
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Cardiovasc. Med., 01 April 2022
Sec. Heart Valve Disease
Volume 9 - 2022 | https://doi.org/10.3389/fcvm.2022.852954
This article is part of the Research TopicAdvances in the Imaging and Treatment of Valvular Heart DiseaseView all 22 articles
 Laura Galian-Gay1
Laura Galian-Gay1 Roxana Andreina Escalona Silva1Gisela Teixidó-Turà1Guillem Casas1Elena Ferrer-Sistach2
Roxana Andreina Escalona Silva1Gisela Teixidó-Turà1Guillem Casas1Elena Ferrer-Sistach2 Cristina Mitroi3Susana Mingo3Vanessa Monivas3Daniel Saura4Bàrbara Vidal5Livia Trasca5Sergio Moral6
Cristina Mitroi3Susana Mingo3Vanessa Monivas3Daniel Saura4Bàrbara Vidal5Livia Trasca5Sergio Moral6 Francisco Calvo7Maria Castiñeira Busto7
Francisco Calvo7Maria Castiñeira Busto7 Violeta Sánchez8Ariana Gonzalez9Gabriela Guzman10Marta Noris Mora11MiguelÁngel Arnau Vives12Jesús Peteiro13Alberto Bouzas13Aleksandra Mas-Stachurska14Teresa González-Alujas1Laura Gutiérrez1Rubén Fernandez-Galera1
Violeta Sánchez8Ariana Gonzalez9Gabriela Guzman10Marta Noris Mora11MiguelÁngel Arnau Vives12Jesús Peteiro13Alberto Bouzas13Aleksandra Mas-Stachurska14Teresa González-Alujas1Laura Gutiérrez1Rubén Fernandez-Galera1 Filipa Valente1
Filipa Valente1 Andrea Guala1Aroa Ruiz-Muñoz1Cesar Augusto Sao Avilés1José F. Rodríguez Palomares1Ignacio Ferreira1*
Andrea Guala1Aroa Ruiz-Muñoz1Cesar Augusto Sao Avilés1José F. Rodríguez Palomares1Ignacio Ferreira1* Artur Evangelista1*
Artur Evangelista1*Objectives: To determine the risk of mortality and need for aortic valve replacement (AVR) in patients with low-flow low-gradient (LFLG) aortic stenosis (AS).
Methods: A longitudinal multicentre study including consecutive patients with severe AS (aortic valve area [AVA] < 1.0 cm2) and normal left ventricular ejection fraction (LVEF). Patients were classified as: high-gradient (HG, mean gradient ≥ 40 mmHg), normal-flow low-gradient (NFLG, mean gradient < 40 mmHg, indexed systolic volume (SVi) > 35 ml/m2) and LFLG (mean gradient < 40 mmHg, SVi ≤ 35 ml/m2).
Results: Of 1,391 patients, 147 (10.5%) had LFLG, 752 (54.1%) HG, and 492 (35.4%) NFLG. Echocardiographic parameters of the LFLG group showed similar AVA to the HG group but with less severity in the dimensionless index, calcification, and hypertrophy. The HG group required AVR earlier than NFLG (p < 0.001) and LFLG (p < 0.001), with no differences between LFLG and NFLG groups (p = 0.358). Overall mortality was 27.7% (CI 95% 25.3–30.1) with no differences among groups (p = 0.319). The impact of AVR in terms of overall mortality reduction was observed the most in patients with HG (hazard ratio [HR]: 0.17; 95% CI: 0.12–0.23; p < 0.001), followed by patients with LFLG (HR: 0.25; 95% CI: 0.13–0.49; p < 0.001), and finally patients with NFLG (HR: 0.29; 95% CI: 0.20–0.44; p < 0.001), with a risk reduction of 84, 75, and 71%, respectively.
Conclusions: Paradoxical LFLG AS affects 10.5% of severe AS, and has a lower need for AVR than the HG group and similar to the NFLG group, with no differences in mortality. AVR had a lower impact on LFLG AS compared with HG AS. Therefore, the findings of the present study showed LFLG AS to have an intermediate clinical risk profile between the HG and NFHG groups.
Degenerative aortic stenosis (AS) is the most common valve disease in developed countries and, owing to aging of the population, threatens to become a true epidemic in coming decades (1). Paradoxical low-flow low-gradient (LFLG) AS poses diagnostic challenges and uncertainties regarding the true severity of the disease and appropriate therapeutic decision-making. Initial studies considered LFLG AS to be an entity with worse prognosis than high-gradient (HG) AS and could thus benefit from surgical or percutaneous treatment as or earlier than in HG AS (2–4). However, recent meta-analyses questioned these results, considering that LFLG AS probably behaves in an intermediate manner between moderate and severe AS (5–8). The present study aimed to assess, in a large and contemporary cohort of patients with AS, the natural history and prognosis of LFLG AS in comparison with HG and normal-flow low-gradient (NFLG) AS, as well as the impact of aortic valve replacement (AVR) in each subgroup.
A retrospective longitudinal observational study was conducted of consecutive patients from 14 tertiary hospitals nationwide diagnosed between 2008 and 2016 with severe AS (aortic valve area (AVA) < 1.0 cm2) with left ventricular ejection fraction (LVEF) ≥ 50% on the transthoracic ECG (Figure 1). Exclusion criteria were: age < 18 years, atrial fibrillation or pacemaker rhythm, aortic regurgitation more than mild, other valvular heart disease more than mild, left ventricular outflow tract dynamic gradient exceeding a velocity >1 m/s, previous heart surgery, suboptimal echocardiographic window, poor blood pressure control, and comorbidities at baseline that could themselves cause an alteration in functional grade or prognosis (e.g., severe chronic obstructive pulmonary disease [COPD]).
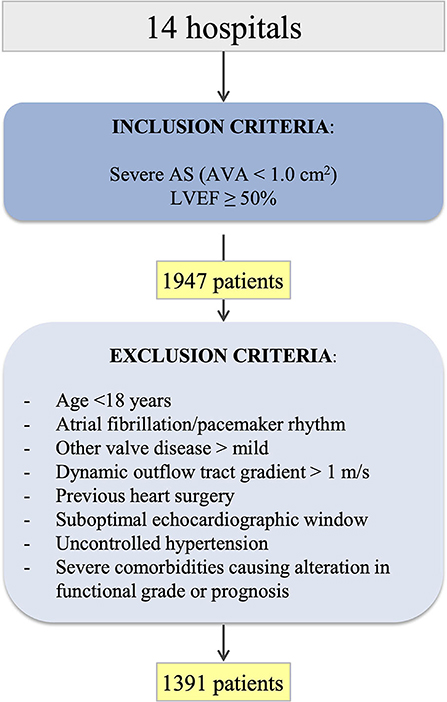
Figure 1. A flowchart of patients participating in the study. AS, aortic stenosis; AVA, aortic valve area; LVEF, left ventricular ejection fraction.
The approval for the study was obtained from the Ethics Committee of the Vall d'Hebron Hospital (PR (AG) 60/2018). The study protocol conformed to the ethical guidelines of the Declaration of Helsinki 1975 as reflected in the Ethics Committee approval.
Baseline demographic and clinical data were collected. The presence of coronary artery disease was defined when a history of acute myocardial infarction, significant ischaemic or the presence of coronary artery disease were documented. The presence of baseline symptoms was considered when the functional status of the New York Heart Association was ≥ II, or syncope or angina was reported in clinical reports. Follow-up clinical data, such as the need for surgery or TAVI, status (alive/deceased), and cause of death (cardiovascular/non-cardiovascular) were also obtained. AVR was indicated at the participating centers according to current guideline indications (9).
Echocardiographic studies were performed in all patients by expert imaging cardiologists at the participating centers. Measurements were obtained following European Association of Cardiovascular Imaging (EACVI) standards and were validated by a senior expert from each center. AVA was calculated through continuity equation. The degree of aortic valve calcification and stenosis was established semi-quantitatively as recommended by current guidelines (10). Patients were classified into 3 groups according to baseline ECG data regarding the gradient and indexed systolic volume (SVi) as recommended by current guidelines (10): high-gradient (HG) if mean gradient ≥ 40 mmHg, normal-flow low-gradient (NFLG) if mean gradient < 40 mmHg and SVi > 35 ml/m2, and LFLG if mean gradient < 40 mmHg and SVi ≤ 35 ml/m2. Patients were not involved in the design, conducting, reporting, or dissemination plans of our research.
All analyses were made with Stata software version 13.1. Continuous variables were expressed as mean and SD when the normality assumptions were met and as median and interquartile range (IQR) otherwise. Categorical variables were expressed as absolute numbers and percentages. Demographic, echocardiographic, and AVR variables were evaluated among the different groups using ANOVA test, chi-square test, or Fisher's exact test, as appropriate. Kaplan–Meier analysis was used for time-to-event variables (time-mortality and time-AVR) and the log-rank test to compare survival and time-AVR curves among groups. A multivariate Cox regression analysis was used to identify independent variables associated with the response variable (predictors of mortality and AVR), such as variables with statistical significance (p < 0.20) in the univariate analysis or with significant clinical relevance.
In this study, 1,391 patients with baseline ECG with AVA < 1 cm2 and normal LVEF from 14 tertiary hospitals (Figure 1), mean age 74.5 (10.9) years and 53.6% women were included. In the whole cohort, 752 (54.1%) were classified as HG, 492 (35.4%) as NFLG, and 147 (10.5%) as LFLG. No significant differences were observed among groups regarding age, sex, or cardiovascular risk factors, except for smoking and body weight (Table 1). The mean total follow-up time was 59.0 months (IQR 39.7–82.9 months), with no significant differences among groups.
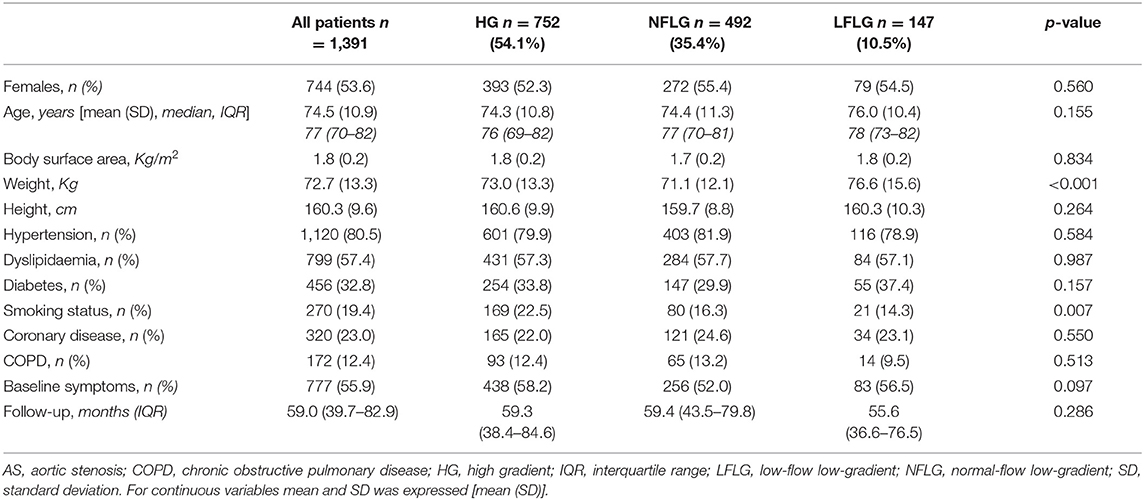
Table 1. Clinical and demographic data according to aortic stenosis (AS) subgroups at baseline.
The echocardiographic data of each AS subtype are shown in Table 2. Remarkably, AVA of the LFLG group was similar to AVA of the HG group [0.74 (0.14) vs. 0.73 (0.16) cm2; p = NS] and significantly lower than that of the NFLG group [0.89 (0.09), p < 0.001]. However, the dimensionless index (ratio between LVOT VTI and aortic VTI) value in the LFLG group was intermediate between the HG group [0.25 (0.06) vs. 0.22 (0.05); p < 0.001] and the NFLG group [0.25 (0.06) vs. 0.27 (0.04); p < 0.001], with differences between the HG and NFLG groups also being significant [0.22 (0.05) vs. 0.27 (0.04); p < 0.001]. Left ventricular hypertrophy was significantly lower in patients of the LFLG group compared with the HG group and similar to the NFLG group (Table 2). Severe valve calcification in the LFLG group was lower than in the HG group and showed no significant differences with the NFLG group.
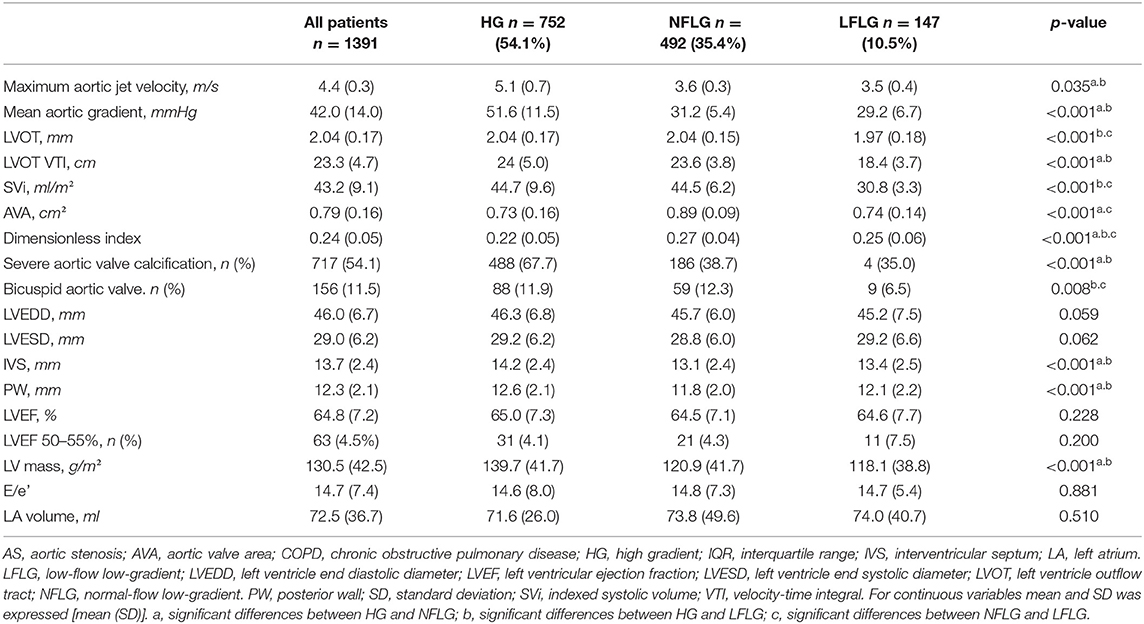
Table 2. Echocardiographic data according to the AS subgroup at baseline.
In total, 1,248 patients had complete data related to AVR (676 (54.2%) with HG, 450 (36.0%) with NFLG and 122 (9.8%) with LFLG). Throughout the follow-up, 857 patients (68.7%, CI 95% 66.0–71.2) underwent AVR [685 surgery and 172 Transcater Aortic Valve Implantation (TAVI)]: 529 with HG (78.2%, CI 95% 75.0–81.3; median time: 17.7 months, IQR 5.5–43.4 months), 74 with LFLG (60.6%, CI 95% 51.4–69.4; median time: 41.0 months, IQR 13.6–78.9 months) and 254 with NFLG (56.4%, CI 95% 51.7–61.1; median time: 46.9 months, IQR: 26.0–70.0 months) (Figure 2) with differences among groups in the estimated survival free from AVR that persisted after adjustment for age, smoking, diabetes mellitus, presence of symptoms, and LVEF (p < 0.001). In HG AS, AVR was indicated earlier compared with NFLG (log-rank p < 0.001) and LFLG AS (log-rank p < 0.001). No significant differences were observed between the LFLG and NFLG groups (log-rank p = 0.358).
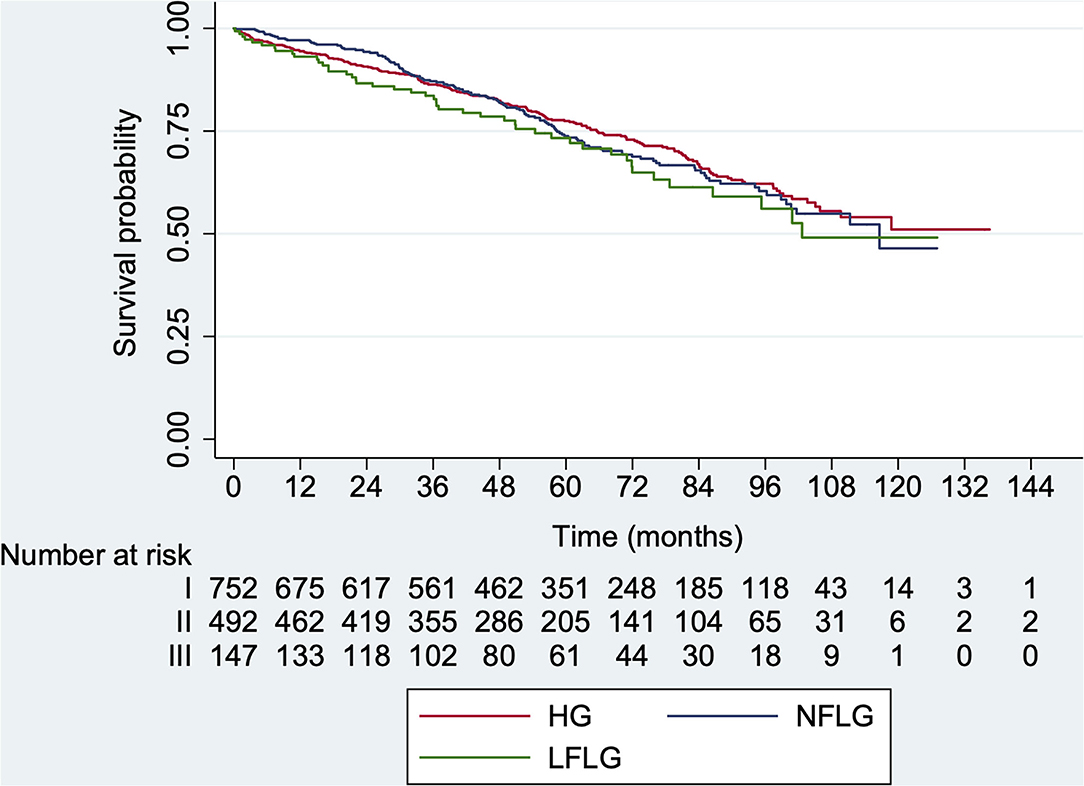
Figure 2. Kaplan–Meier aortic valve replacement (AVR)-free survival curves according to AS subtype at baseline. HG, high-gradient; LFLG, low-flow low-gradient; NFLG, normal-flow low-gradient (log-rank p < 0.001).
On multivariate analysis, indication of AVR was inversely associated with age (hazard ratio [HR] 0.99, CI 95%: 0.98–0.99; p = 0.002); nevertheless, the presence of symptoms (HR 1.82, 95% CI: 1.57–2.01; p < 0.001) and coronary artery disease (HR 1.21, 95% CI: 1.03–1.43; p = 0.018) were independently related to AVR indication. Regarding echocardiographic parameters, AVA (AVA < 0.8 cm2: HR 1.25, 95% CI: 1.04–1.48; p = 0.014), mean gradient (mean gradient ≥ 40 mmHg: HR 1.95, 95% CI: 1.67–2.29, p < 0.001), dimensionless index (dimensionless index ≤ 0.25: HR 1, 39, 95% CI: 1.18–1.65, p < 0.001), and LVEF 50–55% (HR 1.52, 95% CI: 1.21–1.91, p < 0.001) were also independently associated to AVR indication (Supplementary Table 1).
Overall mortality during follow-up was 27.7% (385 patients, CI 95% 25.3–30.1): 46 of the LFLG group (31.3%, CI 95% 23.9–39.5; median time: 50.8 months, IQR: 29.6–75.8), 205 of the HG group (27.3%, CI 95% 24.1–30.6; median time: 56.1 months, IQR: 33.8–83.7), and 134 of the NFLG group (27.2%, CI 95% 23.3–31.4; median time: 53.2 months, IQR: 31.0–76.9). Kaplan–Meier survival curves showed no significant differences among groups (Figure 3, log-rank p = 0.319). Early mortality after AVR (<30 days) was 6.5% (25 patients, CI 95% 1.2–2.6) with no differences among groups.
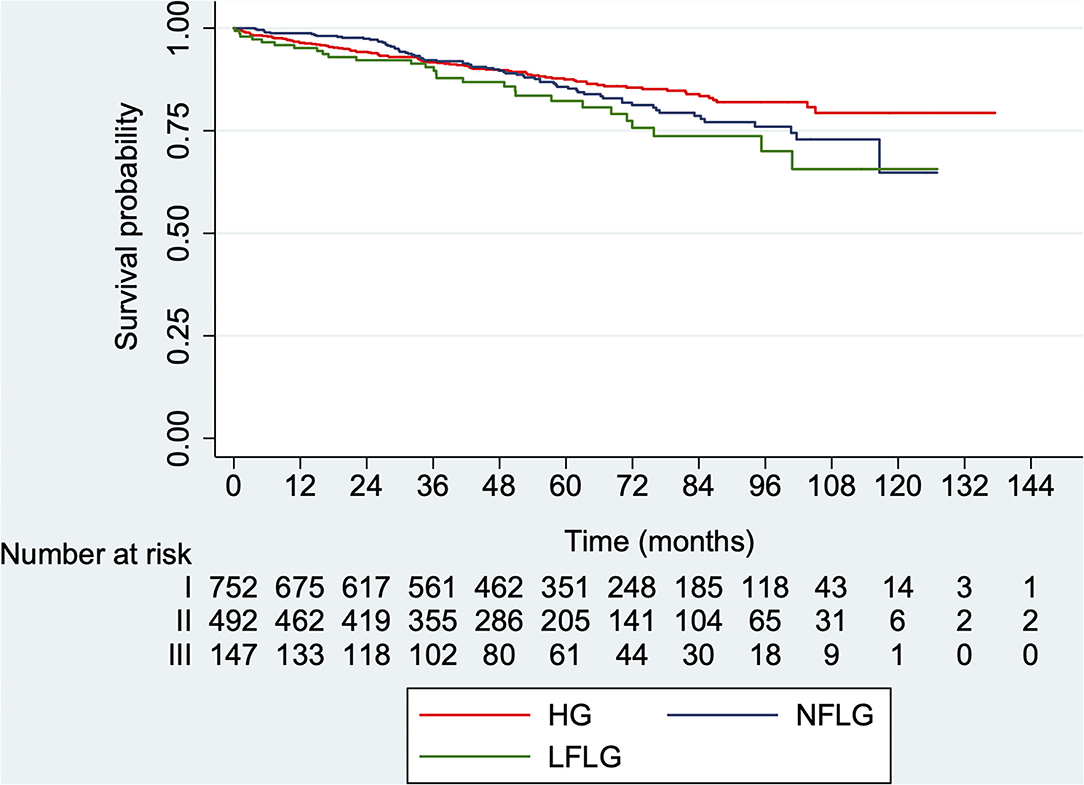
Figure 3. Kaplan–Meier survival curves for overall mortality according to AS subtype at baseline. HG, high-gradient; LFLG, low-flow low-gradient; NFLG, normal-flow low-gradient (log-rank p = 0.319).
Death from cardiovascular cause occurred in 195 cases (14%, CI 95% 12.2–16.0) representing a 50.6% of overall mortality: 28 patients with LFLG (19%, CI 95% 13.0–26.3; median time: 50.9 months, ICR: 32.0–75.9), 95 patients with HG (12.6%, CI 10.3–15.2; median time: 56.1 months, ICR: 33.8–83.7), and 72 patients with NFLG (14.6%, CI 95% 11.6–18.1; median time: 52.5 months, ICR: 29.0–76.9), with no significant differences among groups (Figure 4, log-rank p = 0.061).
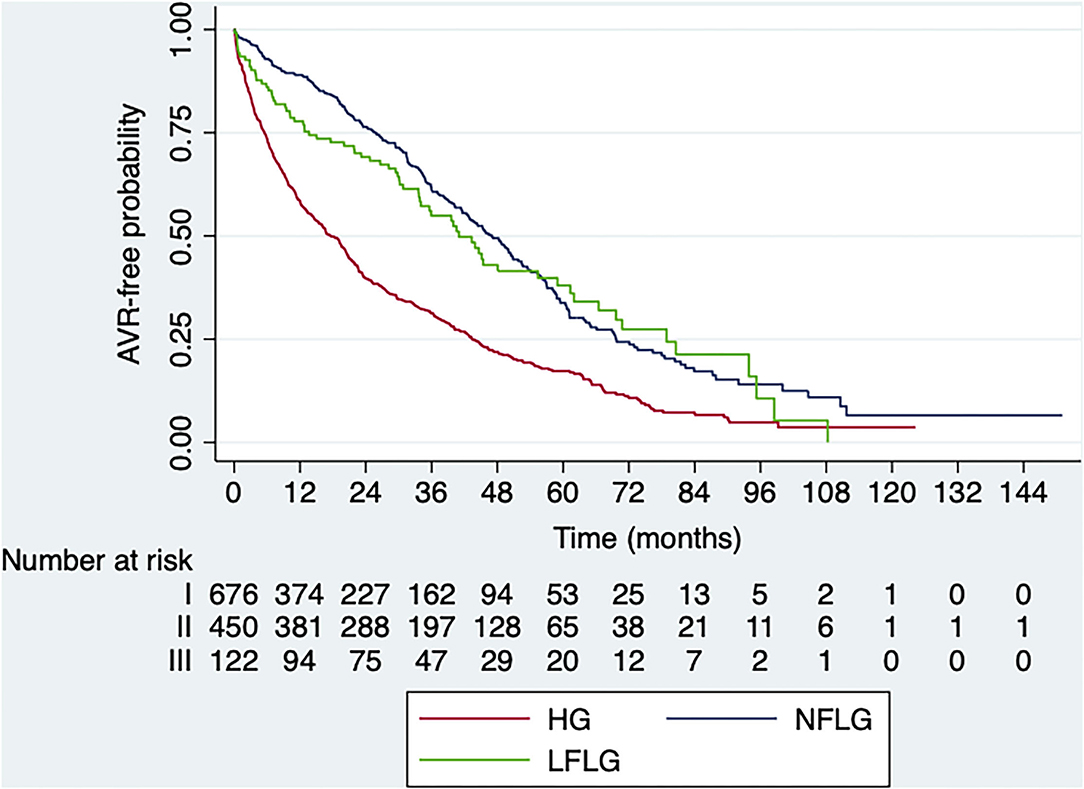
Figure 4. Kaplan–Meier survival curves for cardiovascular mortality according to AS subtype at baseline. HG, high-gradient; LFLG, low-flow low-gradient; NFLG, normal-flow low-gradient (log-rank p = 0.061).
In patients undergoing AVR, no significant differences in mortality were observed among groups (log-rank p = 0.612) after adjustment for significant clinical variables and AVA. However, in non-operated patients, differences were observed among groups (log-rank p = 0.004), with low event-free survival in the HG group compared with the NFLG group (log-rank p = 0.001), with no significant differences between the LFLG and HG groups (log-rank p = 0.354) or between the LFLG and NFLG groups (log-rank p = 0.171).
In the multivariate analysis, age (HR 1.06, 95% CI: 1.04–1.08; p < 0.001), diabetes mellitus (HR 1.52; 95% CI: 1.23–1.89; p < 0.001), smoking (HR: 1.77, 95% CI: 1.32–2.37; p < 0.0001), COPD (HR 1.45, 95% CI: 1.09–1.92; p = 0.010), and the presence of symptoms (HR 1.48, 95% CI: 1.18–1.85; p = 0.001) were clinical variables associated to overall mortality (Supplementary Table 2). Echocardiographic variables independently associated with mortality were mean gradient > 50 mmHg (HR 1.56, 95% CI: 1.17–2.08; p = 0.002) and LVEF 50–55% (HR 1.68, 95% CI: 1.07–2.63; p = 0.023).
Overall mortality was higher in those patients who did not undergo AVR. The impact of AVR on mortality reduction in the whole population with AS was significant (HR: 0.22; 95% CI: 0.18–0.28; p < 0.001) after adjustment for significant clinical variables and AVA. AVR reduced mortality risk by 83% in patients with HG AS (HR: 0.17; 95% CI: 0.12–0.23; p < 0.001), 75% in patients with LFLG (HR: 0.25; 95% CI: 0.13–0.49; p < 0.001), and 71% in patients with NFLG AS (HR: 0.29; 95% CI: 0.20–0.44; p < 0.001; Figure 5).
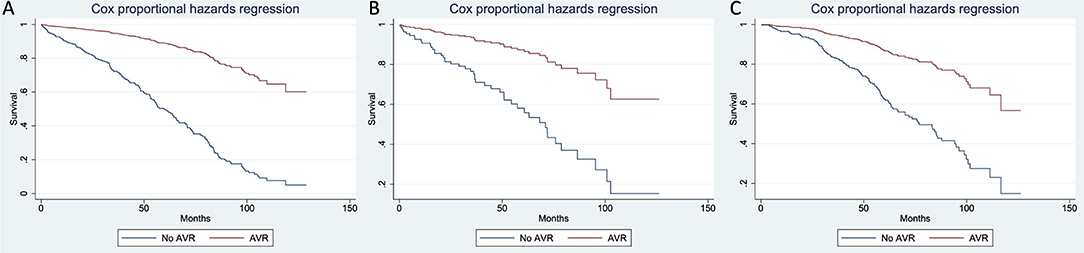
Figure 5. Cox survival curves for overall mortality in the population with severe AS according to AVR and AS subtype [(A): HG; (B): LFLG; (C): NFLG)]. AVR, aortic valve replacement.
In this large multicentre retrospective cohort of consecutive patients with AS and normal ejection fraction and sinus rhythm, the prevalence of paradoxical LFLG AS was 10%. Echocardiographic parameters showed a similar AVA in comparison with HG and NFLG groups, but less severity in the dimensionless index, valve calcification, and LV hypertrophy than in HG AS. However, overall/cardiovascular mortality and the impact of AVR on mortality reduction were similar to patients with HG AS.
In the present series, patients with LFLG AS had a similar AVA value to the HG group and lower than NFLG group. However, in the remaining echocardiographic parameters, such as left ventricular hypertrophy and degree of valve calcification, LFLG did not significantly differ from NFLG AS. Interestingly, the dimensionless index in LFLG AS laid between HG and NFLG AS. Thus, LFLG AS presented intermediate-severity echocardiographic parameters between HG and NFLG AS. Other series yielded similar results (4). Clavel et al. in a series of 561 patients with AS, found LFLG patients to have significantly lower velocity and transaortic gradients than HG AS while AVA was practically the same (11). Several studies reported that this entity was associated with small ventricles and a high degree of hypertrophy (2); however, the present LFLG group had a significantly lower degree of hypertrophy than patients with HG AS but similar to those with NFLG AS. Other studies using echocardiography or CMR stated that patients with LFLG AS do not have a greater degree of hypertrophy than HG AS, but lower or similar to NFLG AS or moderate AS (4, 5, 12). Few studies analyzed the degree of calcification in LFLG AS by echocardiography or multidetector CT (MDCT), although this is currently one of the more recommended approaches to diagnose severe AS (10, 13). Calcification by MDCT may be highly useful in patients with discordant severity data on echocardiography (13).
The risk throughout follow-up of undergoing AVR was higher for patients with HG, lower in patients with LFLG AS and comparable to patients with NFLG AS, as previously reported (14). Mortality was 27% and no significant differences were detected between patients with LFLG AS and the other groups. Patients of the three hemodynamic groups who underwent AVR had a similar prognosis, whereas patients who did not undergo surgery had higher mortality in the HG group compared with the NFLG group, with no differences between the LFLG and HG groups. Different series previously reported poorer survival and a higher rate of events in the LFLG population compared with HG AS (3, 11, 15); however, the trend in the more contemporary series has changed the paradigm, suggesting that higher mortality is associated with HG AS, with the behavior of LFLG AS being more similar to moderate AS or intermediate between HG and NFLG AS (8, 16). Recent evidence suggested that moderate forms of AS are not as benign as historically assumed, particularly if left ventricular dysfunction is present (17). A recent study analyzing data from the Australian national echocardiography database showed mortality in patients with moderate AS to be similar to severe AS (18). Another contemporary study reported that patients with NFLG who did not undergo surgery had 6.3 times more overall mortality compared with surgically-treated patients, with surgery being associated with a significant increase in survival (19). Taking the results of this study and previous reported findings into account, there may be sufficient reasons to consider AS severity as moderate-severe when the AVA is between 0.8–1.2 cm2 and severe when < 0.8 cm2. In moderate-severe patients with AS, other multimodality parameters, such as calcium score by CT, exercise test, or left ventricle overall strain could help to identify a subgroup of patients in whom AVR would be indicated.
Overall, patients with significant AS benefited from intervention on the AV, and despite the HG AS group benefited the most, both LFLG and NFLG AS also obtained significant benefit. Although few studies failed to show this benefit in patients with LFLG AS (5, 20), most series suggested a beneficial effect of valve replacement in the LFLG population (and even in NFLG and moderate AS) compared with conservative management (4, 18, 19). Thus, evidence of the effectiveness of aggressive treatment (surgical or percutaneous) of AS continues to grow and, though data remain discrepant, the trend is toward a more aggressive approach and in a wider range of the disease.
In this study, patients with AS who died were older, more symptomatic, had more cardiovascular risk factors and a smaller AVA. However, the multivariate analysis failed to show AVA to be independently associated with mortality which instead was related to age, risk factors (diabetes, smoking, and COPD), symptoms, mean gradient > 50 mmHg, and LVEF from 50–54%. Some studies showed mortality in AS to be associated with maximum velocity, aortic calcification, and LVEF. Valvular heart disease guidelines recommended as class I an AVR indication in systolic dysfunction (LVEF < 50%) regardless of the presence of symptoms (9, 21). However, recent studies reported that patients with LVEF < 55% had poor prognosis (22–24). All these results suggest that the cut-off point of <50% for LVEF could be too low, indicating that left ventricular dysfunction is already present when LVEF is between 50 and 60% and, in fact, recent guidelines recommend that patients with LVEF <60% on serial studies and severe AS should undergo surgery (21). Cardiac magnetic resonance demonstrated the presence of late gadolinium enhancement and increased extracellular volume in AS patients with normal ejection fraction, which have been related to prognosis (25). Other imaging techniques, such as strain by speckle tracking echocardiography can detect patients with subclinical ventricular dysfunction, (26) with overall longitudinal strain values < −15% being associated with worse prognosis (27, 28). Global LV strain values may become one of the markers that will provide additional data to decide whether or not the patient could have a higher risk and deserves surgery. Given that patients with LFLG AS benefit significantly from AVR, they should be followed with caution, with the accuracy in echocardiographic severity evaluation to be maximized to avoid possible errors in SVi quantification. Furthermore, additional information through other imaging techniques (myocardial strain, CMR of calcium score by CT) are likely to be useful to determine whether data support the AS severity and/or suggest incipient ventricular dysfunction, to sustain the choice to treat paradoxical LFLG as HG AS.
The main limitation of this study was its retrospective nature. In the present series, confirmation of the low-flow state was not requested for inclusion. Exclusion of patients with atrial fibrillation was considered in the design of the study since the continuity equation may be less accurate in AVA calculation. Calcification of the aortic valve was analyzed following the semi-quantitative approach recommended by the current guidelines, although the optimal method is cardiac CT. Myocardial strain would have added complementary information; however, owing to the multicentre nature of the study and the years of inclusion established, variability of the values depending on the different vendors used would have resulted in difficult result analysis.
Low-flow low-gradient AS has intermediate echocardiographic severity parameters and clinical outcomes between NFLG and HG AS, with lower AVR requirements than HG AS, but with overall mortality and benefits of surgery similar to the other two haemodynamic groups. Given that patients classified within this group benefited significantly from AVR, they should be followed with caution as in HG AS. The most appropriate option to adequately manage this subgroup may be to maximize the accuracy of the echocardiographic evaluation, provide additional information through other imaging techniques and determine whether there are data supporting the severity of AS or suggestive of incipient ventricular dysfunction, for them to be treated as HG AS.
The datasets presented in this article are not readily available because further analyses are still underway for other papers awaiting publication. Requests to access these datasets should be directed to LG-G, bGF1cmFnYWxpYW5nYXlAZ21haWwuY29t.
The studies involving human participants were reviewed and approved by CEIm - Comitè d'Ètica d'Investigació amb medicaments - VHIR. Informed consent was not available due to the retrospective nature of the study.
LG-G, GT-T, GC, and AE designed the study. LG-G, RE, GC, EF-S, CM, SMi, VM, DS, BV, LT, SM, FC, MC, VS, AGo, GG, MM, MA, JP, AB, AM-S, TG-A, LG, RF-G, FV, and AR-M contributed to conduction and reporting of the study. LG-G and AS performed the statistical analysis. AE, AGu, JFP, and IF contributed to manuscript revision. AE and IF are the responsible for the overall content as guarantors. All authors contributed to the article and approved the submitted version.
AGu has received funding from the Spanish Ministry of Science, Innovation and Universities (IJC2018- 037349-I).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
We wish to thank Christine O'Hara for help with the English version of the manuscript.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fcvm.2022.852954/full#supplementary-material
1. Osnabrugge RLJ, Mylotte D, Head SJ, Van Mieghem NM, Nkomo VT, LeReun CM, et al. Aortic stenosis in the elderly. J Am Coll Cardiol. (2013) 62:1002–12. doi: 10.1016/j.jacc.2013.05.015
2. Hachicha Z, Dumesnil JG, Bogaty P, Pibarot P. Paradoxical low-flow, low-gradient severe aortic stenosis despite preserved ejection fraction is associated with higher afterload and reduced survival. Circulation. (2007) 115:2856–64. doi: 10.1161/CIRCULATIONAHA.106.668681
3. Lancellotti P, Magne J, Donal E, Davin L, O'Connor K, Rosca M, et al. Clinical outcome in asymptomatic severe aortic stenosis: Insights from the new proposed aortic stenosis grading classification. J Am Coll Cardiol. (2012) 59:235–43. doi: 10.1016/j.jacc.2011.08.072
4. Eleid MF, Sorajja P, Michelena HI, Malouf JF, Scott CG, Pellikka PA. Flow-gradient patterns in severe aortic stenosis with preserved ejection fraction: Clinical characteristics and predictors of survival. Circulation. (2013) 128:1781–9. doi: 10.1161/CIRCULATIONAHA.113.003695
5. Tribouilloy C, Rusinaru D, Marchaux S, Castel AL, Debry N, Maizel J, et al. Low-gradient, low-flow severe aortic stenosis with preserved left ventricular ejection fraction: Characteristics, outcome, and implications for surgery. J Am Coll Cardiol. (2015) 65:55–66. doi: 10.1016/j.jacc.2014.09.080
6. Jander N, Minners J, Holme I, Gerdts E, Boman K, Brudi P, et al. Outcome of patients with low-gradient severe aortic stenosis and preserved ejection fraction. Circulation. (2011) 123:887–95. doi: 10.1161/CIRCULATIONAHA.110.983510
7. Maes F, Boulif J, Piérard S, De Meester C, Melchior J, Gerber B, et al. Natural history of paradoxical low-gradient severe aortic stenosis. Circ Cardiovasc Imag. (2014) 7:714–22. doi: 10.1161/CIRCIMAGING.113.001695
8. Rezzoug N, Vaes B, Pasquet A, Gerber B, de Meester C, Van Pottelbergh G, et al. Prevalence and prognostic impact of valve area—gradient patterns in patients ≥80 years with moderate-to-severe aortic stenosis (from the prospective BELFRAIL study). Am J Cardiol. (2015) 116:925–32. doi: 10.1016/j.amjcard.2015.05.062
9. Baumgartner H, Falk V, Bax JJ, De Bonis M, Hamm C, Holm PJ, et al. 2017 ESC/EACTS Guidelines for the management of valvular heart disease. Eur Heart J. (2017) 38:2739–91. doi: 10.1016/j.rec.2017.12.013
10. Baumgartner H, Hung J, Bermejo J, Chambers JB, Edvardsen T, Goldstein S, et al. Recommendations on the echocardiographic assessment of aortic valve stenosis: a focused update from the european association of cardiovascular imaging and the american society of echocardiography. J Am Soc Echocardiogr. (2017) 30:372–92. doi: 10.1016/j.echo.2017.02.009
11. Clavel M-A, Dumesnil JG, Capoulade R, Mathieu P, Sénéchal M, Pibarot P. Outcome of patients with aortic stenosis, small valve area, and low-flow, low-gradient despite preserved left ventricular ejection fraction. J Am Coll Cardiol. (2012) 60:1259–67. doi: 10.1016/j.jacc.2011.12.054
12. Barone-Rochette G, Piérard S, Seldrum S, de Meester de., Ravenstein C, Melchior J, Maes F, et al. Aortic valve area, stroke volume, left ventricular hypertrophy, remodeling, and fibrosis in aortic stenosis assessed by cardiac magnetic resonance imaging: comparison between high and low gradient and normal and low flow aortic stenosis. Circ Cardiovasc Imaging. (2013) 6:1009–17. doi: 10.1161/CIRCIMAGING.113.000515
13. Clavel M-A, Messika-Zeitoun D, Pibarot P, Aggarwal SR, Malouf J, Araoz PA, et al. The complex nature of discordant severe calcified aortic valve disease grading: new insights from combined Doppler echocardiographic and computed tomographic study. J Am Coll Cardiol. (2013) 62:2329–38. doi: 10.1016/j.jacc.2013.08.1621
14. González Gómez A, Fernández-Golfín C, Monteagudo JM, Izurieta C, Hinojar R, García A, et al. Severe aortic stenosis patients with preserved ejection fraction according to flow and gradient classification: prevalence and outcomes. Int J Cardiol. (2017) 248:211–5. doi: 10.1016/j.ijcard.2017.06.064
15. Parikh R, Goodman AL, Barr T, Sabik JF, Svensson LG, Rodriguez LL, et al. Outcomes of surgical aortic valve replacement for severe aortic stenosis: Incorporation of left ventricular systolic function and stroke volume index. J Thorac Cardiovasc Surg. (2015) 149:1558–66e1. doi: 10.1016/j.jtcvs.2015.03.008
16. Kavianipour M, Farkhooy A, Flachskampf FA. Clinical outcome and functional characteristics of patients with asymptomatic low-flow low-gradient severe aortic stenosis with preserved ejection fraction are closer to high-gradient severe than to moderate aortic stenosis. Int J Cardiovasc Imaging. (2017) 34:545–52. doi: 10.1007/s10554-017-1264-2
17. van Gils L, Clavel M-A, Vollema EM, Hahn RT, Spitzer E, Delgado V, et al. Prognostic implications of moderate aortic stenosis in patients with left ventricular systolic dysfunction. J Am Coll Cardiol. (2017) 69:2383–92. doi: 10.1016/j.jacc.2017.03.023
18. Strange G, Stewart S, Celermajer D, Prior D, Scalia GM, Marwick T, et al. Poor long-term survival in patients with moderate aortic stenosis. J Am Coll Cardiol. (2019) 74:1851–63. doi: 10.1016/j.jacc.2019.08.004
19. Saeed S, Vamvakidou A, Seifert R, Khattar R, Li W, Senior R. The impact of aortic valve replacement on survival in patients with normal flow low gradient severe aortic stenosis: a propensity-matched comparison. Eur Heart J Cardiovasc Imaging. (2019) 20:1094–101. doi: 10.1093/ehjci/jez191
20. Zheng Q, Djohan AH, Lim E, Ding ZP, Ling LH, Chan ES, et al. Effects of aortic valve replacement on severe aortic stenosis and preserved systolic function: systematic review and network meta-analysis. Sci Rep. (2017) 7:1–9. doi: 10.1038/s41598-017-05021-9
21. Otto CM, Nishimura RA, Bonow RO, Carabello BA, III JPE, Gentile F, et al. 2020 ACC/AHA guideline for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association joint committee on clinical practice guidelines. Circulation. (2021) 143:E72–227. doi: 10.1161/CIR.0000000000000923
22. Dahl JS, Eleid MF, Michelena HI, Scott CG, Suri RM, Schaff H V, et al. Effect of left ventricular ejection fraction on postoperative outcome in patients with severe aortic stenosis undergoing aortic valve replacement. Circ Cardiovasc Imaging. (2015) 8:1–8. doi: 10.1161/CIRCIMAGING.114.002917
23. Capoulade R, Le Ven F, Clavel M-A, Dumesnil JG, Dahou A, Thébault C, et al. Echocardiographic predictors of outcomes in adults with aortic stenosis. Heart. (2016) 102:934–42. doi: 10.1136/heartjnl-2015-308742
24. Ito S, Miranda WR, Nkomo VT, Connolly HM, Pislaru S V, Greason KL, et al. Reduced left ventricular ejection fraction in patients with aortic stenosis. J Am Coll Cardiol. (2018) 71:1313–21. doi: 10.1016/j.jacc.2018.01.045
25. Chin CWL, Everett RJ, Kwiecinski J, Vesey AT, Yeung E, Esson G, et al. Myocardial fibrosis and cardiac decompensation in aortic stenosis. JACC Cardiovasc Imaging. (2017) 10:1320–33. doi: 10.1016/j.jcmg.2016.10.007
26. Galli E, Lancellotti P, Sengupta PP, Donal E. LV mechanics in mitral and aortic valve diseases :value of functional assessment beyond ejection fraction. JACC: Cardiovasc Imaging. (2014) 7:151–66. doi: 10.1016/j.jcmg.2014.07.015
27. Ng ACT, Prihadi EA, Antoni ML, Bertini M, Ewe SH, Ajmone Marsan N, et al. Left ventricular global longitudinal strain is predictive of all-cause mortality independent of aortic stenosis severity and ejection fraction. Eur Hear J - Cardiovasc Imaging. (2018) 19:859–67. doi: 10.1093/ehjci/jex189
28. Magne J, Cosyns B, Popescu BA, Carstensen HG, Dahl J, Desai MY, et al. Distribution and prognostic significance of left ventricular global longitudinal strain in asymptomatic significant aortic stenosis an individual participant data meta-analysis. JACC: Cardiovasc Imag. (2019) 12:84–92. doi: 10.1016/j.jcmg.2018.11.005
Keywords: aortic stenosis, paradoxical low-flow low-gradient, echocardiography, aortic valve surgery, heart valve disease
Citation: Galian-Gay L, Escalona Silva RA, Teixidó-Turà G, Casas G, Ferrer-Sistach E, Mitroi C, Mingo S, Monivas V, Saura D, Vidal B, Trasca L, Moral S, Calvo F, Castiñeira Busto M, Sánchez V, Gonzalez A, Guzman G, Mora MN, Arnau Vives M, Peteiro J, Bouzas A, Mas-Stachurska A, González-Alujas T, Gutiérrez L, Fernandez-Galera R, Valente F, Guala A, Ruiz-Muñoz A, Avilés CAS, Palomares JFR, Ferreira I and Evangelista A (2022) Prognosis of Paradoxical Low-Flow Low-Gradient Aortic Stenosis: A Severe, Non-critical Form, With Surgical Treatment Benefits. Front. Cardiovasc. Med. 9:852954. doi: 10.3389/fcvm.2022.852954
Received: 11 January 2022; Accepted: 07 February 2022;
Published: 01 April 2022.
Edited by:
Ronak Rajani, Guy's and St Thomas' NHS Foundation Trust, United KingdomReviewed by:
Choon Hwai Yap, Imperial College London, United KingdomCopyright © 2022 Galian-Gay, Escalona Silva, Teixidó-Turà, Casas, Ferrer-Sistach, Mitroi, Mingo, Monivas, Saura, Vidal, Trasca, Moral, Calvo, Castiñeira Busto, Sánchez, Gonzalez, Guzman, Mora, Arnau Vives, Peteiro, Bouzas, Mas-Stachurska, González-Alujas, Gutiérrez, Fernandez-Galera, Valente, Guala, Ruiz-Muñoz, Avilés, Palomares, Ferreira and Evangelista. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Artur Evangelista, YXJ0dXJldmFuZ2VsaXN0YW1hc2lwQGdtYWlsLmNvbQ==; Ignacio Ferreira, bmFjaG9mZXJyZWlyYUBzZWNhcmRpb2xvZ2lhLmVz
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.