
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Cardiovasc. Med., 22 April 2022
Sec. Cardiovascular Epidemiology and Prevention
Volume 9 - 2022 | https://doi.org/10.3389/fcvm.2022.859277
This article is part of the Research TopicSports CardiologyView all 19 articles
 Juntae Kim1†
Juntae Kim1† Pil-Sung Yang2†Byoung-Eun Park1Tae Soo Kang1Seong-Hoon Lim1
Pil-Sung Yang2†Byoung-Eun Park1Tae Soo Kang1Seong-Hoon Lim1 Sungsoo Cho1Su-Yeon Lee1
Sungsoo Cho1Su-Yeon Lee1 Young Hak Chung1
Young Hak Chung1 Myung-Yong Lee1Dongmin Kim1
Myung-Yong Lee1Dongmin Kim1 Boyoung Joung3*
Boyoung Joung3*Background: There is a paucity of information about mortality related to light-intensity physical activity (LPA) in the older population. We examine the associations between physical activity and mortality, focusing on the effect of light-intensity physical activity and the dose-response relationship between physical activity and mortality.
Methods: We analyzed a total of 58,537 participants aged ≥ 65 years (mean age, 73.9 ± 5.8 years; male, 36.0%) in the Korean National Health Insurance Service database between 2009 and 2012. The Date of the end of follow-up was December 31, 2013. Individuals were divided into four categories according to physical activity intensity: totally sedentary (43.3%), LPA only (35.8%), LPA and moderate- to vigorous-intensity physical activity (MVPA) (16.3%), MVPA only (4.5%). Physical activity was quantified using standardized self-reported questionnaires which composed of the duration and frequency of physical activity.
Results: During a mean follow-up of 39.6 ± 14.0 months, 5,651 (9.7%) deaths occurred. Compared with totally sedentary individuals, those in the LPA only, LPA and MVPA, and MVPA only groups showed 26% [hazard ratio (HR) 0.74, 95% confidence interval (CI) 0.68–0.82], 27% (HR 0.73, 95% CI 0.63–0.84), and 34% (HR 0.66, 95% CI 0.54–0.79) lower all-cause mortality risk, showing an inverse relationship between physical activity intensity and mortality risk. In contrast, the LPA only, LPA and MVPA, and MVPA only groups represented a stronger inverse association with CV mortality (LPA: HR 0.76, 95% CI 0.62–0.92; LPA with MVPA: HR 0.74, 95% CI 0.55–0.999; MVPA, HR 0.57, 95% CI 0.37–0.87). Among participants performing LPA alone, participants performing less than the recommended dose of physical activity had lower all-cause mortality than those with sedentary activity (1–249 MET-min/week: HR 0.74, 95% CI 0.67–0.82, 250–499 MET-min/week: HR 0.65, 95% CI 0.59–0.72).
Conclusion: Physical activity, even low doses of LPA, was associated with reduced mortality risk in the elderly population. This study may motivate sedentary individuals to engage in any physical activity for mortality benefits.
Physical activity is associated with a reduced risk of vascular, non-vascular disease, and mortality (1). Recent physical activity guidelines recommend at least 150–300 min per week of moderate-intensity physical activity (MPA) or 75–150 min per week of vigorous-intensity physical activity (VPA), which is equivalent to 500–999 metabolic equivalent task (MET)-min/week, in elderly (aged ≥ 65 years) (2, 3). Achieving >150 min/week moderate-intensity aerobic exercise is associated with a lower risk of morbidity, mortality, disability, and frailty compared with being sedentary (4, 5). However, most guidelines of physical activity are similar in middle-aged adults and older adults (3). It is estimated that >60% of elderly adults could not achieve 150 min per week of moderate- to vigorous-intensity physical activity (MVPA) (6). They have difficulty engaging in exercise due to their health condition. Also, the insufficiency of knowledge of the association between physical activity and health benefits and lack of physician advice to encourage exercise were barriers to exercise (6). Recently, the benefits of physical activity at doses below the current guideline-recommended level were reported. Wen et al. (7) reported health benefits in individuals who engaged in moderate-intensity physical activity at half the recommended amount. Hupin et al. reported a low dose of MVPA below recommended level reduced mortality by 22% in elderly adults. Mortality was further reduced in those who engaged in a higher dose of physical activity in a dose-dependent manner (8). However, whether light-intensity physical activity (LPA) can reduce mortality in the older population has not been revealed. To investigate this association, we analyzed the association between physical activity and mortality in older adults in a nationwide cohort. We focused on the dose-response relationship between LPA and mortality.
Data were collected from the National Health Insurance Service of Korea (NHIS)-Senior database, which included data on 558,147 individuals recruited by the 10% simple random sampling method from a total of 5.5 million subjects aged ≥ 60 years in the National Health Information Database (9, 10). The NHIS-Senior database covered the following parameters: sociodemographic and socioeconomic information, health check-up examinations, insurance status, and records of participants’ medical histories. This study was approved by the Institutional Review Board of the Yonsei University Health System (4-2021-0850).
From the Korean NHIS-Senior database, 278,003 participants aged ≥ 65 years who had available health check-up data between 2009 and 2012 were enrolled in this study. We excluded those with missing information on physical activity (n = 209,503). Also, those who achieved energy expenditure exceeding the guideline target range (>1,000 MET min/week) (n = 9,963) were excluded to evaluate the dose-response of physical activity below the recommended dose. Finally, a total of 58,537 subjects were included in the study and followed up until December 2013 (Figure 1).
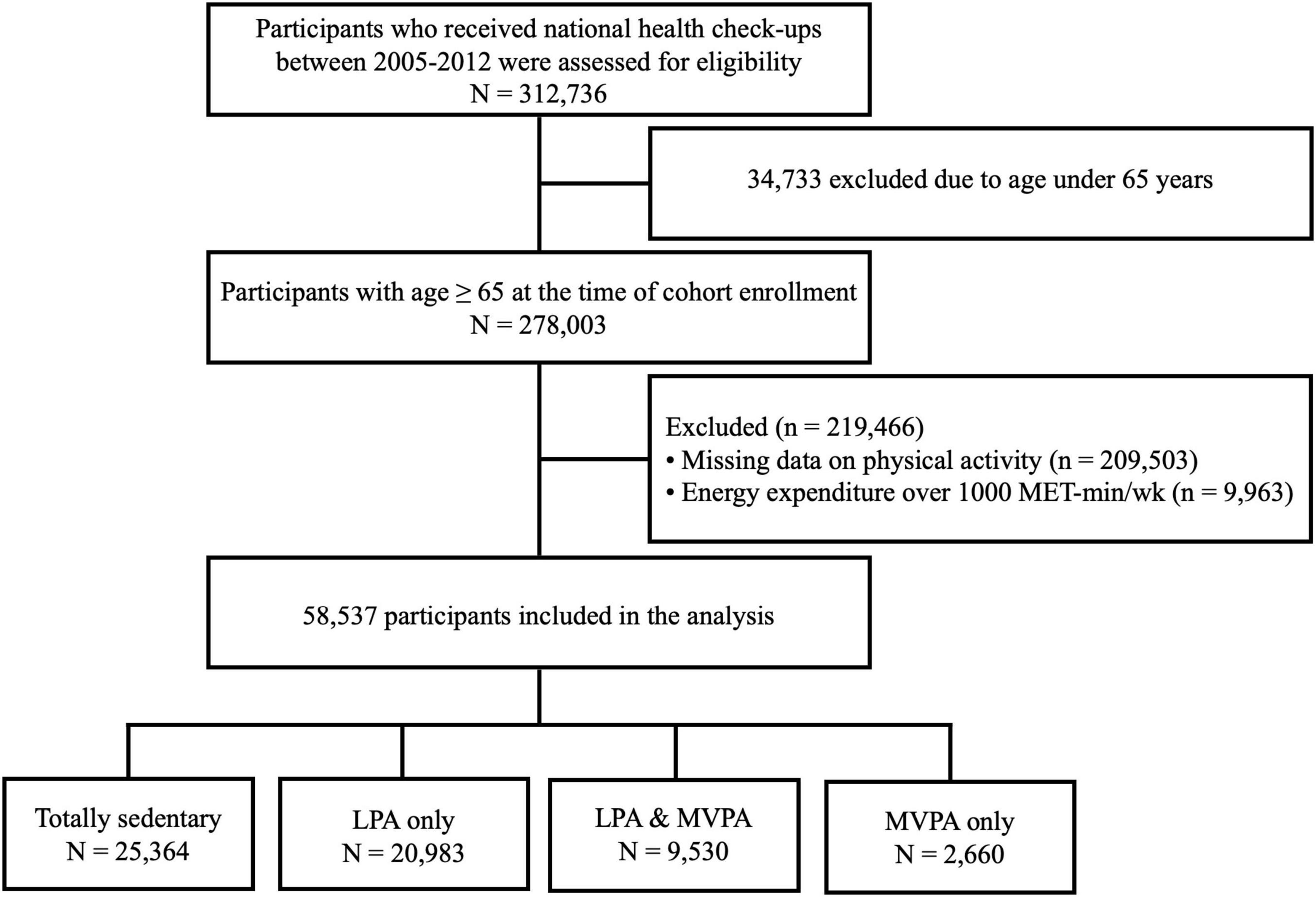
Figure 1. Summary of the statistical analysis design. LPA, light intensity physical activity; MVPA, moderate- to vigorous-intensity physical activity; MET, metabolic equivalent of task.
The leisure-time physical activity level was quantified using standardized self-reported questionnaires using a 7-day recall method (11). The survey was composed of three questions that addressed the usual frequency (days per week) of (i) VPA for at least 20 min, (ii) MPA for at least 30 min, and (iii) LPA for at least 30 min. VPA was defined as intense exercise that caused severe shortness of breath, such as running and bicycling at high speed. MPA was defined as exercise that caused mild shortness of breath, such as brisk walking and bicycling at the usual speed. LPA was defined as walking at a slow or leisurely pace.
Ratings of 3.0, 4.0, and 8.0 METs were assigned for LPA, MPA, and VPA, respectively (12). Physical activity-related energy expenditure (MET-min/week) was calculated by summing the product of frequency, intensity, and duration. The total energy expenditure level was stratified into 0, <250, 250–499, and 500–1,000 in an explorative manner. Totally sedentary group was defined as individuals without any leisure-time physical activity. The participants were categorized according to physical activity intensity into LPA only, LPA and MVPA, and MVPA only groups.
Sociodemographic variables included age, gender, and economic status. The baseline economic status was determined based on the relative economic levels categorized into 11 levels ranging from group 0 (lowest) to group 10 (highest) according to their health insurance premiums paid, which directly reflect each individual’s income level. Baseline comorbidities were verified using the International Classification of Disease-10 (ICD-10) codes and prescription medication before the index data (Supplementary Table 1). To improve diagnostic accuracy, comorbidities were identified when the condition was a discharge diagnosis or was recorded at least twice in an outpatient setting, similar to our previous studies (10, 12–20).
The primary outcome was all-cause mortality. The date of death and ICD-10 codes were verified from the National Population Registry of the Korea National Statistical Office using unique personal identification numbers (10, 12–20). NHIS and the National Statistical Office are national agencies serving all residents in the Republic of Korea, providing a complete event check. We investigated cause-specific mortality based on causes of death because exercise can be associated with cardiovascular (CV)-related and non-CV-related mortality. We defined CV death as death from diseases of the circulatory system (ICD codes I00–I78). The follow-up period was defined as the time from the index date that participants registered in this cohort to death or the end of the study period, whichever came first.
Descriptive statistics were used to analyze baseline characteristics and comorbidities. Categorical variables are expressed as frequencies (percentages). Continuous variables were reported as means ± standard deviations or medians with interquartile ranges. Categorical variables were compared using the Pearson chi-square test, and continuous variables were compared using one-way analysis of variance or the Kruskal-Wallis test, as appropriate.
The incidence rates of outcomes were calculated by dividing the number of events by person-time at risk and presented as the rate per 1,000 person-years. We analyzed the hazard ratios (HRs) and 95% confidence intervals (CIs) for mortality according to physical activity level. Multivariable Cox regression models were constructed with adjustment for age, sex, income level, residential area (urban or non-urban), body mass index, hypertension, diabetes mellitus, dyslipidemia, smoking, alcohol intake, chronic kidney disease, chronic obstructive lung disease, chronic liver disease, malignancy, cardiovascular medications (aspirin, P2Y12 inhibitor, statin, anticoagulant, beta-blocker, angiotensin converting enzyme inhibitor or angiotensin receptor blocker, calcium channel blocker, digoxin, and diuretics) and Charlson comorbidity index. Categorical measures of physical activity intensity and energy expenditure level were treated as an ordered value in Cox regression analysis to evaluate P value for linear trend. Restricted cubic spline curves were used to examine the effects of continuous values of physical activity (0 MET-min/week as reference) on death. Restricted cubic splines were fitted with three knots by treating the amount of physical activity as a continuous variable using the “rms” package.
We conducted subgroup analyses for the primary outcome stratified by age, sex, body mass index, and other baseline comorbidities. For sensitivity analysis, we performed separate analyses in those who did not perform any activity exceeding LPA.
All tests were two-tailed, with a p-value of <0.05 considered significant. Statistical analyses were conducted using R programming version 4.1.0 (The R Foundation for Statistical Computing, Vienna, Austria).
In total, 58,537 participants (men 36.0%) with a mean age of 73.9 ± 5.8 years were included in the analysis. Baseline characteristics according to physical activity intensity are summarized in Table 1. With regard to physical activity intensity, 43.3, 35.8, 16.3, and 4.5% of participants were included in the totally sedentary, LPA only, LPA and MVPA, and MVPA only groups, respectively. Of the total participants, 46,347 (79.2%) did not perform any activity beyond LPA. The distribution of exercise dose according to physical activity intensity is presented in Supplementary Figure 1. Participants performing physical activity tended to be younger, male-predominant, less likely to have comorbidities (particularly hypertension, chronic obstructive pulmonary disease (COPD), chronic kidney disease, and osteoporosis), and less affected by gait disturbances during the Timed Up and Go Test than totally sedentary participants. There were no significant differences in Activities of Daily Living scale, which represents the functional status of older adults.
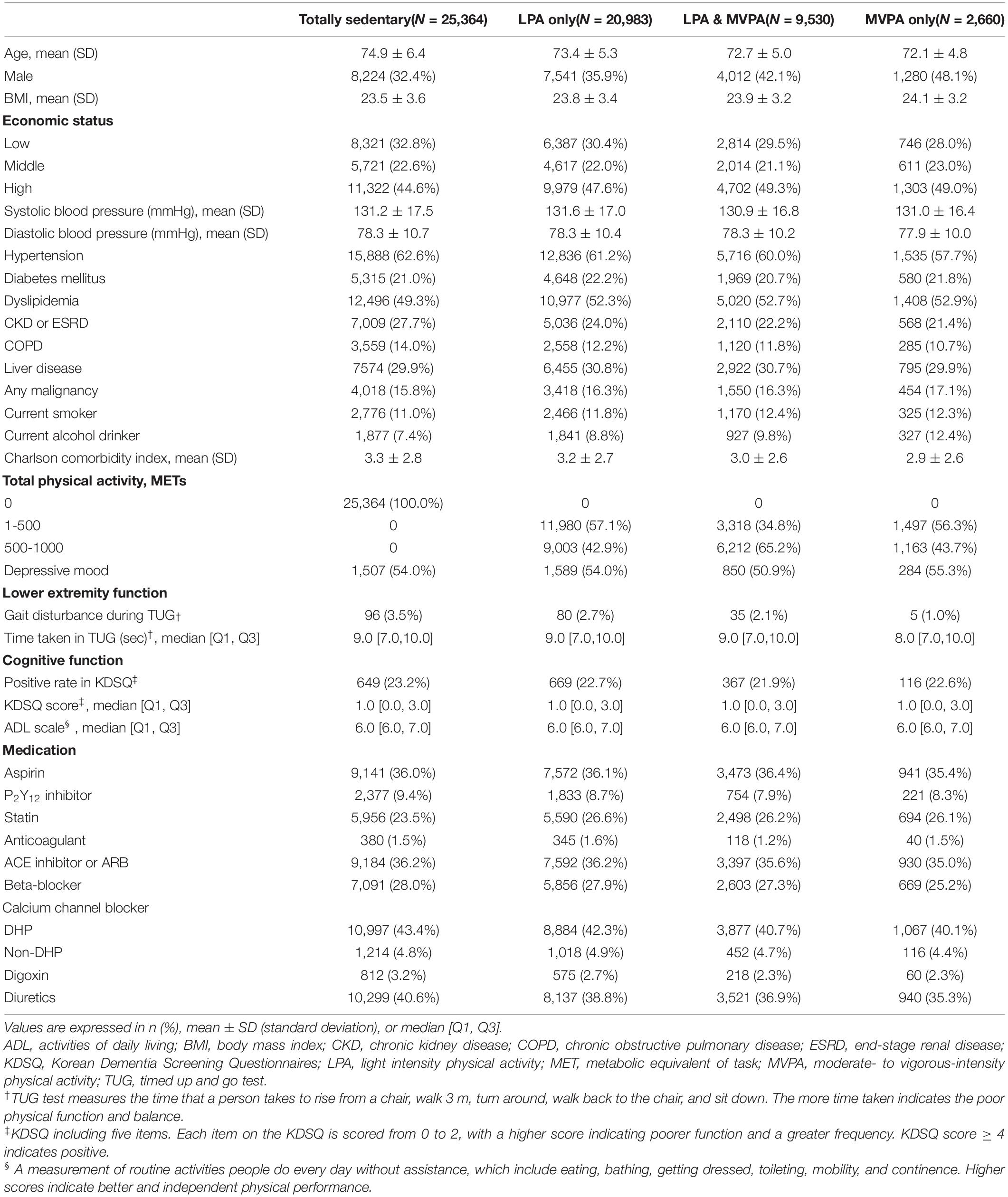
Table 1. Baseline characteristics.
During a mean follow-up of 39.6 ± 14.0 months, 5,651 (9.7%) deaths occurred. The overall incidence of mortality during follow-up was 29.3 per 1,000 person-years. When stratified by physical activity intensity, the incidence was 40.5, 22.6, 19.0, and 16.2 per 1,000 person-years in the totally sedentary, LPA only, LPA and MVPA, and MVPA only groups, respectively (Table 2). Compared with the totally sedentary group, the LPA only (HR 0.74, 95% CI 0.68–0.82), LPA and MVPA (HR 0.73, 95% CI 0.63–0.84), and MVPA only groups (HR 0.66, 95% CI 0.54–0.79) were associated with a lower risk of mortality.
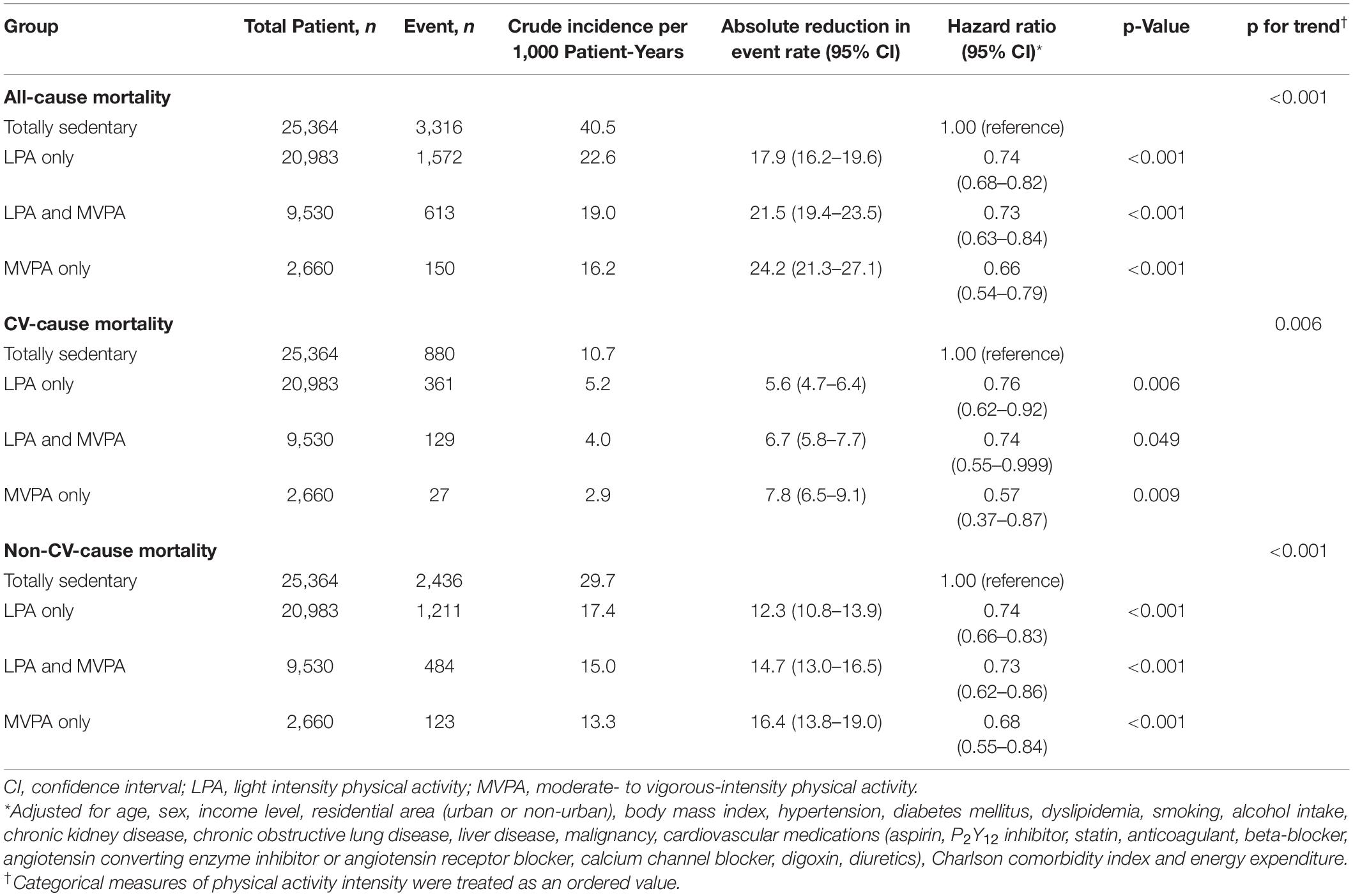
Table 2. Incidence and hazard ratio with 95% confidence intervals for all-cause death, cardiovascular (CV) cause death, and non-CV-cause death according to physical activity intensity.
The incidence of CV mortality was 10.7, 5.2, 4.0, and 2.9 per 1,000 person-years in the totally sedentary, LPA only, LPA and MVPA, and MVPA only groups, respectively. Compared with the totally sedentary group, the LPA only (HR 0.76, 95% CI 0.62–0.92), LPA and MVPA (HR 0.74, 95% CI 0.55–0.999), and MVPA only groups (HR 0.57, 95% CI 0.37–0.87) were associated with a lower risk of mortality (Table 2).
The incidence of non-CV mortality was 29.7, 17.4, 15.0, and 13.3 per 1,000 person-years in the totally sedentary, LPA only, LPA and MVPA, and MVPA only groups, respectively. Compared with the totally sedentary group, the LPA only (HR 0.74, 95% CI 0.66–0.83), LPA and MVPA (HR 0.73, 95% CI 0.62–0.86), and MVPA only groups (HR 0.68, 95% CI 0.55–0.84) were associated with a lower risk of mortality (Table 2).
The cumulative incidence of all-cause mortality, CV mortality, and non-CV mortality showed progressively lower trends with increasing physical activity intensity (Supplementary Figure 2).
Among the 58,537 participants, 46,347 (79.2%) participants, including 20,983 with LPA, did not perform any activity beyond LPA. In the LPA only group, 4,971 (10.7%), 7,009 (15.1%), and 9,003 (19.4%) participants performed 1–249, 250–499, and 500–1,000 MET-min/week of LPA, respectively. The cumulative incidence of mortality was lower in the group with 250–499 MET-min/week of LPA (Supplementary Figure 3). Compared with those in the totally sedentary group, participants with 1–249 MET-min/week of LPA (HR 0.74, 95% CI 0.67–0.82), 250–499 MET-min/week (HR 0.65, 95% CI 0.59–0.72), and 500–1,000 MET-min/week of LPA (HR 0.70, 95% CI 0.64–0.76) showed a lower risk of mortality (Table 3). Similar trends were observed in the MVPA group (Supplementary Figure 4). Even once a week of LPA was associated with significantly lower risks of all-cause mortality than the totally sedentary group (Figure 2).
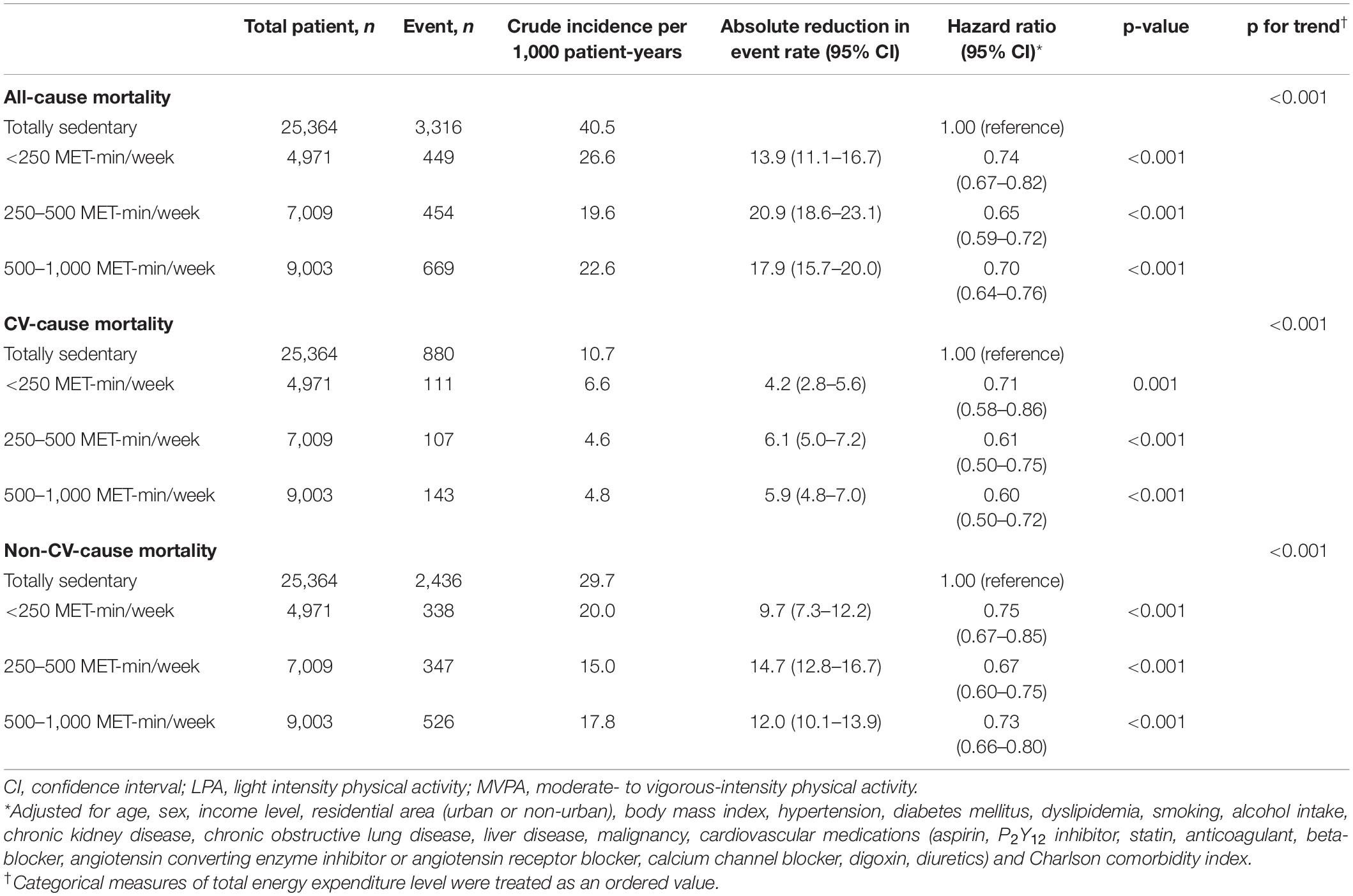
Table 3. Incidence and hazard ratio with 95% confidence intervals for all-cause death, CV cause death, and non-CV-cause death in those who did not perform any activity beyond LPA, according to energy expenditure (MET-min/week).
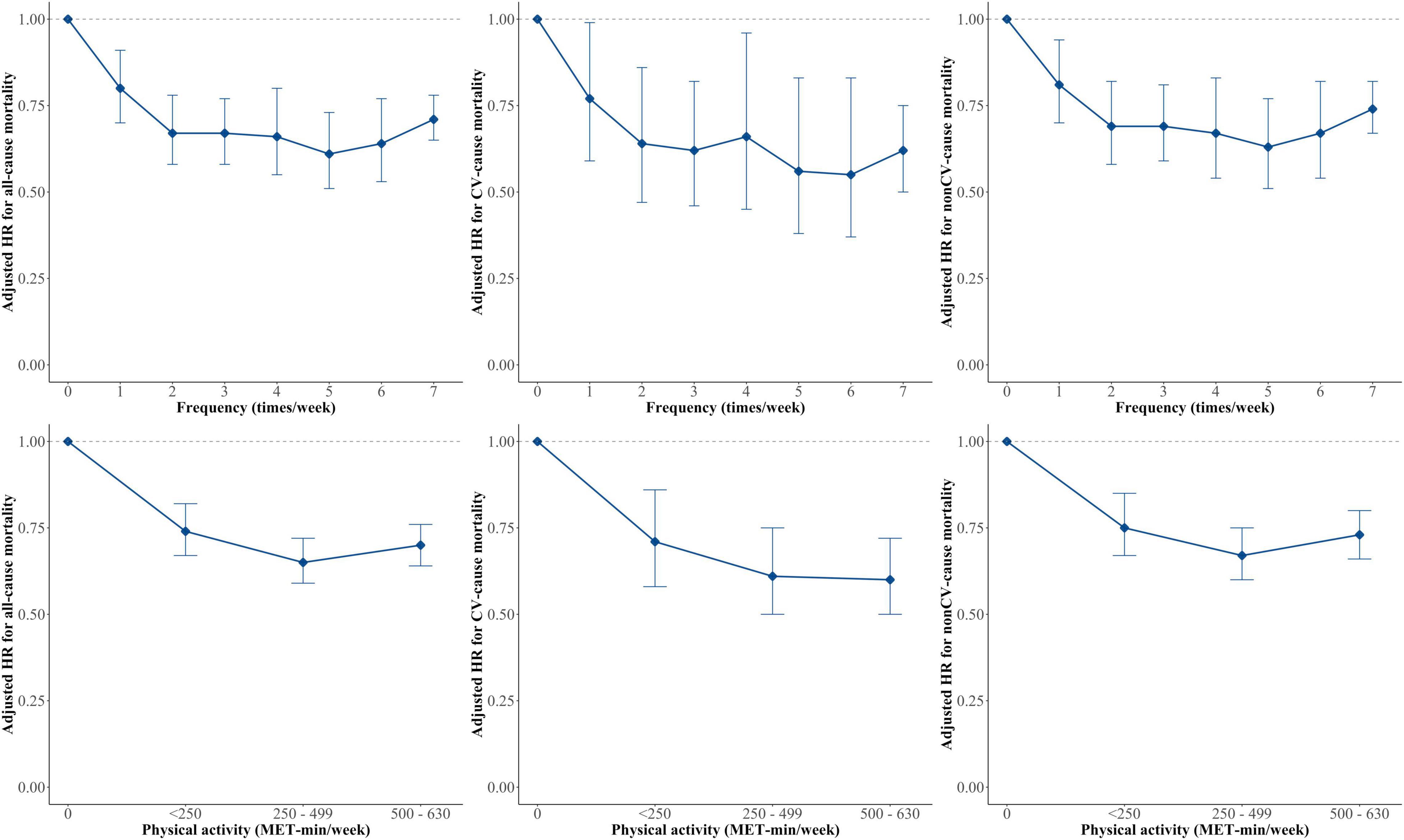
Figure 2. Hazard ratios (HRs) of All-cause, CV, and non-CV-mortality by exercise frequency, and physical activity level in those who did not perform any activity beyond LPA. Multivariable Cox regression models were constructed with adjustment for age, sex, income level, residential area (urban or non-urban), body mass index, hypertension, diabetes mellitus, dyslipidemia, smoking, alcohol intake, chronic kidney disease, chronic obstructive lung disease, liver disease, malignancy, cardiovascular medications (aspirin, P2Y12 inhibitor, statin, anticoagulant, beta-blocker, angiotensin converting enzyme inhibitor or angiotensin receptor blocker, calcium channel blocker, digoxin, diuretics) and Charlson comorbidity index. CV, cardiovascular; MPA, moderate-intensity physical activity; MET, metabolic equivalent of task.
Figure 3 shows the relationship between physical activity and all-cause mortality risk according to physical activity intensity using a restricted cubic spline curve. A non-linear relationship between LPA and mortality risk showed a continuous decrease in mortality risk until 360 MET-min/week (120 min/week: HR 0.63, 95% CI 0.57–0.71) and a plateau. The relationship between MVPA and mortality risk showed a continuous decrease in mortality risk until 528 MET-min/week or 132 min/week. For the same exercise duration, MVPA was associated with lower all-cause mortality than LPA.
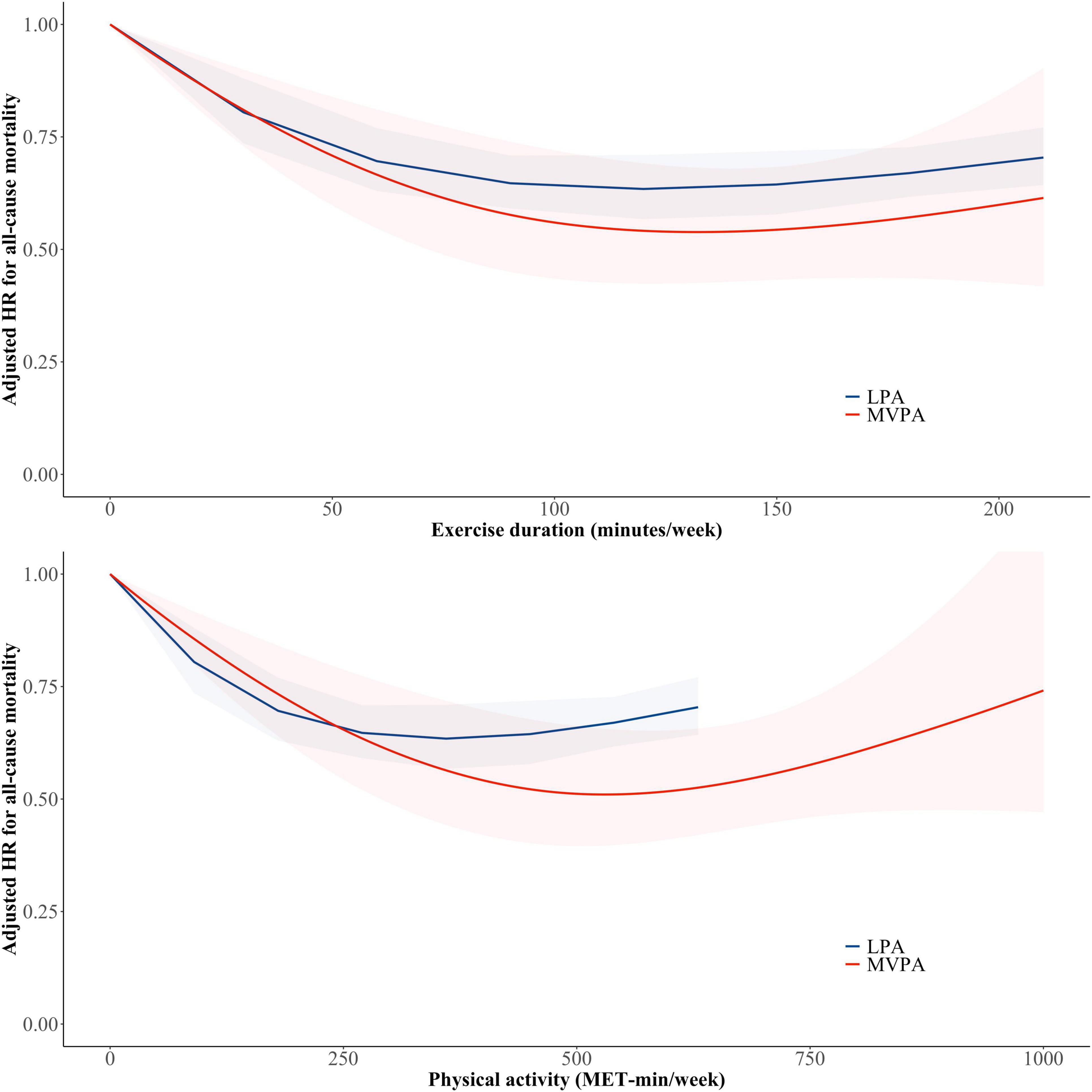
Figure 3. Non-linear relationship between physical activity and all-cause mortality risk according to physical activity intensity. Restricted cubic spline curves were constructed with regard to physical activity treated as a continuous variable. The red and blue lines and shades indicate adjusted hazard ratio and 95% confidence intervals for subjects with light-intensity physical activity and moderate to vigorous physical activity, respectively. LPA, light-intensity physical activity; MET, metabolic equivalent of task; MVPA, moderate- to vigorous-intensity physical activity.
The HR for all-cause mortality according to physical activity dose in different subgroups in those who did not perform any activity beyond LPA is presented in Supplementary Figure 5 and shows a consistent decrease in risk regardless of subgroups except in subjects with obesity and COPD. The HR for all-cause mortality according to physical activity intensity in different subgroups in the overall population is presented in Supplementary Figure 6.
In this study, 46,347 (79.2%) older participants did not perform any activity beyond LPA. Second, compared with those in the totally sedentary group, older adults performing LPA alone had a reduced risk of all-cause mortality, CV mortality, and non-CV mortality. Third, this finding was consistently observed regardless of the comorbidities. Finally, the risk of all-cause mortality was continuously reduced by LPA alone until 360 MET-min/week and reached a plateau. These results suggest that light physical activity alone can be beneficial in reducing mortality in older adults.
It is estimated that >60% of older people could not achieve 150 min per week of MVPA (6). In this study, 82.7% (55,616/68,500) of older adults were not able to achieve guideline-recommended exercise, suggesting that it may have been too demanding for them. Moreover, 79.2% of the older adults did not have physical activity beyond LPA.
Recent studies reported that the effect of LPA might be beneficial in older adults (7, 21, 22). Previous guidelines recommended MPA or VPA alone in elderly adults, although recent studies showed that LPA was also associated with improving cardio-metabolic health and reducing mortality risk (23). Another study showed that sedentary behavior was associated with negative health effects (24). Therefore, recently published WHO 2020 Guidelines on physical activity recommended replacing sedentary time with physical activity of any intensity, including LPA (3). The latest International Exercise Recommendations in Older Adults suggested that aerobic exercises including walking, stair climbing, stationary cycling, dancing, and aquatic exercise may start with a duration of 5–10 min and progress to 15–30 min with appropriate intensity using heart rate and/or perceived exertional scales (25). However, recent studies on LPA and mortality had a small number of participants and did not show consistent results (26, 27).
This study showed that all-cause mortality can be reduced even with LPA alone in older adults. Manson et al. (28) reported that both walking and vigorous exercise are associated with reduced cardiovascular events among 73,743 postmenopausal women aged 50–79 years. According to Saint-Maurice et al.’s study (29), based on a representative sample of US adults (mean age, 56.8 years), daily step count was significantly associated with all-cause mortality. However, higher step intensity was not associated with lower mortality after adjusting for the total number of steps per day.
We found the dose-response relationship between physical activity and mortality by calculating the total amount of physical activity as a continuous variable. The positive effect of increased physical activity on mortality started at a low dose of total physical activity. These results imply that even a low dose of physical activity, rather than sedentary behavior, could reduce the mortality risk.
The reduction in the risk of all-cause mortality was decreased in both LPA and MVPA with a further increase in the amount of exercise. The risk of all-cause death was reduced by 37% at 360 MET-min/week and by 49% at 528 MET-min/week in the LPA only and MVPA only groups, respectively. This finding suggests that the reduction in all-cause mortality is greater with more intensive exercise. Wang et al. (30) suggested that participants with a higher proportion of VPA to total physical activity had a lower mortality.
The physical activity for older adults should be individualized according to their biological age, comorbidity, safety, and functional capacity (31). Nauman et al. (32) suggested that personalized metric for physical activity using individual’s sex, age, and heart rates was useful for quantifying the amount of PA needed to produce significant health benefits. Recommendation from the American College of Sports Medicine and American Heart Association (ACSM/AHA) define aerobic intensity for healthy adults in absolute terms, e.g., moderate-intensity comprises 3.0–6.0 MET activities. The older adult recommendation from ACSM/AHA defines exercise intensity as relative to fitness (33). The range of 30–60 min of light-intensity activity a day could be sufficient in older adults with functional limitations.
This study had some limitations. First, such studies using administrative databases could be susceptible to errors arising from coding inaccuracies. To minimize this issue, we used the same definitions that we had already validated in previous studies using the Korean NHIS cohort (10, 12–20). Second, it relied on self-reported data on physical activity, as collected at baseline. The answer at the time of questionnaire completion may not represent the actual physical activity status throughout life. Furthermore, behavioral changes that occurred during the follow-up period could not be assessed in this study. Also, it might be inappropriate to assign MET levels for the respective intensity groupings without knowing the cardiorespiratory fitness levels of the participants. This is because a proportion of the older adults likely had low fitness levels which would have made it difficult to perform activity in between 4 and 8 and above 8 METs. Despite these limitations, this study has strength in that it included a large number of older adults who had physical activity data. We assessed the dose-response relationship between physical activity and mortality and focused on the effect of LPA on the incidence of mortality. Various sensitivity analyses showed consistent results, which supports our main result.
The analyses of the Korean NHIS-Senior database showed a reduced mortality risk in individuals with LPA than in those with totally sedentary behavior. The mortality risk was reduced in a dose-dependent manner even less than the recommended dose of physical activity. Replacing sedentary time with any activity, even low doses of LPA could play a role in reducing the mortality risk in inactive older adults.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
The studies involving human participants were reviewed and approved by Institutional Review Board of the Yonsei University Health System (4-2021-0850). Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
JK and BJ designed the study. P-SY, B-EP, TSK, and S-HL assisted with data acquisition and interpretation. SC, S-YL, and YHC performed statistical analyses. DK and M-YL contributed to the discussion. JK, DK, and BJ drafted the manuscript. P-SY and BJ revised the manuscript. All authors read and approved the final manuscript.
This study was supported by a research grant from the Korean Healthcare Technology R&D project funded by the Ministry of Health and Welfare (HI15C1200, HC19C0130, and HI19C0622). The funders had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.
BJ has served as a Speaker for Bayer, BMS/Pfizer, Medtronic, and Daiichi-Sankyo and received research funds from Medtronic and Abbott.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The National Health Information Database was provided by the NHIS of Korea. The authors would like to thank the National Health Insurance Service for cooperation.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fcvm.2022.859277/full#supplementary-material
ACSM/AHA, American College of Sports Medicine and American Heart Association; CI, confidence interval; CV, cardiovascular; HR, hazard ratio; ICD-10, The International Classification of Disease-10th revision; LPA, light-intensity physical activity; MET, metabolic equivalent task; MPA, moderate-intensity physical activity; MVPA, moderate- to vigorous-intensity physical activity; NHIS, The National Health Insurance Service of Korea; VPA, vigorous-intensity physical activity.
1. Lear SA, Hu W, Rangarajan S, Gasevic D, Leong D, Iqbal R, et al. The effect of physical activity on mortality and cardiovascular disease in 130 000 people from 17 high-income, middle-income, and low-income countries: the pure study. Lancet. (2017) 390:2643–54. doi: 10.1016/S0140-6736(17)31634-3
2. Piercy KL, Troiano RP, Ballard RM, Carlson SA, Fulton JE, Galuska DA, et al. The physical activity guidelines for Americans. JAMA. (2018) 320:2020–8. doi: 10.1001/jama.2018.14854
3. Bull FC, Al-Ansari SS, Biddle S, Borodulin K, Buman MP, Cardon G, et al. World health organization 2020 guidelines on physical activity and sedentary behaviour. Br J Sports Med. (2020) 54:1451–62. doi: 10.1136/bjsports-2020-102955
4. Rogers NT, Marshall A, Roberts CH, Demakakos P, Steptoe A, Scholes S. Physical activity and trajectories of frailty among older adults: evidence from the english longitudinal study of ageing. PLoS One. (2017) 12:e0170878. doi: 10.1371/journal.pone.0170878
5. Chou WT, Tomata Y, Watanabe T, Sugawara Y, Kakizaki M, Tsuji I. Relationships between changes in time spent walking since middle age and incident functional disability. Prev Med. (2014) 59:68–72. doi: 10.1016/j.ypmed.2013.11.019
6. Schutzer KA, Graves BS. Barriers and motivations to exercise in older adults. Prev Med. (2004) 39:1056–61. doi: 10.1016/j.ypmed.2004.04.003
7. Wen CP, Wai JP, Tsai MK, Yang YC, Cheng TY, Lee MC, et al. Minimum amount of physical activity for reduced mortality and extended life expectancy: a prospective cohort study. Lancet. (2011) 378:1244–53. doi: 10.1016/S0140-6736(11)60749-6
8. Hupin D, Roche F, Gremeaux V, Chatard JC, Oriol M, Gaspoz JM, et al. Even a low-dose of moderate-to-vigorous physical activity reduces mortality by 22% in adults aged >/=60 years: a systematic review and meta-analysis. Br J Sports Med. (2015) 49:1262–7. doi: 10.1136/bjsports-2014-094306
9. Kim YI, Kim YY, Yoon JL, Won CW, Ha S, Cho KD, et al. Cohort profile: national health insurance service-senior (NHIS-senior) cohort in Korea. BMJ open. (2019) 9:e024344. doi: 10.1136/bmjopen-2018-024344
10. Kim D, Yang PS, Yu HT, Kim TH, Jang E, Sung JH, et al. Risk of dementia in stroke-free patients diagnosed with atrial fibrillation: data from a population-based cohort. Eur Heart J. (2019) 40:2313–23. doi: 10.1093/eurheartj/ehz386
11. Chun MY. Validity and reliability of Korean version of international physical activity questionnaire short form in the elderly. Korean J Fam Med. (2012) 33:144–51. doi: 10.4082/kjfm.2012.33.3.144
12. Jin MN, Yang PS, Song C, Yu HT, Kim TH, Uhm JS, et al. Physical activity and risk of atrial fibrillation: a nationwide cohort study in general population. Sci Rep. (2019) 9:13270. doi: 10.1038/s41598-019-49686-w
13. Kim D, Yang PS, Jang E, Yu HT, Kim TH, Uhm JS, et al. 10-year nationwide trends of the incidence, prevalence, and adverse outcomes of non-valvular atrial fibrillation nationwide health insurance data covering the entire Korean population. Am Heart J. (2018) 202:20–6. doi: 10.1016/j.ahj.2018.04.017
14. Kim D, Yang PS, Jang E, Yu HT, Kim TH, Uhm JS, et al. Increasing trends in hospital care burden of atrial fibrillation in Korea, 2006 through 2015. Heart. (2018) 104:2010–7. doi: 10.1136/heartjnl-2017-312930
15. Kim D, Yang PS, Kim TH, Jang E, Shin H, Kim HY, et al. Ideal blood pressure in patients with atrial fibrillation. J Am Coll Cardiol. (2018) 72:1233–45. doi: 10.1016/j.jacc.2018.05.076
16. Kim TH, Yang PS, Yu HT, Jang E, Shin H, Kim HY, et al. Effect of hypertension duration and blood pressure level on ischaemic stroke risk in atrial fibrillation: nationwide data covering the entire Korean population. Eur Heart J. (2019) 40:809–19. doi: 10.1093/eurheartj/ehy877
17. Kim D, Yang PS, You SC, Sung JH, Jang E, Yu HT, et al. Treatment timing and the effects of rhythm control strategy in patients with atrial fibrillation: nationwide cohort study. BMJ. (2021) 373:n991. doi: 10.1136/bmj.n991
18. Kim D, Yang PS, Jang E, Tae Yu H, Kim TH, Uhm JS, et al. Blood pressure control and dementia risk in midlife patients with atrial fibrillation. Hypertension. (2020) 75:1296–304. doi: 10.1161/HYPERTENSIONAHA.119.14388
19. Kim D, Yang PS, Sung JH, Jang E, Yu HT, Kim TH, et al. Less dementia after catheter ablation for atrial fibrillation: a nationwide cohort study. Eur Heart J. (2020) 41:4483–93. doi: 10.1093/eurheartj/ehaa726
20. Yang PS, Jang E, Yu HT, Kim TH, Pak HN, Lee MH, et al. Changes in cardiovascular risk factors and cardiovascular events in the elderly population. J Am Heart Assoc. (2021) 10:e019482. doi: 10.1161/JAHA.120.019482
21. Ku PW, Hamer M, Liao Y, Hsueh MC, Chen LJ. Device-measured light-intensity physical activity and mortality: a meta-analysis. Scand J Med Sci Sports. (2020) 30:13–24. doi: 10.1111/sms.13557
22. Rees-Punia E, Deubler E, Campbell P, Gapstur SM, Patel A. Light-intensity physical activity in a large prospective cohort of older us adults: a 21-year follow-up of mortality. Gerontology. (2020) 66:259–65. doi: 10.1159/000502860
23. Chastin SF, De Craemer M, De Cocker K, Powell L, Van Cauwenberg J, Dall P, et al. How does light-intensity physical activity associate with adult cardiometabolic health and mortality? Systematic review with meta-analysis of experimental and observational studies. Br J Sports Med. (2019) 53:370–6. doi: 10.1136/bjsports-2017-097563
24. Saunders TJ, McIsaac T, Douillette K, Gaulton N, Hunter S, Rhodes RE, et al. Sedentary behaviour and health in adults: an overview of systematic reviews. Appl Physiol Nutr Metab. (2020) 45:S197–217. doi: 10.1139/apnm-2020-0272
25. Izquierdo M, Merchant RA, Morley JE, Anker SD, Aprahamian I, Arai H, et al. International exercise recommendations in older adults (icfsr): expert consensus guidelines. J Nutr Health Aging. (2021) 25:824–53. doi: 10.1007/s12603-021-1665-8
26. Schooling CM, Lam TH, Li ZB, Ho SY, Chan WM, Ho KS, et al. Obesity, physical activity, and mortality in a prospective Chinese elderly cohort. Arch Intern Med. (2006) 166:1498–504. doi: 10.1001/archinte.166.14.1498
27. Hayasaka S, Shibata Y, Ishikawa S, Kayaba K, Gotoh T, Noda T, et al. Physical activity and all-cause mortality in Japan: the JICHI medical school (JMS) cohort study. J Epidemiol. (2009) 19:24–7. doi: 10.2188/jea.JE20080043
28. Manson JE, Greenland P, LaCroix AZ, Stefanick ML, Mouton CP, Oberman A, et al. Walking compared with vigorous exercise for the prevention of cardiovascular events in women. N Engl J Med. (2002) 347:716–25. doi: 10.1056/NEJMoa021067
29. Saint-Maurice PF, Troiano RP, Bassett DR Jr, Graubard BI, Carlson SA, Shiroma EJ, et al. Association of daily step count and step intensity with mortality among us adults. JAMA. (2020) 323:1151–60. doi: 10.1001/jama.2020.1382
30. Wang Y, Nie J, Ferrari G, Rey-Lopez JP, Rezende LFM. Association of physical activity intensity with mortality: a national cohort study of 403681 US adults. JAMA Intern Med. (2021) 181:203–11. doi: 10.1001/jamainternmed.2020.6331
31. Pelliccia A, Sharma S, Gati S, Back M, Borjesson M, Caselli S, et al. 2020 ESC guidelines on sports cardiology and exercise in patients with cardiovascular disease. Eur Heart J. (2021) 42:17–96.
32. Nauman J, Nes BM, Zisko N, Revdal A, Myers J, Kaminsky LA, et al. Personal activity intelligence (PAI): a new standard in activity tracking for obtaining a healthy cardiorespiratory fitness level and low cardiovascular risk. Prog Cardiovasc Dis. (2019) 62:179–85. doi: 10.1016/j.pcad.2019.02.006
Keywords: sport cardiology, exercise, light-intensity physical activity, elderly, all-cause mortality, cardiovascular mortality
Citation: Kim J, Yang P-S, Park B-E, Kang TS, Lim S-H, Cho S, Lee S-Y, Chung YH, Lee M-Y, Kim D and Joung B (2022) Association of Light-Intensity Physical Activity With Mortality in the Older Population: A Nationwide Cohort Study. Front. Cardiovasc. Med. 9:859277. doi: 10.3389/fcvm.2022.859277
Received: 21 January 2022; Accepted: 29 March 2022;
Published: 22 April 2022.
Edited by:
Sabina Gallina, University of Studies G. d’Annunzio Chieti and Pescara, ItalyReviewed by:
Marco Matteo Ciccone, University of Bari Aldo Moro, ItalyCopyright © 2022 Kim, Yang, Park, Kang, Lim, Cho, Lee, Chung, Lee, Kim and Joung. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Boyoung Joung, Y2J5NjkwOEB5dWhzLmFj
†These authors have contributed equally to this work and share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.