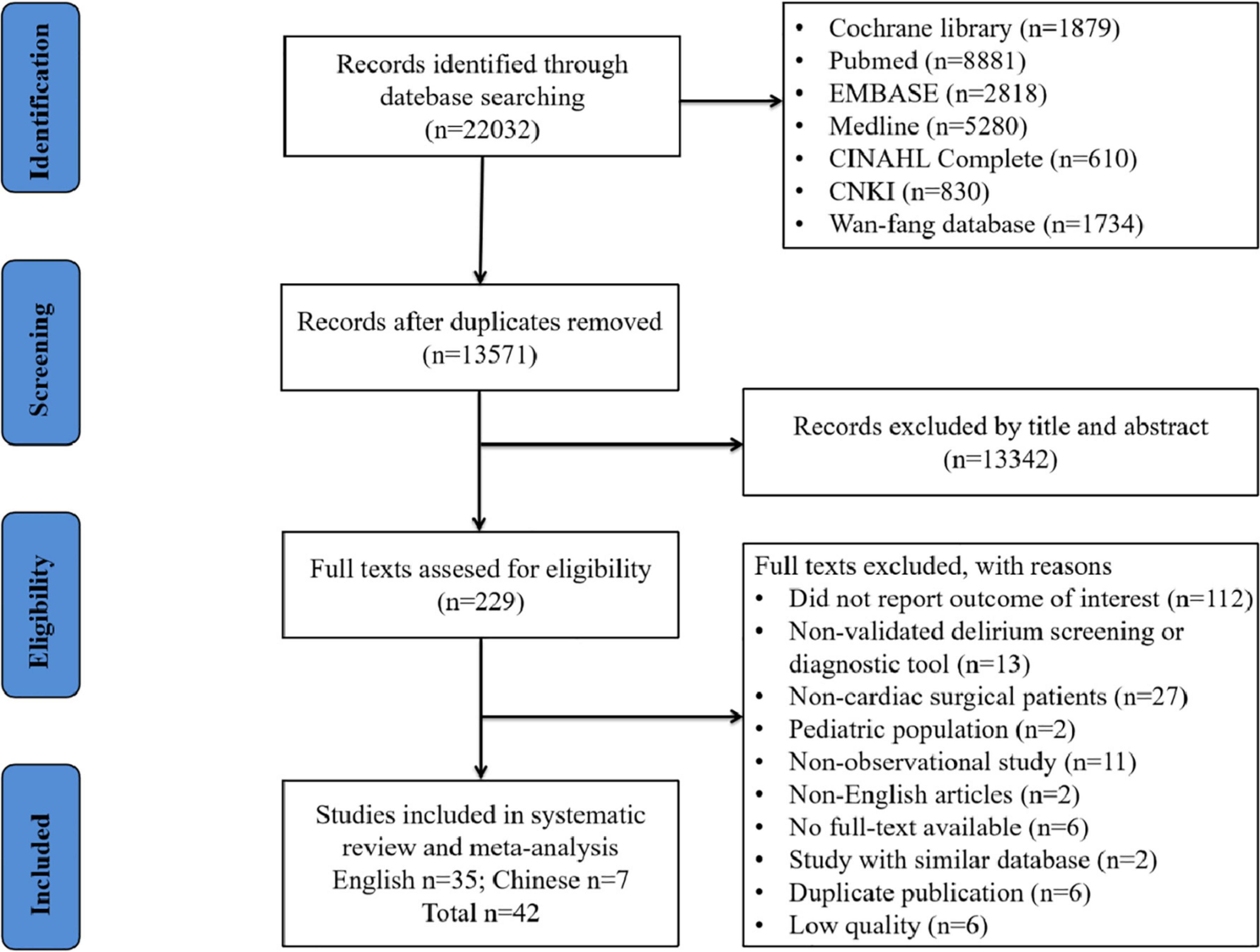
Figure 1. Flow diagram to identify studies reporting the outcome of postoperative delirium in patients undergoing cardiac surgery.
The characteristics of included studies were shown in Table 1. Among the 42 studies, 31 were prospective studies (9, 12, 19–47), and 11 were retrospective studies (10, 48–57), which were published between 2004 and 2021. Sample sizes ranged from 66 to 3397. A total of 19785 patients were included and the male proportion of each study varied from 36.9 to 84.3%. Concerning procedure types, it includes acute CABG (22, 38, 42, 48, 53), valve surgery (10, 21, 26, 31–33, 46, 49, 51), AAD surgery (44, 52, 54, 57), and mixed cardiac surgery (9, 12, 19, 20, 23–25, 27–29, 35, 36, 47, 55, 56).
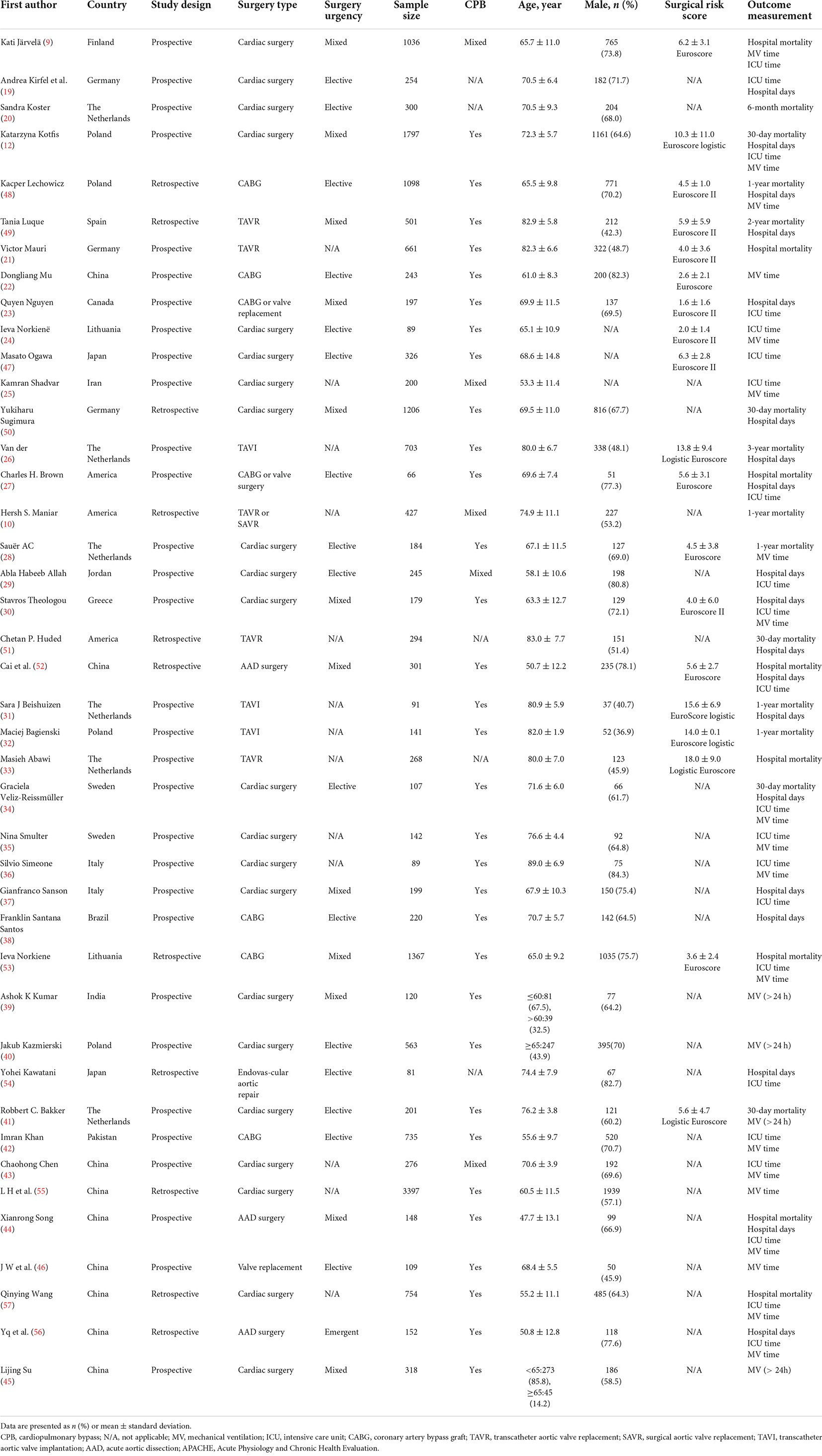
Table 1. Characteristics of the included studies.
Table 2 displays the screening and morbidity of POD reported by the included studies. The overall incidence of POD was 17.0% (3368 of 19785 patients). As for the assessment tool for POD, a total of 33 studies were reported using a single measurement. Among them, 15 studies used CAM-ICU (10, 21, 22, 25, 30, 36, 39, 41, 44–46, 49, 50, 52, 55), six studies used DMS-4 (26, 31, 38, 40, 42, 53), 2 studies used DMS-5 (12, 57), five studies used ICDSC (9, 24, 37, 47, 54), two studies used CAM (34, 56), two studies used DOS (20, 33), and one study used CHART-DEL (29). Two or more tools were used to diagnose delirium in other studies (19, 23, 27–29, 35, 43, 48, 51).
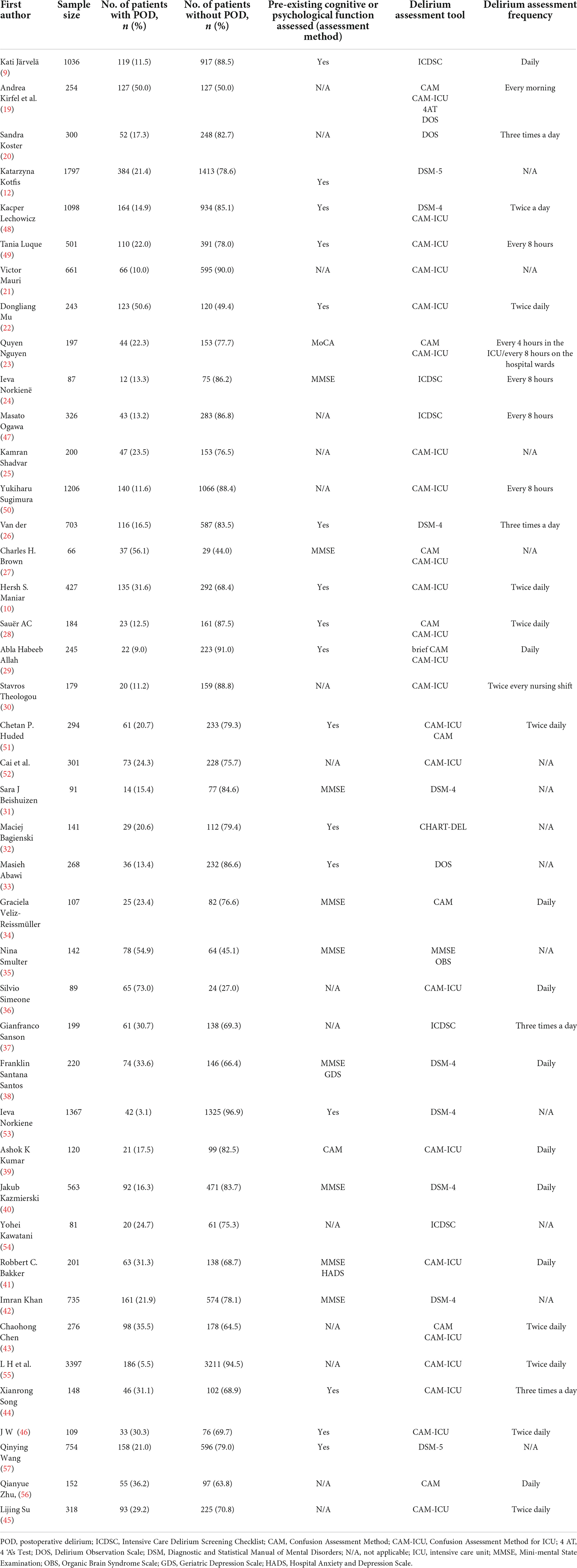
Table 2. Postoperative delirium screening and prevalence data from the included studies.
The quality of included studies was assessed using the NOS quality scale. Three domains were assessed: selection, comparability, and outcome. The results of the quality assessment are shown in Supplementary Table 3. All included studies scored greater than four points, 31 studies were classified as high-quality, and 11 studies were classified as moderate-quality.
Twenty-one studies (9, 10, 12, 20, 21, 26–28, 31–34, 41, 44, 48–53, 57) reported the incidence of mortality, which included 11643 individuals. The results of a random-effects model showed that patients with POD had 2.77-fold mortality compared to those without POD (OR = 2.77, 95% CI 1.86–4.11, P < 0.001), with a significant heterogeneity (I2 = 76%; Figure 2A). Furthermore, we analyzed mortality based on different time points (short term ≤6 months and long term >6 months). The pooled results showed that there was a significant association between POD and short-term mortality (OR = 2.80, 95% CI 1.39–5.64, P = 0.004; I2 = 81%) and long-term mortality (OR = 2.65, 95% CI 1.86–4.11, P < 0.001; I2 = 76%), with a low heterogeneity between two groups (I2 = 0%; Figure 2B).
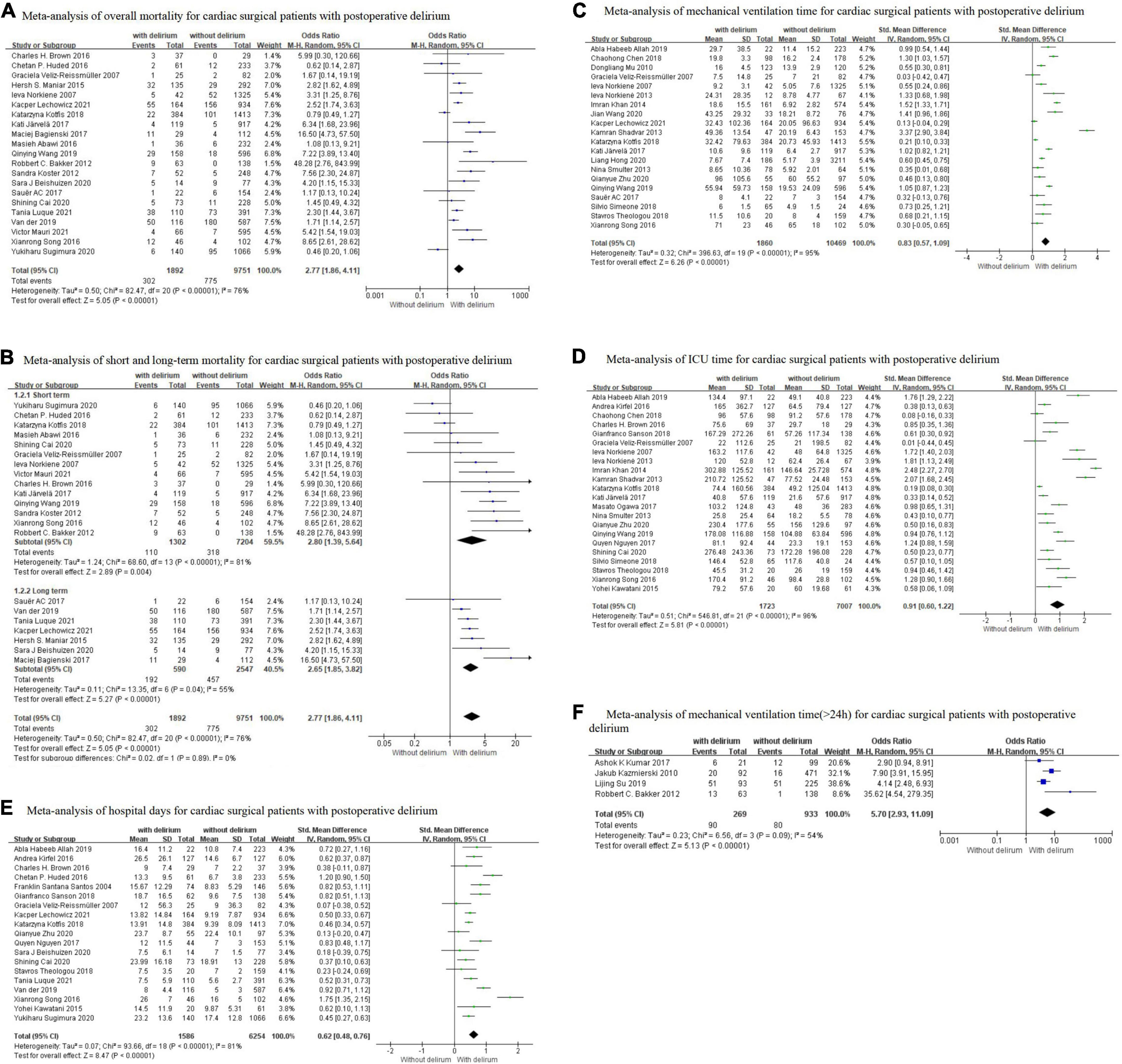
Figure 2. Results of meta-analysis on the association between postoperative delirium and outcomes (A) Overall mortality; (B) Short-term and long-term mortality; (C) Mechanical ventilation time; (D) ICU time; (E) Hospital days; (F) Prolonged mechanical ventilation time (>24h). The summary effects were obtained using a random-effects model. The size of the data markers indicates the weight of the study. The diamond data markers indicate pooled ORs or SMD, and 95% CI.
To explore the sources of heterogeneity, subgroup analyses for mortality were conducted by the study design, sample size, male proportion, surgery type, and study region as shown in Table 3. When subgroups were stratified by study design, we found a significant effect between prospective studies (OR = 3.81, P < 0.001) and retrospective studies (OR = 2.12, P = 0.004). When subgroups were stratified by sample size, the mortality was significantly higher in patients with POD in the <500 subgroups (OR = 3.60, P < 0.001) and ≥500 subgroups (OR = 2.26, P = 0.002). When subgroups were stratified by male proportion, the risk of mortality was higher in the <50% subgroup (OR = 3.20, P < 0.001) than in the 50–70% subgroup (OR = 2.47, P = 0.030). When subgroups were stratified by surgery type, summary effects were only statistically significant in mixed cardiac surgery (OR = 2.93, P = 0.040), valve surgery (OR = 2.72, P < 0.001), and CABG (OR = 2.60, P < 0.001), whereas no significant was found in aortic surgery subgroup. When subgroups were stratified by region, the mortality was significantly higher in the Asia subgroup (OR = 4.63, P = 0.004) and Europe subgroup (OR = 2.63, P < 0.001), but not in the America subgroup. The forest plots are presented in Supplementary Figure 1. It was discovered that the results of each subgroup analysis were consistent with the overall results, but the between-study heterogeneity within subgroups remained substantial. After excluding five studies (12, 26, 32, 50, 57), the heterogeneity decreased substantially and the result of each subgroup was not significantly changed.
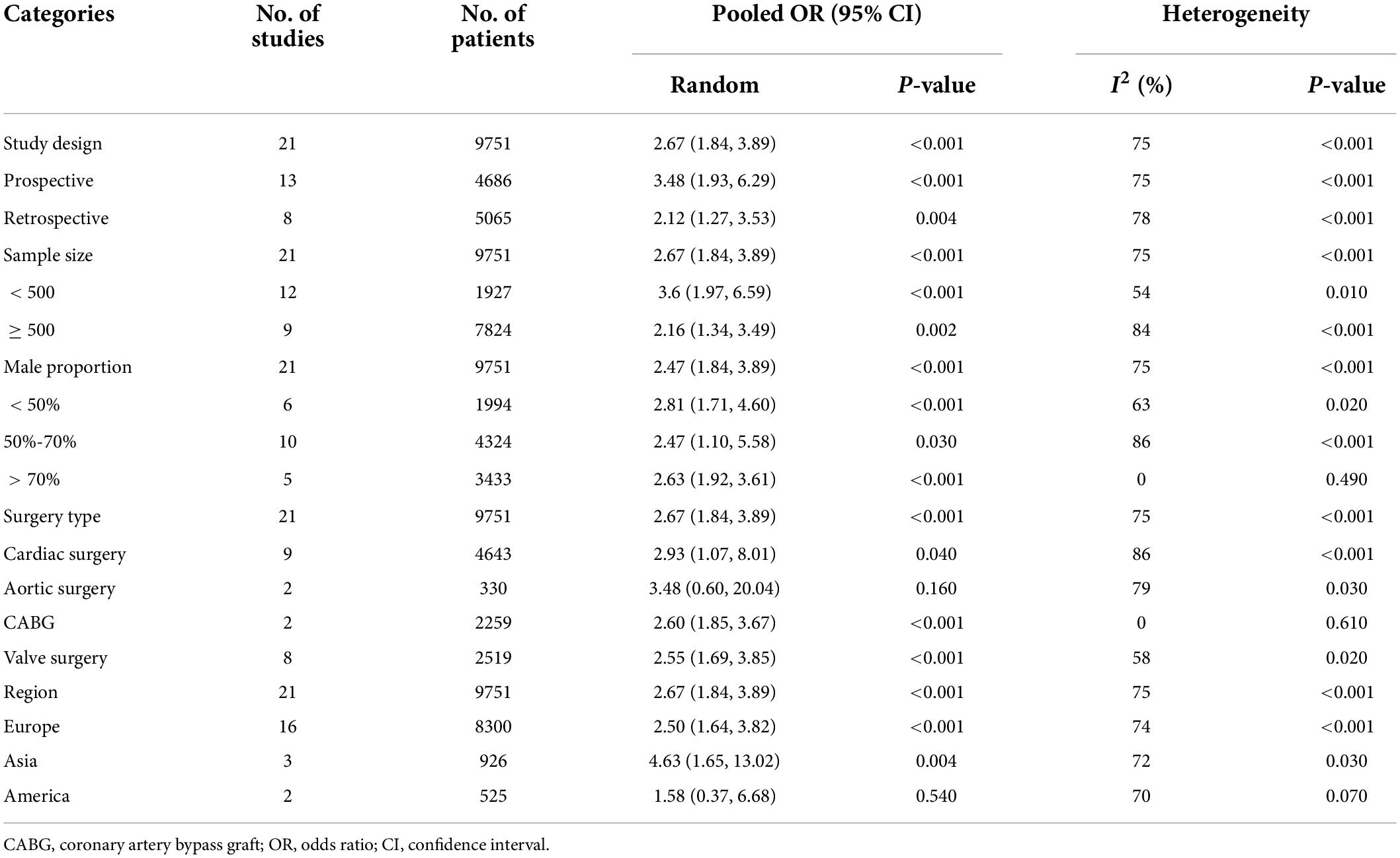
Table 3. Subgroup analysis of pooled OR for mortality.
Twenty studies (9, 12, 22, 24, 25, 28–30, 34–36, 42, 47, 48, 53) reported the MV time as an outcome measure, which included 13503 individuals. Using a random-effects model, the pooled SMD was 0.83 (SMD = 0.83, 95% CI 0.57–1.09, P < 0.001) with significant heterogeneity (I2 = 95%), which showed that patients with POD had significantly longer MV time compared to those without POD (Figure 2C). Findings from subgroup analysis showed that the MV time was longer in patients aged <60 (SMD = 1.27, 95% CI 0.65–1.89, P < 0.001), and the studies with male proportion <60% (SMD = 0.98, 95% CI 0.18–1.79, P = 0.020). Nevertheless, the subgroup analysis still showed considerable heterogeneity (> 90%; Supplementary Table 3). Sensitivity analysis also failed to find the source of heterogeneity.
Twenty-two studies (9, 12, 19, 23–25, 27, 29, 30, 34, 47, 52, 53, 56) reported the ICU time as an outcome measure, which included 9231 individuals. The results with a random-effects model showed that the ICU time was significantly longer for patients with POD than for those without POD patients (SMD = 0.91, 95% CI 0.60–1.22, P < 0.001) with significant heterogeneity (I2 = 96%; Figure 2D). The subgroup analysis showed that the ICU time was longer in elective surgery patients (SMD = 1.10, 95% CI 0.38–1.83, P = 0.003), and the Asia population (SMD = 1.13, 95% CI 0.46–1.62, P < 0.001). Study design, sample size, operation time, and study region were not sources of heterogeneity because heterogeneity was still high after subgroup analysis (Supplementary Table 4). Furthermore, the sensitivity analysis did not find any study that significantly affected heterogeneity.
Nineteen studies (12, 19, 23, 26, 27, 29–31, 47–52) reported the length of hospital days as an outcome measure, which included 7840 individuals. The results with a random-effects model showed that the hospital days of the delirium group were 0.62 days longer than those without delirium (SMD = 0.62, 95% CI 0.48–0.76, P < 0.001) with significant heterogeneity (I2 = 81%; Figure 2E). The subgroup analysis showed that the hospital days was longer in the valve surgery patient (SMD = 0.75, 95% CI 0.39–1.11, P < 0.001), patient >60 (SMD = 0.75, 95% CI 0.39–1.11, P < 0.001), and the studies with male proportion <60 (SMD = 0.75, 95% CI 0.39–1.11, P < 0.001). It was discovered that the results of each subgroup analysis were consistent with the overall results, but the between-study heterogeneity within subgroups remained substantial (Supplementary Table 5). After excluding four studies (26, 37, 44, 51), the heterogeneity decreased substantially and the result of each subgroup was not significantly changed.
Four studies (39–41, 45) reported the incidence of MV (>24h) as an outcome measure, which included 1202 individuals. The pooled OR using a random-effects model was 5.70 (95% CI 2.93–11.09, P < 0.001) with moderate heterogeneity (I2 = 54%), which showed that patients with POD had a 5.7-fold incidence of MV (>24h) compared to those without POD (Figure 2F). The sensitivity analysis showed that heterogeneity was evidently reduced (I2 = 34%, P = 0.22) after excluding Bakker et al.’s study (41), which may be due to the difference in age of the study population.
To assess potential publication bias, the tendency that significant results are more likely to be published than negative results, we examined each outcome by funnel plot. As shown in Figure 3, a certain degree of asymmetry was observed, which indicated slight publication bias.
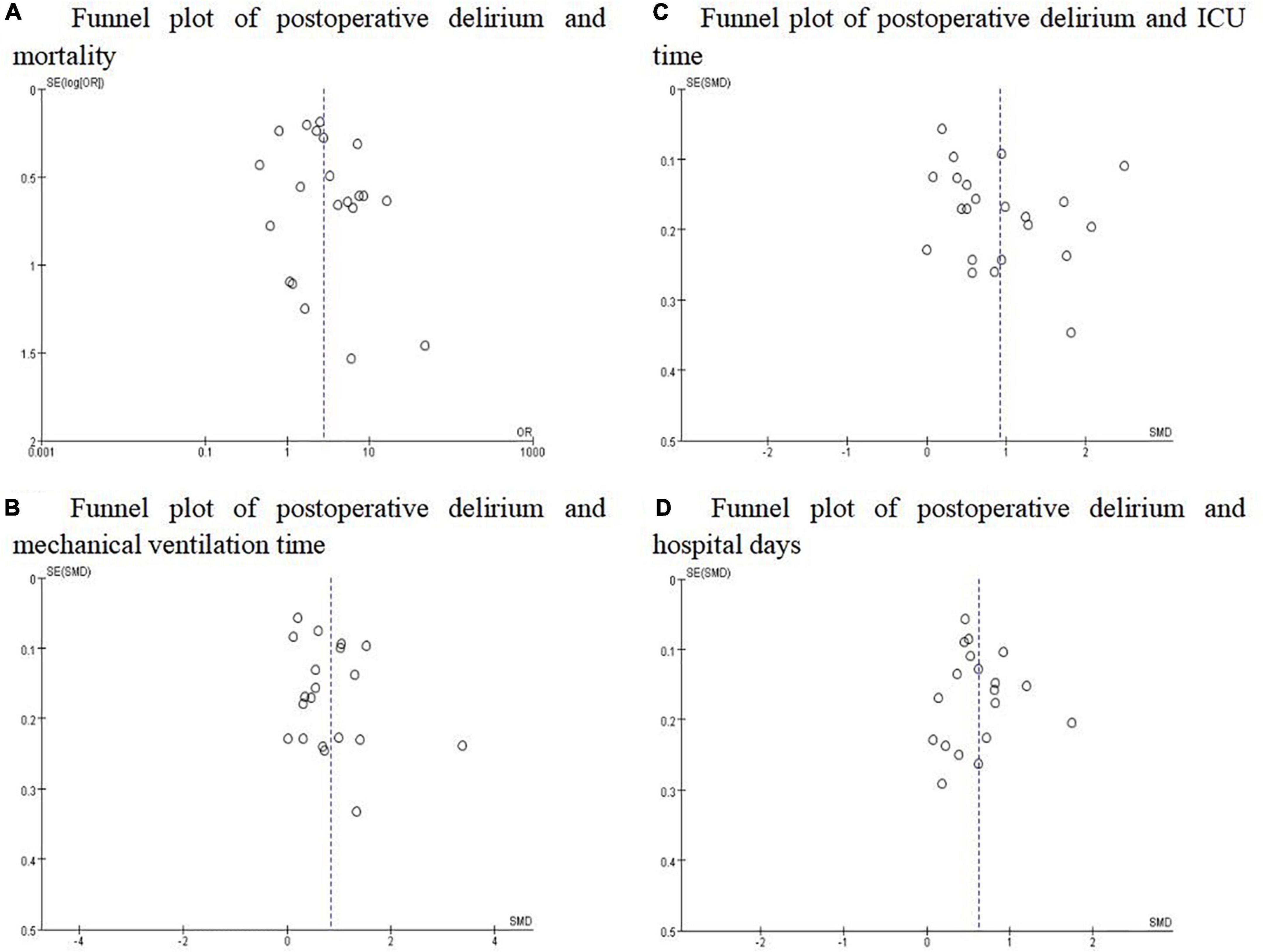
Figure 3. Funnel plots for the studies involved in the meta-analysis. (A) Mortality; (B) Mechanical ventilation time; (C) ICU time; (D) Hospital days. The distribution was not completely symmetrical around the funnel plot, which suggested the possibility of publication bias.
Based on the GRADE approach, the evidence quality of overall mortality was low, and the evidence quality of MV time, ICU time, and hospital days were very low. Besides, we found a moderate quality of evidence for MV time (>24h) (as shown in Figure 4).
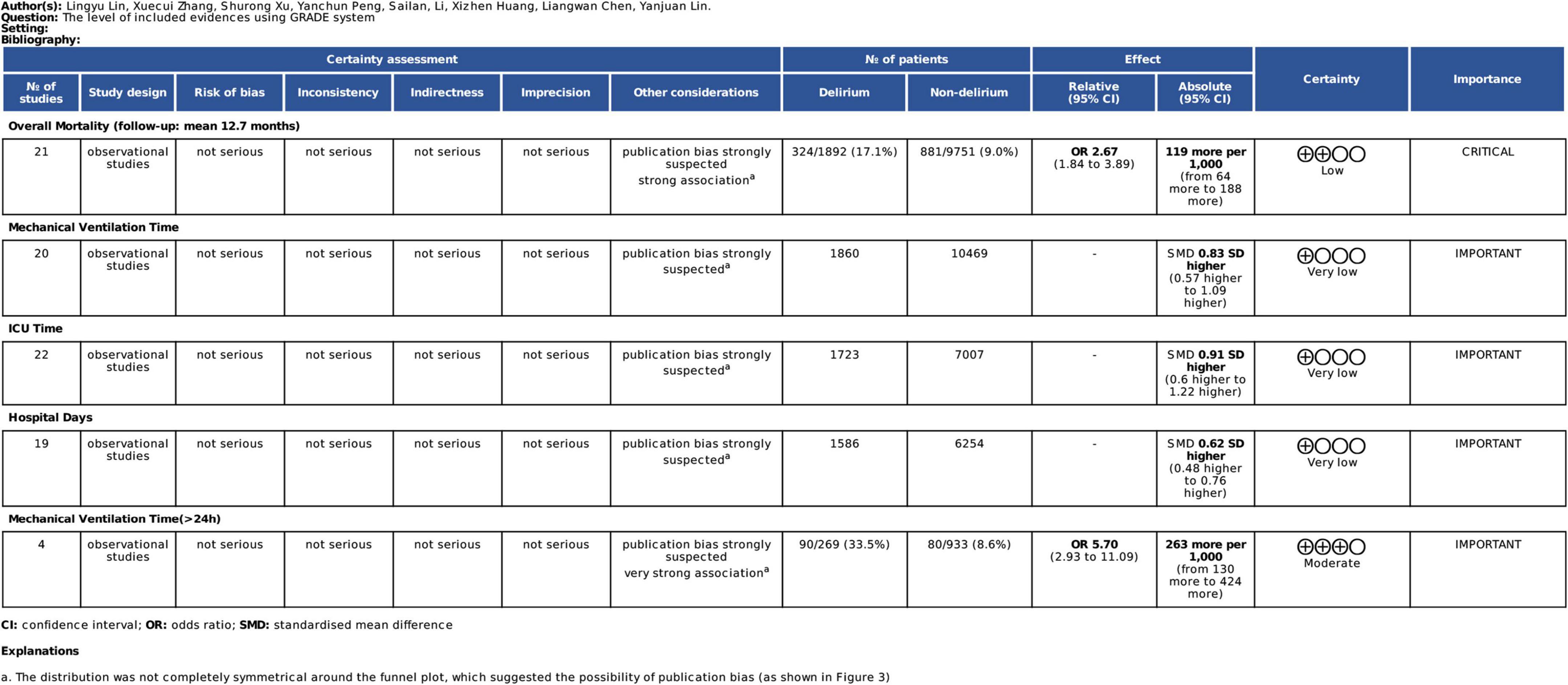
Figure 4. Grading of recommendations, assessment, development and evaluation (GRADE) summary of findings table.
The present systematic review and meta-analysis identified 42 studies enrolling a total of 19,785 patients, to summarize the relationship between POD and outcomes in patients undergoing cardiac surgery. The overall incidence of POD was 17.0%, and the results of the meta-analysis showed POD has been associated with increased mortality, longer duration of MV time, ICU stays, and hospitalization among cardiac surgical patients. Given certain heterogeneity among studies, we next conducted subgroup analysis based on study design, sample size, male proportion, surgery type, study region, etc. Despite remaining heterogeneity after subgroup analysis, it was partly reduced in some subgroups. This suggests that POD is a very common and severe neuropsychiatric syndrome, that seriously affects the prognosis of patients.
In this study, POD was significantly linked to mortality. However, due to the significant heterogeneity across studies, this relationship may be limited. Subgroup analyses were conducted based on the timing of mortality, and the results indicated that POD is related to short- and long-term mortality of cardiac surgery patients, which was partially consistent with Crocker et al. (58). The difference was that Crocker et al. indicated that POD was no significant association with short-term mortality. This may be linked to no meta-regression analysis performed to assess the influence of POD on short-term mortality in their study, as only two of the included studies had reported 6-month mortality. However, short-term mortality was reported in 13 studies in our article, where a larger sample size may yield different results.
The mechanism by which POD increases mortality risk is not understood. We propose the following explanations to comprehend the results. First, higher levels of postoperative pro-inflammatory cytokines (e.g., IL-2, IL-6, TNF-α, MCP-1) were associated with a higher risk to develop POD in cardiac surgery patients (59, 60). Elevated levels of pro-inflammatory cytokines reflect an active inflammatory response in the body, which may cause systemic inflammatory response syndrome. Systemic inflammation can alter the brain’s inflammatory status, produce acute cognitive impairments, such as POD, and drive new pathology and accelerated decline (61). Thus, the presence of POD can be considered a marker of hyperinflammatory conditions, which are associated with higher mortality (62, 63). Second, Holmes et al. (64) indicated that POD may represent an extreme non-adaptive presentation of sickness. Patients who develop delirium after cardiac surgery could cause cognitive impairment, decreased consciousness, behavioral abnormalities, etc., which increase cerebrovascular accidents, bleeding, infection, and other complications risk (50, 65, 66), and patients with hypoactive motor-type delirium may present with more severe systemic disease, increased complications of inactivity (e.g., dehydration, pressure ulcers, hypoventilation, and venous thrombosis; 67), these complications are associated with higher mortality (68). Finally, POD is closely associated with the presence of hemodynamic or electrical instability, and disorders of fluids and electrolytes, which may increase the risk of mortality (69). The accidental extubation, difficulty in weaning, or reintubation in patients with MV were also increased (70–73), which required an increased duration of MV, and it has been well documented that prolonged MV time is an independent predictor of increased mortality (74). The data also showed that POD could result in prolonged hospital and ICU stays of the patients, concordant with the results of Salluh’s study (8). The longer the patients stay in the hospital, the more they are at risk of complications and death. All these factors may explain the increased mortality risk among patients who develop POD. Further investigation regarding the pathophysiological mechanism of POD is still warranted to fully understand the reasons why POD led to poor outcomes among cardiac surgical patients.
Given the poor outcomes among cardiac surgery patients who developed POD, there exists a great opportunity to improve the outcomes among these patients. A review (75) in Lancet reported that 30 to 40% of delirium may be prevented by early detection, and takes pharmacologic or non-pharmacologic interventions. Current guidelines (76) recommend using a multicomponent, non-pharmacologic intervention to reduce delirium. The strategies include cognitive training, improving sleep quality, improving wakefulness, early rehabilitation, etc. (conditional recommendation, low quality of evidence). However, it is still uncertain as to which interventions result in the effect. In the future, emphasis should be put on improving the awareness of medical staff on delirium, and undertaking studies to validate the intervention effects, to provide widely applicable evidence for healthcare policymakers.
There was a high degree of heterogeneity observed in our meta-analysis. The reasons might be as follows: first, the methods for diagnosing delirium were different. The incidence of delirium may be dependent on the different diagnostic criteria applied, different tools used, and different evaluators. Second, the study periods of the included studies were different. With the progressive developments in delirium research, the attention toward POD has gradually increased. In previous years, POD has not yet attracted enough attention from medical staff, and there is also wide variation across hospitals in the treatment of POD. In addition, sample sources were different. The structure of the population in different studies was different such as age, gender ratio, race, disease severity, and surgery types, which could contribute to the different clinical outcomes. Most of the included studies did not provide adjusted data due to the high risk of confounding bias, for example, age, sex, and disease severity, which is the reason why we did not use the adjusted data for further analysis. Regarding the mortality outcome, we conducted a sensitivity analysis. The heterogeneity was reduced from 75 to 24% after the removal of five studies (12, 26, 32, 50, 57), which indicates that the five studies were the source of heterogeneity.
The present meta-analysis exhibited several strengths, compared to the previously published meta-analysis (13, 58). In the first instance, we used a robust methodology following PRISMA guidelines and a comprehensive search strategy, to ensure the inclusion of all relevant literature. Second, we included 42 studies with a larger sample size. It could provide high statistical power to quantitatively evaluate the association between POD and clinical outcomes. Hence, the validity of the results is more reliable. In addition, the included studies in this meta-analysis had high NOS scores which were strictly following the inclusion and exclusion criteria, thus, reducing the potential selection bias.
However, there remain limitations in this study as well. First, a meta-analysis of MV time, and ICU time showed heterogeneity, but sensitivity analysis and subgroup analysis failed to eliminate it. The random-effects model is used for data processing, which may have a slight impact on the reliability of the results. We speculate that heterogeneity might be partially explained by the differences in factors such as patient characteristics (age, sex, type of surgery, etc.), different diagnostic criteria for delirium, unequal levels of regional medical care, and frequency of delirium assessment. Second, variations in the assessment tools and the assessment time-points of delirium might affect the results. Delirium is a fluctuation in mental status that can change over time and may have occurred before or after assessments. Thus, the true incidence of POD and its effects on clinical outcomes might be underestimated. All included studies screened patients utilizing validated delirium assessment tools, but the latest research states that POD needs to meet DSM-5 diagnostic criteria (13), and not all studies achieve this. Future prospective studies with standardized delirium assessment methods are still needed to detect delirium accurately and reliably. Third, due to insufficient data, we could not further evaluate other potential factors that may affect the heterogeneity between studies, such as Euroscore score, complications, and the use of anesthetic drugs. Finally, publication bias remains a major concern for all kinds of meta-analyses because non-significant or negative results are less likely to be published than studies with positive and significant results. To comprehensively identify negative or insignificant outcomes, we used delirium and cardiac surgery as keywords which meant the kinds of literature published on this topic were eligible, to ensure we identified as many relevant studies as possible; and also incorporated all reported outcome measures from each study. In addition, funnel plots were constructed to assess potential publication bias, and it is worth mentioning that there was no observable publication bias.
In this meta-analysis, we found that POD was involved in poor prognosis among cardiac surgical patients. Patients who develop POD exhibit longer MV time, ICU stay, hospital stay, and greater risk of mortality than patients without POD. Future research should focus on developing and testing interventions for delirium, to reduce its incidence and thereby lower the risk of adverse outcomes in these patients.
The original contributions presented in this study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author/s.
LL: project administration, conceptualization, investigation, date curation, methodology, formal analysis, and writing—original draft, review and editing. XZ: conceptualization, investigation, date curation, formal analysis, and writing—original draft, review and editing. SX: methodology, date curation, and writing—original draft, review and editing. YP: conceptualization and writing—original draft, review and editing. SL: software, date curation, and writing—review and editing. XH: date curation and writing—review and editing. LC: supervision and funding acquisition. YL: conceptualization, supervision, and funding acquisition.
This work was supported by the Guiding project of Fujian Provincial Department of Science and Technology (grant numbers: 2021Y0023); Joint Finds for the innovation of science and Technology, Fujian province (grant numbers: 2017Y9052); and Fujian Key Laboratory of Cardio-Thoracic Surgery (Union Hospital, Fujian Medical University).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fcvm.2022.884144/full#supplementary-material
POD, postoperative delirium; ICU, intensive care unit; MV, mechanical ventilation; PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses; CAM-ICU, Confusion Assessment Method for ICU; CAM, Confusion Assessment Method; ICDSC, Intensive Care Delirium Screening Checklist; DSM, Diagnostic and Statistical Manual of Mental Disorders; NOS, Newcastle-Ottawa scale; SMD, standardized mean difference; OR, odds ratio; CI, confidence interval; CABG, coronary artery bypass graft; AAD, acute aortic dissection; DOS, Delirium Observation Screening Scale; CHART-DEL, Chart-Based Delirium Identification Instrument; CPB, cardiopulmonary bypass; N/A, not applicable; TAVR, transcatheter aortic valve replacement; SAVR, surgical aortic valve replacement; TAVI, transcatheter aortic valve implantation; APACHE, Acute Physiology and Chronic Health Evaluation; 4 ‘AT’, 4 ‘A’s test; MMSE, Mini-Mental State Examination; OBS, Organic Brain Syndrome Scale; GDS, Geriatric Depression Scale; HADS, Hospital Anxiety And Depression Scale.
1. Virani SS, Alonso A, Benjamin EJ, Bittencourt MS, Callaway CW, Carson AP, et al. Heart disease and stroke statistics-2020 update: a report from the American Heart Association. Circulation. (2020) 141:e139–596. doi: 10.1161/cir.0000000000000757
2. Bansilal S, Castellano JM, Fuster V. Global burden of Cvd: focus on secondary prevention of cardiovascular disease. Int J Cardiol. (2015) 201:S1–7. doi: 10.1016/s0167-5273(15)31026-3
3. Vervoort D, Swain JD, Pezzella AT, Kpodonu J. Cardiac surgery in low- and middle-income countries: a state-of-the-art review. Ann Thorac Surg. (2021) 111:1394–400. doi: 10.1016/j.athoracsur.2020.05.181
4. Cai S, Latour JM, Lin Y, Pan W, Zheng J, Xue Y, et al. Preoperative cardiac function parameters as valuable predictors for nurses to recognise delirium after cardiac surgery: a prospective cohort study. Eur J Cardiovasc Nurs. (2020) 19:310–9. doi: 10.1177/1474515119886155
5. Gosselt AN, Slooter AJ, Boere PR, Zaal IJ. Risk factors for delirium after on-pump cardiac surgery: a systematic review. Crit Care. (2015) 19:346. doi: 10.1186/s13054-015-1060-0
6. de la Varga-Martínez O, Gómez-Pesquera E, Muñoz-Moreno MF, Marcos-Vidal JM, López-Gómez A, Rodenas-Gómez F, et al. Development and validation of a delirium risk prediction preoperative model for cardiac surgery patients (Deliprecas): an observational multicentre study. J Clin Anesth. (2021) 69:110158. doi: 10.1016/j.jclinane.2020.110158
7. Oh ES, Fong TG, Hshieh TT, Inouye SK. Delirium in older persons: advances in diagnosis and treatment. JAMA. (2017) 318:1161–74. doi: 10.1001/jama.2017.12067
8. Salluh JI, Wang H, Schneider EB, Nagaraja N, Yenokyan G, Damluji A, et al. Outcome of delirium in critically ill patients: systematic review and meta-analysis. BMJ. (2015) 350:h2538. doi: 10.1136/bmj.h2538
9. Järvelä K, Porkkala H, Karlsson S, Martikainen T, Selander T, Bendel S. Postoperative delirium in cardiac surgery patients. J Cardiothorac Vasc Anesth. (2018) 32:1597–602. doi: 10.1053/j.jvca.2017.12.030
10. Maniar HS, Lindman BR, Escallier K, Avidan M, Novak E, Melby SJ, et al. Delirium after surgical and transcatheter aortic valve replacement is associated with increased mortality. J Thorac Cardiovasc Surg. (2016) 151:815e–23e. doi: 10.1016/j.jtcvs.2015.10.114
11. Jones D, Matalanis G, Mårtensson J, Robbins R, Shaw M, Seevanayagam S, et al. Predictors and outcomes of cardiac surgery-associated delirium. A single centre retrospective cohort study. Heart Lung Circ. (2019) 28:455–63. doi: 10.1016/j.hlc.2018.01.007
12. Kotfis K, Szyliñska A, Listewnik M, Strzelbicka M, Brykczyñski M, Rotter I, et al. Early delirium after cardiac surgery: an analysis of incidence and risk factors in elderly (≥65 Years) and very elderly (≥80 years) patients. Clin Interv Aging. (2018) 13:1061–70. doi: 10.2147/cia.S166909
13. Prasitlumkum N, Mekritthikrai R, Kewcharoen J, Kanitsoraphan C, Mao MA, Cheungpasitporn W. Delirium is associated with higher mortality in transcatheter aortic valve replacement: systemic review and meta-analysis. Cardiovasc Interv Therapeut. (2020) 35:168–76. doi: 10.1007/s12928-019-00592-y
14. Arachchi TMJ, Pinto V. Understanding the barriers in delirium care in an intensive care unit: a survey of knowledge, attitudes, and current practices among medical professionals working in intensive care units in teaching hospitals of Central Province, Sri Lanka. Ind J Crit Care Med. (2021) 25:1413–20. doi: 10.5005/jp-journals-10071-24040
15. Trogrliæ Z, Ista E, Ponssen HH, Schoonderbeek JF, Schreiner F, Verbrugge SJ, et al. Attitudes, knowledge and practices concerning delirium: a survey among intensive care unit professionals. Nurs Crit Care. (2017) 22:133–40. doi: 10.1111/nicc.12239
16. Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the prisma statement. PLoS Med. (2009) 6:e1000097. doi: 10.1371/journal.pmed.1000097
17. Stang A. Critical evaluation of the newcastle-ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur J Epidemiol. (2010) 25:603–5. doi: 10.1007/s10654-010-9491-z
18. Zhang HJ, Ma XH, Ye JB, Liu CZ, Zhou ZY. Systematic review and meta-analysis of risk factor for postoperative delirium following spinal surgery. J Orthop Surg Res. (2020) 15:509. doi: 10.1186/s13018-020-02035-4
19. Kirfel A, Menzenbach J, Guttenthaler V, Feggeler J, Mayr A, Coburn M, et al. Postoperative delirium after cardiac surgery of elderly patients as an independent risk factor for prolonged length of stay in intensive care unit and in hospital. Aging Clin Exp Res. (2021) 33:3047–56. doi: 10.1007/s40520-021-01842-x
20. Koster S, Hensens AG, Schuurmans MJ, van der Palen J. Consequences of delirium after cardiac operations. Ann Thorac Surg. (2012) 93:705–11. doi: 10.1016/j.athoracsur.2011.07.006
21. Mauri V, Reuter K, Körber MI, Wienemann H, Lee S, Eghbalzadeh K, et al. Incidence, risk factors and impact on long-term outcome of postoperative delirium after transcatheter aortic valve replacement. Front Cardiovasc Med. (2021) 8:645724. doi: 10.3389/fcvm.2021.645724
22. Mu DL, Wang DX, Li LH, Shan GJ, Li J, Yu QJ, et al. High serum cortisol level is associated with increased risk of delirium after coronary artery bypass graft surgery: a prospective cohort study. Crit Care. (2010) 14:R238. doi: 10.1186/cc9393
23. Nguyen Q, Uminski K, Hiebert BM, Tangri N, Arora RC. Midterm outcomes after postoperative delirium on cognition and mood in patients after cardiac surgery. J Thorac Cardiovasc Surg. (2018) 155:660.e–7.e. doi: 10.1016/j.jtcvs.2017.09.131
24. Norkienë I, Ringaitienë D, Kuzminskaitë V, Šipylaitë J. Incidence and risk factors of early delirium after cardiac surgery. Biomed Res Int. (2013) 2013:323491. doi: 10.1155/2013/323491
25. Shadvar K, Baastani F, Mahmoodpoor A, Bilehjani E. Evaluation of the prevalence and risk factors of delirium in cardiac surgery Icu. J Cardiovasc Thorac Res. (2013) 5:157–61. doi: 10.5681/jcvtr.2013.034
26. van der Wulp K, van Wely M, van Heijningen L, van Bakel B, Schoon Y, Verkroost M, et al. Delirium after transcatheter aortic valve implantation under general anesthesia: incidence, predictors, and relation to long-term survival. J Am Geriatr Soc. (2019) 67:2325–30. doi: 10.1111/jgs.16087
27. Brown CH, Laflam A, Max L, Lymar D, Neufeld KJ, Tian J, et al. The impact of delirium after cardiac surgical procedures on postoperative resource use. Ann Thorac Surg. (2016) 101:1663–9. doi: 10.1016/j.athoracsur.2015.12.074
28. Sauër AC, Veldhuijzen DS, Ottens TH, Slooter AJC, Kalkman CJ, van Dijk D. Association between delirium and cognitive change after cardiac surgery. Br J Anaesthes. (2017) 119:308–15. doi: 10.1093/bja/aex053
29. Habeeb-Allah A, Alshraideh JA. Delirium post-cardiac surgery: incidence and associated factors. Nurs Crit Care. (2021) 26:150–5. doi: 10.1111/nicc.12492
30. Theologou S, Giakoumidakis K, Charitos C. Perioperative predictors of delirium and incidence factors in adult patients post cardiac surgery. Pragmat Observ Res. (2018) 9:11–9. doi: 10.2147/por.S157909
31. Beishuizen SJ, Festen S, Loonstra YE, van der Werf HW, de Rooij SE, van Munster BC. Delirium, functional decline and quality of life after transcatheter aortic valve implantation: an explorative study. Geriatr Gerontol Int. (2020) 20:1202–7. doi: 10.1111/ggi.14064
32. Bagienski M, Kleczynski P, Dziewierz A, Rzeszutko L, Sorysz D, Trebacz J, et al. Incidence of postoperative delirium and its impact on outcomes after transcatheter aortic valve implantation. Am J Cardiol. (2017) 120:1187–92. doi: 10.1016/j.amjcard.2017.06.068
33. Abawi M, Nijhoff F, Agostoni P, Emmelot-Vonk MH, de Vries R, Doevendans PA, et al. Incidence, predictive factors, and effect of delirium after transcatheter aortic valve replacement. JACC Cardiovasc Interv. (2016) 9:160–8. doi: 10.1016/j.jcin.2015.09.037
34. Veliz-Reissmüller G, Agüero Torres H, van der Linden J, Lindblom D, Eriksdotter Jönhagen M. Pre-operative mild cognitive dysfunction predicts risk for post-operative delirium after elective cardiac surgery. Aging Clin Exp Res. (2007) 19:172–7. doi: 10.1007/bf03324686
35. Smulter N, Lingehall HC, Gustafson Y, Olofsson B, Engström KG. Delirium after cardiac surgery: incidence and risk factors. Interact Cardiovasc Thorac Surg. (2013) 17:790–6. doi: 10.1093/icvts/ivt323
36. Simeone S, Pucciarelli G, Perrone M, Teresa R, Gargiulo G, Guillari A, et al. Delirium in Icu patients following cardiac surgery: an observational study. J Clin Nurs. (2018) 27:1994–2002. doi: 10.1111/jocn.14324
37. Sanson G, Khlopenyuk Y, Milocco S, Sartori M, Dreas L, Fabiani A. Delirium after cardiac surgery. incidence, phenotypes, predisposing and precipitating risk factors, and effects. Heart Lung. (2018) 47:408–17. doi: 10.1016/j.hrtlng.2018.04.005
38. Santos FS, Velasco IT, Fráguas R Jr. Risk factors for delirium in the elderly after coronary artery bypass graft surgery. Int Psychogeriatr. (2004) 16:175–93.
39. Kumar AK, Jayant A, Arya VK, Magoon R, Sharma R. Delirium after cardiac surgery: a pilot study from a single tertiary referral center. Ann Card Anaesth. (2017) 20:76–82. doi: 10.4103/0971-9784.197841
40. Kazmierski J, Kowman M, Banach M, Fendler W, Okonski P, Banys A, et al. Incidence and predictors of delirium after cardiac surgery: results from the IPDACS study. J Psychosom Res. (2010) 69:179–85. doi: 10.1016/j.jpsychores.2010.02.009
41. Bakker RC, Osse RJ, Tulen JH, Kappetein AP, Bogers AJ. Preoperative and operative predictors of delirium after cardiac surgery in elderly patients. Eur J Cardio Thorac Surg. (2012) 41:544–9. doi: 10.1093/ejcts/ezr031
42. Khan I, Khan AH, Gull S, Kausar S, Iqbal M, Waheed A. Incidence and predictors of delirium in postoperative coronary artery bypass surgery patients in pakistani population. Pak J Med Health Sci. (2014) 8:92–7.
43. Chen C, Xp L, Yl C, Xh C, Al L. Research on the prediction of comprehensive geriatric assessment on postoperative delirium in elderly patients in cardiac surgery department. Chin J Mod Nurs. (2018) 2018:809–13.
44. Xianrong S, Zy C, Fr L, Fy D. Risk factors for postoperative delirium in patients after stanford a aortic dissection surgery: a prospective cohort study. Chin J Thorac Cardiovasc Surg. (2016) 32:607–11.
45. Su L, Yan Y, Huang W, Xu Q, Liao J, Lin H, et al. Risk factors for intensive care unit delirium after cardiac operation. Chin Crit Care Med. (2019) 31:165–71.
46. J W, Xc W, Jz L, Sy H, L J, F G, et al. Correlation between biomarkers for neuronal injury and delirium in elderly patients after cardiac valve replacement surgery. Chin J Mult Organ Dis Elderly. (2021) 19:886–90.
47. Ogawa M, Izawa KP, Satomi-Kobayashi S, Tsuboi Y, Komaki K, Gotake Y, et al. Impact of delirium on postoperative frailty and long term cardiovascular events after cardiac surgery. PLoS One. (2017) 12:e0190359. doi: 10.1371/journal.pone.0190359
48. Lechowicz K, Szyliñska A, Listewnik M, Drożdżal S, Tomska N, Rotter I, et al. Cardiac delirium index for predicting the occurrence of postoperative delirium in adult patients after coronary artery bypass grafting. Clin Interv Aging. (2021) 16:487–95. doi: 10.2147/cia.S302526
49. Luque T, Noriega FJ, McInerney A, Travieso A, Corrochano D, Tirado-Conte G, et al. Impact of delirium in acute cardiac care unit after transcatheter aortic valve replacement. Int J Cardiol. (2021) 330:164–70. doi: 10.1016/j.ijcard.2021.01.053
50. Sugimura Y, Sipahi NF, Mehdiani A, Petrov G, Awe M, Minol JP, et al. Risk and consequences of postoperative delirium in cardiac surgery. Thorac Cardiovasc Surgeon. (2020) 68:417–24. doi: 10.1055/s-0040-1708046
51. Huded CP, Huded JM, Sweis RN, Ricciardi MJ, Malaisrie SC, Davidson CJ, et al. The impact of delirium on healthcare utilization and survival after transcatheter aortic valve replacement. Catheteriz Cardiovasc Intervent. (2017) 89:1286–91. doi: 10.1002/ccd.26776
52. Cai S, Zhang X, Pan W, Latour JM, Zheng J, Zhong J, et al. Prevalence, predictors, and early outcomes of post-operative delirium in patients with type a aortic dissection during intensive care unit stay. Front Med. (2020) 7:572581. doi: 10.3389/fmed.2020.572581
53. Norkiene I, Ringaitiene D, Misiuriene I, Samalavicius R, Bubulis R, Baublys A, et al. Incidence and precipitating factors of delirium after coronary artery bypass grafting. Scand Cardiovasc J. (2007) 41:180–5. doi: 10.1080/14017430701302490
54. Kawatani Y, Nakamura Y, Hayashi Y, Taneichi T, Ito Y, Kurobe H, et al. Development of delirium in the intensive care unit in patients after endovascular aortic repair: a retrospective evaluation of the prevalence and risk factors. Crit Care Res Pract. (2015) 2015:405817. doi: 10.1155/2015/405817
55. L H, JK S, X S, QK S. Risk factors analysis and prediction model construction of postoperative delirium after cardiac surgery. LINCHUANG MAZUIXUE ZAZHI. (2020) 36:1195–200.
56. Yq Z, J Y, X S, Y R, Y Z, H Y. Analysis of risk factors of postoperative delirium in patients with acute stanford type a dissection. J Pract Med. (2020) 36:940–3. doi: 10.1186/s13019-020-01217-9
57. Qinying W, Xy X, Y W, Lg W. Incidence and effect factors in patients with delirium after cardiac surgery. Int Nurs Med. (2019) 1:150–4.
58. Crocker E, Beggs T, Hassan A, Denault A, Lamarche Y, Bagshaw S, et al. Long-Term effects of postoperative delirium in patients undergoing cardiac operation: a systematic review. Ann Thorac Surg. (2016) 102:1391–9. doi: 10.1016/j.athoracsur.2016.04.071
59. Kazmierski J, Banys A, Latek J, Bourke J, Jaszewski R. Raised Il-2 and Tnf-A concentrations are associated with postoperative delirium in patients undergoing coronary-artery bypass graft surgery. Int Psychogeriatr. (2014) 26:845–55. doi: 10.1017/s1041610213002378
60. Kaźmierski J, Miler P, Pawlak A, Jerczyñska H, Woźniak J, Frankowska E, et al. Elevated monocyte chemoattractant protein-1 as the independent risk factor of delirium after cardiac surgery. A prospective cohort study. J Clin Med. (2021) 10:1587. doi: 10.3390/jcm10081587
61. Hennessy E, Gormley S, Lopez-Rodriguez AB, Murray C, Murray C, Cunningham C. Systemic Tnf-A produces acute cognitive dysfunction and exaggerated sickness behavior when superimposed upon progressive neurodegeneration. Brain Behav Immun. (2017) 59:233–44. doi: 10.1016/j.bbi.2016.09.011
62. Squiccimarro E, Labriola C, Malvindi PG, Margari V, Guida P, Visicchio G, et al. Prevalence and clinical impact of systemic inflammatory reaction after cardiac surgery. J Cardiothorac Vasc Anesth. (2019) 33:1682–90. doi: 10.1053/j.jvca.2019.01.043
63. Sinning JM, Scheer AC, Adenauer V, Ghanem A, Hammerstingl C, Schueler R, et al. Systemic inflammatory response syndrome predicts increased mortality in patients after transcatheter aortic valve implantation. Eur Heart J. (2012) 33:1459–68. doi: 10.1093/eurheartj/ehs002
64. Holmes C, Cunningham C, Zotova E, Culliford D, Perry VH. Proinflammatory cytokines, sickness behavior, and alzheimer disease. Neurology. (2011) 77:212–8. doi: 10.1212/WNL.0b013e318225ae07
65. Stachon P, Kaier K, Zirlik A, Reinöhl J, Heidt T, Bothe W, et al. Risk factors and outcome of postoperative delirium after transcatheter aortic valve replacement. Clin Res Cardiol. (2018) 107:756–62. doi: 10.1007/s00392-018-1241-3
66. Mangusan RF, Hooper V, Denslow SA, Travis L. Outcomes associated with postoperative delirium after cardiac surgery. Am J Crit Care. (2015) 24:156–63. doi: 10.4037/ajcc2015137
67. O’Regan NA, Fitzgerald J, Timmons S, O’Connell H, Meagher D. Delirium: a key challenge for perioperative care. Int J Surg. (2013) 11:136–44. doi: 10.1016/j.ijsu.2012.12.015
68. Dharmarajan K, Swami S, Gou RY, Jones RN, Inouye SK. Pathway from delirium to death: potential in-hospital mediators of excess mortality. J Am Geriatr Soc. (2017) 65:1026–33. doi: 10.1111/jgs.14743
69. Falsini G, Grotti S, Porto I, Toccafondi G, Fraticelli A, Angioli P, et al. Long-Term prognostic value of delirium in elderly patients with acute cardiac diseases admitted to two cardiac intensive care units: a prospective study (Delirium Cordis). Eur Heart J Acute Cardiovasc Care. (2018) 7:661–70. doi: 10.1177/2048872617695235
70. Jeon K, Jeong BH, Ko MG, Nam J, Yoo H, Chung CR, et al. Impact of delirium on weaning from mechanical ventilation in medical patients. Respirology. (2016) 21:313–20. doi: 10.1111/resp.12673
71. Stransky M, Schmidt C, Ganslmeier P, Grossmann E, Haneya A, Moritz S, et al. Hypoactive delirium after cardiac surgery as an independent risk factor for prolonged mechanical ventilation. J Cardiothorac Vasc Anesth. (2011) 25:968–74. doi: 10.1053/j.jvca.2011.05.004
72. van den Boogaard M, Schoonhoven L, van der Hoeven JG, van Achterberg T, Pickkers P. Incidence and short-term consequences of delirium in critically ill patients: a prospective observational cohort study. Int J Nurs Stud. (2012) 49:775–83. doi: 10.1016/j.ijnurstu.2011.11.016
73. Pandharipande PP, Ely EW, Arora RC, Balas MC, Boustani MA, La Calle GH, et al. The intensive care delirium research agenda: a multinational, interprofessional perspective. Intens Care Med. (2017) 43:1329–39. doi: 10.1007/s00134-017-4860-7
74. Fernandez-Zamora MD, Gordillo-Brenes A, Banderas-Bravo E, Arboleda-Sánchez JA, Hinojosa-Pérez R, Aguilar-Alonso E, et al. Prolonged mechanical ventilation as a predictor of mortality after cardiac surgery. Respirat Care. (2018) 63:550–7. doi: 10.4187/respcare.04915
75. Inouye SK, Westendorp RG, Saczynski JS. Delirium in elderly people. Lancet. (2014) 383:911–22. doi: 10.1016/s0140-6736(13)60688-1
76. Devlin JW, Skrobik Y, Gélinas C, Needham DM, Slooter AJC, Pandharipande PP, et al. Clinical practice guidelines for the prevention and management of pain, agitation/sedation, delirium, immobility, and sleep disruption in adult patients in the Icu. Crit Care Med. (2018) 46:e825–73. doi: 10.1097/ccm.0000000000003299
Keywords: postoperative delirium, outcome, cardiac surgery, mortality, systematic review, meta-analysis
Citation: Lin L, Zhang X, Xu S, Peng Y, Li S, Huang X, Chen L and Lin Y (2022) Outcomes of postoperative delirium in patients undergoing cardiac surgery: A systematic review and meta-analysis. Front. Cardiovasc. Med. 9:884144. doi: 10.3389/fcvm.2022.884144
Received: 25 February 2022; Accepted: 21 July 2022;
Published: 09 August 2022.
Edited by:
Lian-Ping He, Taizhou University, ChinaReviewed by:
Zongshi Qin, The University of Hong Kong, Hong Kong SAR, ChinaCopyright © 2022 Lin, Zhang, Xu, Peng, Li, Huang, Chen and Lin. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yanjuan Lin, Zmp4aHlqbEAxNjMuY29t; Liangwan Chen, Y2hlbmxpYW5nd2FuQHRvbS5jb20=
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.