
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Cardiovasc. Med., 25 April 2022
Sec. Cardiovascular Epidemiology and Prevention
Volume 9 - 2022 | https://doi.org/10.3389/fcvm.2022.847982
This article is part of the Research TopicWomen in Cardiovascular Epidemiology and PreventionView all 35 articles
 Helena Tizón-Marcos1,2,3,4*
Helena Tizón-Marcos1,2,3,4* Beatriz Vaquerizo1,2,3,4,5
Beatriz Vaquerizo1,2,3,4,5 Josepa Mauri Ferré6,7Núria Farré1,2,3,4,5Rosa-Maria Lidón4,8Joan Garcia-Picart9Ander Regueiro10Albert Ariza11Xavier Carrillo6Xavier Duran3,12
Josepa Mauri Ferré6,7Núria Farré1,2,3,4,5Rosa-Maria Lidón4,8Joan Garcia-Picart9Ander Regueiro10Albert Ariza11Xavier Carrillo6Xavier Duran3,12 Paul Poirier13Mercè Cladellas1,2,3,5Anna Camps-Vilaró3,4Núria Ribas1,2,3,5Hector Cubero-Gallego1,2,3Jaume Marrugat3,4
Paul Poirier13Mercè Cladellas1,2,3,5Anna Camps-Vilaró3,4Núria Ribas1,2,3,5Hector Cubero-Gallego1,2,3Jaume Marrugat3,4Background: Despite the spread of ST-elevation myocardial infarction (STEMI) emergency intervention networks, inequalities in healthcare access still have a negative impact on cardiovascular prognosis. The Family Income Ratio of Barcelona (FIRB) is a socioeconomic status (SES) indicator that is annually calculated. Our aim was to evaluate whether SES had an effect on mortality and complications in patients managed by the “Codi IAM” network in Barcelona.
Methods: This is a cohort study with 3,322 consecutive patients with STEMI treated in Barcelona from 2010 to 2016. Collected data include treatment delays, clinical and risk factor characteristics, and SES. The patients were assigned to three SES groups according to FIRB score. A logistic regression analysis was conducted to estimate the adjusted effect of SES on 30-day mortality, 30-day composite cardiovascular end point, and 1-year mortality.
Results: The mean age of the patients was 65 ± 13% years, 25% were women, and 21% had diabetes mellitus. Patients with low SES were younger, more often hypertensive, diabetic, dyslipidemic (p < 0.003), had longer reperfusion delays (p < 0.03) compared to participants with higher SES. Low SES was not independently associated with 30-day mortality (OR: 0.95;9 5% CI: 0.7–1.3), 30-day cardiovascular composite end point (OR: 1.03; 95% CI: 0.84–1.26), or 1-year all-cause mortality (HR: 1.09; 95% CI: 0.76–1.56).
Conclusion: Although the low-SES patients with STEMI in Barcelona city were younger, had worse clinical profiles, and had longer revascularization delays, their 30-day and 1-year outcomes were comparable to those of the higher-SES patients.
Ischaemic heart disease is the leading component of cardiovascular disease (CVD), which is the first cause of mortality and morbidity worldwide (1, 2). Loss in quality-of-life and mortality due to cardiovascular disease has globally declined because of the implementation of evidence-based treatments and early and efficient management of acute coronary syndromes (ACSs), as well as appropriate drugs for secondary prevention and cardiac rehabilitation (3). Improvements in morbidity and survival after an ACS have spread unevenly throughout world regions, and they are more developed and implemented often in high-income countries (4). These differences may be partially explained by varying ACS emergency management modalities and population epidemiologic settings, including the influence of socioeconomic status (SES).
Multiple studies have shown that SES, measured by education level, occupation, or income, is associated with cardiovascular risk factors and outcomes after acute myocardial infarction (5–7). Even in high-income countries, poor socioeconomic circumstances may limit access to and increase delays in revascularization procedures, resulting in larger infarct size, lower compliance to secondary prevention drugs, and in general, poor application of and compliance with specialized state-of-the-art cardiac treatments (8, 9).
Implementation of coordinated and standardized treatment networks for acute ST-elevation myocardial infarction (STEMI) increases detection, decreases treatment times, and increases survival in all kinds of socioeconomic environments (6, 10).
The aim of this study was to analyze whether low SES determines more 30-day complications and 1-year all-cause mortality in patients with STEMI managed by the “Codi Infart Agut de Miocardi amb Elevació ST (Codi IAM)” emergency STEMI care network in Barcelona in a contemporary cohort from a European southern city.
In this retrospective cohort study, we included patients from the registry of the “Codi IAM” emergency management network diagnosed with STEMI from 2010 to 2016 who were residents of Barcelona. The registry includes, in addition, cardiac arrest or patients who died with an initial electrocardiogram showing ST-segment elevation or patients with a new left bundle-branch block. Barcelona patients were treated in other facilities outside Barcelona and non-residents were excluded.
The “Codi IAM” STEMI emergency management network was launched in 2010 in a region of 7.6 million inhabitants. The three main objectives of the network were (i) to increase the rate of reperfusion therapy among patients with STEMI, (ii) to achieve primary percutaneous coronary intervention (PPCI) in less than 120 min from the first contact with the health system (3), and (iii) to monitor the results of the network with a registry. The city of Barcelona was the first to be completely covered by the network because of its high-density population. Three PPCI hospitals that are open 24 h/7 days a week and one hospital with daytime PPCI cover the city's STEMI management needs. Updated operating details of the network have been recently published by our group (11). Basically, an emergency medical service (EMS) is responsible for detecting patients with STEMI and coordinates facilities (EMS ambulances and helicopters, with PPCI hospitals).
ST-elevation myocardial infarction was defined according to current guidelines (3). Fibrinolysis was only considered if expected delays in PPCI treatment were not acceptable and there were no contraindications. Percutaneous coronary intervention (PCI) post-fibrinolysis was initially only considered in the absence of effective reperfusion. The local health system provides universal health coverage; in addition, it provides a partial subsidy for medication costs depending on patients' income and working status.
The registry of the “Codi IAM” activity started in 2010 and includes demographic, clinical, therapeutic, and discharge data collected in an electronic form from patients with STEMI occurring within the previous 12 h. Epicardial coronary flow in the culprit STEMI artery is graded according to Thrombolysis in Myocardial Infarction (TIMI) flow grade (12), and reperfusion is considered optimal when TIMI 3 flow is obtained in the culprit lesion. Data collection was extended to new variables in 2012 (acute pulmonary edema, number of diseased vessels, and TIMI flow) and in 2015 (hypertension, dyslipidemia, smoking status, previous stroke, previous treatment, and type and number of stents). Bleeding was included only in cases requiring transfusion.
The Family Income Ratio of Barcelona (FIRB) is an indicator of the mean income ratio of inhabitants of the 73 districts in Barcelona city and shows imbalances relative to the mean value of the city, which is set at 100. The FIRB has been calculated annually since 2007 by the Technical Office of the Barcelona City Council, and it can be accessed online (13). This indicator combines five concepts: i) ratio of university graduates, ii) ratio of unemployed to employable inhabitants, iii) the number of vehicles per inhabitant, iv) engine power of new vehicles acquired, and v) price of second-hand housing. FIRB was assigned to patients according to their address and district affiliation, and it has been used as a surrogate of socioeconomic status (SES) in this study. The patients were assigned to three SES classes according to the FIRB classification used by the Technical Office: low SES (low and very low SES corresponding to FIRB values below 80), mid SES (mid-low and mid-high corresponding to FIRB values from 81 to 125), and high SES (high and very high SES corresponding to FIRB values from 126 to 159) (13).
Mortality data of the patients were obtained from the National Mortality Registry. The quality of the data included in the registry is periodically verified by external audits.
Primary assessment end points were 30-day mortality, a 30-day composite end point including death, ventricular fibrillation, pulmonary edema, or cardiogenic shock during admission, and 1-year all-cause mortality in 30-day survivors.
Categorical variables are shown as numbers and percentages; continuous variables are shown as mean and SD or as median and interquartile range, or as specified otherwise.
Patient characteristics and treatment times were compared according to each end point. Student's t-test or Mann-Whitney U-test was conducted for continuous variables and Chi-squared test, Fisher exact test, or ANOVA for categorical variables; p-tendency was used in all comparisons. A p-value < 0.05 was considered statistically significant. The association between SES and 30-day death or complications was evaluated with odds ratios (ORs) calculated using logistic regression models, and 1-year mortality in 30-day survivors was evaluated with hazard ratios (HRs) using Cox proportional-hazards regression models. The models were adjusted considering confounding variables associated with STEMI prognosis, which had <8% missing values: age, sex, diabetes mellitus, recruitment year, type of initial care, place of treatment, time from electrocardiogram to PPCI, and Killip class. Kaplan Meier survival curves were fitted for the three SES categories, and log-ranked p-values were used for comparison.
The Patients were assigned to the hospital where they spent most of their hospital stay.
In order to calculate 1-year mortality, the mortality of patients admitted in 2016 was analyzed up to 2017. Analyses were performed using SPSS software version 24.0. This project was approved by the ethics committee of Hospital del Mar (2020/9056), and all data are anonymous. The project was approved by the Scientific Committee of “Codi IAM”. Procedures and data collection complied with the Declaration of Helsinki and Spanish data protection laws.
The distribution of patients with STEMI treated in Barcelona city according to their SES is shown in Figure 1, in Figure 1: 43.4% had low SES, 41.1% had mid SES, and 15.4% had high SES. The annual hospitalization rate of patients with STEMI is shown in Supplementary Material 1. The number of patients with STEMI treated from the lowest SES was higher than the mean rate during the 7 years of the study.
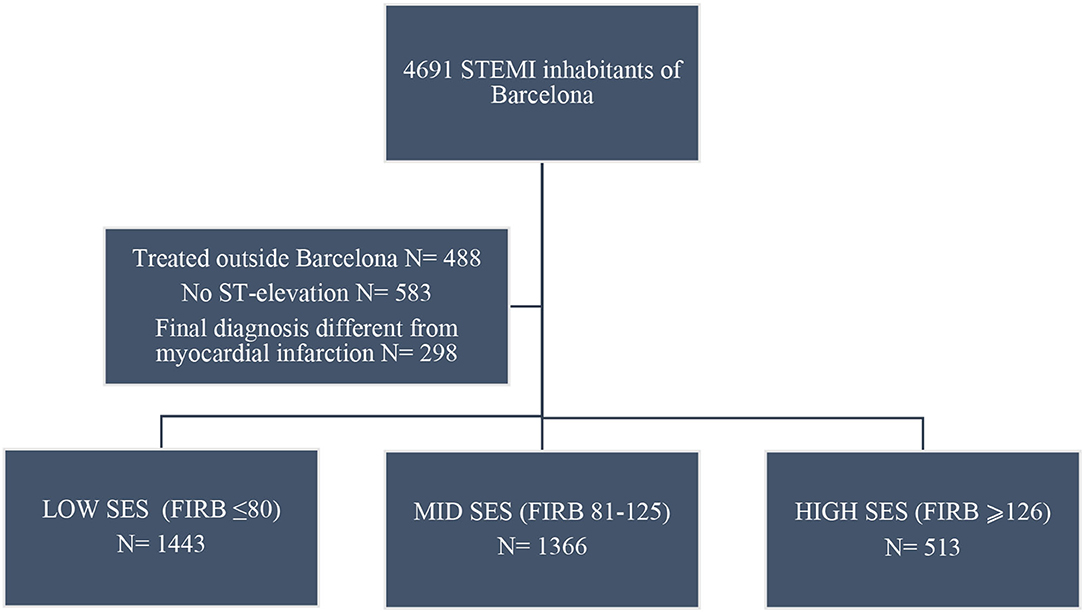
Figure 1. “Codi IAM” ST-elevation myocardial infarction (STEMI) patient inclusion flowchart.
Patients with low SES were younger, had a higher prevalence of cardiovascular risk factors, and were more often initially cared for by general practitioners (Table 1). In addition, they had a more deleterious cardiovascular risk factor profile than patients with higher SES. There was no difference in Killip class at STEMI presentation by SES.
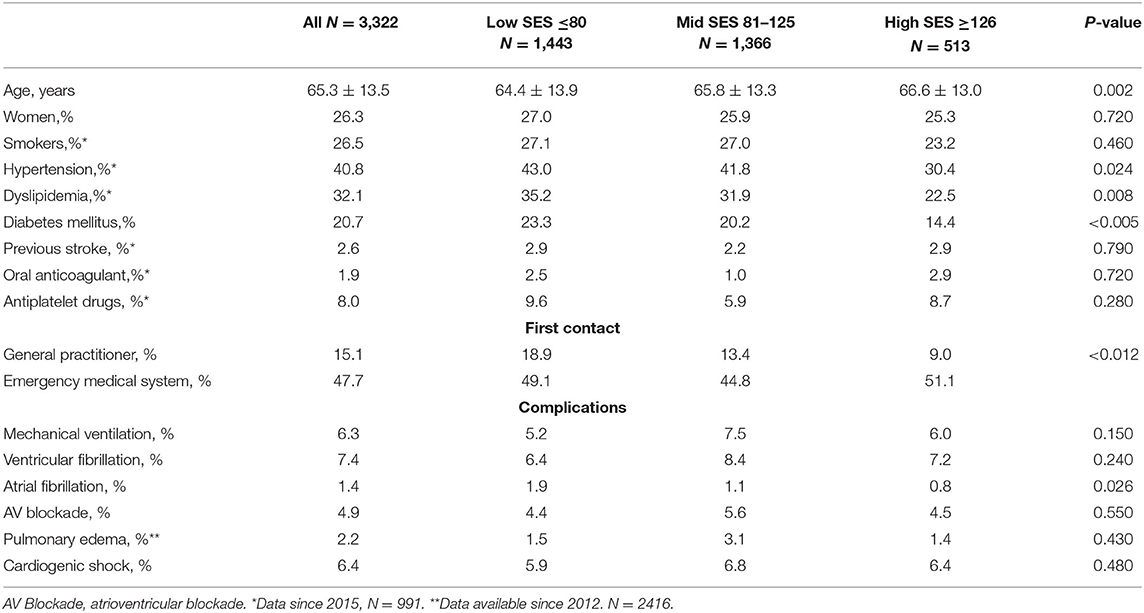
Table 1. Baseline clinical characteristics according to socioeconomic status (SES) classification.
Patients received PPCI as the first treatment in more than 93% of the cases but with no significant differences according to SES. Patients with higher SES had significant epicardial coronary disease significantly less often than those with mid and low SES (Table 2). Patients with lower SES had a tendency to be less often treated with drug-eluting stents (DESs) than those with mid and higher SES (55.1 vs. 57.5 vs. 69%, respectively, p < 0.35). Supplementary Material 2 shows differences in patients treated with DESs vs. bare-metal stents (BMS). DESs are significantly less used in the lower SES group; nevertheless, this difference is not greater than one unit.
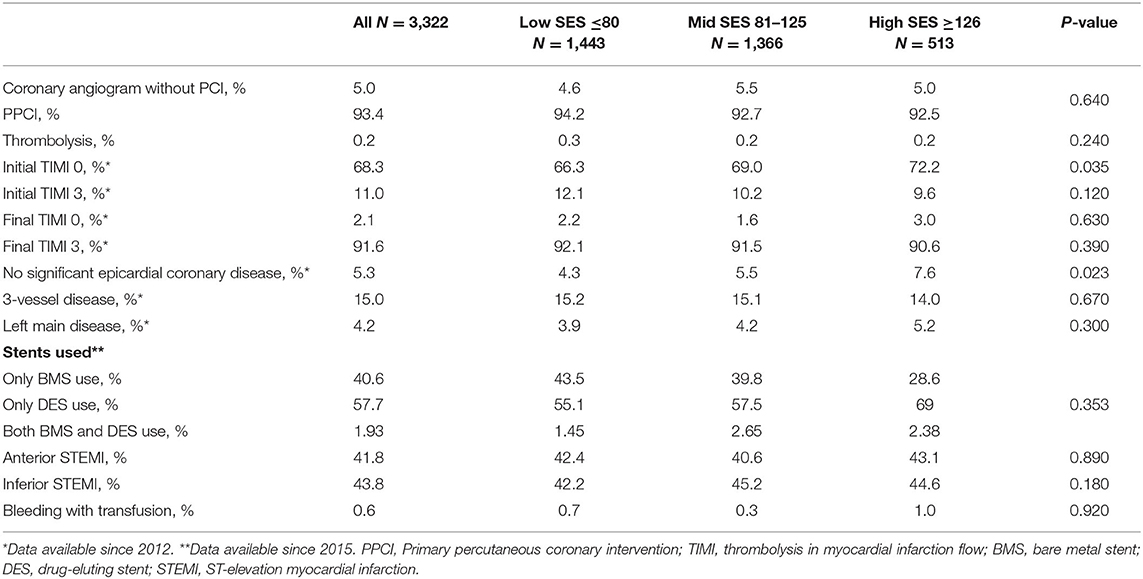
Table 2. Primary reperfusion procedure in the “Codi IAM” network during the period 2010–2016 according to SES.
Patients with lower SES had longer delays regarding time from symptom onset to diagnosis (first electrocardiogram) than those with highest SES (Table 3), and longer times from symptom onset to PPCI hospital than the mid and high SES groups. Electrocardiogram-to-open-artery times showed a decreasing trend with SES. Longer ischemic times were observed in patients with lower SES. Accordingly, ratios of PPCI in less than 120 min were higher in those patients with higher SES compared to those with lower SES.
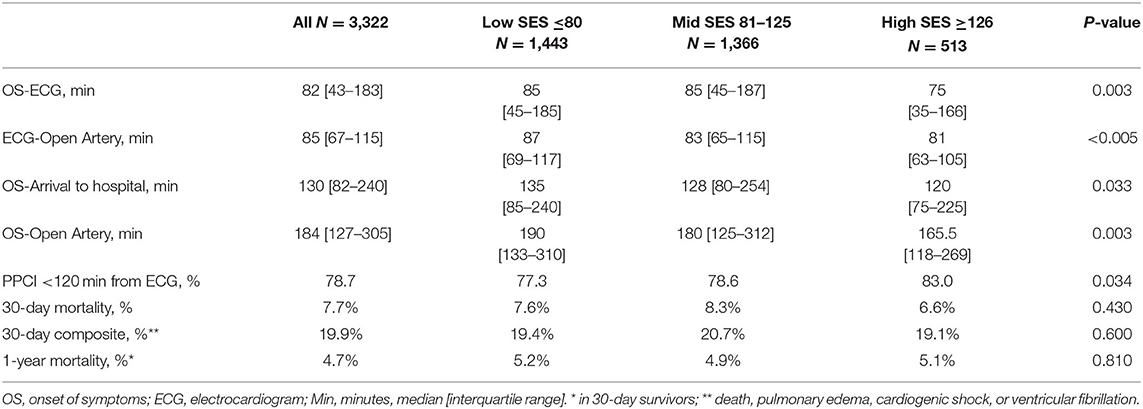
Table 3. Delays in initial medical care, diagnosis, and revascularization according to SES during the period 2010–2016.
In Table 4, we show that 30-day mortality, 30-day cardiovascular complications, and 1-year mortality did not differ between the SES groups after adjusting for confounding factors. There were no significant differences in survival curves at 1-year according to SES (Figure 2).
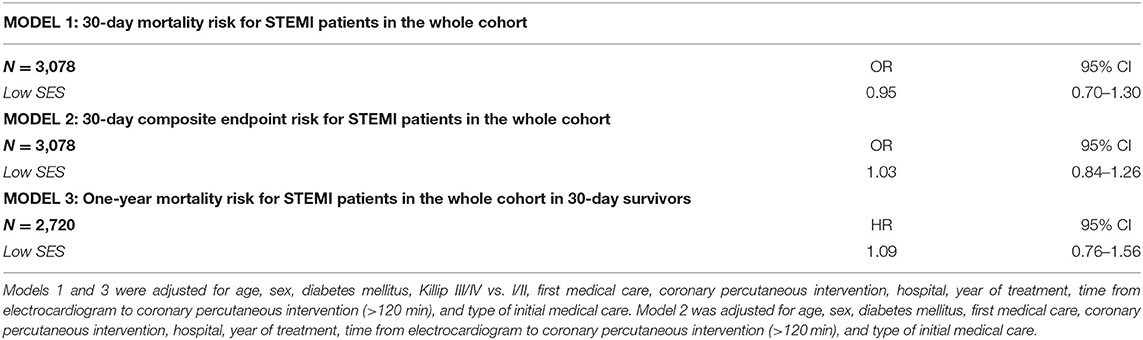
Table 4. Low-SES patients with ST-elevation myocardial infarction (STEMI) adjusted odds ratio (OR) of 30-day mortality (model 1); a 30-day composite end point (death, ventricular fibrillation, acute pulmonary edema, or cardiogenic shock) (model 2); and hazard ratio (HR) of 1-year mortality in 30-day survivors (model 3) in the “Codi IAM” network during the 2010-2016 period.
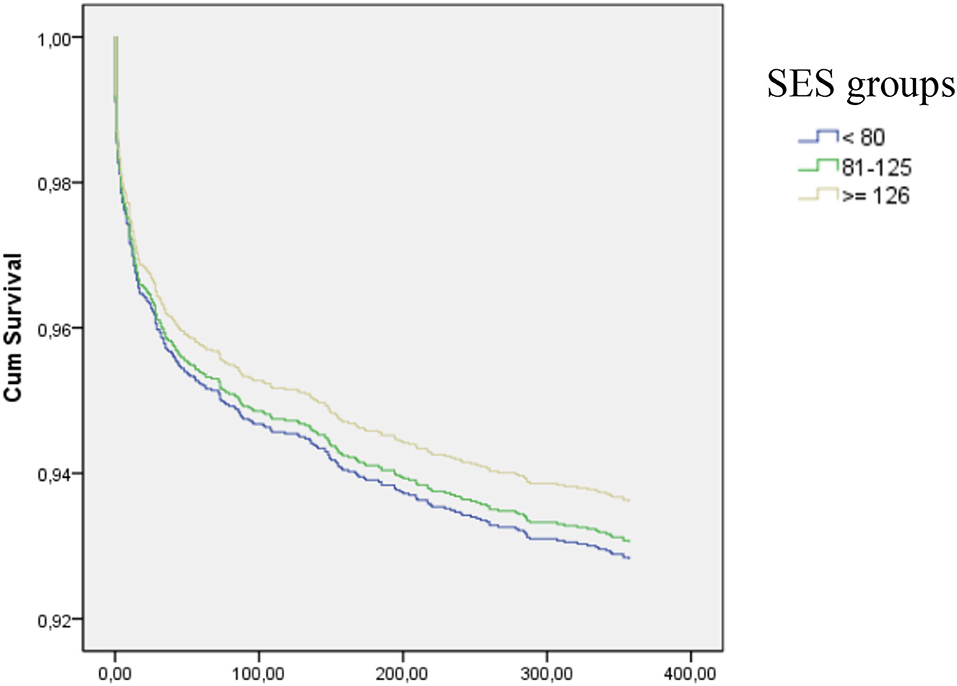
Figure 2. Cumulative survival according to socioeconomic status (SES). Global log-ranked p-values = 0.79; mid SES vs. low SES = 0.78; high SES vs. low SES = 0.49.
Low-SES patients with STEMI treated in Barcelona by the “Codi IAM” emergency network have a higher burden of cardiovascular risk factors and longer treatment delays than patients with higher SES. Despite this, they have similar mortality or cardiovascular complication rate at 30 days and similar 1-year mortality.
Recent STEMI guidelines have emphasized the importance of performing research addressing gaps in knowledge and the need for observational data and real-world evidence to ensure high-quality rapid and equal care for patients with STEMI in geographic areas (14). Previous studies from the late 1990s and early new century showed that SES was associated with both short- and long-term mortalities after ACS (15) and that an inverse trend in survival after myocardial infarction was also observed with SES levels in district-based studies (16, 17). However, these data come from heterogeneous studies, different time frames and may reflect inequalities in disease incidence, access to healthcare systems, and poor compliance with secondary prevention medications (18). Moreover, different SES indicators were used in previous studies: household income (14), highest educational level (15), geographical area (18), racial aspects (16), and various composite indexes (17, 19–21). Composite indexes can include varying combinations of household income, educational level, unemployment rate, vehicle ownership and engine power, prices of housing, the proportion of families with > 4 children, community services, environmental conditions, and crime level. These composites indexes reflect a multilevel stratum of social, educational, and economic data, which can give a better picture of concurring effects that determine health, acute and chronic treatments, and follow-up compared to strictly economic information.
Studies from various geographical areas have found that access to revascularization procedures is reduced in groups with lower SES (22). The population analyzed in this study represents a sample of homogeneously treated patients with STEMI: mostly (>93%) treated by PPCI in a public integrated medical system and features the inclusion of patients not treated with PPCI. The use of PPCI methods in patients with STEMI varies largely by region and can be explained by several factors such as supply factors, the number of physicians, and the number of available hospitalization beds for acute conditions, as well as constraining measures and “patient-level” factors (10). However, the standardization of treatments driven by new evidence-based medicine and consequent guidelines allows countries with different income levels to progressively organize emergency networks for the early management of high-impact diseases in terms of incidence, hospitalization, and case fatality such as in STEMI (23, 24).
Network organization and public access to care and health may result in the neutralization of both higher incidence of the disease and adverse clinical baseline characteristics in low SES groups (25, 26). In our study, the low SES group had a worse cardiovascular profile, longer treatment delays, and different access routes to the health system, which did not, however, translate into worsened 30-day complications or 1-year mortality. Besides, when adjusting for potential confounders, SES data were not associated with either end points, suggesting that a robust healthcare system may flatten socioeconomic baseline disparity potential effect. Similar findings have been described in international cohorts in different studies performed in a single-center fashion (22), in groups of hospitals within a geographical area (20, 26), or within a city (17). Those studies have in common the inclusion of patients with STEMI treated with PPCI as a standard treatment within a structural public STEMI network and showed no interaction of SES with mortality. However, most of these registries reported results from cohorts of patients before 2010. Other previous registries also included patients with other conditions such as non-ST-elevation myocardial infarction (21) or excluded patients treated with fibrinolysis (27). Exclusion of patients treated with fibrinolysis or patients who did not receive PPCI may, however, bias the results of any study aiming to clarify the importance of socioeconomic factors in STEMI prognosis because of the geographical gradient toward the periphery for lower-income groups and its relationship with the optimal timing of treatment for PPCI (17, 28, 29).
The lower tendency of use of DESs in the low-SES group observed in our study has also been reported in American cohorts (30–32), which is a “treatment-risk paradox” in which higher-risk patients are not treated with optimal or evidence-based strategies, and the use of mechanical support devices is reduced, and it may result in prognosis worsening (19, 33, 34). This finding may reflect the fact that differences in outcomes may not only be related to the use of a specific treatment/device in the acute period but to a whole standardized medical approach in which access to secondary prevention may be of utmost importance (35) and that the health system may override the burden of higher risk subsets.
Our study has several limitations. First, the data are derived from the first 7 years of implementation of a regional STEMI network, and its registry has evolved over the years and includes progressively more detailed data such as treated hypertension, treated dyslipidemia, smoking status, previous stroke, number and type of stents, and LV function. Moreover, there were no available records on the medical treatment administered during the index admission, at discharge, and/or regarding other therapies during follow-up such as cardiovascular rehabilitation. These treatments as well as the patients' adherence to prescriptions have been shown to have a direct impact on mortality (35, 36) and may also be related to socioeconomic conditions (21). Finally, the FIRB is a composite index that aggregates data from all inhabitants of a given district, so it does not allow analyzing effects of individual-level SES. However, the FIRB as a surrogate of SES by zip code results in a useful tool. Several prior studies have validated this approach of imputing individual SES in epidemiologic studies reflecting aggregate characteristics of a population and prevailing habits as well as its environmental attributes (such as available health resources) that impact its residents' health (37, 38).
Barcelona citizens with lower SES who are admitted with STEMI show more unfavorable clinical and cardiovascular risk factor features than citizens with higher SES. Nevertheless, the “Codi IAM” emergency network for STEMI management documented similar 30-day complications and 1-year mortality regardless of SES suggesting that a robust healthy system may override baseline adverse patients' characteristics.
The datasets presented in this article are not readily available because the dataset belongs to Departament de Salut, Generalitat de Catalunya, and the researchers only have access to statistical analysis.
The studies involving human participants were reviewed and approved by Hospital del Mar Ethics Committee. The patients/participants provided their written informed consent to participate in this study.
HT-M: study management, data collection, interpretation of collected data, and preparation of the manuscript. BV: critical revisions of the manuscript. JM: participation in study management and acquisition of data and revision of the manuscript. RL, AA, and NF: critical revisions of the manuscript and data collection. XC: revision of the manuscript and data collection. JG-P, AR, MC, AC-V, XD, NR, and HC-G: revision of the manuscript. PP: extensive revision of the manuscript. JM: study management, interpretation of collected data, statistical analysis, and extensive revision of the manuscript.
This project was supported by the CIBERCV of research on cardiovascular diseases personnel hired with its resources.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
We would like to thank Isaac Aparicio Verdoy and Marius Boada from Oficina Municipal de Dades, Ajuntament de Barcelona, and Josep Jimenez, from Departament de Salut, Generalitat de Catalunya for data management, and Marina Lee Crombie for the English revision. Part of this article appeared on the doctoral thesis of the corresponding author.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fcvm.2022.847982/full#supplementary-material
ACS, Acute coronary syndrome; BMS, bare-metal stent; CHD, coronary heart disease; DES, drug-eluting stent; ECG, electrocardiogram; EMS, emergency medical system; FIRB, Family Income Ratio of Barcelona; OSs, onset of symptoms; PCI, percutaneous coronary intervention; PPCI, primary percutaneous coronary intervention; SES, socioeconomic status; STEMI, ST-elevation myocardial infarction; TIMI, thrombolysis in myocardial infarction.
1. Roth GA, Johnson C, Abajobir A, Abd-Allah F, Abera SF, Abyu G, et al. Global, Regional, and National Burden of Cardiovascular Diseases for 10 Causes, 1990 to 2015. J Am Coll Cardiol. (2017) 70:1–25. doi: 10.1016/j.jacc.2017.04.052
2. Organization WH. Global Health Estimates 2016: Deaths by Cause, Age, Sex, by Country and by Region, 2000-2016. In: Organization WH, editor. Geneva: World Health Organization.
3. Ibanez B, James S, Agewall S, Antunes MJ, Bucciarelli-Ducci C, Bueno H, et al. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: The Task Force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur Heart J. (2018) 39:119–77. doi: 10.1093/eurheartj/ehx393
4. Moran AE, Forouzanfar MH, Roth GA, Mensah GA, Ezzati M, Murray CJ, et al. Temporal trends in ischemic heart disease mortality in 21 world regions, 1980 to 2010: the Global Burden of Disease 2010 study. Circulation. (2014) 129:1483–92. doi: 10.1161/CIRCULATIONAHA.113.004042
5. Kaplan GA, Keil JE. Socioeconomic factors and cardiovascular disease: a review of the literature. Circulation. (1993) 88:1973–98. doi: 10.1161/01.CIR.88.4.1973
6. Kampfer J, Yagensky A, Zdrojewski T, Windecker S, Meier B, Pavelko M, et al. Long-term outcomes after acute myocardial infarction in countries with different socioeconomic environments: an international prospective cohort study. BMJ Open. (2017) 7:e012715. doi: 10.1136/bmjopen-2016-012715
7. Rao SV, Schulman KA, Curtis LH, Gersh BJ, Jollis JG. Socioeconomic status and outcome following acute myocardial infarction in elderly patients. Arch Intern Med. (2004) 164:1128–33. doi: 10.1001/archinte.164.10.1128
8. Rosvall M, Chaix B, Lynch J, Lindstrom M, Merlo J. The association between socioeconomic position, use of revascularization procedures and five-year survival after recovery from acute myocardial infarction. BMC Public Health. (2008) 8:44. doi: 10.1186/1471-2458-8-44
9. Hawkins NM, Scholes S, Bajekal M, Love H, O'Flaherty M, Raine R, et al. The UK National Health Service: delivering equitable treatment across the spectrum of coronary disease. Circ Cardiovasc Qual Outcomes. (2013) 6:208–16. doi: 10.1161/CIRCOUTCOMES.111.000058
10. Yusuf S, Rangarajan S, Teo K, Islam S, Li W, Liu L, et al. Cardiovascular risk and events in 17 low-, middle-, and high-income countries. N Engl J Med. (2014) 371:818–27. doi: 10.1056/NEJMoa1311890
11. Tizon-Marcos H, Vaquerizo B, Marrugat J, Ariza A, Carrillo X, Munoz JF, et al. Differences in 30-day complications and 1-year mortality by sex in patients with a first STEMI managed by the Codi IAM network between 2010 and 2016. Rev Esp Cardiol (Engl Ed). (2020). doi: 10.1016/j.rec.2020.06.002
12. Group TS. The Thrombolysis in Myocardial Infarction (TIMI) trial. Phase I findings N Engl J Med. (1985) 312:932–6. doi: 10.1056/NEJM198504043121437
13. Barcelona Ad, Economia B. Any 2016 - Distribució Territorial de la Renda Familiar Disponible per Càpita a Barcelona- (Desembre de 2017) Any 2015 - Distribució Territorial de la Renda Familiar Disponible per Càpita a Barcelona- (Desembre de 2016) Any 2014 - Distribució Territorial de la Renda Familiar Disponible per Càpita a Barcelona- (Desembre de 2015) Any 2013 - Distribució Territorial de la Renda Familiar Disponible per Càpita a Barcelona - (Desembre de 2014) Any 2012 - Distribució Territorial de la Renda Familiar Disponible per Càpita a Barcelona - (Gener de 2014) Any 2011 - Barcelona Economia n.80 (nov. de 2012) Any 2010 - Barcelona Economia n.77 (nov. de 2011). In: Programació Gtd, Programació DdEi, editors. Barcelona: Ajuntament de Barcelona (2010-2016).
14. van Oeffelen AA, Agyemang C, Bots ML, Stronks K, Koopman C, van Rossem L, et al. The relation between socioeconomic status and short-term mortality after acute myocardial infarction persists in the elderly: results from a nationwide study. Eur J Epidemiol. (2012) 27:605–13. doi: 10.1007/s10654-012-9700-z
15. Igland J, Vollset SE, Nygard OK, Sulo G, Sulo E, Ebbing M, et al. Educational inequalities in 28 day and 1-year mortality after hospitalisation for incident acute myocardial infarction–a nationwide cohort study. Int J Cardiol. (2014) 177:874–80. doi: 10.1016/j.ijcard.2014.10.045
16. Bucholz EM, Ma S, Normand SL, Krumholz HM. Race, socioeconomic status, and life expectancy after acute myocardial infarction. Circulation. (2015) 132:1338–46. doi: 10.1161/CIRCULATIONAHA.115.017009
17. Biswas S, Andrianopoulos N, Duffy SJ, Lefkovits J, Brennan A, Walton A, et al. Impact of socioeconomic status on clinical outcomes in patients with st-segment-elevation myocardial infarction. Circ Cardiovasc Qual Outcomes. (2019) 12:e004979. doi: 10.1161/CIRCOUTCOMES.118.004979
18. Stirbu I, Looman C, Nijhof GJ, Reulings PG, Mackenbach JP. Income inequalities in case death of ischaemic heart disease in the Netherlands: a national record-linked study. J Epidemiol Community Health. (2012) 66:1159–66. doi: 10.1136/jech-2011-200924
19. Steele L, Palmer J, Lloyd A, Fotheringham J, Iqbal J, Grech ED. Impact of socioeconomic status on survival following ST-elevation myocardial infarction in a universal healthcare system. Int J Cardiol. (2019) 276:26–30. doi: 10.1016/j.ijcard.2018.11.111
20. Denvir MA, Lee AJ, Rysdale J, Walker A, Eteiba H, Starkey IR, et al. Influence of socioeconomic status on clinical outcomes and quality of life after percutaneous coronary intervention. J Epidemiol Community Health. (2006) 60:1085–8. doi: 10.1136/jech.2005.044255
21. Shimony A, Zahger D, Ilia R, Shalev A, Cafri C. Impact of the community's socioeconomic status on characteristics and outcomes of patients undergoing percutaneous coronary intervention. Int J Cardiol. (2010) 144:379–82. doi: 10.1016/j.ijcard.2009.04.033
22. Britton A, Shipley M, Marmot M, Hemingway H. Does access to cardiac investigation and treatment contribute to social and ethnic differences in coronary heart disease? Whitehall II prospective cohort study. BMJ. (2004) 329:318. doi: 10.1136/bmj.38156.690150.AE
23. Radovanovic D, Maurer L, Bertel O, Witassek F, Urban P, Stauffer JC, et al. Treatment and outcomes of patients with recurrent myocardial infarction: a prospective observational cohort study. J Cardiol. (2016) 68:498–503. doi: 10.1016/j.jjcc.2015.11.013
24. Galappatthy P, Bataduwaarachchi VR, Ranasinghe P, Galappatthy GKS, Wijayabandara M, Warapitiya DS, et al. Management, characteristics and outcomes of patients with acute coronary syndrome in Sri Lanka. Heart. (2018) 104:1424–31. doi: 10.1136/heartjnl-2017-312404
25. Agarwal S, Garg A, Parashar A, Jaber WA, Menon V. Outcomes and resource utilization in ST-elevation myocardial infarction in the United States: evidence for socioeconomic disparities. J Am Heart Assoc. (2014) 3:e001057. doi: 10.1161/JAHA.114.001057
26. Pancholy S, Patel G, Pancholy M, Nanavaty S, Coppola J, Kwan T, et al. Association between health insurance status and in-hospital outcomes after ST-segment elevation myocardial infarction. Am J Cardiol. (2017) 120:1049–54. doi: 10.1016/j.amjcard.2017.06.041
27. Fournier S, Muller O, Ludman AJ, Lauriers N, Eeckhout E. Influence of socioeconomic factors on delays, management and outcome amongst patients with acute myocardial infarction undergoing primary percutaneous coronary intervention. Swiss Med Wkly. (2013) 143:w13817. doi: 10.4414/smw.2013.13817
28. Terkelsen CJ, Sorensen JT, Maeng M, Jensen LO, Tilsted HH, Trautner S, et al. System delay and mortality among patients with STEMI treated with primary percutaneous coronary intervention. JAMA. (2010) 304:763–71. doi: 10.1001/jama.2010.1139
29. Kjaerulff TM, Bihrmann K, Andersen I, Gislason GH, Larsen ML, Ersboll AK. Geographical inequalities in acute myocardial infarction beyond neighbourhood-level and individual-level sociodemographic characteristics: a Danish 10-year nationwide population-based cohort study. BMJ Open. (2019) 9:e024207. doi: 10.1136/bmjopen-2018-024207
30. Hannan EL, Racz M, Walford G, Clark LT, Holmes DR, King SB, et al. Differences in utilization of drug-eluting stents by race and payer. Am J Cardiol. (2007) 100:1192–8. doi: 10.1016/j.amjcard.2007.05.039
31. Rao SV, Shaw RE, Brindis RG, Klein LW, Weintraub WS, Krone RJ, et al. Patterns and outcomes of drug-eluting coronary stent use in clinical practice. Am Heart J. (2006) 152:321–6. doi: 10.1016/j.ahj.2006.03.005
32. Yong CM, Abnousi F, Asch SM, Heidenreich PA. Socioeconomic inequalities in quality of care and outcomes among patients with acute coronary syndrome in the modern era of drug eluting stents. J Am Heart Assoc. (2014) 3:e001029. doi: 10.1161/JAHA.114.001029
33. Baumbach A, Heg D, Raber L, Ostoijc M, Brugaletta S, Strange JW, et al. Selective use of contemporary drug-eluting stents in primary angioplasty for ST-elevation myocardial infarction: pooled analysis of COMFORTABLE AMI and EXAMINATION. EuroIntervention. (2017) 12:1577–86. doi: 10.4244/EIJ-D-15-00408
34. Brugaletta S, Gomez-Lara J, Ortega-Paz L, Jimenez-Diaz V, Jimenez M, Jimenez-Quevedo P, et al. 10-year follow-up of patients with everolimus-eluting versus bare-metal stents after ST-segment elevation myocardial infarction. J Am Coll Cardiol. (2021) 77:1165–78. doi: 10.1016/j.jacc.2020.12.059
35. Szummer K, Wallentin L, Lindhagen L, Alfredsson J, Erlinge D, Held C, et al. Improved outcomes in patients with ST-elevation myocardial infarction during the last 20 years are related to implementation of evidence-based treatments: experiences from the SWEDEHEART registry 1995-2014. Eur Heart J. (2017) 38:3056–65. doi: 10.1093/eurheartj/ehx515
36. Hermann M, Witassek F, Erne P, Rickli H, Radovanovic D. Impact of cardiac rehabilitation referral on one-year outcome after discharge of patients with acute myocardial infarction. Eur J Prev Cardiol. (2019) 26:138–44. doi: 10.1177/2047487318807766
37. Krieger N. Overcoming the absence of socioeconomic data in medical records: validation and application of a census-based methodology. Am J Public Health. (1992) 82:703–10. doi: 10.2105/AJPH.82.5.703
Keywords: ST-elevation myocardial infarction, reperfusion, primary percutaneous coronary intervention, mortality, inequalities
Citation: Tizón-Marcos H, Vaquerizo B, Ferré JM, Farré N, Lidón R-M, Garcia-Picart J, Regueiro A, Ariza A, Carrillo X, Duran X, Poirier P, Cladellas M, Camps-Vilaró A, Ribas N, Cubero-Gallego H and Marrugat J (2022) Socioeconomic Status and Prognosis of Patients With ST-Elevation Myocardial Infarction Managed by the Emergency-Intervention “Codi IAM” Network. Front. Cardiovasc. Med. 9:847982. doi: 10.3389/fcvm.2022.847982
Received: 03 January 2022; Accepted: 18 March 2022;
Published: 25 April 2022.
Edited by:
Pietro Amedeo Modesti, University of Florence, ItalyReviewed by:
Jun Lyu, First Affiliated Hospital of Jinan University, ChinaCopyright © 2022 Tizón-Marcos, Vaquerizo, Ferré, Farré, Lidón, Garcia-Picart, Regueiro, Ariza, Carrillo, Duran, Poirier, Cladellas, Camps-Vilaró, Ribas, Cubero-Gallego and Marrugat. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Helena Tizón-Marcos, aHRpem9uQHBzbWFyLmNhdA==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.