 Yalin Cao1†
Yalin Cao1† Mingyu Zhou
Mingyu Zhou Wengen Zhu
Wengen Zhu
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Cardiovasc. Med. , 25 March 2022
Sec. General Cardiovascular Medicine
Volume 9 - 2022 | https://doi.org/10.3389/fcvm.2022.840452
Background: Several published studies have disagreements on whether the use of antidepressants is associated with increased risk of arrhythmias. In this study, we performed this meta-analysis to assess the association of antidepressants with cardiac arrhythmias in patients who require antidepressants.
Methods: The PubMed and Embase databases were systematically searched until December 2021 to find studies that investigated the association between antidepressant use and cardiac arrhythmias. Studies that assessed the effects of any antidepressant on arrhythmias in patients who require antidepressants compared with those who require no antidepressants were included. We used a random-effects model to pool the adjusted risk ratios (RRs) and 95% confidence intervals (CIs). The stability of the results was examined by omitting an individual study at a time.
Results: A total of 3,396 studies were screened and 6 studies with 2,626,746 participants were finally included in this meta-analysis. When compared with no antidepressants, the use of antidepressants was significantly associated with an increased risk of atrial fibrillation (RR = 1.37, 95% CI: 1.16–1.61). However, there was no difference in the risk of ventricular arrhythmias or sudden cardiac death (RR = 1.33, 95% CI: 0.88–2.01) between the two studied groups. In the subgroup analysis, tricyclic antidepressants (RR = 1.12, 95% CI: 0.89–1.41), selective serotonin reuptake inhibitors (RR = 1.46, 95% CI: 0.63–3.38), and selective serotonin reuptake inhibitors (RR = 0.99, 95% CI: 0.97–1.01) did not increase the risk of ventricular arrhythmias and/or sudden cardiac death.
Conclusion: Recently published data suggested that the use of antidepressants did not increase the risk of ventricular arrhythmias or sudden cardiac death. Antidepressants were associated with an increased risk of atrial fibrillation but that still needs further confirmation.
A published study of the United States with 36,309 respondents demonstrated that 10.4% of respondents suffered from a 12-month depressive disorder, and 20.6% of respondents suffered from a lifetime depressive disorder (1). Previously published studies have indicated that depression might increase the risks of chronic diseases (2). As such, the use of antidepressants is not rare in the management of major depressive disorders (3). Tricyclic antidepressants (TCAs) and selective serotonin reuptake inhibitors (SSRIs) are the most frequently used, whereas other antidepressants include serotonin-norepinephrine reuptake inhibitors (SNRIs), mono-amino oxidase inhibitors (MAOs), specific serotonergic antidepressants (NaSSAs), and serotonin antagonist and reuptake inhibitors (SAIRs). However, antidepressant medications sometimes have no effects on treatment-resistant patients and even lead to unexpected adverse cardiovascular outcomes (4, 5).
Arrhythmia is a widely distributed disease that needs better medical resources and can lead to life and economic burden (6). Atrial fibrillation (AF) is the most frequent type of arrhythmias. Ventricular arrhythmia or sudden cardiac death (VA/SCD) are also severe outcomes associated with fatality. Several studies have investigated the association between antidepressant use and the risks of AF or VA/SCD, but their results remain controversial. The study of Garg et al. suggested that the treatment of antidepressants has a weaker association with incident AF, which might reflect severe depressive symptoms but not the limited effectiveness of drugs (7). However, the study of Rayne et al. suggested that a low dose of TCAs did not increase the risk of SCD (8), and some other studies reported that there was no reliable relationship between antidepressants and arrhythmias, including cAF, SCD, and VA (9–11). Therefore, the effect of antidepressants on arrhythmia risks remains uncertain. To assess the risk of arrhythmias in patients who require antidepressants, we performed a meta-analysis to assess the association between antidepressant use and the risks of AF or VA/SCD.
We used the Preferred Reporting Items for Systematic Review and Meta-Analyses (PRISMA) 2020 statement to report our findings (12). Ethical approval was not required since our meta-analysis was based on the literature that was already published. The data that support the findings of this meta-analysis would be available from the corresponding authors on reasonable requests.
We comprehensively searched the PubMed and Embase databases from inception to December 2021 for the relevant studies that reported whether antidepressants increased the risks of arrhythmias. According to our search strategies, two kinds of search terms, namely, antidepressants (e.g., antidepressants, TCAs, SSRIs, SNRIs, and NaSSAs) and arrhythmias (e.g., AF, atrial flutter, and VA), were included. Our concrete search strategies of the PubMed and Embase databases are mentioned in Supplementary Table 1. No language restrictions were used in our search.
We included studies fulfilling the following criteria:
(1) Studies assessed the effects of any antidepressant on arrhythmias in patients taking antidepressants. The comparison population was those not taking antidepressants.
(2) The outcomes were arrhythmias including AF or VA/SCD.
(3) The effects of antidepressant use on the studied outcomes were expressed as adjusted effect estimates risk.
We excluded studies having the following criteria:
(1) Studies with unadjusted data were excluded.
(2) Comparisons between different antidepressants were excluded.
(3) Study types such as reviews, case reports, editorials, letters, and meeting abstracts were excluded.
In the case of multiple publications using the same data, the study with the longest follow-up time or with the largest number of participants was included.
According to the process of study selection, two authors independently screened the studies based on titles and abstracts. Then, the full texts were assessed in detail based on the inclusion criteria to identify the final eligibility. All disagreements were resolved by discussion. Two authors also extracted data independently; the first author, publication year, data sources, country, sample size, mean age, sex, follow-up time, interventions, antidepressants in the control groups, adjusted risk ratios (RRs), and 95% confidence intervals (CIs) were included.
Our main outcomes were AF and VA/SCD. VA/SCD was defined as ventricular tachycardia, torsades de pointes, ventricular fibrillation, ventricular flutter, sudden cardiac arrest, and SCD. Since SCD was specific and often caused by VA, we set VA and SCD as a composite group.
According to the eligibility, the Newcastle-Ottawa Scale (NOS) was used to evaluate the quality of observational studies, with a total score of 9 points. The NOS of cohort studies included the selection of cohorts (i.e., 0–4 points), the comparability of cohorts (i.e., 0–2 points), and the assessment of outcomes (i.e., 0–3 points). A quota was defined to evaluate the concrete quality, that is, the total of scores > 6 was considered moderate to high quality, while the total of scores < 6 was regarded as low quality (13).
All the statistical analyses were performed using the Review Manager version 5.4 software (the Cochrane Collaboration 2014, Nordic Cochrane Center Copenhagen, Denmark; https://community.cochrane.org/). The I2 statistic was used to assess the statistical heterogeneity. If I2 values were ≤ 25%, 50%, and ≥75%, the included studies will correspond to low, moderate, and high heterogeneity, respectively. We extracted odds ratios from the case-control studies and hazard ratios from cohort studies. Ultimately, we selected RRs and 95% CIs to represent all the effect estimates in the results, which did not influence the final interpretation (14). The effects of antidepressant use on the studied outcomes were expressed as adjusted RRs and 95% CIs. We calculated the adjusted RRs and 95% CIs to their corresponding natural logarithms and standard errors. To better evaluate studies with high heterogeneity, we applied a random-effects model to pool our data. In the sensitivity analysis, we examined the stability of the results after omitting an individual study at a time. We also reperformed the analysis using a fixed-effects model. In addition, a subgroup analysis based on the drug classes of antidepressants was performed. We did not assess the publication bias because the number of included studies was < 10. In this study, a p < 0.05 indicated statistical significance.
In general, 7,091 records were searched from PubMed and Embase databases. After screening all the titles and abstracts, 6,005 records were excluded. Then, 215 records were excluded based on the full texts. Ultimately, 6 studies [6 cohort studies (7, 8, 15–18)] with 2,626,746 participants were included. The retrieval process flowchart is shown in Figure 1.
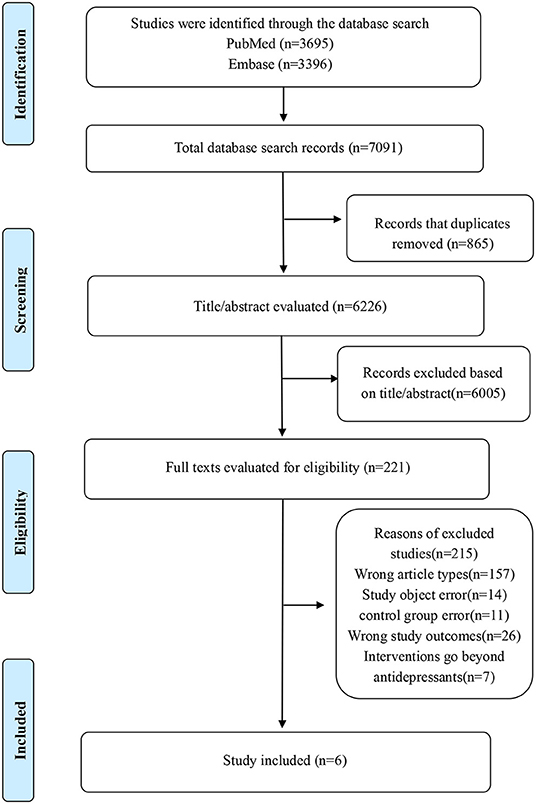
Figure 1. The concrete retrieval process flowchart of our meta-analysis.
The detailed baseline characteristics of the included studies are presented in Table 1. There are 5 studies from the United States and 1 study from Denmark, and there are no duplicates in the data sources. Many antidepressant drug classes were estimated, including TCAs, SSRIs, and SNRIs. The definition of outcomes in our included studies is displayed in Supplementary Tables 2, 3. The detailed confounding factors of included studies are presented in Supplementary Table 4.
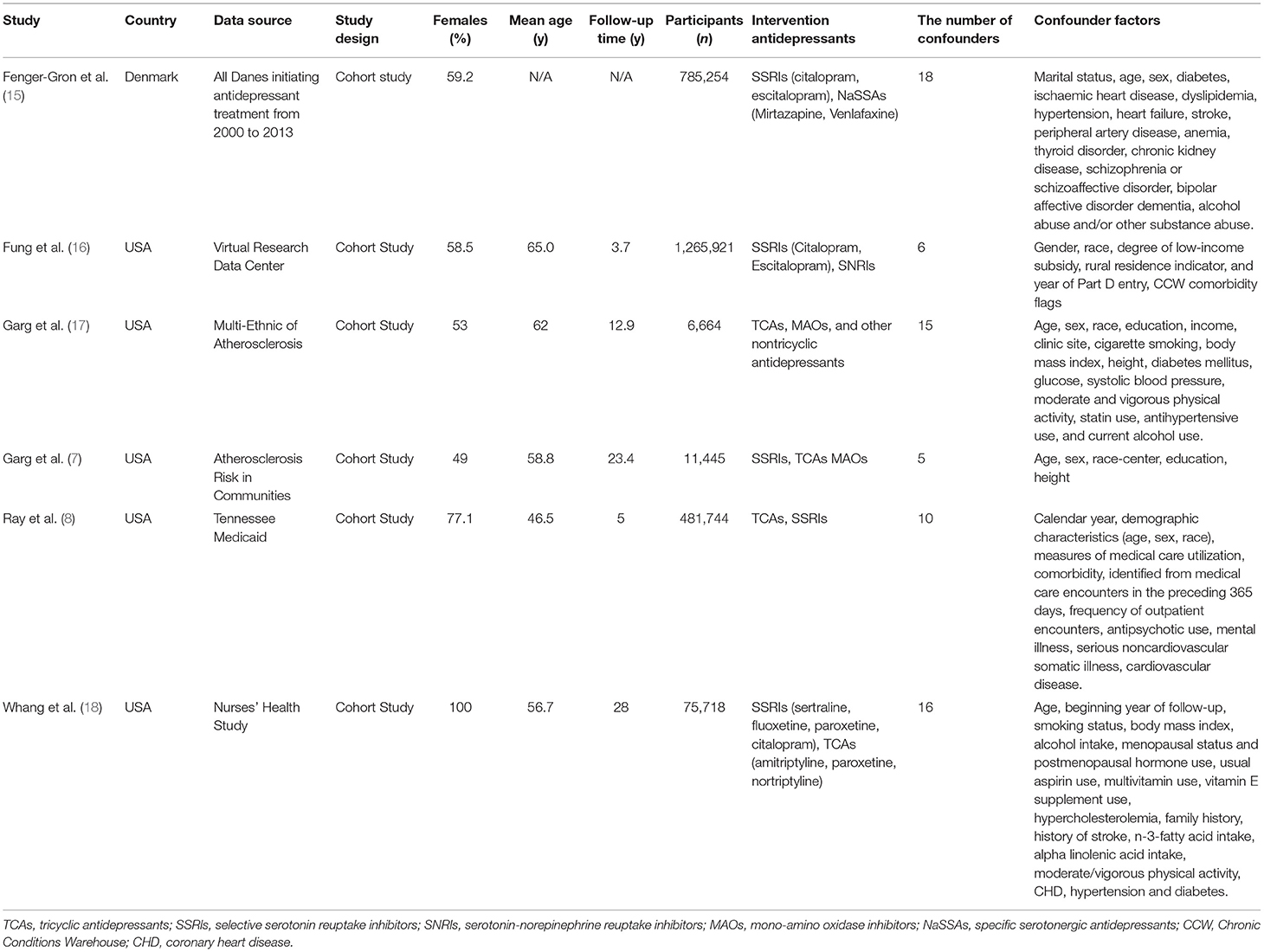
Table 1. Baseline characteristics of the included studies.
Among the 3 studies that reported the outcome of AF, the study of Garg et al. (7) suggested the association between antidepressants and incident AF in a cohort of middle and old-aged adults. Garg et al. (17) reported the increased risk of AF that is associated with depression symptoms. The risk of AF associated with the use of antidepressants seemed more pronounced in women instead of men. Fenger-Grøn et al. (15) indicated the incidence rate of AF in different periods after using antidepressants. In the pooled analysis, antidepressant use did not increase the risk of AF in the comparison with no antidepressants (RR = 1.82, 95% CI: 0.94–3.55, P = 0.08, I2 = 98%) (Supplementary Figure 1). After omitting the study of Fenger-Grøn et al., the heterogeneity decreased significantly from 98% to 0%. Thus, we reperformed the analysis by removing this study and found that the use of antidepressants significantly increased the risk of AF (RR = 1.37, 95% CI: 1.16–1.61, P = 0.0002, I2 = 0%; Figure 2).
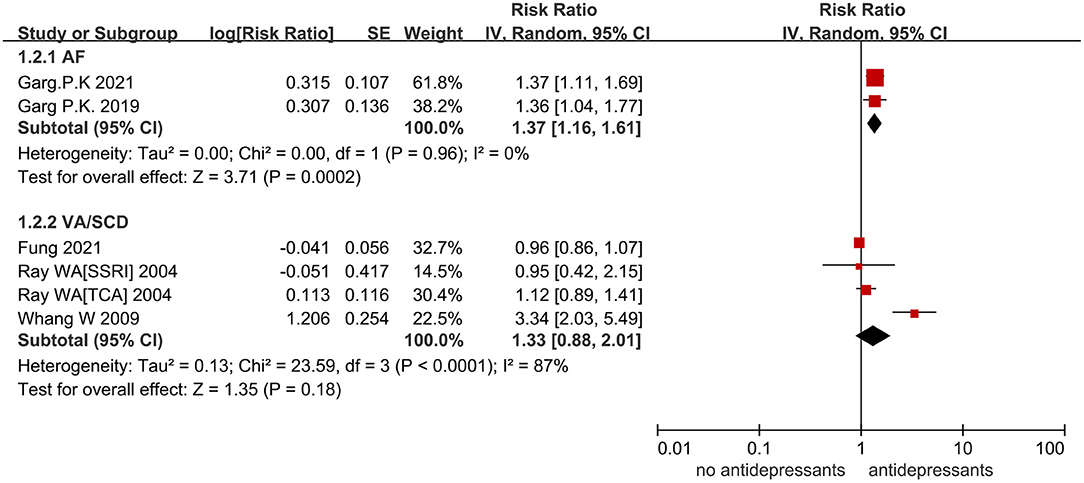
Figure 2. A forest plot of the association between antidepressant use and the increased risk of arrhythmias compared with nonusers. AF, atrial fibrillation; VA, ventricular arrhythmia; SCD, sudden cardiac death; RR, risk ratio; TCA, tricyclic antidepressant; SSRI, selective serotonin reuptake inhibitor; SNRI, serotonin norepinephrine reuptake inhibitor; CI, confidence interval; SE, standard error; IV, inverse of the variance.
A total of 3 studies concentrated on whether antidepressants increased the risk of VA/SCD. The study of Whang et al. (18) indicated an elevation in the risk of SCD in a women cohort who reported antidepressant use. The study of Fung et al. (16) demonstrated the reduced risk of both citalopram and escitalopram with cumulative use of more than 12 months through medical data of old adults. In the pooled analysis, the use of antidepressants had no association with the increased risk of VA/SCD (RR = 1.33, 95% CI: 0.88–2.01, I2 = 87%; P = 0.18) (Figure 2). For heterogeneity analysis, an I2 of 87% signified high heterogeneity. After omitting the study of Whang et al., I2 decreased from 87 to 0%
The subgroup analysis based on drug classes of antidepressants was not performed for the outcome of AF due to the limitation of data. For the risk of VA/SCD, studies were divided into 3 subgroups based on the types of antidepressants. As shown in Figure 3, TCAs (RR = 1.12, 95% CI: 0.89–1.41, P = 0.33), SSRIs (RR = 1.46, 95% CI: 0.63–3.38, P = 0.38), and SNRIs (RR = 0.99, 95% CI: 0.97–1.01, P = 0.21) did not increase the risk of VA/SCD.
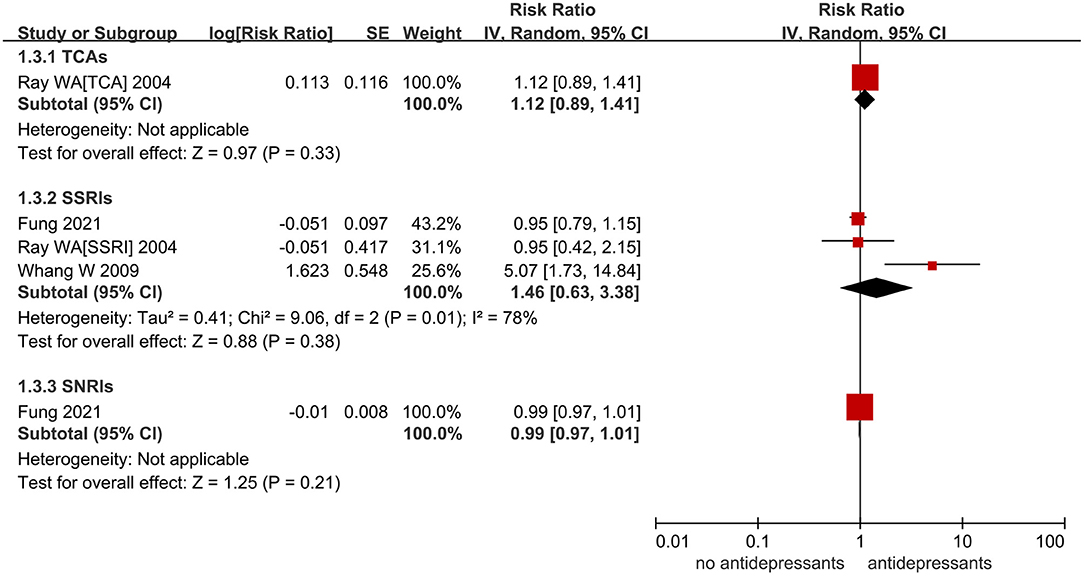
Figure 3. A forest plot of the use of antidepressant on ventricular arrhythmia (VA)/sudden cardiac death (SCD) in patients who require antidepressants based on the classes of antidepressants, including TCAs, SSRIs, and SNRIs. TCAs, tricyclic antidepressants; SSRIs, selective serotonin reuptake inhibitors; SNRIs, serotonin-norepinephrine reuptake inhibitors; RR, risk ratio; CI, confidence interval; SE, standard error; IV, inverse of the variance.
In the analysis of AF, after removing the study of Fenger-Grøn et al. (15), the heterogeneity decreased significantly from 98 to 0%. The reason might contribute to a distinct difference in the follow-up time between the studies of Fenger-Grøn et al. and Garg et al. In the analysis of VA/SCD, omitting the study of Whang et al. (18) also decreased the I2 from 87 to 0%. It might be because it contained a women cohort, which may influence the result by sex. The outcomes of SCD in this study may not be caused by the risk of arrhythmia precisely. Omitting the aforementioned studies, the origin results remained stable. When we transformed the analysis to the fixed-effects models, the results of the association between antidepressants and the risk of VA/SCD changed slightly.
After assessing their quality based on the NOS score, the scores of included observational studies were all between 6 and 8, which represented moderate to high quality (Supplementary Table 5).
Although the presented meta-analysis is based on the current published literature, we took two outcomes to represent arrhythmias, namely, AF and VA/SCD. Overall, the use of antidepressants did not increase the risks of VA/SCD. Antidepressants were associated with an increased risk of AF.
For the association between antidepressants and the risk of AF, because of the limitation that most studies concentrated on VAs, the potential mechanisms between antidepressants and AF have no accurate interpretation, and we postulated the following hypothesis. Primarily, several previous studies demonstrated that the reducing effect of 5-hydroxytryptamine (5-HT) on L-type Ca2+ current (ICaL) and action potential duration at 50% (APD50) seemed to have a relationship with AF (19–21). Moreover, the increased risk may be because of the indication for antidepressant use instead of actual antidepressant use (22). In the data from the Danish study that adjusted for sociodemographic and clinical confounds, there was a significantly increased risk of AF in antidepressant users during days 1–15 and days 16–30 before antidepressant initiation. Since antidepressants could not lead to AF before the initiation, the indication for the treatment of antidepressants or common characteristics of patients could reasonably be suspected to be the cause. Some prior studies reported that positive association between depression and AF since depression might increase the activation of the autonomic nervous system, the hypothalamic–pituitary–adrenal axis, and the renin-angiotensin aldosterone system. Owing to different psychological assessment methods that could lead to different results, investigating the effect of depression in AF was challenging (15, 23). Simultaneously, some interpretations suggested that enhanced AF symptoms might be due to lateralization of cerebral activity caused by emotional stress and high sympathetic nervous activity caused by major depressive disorder (24, 25).
Compared with no antidepressants, our analysis indicated that the use of TCAs, SSRIs, and SNRIs did not increase the risk of VA/SCD. In the 3 included studies of VA/SCD, only the study of Fung et al. (16) adopted the outcome that was completely consistent with our meta-analysis (composite VA/SCD). The outcomes of the other two studies focused more on SCD. Furthermore, only the study of Fung et al. (16) indicated that the cumulative time of antidepressant use might have an effect on the risk of VA/SCD. Patients who took cumulative use of > 12 months had a lower risk of arrhythmias. Since there were no definite reasons for this phenomenon, it was possible that the risk of arrhythmias increased significantly in the beginning, so the treatment of antidepressants was stopped. Immortal time bias should also be taken into account. A previously published meta-analysis reported that antidepressants had no valid effect on the increased risk of SCD in the comparison with different antidepressants (26). The concrete reasons are still discussed, and we postulated the following hypothesis. As for TCAs, TCAs can inhibit the sodium channel conductance and delay 0-phase cardiac depolarization, which can lead to the slower conduction velocity of His-Purkinje fibers and ventricular myocardium, due to which the prolongation of the Q wave, R wave, and S wave (QRS) complex happens on ECG (24). For SSRIs, fluoxetine and citalopram can inhibit the human ether-a-go-go-related gene (hERG) potassium channel that plays an important role in the repolarization of the cardiac action potential, which may have a relationship with the prolongation of the corrected QT interval (QTc) interval and lead to adverse reactions, such as VAs (28, 29).
Several studies reported that using TCAs had a lower risk of VA/SCD than SSRIs (30) because a moderate to a high dose of TCA use seemed to increase the risk of VA/SCD instead of a low dose. However, the use of TCAs was mainly in the case of low doses based on obvious side effects (31). As for SSRIs, several studies reported with greater evidence that the prolongation of the QTc interval and cardiotoxicity was associated with antidepressant overdose, whereas evidence rarely existed when treating with therapeutic administration (27, 32). However, we did not analyze the relationship between drug dose and arrhythmias because the data on dose and types of antidepressants varied among the included studies, which was limited and beyond the scope of discussion. Despite SNRIs being considered as the newer classes of antidepressants that were not fully explored, several studies indicated that they seemed not to increase the risk of arrhythmias, including SCD and VA (10, 11, 33, 34).
With the increasing attention to depression, the use of antidepressants has also increased and expanded (35). In addition, a previously delivered meta-analysis demonstrated that the risk of VA was related to patients with depression, especially patients with coronary heart disease, so the treatment with antidepressants should be administered carefully (36). However, our discussion on whether antidepressants increased the risks of AF is based on current studies. Further studies can find more definite conclusions in doses and classes of antidepressants.
This meta-analysis has the following limitations that should be taken into account. First, there were insufficient studies in subgroups, such as AF, which might cause the worse accuracy of results. Second, since the included studies used different data sources and analysis methods, the residual confounders should be included. Third, owing to the limitation of drug doses in the included literature, the statistical analysis about the doses of antidepressants was not supported. Moreover, a comparison between different antidepressants was excluded in our meta-analysis. In sensitivity analysis, after omitting one study at a time, heterogeneity decreased significantly, such that a greater heterogeneity between studies might influence the validity of the results. Finally, further studies could focus on the relationship between doses of antidepressants and cardiac arrhythmias.
According to the published literature, our analysis demonstrated that the use of antidepressants did not increase the risks of VA/SCD. Antidepressants were associated with an increased risk of AF. Further studies are required to confirm these findings.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author/s.
All authors listed have made a substantial, direct, and intellectual contribution to the work and approved it for publication.
This study was supported by the Clinical Research Center Project of the Department of Science and Technology of Guizhou Province [Grant No. (2017) 5405].
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fcvm.2022.840452/full#supplementary-material
1. Hasin DS, Sarvet AL, Meyers JL, Saha TD, Ruan WJ, Stohl M, et al. Epidemiology of adult DSM-5 major depressive disorder and its specifiers in the United States. JAMA Psychiatry. (2018) 75:336–46. doi: 10.1001/jamapsychiatry.2017.4602
2. Moussavi S, Chatterji S, Verdes E, Tandon A, Patel V, Ustun B. Depression, chronic diseases, and decrements in health: results from the World Health Surveys. Lancet. (2007) 370:851–8. doi: 10.1016/S0140-6736(07)61415-9
3. Hillhouse TM, Porter JH. A brief history of the development of antidepressant drugs: from monoamines to glutamate. Exp Clin Psychopharmacol. (2015) 23:1–21. doi: 10.1037/a0038550
4. Castro VM, Clements CC, Murphy SN, Gainer VS, Fava M, Weilburg JB, et al. QT interval and antidepressant use: a cross sectional study of electronic health records. BMJ. (2013) 346:f288. doi: 10.1136/bmj.f288
5. Eriksson M, Asplund K, Glader EL, Norrving B, Stegmayr B, Terént A, et al. Self-reported depression and use of antidepressants after stroke: a national survey. Stroke. (2004) 35:936–41. doi: 10.1161/01.STR.0000121643.86762.9a
6. Tang DH, Gilligan AM, Romero K. Economic burden and disparities in healthcare resource use among adult patients with cardiac arrhythmia. Appl Health Econ Health Policy. (2014) 12:59–71. doi: 10.1007/s40258-013-0070-9
7. Garg PK, Claxton JS, Soliman EZ, Chen LY, Lewis TT, Mosley T, et al. Associations of anger, vital exhaustion, anti-depressant use, and poor social ties with incident atrial fibrillation: the atherosclerosis risk in communities study. Eur J Prev Cardiol. (2021) 28:633–40. doi: 10.1177/2047487319897163
8. Ray WA, Meredith S, Thapa PB, Hall K, Murray KT. Cyclic antidepressants and the risk of sudden cardiac death. Clin Pharmacol Ther. (2004) 75:234–41. doi: 10.1016/j.clpt.2003.09.019
9. Lapi F, Azoulay L, Kezouh A, Benisty J, Matok I, Mugelli A, et al. The use of antidepressants and the risk of chronic atrial fibrillation. J Clin Pharmacol. (2015) 55:423–30. doi: 10.1002/jcph.435
10. Leonard CE, Bilker WB, Newcomb C, Kimmel SE, Hennessy S. Antidepressants and the risk of sudden cardiac death and ventricular arrhythmia. Pharmacoepidemiol Drug Saf. (2011) 20:903–13. doi: 10.1002/pds.2181
11. Martinez C, Assimes TL, Mines D, Dell'Aniello S, Suissa S. Use of venlafaxine compared with other antidepressants and the risk of sudden cardiac death or near death: a nested case-control study. BMJ. (2010) 340:c249. doi: 10.1136/bmj.c249
12. Page MJ, Mckenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. (2021) 372:n71. doi: 10.1136/bmj.n71
13. Chen C, Cao Y, Zheng Y, Dong Y, Ma J, Zhu W, et al. Effect of rivaroxaban or apixaban in atrial fibrillation patients with stage 4-5 chronic kidney disease or on dialysis. Cardiovasc Drugs Ther. (2021) 35:273–81. doi: 10.1007/s10557-021-07144-8
14. Dahabreh IJ, Sheldrick RC, Paulus JK, Chung M, Varvarigou V, Jafri H, et al. Do observational studies using propensity score methods agree with randomized trials? a systematic comparison of studies on acute coronary syndromes. Eur Heart J. (2012) 33:1893–901. doi: 10.1093/eurheartj/ehs114
15. Fenger-Grøn M, Vestergaard M, Pedersen HS, Frost L, Parner ET, Ribe AR, et al. Depression, antidepressants, and the risk of non-valvular atrial fibrillation: a nationwide Danish matched cohort study. Eur J Prev Cardiol. (2019) 26:187–95. doi: 10.1177/2047487318811184
16. Fung KW, Baye F, Kapusnik-Uner J, Mcdonald CJ. Using medicare data to assess the proarrhythmic risk of non-cardiac treatment drugs that prolong the QT interval in older adults: an observational cohort study. Drugs Real World Outcomes. (2021) 8:173–85. doi: 10.1007/s40801-021-00230-1
17. Garg PK, O'Neal WT, Diez-Roux AV, Alonso A, Soliman EZ, Heckbert S. Negative affect and risk of atrial fibrillation: MESA. J Am Heart Assoc. (2019) 8:e010603. doi: 10.1161/JAHA.118.010603
18. Whang W, Kubzansky LD, Kawachi I, Rexrode KM, Kroenke CH, Glynn RJ, et al. Depression and risk of sudden cardiac death and coronary heart disease in women: results from the Nurses' Health Study. J Am Coll Cardiol. (2009) 53:950–8. doi: 10.1016/j.jacc.2008.10.060
19. Kaumann AJ, Gaster LM, King FD, Brown AM. Blockade of human atrial 5-HT4 receptors by SB 207710, a selective and high affinity 5-HT4 receptor antagonist. Naunyn Schmiedebergs Arch Pharmacol. (1994) 349:546–8. doi: 10.1007/BF00169146
20. Pau D, Workman AJ, Kane KA, Rankin AC. Electrophysiological and arrhythmogenic effects of 5-hydroxytryptamine on human atrial cells are reduced in atrial fibrillation. J Mol Cell Cardiol. (2007) 42:54–62. doi: 10.1016/j.yjmcc.2006.08.007
21. Pino R, Cerbai E, Calamai G, Alajmo F, Borgioli A, Braconi L, et al. Effect of 5-HT4 receptor stimulation on the pacemaker current I(f) in human isolated atrial myocytes. Cardiovasc Res. (1998) 40:516–22. doi: 10.1016/S0008-6363(98)00198-9
22. Andrade C. Antidepressants and atrial fibrillation. J Clin Psychiatry. (2019) 80:19f12729. doi: 10.4088/JCP.19f12729
23. Fu Y, He W, Ma J, Wei B. Relationship between psychological factors and atrial fibrillation: a meta-analysis and systematic review. Medicine. (2020) 99:e19615. doi: 10.1097/MD.0000000000019615
24. Barton DA, Dawood T, Lambert EA, Esler MD, Haikerwal D, Brenchley C, et al. Sympathetic activity in major depressive disorder: identifying those at increased cardiac risk? J Hypertens. (2007) 25:2117–24. doi: 10.1097/HJH.0b013e32829baae7
25. Ziegelstein RC. Acute emotional stress and cardiac arrhythmias. JAMA. (2007) 298:324–9. doi: 10.1001/jama.298.3.324
26. Prasitlumkum N, Cheungpasitporn W, Tokavanich N, Ding KR, Kewcharoen J, Thongprayoon C, et al. Antidepressants and risk of sudden cardiac death: a network meta-analysis and systematic review. Med Sci. (2021) 9:26. doi: 10.3390/medsci9020026
27. Waring WS. Clinical use of antidepressant therapy and associated cardiovascular risk. Drug Healthc Patient Saf. (2012) 4:93–101. doi: 10.2147/DHPS.S28804
28. Pacher P, Kecskemeti V. Cardiovascular side effects of new antidepressants and antipsychotics: new drugs, old concerns? Curr Pharm Des. (2004) 10:2463–75. doi: 10.2174/1381612043383872
29. Zemrak WR, Kenna GA. Association of antipsychotic and antidepressant drugs with Q-T interval prolongation. Am J Health Syst Pharm. (2008) 65:1029–38. doi: 10.2146/ajhp070279
30. Wu CS, Tsai YT, Hsiung CA, Tsai HJ. Comparative risk of ventricular arrhythmia and sudden cardiac death across antidepressants in patients with depressive disorders. J Clin Psychopharmacol. (2017) 37:32–9. doi: 10.1097/JCP.0000000000000631
31. Witchel HJ, Hancox JC, Nutt DJ. Psychotropic drugs, cardiac arrhythmia, and sudden death. J Clin Psychopharmacol. (2003) 23:58–77. doi: 10.1097/00004714-200302000-00010
32. Funk KA, Bostwick JR. A comparison of the risk of QT prolongation among SSRIs. Ann Pharmacother. (2013) 47:1330–41. doi: 10.1177/1060028013501994
33. Grace SL, Medina-Inojosa JR, Thomas RJ, Krause H, Vickers-Douglas KS, Palmer BA, et al. Antidepressant use by class: association with major adverse cardiac events in patients with coronary artery disease. Psychother Psychosom. (2018) 87:85–94. doi: 10.1159/000486794
34. Spindelegger CJ, Papageorgiou K, Grohmann R, Engel R, Greil W, Konstantinidis A, et al. Cardiovascular adverse reactions during antidepressant treatment: a drug surveillance report of German-speaking countries between 1993 and 2010. Int J Neuropsychopharmacol. (2014) 18:pyu080. doi: 10.1093/ijnp/pyu080
35. Ding R, Wang Y, Ye X, Zhu D, Shi X, He P. Antidepressant use and expenditure in the treatment of patients with depression: evidence from China urban medical claims data. J Affect Disord. (2021) 296:603–8. doi: 10.1016/j.jad.2021.10.008
Keywords: antidepressants, arrhythmia, atrial fibrillation, sudden cardiac death, meta-analysis
Citation: Cao Y, Zhou M, Guo H and Zhu W (2022) Associations of Antidepressants With Atrial Fibrillation and Ventricular Arrhythmias: A Systematic Review and Meta-Analysis. Front. Cardiovasc. Med. 9:840452. doi: 10.3389/fcvm.2022.840452
Received: 21 December 2021; Accepted: 18 February 2022;
Published: 25 March 2022.
Edited by:
Alessandro Zorzi, University Hospital of Padua, ItalyReviewed by:
Yi-Ting Lin, National Taiwan University Hospital, TaiwanCopyright © 2022 Cao, Zhou, Guo and Zhu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Wengen Zhu, MTgxNzAwNDQyMjRAMTYzLmNvbQ==
†These authors share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.