 Nayana F. A. Gomes1
Nayana F. A. Gomes1 Vicente Rezende Silva1
Vicente Rezende Silva1 Robert A. Levine2
Robert A. Levine2 William A. M. Esteves1Marildes Luiza de Castro1
William A. M. Esteves1Marildes Luiza de Castro1 Livia S. A. Passos3Jacob P. Dal-Bianco2Alexandre Negrão Pantaleão1Jose Luiz Padilha da Silva4
Livia S. A. Passos3Jacob P. Dal-Bianco2Alexandre Negrão Pantaleão1Jose Luiz Padilha da Silva4 Timothy C. Tan5
Timothy C. Tan5 Walderez O. Dutra6
Walderez O. Dutra6 Elena Aikawa3Judy Hung2
Elena Aikawa3Judy Hung2 Maria Carmo P. Nunes1*
Maria Carmo P. Nunes1*- 1School of Medicine, Hospital das Clínicas, Federal University of Minas Gerais, Belo Horizonte, Brazil
- 2Cardiac Ultrasound Lab, Harvard Medical School, Massachusetts General Hospital, Boston, MA, United States
- 3The Center for Excellence in Vascular Biology, Cardiovascular Medicine, Brigham and Women's Hospital, Harvard Medical School, Boston, MA, United States
- 4Department of Statistics, Federal University of Paraná, Curitiba, Brazil
- 5Department of Cardiology, Blacktown Hospital, University of Western Sydney, Penrith, NSW, Australia
- 6Department of Morphology, Institute of Biological Sciences, Federal University of Minas Gerais, and National Institutes for Science and Technology, Belo Horizonte, Brazil
Introduction: Mitral regurgitation (MR) is the most common valve abnormality in rheumatic heart disease (RHD) often associated with stenosis. Although the mechanism by which MR develops in RHD is primary, longstanding volume overload with left atrial (LA) remodeling may trigger the development of secondary MR, which can impact on the overall progression of MR. This study is aimed to assess the incidence and predictors of MR progression in patients with RHD.
Methods: Consecutive RHD patients with non-severe MR associated with any degree of mitral stenosis were selected. The primary endpoint was a progression of MR, which was defined as an increase of one grade in MR severity from baseline to the last follow-up echocardiogram. The risk of MR progression was estimated accounting for competing risks.
Results: The study included 539 patients, age of 46.2 ± 12 years and 83% were women. At a mean follow-up time of 4.2 years (interquartile range [IQR]: 1.2–6.9 years), 54 patients (10%) displayed MR progression with an overall incidence of 2.4 per 100 patient-years. Predictors of MR progression by the Cox model were age (adjusted hazard ratio [HR] 1.541, 95% CI 1.222–1.944), and LA volume (HR 1.137, 95% CI 1.054–1.226). By considering competing risk analysis, the direction of the association was similar for the rate (Cox model) and incidence (Fine-Gray model) of MR progression. In the model with LA volume, atrial fibrillation (AF) was no longer a predictor of MR progression. In the subgroup of patients in sinus rhythm, 59 had an onset of AF during follow-up, which was associated with progression of MR (HR 2.682; 95% CI 1.133–6.350).
Conclusions: In RHD patients with a full spectrum of MR severity, progression of MR occurs over time is predicted by age and LA volume. LA enlargement may play a role in the link between primary MR and secondary MR in patients with RHD.
Introduction
Rheumatic heart disease (RHD) remains a serious global health concern as the leading cause of cardiovascular death in children and young adults (1, 2). The prevalence of RHD has been rising steadily since 1990, reaching 40.5 million in 2019, and accounting for 306,000 deaths annually as a consequence of severe valvular disease (3). Mitral regurgitation (MR) is the most common valvular abnormality at the early RHD stages, usually associated with ongoing inflammatory rheumatic activity in children (4–7). This pure MR may resolve with effective treatment of the acute carditis and continued prophylactic therapy. In the late time course, MR is often associated with stenosis owing to intrinsic valvular lesions that include fibrosis with retracted leaflets, restricted mobility, and commissural fusion (8).
Although the mechanism by which MR develops in RHD is primarily related to the structural impairment of the mitral valve (MV) apparatus (8), longstanding volume overload with left-sided chamber alterations may trigger the development of secondary MR (9). Moreover, in the presence of atrial fibrillation (AF), which often occurs in patients with rheumatic MV disease, MR may also arise as a consequence of left atrial (LA) enlargement and mitral annular dilatation. Functional MR in patients with AF has been increasingly recognized (10–12). However, whether mitral annular dilatation causes MR in patients without left ventricular dysfunction remains controversial.
There is a growing awareness that MR continues to progress over time as the increased volume load on the left ventricle and LA results in geometric changes that lead to a further increase in the severity of MR (13, 14). Additionally, the most common pattern of MV pathology in middle-aged adults with RHD is mixed MV disease, which begets LA enlargement (8, 15). Taken together, both primary MR and secondary MR may coexist in the setting of RHD, which may have an impact on MR progression. However, because of the paucity of data available on the progression of rheumatic MR, the underlying mechanisms are not certain.
Previous studies addressing the progression of MR in adult patients with RHD have focused mainly on MR following valvuloplasty (16–20). In this context, the progression and prognosis are variables depending on the mechanism by which MR develops. We previously showed that MR originated at the site of commissural split or at the central orifice of the valve and remains stable over time. On the other hand, MR due to leaflet tearing at central scallop location or subvalvular damage results in severe adverse hemodynamics that require immediate surgery (20). However, there is a lack of studies on the natural history of rheumatic MR without intervention, as it requires large cohorts of patients with repeated echocardiograms and long-term follow-up. To fill these gaps of knowledge, we sought to investigate the incidence and predictors of MR progression in a substantial population of patients with RHD.
Methods
Study Population
Patients were recruited prospectively from a tertiary center for heart valve disease among those routinely referred for management of RHD from 2011 to 2021. Patients with rheumatic MV disease with trivial, mild, or moderate MR associated with any degree of mitral stenosis based on the presence of typical rheumatic features by echocardiography criteria (21) were initially eligible for the study (Study flow is shown in Figure 1). Exclusion criteria included severe MR at baseline or following percutaneous mitral valvuloplasty, associated significant aortic valve disease, and no echocardiographic assessment of MR at last follow-up. Among 694 patients initially eligible for the study, 539 fulfilled the inclusion criteria and were enrolled.
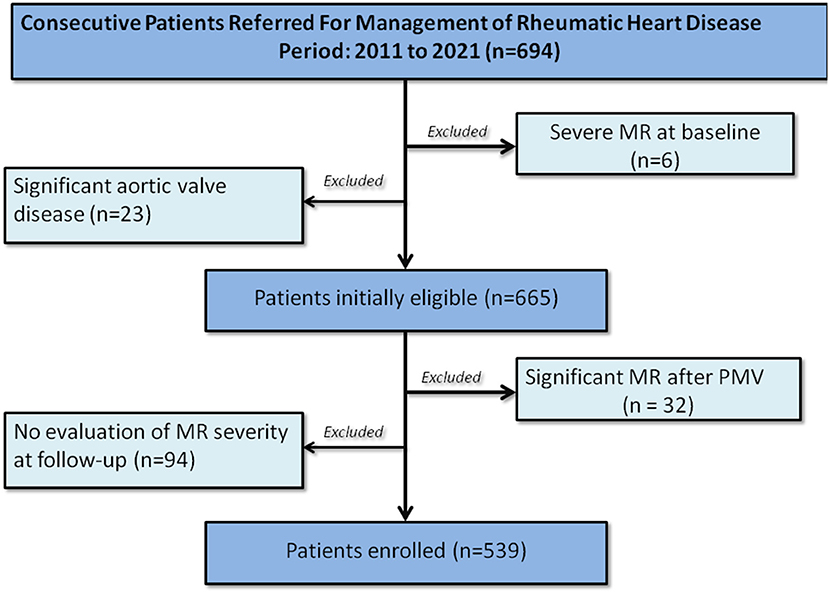
Figure 1. Study population.
Information on demographic data, functional capacity, right-sided heart failure, and current medications was obtained at baseline. AF was diagnosed based on a history of permanent AF, supported by a past 12-lead ECG. A diagnosis of new-onset AF in patients with sinus rhythm at the time of enrollment in the study was confirmed by a 12-lead ECG. All patients gave written informed consent, and the study protocol was approved by the UFMG institutional ethics committee.
Echocardiography
Comprehensive two-dimensional (2D) and Doppler echocardiographic examinations were performed in all patients at baseline and at follow-up using commercially available echocardiography machines. Measures of left ventricular dimensions and function were assessed as recommended (22). MR was graded as none/trace, mild, moderate, or severe by using an integrative approach (23). Parameters used to grade MR included the vena contracta width, regurgitant volume, and effective orifice area, qualitative assessment of the color flow jet, and, when available, the pulmonary venous flow signal. MV area was measured using direct planimetry. Peak and mean transmitral diastolic pressure gradients were measured from Doppler profiles recorded in the apical four-chamber view. The presence and severity of tricuspid regurgitation and systolic pulmonary artery pressure were evaluated according to the guidelines (20). LA volume was assessed by the biplane area-length method from apical 2- and 4-chamber views.
Definition of MR Progression
Progression of MR was defined as an increase of one grade in MR severity from baseline to the last follow-up echocardiogram. Patients in whom MR did not progress but died or underwent MV replacement were censored at the time of the events and also analyzed considering these events as competing risks (24). Patients who underwent percutaneous mitral valvuloplasty were censored at the time of the procedure and post-procedural MR was not considered as progression.
Statistical Analysis
Categorical variables were expressed as numbers and percentages and were compared by using chi-square or Fisher exact tests as appropriate. Continuous data were expressed as mean ± SD and were compared by using unpaired Student's t-test or Mann-Whitney test as appropriate.
The incidence rate of MR progression was calculated by dividing the number of progression by the person-years of follow-up calculated from the baseline until either the date of death or MV replacement or last follow-up echocardiogram.
Predictors of MR progression were assessed using two regression models. The first was the Cox proportional hazards model in which patients were censored at the time of death or MV replacement if it was not preceded by MR progression. The second model was the Fine-Gray competing risk model in which MR progression was the primary event and death or MV replacement was the competing risk (24) that may prevent progression of the valve regurgitation. The estimated regression coefficients for each variable were compared between the two models to assess differences in the direction of their association with the rate of MR progression (derived from the Cox model) vs. its incidence (derived from the Fine-Gray model) (24). Schoenfeld residuals were used to check the proportional hazards assumption.
Long-term MR progression according to cardiac rhythm was estimated by the Kaplan-Meier method and compared by the log-rank test. Statistical analysis was performed using the Statistical Package for Social Sciences for Windows, version 22.0 (SPSS Inc., Chicago, IL, USA) and R for Statistical Computing version 3.6.3 (R Foundation, Vienna, Austria).
Results
Patient Characteristics
Our final cohort consisted of 539 patients, age of 46.2 ± 12 years, and 454 patients were women (83%). Baseline demographic and clinical characteristics according to MR progression are summarized in Table 1. At baseline, trivial MR was detected in 80 patients (15%), mild MR in 416 (77%), and moderate in 43 (8%). Most of the patients were in the New York Heart Association (NYHA) classes I and II (64%), whereas 194 (36%) patients were in NYHA classes III and IV at presentation. One hundred and sixteen patients (22%) were presented with right-sided heart failure. The medications most frequently used were beta-blockers (74% of cases) followed by diuretics (69% of cases).
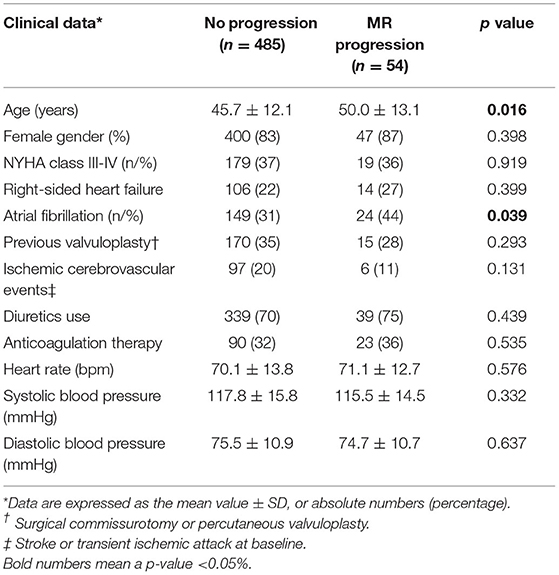
Table 1. Demographic and clinical characteristics of the study population stratified by mitral regurgitation (MR) progression.
In the overall population, the left atrium was severely dilated, with a mean volume of 54 ml/m2 in the patients in sinus rhythm compared with 74 ml/m2 in AF (p < 0.001). One hundred and thirty-five patients (25%) had a history of hypertension and 3% of diabetes. The majority of patients had no comorbidities.
Regarding baseline echocardiographic characteristics, patients who progressed had larger left ventricular chamber dimensions, LA volume, and lower ejection fraction. Of note, the severity of the associated mitral stenosis was similar between the patients with a mean valve area of 1.1 cm2 in those patients who progressed or did not. Baseline echocardiographic features according to MR progression are summarized in Table 2.
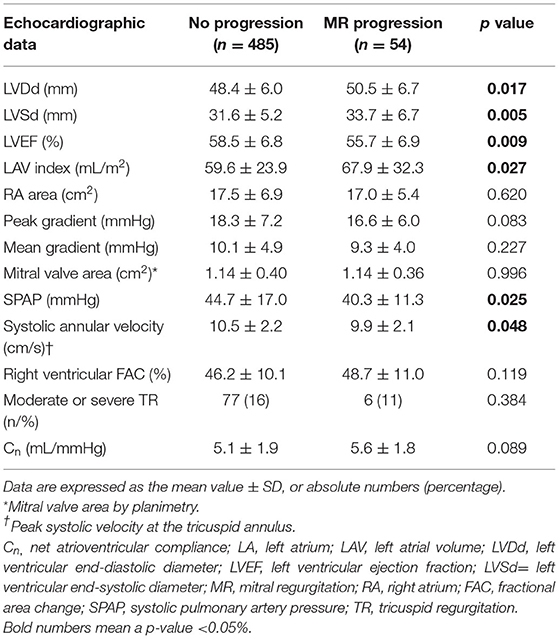
Table 2. Baseline echocardiographic characteristics of the study population stratified by MR progression.
At a mean follow-up time of 4.2 years (interquartile range [IQR]: 1.2–6.9 years), 54 patients (10%) displayed MR progression. The majority of the patients progressed from mild-to-moderate MR (n = 42, 77.8%), mild-to-severe (n = 6, 11.1%), trivial MR-to-moderate (n = 3, 5.5%), and the other 3 patients (5.5%) from moderate-to-severe MR. Patients who progressed MR were older compared with those who did not progress. Permanent AF at baseline was found in 173 patients, more frequent in patients who had MR progression.
Predictors of MR Progression
The overall incidence of MR progression was 2.4 per 100 patient-years. During the follow-up, 120 patients underwent cardiac surgery for MV replacement and 27 patients died, being 23 cardiovascular-related and four non-cardiovascular-related deaths (Figure 2). In the Cox proportional hazard regression model, older age, the presence of AF, and larger LA volume were univariately associated with MR progression. Interestingly, prior mitral valvuloplasty, i.e., either percutaneous or surgical intervention, was inversely associated with MR progression. The severity of tricuspid regurgitation was not associated with MR progression (Table 3).
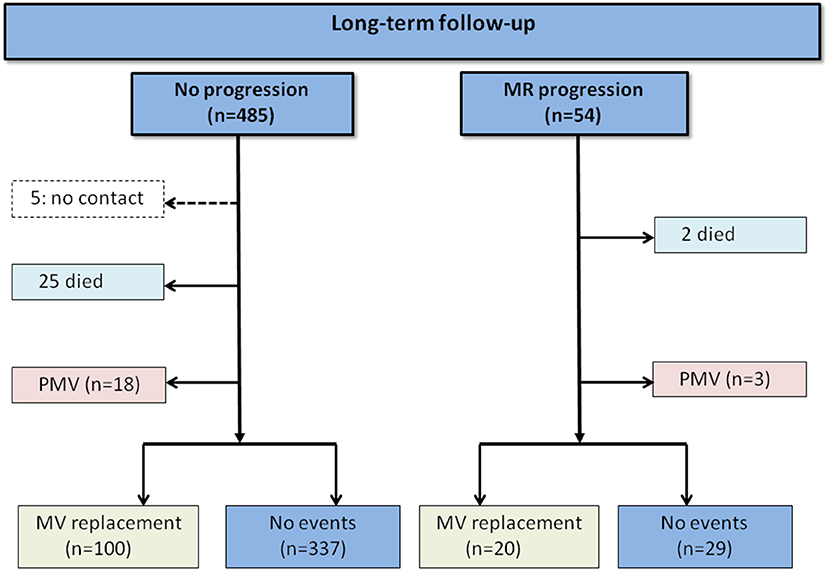
Figure 2. Long-term follow-up of patients with rheumatic heart disease (RHD).
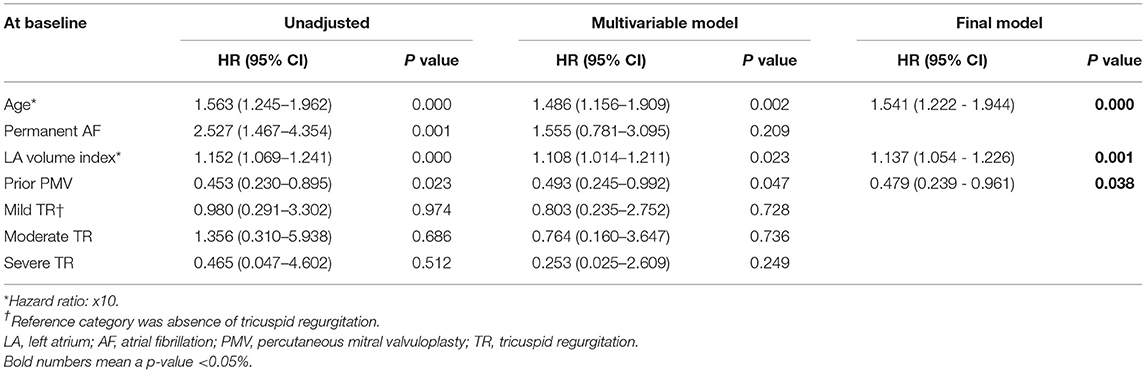
Table 3. Clinical and echocardiographic characteristics associated with MR progression in patients with RHD: Cox regression model.
As death and MV replacement constitute a competing risk that may preclude the natural progression of MR, time-to-event analyses were performed considering competing risks. In the Cox proportional hazard regression model, MR progression was the primary outcome, and patients who underwent MV replacement or died were censored. In the Fine-Gray model, MV replacement and death were analyzed as competing events (Table 4). In the multivariable models, age and LA volume were independent predictors of MR progression during the follow-up (Tables 3, 4). In the model with LA volume, AF was no longer a predictor of MR progression. The severity of TR regurgitation was included in the model as this entity is also associated with AF and right atrial dilation. For all variables included, the direction of the association was similar for the rate (Cox model) and incidence (Fine-Gray model) of MR progression. The hazard ratios of each predictor comparing Cox and Fine-Gray models are shown in Figure 3.
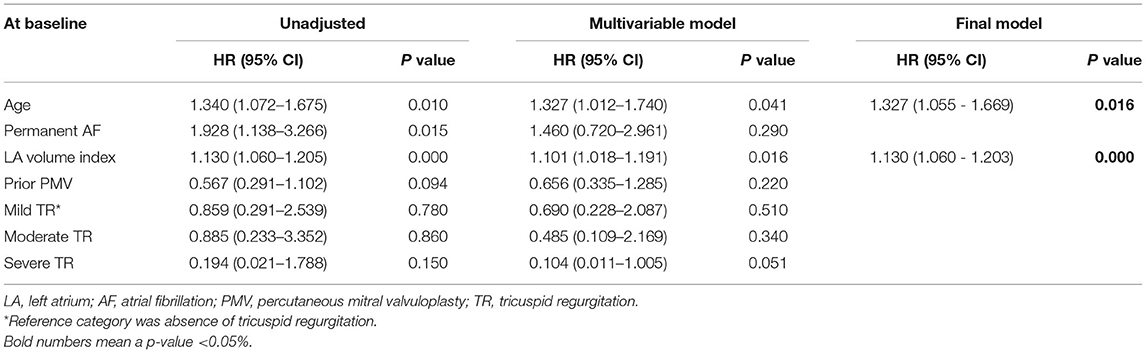
Table 4. Clinical and echocardiographic characteristics associated with MR progression in patients with RHD: Fine-Gray model.
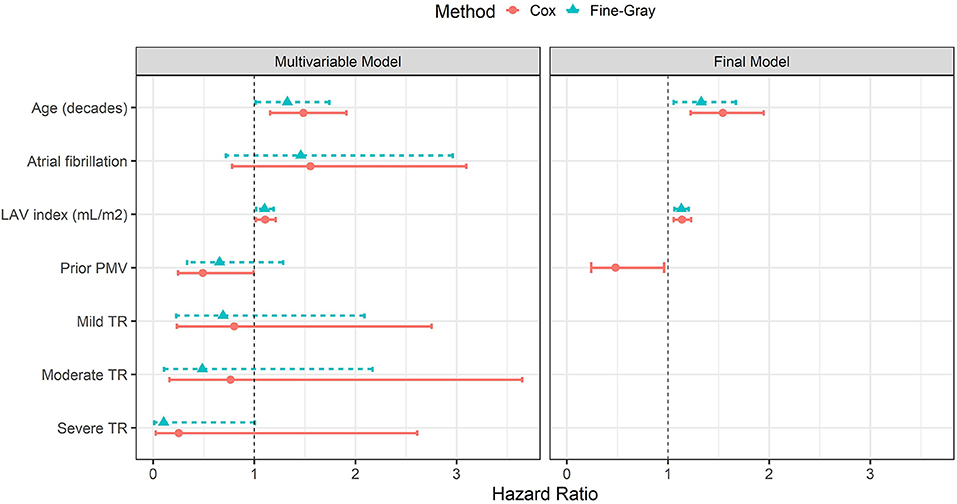
Figure 3. Multivariable predictive models for prediction of mitral regurgitation (MR) progression in patients with rheumatic heart disease (RHD). Cox proportional hazards model considering mitral regurgitation (MR) progression as the primary event and the Fine-Gray model analyzing death and mitral valve replacement as a competing event.
We performed a subgroup analysis stratifying according to the MR grade at the follow-up. To do so, we categorized MR progression in moderate (n = 45) and severe (n = 9), irrespective of the MR grade at baseline. By considering only severe MR in the Cox model, age was the most important predictor of progression (hazard ratio [HR] 2.592; 95% 1.357–4.952), and the effect of LA volume was attenuated (HR 1.121; 95% CI 0.807–1.557). However, the small number of patients in the severe MR category limits this analysis.
In the subset of patients in sinus rhythm, 59 patients showed an onset of AF during the course of the follow-up, which was associated with MR progression (HR 2.682; 95% CI 1.133–6.350). Of note, the risk of MR progression was higher in patients with permanent AF at enrollment (HR 4.549; 95% CI 2.148–9.631) compared with those who had new-onset of AF during the follow-up (HR 2.447; 95% CI 1.035–5.788; Figure 4). As expected, patients with new-onset of AF displayed larger LA volume compared with the patients who remained in sinus rhythm (61 and 54 ml/m2, respectively).
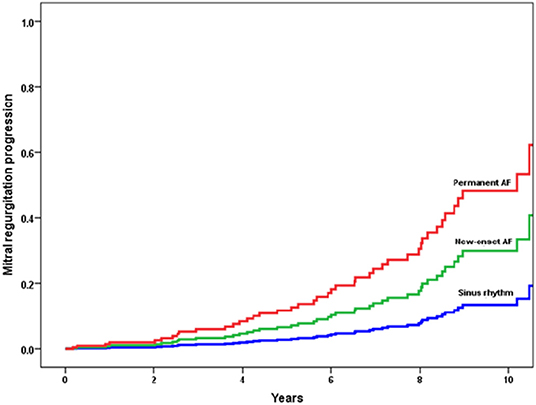
Figure 4. Incidence of mitral regurgitation (MR) progression according to cardiac rhythm. Patients who had sinus rhythm at baseline but with a new-onset of atrial fibrillation during the follow-up were at risk for progression with a hazard ratio of 2.447 (95% CI 1.035–5.788). Patients with permanent atrial fibrillation were at the highest risk for progression with a hazard ratio of 4.459 (95% CI 2.148–9.631) when compared with patients in sinus rhythm.
Discussion
The natural history of MR varies according to the time course of RHD. While MR in acute carditis may resolve with the control of inflammatory changes, MR at the late disease stages tends to progress over time, which in turn leads to clinical complications (25, 26). The present study showed that in RHD, progression of MR occurs over time with the overall incidence of 2.4 events of progression per 100 patient-years. Age and LA enlargement were major independent determinants of the progression of MR. New-onset AF during the course of the follow-up was associated with MR progression. The study accounts for competing risks to conduct time-to-event analyses appropriately of MR incidence in RHD patients with mixed MV disease.
Primary MR Progression
The severity of primary MR may increase over time as a consequence of the adverse remodeling of the left atrium and ventricle (27). The degree of regurgitation is an essential determinant of the hemodynamic changes, remodeling of left-sided chambers, and poor outcome. A previous study that includes primary MR, mainly valve prolapse, showed that progression of MR is variable and determined by the progression of lesions or mitral annulus size (28). The most important determinant of marked aggravation of MR is the occurrence of a new flail leaflet followed by an increase in annular diameter, which results in reduced leaflet coaptation. Another study evaluating patients with MV prolapse demonstrated that only mitral annular diameter is a predictor of progression to severe MR (29).
Data on MR progression in patients with RHD are scarce and limited to acute carditis or MR related to percutaneous valve intervention (8, 16–18, 20, 25). In the setting of RHD, given the presence of mixed MV disease, mitral annular enlargement may be induced by both left ventricular and atrial enlargement, which contribute to aggravate the MR severity over time. However, as we included only non-severe MR, the impact of volume overload on the adverse remodeling of the left ventricle might be lower than in severe MR. Additionally, combined valve disease often occurs in RHD and patients may undergo valve replacement for stenosis as the predominant lesion, which influences the natural history of MR progression in the native valve. To address this issue, MV replacement was considered a competing risk that may preclude the occurrence of progression, avoiding biased estimates of progression risk with traditional time-to-event methods (30). The Fine-Gray model constitutes a tool that determines a sub-distribution in a correct way of the role of risk factors, thus taking into account the competition between pairs of events (31).
The significant regurgitant lesion in rheumatic MV has long been considered merely an anatomic variant of its stenotic counterpart, in which retraction of scarred valve leaflets has disrupted the integrity of the mitral seal (8, 32, 33). As the chronic rheumatic process is usually accompanied by at least some fusion of mitral commissures, the relative prevalence of pure regurgitation among hemodynamically severe MV lesions has consistently been reported to be low (8, 34). In agreement with the literature, our population with mixed MV disease, characteristics of pure regurgitation, and pure stenosis were overlapped, which makes it difficult to analyze the progression of the regurgitant lesion alone (13).
LA Enlargement in MR: The Link Between Primary and Secondary MR
In patients with primary MR, secondary MR can also develop because LA dilation leads to mitral enlargement of the MV annulus. In this context, the overlapping of secondary MR may contribute to further overall progression of the regurgitation. Indeed, there are instances in which both primary MR and secondary MR are present (13).
Left atrial enlargement in MR has been reported either as a compensatory mechanism with the aim to reduce atrial and pulmonary pressure or, conversely, as a marker of poor prognosis (35). Atrial enlargement is accompanied by chronic inflammatory changes, cellular hypertrophy, and wall fibrosis, which leads to reduced compliance and increased LA pressure and risk of AF (36). This association supports the poor prognosis of patients with LA enlargement due to primary MR (36–38).
Although the value of LA enlargement in predicting heart failure and death in the general population has been reported, in primary MR, there are limited data on its prognostic implications (35). A multicenter study showed that LA diameter is an independent predictor of survival in patients with chronic MR due to flail leaflets in sinus rhythm under medical treatment. The association between LA diameter ≥55 mm and the outcome is independent of symptoms or left ventricular dysfunction (37). Another study included 305 patients with MV prolapse and sinus rhythm who underwent MV repair. After a mean follow-up period of 8 years, patients with an area of >30 cm2 presented a 2-fold increase in the risk of mortality when compared with those with an area of <25 cm2. LA enlargement was a predictor of long-term mortality after surgery for valve repair in sinus rhythm patients (39).
In patients with rheumatic MV disease, a chronic pressure-volume overload on the left atrium leads to a range of adaptive processes that include LA remodeling (40), which encompasses changes in atrial size, function, and shape. LA enlargement also reflects the intrinsic compliance of the left atrium, risk of subsequent AF, and overall disease severity. In the presence of mixed MV disease, LA is affected by both stenosis and regurgitation, which aggravates its remodeling over time with the progression of MR as a consequence of the mitral annulus size. Subsequent progression of primary rheumatic lesions should also be considered. Turbulent flow drives valvular tissue injury, continuously stimulating inflammatory processes and mechanical trauma, which contribute to perpetuate the valvular damage (8). Additionally, patients with RHD often have associated AF, which may contribute to the progression of LA and annular dilation thus increasing the severity of MR. Indeed, there are cumulative pieces of evidence using three-dimensional (3D) echocardiography showing that significant secondary MR can sometimes occurs in AF patients with dilatation of mitral annulus and left atrium. In the present study, 32% of the patients had permanent AF at enrollment and 11% developed AF during the follow-up. Regardless of the cardiac rhythm, LA enlargement was an important predictor of MR progression.
Study Limitation
Despite providing relevant clinical information on LA remodeling and MV involvement in RHD, this study has some limitations. First, 3D analysis of MV accurately assesses morphology and regurgitation mechanisms. Leaflet remodeling, rather than crude annular dilatation, is associated with the severity of functional MR in patients with AF (41). In our study, mitral annulus by 3D was not assessed and LA dilation was considered a surrogate for mitral annulus enlargement. However, the previous study with 3D-transesophageal echocardiography showed that LA volume is the main predictor of mitral annulus enlargement (42). Moreover, large patient population is required to determine MR progression and 3D analysis of MV in all patients is a challenge. Second, assessment of LA function using novel parameters that include LA strain may be able to detect the onset of decreasing LA compliance and contractile dysfunction that is known to occur in more advanced diseases. In our study, LA function was not assessed. Indeed, atrial disease and remodeling form the basis of the atrial cardiopathy, which plays a critical role in the pathogenesis of AF (43). Third, LV volume and pressure were not measured directly in our study, which influence the amount of MR for a given lesion under different hemodynamic conditions (44).
Finally, the majority of our patients was progressed to moderate MR, which may not have an impact on clinical outcomes. However, the complex nature of mixed MV disease in the setting of RHD makes it necessary to consider all available data to reach a final management decision (13).
Conclusions
In patients with RHD with a full spectrum of MR severity, progression of MR occurs over time predicted by age and LA volume, corrected by competing risks. LA enlargement may play a role in the link between primary MR and secondary MR in patients with RHD. Assessment of MR progression may provide important insight into the long-term consequences of the disease and the rationale for patient management.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics Statement
The studies involving human participants were reviewed and approved by UFMG Institutional Ethics Committee (No. 3.586.751). The patients/participants provided their written informed consent to participate in this study.
Author Contributions
NG, VS, and MN: conception and design of the research. WE, MC, LP, and AP: acquisition of data. JS and MN: analysis and interpretation of data and statistical analysis. RL and WD: obtaining financing. NG and MN: writing of the manuscript and responsible for the overall content as guarantors. RL, JD-B, EA, TT, and JH: critical revision of the manuscript for intellectual content. All authors contributed to the article and approved the submitted version.
Funding
This study was partly funded by grants from CAPES, FAPEMIG, and CNPq (Project number 431138/2018-4), Brazil. MN and WD are CNPq scholarship recipients. EA and RL labs are funded by the National Institutes of Health grant R01 HL 141917.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Watkins DA, Johnson CO, Colquhoun SM, Karthikeyan G, Beaton A, Bukhman G, et al. Global, regional, and national burden of rheumatic heart disease, 1990-2015. N Engl J Med. (2017) 377:713–22. doi: 10.1056/NEJMoa1603693
2. Watkins DA, Beaton AZ, Carapetis JR, Karthikeyan G, Mayosi BM, Wyber R, et al. Rheumatic heart disease worldwide: JACC scientific expert panel. J Am Coll Cardiol. (2018) 72:1397–416. doi: 10.1016/j.jacc.2018.06.063
3. Roth GA, Mensah GA, Johnson CO, Addolorato G, Ammirati E, Baddour LM, et al. Global burden of cardiovascular diseases and risk factors, 1990–2019: update from the GBD 2019 study. J Am Coll Cardiol. (2020) 76:2982–3021.
4. Saxena A. Echocardiographic diagnosis of chronic rheumatic valvular lesions. Glob Heart. (2013) 8:203–12. doi: 10.1016/j.gheart.2013.08.007
5. Nunes MCP, Sable C, Nascimento BR, Lima EM, da Silva JLP, Diamantino AC, et al. Simplified echocardiography screening criteria for diagnosing and predicting progression of latent rheumatic heart disease. Circ Cardiovasc Imaging. (2019) 12:e007928. doi: 10.1161/CIRCIMAGING.118.007928
6. Leal M, Passos LSA, Guarconi FV, Aguiar JMS, Silva R, Paula TMN, et al. Rheumatic heart disease in the modern era: recent developments and current challenges. Rev Soc Bras Med Trop. (2019) 52:e20180041. doi: 10.1590/0037-8682-0041-2019
7. Passos LS, Nunes MCP, Aikawa E. Rheumatic heart valve disease pathophysiology and underlying mechanisms. Front Cardiovascular Med. (2021) 7:411. doi: 10.3389/fcvm.2020.612716
8. Marcus RH, Sareli P, Pocock WA, Barlow JB. The spectrum of severe rheumatic mitral valve disease in a developing country: correlations among clinical presentation, surgical pathologic findings, and hemodynamic sequelae. Ann Intern Med. (1994) 120:177–83. doi: 10.7326/0003-4819-120-3-199402010-00001
9. Chaput M, Handschumacher MD, Tournoux F, Hua L, Guerrero JL, Vlahakes GJ, et al. Mitral leaflet adaptation to ventricular remodeling: occurrence and adequacy in patients with functional mitral regurgitation. Circulation. (2008) 118:845–52. doi: 10.1161/CIRCULATIONAHA.107.749440
10. Kagiyama N, Mondillo S, Yoshida K, Mandoli GE, Cameli M. Subtypes of atrial functional mitral regurgitation: imaging insights into their mechanisms and therapeutic implications. JACC Cardiovascular imaging. (2020) 13:820–35. doi: 10.1016/j.jcmg.2019.01.040
11. Deferm S, Bertrand PB, Verbrugge FH, Verhaert D, Rega F, Thomas JD, et al. Atrial functional mitral regurgitation: JACC review topic of the week. J Am Coll Cardiol. (2019) 73:2465–76. doi: 10.1016/j.jacc.2019.02.061
12. Kim D-H, Heo R, Handschumacher MD, Lee S, Choi Y-S, Kim K-R, et al. Mitral valve adaptation to isolated annular dilation: insights into the mechanism of atrial functional mitral regurgitation. JACC: Cardiovascular Imaging. (2019) 12:665–77. doi: 10.1016/j.jcmg.2017.09.013
13. Members WC, Otto CM, Nishimura RA, Bonow RO, Carabello BA, Erwin JP III, et al. 2020 ACC/AHA guideline for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J Am Coll Cardiol. (2021) 77:e25–e197.
14. Neilan TG, Ton-Nu T-T, Kawase Y, Yoneyama R, Hoshino K, Del Monte F, et al. Progressive nature of chronic mitral regurgitation and the role of tissue Doppler-derived indexes. Am J Physiol-Heart and Circulatory Physio. (2008) 294:H2106–H11. doi: 10.1152/ajpheart.01128.2007
15. Sliwa K, Carrington M, Mayosi BM, Zigiriadis E, Mvungi R, Stewart S. Incidence and characteristics of newly diagnosed rheumatic heart disease in urban African adults: insights from the heart of Soweto study. Eur Heart J. (2010) 31:719–27. doi: 10.1093/eurheartj/ehp530
16. Kim MJ, Song JK, Song JM, Kang DH, Kim YH, Lee CW, et al. Long-term outcomes of significant mitral regurgitation after percutaneous mitral valvuloplasty. Circulation. (2006) 114:2815–22. doi: 10.1161/CIRCULATIONAHA.106.658088
17. Padial LR, Freitas N, Sagie A, Newell JB, Weyman AE, Levine RA, et al. Echocardiography can predict which patients will develop severe mitral regurgitation after percutaneous mitral valvulotomy. J Am Coll Cardiol. (1996) 27:1225–31. doi: 10.1016/0735-1097(95)00594-3
18. Hernandez R, Banuelos C, Alfonso F, Goicolea J, Fernandez-Ortiz A, Escaned J, et al. Long-term clinical and echocardiographic follow-up after percutaneous mitral valvuloplasty with the Inoue balloon. Circulation. (1999) 99:1580–6. doi: 10.1161/01.CIR.99.12.1580
19. Herrmann HC, Lima JA, Feldman T, Chisholm R, Isner J, O'Neill W, et al. Mechanisms and outcome of severe mitral regurgitation after Inoue balloon valvuloplasty. J Am Coll Cardiol. (1993) 22:783–9. doi: 10.1016/0735-1097(93)90191-3
20. Nunes MCP, Levine RA, Braulio R, Pascoal-Xavier MA, Elmariah S, Gomes NF, et al. Mitral regurgitation after percutaneous mitral valvuloplasty: insights into mechanisms and impact on clinical outcomes. Cardiovascular Imaging. (2020) 13:2513–26. doi: 10.1016/j.jcmg.2020.07.020
21. Remenyi B, ElGuindy A, Smith SC Jr, Yacoub M, Holmes DR Jr. Valvular aspects of rheumatic heart disease. Lancet. (2016) 387:1335–46. doi: 10.1016/S0140-6736(16)00547-X
22. Lang RM, Badano LP, Mor-Avi V, Afilalo J, Armstrong A, Ernande L, et al. Recommendations for cardiac chamber quantification by echocardiography in adults: an update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J Am Soc Echocardiogr. (2015) 28:1–39 e14. doi: 10.1016/j.echo.2014.10.003
23. Zoghbi WA, Adams D, Bonow RO, Enriquez-Sarano M, Foster E, Grayburn PA, et al. Recommendations for noninvasive evaluation of native valvular regurgitation: a report from the American Society of Echocardiography developed in collaboration with the Society for Cardiovascular Magnetic Resonance. J Am Society of Echocardiog. (2017) 30:303–71. doi: 10.1016/j.echo.2017.01.007
24. Zhang Z. Survival analysis in the presence of competing risks. Ann Transl Med. (2017) 5. doi: 10.21037/atm.2016.08.62
25. Massell BF, Chute CG, Walker AM, Kurland GS. Penicillin and the marked decrease in morbidity and mortality from rheumatic fever in the United States. N Engl J Med. (1988) 318:280–6. doi: 10.1056/NEJM198802043180504
26. ToMPKINS DG, Boxerbaum B, Liebman J. Long-term prognosis of rheumatic fever patients receiving regular intramuscular benzathine penicillin. Circulation. (1972) 45:543–51. doi: 10.1161/01.CIR.45.3.543
27. Gaasch WH, Meyer TE. Left ventricular response to mitral regurgitation: implications for management. Circulation. (2008) 118:2298–303. doi: 10.1161/CIRCULATIONAHA.107.755942
28. Enriquez-Sarano M, Basmadjian A-J, Rossi A, Bailey KR, Seward JB, Tajik AJ. Progression of mitral regurgitation: a prospective Doppler echocardiographic study. J Am Coll Cardiol. (1999) 34:1137–44. doi: 10.1016/S0735-1097(99)00313-7
29. Ma JI, Igata S, Strachan M, Nishimura M, Wong DJ, Raisinghani A, et al. Predictive factors for progression of mitral regurgitation in asymptomatic patients with mitral valve prolapse. Am J Cardiol. (2019) 123:1309–13. doi: 10.1016/j.amjcard.2019.01.026
30. Abdel-Qadir H, Fang J, Lee DS, Tu JV, Amir E, Austin PC, et al. Importance of considering competing risks in time-to-event analyses: application to stroke risk in a retrospective cohort study of elderly patients with atrial fibrillation. Circ Cardiovasc Qual Outcomes. (2018) 11:e004580. doi: 10.1161/CIRCOUTCOMES.118.004580
31. Feakins BG, McFadden EC, Farmer AJ, Stevens RJ. Standard and competing risk analysis of the effect of albuminuria on cardiovascular and cancer mortality in patients with type 2 diabetes mellitus. Diagn Progn Res. (2018) 2:13. doi: 10.1186/s41512-018-0035-4
32. Olson LJ, Subramanian R, Ackermann DM, Orszulak TA, Edwards WD, editors. Surgical pathology of the mitral valve: a study of 712 cases spanning 21 years. Mayo Clinic Proceedings. Elsevier. (1987). doi: 10.1016/S0025-6196(12)61522-5
33. Selzer A, Cohn KE. Natural history of mitral stenosis: a review. Circulation. (1972) 45:878–90. doi: 10.1161/01.CIR.45.4.878
34. Waller BF, Morrow AG, Maron BJ, Del Negro AA, Kent KM, McGrath FJ, et al. Etiology of clinically isolated, severe, chronic, pure mitral regurgitation: analysis of 97 patients over 30 years of age having mitral valve replacement. Am Heart J. (1982) 104:276–88. doi: 10.1016/0002-8703(82)90204-6
35. Messika-Zeitoun D, Bellamy M, Avierinos J-F, Breen J, Eusemann C, Rossi A, et al. Left atrial remodelling in mitral regurgitation—methodologic approach, physiological determinants, and outcome implications: a prospective quantitative Doppler-echocardiographic and electron beam-computed tomographic study. Eur Heart J. (2007) 28:1773–81. doi: 10.1093/eurheartj/ehm199
36. Munoz-Guijosa C, Berastegui E, Bayes-Genis A. Left atrial dimension, primary mitral regurgitation, and the need of early surgery. Cardiology. (2019) 143:239–41. doi: 10.1159/000500447
37. Rusinaru D, Tribouilloy C, Grigioni F, Avierinos JF, Suri RM, Barbieri A, et al. Left atrial size is a potent predictor of mortality in mitral regurgitation due to flail leaflets: results from a large international multicenter study. Circulation: Cardiovascular Imaging. (2011) 4:473–81. doi: 10.1161/CIRCIMAGING.110.961011
38. Reed D, Abbott RD, Smucker ML, Kaul S. Prediction of outcome after mitral valve replacement in patients with symptomatic chronic mitral regurgitation. The importance of left atrial size. Circulation. (1991) 84:23–34. doi: 10.1161/01.CIR.84.1.23
39. Szymanski C, Bohbot Y, Rusinaru D, Touati G, Tribouilloy C. Impact of preoperative left atrial dimension on outcome in patients in sinus rhythm undergoing surgical valve repair for severe mitral regurgitation due to mitral valve prolapse. Cardiology. (2019) 142:189–93. doi: 10.1159/000499577
40. Casaclang-Verzosa G, Gersh BJ, Tsang TS. Structural and functional remodeling of the left atrium: clinical and therapeutic implications for atrial fibrillation. J Am Coll Cardiol. (2008) 51:1–11. doi: 10.1016/j.jacc.2007.09.026
41. Kagiyama N, Hayashida A, Toki M, Fukuda S, Ohara M, Hirohata A, et al. Insufficient leaflet remodeling in patients with atrial fibrillation: association with the severity of mitral regurgitation. Circ Cardiovasc Imaging. (2017) 10(3). doi: 10.1161/CIRCIMAGING.116.005451
42. Boilève V, Dreyfus J, Attias D, Scheuble A, Codogno I, Brochet E, et al. Predictors of mitral annulus enlargement? A real-time three-dimensional transesophageal study. Int J Cardiology. (2018) 270:349–52. doi: 10.1016/j.ijcard.2018.06.004
43. Bhat A, Gan GCH, Chen HHL, Khanna S, Nawaz S, Nunes MCP, et al. Association of left atrial metrics with atrial fibrillation rehospitalization and adverse cardiovascular outcomes in patients with nonvalvular atrial fibrillation following index hospitalization. J Am Soc Echocardiogr. (2021) 34:1046–55 e3. doi: 10.1016/j.echo.2021.06.015
Keywords: progression, atrial fibrillation, mitral stenosis, left atrial, mitral regurgitation, rheumatic heart disease
Citation: Gomes NFA, Silva VR, Levine RA, Esteves WAM, de Castro ML, Passos LSA, Dal-Bianco JP, Pantaleão AN, da Silva JLP, Tan TC, Dutra WO, Aikawa E, Hung J and Nunes MCP (2022) Progression of Mitral Regurgitation in Rheumatic Valve Disease: Role of Left Atrial Remodeling. Front. Cardiovasc. Med. 9:862382. doi: 10.3389/fcvm.2022.862382
Received: 25 January 2022; Accepted: 14 February 2022;
Published: 11 March 2022.
Edited by:
Ernesto Greco, Sapienza University of Rome, ItalyReviewed by:
Antonino S. Rubino, University of Campania Luigi Vanvitelli, ItalyGiuseppe Nasso, Anthea Hospital, Italy
Copyright © 2022 Gomes, Silva, Levine, Esteves, de Castro, Passos, Dal-Bianco, Pantaleão, da Silva, Tan, Dutra, Aikawa, Hung and Nunes. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Maria Carmo P. Nunes, mcarmo@waymail.com.br