
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Cardiovasc. Med. , 08 July 2022
Sec. Heart Failure and Transplantation
Volume 9 - 2022 | https://doi.org/10.3389/fcvm.2022.847450
This article is part of the Research Topic Role of Congestion in Heart Failure: from Bench to Clinical Practice View all 10 articles
 Jose Civera1,2†Gema Miñana1,2,3†
Jose Civera1,2†Gema Miñana1,2,3† Rafael de la Espriella1,2
Rafael de la Espriella1,2 Enrique Santas1,2Clara Sastre1,2Anna Mollar1,2Adriana Conesa1,2Ana Martínez1,2Eduardo Núñez1,2
Enrique Santas1,2Clara Sastre1,2Anna Mollar1,2Adriana Conesa1,2Ana Martínez1,2Eduardo Núñez1,2 Antoni Bayés-Genís3,4,5
Antoni Bayés-Genís3,4,5 Julio Núñez1,2,3*
Julio Núñez1,2,3*Aims: Venous leg compression (VLC) with elastic bandages has been proposed as a potentially useful strategy for decreasing tissue congestion. We aimed to evaluate the effect of VLC on short-term changes on intravascular refill, assessed by inferior vena cava (IVC) diameter in patients with worsening heart failure (WHF) requiring parenteral furosemide. Additionally, we sought to evaluate whether early changes in IVC were related to short-term decongestion.
Methods: This is a prospective study in which we included 20 consecutive ambulatory patients with WHF treated with subcutaneous furosemide and VLC for at least 72 h. The endpoints were (a) short-term changes in IVC, (b) the association between decongestion and 3-h IVC changes following VLC. Changes in continuous endpoints and their longitudinal trajectories were estimated with linear mixed regression models. All analyses were adjusted for multiple comparisons.
Results: Following administration of subcutaneous furosemide and VLC, we found a significant increase in 3-h IVC diameter (ΔIVC = 1.6 mm, CI 95%: 0.7–2.5; p < 0.001), with a greater increase in those with baseline IVC≤21 mm (2.4 vs. 0.8 mm; p < 0.001). 3-h intravascular refill (increase in IVC≥2 mm) was associated with greater decongestion (natriuresis, weight, peripheral edemas, and dyspnea) in those with baseline IVC≤21 mm but not when IVC>21 mm (p < 0.05 for all comparisons).
Conclusions: In this cohort of patients with congestive WHF treated with subcutaneous furosemide and VLC, we found a greater increase in short-term IVC in those with IVC ≤21 mm at baseline. In this subset of patients, a 3-h increase in IVC≥2 mm was associated with greater short-term decongestion.
Fluid overload explains most of the symptoms and signs of patients with worsening heart failure (WHF) (1, 2). Diuretics constitute the mainstay armamentarium in these patients, although the evidence endorsing the optimal diuretic strategy (intensity and sequence of the diuretic prescription) is scarce (3, 4). Optimal decongestion should imply tissue and vascular decongestion. However, at least in the short-term, most used interventions, such as parenteral diuretics, have a predominant effect by reducing intravascular congestion (3, 4). Several strategies have been postulated to mobilize extravascular volumes, such as infusion of loop diuretics and hypertonic solutions (sodium or albumin), without consistent evidence about their utility (5, 6). Venous leg compression (VLC) by using elastic bandages has been proposed as another potentially useful strategy for decreasing tissue congestion. However, its efficacy and safety in heart failure (HF) patients require a profound evaluation (7).
In this work, we sought to evaluate the association between VLC and short-term changes in intravascular refill and whether these changes are related to decongestion parameters in patients with WHF that require parenteral furosemide administration.
This is a one-arm open-label prospective study in which we included 20 consecutive ambulatory patients with WHF treated with subcutaneous furosemide and VLC for at least 72 h between January 1st, 2020, and June 1st, 2021, at an outpatient HF-Clinic in Spain (Hospital Clinic Universitari, Valencia-Spain). All patients received a subcutaneous furosemide infusion for the treatment of WHF. Patients were eligible if they presented with WHF with peripheral edema (at least grade 1+) that required parenteral ambulatory administration of furosemide. All patients had an established diagnosis of HF according to ESC guidelines (8). Exclusion criteria consisted of (a) acute decompensated HF requiring hospital admission (acute pulmonary edema, evidence of hypoxemia, defined as an oxygen saturation <90% in pulse oximetry or oxygen partial pressure <80 mmHg in arterial blood gas analysis), (b) cardiogenic shock, (c) symptomatic hypotension or any systolic blood pressure (SBP) <90 mmHg, and d) index event triggered by an uncontrolled arrhythmia (advanced heart block without a pacemaker, sustained ventricular tachycardia, therapeutic defibrillator shock, or atrial fibrillation/flutter with sustained ventricular response >150 bpm), infection/sepsis, or severe anemia (hemoglobin <7 g/dL), and patient that require hospitalization at clinician judgment. Patients on renal replacement therapy or ultrafiltration were also excluded. This study complied with the Declaration of Helsinki and was approved by the local institutional review committees. All patients signed an informed consent form.
Subcutaneous furosemide was administered by using a single-use, continuous infusion pump system (DOSI-FUSER®, Leventon, S.A.U, Barcelona, Spain) and a standard commercial subcutaneous infusion set. The infusion pump system consists of an elastomeric balloon inside a rigid container, an infusion line with the capillary device, and a Luer-lock connector that attaches to the standard subcutaneous infusion set. After the balloon is inflated, the medication flows through the capillary device due to the pressure from the elastomeric balloon, which determines the flow rate. We used an infusion pump containing a 250 mL balloon reservoir with a nominal continuous flow rate of 2.1 mL/h over 72 h.
Subcutaneous furosemide dose was calculated based on the subject's outpatient oral dose using a 1:1.25 conversion (80 mg of oral furosemide = 100 mg of subcutaneous furosemide). Therefore, for administering a daily dose of 100 mg of subcutaneous furosemide, a 2 mg/mL drug concentration was required (dilution: 500 mg of non-formulated furosemide in 250 mL of 0.9% sodium chloride). Specialized HF nurses filled the infusion system following the manufacturer's instructions, placed the subcutaneous catheter, and thoroughly explained general guidelines and troubleshooting to study participants.
Compression of the lower limbs was performed with a multi-component layer compression bandage system at a pressure of 20 mmHg (UrgoK2 LITE®) consisting of two dynamic components: an inelastic and elastic bandage. When combined, the two layers constitute one compression bandaging system that provides both a dynamic static stiffness profile and tolerable resting pressures. The first layer, KTech®, is an inelastic bandage (approximately 75% extensibility), consisting of viscose and polyester wadding with a knitted layer made of polyamide and elastane. When in contact with the skin, the KTech® layer distributes the pressure uniformly over the surface of the leg and provides compression, along with protection and absorbency when needed (9). Ktech® provides a high working pressure with a low resting pressure, which in combination with the action of the calf muscle creates a massage effect, assisting venous return and reducing edema levels. The second layer, KPress®, is an elastic cohesive bandage of approximately 160% extensibility, made from synthetic components, such as acrylic, polyamide, and elastane. This outer bandage provides the additional compression necessary to achieve the required therapeutic pressure and, more critically, maintains the recommended resting pressures necessary to maintain improved blood flow (9). These pressures are consistently maintained over time (during 7 days) (10). Each bandage layer displays an oval indicator (the PresSure® system, also known as the etalonnage) that expands into a circle when stretched correctly. Proper application is further enhanced by guides for appropriate overlap of layering. There are two different sizes of UrgoK2 LITE® according to the ankle perimeter (18–25 or 25–32 cm). For each patient, the ankle perimeter was measured, and the right size was selected.
The inferior vena cava (IVC) diameter was visualized by echography (11), with patients in the supine position, using subcostal 4 chamber view (midline, inferior to the xiphoid, angling to the right). The maximum IVC diameter during the respiratory cycle was measured approximately 3 cm before the merger with the right atrium. An IVC maximum diameter of >21 mm was defined as dilated IVC. IVC diameter was evaluated at baseline and 3, 24, 48, and 72 h after applying the compression bandage. A change in IVC at 3-h >2 mm was considered significant.
All patients were physically visited on the day of presentation, at 24, 48, and 72-h. At these encounters, we registered the New York Heart Association (NYHA) class, pedal edema, weight, and vital signs. The pedal edema was assessed by 1+ to 4+ grade (grade 1+: slight pitting 2 mm depth, grade 2+: somewhat deeper pit 4 mm, grade 3+: noticeably deep pit 6 mm, and grade 4+: very deep pit 8 mm), and by measuring the diameter of lower limbs 10 cm above the external malleolus. The mean diameter between both limbs was registered.
We also assessed dyspnea visual analog scale (VAS) and standard plasma laboratory data [estimated glomerular filtration rate (eGFR), plasma electrolytes (sodium and potassium), and amino-terminal pro-brain natriuretic peptide (NT-proBNP)] at presentation and 72-h. The dyspnea VAS scale of 0 corresponds to the patient's subjective feeling of “I can breathe normally,” and a dyspnea VAS score of 10 corresponds to “I can't breathe at all.” Spot urinary sodium was assessed each 24-h after treatment intervention, at 24, 48, and 72 h.
The endpoints were: a) changes in short-term IVC following administration of subcutaneous furosemide and VLC, and b) the relationship between 3-h changes in IVC and parameters of decongestion (natriuresis, pedal edema, weight, dyspnea VAS, and NT-proBNP). In addition, safety endpoints included changes in eGFR, SBP, electrolytes, and the proportion of patients that symptomatically did not tolerate the 72-h leg venous compression.
Continuous baseline variables were expressed as median [interquartile interval (IQI)]. Discrete variables were presented as numbers (percentages). Changes in continuous endpoints and their longitudinal trajectories were estimated with linear mixed regression models (LMRMs). Continuous exposures with a non-parametric distribution were log-transformed [NT-proBNP (lnNT-proBNP)]. Multivariate estimates were adjusted for age, sex, baseline eGFR, left ventricular ejection fraction (LVEF), and the baseline endpoint value regardless of their p-value. The LMRMs are presented as least square means (LSM) with their respective 95% confidence intervals. P-values were adjusted for multiple comparisons (Sidak procedure). A 2-sided p-value of < 0.05 was set as a criterion for statistical significance. All analyses were performed in Stata 15.1 (Stata Statistical Software, Release 15 [2017]; StataCorp LP, College Station, TX, USA).
The median age was 80 years (73–85), 8 (40%) patients were female, 15 (75%) showed a prior history of NYHA III, and all of them were previously admitted for acute HF, all of them were on treatment with oral loop diuretics [median furosemide equivalent doses 80 mg/day (40–120)] and showed peripheral edema at presentation (90% with grades 3+ to 4+). The median (p25–p75%) SBP, heart rate, eGFR, NT-proBNP and carbohydrate antigen (CA125) at presentation were 127 mmHg (110–139), 74 bpm (64–82), 44 ml/min/1.73 m2 (33–61), 2,738 pg/ml (1,290–8,585), and 34 U/mL (15–125), respectively. The median (p25–p75%) of LVEF and tricuspid annular plane systolic excursion (TAPSE) were 52% (36–60) and 17.5 mm (14–19), respectively. A total of 12 (60%) patients had LVEF ≥50%. The median (p25–p75%) of IVC diameter was 22.5 mm (15–27). Half of the patients displayed IVC diameter ≤21 mm. Patients were treated with homogenous doses of subcutaneous furosemide [median 100 mg/day (min: 80, and max: 120)].
Baseline characteristics across IVC status (≤21 vs. >21 mm) are summarized in Table 1. Patients with IVC ≤21 mm showed lower NYHA class, NT-proBNP, and jugular engorgement (Table 1). There were no differences in the severity of peripheral edema or other clinical parameters of congestion.
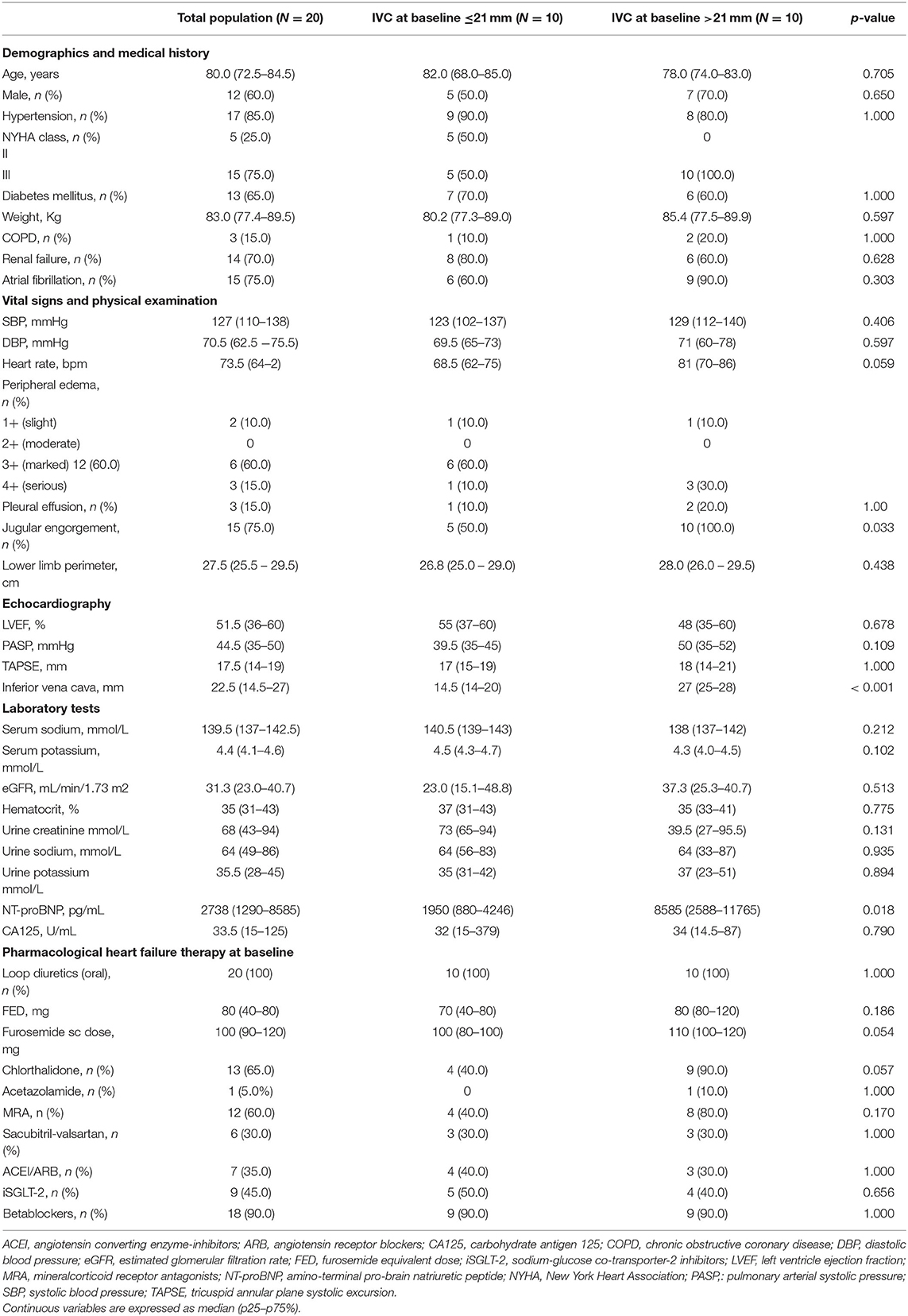
Table 1. Baseline characteristics.
Following administration of subcutaneous furosemide and VLC, we found a significant increase in 3-h IVC diameter (ΔIVC = 1.6 mm, 95% CI: 0.7 to 2.5; p < 0.001). A total of 9 patients (45%) displayed a 3-h increase in IVC ≥2 mm. Afterward, a stepwise decrease of IVC diameter was noticed at 24, 48, and 72-h (Figure 1). However, the effect of VLC on the short-term trajectory of IVC diameter was heterogeneous across IVC status at baseline (p-value for interaction <0.001). In patients in which IVC was below or equal to the median (≤21 mm), we found a greater increase in 3-h IVC diameter (ΔIVC = 2.4 mm, 95%CI: 1.0 to 3.8; p < 0.001). In those with IVC >21 mm, IVC did not significantly increase at 3-h (ΔIVC = 0.8 mm, 95% CI:−0.6–2.2; p = 0.611), as is shown in Figure 2. The number of patients that increased IVC at least 2 mm at 3-h was higher in those with baseline IVC ≤21 mm [7 (70%) vs. 2 (20%), p = 0.025]. At later time-points (24, 48, and 72-h), and compared to baseline values, we found a greater decrease in IVC diameters in those with dilated IVC (>21 mm), but a neutral effect in those with IVC ≤21 mm (Figure 2).
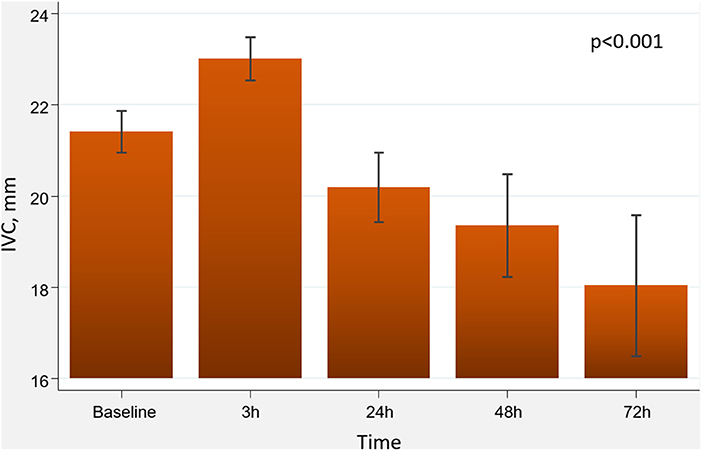
Figure 1. Changes in IVC diameter following administration of subcutaneous furosemide and venous leg compression. IVC, inferior vena cava.
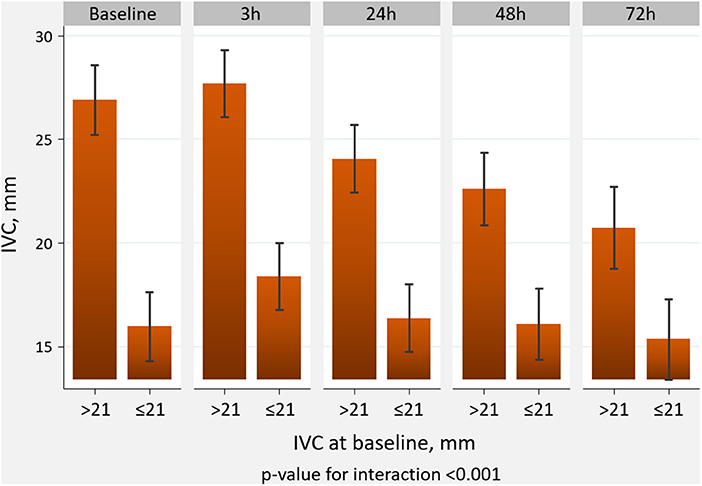
Figure 2. Effect of venous compression on the trajectory of IVC diameter across IVC status at baseline. IVC, inferior vena cava.
In the whole sample, and compared to baseline values, we found a significant increase in natriuresis, weight reduction, and decreased peripheral edema during the first 72 h (Supplementary Figure 1). Likewise, dyspnea VAS significantly decreased at 72-h (ΔVAS = −3.4, 95% CI: −4.1–−2.6; p < 0.001). We did not find significant changes in 72-h NT-proBNP (ΔLnNT-proBNP = −0.05, 95% CI: −0.23–0.34; p = 0.718). Renal function decreased at 72-h (ΔGFR = −4.2, 95% CI: −7.7–−0.7; p = 0.019). We also found a significant SBP and heart rate reduction at 24-h with posterior recovery (Supplementary Figure 1).
Overall, a short-term increase in IVC ≥2 mm was differentially associated with diuretic efficacy across baseline IVC diameter. An increase in IVC ≥2 mm was associated with a greater decongestion in those with baseline IVC ≤21 mm compared to those with dilated IVC (Figures 3, 4). All patients tolerated 72-h venous leg compression.
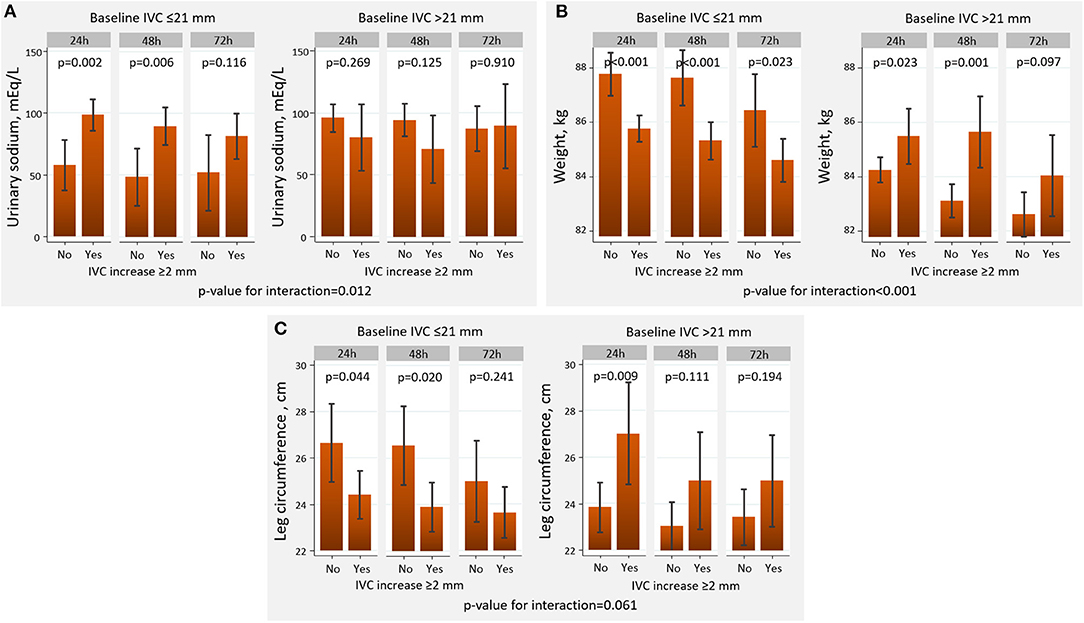
Figure 3. Changes in decongestion parameters across baseline IVC diameter and the presence of IVC increase at 3-h. (A) Urinary sodium. (B) Weight. (C) Leg circumference. IVC, inferior vena cava.
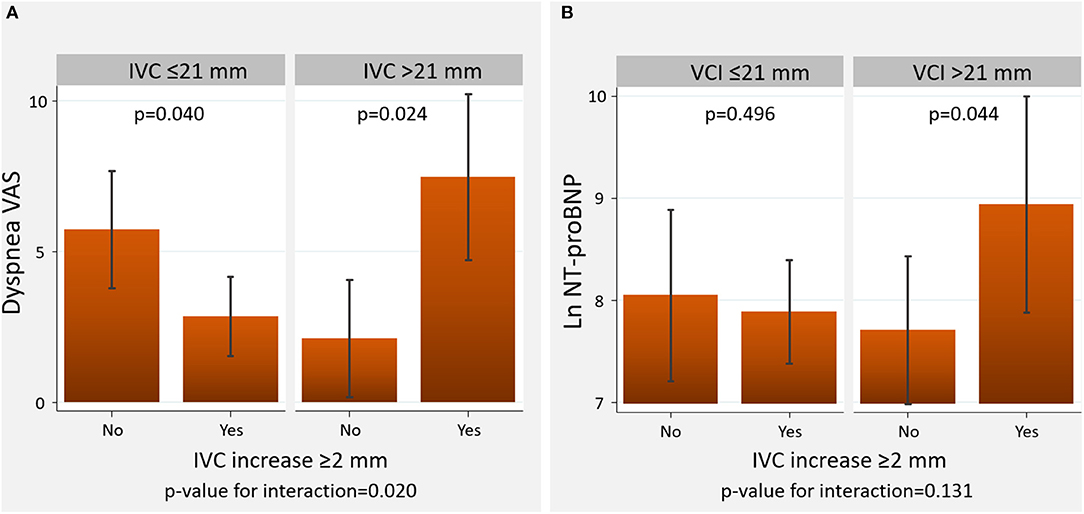
Figure 4. Changes in VAS and the logarithm of NT-proBNP across baseline IVC diameter and the presence of IVC increase at 3-h. (A) Visual analog scale. (B) Amino-terminal pro-brain natriuretic peptide. NT-proBNP, amino-terminal pro-brain natriuretic peptide, IVC, inferior vena cava; VAS, visual analog scale.
A 3-hour increase in IVC ≥2 mm was associated with a greater natriuresis in those with IVC ≤21 mm but not in those with IVC >21 mm, in which most of the comparisons were neutral (p-value for interaction=0.012) (Figure 3A).
An increase in IVC ≥2 mm at 3-h was associated with a greater weight reduction when IVC ≤21 mm compared to those with IVC >21 mm (p-for interaction <0.001). In this latter group, intravascular refill was associated with higher weight (Figure 3B).
The increase in IVC was borderline differentially associated with the resolution of edemas (p-value for interaction = 0.061). Intravascular refill led to a significant decrease in leg diameter in those with IVC ≤21 mm. Conversely, higher leg diameters were found in those with an increase in IVC ≥2 mm and baseline IVC >21 mm (Figure 3C).
IVC increase ≥2 mm at 3-h was associated with resolution of dyspnea in those with IVC ≤21 mm at 72-h, but not in those with IVC >21 mm (p-value for interaction=0.020). In this latter group, IVC increase ≥2 mm was associated with greater dyspnea at 72 h (Figure 4A).
The relationship between an increase in IVC and 72-h NT-proBNP did not significantly differ across IVC status at baseline (p-value for interaction=0.131). However, we found higher LnNT-proBNP values in those with increased 3-h IVC and plethoric IVC at baseline (Figure 4B).
IVC 3-hour increase ≥2 mm was not differentially related to 72-h eGFR across baseline IVC (p-value for interaction = 0.835), as is presented in Figure 5A.
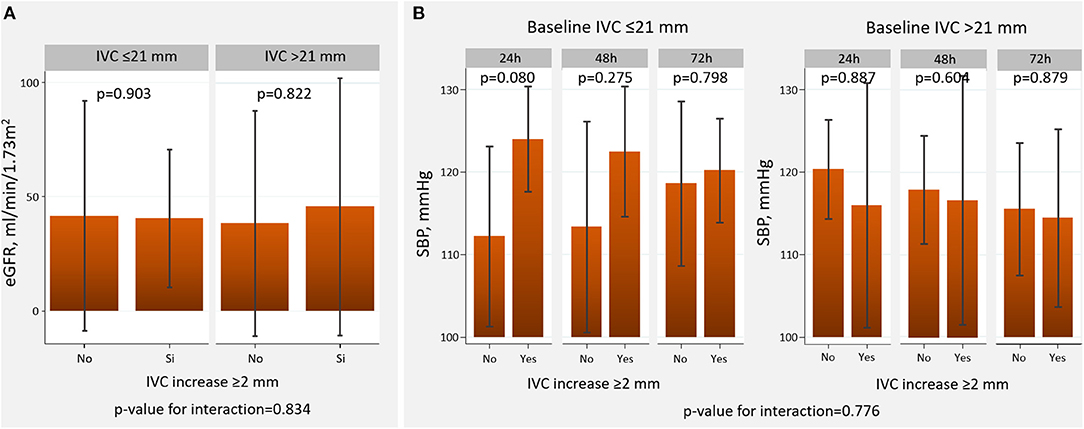
Figure 5. Changes in eGFR and SBP across baseline IVC diameter and the presence of IVC increase at 3-h. (A) Estimated glomerular filtration rate. (B) Systolic blood pressure. eGFR, estimated glomerular filtration rate; IVC, inferior vena cava; SBP, systolic blood pressure.
Short-term IVC increase ≥2 mm was not associated with a differential effect across baseline IVC (p-value for interaction = 0.776) (Figure 5B).
Summary of the main findings is presented in a central illustration.
We found that short-term VLC using elastic bandages may be useful for enhancing diuretic response in patients with congestive WHF treated with subcutaneous furosemide and absence of intravascular congestion (IVC ≤21 mm) at baseline. Conversely, it seems to have no role in those with intravascular congestion (Figure 6).
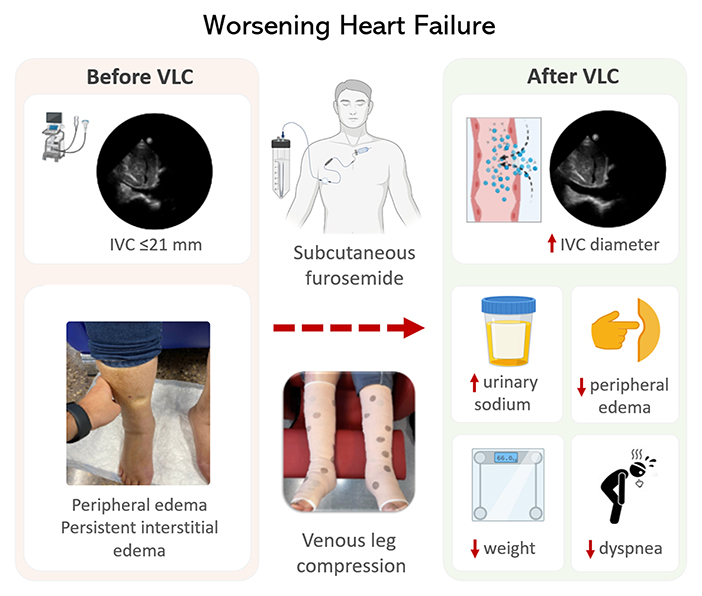
Figure 6. Central illustration. The use of venous leg compression in congestive heart failure. IVC, inferior vena cava.
Parenteral loop diuretic agents are the mainstay of the treatment of patients with congestive WHF (3, 4, 8). Despite their ubiquitous use in daily clinical practice, the evidence base for the appropriate use of these agents remains largely empirical (3, 4, 8). Clinical trials are scarce, and most of them have resulted in non-conclusive results (3, 4, 8, 12, 13). Although congestion explains most symptoms and signs in decompensated patients, the severity and body distribution are largely heterogeneous (1, 2, 14, 15). Clinical proxies of congestion have also shown a limited ability for profiling the congestive phenotype in WHF (16), a fact that may easily explain the disappointing findings in several randomized clinical trials. Thus, there is consensus about the need to improve the assessment of HF congestion by using a multiparametric approach, including imaging, biomarkers, and clinical parameters (15, 16).
Most of the volume overload, especially at more advanced phases of the disease, corresponded to tissue and not circulatory congestion (17). Patients with predominant tissue congestion identified a subset of patients with lower diuretic efficiency and at higher risk of diuretic resistance (3, 4). Traditional depletive strategies mainly play a role in controlling intravascular congestion (3, 4), while effective treatment strategies for targeting tissue/extravascular congestion remain a clinical challenge (3, 4). To manage tissue congestion, different approaches aiming to facilitate the intravascular volume recruitment (transferring water from extravascular to an intravascular compartment) by increasing plasmatic osmolarity are used without robust evidence. These strategies included the infusion of loop diuretic together with a saline hypertonic solution or albumin (5, 6, 18, 19). Another approach consists of using pharmacological agents such as SGLT2i or tolvaptan that increase urine-free water elimination (4, 20).
This study postulates that VLC in patients with WHF, evident tissue congestion, and absence of intravascular congestion, might be a widely available therapeutic alternative for short-term intravascular compartment expansion. Interestingly, we found that intravascular expansion following VLC was greater in those with normal-low intravascular volume, and, in this subset of patients, it was positively associated with a greater decongestion. On the contrary, this maneuver appears futile or even not recommended in cases with circulatory volume overload.
To date, studies of VLC mainly focused on the treatment of chronic lower limb edema and ulcer, and few studies have been performed in congestive HF (7). Moreover, VLC in patients with severe and WHF appears as a contraindication in the guidelines dedicated to leg ulcer treatment (21), as a sudden movement of a large amount of blood from lower limbs veins could lead to a rapid increase in preload and afterload, precipitating pulmonary edema (7, 22). However, a contemporary report has suggested this strategy as safe in patients with venous ulcers and HF (23).
Among available studies in patients with HF, different populations have been analyzed. Dereppe et al. performed an invasive measurement of venous pressures using a Swan-Ganz catheter in 11 patients with HF (5 with chronic HF and 6 with acute myocardial infarction). After VLC, a significant increase in right auricular, pulmonary artery, and pulmonary wedge pressures was observed, and the values returned to baseline 30 min after finishing compression (24). Brain et al. also reported, in 15 patients with moderate to severe HF, that pneumatic VLC was associated with an increase in both mean right atrial pressure and pulmonary pressure, which did not translate into significant changes in left-sided heart function (25). However, Wilputte et al. observed, in 5 patients with HF and NYHA class III and IV that simultaneous bandage VLC and muscle contraction induced a significant increase in the right arterial pressure and a transient deterioration of the right and left ventricular function (26).
More recently, the effects of VLC with elastic bandages compared to hypertonic albumin on diuretic efficiency were evaluated in a large retrospective cohort of patients (N = 1147) with volume overload and diuretic resistance during the de-escalation phase of sepsis resuscitation (27). The use of elastic bandages was associated with superior diuretic efficiency than hypertonic albumin solution, despite lower baseline serum albumin levels in those receiving elastic bandages (27). Unfortunately, none of the prior works evaluated the effect of VLC across the intravascular status.
In case of safety and efficacy confirmation, VLC by using elastic bandages is a widely available, simple, well-tolerated, and cheap intervention that may be easily translated into daily clinical practice.
These findings underscore (a) the heterogeneous pathophysiology of congestion in WHF, (b) the complexity of managing congestion in HF, and (c) the need for moving toward a more precise medicine when tackling congestion in HF. Larger and more controlled studies are required to confirm current findings and unravel whether VLC may have a clinical role in managing patients with congestive HF with predominant tissue but not intravascular congestion.
First, it is a one-arm small pilot study with the absence of a control group. Further controlled studies are required comparing the effect of VLC plus parenteral administration of furosemide vs. parenteral administration of furosemide only. Second, the patients evaluated were older, with predominant preserved ejection fraction and features of advanced HF. Thus, current findings cannot be extrapolated to milder forms of the disease and those with predominantly left ventricular systolic dysfunction. Third, this study has the inherent limitations of the small number of participants. As such, we cannot discard that the neutral finding on some exposures may be due to low statistical power (Type II error). Fourth, the patients here included were those with ambulatory WHF. Leg compression's feasibility, efficacy, and safety should also be tested in hospitalized patients. Finally, the diuretic strategy used here was the subcutaneous administration of furosemide. Further studies should confirm current findings using intravenous administration of loop diuretics and better define the causal contribution of VLC in intravascular refilling.
VLC treatment is safe in patients with congestive WHF. Treatment with VLC and subcutaneous furosemide was associated with a greater 72-h decongestion when IVC at baseline is within normal values. Conversely, it appears not to have a role in increasing diuretic response in those with WHF and dilated IVC at presentation.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by Comité de Investigación del Instituto de investigación del Hospital Clínico Universitario de Valencia. Written informed consent to participate in this study was provided by the participants' legal guardian/next of kin.
JC and GM: conceptualization, data curation, investigation, methodology, project administration, validation, visualization, writing–original draft, and writing–review and editing. RE, ES, and AB-G: data curation, investigation, methodology, validation, visualization, and writing–review and editing. CS, AMo, AC, and AMa: data curation, visualization, and writing–review and editing. EN: formal analysis, investigation, methodology, resources, software, supervision, validation, and writing–review and editing. JN: conceptualization, formal analysis, funding acquisition, investigation, methodology, project administration, resources, software, supervision, validation, visualization, writing–original draft, and writing–review and editing. All authors contributed to the article and approved the submitted version.
This work was supported by grants from the Ministry of Economy and Competitiveness, Instituto Carlos III (PI20/00392), CIBER Cardiovascular (16/11/00420 and 16/11/00403). The authors have no other funding, financial relationships, or conflicts of interest to disclose relative to this work.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fcvm.2022.847450/full#supplementary-material
1. Chioncel O, Mebazaa A, Harjola VP, Coats AJ, Piepoli MF, Crespo-Leiro MG, et al. ESC Heart Failure Long-Term Registry Investigators. Clinical phenotypes and outcome of patients hospitalized for acute heart failure: the ESC Heart Failure Long-Term Registry. Eur J Heart Fail. (2017) 19:1242–54. doi: 10.1002/ejhf.890
2. Javaloyes P, Miró Ò, Gil V, Martín-Sánchez FJ, Jacob J, Herrero P, et al. ICA-SEMES Research Group. Clinical phenotypes of acute heart failure based on signs and symptoms of perfusion and congestion at emergency department presentation and their relationship with patient management and outcomes. Eur J Heart Fail. (2019) 21:1353–65. doi: 10.1002/ejhf.1502
3. Felker GM, Ellison DH, Mullens W, Cox ZL, Testani JM. Diuretic therapy for patients with heart failure: JACC state-of-the-art review. J Am Coll Cardiol. (2020) 75:1178–95. doi: 10.1016/j.jacc.2019.12.059
4. Boorsma EM, Ter Maaten JM, Damman K, Dinh W, Gustafsson F, Goldsmith S, et al. Congestion in heart failure: a contemporary look at physiology, diagnosis and treatment. Nat Rev Cardiol. (2020) 17:641–55. doi: 10.1038/s41569-020-0379-7
5. Paterna S, Di Pasquale P, Parrinello G, Fornaciari E, Di Gaudio F, Fasullo S, et al. Changes in brain natriuretic peptide levels and bioelectrical impedance measurements after treatment with high-dose furosemide and hypertonic saline solution versus high-dose furosemide alone in refractory congestive heart failure: a double-blind study. J Am Coll Cardiol. (2005) 45:1997–2003. doi: 10.1016/j.jacc.2005.01.059
6. Kitsios GD, Mascari P, Ettunsi R, Gray AW. Co-administration of furosemide with albumin for overcoming diuretic resistance in patients with hypoalbuminemia: a meta-analysis. J Crit Care. (2014) 29:253–9. doi: 10.1016/j.jcrc.2013.10.004
7. Urbanek T, Juśko M, Kuczmik WB. Compression therapy for leg oedema in patients with heart failure. ESC Heart Fail. (2020) 7:2012–20. doi: 10.1002/ehf2.12848
8. Ponikowski P, Voors AA, Anker SD, Bueno H, Cleland JG, Coats AJ, et al. Authors/Task Force Members; Document ReviewersDocument Reviewers. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur J Heart Fail. (2016) 18:891–975. doi: 10.1002/ejhf.592
9. Young T, Connolly N, Dissemond J. UrgoKTwo® Compression Bandage System made easy. Wounds Int. (2013) 4:1–6.
10. Rekha PD, Rao SS, Sahana TG, Prabhu A. Diabetic wound management. Br J Community Nurs. (2018) 23 (Suppl 9):S16–22. doi: 10.12968/bjcn.2018.23.Sup9.S16
11. Rudski LG, Lai WW, Afilalo J, Hua L, Handschumacher MD, Chandrasekaran K, et al. Guidelines for the echocardiographic assessment of the right heart in adults: a report from the American Society of Echocardiography endorsed by the European Association of Echocardiography, a registered branch of the European Society of Cardiology, and the Canadian Society of Echocardiography. J Am Soc Echocardiogr. (2010) 23:685–788. doi: 10.1016/j.echo.2010.05.010
12. Felker GM, Lee KL, Bull DA, Redfield MM, Stevenson LW, Goldsmith SR, et al. NHLBI Heart Failure Clinical Research Network. Diuretic strategies in patients with acute decompensated heart failure. N Engl J Med. (2011) 364:797–805. doi: 10.1056/NEJMoa1005419
13. Wu MY, Chang NC, Su CL, Hsu YH, Chen TW, Lin YF, et al. Loop diuretic strategies in patients with acute decompensated heart failure: a meta-analysis of randomized controlled trials. J Crit Care. (2014) 29:2–9. doi: 10.1016/j.jcrc.2013.10.009
14. Fudim M, Hernandez AF, Felker GM. Role of volume redistribution in the congestion of heart failure. J Am Heart Assoc. (2017) 6:e006817. doi: 10.1161/JAHA.117.006817
15. Mullens W, Damman K, Harjola VP, Mebazaa A, Brunner-La Rocca HP, Martens P, et al. The use of diuretics in heart failure with congestion - a position statement from the Heart Failure Association of the European Society of Cardiology. Eur J Heart Fail. (2019) 21:137–55. doi: 10.1002/ejhf.1369
16. Girerd N, Seronde MF, Coiro S, Chouihed T, Bilbault P, Braun F, et al. INI-CRCT, Great Network, and the EF-HF Group. Integrative assessment of congestion in heart failure throughout the patient journey. JACC Heart Fail. (2018) 6:273–85. doi: 10.1016/j.jchf.2017.09.023
17. Cleland J, Pfeffer MA, Clark AL, Januzzi JL, McMurray J, Mueller C, et al. The struggle towards a Universal Definition of Heart Failure-how to proceed? Eur Heart J. (2021) 42:2331–43. doi: 10.1093/eurheartj/ehab082
18. Lee TH, Kuo G, Chang CH, Huang YT, Yen CL, Lee CC, et al. Diuretic effect of co-administration of furosemide and albumin in comparison to furosemide therapy alone: An updated systematic review and meta-analysis. PLoS ONE. (2021) 16:e0260312. doi: 10.1371/journal.pone.0260312
19. Paterna S, Di Gaudio F, La Rocca V, Balistreri F, Greco M, Torres D, et al. Hypertonic Saline in Conjunction with High-Dose Furosemide Improves Dose-Response Curves in Worsening Refractory Congestive Heart Failure. Adv Ther. (2015) 32:971–82. doi: 10.1007/s12325-015-0254-9
20. de la Espriella R, Miñana G, Santas E, Núñez G, Lorenzo M, Núñez E, et al. Effects of empagliflozin on CA125 trajectory in patients with chronic congestive heart failure. Int J Cardiol. (2021) 339:102–5. doi: 10.1016/j.ijcard.2021.06.045
21. Andriessen A, Apelqvist J, Mosti G, Partsch H, Gonska C, Abel M. Compression therapy for venous leg ulcers: risk factors for adverse events and complications, contraindications - a review of present guidelines. J Eur Acad Dermatol Venereol. (2017) 31:1562–8. doi: 10.1111/jdv.14390
22. Hirsch T. Oedema drainage and cardiac insufficiency–when is there a contraindication for compression and manual lymphatic drainage? Phlebology. (2018) 47:115–9. doi: 10.12687/phleb2420-3-2018
23. Attaran RR, Cavanaugh A, Tsay C, Ahmad T, Ochoa Chaar CI, Persing S, et al. Safety of compression therapy for venous ulcer disease in the setting of congestive heart failure. Phlebology. (2020) 35:556–60. doi: 10.1177/0268355520905178
24. Dereppe H, Hoylaerts M, Renard M, Leduc O, Bernard R, Leduc A. Hemodynamic impact of pressotherapy. J Mal Vasc. (1990) 15:267–9.
25. Bain RJ, Tan LB, Murray RG, Davies MK, Littler WA. Central haemodynamic changes during lower body positive pressure in patients with congestive cardiac failure. Cardiovas Res. (1989) 23:833–7. doi: 10.1093/cvr/23.10.833
26. Wilputte F, Renard M, Venner JP. Hemodynamic response to multilayered bandages dressed on a lower limb of patients with heart failure. Eur J Lym. (2005) 15:1–4.
Keywords: worsening heart failure, congestion, diuretic efficiency, inferior vena cava, venous leg compression
Citation: Civera J, Miñana G, de la Espriella R, Santas E, Sastre C, Mollar A, Conesa A, Martínez A, Núñez E, Bayés-Genís A and Núñez J (2022) Venous Leg Compression for Tissue Decongestion in Patients With Worsening Congestive Heart Failure. Front. Cardiovasc. Med. 9:847450. doi: 10.3389/fcvm.2022.847450
Received: 02 January 2022; Accepted: 17 June 2022;
Published: 08 July 2022.
Edited by:
Carlos Garcia Santos-Gallego, Mount Sinai Hospital, United StatesReviewed by:
Kenichi Hongo, Jikei University School of Medicine, JapanCopyright © 2022 Civera, Miñana, de la Espriella, Santas, Sastre, Mollar, Conesa, Martínez, Núñez, Bayés-Genís and Núñez. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Julio Núñez, eXVsbnVuZXpAZ21haWwuY29t; anVlbnV2aUB1di5lcw==; orcid.org/0000-0003-1672-7119
†These authors share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.