
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Cardiovasc. Med., 12 April 2022
Sec. Thrombosis and Haemostasis
Volume 9 - 2022 | https://doi.org/10.3389/fcvm.2022.872115
This article is part of the Research TopicInsights in Thrombosis: 2022View all 9 articles
 David Jiménez1,2,3*
David Jiménez1,2,3* Carmen Rodríguez1Beatriz Pintado1Andrea Pérez1
Carmen Rodríguez1Beatriz Pintado1Andrea Pérez1 Luis Jara-Palomares4Raquel López-Reyes5Pedro Ruiz-Artacho3,6,7Alberto García-Ortega5Behnood Bikdeli8,9,10José Luis Lobo3,11 and the IPEP investigators
Luis Jara-Palomares4Raquel López-Reyes5Pedro Ruiz-Artacho3,6,7Alberto García-Ortega5Behnood Bikdeli8,9,10José Luis Lobo3,11 and the IPEP investigatorsBackground: A recent trial showed that management driven by prognostic assessment was effective in reducing the length of stay (LOS) for acute stable pulmonary embolism (PE). The efficacy and safety of this strategy in each subgroup of risk stratification remains unknown.
Methods: We conducted a post-hoc analysis of the randomized IPEP study to evaluate the effect of a management strategy guided by early use of a prognostic pathway in the low- and intermediate-high risk subgroups defined by the European Society of Cardiology (ESC) model. These subgroups were retrospectively identified in the control arm. The primary outcome was LOS. The secondary outcomes were 30-day clinical outcomes.
Results: Of 249 patients assigned to the intervention group, 60 (24%) were classified as low-, and 30 (12%) as intermediate-high risk. Among 249 patients assigned to the control group, 66 (27%) were low-, and 13 (5%) intermediate-high risk. In the low-risk group, the mean LOS was 2.1 (±0.9) days in the intervention group and 5.3 (±2.9) days in the control group (P < 0.001). In this group, no significant differences were observed in 30-day readmissions (0% vs. 3.0%, respectively), all-cause (0% vs. 0%) and PE-related mortality rates (0% vs. 0%), or severe adverse events (0% vs. 1.5%). In the intermediate-high risk group, the mean LOS was 5.3 (±1.8) days in the intervention group and 6.5 (±2.5) days in the control group (P = 0.08). In this group, no significant differences were observed in 30-day readmissions (3.3% vs. 3.0%, respectively), all-cause (6.7% vs. 7.7%) and PE-related mortality rates (6.7% vs. 7.7%), or severe adverse events (16.7% vs. 15.4%).
Conclusion: The use of a prognostic assessment and management pathway was effective in reducing the LOS for acute PE without comprising safety across subgroups of risk stratification.
Clinical Trial Registration: [ClinicalTrials.gov], Identifier [NCT02733198].
Pulmonary embolism (PE) is a common condition and a leading health issue worldwide with associated substantial morbidity and mortality (1, 2). PE affects about 400,000 people each year in Europe (3). In the United States, between 300,000 and 600,000 cases occur each year (4), which contribute to at least 40,000 deaths (5).
Pulmonary embolism is associated with considerable health care resource utilization (6). Much of the economic burden of venous thromboembolism (VTE) is related to hospitalization costs (7–10) and increasing the number of patients with PE treated as outpatients could potentially reduce PE-related hospital burdens. Although approximately 30% of patients with PE might be suitable for outpatient therapy of their disease (11), the vast majority is still admitted to the hospital (12, 13). In addition, despite recent trends indicating a decline in length of hospital stay (LOS) after PE diagnosis (14), duration of hospitalization is still high (15, 2). Therefore, validation of strategies aimed at safely reducing the LOS are of paramount importance.
For hospitalized patients with acute symptomatic PE, the recent Prognostication in acute Pulmonary Embolism (IPEP) trial showed that prognostication and use of objective criteria for mobilization and early hospital discharge to be safe and associated with reduction in downstream laboratory or echocardiographic testing, and that it was effective in reducing LOS by 2 days, compared with usual care (16). Since the trial used a risk stratification scheme and specific criteria for mobilization and hospital discharge in each subgroup of risk, it would be key to assess whether the efficacy and safety of the intervention was maintained among those patients who benefit most from early discharge (low-risk), and among those at highest risk for short-term complications (intermediate-high risk).
Using the results of a previous randomized trial, the objective of the current manuscript was to specifically assess the effect of a management strategy guided by early use of a prognostic pathway in the low- and intermediate-high risk subgroups defined by the European Society of Cardiology (ESC) model (17).
We performed post-hoc analyses of the recently completed IPEP trial. IPEP was a multicenter, open-label, randomized, clinical trial aimed at evaluating whether a management strategy guided by early use of a prognostic pathway would be more effective than usual care in reducing LOS in hospitalized patients with acute PE. The rationale, design, and primary results of the IPEP study were described previously (16). The trial was conducted in nine academic hospitals across Spain. The institutional review board at each of the participating sites approved the protocol, and each patient provided written informed consent.
Briefly, patients hospitalized with hemodynamically stable acute PE were randomized to either a prognostic assessment and management pathway including risk stratification, followed by predefined criteria for mobilization and hospital discharge (intervention group) vs. usual care (control group). Per protocol, intervention for patients in the active arm was provided by trial investigators who were strictly advised to follow the protocol-recommended pathway, while management of patients in the control arm was performed by other clinicians according to their routine practice.
For patients in the intervention arm, trial investigators measured vital signs to calculate the simplified Pulmonary Embolism Severity Index (sPESI) (18). An sPESI score of 0 identified low-risk patients. Patients with a sPESI > 1 constituted an intermediate-risk group. Within this group, patients had to undergo troponin testing and, for those with a positive result, echocardiographic assessment for right ventricular (RV) dysfunction. Patients with an sPESI > 1 and abnormality for only troponin levels or only echocardiographic RV dysfunction (or neither) comprised the intermediate-low risk group. In turn, patients with an sPESI > 1 and both elevated troponin levels and echocardiographic RV dysfunction comprised the intermediate-high risk group (Supplementary Figure 1).
For the present analysis, only low- and intermediate-high risk patients were included, and prognostication of patients randomly assigned to usual care was done retrospectively.
The primary outcome of the trial was the LOS, defined as the interval from diagnosis of PE at the emergency department to discharge from the hospital. Secondary outcomes included 30-day event rates for readmissions, as well as all-cause and PE-related mortality, and serious adverse events.
For primary and secondary outcomes, a two-sided hypothesis with P-value of less than 0.05 was considered to indicate statistical significance. Because subgroup analyses in the present study were exploratory, the P-values were not adjusted for multiple comparisons and should be interpreted with caution. Comparisons were made with the use of the t-test, the Mann–Whitney U test, Fisher’s exact test, or the chi-squared test, as appropriate. The statistical analyses were performed with the use of the SPSS software package (version 26.0, SPSS) and Stata (version 16.1; StataCorp, College Station, TX, United States).
A total of 651 patients underwent screening, 500 patients underwent randomization and 498 were included in the modified intention-to-treat analysis – 249 patients were assigned to the intervention group and 249 to the control group. The mean age was 66 years and less than 50% of the patients were women.
Of the 249 patients assigned to the intervention group, 60 (24%) were classified as low-, 159 (64%) as intermediate-low, and 30 (12%) as intermediate-high risk. Among 249 patients who were assigned to the control group, 66 (27%; difference 2.4%; 95% confidence interval [CI], −5.5–10.3%) were low-, 170 (68%; difference 4.4%; 95% CI, −4.2–12.9%) intermediate-low, and 13 (5%; difference 6.8%; 95% CI, 1.6–12.2%) intermediate-high risk. Both in the low-risk and in the intermediate-high risk group of patients, the demographic and clinical characteristics of the patients at baseline did not differ between the two trial (intervention and control) groups (Table 1).
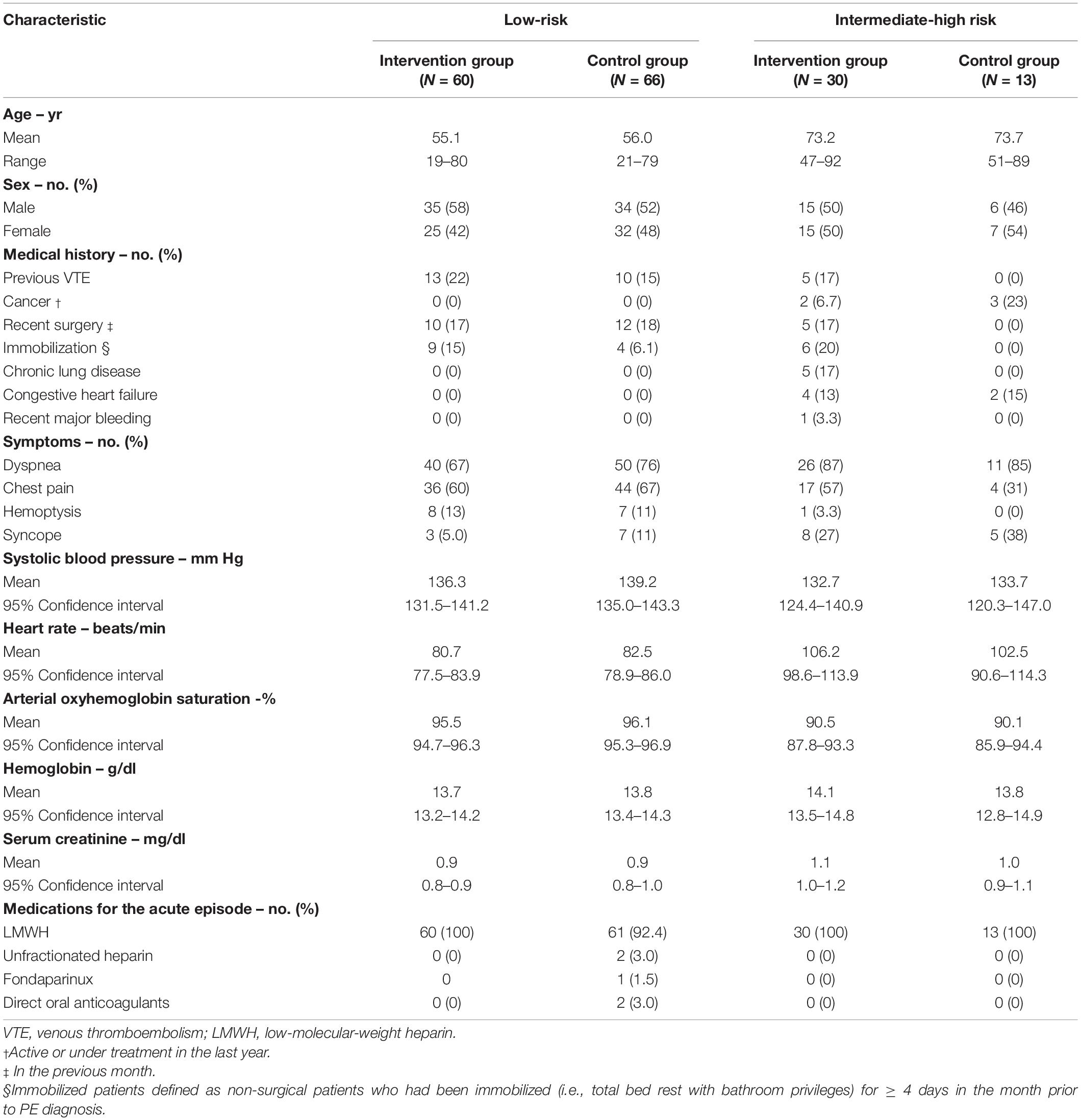
Table 1. Baseline characteristics of the patients.
In the low-risk group according to the ESC criteria, the mean (±SD) time from randomization to the initiation of mobilization was 0.1 ± 0.3 days in the intervention group vs. 1.0 ± 0.7 days in the control group (mean difference, −1.0 days; 95% CI, −0.8 to −1.2 days; P < 0.001). In the intermediate-high risk group, the mean (±SD) time from randomization to the initiation of mobilization was 1.6 ± 0.9 days in the intervention group vs. 1.4 ± 1.0 days in the control group (mean difference, 0.2 days; 95% CI, −0.4 to 0.8 days).
Table 2 summarizes the outcomes for study patients according to the subgroup of risk classification. For patients in the low-risk category, the mean LOS was 2.1 (±0.9) days among those randomized to the intervention group vs. 5.3 (±2.9) days among those randomized to the control group (mean difference, −3.2 days; 95% CI, −2.4 to −3.9 days; P < 0.001) (Figure 1A). For patients in the intermediate-high risk category, the mean LOS was 5.3 (±1.8) days among those randomized to the intervention group vs. 6.5 (±2.5) days among those randomized to the control group (mean difference, −1.2 days; 95% CI, −2.6 to 0.1 days; P = 0.08) (Figure 1B).
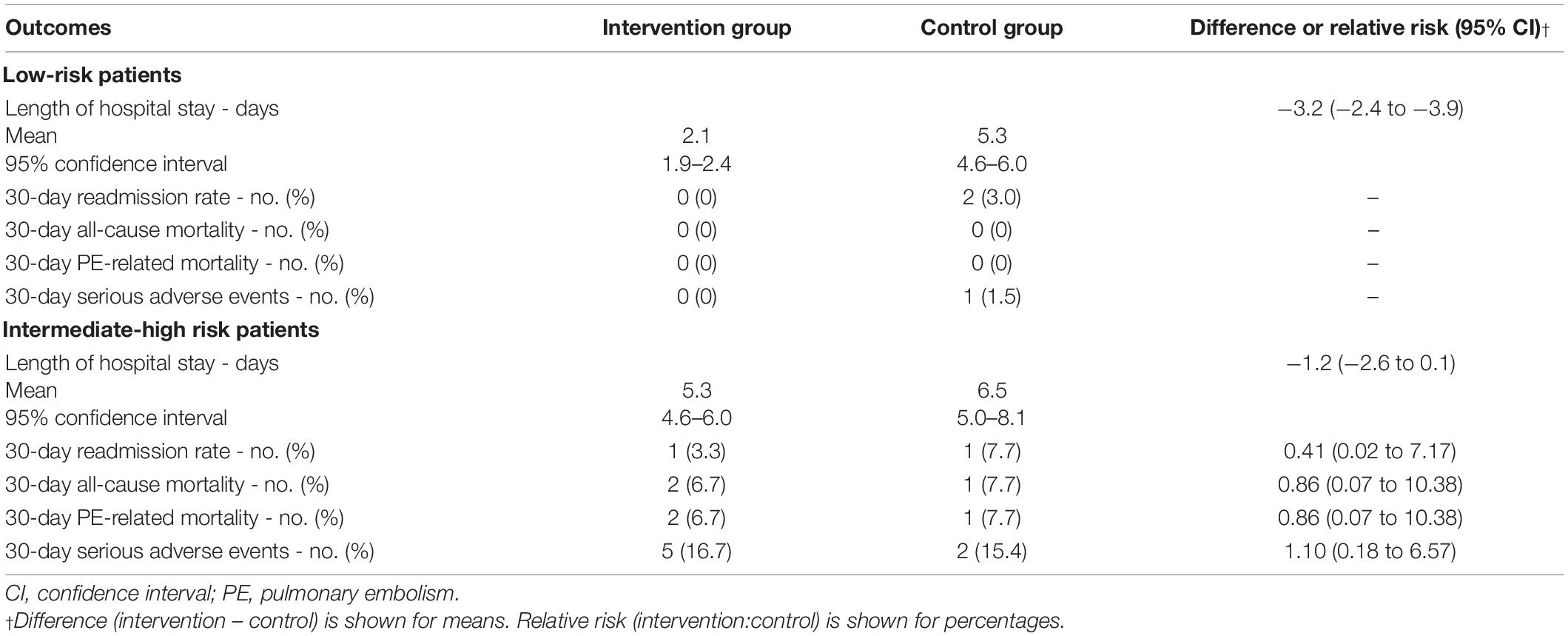
Table 2. Outcomes according to subgroups of risk stratification.
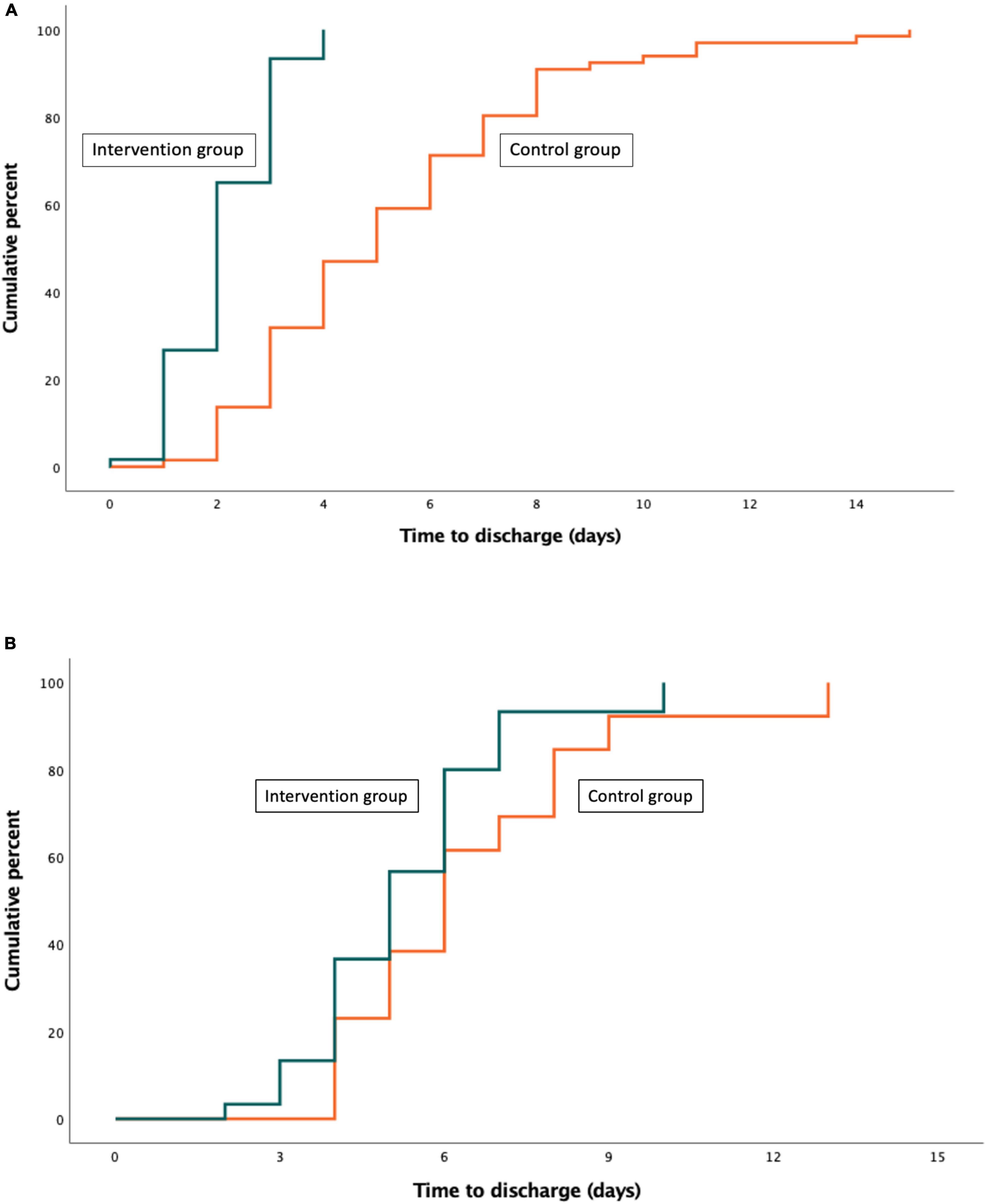
Figure 1. Cumulative frequency distribution curve for the time to discharge of patients in the intervention group as compared with those in the control group. (A) Low-risk (B) Intermediate-high risk.
Thirty-day follow-up data were available for all patients. Among low-risk patients, none of them died during follow-up. Thirty-day all-cause readmission rates were similarly low in the intervention and control groups (0 vs. 3.0%; difference, −3.0%; 95% CI, −11.5 to 4.9%). Thirty-day severe adverse events (0 vs. 1.5%; difference, −1.5%; 95% CI, −9.3 to 6.1%) were not significantly different in the intervention and control groups (Table 2).
Among intermediate-high risk patients, all-cause readmission rates were similar in the intervention and control groups. Thirty-day all-cause (6.7 vs. 7.7%; relative risk, 0.86; 95% CI, 0.07 to 10.38), PE-related mortality (6.7 vs. 7.7%; relative risk, 0.86; 95% CI, 0.07 to 10.38), or severe adverse events (16.7 vs. 15.4%; relative risk, 1.10; 95% CI, 0.18 to 6.57) were not significantly different in the intervention and control groups (Table 2).
This subanalysis of a multicenter randomized trial showed that the use of an standardized prognostic algorithm, compared with usual care, identifies a significantly higher proportion of patients with intermediate-high risk PE. The use of specific criteria for mobilization and discharge was effective and safe in reducing the LOS for subgroups of low- and intermediate-high risk acute PE.
The recent HOME-PE study showed that the HESTIA rule and the sPESI score were similar regarding the proportion of normotensive patients with acute PE treated at home (11). Compared to that trial, IPEP identified fewer patients as low-risk with the sPESI. Possible reasons for this discrepancy are differences in design, hospital settings and patient characteristics. Conversely, the 25% rate of patients with an sPESI of 0 points was similar to the rate in two other recent studies (19, 20). Compared to previous studies (11, 21), our trial used a heart rate less than 100/min as a predefined criterion for discharge. Though the sPESI (which uses a heart rate cutoff of 110/min) has been reported to be helpful to identify low-risk PE patients who might be suitable for home therapy, recent data suggest that a lower heart rate at admission might portend a more favorable prognosis with respect to mortality (22). In fact, none of the low-risk patients in the intervention arm experienced short-term complications. Nevertheless, a prognostic guided management still reduced the LOS by 3 days among low-risk patients, and the mean LOS in the intervention group was not different to that among patients who enrolled the clinical trials of outpatient therapy (11, 21, 22).
An interesting finding of our study is that the use of a standardized prognostic pathway, compared with usual care, identified a significantly higher proportion of patients at intermediate-high risk for short-term complications. This is particularly important since approximately 5% of these patients might deteriorate after diagnosis and initiation of therapy, and require monitoring over the 1st h or days (17). If there was no clinical deterioration within the first 48 h of bed rest, the trial managed intermediate-high risk patients the same way as intermediate-low risk patients (16). With this strategy, the rate of complications was low, and the LOS was reduced by 1.2 days among these intermediate-high risk patients.
Our study has limitations. This was a post-hoc analysis, and risk stratification of patients randomly assigned to usual care was done retrospectively. However, all potentially relevant baseline parameters had been documented in the original case report forms of IPEP. Despite the large number of patients enrolled in the trial, the relatively small sample size of the risk subgroups lowered the statistical power of the study. In addition, IPEP was not formally powered to compare the rate of adverse events in the subgroups of risk, but the very low rate of complications reinforces the validity of our approach. We believe that our results could help to generate clinically relevant hypotheses and provide the background for the design of future trials. Finally, the impact of the overall intervention would likely depend on what represents standard of care in a particular institution. This varies widely within and between countries, depending on resourcing of VTE care and awareness of risk stratification strategies.
In conclusion, this analysis shows that the use of a prognostic assessment and management pathway, compared to usual care, is effective in reducing LOS both in the low- and the intermediate-high risk subgroups. The efficacy and safety of differentiated criteria for mobilization and discharge according to the subgroup of risk stratification are important remaining questions that should be addressed in subsequent studies.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by the Ramon y Cajal Hospital Ethics Committee. The patients/participants provided their written informed consent to participate in this study.
DJ and JL: concept and design. DJ, CR, BP, AP, LJ-P, RL-R, PR-A, AG-O, BB, and JL: acquisition, analysis, or interpretation of data, statistical analysis, and critical revision of the manuscript for important intellectual content. DJ, CR, BB, and JL: drafting of the manuscript. DJ: obtain funding, study supervision, and had full access to all of the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. All authors contributed to the article and approved the submitted version.
This work was funded by the Instituto de Salud Carlos III (PI15/00207) and cofinanced by the European Development Regional Fund “A way to achieve Europe.”
DJ has served as an advisor or consultant for Bayer HealthCare Pharmaceuticals, Boehringer Ingelheim, Bristol-Myers Squibb, Daiichi Sankyo, Leo Pharma, Pfizer, ROVI, and Sanofi; served as a speaker or a member of a speakers’ bureau for Bayer HealthCare Pharmaceuticals, Boehringer Ingelheim, Bristol-Myers Squibb, Daiichi Sankyo, Leo Pharma, ROVI, and Sanofi; received grants for clinical research from Daiichi Sankyo, Sanofi, and ROVI. LJ-P has served as an advisor or consultant for Actelion Pharmaceuticals, Bayer HealthCare Pharmaceuticals, Leo Pharma, Menarini, Pfizer, and ROVI. PR-A has served as an advisor or consultant for Leo Pharma and Viatris; served as a speaker or a member of a speakers’ bureau for Bristol-Myers Squibb, Pfizer, Daiichi Sankyo, ROVI, and Viatris; received grants for clinical research from ROVI. BB is a recipient of the IGNITE Award from the Mary Horrigan Connors Center for Women’s Health and Gender Biology at Brigham and Women’s Hospital and reports that he is a consulting expert, on behalf of the plaintiff, for litigation related to two specific brand models of IVC filters.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
We express our gratitude to S&H Medical Science Service, for their quality control data, logistic, and administrative support.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fcvm.2022.872115/full#supplementary-material
Supplementary Figure 1 | Prognostic assessment and management pathway.
1. Barco S, Mahmoudpour SH, Valerio L, Klok FA, Münzel T, Middeldorp S, et al. Trends in mortality related to pulmonary embolism in the European region, 2000-15: analysis of vital registration data from the WHO mortality database. Lancet Respir Med. (2020) 8:277–87. doi: 10.1016/S2213-2600(19)30354-6
2. Bikdeli B, Wang Y, Jimenez D, Parikh SA, Monreal M, et al. Pulmonary embolism hospitalization, readmission, and mortality rates in US older adults, 1999-2015. JAMA. (2019) 322:574–6. doi: 10.1001/jama.2019.8594
3. Raskob GE, Angchaisuksiri P, Blanco AN, Buller H, Gallus A, Hunt BJ, et al. Thrombosis: a major contributor to global disease burden. Arterioscler Thromb Vasc Biol. (2014) 34:2363–71. doi: 10.1161/atvbaha.114.304488
4. Rahimtoola A, Bergin JD. Acute pulmonary embolism: an update on diagnosis and management. Curr Probl Cardiol. (2005) 30:61–114. doi: 10.1016/j.cpcardiol.2004.06.001
5. Barco S, Valerio L, Ageno W, Cohen AT, Goldhaber SZ, Hunt BJ, et al. Age-sex specific pulmonary embolism-related mortality in the USA and Canada, 2000-18: an analysis of the WHO mortality database and of the CDC multiple cause of death database. Lancet Respir Med. (2020) 9:33–42. doi: 10.1016/S2213-2600(20)30417-3
6. Peacock WF, Singer AJ. Reducing the hospital burden associated with the treatment of pulmonary embolism. J Thromb Haemost. (2019) 17:720–36. doi: 10.1111/jth.14423
7. Dobesh PP. Economic burden of venous thromboembolism in hospitalized patients. Pharmacotherapy. (2009) 29:943–53. doi: 10.1592/phco.29.8.943
8. Fanikos J, Rao A, Seger AC, Carter D, Piazza G, Goldhaber SZ. Hospital costs of acute pulmonary embolism. Am J Med. (2013) 126:127–32. doi: 10.1016/j.amjmed.2012.07.025
9. Fernandez MM, Hogue S, Preblick R, Kwong WJ. Review of the cost of venous thromboembolism. Clinicoecon Outcomes Res. (2015) 7:451–62. doi: 10.2147/ceor.s85635
10. Nielsen A, Poulsen PB, Dybro L, Kloster B, Lorentzen A, Olsen J, et al. Total costs of treating venous thromboembolism: implication of different cost perspectives in a Danish setting. J Med Econ. (2019) 22:1321–7. doi: 10.1080/13696998.2019.1668193
11. Roy PM, Penaloza A, Hugli O, Klok FA, Arnoux A, Elias A, et al. Triaging acute pulmonary embolism for home treatment by Hestia or simplified PESI criteria: the HOME-PE randomized trial. Eur Heart J. (2021) 42:3146–57. doi: 10.1093/eurheartj/ehab373
12. Van Bellen B, Bamber L, Correa de Carvalho F, Prins M, Wang M, Lensing AWA. Reduction in the length of stay with rivaroxaban as a single-drug regimen for the treatment of deep vein thrombosis and pulmonary embolism. Curr Med Res Opin. (2014) 30:829–37. doi: 10.1185/03007995.2013.879439
13. Singer AJ, Thode HC, Peacock WF. Admission rates for emergency department patients with venous thromboembolism and estimation of the proportion of low risk pulmonary embolism patients: a US perspective. Clin Exp Emerg Med. (2016) 3:126–31. doi: 10.15441/ceem.15.096
14. Willich SN, Chuang LH, van Hout B, Gumbs P, Jimenez D, Kroep S, et al. Pulmonary embolism in Europe – burden of illness in relationship to healthcare resource utilization and return to work. Thromb Res. (2018) 170:181–91. doi: 10.1016/j.thromres.2018.02.009
15. Jiménez D, de Miguel-Díez J, Guijarro R, Trujillo-Santos J, Otero R, Barba R, et al. Trends in the management and outcomes of acute pulmonary embolism: analysis from the RIETE registry. J Am Coll Cardiol. (2016) 67:162–70. doi: 10.1016/j.jacc.2015.10.060
16. Jiménez D, Rodríguez C, León F, Jara-Palomares L, López-Reyes R, Ruiz-Artacho P, et al. Randomised controlled trial of a prognostic assessment and management pathway to reduce the length of hospital stay in normotensive patients with acute pulmonary embolism. Eur Respir J. (2021). doi: 10.1183/13993003.00412-2021
17. Konstantinides SV, Meyer G, Becattini C, Bueno H, Geersing GJ, Harjola VP, et al. 2019 ESC guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the European respiratory society (ERS). The task force for the diagnosis and management of acute pulmonary embolism of the European society of cardiology (ESC). Eur Respir J. (2019) 54:1901647. doi: 10.1183/13993003.01647-2019
18. Jiménez D, Aujesky D, Moores L, Gómez V, Lobo JL, Uresandi F, et al. Simplification of the pulmonary embolism severity index for prognostication in patients with acute symptomatic pulmonary embolism. Arch Intern Med. (2010) 170:1383–9. doi: 10.1001/archinternmed.2010.199
19. Quezada CA, Bikdeli B, Villen T, Barrios D, Mercedes E, Leon F, et al. Accuracy and interobserver reliability of the simplified pulmonary embolism severity index versus the Hestia criteria for patients with pulmonary embolism. Acad Emerg Med. (2019) 26:394–401. doi: 10.1111/acem.13561
20. Wells P, Peacock WF, Fermann GJ, Coleman CI, Wang L, Baser O, et al. The value of sPESI for risk stratification in patients with pulmonary embolism. J Thromb Thrombolysis. (2019) 48:149–57. doi: 10.1007/s11239-019-01814-z
21. Aujesky D, Roy PM, Verschuren F, Righini M, Osterwalder J, Egloff M, et al. Outpatient versus inpatient treatment for patients with acute pulmonary embolism: an international, open-label, randomised, non-inferiority trial. Lancet. (2011) 378:41–8. doi: 10.1016/S0140-6736(11)60824-6
Keywords: prognosis, LOS, mortality, pulmonary embolism, complications
Citation: Jiménez D, Rodríguez C, Pintado B, Pérez A, Jara-Palomares L, López-Reyes R, Ruiz-Artacho P, García-Ortega A, Bikdeli B, Lobo JL and the IPEP investigators (2022) Effect of Prognostic Guided Management of Patients With Acute Pulmonary Embolism According to the European Society of Cardiology Risk Stratification Model. Front. Cardiovasc. Med. 9:872115. doi: 10.3389/fcvm.2022.872115
Received: 09 February 2022; Accepted: 08 March 2022;
Published: 12 April 2022.
Edited by:
Avi Leader, Rabin Medical Center, IsraelReviewed by:
Fionnuala Ni Ainle, University College Dublin, IrelandCopyright © 2022 Jiménez, Rodríguez, Pintado, Pérez, Jara-Palomares, López-Reyes, Ruiz-Artacho, García-Ortega, Bikdeli, Lobo and the IPEP investigators. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: David Jiménez, ZGppbWVuZXouaHJjQGdtYWlsLmNvbQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.