
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Cardiovasc. Med., 28 March 2022
Sec. General Cardiovascular Medicine
Volume 9 - 2022 | https://doi.org/10.3389/fcvm.2022.827524
 Qiang Li1,2†
Qiang Li1,2† Shiqun Chen1,2†
Shiqun Chen1,2† Haozhang Huang1,2†
Haozhang Huang1,2† Weihua Chen3†Liwei Liu1,2
Weihua Chen3†Liwei Liu1,2 Bo Wang1,2
Bo Wang1,2 Wenguang Lai4
Wenguang Lai4 Shixin Yi1,2
Shixin Yi1,2 Ming Ying1,2Ronghui Tang5
Ming Ying1,2Ronghui Tang5 Zhidong Huang1,2Jiayi Deng3
Zhidong Huang1,2Jiayi Deng3 Jiyan Chen1,2,6
Jiyan Chen1,2,6 Jin Liu1,2*
Jin Liu1,2* Yong Liu1,2,6*
Yong Liu1,2,6*Purpose: Left ventricular end-diastolic diameter (LVEDD) is a common indicator in echocardiogram, and dilated LVEDD was correlated with left ventricular insufficiency. However, it is uncertain whether dilated LVEDD is associated with increasing the risk of contrast-associated acute kidney injury (CA-AKI) in patients with coronary artery disease (CAD).
Patients and Methods: We enrolled 8,189 patients with CAD undergoing coronary angiography (CAG) between January 2007 and December 2018. Patients were divided into two groups according to the LVEDD length (normal LVEDD: men: LVEDD ≤56 mm, women: LVEDD ≤51 mm; dilated LVEDD: men: LVEDD >56 mm, women: LVEDD >51 mm). The endpoints were CA-AKI0350 and CA-AKI0525 (CA-AKI0350: an increase in the serum creatinine (Scr) level by >0.3 mg/dl or >50% within the first 48 h after CAG; CA-AKI0525: an absolute Scr increase ≥ 0.5 mg/dl or a relative increase ≥ 25% within 72 h after contrast medium exposure). In-hospital dialysis, 30-day mortality, and 1-year mortality were contained as well. Univariate and multivariable logistic regressions were used to assess the association between LVEDD and CA-AKI.
Results: Among 8,189 participants (men: 76.6%, mean age: 64.4 ± 10.7 years), 1,603 (19.6%) presented with dilated LVEDD. In addition, the dilated LVEDD group indicated an elevation of CA-AKI0350 (12.4 vs. 6.2%, p < 0.001) and CA-AKI0525 (15.0 vs. 8.8%; p < 0.001) when compared with the normal group. According to multivariable logistic analysis, dilated LVEDD was an independent predictor of CA-AKI0350 [adjusted odds ratio (aOR): 1.31; 95% confidence interval (CI): 1.06–1.61, p = 0.010) and CA-AKI0525 (aOR: 1.32; 95% CI: 1.04–1.67; p = 0.020).
Conclusion: In conclusion, these results demonstrated that the dilated LVEDD was a significant and independent predictor of CA-AKI following CAG in patients with CAD. Further verifications are needed to verify the association between LVEDD and CA-AKI.
Contrast-associated acute kidney injury (CA-AKI) is a common complication following coronary angiography (CAG) (1), which is associated with poor outcomes, including dialysis, longer duration of hospitalization, mortality, and increased health-care costs (2–5).
Left ventricular end-diastolic diameter (LVEDD) is a common and important indicator in echocardiogram, which reflects the size of cardiac as well as left ventricular function. It is associated with progressive left ventricular insufficiency (6–9). At the same time, dilated LVEDD is linked to a high risk for heart failure and cardiovascular outcomes (10, 11).
Previous studies have shown that cardiac dysfunction is closely related to the occurrence and development of CA-AKI (12). As a clinically significant index used to assess cardiac function, left ventricular ejection fraction (LVEF) has been proved an independent risk factor for postoperative CA-AKI (13, 14). Similarly, Liu et al. have demonstrated that left ventricular end-diastolic pressure (LVEDP), an indicator of cardiac function, is independently associated with increased risk of CA-AKI among patients undergoing CAG and percutaneous coronary intervention (15). Monitoring hemodynamic parameters, such as LVEDP, is an invasive and expensive test. LVEDD is a novel and convenient imaging predicator reflecting cardiac function, but it has not established a direct relationship between LVEDD and the occurrence of CA-AKI.
Therefore, the aim of our study was to investigate the association of LVEDD levels with CA-AKI in a large registry of patients with coronary artery disease (CAD), who underwent CAG.
The data of this cohort was from the registry of Cardiorenal Improvement (CIN) study (ClinicalTrials.gov NCT04407936) at Guangdong Provincial People's Hospital in China. A total of 8,189 patients with CAD, who underwent CAG between January 2007 and December 2018, were included in the final analysis after excluding 51,478 patients for the following reasons: (1) lack of LVEDD examination (n = 20,858); (2) lack of judgment of CA-AKI0350 and CA-AKI0525(n = 24,958); (3) lack of follow-up information (n = 5,662) (Figure 1). This study was conducted in accordance with the Declaration of Helsinki and was approved by the Research Ethics Committee of Guangdong Provincial People's Hospital (No. GDREC2019555H).
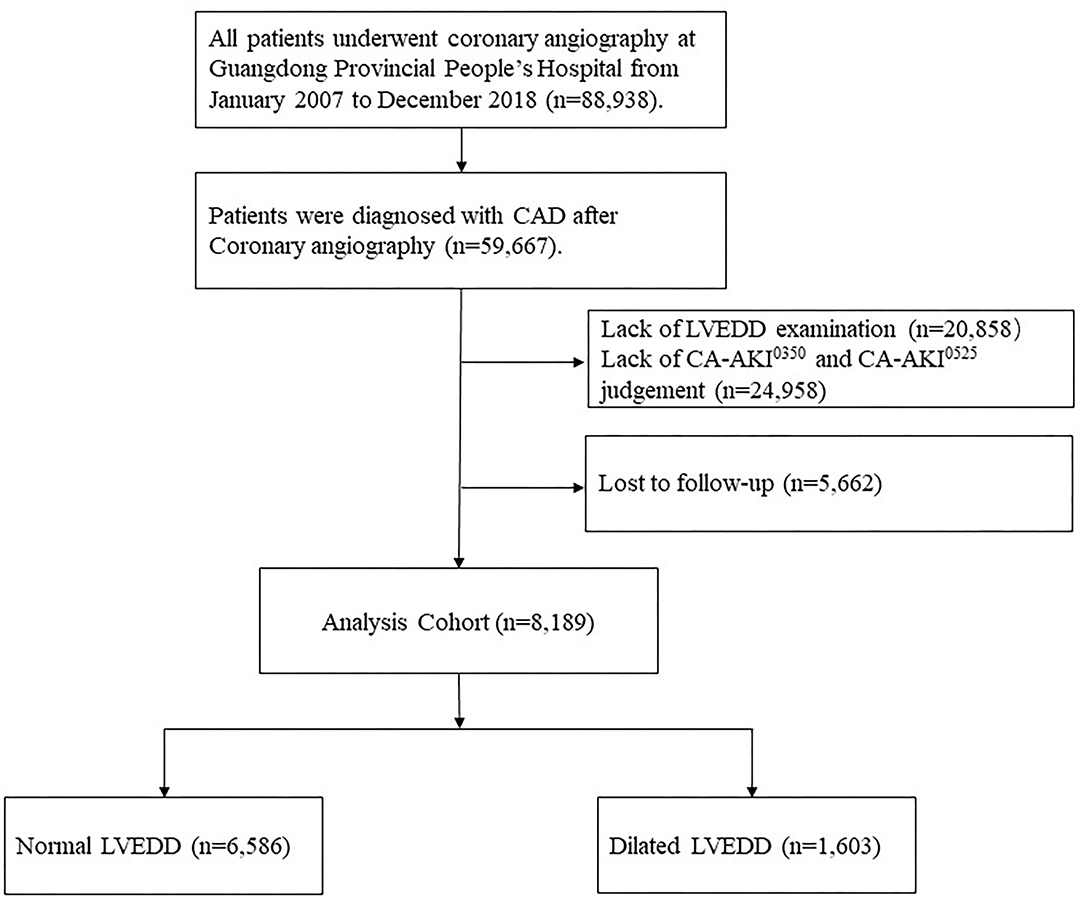
Figure 1. Study flowchart.
The study data were derived from the Clinical Management System of the Guangdong Provincial People's Hospital's electronic health record, which contained details regarding demographics, medical history, laboratory tests, medications, and other clinical data. Senior cardiologists were responsible for the data quality control and periodical data verification. During the study period, the information on death event and date for each patient was retrieved from the Guangdong Public Security System, which was linked to CIN dataset by a unique identification number. CAG or percutaneous coronary intervention was performed according to the standard clinical practice guidelines (16–18).
Echocardiography was performed by trained cardiologists for all patients at the time of admission. LVEDD was measured using an M-mode scan of the parasternal long-axis view with a 2D image. When the M-mode cursor could not be aligned perpendicularly to the left ventricular long axis, LVEDD was measured directly on 2D images (19).
The primary outcome was CA-AKI0350, defined as an absolute increase in serum creatinine (Scr) ≥ 0.3 mg/dl or a relative increase in Scr levels ≥ 50% within 48 h after contrast medium exposure (20). The secondary clinical outcomes included CA-AKI0525 (defined as an absolute increase in Scr levels ≥ 0.5 mg/dl or a relative increase in Scr levels ≥ 25% within 72 h after contrast medium exposure) (21), in-hospital dialysis, 30-day mortality, and 1-year mortality. CAD was confirmed by CAG and discriminated according to the 10th Revision Codes of the International Classification of Diseases (ICD-10; I20.xx–I25.xx, I50.00001, and I91.40001 et al.). Estimated glomerular filtration rate (eGFR) was estimated by the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) equation (22). CKD was defined as eGFR < 60 ml/min/1.73 m2. Anemia was defined as a baseline hematocrit value < 39% for men and <36% for women, according to the World Health Organization (WHO) criteria (23). The echocardiography examination was used to evaluate the LVEF and heart failure with reduced ejection fraction (HFrEF), which was defined as LVEF<40% (24).
To investigate the relationship of elevated LVEDD levels for CA-AKI in patients with CAD, men and women were divided into normal LVEDD group and dilated LVEDD group (men: LVEDD ≤56, and>56 mm; women: LVEDD ≤51, and>51 mm, respectively) (25). We reported descriptive statistics by means (SD), median [interquartile range (IQR)], or number and percentage as and when it was needed. Categorical variables were compared by Pearson chi-square test, and continuous variables by t-test. The association between different LVEDD levels and CA-AKI was tested by univariable and multivariable logistic regression. To investigate the relationship between LVEDD and LVEF, scatter plot and curve fitting were performed as shown in Supplementary Figure 1. All analyses were performed using R software (version 4.0.3; R Foundation for Statistical Computing, Vienna, Austria). A two-sided p < 0.05 indicated significance for all analyses.
After screening, a total of 8,189 CAD patients, who underwent CAG from January 2007 to December 2018, were included in this study. The mean age was (64.4 ± 10.7) years, and 6,273 patients (76.6%) were men. Patients were divided into two groups: 1,603 (19.6%) patients with dilated LVEDD (men: LVEDD>56 mm; women: LVEDD>51 mm), and 6,586 (80.4%) patients with normal LVEDD (men: LVEDD ≤56 mm; women: LVEDD ≤51 mm). Compared with the normal LVEDD group, the dilated LVEDD group was more likely to present with anemia, diabetes mellitus (DM), and reduced LVEF (< 40%), and had worse renal function. All of the baseline clinical characteristics of the patients are shown in Table 1.
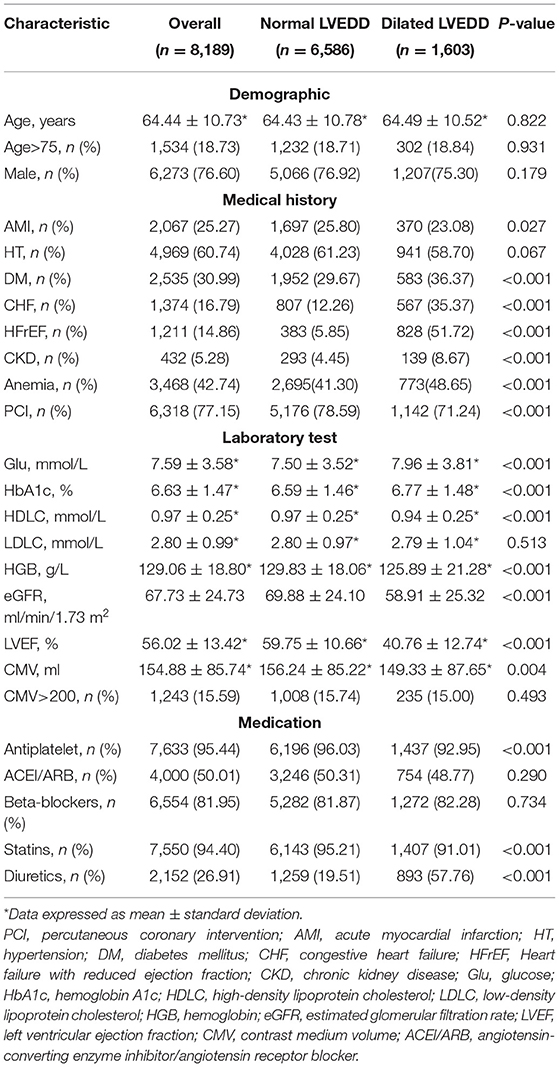
Table 1. Baseline characteristics of the patients.
Totally, 607 (7.4%) patients fulfilled the diagnostic criteria for CA-AKI0350, and the incidence of CA-AKI0350 among the dilated LVEDD group was apparently higher than the normal group (12.4 vs. 6.2%; p < 0.001, Table 2). A similar result was observed in the incidence of CA-AKI0525 (15.0 vs. 8.8%; p < 0.001). The in-hospital dialysis rate, and 30-day and 1-year mortalities were all significantly higher in patients with dilated LVEDD when compared with those with normal LVEDD(4.9 vs. 1.9%, 2.4 vs. 1.2%, 9.7 vs. 4.1%, respectively; all p < 0.001).
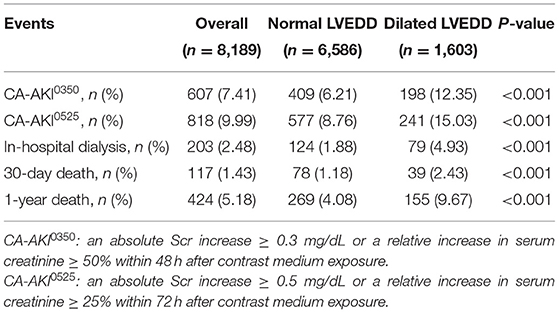
Table 2. Contrast-associated acute kidney injury (CA-AKI) incidence and clinical outcomes.
Univariate logistic regression analysis indicated that the dilated LVEDD [odds ratio (OR): 2.1; 95% confidence interval (CI): 1.78–2.54; p < 0.001, Supplementary Table 1] was significantly associated with CA-AKI0350 after CAG. When using the criteria of CA-AKI0525, similar result was found (OR: 1.8; 95% CI: 1.57–2.16; p < 0.001, Supplementary Table 1). In this study, age, anemia, CKD, DM, and HFrEF were also closely related to CA-AKI0350 and CA-AKI0525 (all p < 0.001, Supplementary Table 1). After adjusting for related risk factors (age, gender, hypertension, acute myocardial infarction (AMI), CKD, HFrEF, DM, contrast medium volume (CMV) >200, and diuretics), dilated LVEDD [adjusted odds ratio (aOR): 1.3; 95% CI: 1.06–1.61; p = 0.010, Table 3) remained significantly associated with CA-AKI0350. Similar results were obtained in CA-AKI0525 (aOR: 1.32; 95% CI: 1.04–1.67; p = 0.020, Table 3).
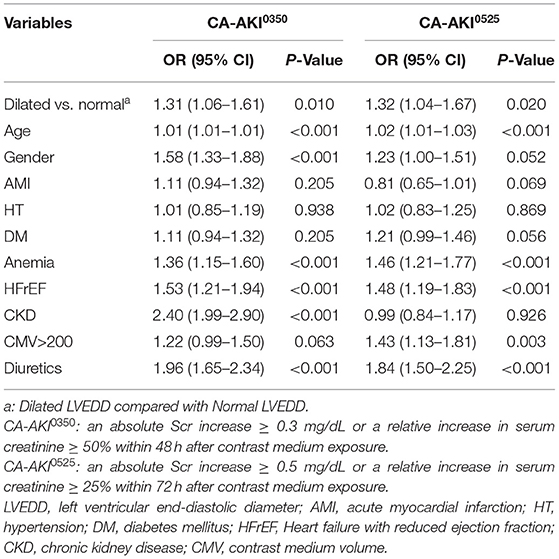
Table 3. Multivariable regression analysis of CA-AKI in different definition.
To our knowledge, this is the first cohort study that investigates the relationship between LVEDD and CA-AKI in patients with CAD. The results of our study showed that dilated LVEDD was markedly related to the incidence of CA-AKI in patients with CAD, regardless of reduced LVEF.
A number of risk factors, such as laboratory examinations (Scr, age, and gender), comorbidities, and medications, have been confirmed to be associated with CA-AKI (26, 27). Some risk models, such as Merhan score and age, creatinine, and ejection fraction (ACEF) score, were commonly used to assess the risk of CA-AKI in clinical practice (28, 29). However, these methods were reviewed and contain multiple variables, which limits their clinical use. Therefore, it is necessary to explore a variable that is common and easy to access to determine the risk of AKI. The echocardiogram is readily available and widely used in the diagnosis of cardiovascular disease.
Left ventricle structural dilation used to be considered as the morphologic substrate of congestive heart failure (CHF) for the first time by a German pathologist Linzbach AJ (30). Using left ventricular dimensions in the risk stratification of patients will aid in the better identification of patients at risk for heart failure and mortality (11). Many studies have indicated that LVEDD dilation is implicated in the development of progressive left ventricular insufficiency and CHF (7, 9). Moreover, dilated LVEDD is associated with major adverse cardiovascular events in patients with heart failure and left ventricular systolic insufficiency (10). Moreover, it was also reported that left ventricular dilation could be used for identifying cardiac death and serious ventricular arrhythmias independently in left ventricular systolic insufficiency (6, 8). Our study suggests that an adjusted large LVEDD is still an independent factor associated with higher incidence of CA-AKI, even after adjusting for ejection fraction <40, which manifests left ventricular systolic insufficiency. It confirms that dilated LVEDD is an independent predictor for CA-AKI without relying on LVEF. Likewise, our study showed that there was no clear relationship between LVEDD and LVEF. The possible reason why related adverse events were caused by left ventricular dilation is that increased ventricular wall stress in the dilated ventricle causes a mismatch in cardiac afterload, which leads to hemodynamic changes and further cardiac and renal adverse events, such as CA-AKI.
Previous studies also have found that LVEDD level is a risk factor for mortality in patients with or without heart failure. Seko et al. retrospectively analyzed data from 4,444 patients, who underwent echocardiography, and found that LVEDD had a deleterious impact on long-term mortality after adjusting for age and body size (31). The conclusion was similar to the study conducted by Kajimoto K et al., which indicated that after adjustment for multiple comorbidities, men with an LVEDD of 61 mm had a significantly higher risk of the outcomes than men with an LVEDD <54 mm, although this conclusion was weakened among women (32). Our study also found that the group with higher LVEDD had worse outcome events and had a significantly higher incidence of CA-AKI than the normal group.
This study has several important clinical significances and research implications. As it was described above, LVEDD was reported to be an important factor of cardiac function. Our results demonstrated that dilated LVEDD was an independent predictor of CA-AKI among patients with CAD, even after adjusting for potential confounding factors. The outcome demonstrates that we should not only focus on LVEF in echocardiogram but also LVEDD. A routine pre-procedural LVEDD measurement may provide useful information for the cardiologist to identify the high risk for the incidence of AKI. The degree of prediction of AKI can also be improved by combining known risk factors. More attention should be given to patients with dilated LVEDD.
This study has several limitations. First, this observational cohort was conducted in a single center that is located in southern China. However, Guangdong Provincial People's Hospital is the largest cardiovascular center in southern China. Moreover, the sample size included in the study is large enough and patients come from different regions, which provide the results with a certain degree of universality. Second, the velocity and volume of preoperative hydration may influence the incidence of CA-AKI, but they were unrecorded. Third, there are some confounding factors that have not been taken into consideration due to the lack of variables, such as body mass index (BMI), smoking, and other influencing factors. However, special attention was given to avoid biases by adjusting the results in accordance with co-morbidities and clinically relevant in-hospital events. Finally, our database lacks information on hemodynamic disturbances, such as cardiogenic shock or the use of mechanical circulatory support, and coronary-artery-bypass-grafting (CABG) incidence following CAG. Therefore, we may fail to consider the impact of hemodynamic disturbances and post-contrast CABG on the results.
Our study found that dilated LVEDD may be remarkably related to an increased risk of CA-AKI following CAG in patients with CAD. LVEDD is an easily obtained indicator in echocardiogram, which can be performed before CAG to identify the risk of CA-AKI in patients with CAD. Precautionary measures should be taken in the perioperative period for patients with dilated LVEDD, who have a high risk for CA-AKI.
The datasets presented in this study can be found in online repositories. The names of the repository/repositories and accession number(s) can be found in the article/Supplementary Material.
The studies involving human participants were reviewed and approved by Research Ethics Committee of Guangdong Provincial People's Hospital. The patients/participants provided their written informed consent to participate in this study.
YL, JL, and JC contributed to supervision, mentorship, research idea, and study design. QL, SC, HH, WC, BW, WL, SY, LL, MY, RT, ZH, and JD contributed to data acquisition. JL and YL contributed to data analysis/interpretation. SC and QL contributed to statistical analysis. All authors contributed important intellectual content during manuscript drafting or revision and accepts accountability for the overall work by ensuring that questions pertaining to the accuracy or integrity of any portion of the work are appropriately investigated and resolved.
This study was supported by Guangdong Provincial Science and Technology Project (2020B1111170011); by Guangdong Provincial Science and Technology Project (KJ022021049); by Beijing Lisheng Cardiovascular Health Foundation (No. LHJJ20141751); by National Key Research and Development Program Grants of China (2016YFC1301202); and by Guangdong Provincial Key Laboratory of Coronary Heart Disease Prevention (No. 2017B030314041). The funders had no role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript. The work was not funded by any industry sponsors.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fcvm.2022.827524/full#supplementary-material
1. Mehran R, Dangas GD, Weisbord SD. Contrast-associated acute kidney injury. N Engl J Med. (2019) 380:2146–55. doi: 10.1056/NEJMra1805256
2. Clermont G, Acker CG, Angus DC, Sirio CA, Pinsky MR, Johnson JP. Renal failure in the ICU: comparison of the impact of acute renal failure and end-stage renal disease on ICU outcomes. Kidney Int. (2002) 62:986–96. doi: 10.1046/j.1523-1755.2002.00509.x
3. Coca SG, Singanamala S, Parikh CR. Chronic kidney disease after acute kidney injury: a systematic review and meta-analysis. Kidney Int. (2012) 81:442–8. doi: 10.1038/ki.2011.379
4. Coca SG, Yusuf B, Shlipak MG, Garg AX, Parikh CR. Long-term risk of mortality and other adverse outcomes after acute kidney injury: a systematic review and meta-analysis. Am J Kidney Dis. (2009) 53:961–73. doi: 10.1053/j.ajkd.2008.11.034
5. Odutayo A, Wong CX, Farkouh M, Altman DG, Hopewell S, Emdin CA, et al. AKI and long-term risk for cardiovascular events and mortality. J Am Soc Nephrol. (2017) 28:377–87. doi: 10.1681/ASN.2016010105
6. Aleong RG, Mulvahill MJ, Halder I, Carlson NE, Singh M, Bloom HL, et al. Left Ventricular dilatation increases the risk of ventricular arrhythmias in patients with reduced systolic function. J Am Heart Assoc. (2015) 4:e001566. doi: 10.1161/JAHA.114.001566
7. Gaudron P, Eilles C, Kugler I, Ertl G. Progressive left ventricular dysfunction and remodeling after myocardial infarction. Potential mechanisms and early predictors. Circulation. (1993) 87:755–63. doi: 10.1161/01.CIR.87.3.755
8. Narayanan K, Reinier K, Teodorescu C, Uy-Evanado A, Aleong R, Chugh H, et al. Left ventricular diameter and risk stratification for sudden cardiac death. J Am Heart Assoc. (2014) 3:e001193. doi: 10.1161/JAHA.114.001193
9. Pfeffer MA, Braunwald E. Ventricular remodeling after myocardial infarction. Experimental observations and clinical implications. Circulation. (1990) 81:1161–72. doi: 10.1161/01.CIR.81.4.1161
10. Quiñones MA, Greenberg BH, Kopelen HA, Koilpillai C, Limacher MC, Shindler DM, et al. Echocardiographic predictors of clinical outcome in patients with left ventricular dysfunction enrolled in the SOLVD registry and trials: significance of left ventricular hypertrophy. Studies of left ventricular dysfunction. J Am Coll Cardiol. (2000) 35:1237–44. doi: 10.1016/S0735-1097(00)00511-8
11. Vasan RS, Larson MG, Benjamin EJ, Evans JC, Levy D. Left ventricular dilatation and the risk of congestive heart failure in people without myocardial infarction. N Engl J Med. (1997) 336:1350–5. doi: 10.1056/NEJM199705083361903
12. Choi JS, Baek SH, Chin HJ, Na KY, Chae DW, Kim YS, et al. Systolic and diastolic dysfunction affects kidney outcomes in hospitalized patients. BMC Nephrol. (2018) 19:292. doi: 10.1186/s12882-018-1103-2
13. Liu W, Xi Z, Gu C, Dong R, AlHelal J, Yan Z. Impact of major bleeding on the risk of acute kidney injury in patients undergoing off-pump coronary artery bypass grafting. J Thorac Dis. (2018) 10:3381–9. doi: 10.21037/jtd.2018.05.98
14. Wang K, Li HL, Bei WJ, Guo XS, Chen SQ, Islam SMS, et al. Association of left ventricular ejection fraction with contrast-induced nephropathy and mortality following coronary angiography or intervention in patients with heart failure. Ther Clin Risk Manag. (2017) 13:887–95. doi: 10.2147/TCRM.S137654
15. Liu C, Caughey MC, Smith SC Jr, Dai X. Elevated left ventricular end diastolic pressure is associated with increased risk of contrast-induced acute kidney injury in patients undergoing percutaneous coronary intervention. Int J Cardiol. (2020) 306:196–202. doi: 10.1016/j.ijcard.2020.01.064
16. Jneid H, Anderson JL, Wright RS, Adams CD, Bridges CR, Casey DE Jr, et al. 2012 ACCF/AHA focused update of the guideline for the management of patients with unstable angina/non-ST-elevation myocardial infarction (updating the 2007 guideline and replacing the 2011 focused update): a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. (2012) 60:645–81. doi: 10.1016/j.jacc.2012.06.004
17. Kushner FG, Hand M, Smith SC Jr, King SB 3rd, Anderson JL, Antman EM, et al. 2009 focused updates: ACC/AHA guidelines for the management of patients with ST-elevation myocardial infarction (updating the 2004 guideline and 2007 focused update) and ACC/AHA/SCAI guidelines on percutaneous coronary intervention (updating the 2005 guideline and 2007 focused update) a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. (2009) 54:2205–41. doi: 10.1016/j.jacc.2009.10.015
18. Levine GN, Bates ER, Blankenship JC, Bailey SR, Bittl JA, Cercek B, et al. 2015 ACC/AHA/SCAI focused update on primary percutaneous coronary intervention for patients with ST-elevation myocardial infarction: an update of the 2011 ACCF/AHA/SCAI guideline for percutaneous coronary intervention and the 2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction. J Am Coll Cardiol. (2016) 67:1235–50. doi: 10.1016/j.jacc.2015.10.005
19. Lang RM, Badano LP, Mor-Avi V, Afilalo J, Armstrong A, Ernande L, et al. Recommendations for cardiac chamber quantification by echocardiography in adults: an update from the American society of echocardiography and the european association of cardiovascular imaging. J Am Soc Echocardiogr. (2015) 28:1–39.e14. doi: 10.1016/j.echo.2014.10.003
20. Moriyama N, Ishihara M, Noguchi T, Nakanishi M, Arakawa T, Asaumi Y, et al. Admission hyperglycemia is an independent predictor of acute kidney injury in patients with acute myocardial infarction. Circ J. (2014) 78:1475–80. doi: 10.1253/circj.CJ-14-0117
21. Murphy SW, Barrett BJ, Parfrey PS. Contrast nephropathy. J Am Soc Nephrol. (2000) 11:177–82. doi: 10.1681/ASN.V111177
22. Levey AS, Stevens LA, Schmid CH, Zhang YL, Castro AF 3rd, Feldman HI, et al. A new equation to estimate glomerular filtration rate. Ann Intern Med. (2009) 150:604–12. doi: 10.7326/0003-4819-150-9-200905050-00006
23. Nutritional anaemias,. Report of a WHO Scientific Group. World Health Organization Technical Report Series (1968). Available online at: https://apps.who.int/iris/handle/10665/40977
24. Al-Mubarak AA, Grote Beverborg N, Anker SD, Samani NJ, Dickstein K, Filippatos G, et al. A clinical tool to predict low serum selenium in patients with worsening heart failure. Nutrients. (2020) 12:2541. doi: 10.3390/nu12092541
25. Harkness A, Ring L, Augustine DX, Oxborough D, Robinson S, Sharma V. Normal reference intervals for cardiac dimensions and function for use in echocardiographic practice: a guideline from the british society of echocardiography. Echo Res Pract. (2020) 7:G1–18. doi: 10.1530/ERP-19-0050
26. Fähling M, Seeliger E, Patzak A, Persson PB. Understanding and preventing contrast-induced acute kidney injury. Nat Rev Nephrol. (2017) 13:169–80. doi: 10.1038/nrneph.2016.196
27. Marenzi G, Lauri G, Assanelli E, Campodonico J, De Metrio M, Marana I, et al. Contrast-induced nephropathy in patients undergoing primary angioplasty for acute myocardial infarction. J Am Coll Cardiol. (2004) 44:1780–5. doi: 10.1016/j.jacc.2004.07.043
28. Mehran R, Aymong ED, Nikolsky E, Lasic Z, Iakovou I, Fahy M, et al. A simple risk score for prediction of contrast-induced nephropathy after percutaneous coronary intervention: development and initial validation. J Am Coll Cardiol. (2004) 44:1393–9. doi: 10.1016/j.jacc.2004.06.068
29. Andò G, Morabito G, de Gregorio C, Trio O, Saporito F, Oreto G. The ACEF score as predictor of acute kidney injury in patients undergoing primary percutaneous coronary intervention. Int J Cardiol. (2013) 168:4386–7. doi: 10.1016/j.ijcard.2013.05.049
30. Linzbach AJ. Heart failure from the point of view of quantitative anatomy. Am J Cardiol. (1960) 5:370–82. doi: 10.1016/0002-9149(60)90084-9
31. Seko Y, Kato T, Morita Y, Yamaji Y, Haruna Y, Izumi T, et al. Age- and body size-adjusted left ventricular end-diastolic dimension in a japanese hospital-based population. Circ J. (2019) 83:604–13. doi: 10.1253/circj.CJ-18-1095
Keywords: acute kidney injury, dilated left ventricular end-diastolic diameter, predictor, coronary angiography, coronary artery disease
Citation: Li Q, Chen S, Huang H, Chen W, Liu L, Wang B, Lai W, Yi S, Ying M, Tang R, Huang Z, Deng J, Chen J, Liu J and Liu Y (2022) Dilated Left Ventricular End-Diastolic Diameter Is a New Risk Factor of Acute Kidney Injury Following Coronary Angiography. Front. Cardiovasc. Med. 9:827524. doi: 10.3389/fcvm.2022.827524
Received: 03 December 2021; Accepted: 28 February 2022;
Published: 28 March 2022.
Edited by:
Gian Marco Rosa, San Martino Hospital (IRCCS), ItalyReviewed by:
Jerzy Chudek, Medical University of Silesia, PolandCopyright © 2022 Li, Chen, Huang, Chen, Liu, Wang, Lai, Yi, Ying, Tang, Huang, Deng, Chen, Liu and Liu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yong Liu, bGl1eW9uZ0BnZHBoLm9yZy5jbg==; Jin Liu, bGphdzM5NzAxNzU2OEAxNjMuY29t
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.