
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Cardiovasc. Med. , 06 April 2022
Sec. Cardiovascular Epidemiology and Prevention
Volume 9 - 2022 | https://doi.org/10.3389/fcvm.2022.835439
This article is part of the Research Topic Women in Cardiovascular Epidemiology and Prevention View all 35 articles
 Zhoulan Zheng1†
Zhoulan Zheng1† Qianyu Guo1†
Qianyu Guo1† Dan Ma1Xuexue Wang1Chengqiang Zhang2Haiyao Wang1Liyun Zhang1Gailian Zhang2*
Dan Ma1Xuexue Wang1Chengqiang Zhang2Haiyao Wang1Liyun Zhang1Gailian Zhang2*Psoriatic arthritis (PsA) is a chronic autoimmune inflammatory joint disease related to psoriasis (PsO). The risk of PsA patients with cardiovascular disease (CVD) is significantly higher than that of the general population. At present, the relevant mechanism is not clear, chronic inflammation and traditional cardiovascular risk factors are the most important factors for the increased risk of CVD in PsA patients. Early assessment of the risk of PsA patients with CVD, and active control of the disease activity of PsA patients and intervention of traditional cardiovascular risk factors can delay the progression of CVD risk. This article reviews the epidemiology and pathogenesis between PsA and CVD, and reviews the latest developments in the risk assessment and management of CVD in PsA patients.
According to the World Health Organization, 17.7 million people die from cardiovascular disease (CVD) each year, accounting for 31% of all deaths worldwide (1). Psoriatic arthritis (PsA)is a chronic, inflammatory and immune-mediated disease that affects up to 30% of patients with psoriasis (PsO) (2). PsA was once considered a relatively mild disease, but more and more studies have shown that it can bring a huge economic burden to patients and families, especially with CVD, including Ischemic Heart Disease, all stable and unstable angina, Myocardial infarction, transient ischemic attack, coronary artery insufficiency, peripheral artery disease, stroke, congestive heart failure (3). Studies have found that CVD is the most common comorbidity in patients with PsA (4, 5). At present, with the advent of targeted therapy, the joint and skin performance of PsA patients has been greatly improved. However, due to insufficient recognition or treatment of PsA combined with CVD, serious morbidity and even mortality have been caused (6). The EULAR for PsA pharmacological management in 2019 recommends that when dealing with PsA patients, comorbidities such as metabolic syndrome and CVD should be considered (7). This article will review the research progress in the epidemiology, pathogenesis, risk assessment and management of PsA combined with CVD.
Compared with the general population, the incidence and mortality of CVD in PsA patients have increased (8–11). CVD-related risk factors and morbidity risks in the PsA population are also higher than those in the general population (12, 13). Polachek et al. (14) conducted a meta-analysis and included 11 studies, the results showed that compared with the general population, the incidence of CVD of PsA increased by 43%, and the risk of incidence increased by 55% in 2017. Among them, myocardial infarction, cerebrovascular disease and the risk of heart failure increased by 68%, 22%, and 31%. Schieir et al. (15) stated in another systematic review and meta-analysis that the risk of myocardial infarction in patients with PsA is significantly increased, even after adjustment for traditional cardiovascular risk factors, the risk of PsA combined with CVD is still significantly increased. A large population-based study in 2019 found that the risk of PsA patients with CVD increased by 29%, and also showed that the increase in CVD risk in PsA and PsO was similar (16). However, some studies have found that compared with PsO patients, PsA patients have a higher burden of carotid artery plaque and a higher incidence of combined CVD (17, 18). But compared with RA, AS and diabetes, patients with PsA have a similar CVD risk (19–21). In recent years, studies have shown that CVD is the main cause of death in PsA patients, Juneblad et al. (22) used Swedish national registration data to compare 464 PsA patients with the general population and found that the standard mortality rate of CVD in PsA patients was significantly higher. Clinicians should pay attention to the comorbidities of PsA patients, multidisciplinary cooperation, and reduce mortality.
The increased risk of CVD cannot be fully explained by traditional cardiovascular risk factors, and PsA inflammation is considered to be the main reason for the increased risk of PsA combined with CVD. There is evidence that the pathogenesis of CVD includes systemic inflammation, insulin resistance, dyslipidemia, angiogenesis, oxidative stress, and endothelial dysfunction (23). Studies have shown that many pro-inflammatory cytokines, including TNF, IL-6, and IL-17, are involved in the pathogenesis of PsA, as well as in the pathogenesis of endothelial dysfunction and atherosclerosis (24) (Figure 1). These inflammatory factors suggest that PsA is potentially related to CVD. In addition, systemic inflammation in PsA patients is thought to change lipid structure and function, thereby forming a pro-atherosclerotic profile, this lipid imbalance has been confirmed in PsA cross-sectional studies, although causal data is lacking (25, 26). Systemic inflammation of PsO can lead to insulin resistance, which in turn leads to endothelial dysfunction, atherosclerosis and ultimately CVD (27). In addition to systemic inflammatory factors, chronic recurring inflammation is also involved in the occurrence of PsA-related CVD, because the number and duration of disease activity will increase the risk of CVD. Studies have shown that cumulative inflammation is related to arteriosclerosis in PsA patients, after correcting for traditional cardiovascular risk factors, chronic inflammation still plays an important role in accelerating the development of cardiovascular risk in PsA patients (28–31). The results of a meta-analysis also showed that PsA-related subclinical atherosclerosis and endothelial dysfunction, suggesting that chronic inflammation plays an important role in its pathogenesis, independently and/or in conjunction with traditional cardiovascular risk factors, increase the risk of CVD (32). PsA patients with tendon enthesitis and/or structural damage are at high risk of CVD (33). A cross-sectional study showed that nail involvement in PsA patients is independently related to carotid plaque, and nail involvement is related to severe skin manifestations and joint involvement, which is caused by increased inflammation burden (34). Baseline increases in joint counts, index inflammation counts, and erythrocyte sedimentation rate (ESR) count levels in patients with PsA are independently associated with increases in cardiovascular events (CVE) (35, 36). In short, inflammation is the core mechanism of PsA combined with CVD, however, the data on the effect of PsA-targeted inflammation on cardiometabolism are limited, and further research is needed.

Figure 1. Pathogenesis of psoriatic arthritis complicated with cardiovascular disease.
Studies have found that traditional cardiovascular risk factors (obesity, hypertension, diabetes, dyslipidemia, metabolic syndrome, smoking) are related to PsA, and it also shows that PsA is closely related to increased CVD risk (37). A large study report in 2017 showed that the traditional cardiovascular risk factors of PsA patients are higher than those of RA and PsO (38). In subsequent studies of PsA patients, almost 88% of patients had at least one modifiable cardiovascular risk factor: smoking 17%, type 2 diabetes 13%, hypertension 45%, dyslipidemia 50%, overweight or obesity >75% (39). Compared with those PsA patients without CVD risk factors, PsA patients with more CVD risk factors showed higher disease activity (40). Among them, the obesity factor is more important, and it has been proven to promote the production of IL-17 in adipose tissue and peripheral tissue, and IL-17 is involved in the pathogenesis of obesity and PsA (41). PsA can produce a variety of pro-inflammatory cytokines, which can interfere with metabolic activities and affect adipose tissue and lipid distribution. This can lead to type 2 diabetes, metabolic syndrome, hyperlipidemia, hypertension, and obesity, which can have a profound impact on the management of PsA patients (42). Hyperuricemia appears to be an independent risk factor for PsA (43). for PsA patients without CVD, serum uric acid concentration is associated with subclinical atherosclerosis (44). Appropriate control of hyperuricemia and metabolic diseases can improve the outcome of cardiovascular disease in PsA and play a preventive role (45).
First-degree relatives with a family history of premature cardiovascular event (CVE) (males before the age of 55, females before the age of 65) can significantly increase the risk of CVD in patients with inflammation and the general population (46). At present, there are few genetic research data on PsA patients with CVD, and more data are about the role of genes in the human leukocyte antigen (HLA) region in RA patients with CVD risk. Other genetic polymorphisms in different inflammatory and metabolic pathways located inside and outside the HLA region appear to increase the risk of CVD in RA patients (47, 48).
In order to achieve better management and prevention of patients with PsA combined with CVD, it is necessary to carry out relevant assessments of their risks (Table 1). Studies have shown that high ESR values are related to the high burden of atherosclerosis and clinical CVD in PsA patients. Another study on the levels of serum cytokines and adhesion molecules related to endothelial function has found that ESR and DAS28 in endothelin-1 and PsA related, suggesting that the progression of PsA combined with CVD may be slowed by controlling ESR and endothelin-1 levels (35, 78). PsA patients have a moderately increased risk of hyperlipoproteinemia (a) which may help improve the CVD risk assessment of PsA patients (79). Imaging examinations such as ultrasound and coronary CT can help assess the risk of CVD in PsA. Study found that 39% of PsA patients showed carotid plaque formation on ultrasound examination (80). Another meta-analysis showed that in patients with PsA, the common carotid artery intima-media thickness (CCA-IMT) increased, and the blood flow-mediated dilatation (FMD) decreased (32). It is suggested that ultrasound can be used to screen and monitor carotid artery plaque, CCA-IMT and brachial artery FMD to predict the possibility of CVD. However, brachial artery FMD is easily affected by the level of technique, which greatly limits its reproducibility and outcome correlation. CCA-IMT ultrasound technology is safe and reproducible, but the accuracy of different doctors may vary. Current studies have found that CCA-IMT can be used as a surrogate marker for atherosclerosis and CVD risk, the HR for CCA-IMT increased by 0.1 mm and related CVE was 1.65 (81). After carotid ultrasound assessment, patients with PsA are more often reclassified into a very high-scoring risk category than the control group, which is explained independently by disease activity (82–84). A recent multicenter study also found that both PsO and PsA are associated with an increased prevalence of coronary artery calcification (85). Szentpetery et al. (29) used coronary CT angiography to evaluate the relationship between PsA and coronary plaques and found that the prevalence of PsA coronary plaques was 76%, compared with 44% in the control group, the total plaque volume was even larger and mixed plaques have a higher incidence in PsA. Mixed plaques contain thin cap fibrous atherosclerosis, which helps PsA with CVD and poor prognosis. The course of arterial stiffness is highly correlated with the risk of CVD, and the risk of CVD in PsA patients can be assessed by detecting the aortic pulse wave velocity (53, 81). At present, EULAR recommends the routine use of Framingham and SCORE for risk scores to calculate the 10-year risk of CVD events in PsA patients. This risk score can easily underestimate the CVD risk of PsA patients, even after adjusting for the traditional risk factors of PsA patients (51, 86). In PsA patients, in addition to the traditional CV risk score, the presence of higher DAPSA and carotid plaque can independently predict CVD events (87). Therefore, the risk assessment of patients with PsA combined with CVD is particularly important.
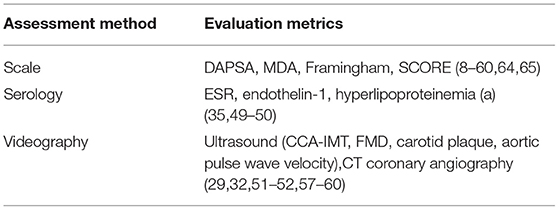
Table 1. Risk assessment of PsA combined with CVD.
The risk of CVD in PsA patients is significantly higher than that of the general population, EULAR recommends that all PsA patients undergo a CVD risk assessment at least once every 5 years to screen and identify risk factors for CVD in order to implement risk management and preventive treatment of CVD, at the same time, it is recommended that when using Framingham and SCORE to assess the 10-year risk of CVD events in PsA patients, if the Framingham score is 10% or the SCORE score is 5%, it is recommended that the patient change lifestyle and use lipid-lowering drugs for treatment (51). For overweight or obese PsA patients, ACR/American Psoriasis Foundation recommends weight loss (88). Weight loss intervention can increase the proportion of patients with PsA who reach minimum disease activity (MDA) (89, 90). Once the MDA level is reached, the MDA level should ideally be extended to prevent the progression of carotid atherosclerosis and arteriosclerosis in PsA patients (91, 92). In addition, studies have shown that exercise has a significant beneficial effect on PsA on disease activity and CVD risk (93). Schieir et al. (15) found in a systematic review and meta-analysis that traditional risk factors are more common when PsA is combined with CVD. Therefore, they support a more comprehensive CVD prevention strategy for this population, with the goal of reducing inflammation and enhancing management of traditional CVD risk factors.
There is evidence that cyclooxygenase-2 inhibitors (COXIBs) and NSAIDs increase the risk of CVD. A recent meta-analysis showed that non-selective NSAIDs and COXIBs have an adverse effect on the CVD outcome of PsA patients (52). It may be that the use of NSAIDs is related to arterial stiffness in PsA patients, increasing the risk of CVD (53). Another cohort study from the United Kingdom found that the incidence of major adverse cardiovascular events (MACE) in PsA patients receiving glucocorticoid therapy was significantly higher (49). An 11-year retrospective study showed that the increased burden of inflammation reflected by elevated CRP levels in PsA patients was associated with an increased risk of CV events, while the use of NSAIDs in PsA patients significantly reduced the risk of CVD (3). In PsA patients, the use of NSAIDs or glucocorticoid therapy is associated with a high risk of new-onset hypertension. Doctors should pay attention to the early diagnosis of hypertension during treatment with such drugs, reduce the risk of PsA combined with CVD (50). There are few direct data on this relationship in PsA, and further research is needed. EULAR recommends that NSAIDs should be used cautiously in patients with CVD records or CVD risk factors for PsA, because these drugs are usually essential when dealing with the disease activity of PsA patients, clinicians should evaluate them based on the patient's specific conditions. Then use NSAIDs according to specific treatment guidelines, and glucocorticoids can eliminate the harm of inflammation to CVD, but it will also increase the risk of CVD. When treating patients with active PsA, the lowest effective dose can be given short-term continuous treatment (51).
EULAR proposed that controlling disease activities can reduce the risk of PsA combined with CVD (Table 2). Current studies have shown that the use of biologics in PsA patients is related to the reduction of major CVD (57, 72). And proper disease activity control will reduce the use of non-steroidal anti-inflammatory drugs and glucocorticoids, which will ultimately help reduce the incidence of new CVE in these patients (35, 94). The most common first-line csDMARDs for the treatment of PsA patients is methotrexate (MTX) (70.9%), and the most common first-line bsDMARDs is adalimumab (30.8%) (95). There is conflicting evidence regarding the clinical cardiovascular end points of myocardial infarction, stroke, and cardiovascular-related death in PsA patients treated with biologics. A meta-analysis of 10 cohort studies including patients with RA, PsO, and PsA found that MTX treatment can reduce overall cardiovascular risk by 21% and myocardial infarction risk by 18%. MTX may be reduce cardiovascular risk by suppressing inflammation (54). Another study found that the vascular endothelial function of PsA patients in the MTX group improved more than that in the TNF-αi-MTX group (55). A recent meta-analysis of observational studies of 14 RA patients found that compared with TNF-αi treatment, methotrexate has an increased risk of MACE and stroke (56). Eder et al. (35) investigated the incidence of CVE in a large PsA clinic and found that there was no difference in MACE between TNF-αi, MTX, and untreated PsA patients. Studies have found that TNF-αi inhibitors can delay the progression of subclinical atherosclerosis, reduce arterial stiffness, and reduce the risk of CVD while treating PsA inflammation (57–64). The reduced cardiovascular morbidity observed in PsA patients receiving TNF-αi therapy may be partly due to its beneficial effects on complement (65). Another meta-analysis showed that the use of TNF-αi to target systemic inflammation can provide cardioprotection for patients with PsO and/or PsA, and can reduce the risk of CVD (66). A systematic review and meta-analysis by Roubille et al. (52). In 2015 showed that in patients with PsO and PsA, biologics and other DMARDs may be related to reducing the risk of CVD, but compared with RA, the evidence is not conclusive. Data from two large commercial databases in the United States show that in patients with PsO or PsA, compared with TNF-αi, there is no difference in the MACE or mortality of uzumumab (IL-12/23) initiation of treatment (67). A national cohort study in 2021 showed that compared with TNF-αi, patients with PsA using IL-12/23 and IL-17 are at greater MACE risk (68). Studies have found that Apremilast can help restore vascular endothelial dysfunction and stability, prevent the progression of atherosclerotic plaque, thereby reducing the risk of CVD (69–71), this is in contrast to a recent study by Ferguson et al. (73). Studies have found that compared with TNF-αi, there is no difference in the risk of MACE for major adverse cardiovascular events in PsA patients using Apremilast (68, 72). Tofacitinib treatment of PsA patients increases the risk of dyslipidemia, while the risk of CVD decreases (74–76). But a real-world study found that tofacitinib has a higher incidence of MACE when treating PsA patients (77). Regarding the effect of drugs on the incidence and mortality of CVD in the PsA population, large-scale, prospective, adequately controlled and powerful studies are still needed.
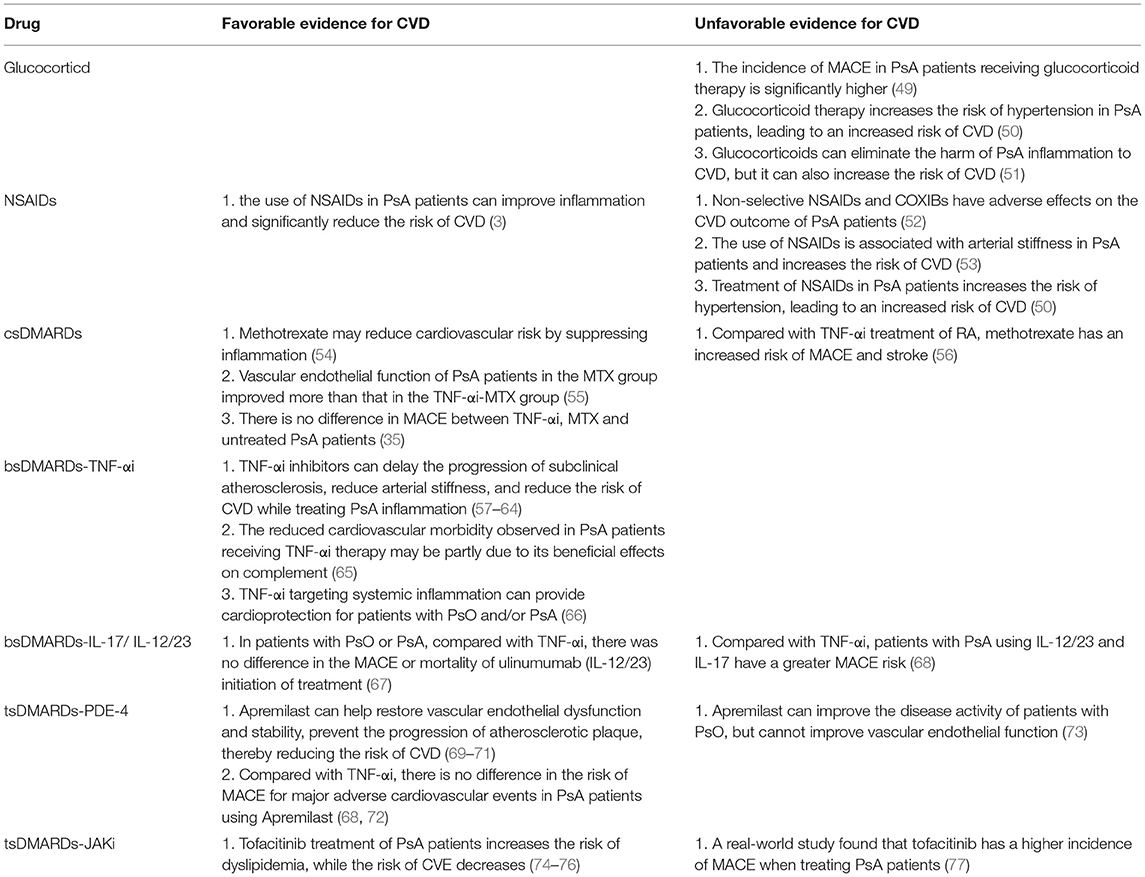
Table 2. Risk of CVD in patients with PsA after drug treatment.
With the improvement of the level of diagnosis and treatment, more and more evidences show that the CVD burden of PsA patients has increased significantly. In terms of management, it is recommended to intervene in the traditional risk factors of CVD that are increased in PsA, and then further research is needed on the impact of anti-inflammatory treatments, especially DMARDs and biological agents (including TNF-αi inhibitors) on the burden of CVD. In addition to considering traditional risk factors, chronic and systemic inflammation may lead to the accelerated development of atherosclerosis, which can be measured by some non-invasive techniques, early identification, early treatment, and reduced incidence rate and death rate.
ZZ: literature search and writing. QG and DM: suggestions and revision points. XW and HW: literature search. CZ and LZ: propose. GZ: provide ideas and suggestions. All authors contributed to the article and approved the submitted version.
This work was supported in part by the Shanxi Province Applied Basic Research Project (201801D121201) and the Shanxi Province Overseas Students Science and Technology Activities Selection Funding Project (20210003).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Thanks to the Third Hospital of Shanxi Medical University for the training and the guidance of all the professors.
1. WHO. World Health Statistics Overview 2019: Monitoring Health for the SDGs, Sustainable Development Goals. Geneva: World Health Organization (2019).
2. Gottlieb A, Merola JF. Psoriatic arthritis for dermatologists. J Dermatolog Treat. (2020) 31:662–79. doi: 10.1080/09546634.2019.1605142
3. Lam SH, So H, Cheng IT, Li EK, Wong P, Li TK, et al. Association of C-reactive protein and non-steroidal anti-inflammatory drugs with cardiovascular events in patients with psoriatic arthritis: a time-dependent Cox regression analysis. Ther Adv Musculoskelet Dis. (2021) 13:1759720X211027712. doi: 10.1177/1759720X211027712
4. Esposito M, Giunta A, Mazzotta A, Zangrilli A, Babino G, Bavetta M, et al. Efficacy and safety of subcutaneous anti-tumor necrosis factor-alpha agents, etanercept and adalimumab, in elderly patients affected by psoriasis and psoriatic arthritis: an observational long-term study. Dermatology. (2012) 225:312–9. doi: 10.1159/000345623
5. Maximilian R, Garbe C, Petersen J, Augustin M, Kirsten N, Biermann MHC, et al. Epidemiology, comorbidity and risk factors for psoriatic arthritis: a health insurance claims database analysis. Acta Derm Venereol. (2021) 101:adv00566. doi: 10.2340/00015555-3879
6. So H, Tam LS. Cardiovascular disease and depression in psoriatic arthritis: multidimensional comorbidities requiring multidisciplinary management. Best Pract Res Clin Rheumatol. (2021) 35:101689. doi: 10.1016/j.berh.2021.101689
7. Gossec L, Baraliakos X, Kerschbaumer A, de Wit M, McInnes I, Dougados M, et al. EULAR recommendations for the management of psoriatic arthritis with pharmacological therapies: 2019 update. Ann Rheum Dis. (2020) 79:700–12. doi: 10.1136/annrheumdis-2020-217159
8. Karmacharya P, Ogdie A, Eder L. Psoriatic arthritis and the association with cardiometabolic disease: a narrative review. Ther Adv Musculoskelet Dis. (2021) 13:1759720X21998279. doi: 10.1177/1759720X21998279
9. Horreau C, Pouplard C, Brenaut E, Barnetche T, Misery L, Cribier B, et al. Cardiovascular morbidity and mortality in psoriasis and psoriatic arthritis: a systematic literature review. J Eur Acad Dermatol Venereol. (2013) 27(Suppl. 3):12–29. doi: 10.1111/jdv.12163
10. Jamnitski A, Symmons D, Peters MJ, Sattar N, McInnes I, Nurmohamed MT. Cardiovascular comorbidities in patients with psoriatic arthritis: a systematic review. Ann Rheum Dis. (2013) 72:211–6. doi: 10.1136/annrheumdis-2011-201194
11. Ogdie A, Yu Y, Haynes K, Love TJ, Maliha S, Jiang Y, et al. Risk of major cardiovascular events in patients with psoriatic arthritis, psoriasis and rheumatoid arthritis: a population-based cohort study. Ann Rheum Dis. (2015) 74:326–32. doi: 10.1136/annrheumdis-2014-205675
12. Kibari A, Cohen AD, Gazitt T, Bitterman H, Lavi I, Feldhamer I, et al. Cardiac and cardiovascular morbidities in patients with psoriatic arthritis: a population-based case control study. Clin Rheumatol. (2019) 38:2069–75. doi: 10.1007/s10067-019-04528-y
13. Landgren AJ, Bilberg A, Eliasson B, Larsson I, Dehlin M, Jacobsson L, et al. Cardiovascular risk factors are highly overrepresented in Swedish patients with psoriatic arthritis compared with the general population. Scand J Rheumatol. (2020) 49:195–9. doi: 10.1080/03009742.2019.1672783
14. Polachek A, Touma Z, Anderson M, Eder L. Risk of cardiovascular morbidity in patients with psoriatic arthritis: a meta-analysis of observational studies. Arthritis Care Res. (2017) 69:67–74. doi: 10.1002/acr.22926
15. Schieir O, Tosevski C, Glazier RH, Hogg-Johnson S, Badley EM. Incident myocardial infarction associated with major types of arthritis in the general population: a systematic review and meta-analysis. Ann Rheum Dis. (2017) 76:1396–404. doi: 10.1136/annrheumdis-2016-210275
16. Charlton R, Green A, Shaddick G, Snowball J, Nightingale A, Tillett W, et al. Risk of type 2 diabetes and cardiovascular disease in an incident cohort of people with psoriatic arthritis: a population-based cohort study. Rheumatology. (2019) 58:144–8. doi: 10.1093/rheumatology/key286
17. Eder L, Jayakar J, Shanmugarajah S, Thavaneswaran A, Pereira D, Chandran V, et al. The burden of carotid artery plaques is higher in patients with psoriatic arthritis compared with those with psoriasis alone. Ann Rheum Dis. (2013) 72:715–20. doi: 10.1136/annrheumdis-2012-201497
18. Skornicki M, Prince P, Suruki R, Lee E, Louder A. Clinical burden of concomitant joint disease in psoriasis: a US-linked claims and electronic health records database analysis. Adv Ther. (2021) 38:2458–71. doi: 10.1007/s12325-021-01698-7
19. Fragoulis GE, Evangelatos G, Tentolouris N, Fragkiadaki K, Panopoulos S, Konstantonis G, et al. Higher depression rates and similar cardiovascular comorbidity in psoriatic arthritis compared with rheumatoid arthritis and diabetes mellitus. Ther Adv Musculoskelet Dis. (2020) 12:1759720X20976975. doi: 10.1177/1759720X20976975
20. Lauper K, Courvoisier DS, Chevallier P, Finckh A, Gabay C. Incidence and prevalence of major adverse cardiovascular events in rheumatoid arthritis, psoriatic arthritis, and axial spondyloarthritis. Arthritis Care Res. (2018) 70:1756–63. doi: 10.1002/acr.23567
21. Rueda-Gotor J, Llorca J, Corrales A, Parra JA, Portilla V, Genre F, et al. Cardiovascular risk stratification in axial spondyloarthritis: carotid ultrasound is more sensitive than coronary artery calcification score to detect high-cardiovascular risk axial spondyloarthritis patients. Clin Exp Rheumatol. (2018).
22. Juneblad K, Rantapaa-Dahlqvist S, Alenius GM. Disease activity and increased risk of cardiovascular death among patients with psoriatic arthritis. J Rheumatol. (2016) 43:2155–61. doi: 10.3899/jrheum.160070
23. Yim KM, Armstrong AW. Updates on cardiovascular comorbidities associated with psoriatic diseases: epidemiology and mechanisms. Rheumatol Int. (2017) 37:97–105. doi: 10.1007/s00296-016-3487-2
24. Ramonda R, Lo Nigro A, Modesti V, Nalotto L, Musacchio E, Iaccarino L, et al. Atherosclerosis in psoriatic arthritis. Autoimmun Rev. (2011) 10:773–8. doi: 10.1016/j.autrev.2011.05.022
25. Shrestha A, Bahce-Altuntas A, Mowrey W, Broder A. Active peripheral inflammation is associated with pro-atherogenic lipid profile in psoriatic arthritis. Semin Arthritis Rheum. (2016) 46:286–90. doi: 10.1016/j.semarthrit.2016.05.011
26. Garg N, Krishan P, Syngle A. Atherosclerosis in psoriatic arthritis: a multiparametric analysis using imaging technique and laboratory markers of inflammation and vascular function. Int J Angiol. (2016) 25:222–8. doi: 10.1055/s-0036-1584918
27. Boehncke WH, Boehncke S, Tobin AM, Kirby B. The 'psoriatic march': a concept of how severe psoriasis may drive cardiovascular comorbidity. Exp Dermatol. (2011) 20:303–7. doi: 10.1111/j.1600-0625.2011.01261.x
28. Shen J, Shang Q, Li EK, Leung YY, Kun EW, Kwok LW, et al. Cumulative inflammatory burden is independently associated with increased arterial stiffness in patients with psoriatic arthritis: a prospective study. Arthritis Res Ther. (2015) 17:75. doi: 10.1186/s13075-015-0570-0
29. Szentpetery A, Healy GM, Brady D, Haroon M, Gallagher P, Redmond CE, et al. Higher coronary plaque burden in psoriatic arthritis is independent of metabolic syndrome and associated with underlying disease severity. Arthritis Rheumatol. (2018) 70:396–407. doi: 10.1002/art.40389
30. Lai YC, Yew YW. Psoriasis as an independent risk factor for cardiovascular disease: an epidemiologic analysis using a national database. J Cutan Med Surg. (2016) 20:327–33. doi: 10.1177/1203475415602842
31. Eder L, Thavaneswaran A, Chandran V, Cook R, Gladman DD. Increased burden of inflammation over time is associated with the extent of atherosclerotic plaques in patients with psoriatic arthritis. Ann Rheum Dis. (2015) 74:1830–5. doi: 10.1136/annrheumdis-2014-205267
32. Di Minno MN, Ambrosino P, Lupoli R, Di Minno A, Tasso M, Peluso R, et al. Cardiovascular risk markers in patients with psoriatic arthritis: a meta-analysis of literature studies. Ann Med. (2015) 47:346–53. doi: 10.3109/07853890.2015.1031822
33. Lorenzo A, Pardo E, Charca L, Pino M, Queiro R. Enthesitis and joint erosions are disease traits associated with cardiovascular risk in psoriatic arthritis. Clin Rheumatol. (2020) 39:2973–79. doi: 10.1007/s10067-020-05088-2
34. Colunga-Pedraza IJ, Galarza-Delgado DA, Azpiri-Lopez JR, Rodriguez-Romero AB, Guajardo-Jauregui N, Cardenas-de la Garza JA, et al. Nail involvement in psoriatic arthritis patients is an independent risk factor for carotid plaque. Ann Rheum Dis. (2021) 80:1629–31. doi: 10.1136/annrheumdis-2021-220782
35. Eder L, Wu Y, Chandran V, Cook R, Gladman DD. Incidence and predictors for cardiovascular events in patients with psoriatic arthritis. Ann Rheum Dis. (2016) 75:1680–6. doi: 10.1136/annrheumdis-2015-207980
36. Kaeley GS, Eder L, Aydin SZ, Gutierrez M, Bakewell C. Dactylitis: a hallmark of psoriatic arthritis. Semin Arthritis Rheum. (2018) 48:263–73. doi: 10.1016/j.semarthrit.2018.02.002
37. Puig L. Cardiometabolic comorbidities in psoriasis and psoriatic arthritis. Int J Mol Sci. (2017) 19. doi: 10.3390/ijms19010058
38. Radner H, Lesperance T, Accortt NA, Solomon DH. Incidence and prevalence of cardiovascular risk factors among patients with rheumatoid arthritis, psoriasis, or psoriatic arthritis. Arthritis Care Res. (2017) 69:1510–8. doi: 10.1002/acr.23171
39. Eder L, Harvey P, Chandran V, Rosen CF, Dutz J, Elder JT, et al. Gaps in diagnosis and treatment of cardiovascular risk factors in patients with psoriatic disease: an international multicenter study. J Rheumatol. (2018) 45:378–84. doi: 10.3899/jrheum.170379
40. Ferraz-Amaro I, Prieto-Pena D, Palmou-Fontana N, Martinez-Lopez D, de Armas-Rillo L, Garcia-Dorta A, et al. The number of traditional cardiovascular risk factors is independently correlated with disease activity in patients with psoriatic arthritis. Medicina. (2020) 56. doi: 10.3390/medicina56080415
41. Chehimi M, Vidal H, Eljaafari A. Pathogenic role of IL-17-producing immune cells in obesity, and related inflammatory diseases. J Clin Med. (2017) 6. doi: 10.3390/jcm6070068
42. Scarpa R, Caso F, Costa L, Peluso R, Del Puente A, Olivieri I. Psoriatic disease 10 years later. J Rheumatol. (2017) 44:1298–301. doi: 10.3899/jrheum.161402
43. Tsuruta N, Imafuku S, Narisawa Y. Hyperuricemia is an independent risk factor for psoriatic arthritis in psoriatic patients. J Dermatol. (2017) 44:1349–52. doi: 10.1111/1346-8138.13968
44. Gonzalez-Gay MA, Gonzalez-Juanatey C, Vazquez-Rodriguez TR, Gomez-Acebo I, Miranda-Filloy JA, Paz-Carreira J, et al. Asymptomatic hyperuricemia and serum uric acid concentration correlate with subclinical atherosclerosis in psoriatic arthritis patients without clinically evident cardiovascular disease. Semin Arthritis Rheum. (2009) 39:157–62. doi: 10.1016/j.semarthrit.2008.06.001
45. AlJohani R, Polachek A, Ye JY, Chandran V, Gladman DD. Characteristic and outcome of psoriatic arthritis patients with hyperuricemia. J Rheumatol. (2018) 45:213–7. doi: 10.3899/jrheum.170384
46. Semb AG, Ikdahl E, Hisdal J, Olsen IC, Rollefstad S. Exploring cardiovascular disease risk evaluation in patients with inflammatory joint diseases. Int J Cardiol. (2016) 223:331–6. doi: 10.1016/j.ijcard.2016.08.129
47. Lopez-Mejias R, Genre F, Remuzgo-Martinez S, Robledo G, Llorca J, Corrales A, et al. Vitamin D receptor GATG haplotype association with atherosclerotic disease in patients with rheumatoid arthritis. Atherosclerosis. (2016) 245:139–42. doi: 10.1016/j.atherosclerosis.2015.12.011
48. Garcia-Bermudez M, Lopez-Mejias R, Genre F, Castaneda S, Llorca J, Gonzalez-Juanatey C, et al. Interferon regulatory factor 5 genetic variants are associated with cardiovascular disease in patients with rheumatoid arthritis. Arthritis Res Ther. (2014) 16:R146. doi: 10.1186/ar4608
49. Li L, Hagberg KW, Peng M, Shah K, Paris M, Jick S. Rates of cardiovascular disease and major adverse cardiovascular events in patients with psoriatic arthritis compared to patients without psoriatic arthritis. J Clin Rheumatol. (2015) 21:405–10. doi: 10.1097/RHU.0000000000000306
50. Lee MS, Chang CH, Lin RY, Lai MS. Risks of hypertension associated with cyclosporine, nonsteroidal anti-inflammatory drugs, and systemic glucocorticoids in patients with psoriasis: a nationwide population-based nested case-control study in Taiwan. Pharmacoepidemiol Drug Saf. (2016) 25:133–40. doi: 10.1002/pds.3890
51. Agca R, Heslinga SC, Rollefstad S, Heslinga M, McInnes IB, Peters MJ, et al. EULAR recommendations for cardiovascular disease risk management in patients with rheumatoid arthritis and other forms of inflammatory joint disorders: 2015/2016 update. Ann Rheum Dis. (2017) 76:17–28. doi: 10.1136/annrheumdis-2016-209775
52. Roubille C, Richer V, Starnino T, McCourt C, McFarlane A, Fleming P, et al. The effects of tumour necrosis factor inhibitors, methotrexate, non-steroidal anti-inflammatory drugs and corticosteroids on cardiovascular events in rheumatoid arthritis, psoriasis and psoriatic arthritis: a systematic review and meta-analysis. Ann Rheum Dis. (2015) 74:480–9. doi: 10.1136/annrheumdis-2014-206624
53. Fohse FK, Rollefstad S, Ikdahl E, Wibetoe G, Sexton J, Hisdal J, et al. Degree of arterial stiffness is comparable across inflammatory joint disease entities. Scand J Rheumatol. (2021) 76:17–28. doi: 10.1080/03009742.2021.1920169
54. Micha R, Imamura F, Wyler von Ballmoos M, Solomon DH, Hernan MA, Ridker PM, et al. Systematic review and meta-analysis of methotrexate use and risk of cardiovascular disease. Am J Cardiol. (2011) 108:1362–70. doi: 10.1016/j.amjcard.2011.06.054
55. Deyab G, Hokstad I, Whist JE, Smastuen MC, Agewall S, Lyberg T, et al. Methotrexate and anti-tumor necrosis factor treatment improves endothelial function in patients with inflammatory arthritis. Arthritis Res Ther. (2017) 19:232. doi: 10.1186/s13075-017-1439-1
56. Singh S, Fumery M, Singh AG, Singh N, Prokop LJ, Dulai PS, et al. Comparative risk of cardiovascular events with biologic and synthetic disease-modifying antirheumatic drugs in patients with rheumatoid arthritis: a systematic review and meta-analysis. Arthritis Care Res. (2020) 72:561–76. doi: 10.1002/acr.23875
57. Lee JL, Sinnathurai P, Buchbinder R, Hill C, Lassere M, March L. Biologics and cardiovascular events in inflammatory arthritis: a prospective national cohort study. Arthritis Res Ther. (2018) 20:171. doi: 10.1186/s13075-018-1669-x
58. Brezinski EA, Follansbee MR, Armstrong EJ, Armstrong AW. Endothelial dysfunction and the effects of TNF inhibitors on the endothelium in psoriasis and psoriatic arthritis: a systematic review. Curr Pharm Des. (2014) 20:513–28. doi: 10.2174/138161282004140213123852
59. Di Minno MN, Iervolino S, Zincarelli C, Lupoli R, Ambrosino P, Pizzicato P, et al. Cardiovascular effects of Etanercept in patients with psoriatic arthritis: evidence from the cardiovascular risk in rheumatic diseases database. Expert Opin Drug Saf. (2015) 14:1905–13. doi: 10.1517/14740338.2015.1111870
60. Shen J, Shang Q, Tam LS. Targeting inflammation in the prevention of cardiovascular disease in patients with inflammatory arthritis. Transl Res. (2016) 167:138–51. doi: 10.1016/j.trsl.2015.05.006
61. Vlachopoulos C, Gravos A, Georgiopoulos G, Terentes-Printzios D, Ioakeimidis N, Vassilopoulos D, et al. The effect of TNF-a antagonists on aortic stiffness and wave reflections: a meta-analysis. Clin Rheumatol. (2018) 37:515–26. doi: 10.1007/s10067-017-3657-y
62. Eder L, Joshi AA, Dey AK, Cook R, Siegel EL, Gladman DD, et al. Association of tumor necrosis factor inhibitor treatment with reduced indices of subclinical atherosclerosis in patients with psoriatic disease. Arthritis Rheumatol. (2018) 70:408–16. doi: 10.1002/art.40366
63. Ortolan A, Ramonda R, Lorenzin M, Pesavento R, Spinazze A, Felicetti M, et al. Subclinical atherosclerosis evolution during 5 years of anti-TNF-alpha treatment in psoriatic arthritis patients. Clin Exp Rheumatol. (2021) 39:158–61.
64. Lorenzo Martin JA, Pardo Campo E, Pino Martinez M, Colazo Burlato M, Queiro Silva MR. Psoriatic arthritis: interaction between cardiometabolic diseases and inflammatory burden of the disease. Reumatol Clin. (2021) 51:240–7. doi: 10.1016/j.reumae.2021.05.003
65. Hokstad I, Deyab G, Wang Fagerland M, Lyberg T, Hjeltnes G, Forre O, et al. Tumor necrosis factor inhibitors are associated with reduced complement activation in spondylarthropathies: an observational study. PLoS ONE. (2019) 14:e0220079. doi: 10.1371/journal.pone.0220079
66. Yang ZS, Lin NN, Li L, Li Y. The effect of TNF inhibitors on cardiovascular events in psoriasis and psoriatic arthritis: an updated meta-analysis. Clin Rev Allergy Immunol. (2016) 51:240–7. doi: 10.1007/s12016-016-8560-9
67. Lee MP, Desai RJ, Jin Y, Brill G, Ogdie A, Kim SC. Association of ustekinumab vs TNF inhibitor therapy with risk of atrial fibrillation and cardiovascular events in patients with psoriasis or psoriatic arthritis. JAMA Dermatol. (2019) 155:700–7. doi: 10.1001/jamadermatol.2019.0001
68. Pina Vegas L, Le Corvoisier P, Penso L, Paul M, Sbidian E, Claudepierre P. Risk of major adverse cardiovascular events in patients initiating biologics/apremilast for psoriatic arthritis: a nationwide cohort study. Rheumatology. (2021) 47:578–82. doi: 10.1093/rheumatology/keab522
69. Mazzilli S, Lanna C, Chiaramonte C, Cesaroni GM, Zangrilli A, Palumbo V, et al. Real life experience of apremilast in psoriasis and arthritis psoriatic patients: preliminary results on metabolic biomarkers. J Dermatol. (2020) 47:578–82. doi: 10.1111/1346-8138.15293
70. De La Rosa IA, López-Montilla MD, Pérez-Sánchez C, Ábalos-Aguilera MD, Ruiz-Ponce M, Jiménez-Gómez Y. SAT0331 Inflammatory markers and adipokines related to cardiovascular risk and metabolic comorbidities in psoriatic arthritis in vivo effects of apremilast. In: Annual European Congress of Rheumatology, EULAR 2018, Amsterdam, 13–16 June 2018 (2018).
71. Imam F, Al-Harbi NO, Al-Harbi MM, Ansari MA, Al-Asmari AF, Ansari MN, et al. Apremilast prevent doxorubicin-induced apoptosis and inflammation in heart through inhibition of oxidative stress mediated activation of NF-kappaB signaling pathways. Pharmacol Rep. (2018) 70:993–1000. doi: 10.1016/j.pharep.2018.03.009
72. Persson R, Hagberg KW, Qian Y, Vasilakis-Scaramozza C, Jick S. The risks of major cardiac events among patients with psoriatic arthritis treated with apremilast, biologics, DMARDs or corticosteroids. Rheumatology. (2021) 60:1926–31. doi: 10.1093/rheumatology/keaa683
73. Ferguson LD, Cathcart S, Rimmer D, Semple G, Brooksbank K, Paterson C, et al. Effect of the phosphodiesterase 4 inhibitor apremilast on cardiometabolic outcomes in psoriatic disease-results of the IMAPA study. Rheumatology. (2021) 71:1387–95. doi: 10.1093/rheumatology/keab474
74. Gladman DD, Charles-Schoeman C, McInnes IB, Veale DJ, Thiers B, Nurmohamed M, et al. Changes in lipid levels and incidence of cardiovascular events following tofacitinib treatment in patients with psoriatic arthritis: a pooled analysis across phase III and long-term extension studies. Arthritis Care Res. (2019) 71:1387–95. doi: 10.1002/acr.23930
75. Xie W, Xiao S, Huang Y, Sun X, Zhang Z. Effect of tofacitinib on cardiovascular events and all-cause mortality in patients with immune-mediated inflammatory diseases: a systematic review and meta-analysis of randomized controlled trials. Ther Adv Musculoskelet Dis. (2019) 11. doi: 10.1177/1759720X19895492
76. Yang X, Wan M, Cheng Z, Wang Z, Wu Q. Tofacitinib inhibits ox-LDL-induced adhesion of THP-1 monocytes to endothelial cells. Artif Cells Nanomed Biotechnol. (2019) 47:2775–82. doi: 10.1080/21691401.2019.1573740
77. Burmester GR, Curtis JR, Yun H, FitzGerald O, Winthrop KL, Azevedo VF, et al. An integrated analysis of the safety of tofacitinib in psoriatic arthritis across phase III and long-term extension studies with comparison to real-world observational data. Drug Saf. (2020) 43:379–92. doi: 10.1007/s40264-020-00904-9
78. Przepiera-Bedzak H, Fischer K, Brzosko M. Serum interleukin-18, fetuin-A, soluble intercellular adhesion molecule-1, and endothelin-1 in ankylosing spondylitis, psoriatic arthritis, and SAPHO syndrome. Int J Mol Sci. (2016) 17. doi: 10.3390/ijms17081255
79. Garcia-Gomez C, Martin-Martinez MA, Fernandez-Carballido C, Castaneda S, Gonzalez-Juanatey C, Sanchez-Alonso F, et al. Hyperlipoproteinaemia(a) in patients with spondyloarthritis: results of the cardiovascular in rheumatology (CARMA) project. Clin Exp Rheumatol. (2019) 37:774–82.
80. Lucke M, Messner W, Kim ES, Husni ME. The impact of identifying carotid plaque on addressing cardiovascular risk in psoriatic arthritis. Arthritis Res Ther. (2016) 18:178. doi: 10.1186/s13075-016-1074-2
81. Ikdahl E, Rollefstad S, Wibetoe G, Olsen IC, Berg IJ, Hisdal J, et al. Predictive value of arterial stiffness and subclinical carotid atherosclerosis for cardiovascular disease in patients with rheumatoid arthritis. J Rheumatol. (2016) 43:1622–30. doi: 10.3899/jrheum.160053
82. Palmou-Fontana N, Martinez-Lopez D, Corrales A, Rueda-Gotor J, Genre F, Armesto S, et al. Disease activity influences cardiovascular risk reclassification based on carotid ultrasound in patients with psoriatic arthritis. J Rheumatol. (2020) 47:1344–53. doi: 10.3899/jrheum.190729
83. Martinez-Vidal MP, Andres M, Jovani V, Santos-Ramirez C, Romera C, Fernandez-Carballido C. Role of carotid ultrasound and systematic coronary risk evaluation charts for the cardiovascular risk stratification of patients with psoriatic arthritis. J Rheumatol. (2020) 47:682–9. doi: 10.3899/jrheum.181223
84. Ibanez-Bosch R, Restrepo-Velez J, Medina-Malone M, Garrido-Courel L, Paniagua-Zudaire I, Loza-Cortina E. High prevalence of subclinical atherosclerosis in psoriatic arthritis patients: a study based on carotid ultrasound. Rheumatol Int. (2017) 37:107–12. doi: 10.1007/s00296-016-3617-x
85. Tinggaard AB, Hjuler KF, Andersen IT, Winther S, Iversen L, Bottcher M. Prevalence and severity of coronary artery disease linked to prognosis in psoriasis and psoriatic arthritis patients: a multi-centre cohort study. J Intern Med. (2021) 290:693–703. doi: 10.1111/joim.13311
86. Martinez-Vidal MP, Fernandez-Carballido C. Is the SCORE chart underestimating the real cardiovascular (CV) risk of patients with psoriatic arthritis? Prevalence of subclinical CV disease detected by carotid ultrasound. Joint Bone Spine. (2018) 85:327–32. doi: 10.1016/j.jbspin.2017.07.002
87. Lam SHM, Cheng IT, Li EK, Wong P, Lee J, Yip RM, et al. DAPSA, carotid plaque and cardiovascular events in psoriatic arthritis: a longitudinal study. Ann Rheum Dis. (2020) 79:1320–6. doi: 10.1136/annrheumdis-2020-217595
88. Singh JA, Guyatt G, Ogdie A, Gladman DD, Deal C, Deodhar A, et al. Special article: 2018 American College of Rheumatology/National Psoriasis Foundation guideline for the treatment of psoriatic arthritis. Arthritis Care Res. (2019) 71:2–29. doi: 10.1002/acr.23789
89. Klingberg E, Bilberg A, Bjorkman S, Hedberg M, Jacobsson L, Forsblad-d'Elia H, et al. Weight loss improves disease activity in patients with psoriatic arthritis and obesity: an interventional study. Arthritis Res Ther. (2019) 21:17. doi: 10.1186/s13075-019-1810-5
90. Di Minno MN, Peluso R, Iervolino S, Russolillo A, Lupoli R, Scarpa R, et al. Weight loss and achievement of minimal disease activity in patients with psoriatic arthritis starting treatment with tumour necrosis factor alpha blockers. Ann Rheum Dis. (2014) 73:1157–62. doi: 10.1136/annrheumdis-2012-202812
91. Cheng IT, Shang Q, Li EK, Wong PC, Kun EW, Law MY, et al. Effect of achieving minimal disease activity on the progression of subclinical atherosclerosis and arterial stiffness: a prospective cohort study in psoriatic arthritis. Arthritis Rheumatol. (2019) 71:271–80. doi: 10.1002/art.40695
92. Cheng IT, Li EK, Wong PC, Law MY, Yim IC, Lai BT, et al. Treat to target and prevention of subclinical atherosclerosis in psoriatic arthritis-which target should we choose? Rheumatology. (2020) 59:2881–92. doi: 10.1093/rheumatology/keaa025
93. Kessler J, Chouk M, Ruban T, Prati C, Wendling D, Verhoeven F. Psoriatic arthritis and physical activity: a systematic review. Clin Rheumatol. (2021) 40:4379–89. doi: 10.1007/s10067-021-05739-y
94. Castaneda S, Vicente-Rabaneda EF, Garcia-Castaneda N, Prieto-Pena D, Dessein PH, Gonzalez-Gay MA. Unmet needs in the management of cardiovascular risk in inflammatory joint diseases. Expert Rev Clin Immunol. (2020) 16:23–36. doi: 10.1080/1744666X.2019.1699058
Keywords: psoriatic arthritis, cardiovascular disease, traditional cardiovascular risk factors, inflammation risk, treatment management
Citation: Zheng Z, Guo Q, Ma D, Wang X, Zhang C, Wang H, Zhang L and Zhang G (2022) Related Risk Factors and Treatment Management of Psoriatic Arthritis Complicated With Cardiovascular Disease. Front. Cardiovasc. Med. 9:835439. doi: 10.3389/fcvm.2022.835439
Received: 14 December 2021; Accepted: 07 March 2022;
Published: 06 April 2022.
Edited by:
Raffaele Scarpa, University of Naples Federico II, ItalyReviewed by:
Eva Reali, University of Milano-Bicocca, ItalyCopyright © 2022 Zheng, Guo, Ma, Wang, Zhang, Wang, Zhang and Zhang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Gailian Zhang, emdsMTExOEAxNjMuY29t
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.